
Abstract
This study aimed to examine autonomic nervous system responses during motor imagery (MI) in healthy adults, using different autonomic markers that reflect cardiac vagal activity and electrodermal activity. 24 healthy individuals were included in this study. Demographic data were assessed using a demographic data form, and MI ability was assessed using mental chronometry, mental rotation, and the Kinesthetic and Visual Imagery Questionnaire (KVIQ-20). Heart rate (HR), heart rate variability (HRV), and electrodermal activity (EDA) were recorded during each 5-min relaxation and MI sessions. HR and HRV were measured using a Polar H10 device, while EDA was measured using the BIOPAC MP36 system. During MI, decreased HRV parameters reflecting cardiac vagal activity, such as Root Mean Square of Successive Differences (RMSSD) and high frequency (HF) band power, were observed (p < 0.05 for all). In addition, significant increase was found in EDA values reflecting electrodermal activity during MI (p < 0.001). Residualized HR was strongly positively correlated with KVIQ-Visual scores (r = 0.511), moderately positively correlated with KVIQ-Total (r = 0.497) and Left-hand accuracy (r = 0.441) scores, while a moderately negative correlation was found between residualized HR and Left-hand reaction time (r = −0.466) (p < 0.05 for all). In conclusion, when assessing MI sessions and MI ability, it is important to use different autonomic indicators (e.g., HRV and EDA) together. The findings suggest that autonomous responses observed during MI may reflect different physiological mechanisms, offering significant implications for the potential use of autonomous biomarkers in MI-based rehabilitation interventions.
Keywords
Introduction
Motor imagery (MI), located at the intersection of cognitive neuroscience and rehabilitation, is defined as a dynamic state in which the representation of a specific motor action, consciously controllable by the individual, is replayed internally in working memory without any explicit motor output (Guillot & Collet, 2010). MI is not merely a process of imagination, but a dynamic mental process based on the reprocessing of motor action in working memory. This is clearly supported by the fact that the cortical and subcortical networks activated during MI overlap to a large extent with those engaged during actual motor execution (Lotze & Halsband, 2006). This neural overlap has made MI a critical tool over the years in various fields, such as improving neuromuscular control, enhancing sports performance, and especially accelerating neurological rehabilitation processes (Schuster et al., 2011). However, the implicit nature of MI makes it difficult to objectively assess the extent to which an individual mentally engages in the MI process and the MI ability.
There are numerous methods in the literature to assess MI ability, including psychometric, behavioral, and psychophysiological approaches (Collet et al., 2011). One of these is the recording of changes in the autonomic nervous system (ANS). During MI, preparatory signals originating in the motor cortex simultaneously modulate the ANS. This modulation results in fluctuations in heart rate (HR), electrodermal activity (EDA), and heart rate variability (HRV) (Collet et al., 2013; Guillot & Collet, 2010; Oishi & Maeshima, 2004). Therefore, autonomic responses can be considered as a concrete indicator of the mental effort and bodily embodiment shown during MI (Decety et al., 1991). Among autonomic measures, HRV and EDA represent partially different physiological mechanisms. Therefore, they can provide important complementary information about ANS activity during MI. While EDA is considered a direct and relatively specific indicator of sympathetic activity HRV, particularly vagal-mediated indices such as root mean square of successive differences (RMSSD) and high-frequency (HF) power, is widely accepted as a non-invasive marker of cardiac parasympathetic modulation and attention regulation (Shaffer & Ginsberg, 2017; Thayer et al., 2012).
While the existing literature examining autonomic responses during MI is promising, most studies are constrained by methodological and theoretical limitations. The distinction between physiological arousal and attentional processes remains unclear (Porges, 1995; Wallin, 1981). Most studies tend to treat autonomic responses as a general “sympathetic activation” (e.g., increased skin conductance). While general physiological arousal is predominantly associated with sympathetic activation, attentional control and self-regulation processes are closely linked to vagal (parasympathetic) modulation (Porges, 1995; Thayer et al., 2012). According to neurovisceral integration models, vagal-mediated HRV is thought to reflect the functional integrity of central autonomic networks involved in attentional regulation, inhibitory control, and adaptive cognitive processing (Thayer & Lane, 2009). Due to the nature of MI, individuals need to maintain introspective attention, monitor body-related representations, and retain the simulated action in working memory without overt action. Therefore, autonomic responses observed during MI may not only reflect non-specific physiological arousal but also represent the underlying attentional and self-regulation processes of the mental simulation of the action.
Therefore, the primary aim of this exploratory study is to characterize ANS responses during MI using multimodal autonomic measures (HRV and EDA) and to examine the relationship between these physiological responses and psychometric and behavioral indicators of MI ability.
Materials and Methods
Study Design and Location
This study was conducted using a within-subject repeated-measures experimental design, in which all participants completed both the relaxation and MI conditions. The manuscript was reported according to the STROBE checklist. The study was approved by the Ethics Committee of Kutahya Health Sciences University (Decision No: 2024/05-08). All measurements were conducted in the Physiology laboratory of Kutahya Health Sciences University between May 2024 and July 2024. Individuals signed the voluntary consent form stating that they were willing to participate in the study. All study procedures were conducted according to the principles of Good Clinical Practice (GCP) and the Helsinki Declaration. The study is registered at the Clinical Trial Registry with NCT06482528.
Participants and Recruitment
The study included 24 healthy individuals. The inclusion criteria were being between the ages of 18 and 30, volunteering to participate in the study, not having any neurological or orthopedic disease, and not having any vision, hearing, or speech problems that would prevent the tests. The individuals with a history of pregnancy, any previous disorder or surgery that alters physical performance or physiological functions, prior experience with MI techniques or training, and those receiving treatment with any medication that affects the central nervous system were excluded.
Study Size
A sensitivity analysis (G*Power 3.1) indicated that with n = 24, α = 0.05, and 80% power, the study was able to detect within-subject effects of at least dz ≈ 0.59, meaning that only medium-to-large autonomic changes could be reliably identified (Cohen, 2013; Lakens, 2013).
Measurements
Demographic Data Form
Individuals’ age, self-reported dominant upper extremities, height, weight, presence of neurological and orthopedic problems, and health history data were recorded with a demographic data form.
Mental Chronometry
The mental chronometry provides information about the temporal connection between real and imagined movements. As part of this evaluation, participants were administered Nine-Hole Wood Peg Test. In the study, participant was instructed to place the wooden sticks in the box, one by one, into the holes on the board as quickly as possible with his dominant hand. After that, they were asked to carry out this activity using the MI. MI trials started with the “3-2-1-Start” countdown and ended with the participants indicating that they had finished the placement process by saying “stop”. The total duration of each test was determined by a chronometer. To ensure consistency, all mental chronometry instructions and timing were completed by the same investigator in all subjects (Braun et al., 2017). After practice, mental chronometry index were calculated as follows: |(motor imagery time – action execution time)| (Collet et al., 2011; Lanata et al., 2020).
Mental Rotation
Mental rotation provides information about the accuracy of imagined movements. The test was administered using the Recognize App Recognize Hand software developed and designed by the NOI group (Neuro Orthopedic Institute, Adelaide, Australia) (https://www.noigroup.com/Recognize). In the study, “Vanilla” mode was used for mental rotation ability. Individuals sat at a table in a comfortable position with a tablet in front of them. According to the protocol, the participant must perform the hand-identification task within a maximum of 5 seconds. The percentage of correct responses and reaction time were provided by the application for both hands (Wajon, 2014).
Kinesthetic and Visual Imagery Questionnaire (KVIQ)
Kinesthetic and Visual Imagery Questionnaire (KVIQ) was developed by Malouin et al. in 2007. KVIQ is a questionnaire that consists of movements performed while seated, cannot be self-administered, consists of kinesthetic and visual imagery subsections, and measures how much individuals can visualize and feel the movement. The KVIQ-20 consists of 5 sections, each scored equally on a scale of 1 to 5. For each movement, the individual performs kinesthetic and visual imagery, and this imagery experience is evaluated by the individual using a 1-5 Likert scale (Dilek et al., 2019; Malouin et al., 2007).
Polar H10
Polar H10 is a wearable sensor chest strap device designed for HRV analysis, aiming to provide laboratory-level accuracy. It is a frequently used device in sports and health that works on the ECG-based measurement principle. The device detects R–R intervals, which represent the time between successive cardiac R waves, with a 1 ms resolution. Polar H10 has proven its validity in accurately assessing RR intervals during both resting and physical exercise conditions (Gilgen-Ammann et al., 2019). The device uses a sensor with a sampling rate of 1000 Hz. Polar H10 is often used with smartphone apps to record, store, and export data.
In this study, Elite HRV App (Version 5.5.1) was used to export data (Schaffarczyk et al., 2022). The Elite HRV application automatically performs R-R filtering and assigns quality labels (“good,” “okay,” or “poor”) after measurement. The application support documentation states that records with a “poor” label should not be included in the analysis (Vondrasek et al., 2023). In this context, only the measurements marked with the quality label “good” were used for analysis in our study (Two participants were excluded during the analysis.)
In this study, we evaluated HRV parameters including both time domain and frequency domain measurements. In the evaluation of HRV data, parameters that are controversial in the literature for reflecting sympathetic activity, such as low-frequency (LF) and LF/HF ratio, were excluded from the analysis; only time and frequency domain parameters with high evidence level reflecting vagal (parasympathetic) tone and general autonomic capacity were used (Gullett et al., 2023; Thomas et al., 2019). In the time domain, RMSSD is the primary indicator of short-term vagal (parasympathetic) modulation and is the most sensitive indicator of decreased vagal activity. In the frequency domain, HF power (0.15–0.40 Hz) is the most reliable frequency component of the parasympathetic (vagal) tone, and a decrease in this band indicates vagal withdrawal (Gullett et al., 2023).
The following auxiliary parameters were included in the analysis to verify the overall functioning of the system and the quality of the data. Standard deviation of NN intervals (SDNN) represents total ANS activity, reflecting the overall variation across all NN ranges. Mean RR Interval, as the inverse of HR, represents the total effect of the sympathetic and parasympathetic systems on the sinoatrial node. Its shortening during MI represents the overall chronotropic acceleration (increased HR. Total Power represents the total energy of all frequency bands. It reflects the overall variability capacity and physiological flexibility of the ANS. pNN50 represents the percentage of successive RR intervals that differ by more than 50 ms. PNN50 is closely associated with parasympathetic nervous system activity. HF Peak is the peak frequency in the 0.15–0.40 Hz band. It is considered an indicator of Respiratory Rate in the literature. This parameter was used as a control variable to verify that participants’ respiratory rates were within the reliable range (0.15–0.40 Hz) for HRV analysis (Basri & Turki, 2025; Electrophysiology, 1996; Quintana et al., 2016; Shaffer & Ginsberg, 2017).
Electrodermal Activity, Respiratory Frequency, Heart Rate and Heart Rate Frequency
EDA, respiratory frequency (RF), HR, and heart rate frequency (HRF) were recorded in the Physiology Research Laboratory of the Faculty of Medicine of X University in a quiet environment with low light and a room temperature of approximately 21°C. EDA was measured via skin conductance (µS) using the BIOPAC MP36 data acquisition system. For EDA recording, Ag/AgCl surface electrodes were placed on the distal phalanges of the second and third fingers and connected to the BIOPAC MP36 system. EDA (skin conductance level), and HR were recorded simultaneously in both the relaxation and MI sessions (Benedek & Kaernbach, 2010; Boucsein, 2012). Respiratory rate was recorded directly using a Respiratory Effort Transducer placed around the chest during the measurement.
Intervention
Template for Intervention Description and Replication (TIDieR Template)
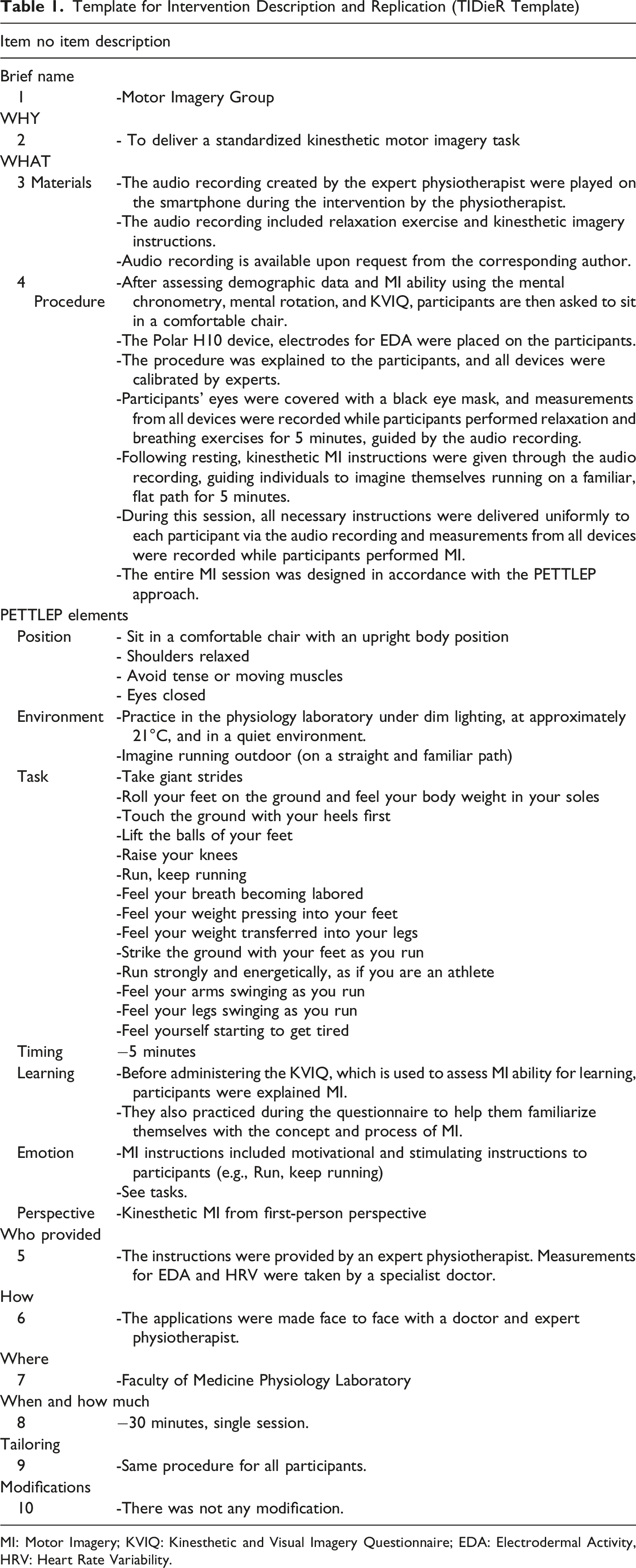
MI: Motor Imagery; KVIQ: Kinesthetic and Visual Imagery Questionnaire; EDA: Electrodermal Activity, HRV: Heart Rate Variability.
Bias
Since the order of conditions was kept constant, possible order effects (habituation, anticipatory responses) were considered a potential limitation of the method.
Statistical Analyses
IBM SPSS Statistics Standard Concurrent User V 26 (IBM Corp., Armonk, New York, USA) and MedCalc® Statistical Software version 19.6 (MedCalc Software Ltd, Ostend, Belgium) statistical software packages were used to analyze the data. The normality assumption of the data was evaluated by examining the Shapiro-Wilk test and Skewness-Kurtosis coefficients. Descriptive statistics were presented as frequency, percentage, mean, standard deviation, median, minimum, and maximum values. To assess changes in ANS responses during MI, all physiological parameters recorded in the resting and MI conditions were analyzed using the Wilcoxon Signed Rank Test because they were paired data and the assumption of normality was not met. Median values for each variable in the resting and MI conditions were reported. The direction of the difference between the two conditions was indicated according to whether the test statistic was based on positive or negative ranks. Furthermore, effect sizes were calculated and presented using the formula r = Z/√N. An effect size between 0 and 0.19 is considered negligible; between 0.2 and 0.49 is considered small; between 0.5 and 0.79 is considered medium; and 0.8 or greater is considered large (Cohen, 2013). To most accurately determine the autonomic response elicited during MI, the distributional properties and baseline-outcome relationships of baseline and task (MI) measurements were examined in preliminary analyses. The high Skewness of the variables and the strong positive correlations between baseline and task measurements for HR (r = .887) and RMSSD (r = .826) indicated that simple difference scores were strongly influenced by initial levels. Therefore, to eliminate the influence of baseline values and isolate true autonomic responses, Residualized Change Scores were used. This was accomplished by simple linear regression of task values (MI) onto baseline values, and the resulting unstandardized residuals were used in the analyses. Relationships between MI ability variables (KVIQ, mental rotation, mental chronometry) and residualized autonomic responses were assessed using the Spearman Rank Correlation Coefficient (r) due to non-normal distribution assumptions. The magnitude of correlation coefficients was interpreted according to Cohen’s (1988) criteria: r = 0.10-0.29 was considered small, r = 0.30-0.49 was considered moderate, and r > 0.50 was considered large (Cohen, 1988). p-value of <0.05 was considered statistically significant.
Results
Demographic Characteristics and Motor Imagery Abilities of the Participants (n = 24)
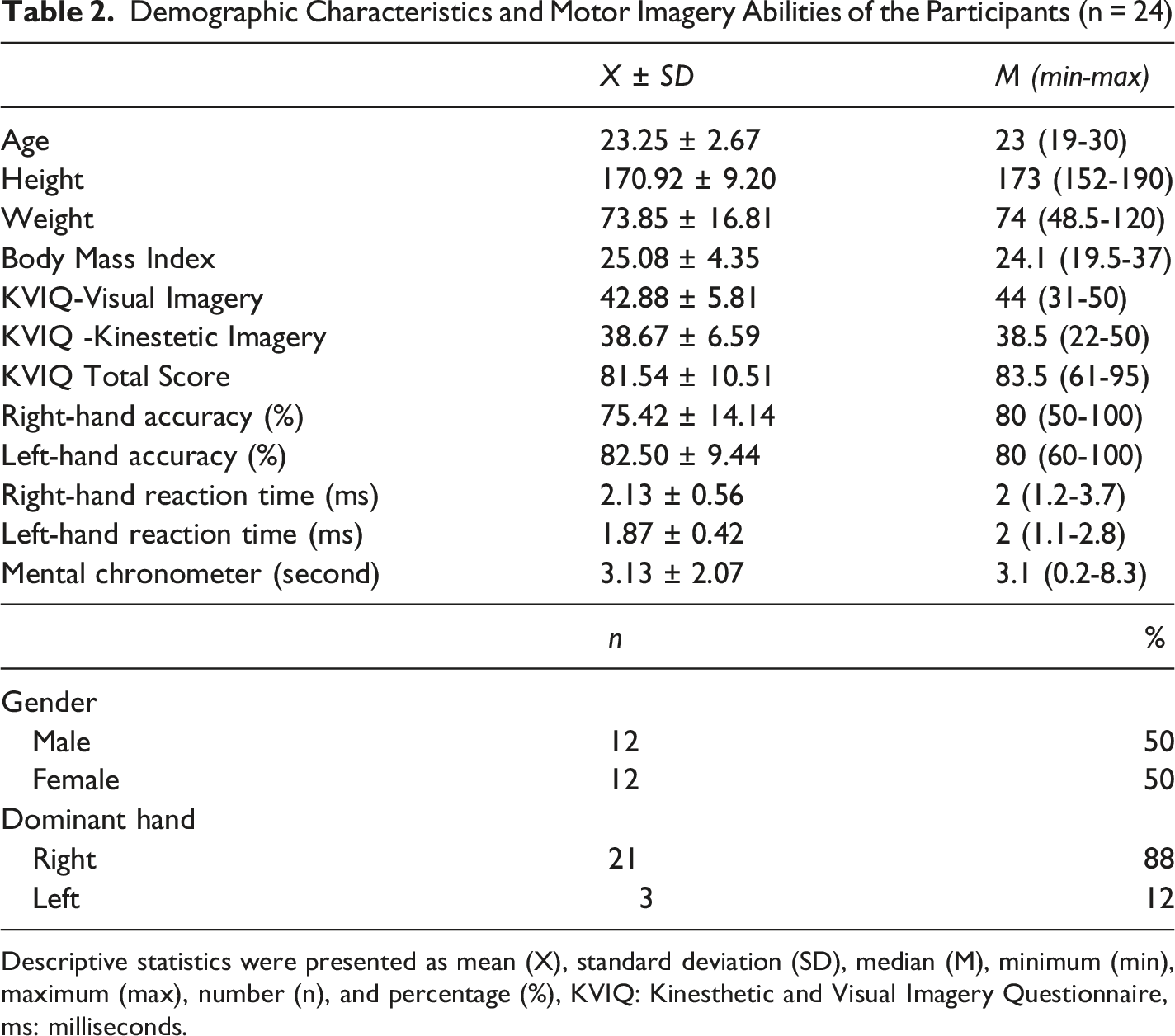
Descriptive statistics were presented as mean (X), standard deviation (SD), median (M), minimum (min), maximum (max), number (n), and percentage (%), KVIQ: Kinesthetic and Visual Imagery Questionnaire, ms: milliseconds.
Comparison of Autonomic Responses Between Resting and Motor Imagery Conditions
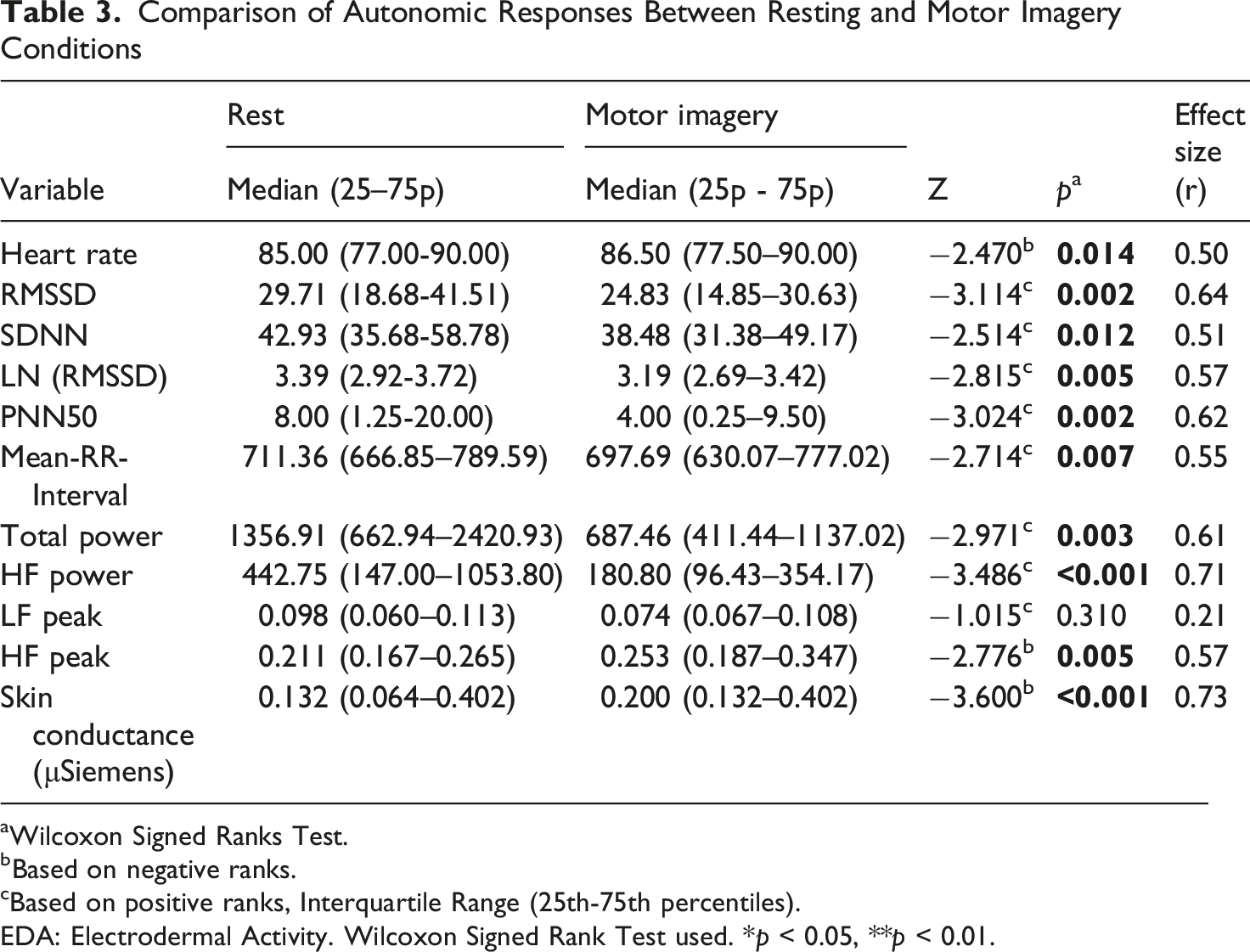
aWilcoxon Signed Ranks Test.
bBased on negative ranks.
cBased on positive ranks, Interquartile Range (25th-75th percentiles).
EDA: Electrodermal Activity. Wilcoxon Signed Rank Test used. *p < 0.05, **p < 0.01.
Spearman Correlation Analysis Between Assessment Tools (N = 24)
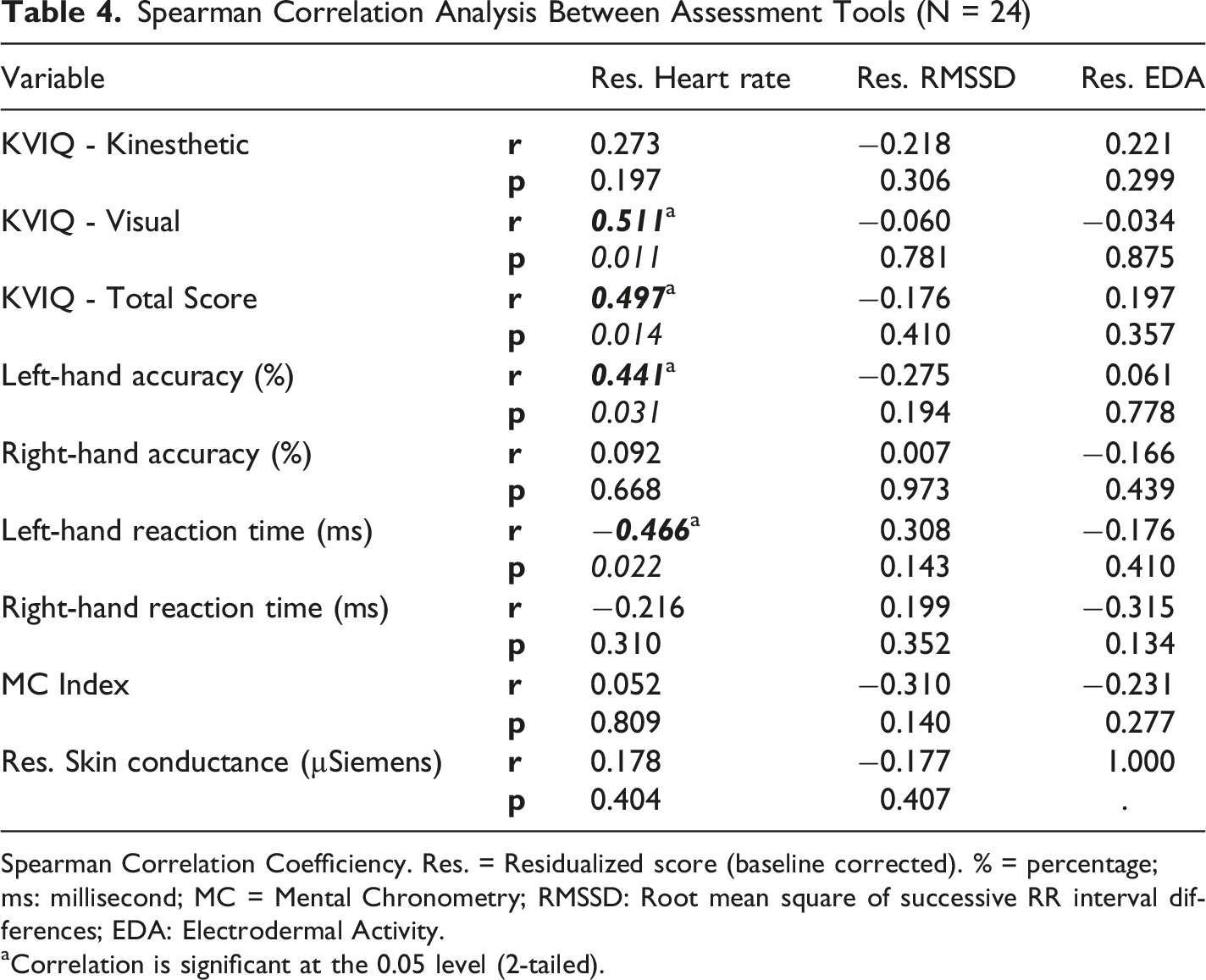
Spearman Correlation Coefficiency. Res. = Residualized score (baseline corrected). % = percentage; ms: millisecond; MC = Mental Chronometry; RMSSD: Root mean square of successive RR interval differences; EDA: Electrodermal Activity.
aCorrelation is significant at the 0.05 level (2-tailed).
Discussion
In this exploratory study, we used multimodal measures (HRV and EDA) to dissociate autonomic responses elicited during a MI session into whether they were due to baseline arousal or specific attentional regulation. We also examined the relationship between these physiological changes and psychometric (KVIQ) and behavioral (mental rotation, mental chronometry) indices of MI ability. Our findings indicate that HRV, an indicator of parasympathetic withdrawal, changes favored parasympathetic withdrawal during MI, and EDA, an indicator of sympathetic nervous system activity, changed favorably during MI. Finally, we found that some MI ability measurements associated with HR. Interestingly, no linear correlation was found between EDA and HRV data in our study.
EDA is a noninvasive peripheral marker of SNS activity. Eccrine sweat glands are controlled solely by the SNS through the release of acetylcholine and lack parasympathetic innervation. Therefore, EDA is considered a direct and relatively specific indicator of sympathetic activity (Visnovcova et al., 2016; Wallin, 1981). The increase in skin conductance observed during MI in our study demonstrates that, despite motor inhibition in the somatic system, the ANS maintains its preparation for action. This suggests that the organism is responding to a sympathetic “gas pedal” response and that MI is not merely cognitive rehearsal but a process of energy mobilization appropriate to the metabolic cost of the planned action. These findings are consistent with the literature (Collet et al., 2011, 2013). For example, Oishi et al. and Cuenca-Martínez et al. found a significant increase in electrodermal activity during MI compared to rest in their study (Cuenca-Martínez et al., 2018; Oishi & Maeshima, 2004). The underlying mechanism for this sympathetic activation and arousal observed during MI is based on central programming and energy mobilization processes implemented by the central nervous system. Current MI models describe MI as a process in which internal “forward models” within the motor system are executed offline, generating predictions regarding the sensory and metabolic consequences of the planned action (Hurst & Boe, 2022; Ridderinkhof & Brass, 2015). MI mobilizes the body’s physiological resources as if preparing for execution of movement and makes the body physiologically ready to expend energy (Jackson et al., 2001; Jeannerod, 1994, 1995). These findings support that EDA can serve as an objective physiological indicator of participation during MI interventions. MI-based rehabilitation protocols are increasingly used in neurological rehabilitation, sports rehabilitation, and pain management. Monitoring EDA during these protocols can help clinicians determine whether patients are actively participating in the imagery process rather than passively following instructions. This can be particularly important in patient with limited motor output or impaired communication ability, such as those with stroke, Parkinson’s disease, or severe motor disability, where behavioral verification of MI participation may be challenging (Mulder, 2007).
HRV is a complex output of sympathetic and parasympathetic interactions on the sinoatrial node and is a critical biomarker reflecting the physiological flexibility of the organism (Electrophysiology, 1996; Shaffer et al., 2014). The strongest consensus in HRV analysis is on the measurement of vagal (parasympathetic) tone (Gullett et al., 2023). HRV analysis provides important information, especially in monitoring parasympathetic (vagal) activity (RMSSD, HF) (Electrophysiology, 1996). In our study, the increase in HR, RMSSD, SDNN, and HF during the MI condition compared to the relaxation session indicate a strong pattern of vagal withdrawal and relative sympathetic dominance. Among the time-domain parameters, the decrease in RMSSD indicates vagal withdrawal, while the decrease in HF power in the frequency domain indicates suppression of efferent parasympathetic activity. This pattern is consistent with the widespread view that MI induces a state of motor readiness similar to the physiological responses elicited during preparation for actual movement (Lotze & Halsband, 2006). Studies examining HRV changes during MI sessions are limited in the literature, and findings vary depending on the participant profile and the nature of the MI task. For example, Kiloatar et al. found no statistically significant changes in HRV parameters during MI in patient with stroke (Kiloatar et al., 2024). This situation can be explained by the fact that brain damage and ANS dysfunctions accompanying stroke pathology weaken neuro-cardiac coupling and mask the physiological effects of MI (Chen et al., 2017; de Vries et al., 2011). In contrast, the significant autonomic changes observed in our study with healthy individuals suggest that MI can produce powerful physiological outcomes in an intact nervous system. On the other hand, Pinto et al., in their study examining different MI strategies, reported that the first-person (kinesthetic) perspective produced greater sympathetic activation than the third-person (visual) perspective, but found no significant differences between strategies in other HRV parameters (Peixoto Pinto et al., 2017). The limited autonomic response in this study may be related to the metabolic demands of the MI task. During MI, the autonomic system generates a motor readiness state proportional to the energy cost of the imaged movement (Decety et al., 1991, 1993; Fusi et al., 2005). Contrary to studies in the literature, in our study, when participants imagined a task requiring high effort and whole-body coordination, such as ‘running on a familiar path’, and having a high metabolic cost, the autonomic system was mobilized more strongly. Specifically, RMSSD and HF-power support the idea that HRV parameters transmitted via the vagal nerve can provide useful information about the physiological load and attention requirements associated with MI. Monitoring HRV responses during MI can help clinicians better understand whether the patient is adequately engaged in the MI task and contribute to the individualization of MI-based rehabilitation protocols. Furthermore, the observed autonomic responses support the view that MI is not merely a passive cognitive rehearsal, but a physiologically embodied process capable of activating central autonomic and motor readiness networks even in the absence of overt movement (Decety, 1996; Jeannerod, 2001).
Our findings reveal a physiological picture characterized by a pronounced vagal withdrawal in HRV parameters (RMSSD, HF) and a concomitant increase in EDA (sympathetic activation). The lack of a significant association between EDA and HRV in our study suggests that the autonomic responses observed during MI may partly reflect different physiological processes. However, given the exploratory nature of the current study, these findings should be interpreted cautiously. EDA has been shown to be an arousal indicator primarily based on sympathetic sweat gland activity, whereas vagally mediated HRV reflects the functional integrity of prefrontal-subcortical neurovisceral networks involved in attention, executive function, and emotional regulation (Critchley, 2002; Forte et al., 2019; Park et al., 2013; Porges, 1995; Thayer & Lane, 2000). Our findings suggest that the observed decrease in RMSSD and HF during MI can be interpreted as a task-specific sustained attention cost, indicating that this vagal brake is partially disengaged as attention is directed to the internal motor representation.
Our current findings support the idea that MI occurs with measurable autonomic changes involving both cardiac autonomic modulation and sympathetic electrodermal activation. This could have significant implications for clinical practice, particularly in neurorehabilitation settings where MI is frequently used to facilitate motor recovery despite limited physical movement capacity. Assessment of HRV and EDA together can provide clinicians and researchers with complementary physiological information about task engagement, attention requirements, and autonomic load during MI implementation. Such multimodal autonomic monitoring could contribute to the development of more individualized and physiologically informed MI interventions in conditions such as stroke, Parkinson’s disease, chronic pain, and multiple sclerosis.
Finally, no strong and widespread correlation was found between measurements reflecting MI abilities (KVIQ subscales, mental rotation accuracy and duration, mental chronometry error) and residualized values of autonomic responses (HR, RMSSD, EDA) during MI. Only moderate positive correlations were found between residualized HRe and KVIQ-Visual and KVIQ-Total scores, as well as positive correlations with left-hand mental rotation accuracy and negative correlations with left-hand mental rotation duration. These findings suggest that as visual imagery vividness and left-sided spatial rotation performance increase, increased HR becomes more pronounced during MI. In contrast, the fact that the change in RMSSD, a vagally mediated HRV parameter, and EDA responses did not show a significant relationship with either the KVIQ or mental rotation and mental chronometry indicators indicates that the physiological and cognitive dimensions of MI are partially dissociated. This pattern suggests that MI is not a unidimensional capacity. This is consistent with the literature highlighting that different components of cognitive function are captured by self-report measures, mental rotation/chronometry performance, and ANS indicators (Collet et al., 2011). While psychometric vividness scales and timing/accuracy measures reflect trait-like characteristics such as imagery’s representational quality, strategy use, and cognitive efficiency; residualized HR, RMSSD, and EDA values are state indicators representing the physiological costs of MI at that moment, namely, arousal and attentional/regulatory control load. Furthermore, the fact that autonomic variables were treated as residualized in this study, purified from the baseline, is intended to capture task-specific, dynamic responses rather than individual initial levels. Therefore, the observation of weak correlations between trait-level MI ability and this “pure task cost” is methodologically expected. This suggests not the absence of physiological effects of MI, but rather that MI ability and the autonomic load of MI are distinct but complementary dimensions of the same phenomenon, and that these dimensions should be considered separately in clinical practice and research. However, the exploratory nature of the current design does not allow for a definitive separation of effects related to motor imagery from effects related to attention, emotion, breathing, or sequencing. More comprehensive studies are needed to clarify this.
This study has several limitations. First, only one specific MI task (running on a familiar track) was used in the study. It is known in the literature that different motor tasks (e.g., fine motor skills or static tasks requiring strength) can produce different autonomic response profiles. Therefore, the results cannot be generalized to all types of MI. Second, the sample size was relatively small (n = 24) and comprised a young, healthy group, likely with similar characteristics. This limits the generalizability of our study’s results to all populations. Finally, although participants were assessed under standardized laboratory conditions, various factors known to influence autonomic parameters, such as individual stress levels, respiratory patterns, physical fitness, sleep quality, caffeine intake, and baseline psychological status, were not directly controlled. Since HRV parameters are particularly sensitive to these physiological and psychological variables, their potential impact on autonomic responses during MI should be considered when interpreting the findings. Future studies with larger sample sizes and tighter control of autonomic confounding factors are needed to better isolate MI-specific physiological effects.
Conclusions
In conclusion, our findings contribute to the literature suggesting that MI is not merely a cognitive process but also involves measurable autonomic and physiological responses associated with motor readiness and internal action simulation. Clinically, the combined assessment of HRV and EDA may provide complementary information about autonomic involvement during MI implementation and help improve physiological monitoring of MI-based interventions in rehabilitation settings. However, given the exploratory nature of the present study, these findings should be interpreted cautiously. Future studies involving larger and more diverse populations, different mental imagery tasks, and more rigorous control of potential autonomic confounding factors are needed to better elucidate the relationship between autonomic responses, attention regulation, and mental imagery ability.
Footnotes
Acknowledgement
We would like to thank our research participants.
Ethical Considerations
The study was approved by the Ethics Committee of Kutahya Health Sciences University (Decision No: 2024/05-08).
Author contributions
MI: Supervision, Writing – original draft, Methodology, Conceptualization, Data curation. AAD: Writing – original draft, Methodology, Conceptualization, Data curation. AK: Supervision, Writing – review & editing, Methodology, Conceptualization. ET: Writing – review & editing, Methodology, Conceptualization, Data curation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors state that they have no known financial conflicts of interest or personal relationships that could have influenced the work presented in this paper.
Data Availability Statement
The dataset is available from the corresponding author on reasonable request.
Clinical Trials Registration
The study is registered at the Clinical Trial Registry with NCT06482528.