
Abstract
Background
The purpose of this study was to explore the alignment of caregivers’ perceptions and expectations of their preschool-aged children’s physical activity (PA) and motor competence (MC) with children’s actual performance located within the rural southeastern United States. Emphasizing a systems approach, we identified gaps in caregiver understanding of PA and MC to inform future interventions targeting health disparities in young children.
Method
A collective case study design involved 11 caregiver-child dyads from the southeastern United States. Data included caregiver interviews and visual representations of their children’s PA alongside objective measures of PA, body mass index, and MC. Analyses followed a two-phase process through the examination of individual case narratives and cross-case synthesis for emergent themes.
Results
Five key themes were identified: (1) caregivers’ high valuation of PA; (2) vague definitions of PA; (3) overestimation of child PA levels; (4) limited awareness of MC; and (5) differences in PA engagement (sport-oriented vs. general PA). Caregivers consistently valued PA but often misjudged their children’s PA levels and MC. Child step-counts were low-to-average, with only about half reaching the equivalent of 60–100 minutes per day, highlighting discrepancies between perceived and actual PA.
Conclusion
Findings highlight the need for accessible caregiver education on PA and MC. Tailored community programs through a systems approach could be the next step to bridge gaps in caregiver perceptions and shrink children’s health disparities.
Poverty is a multifaceted and deeply ingrained determinant of health, with both proximal and distal health factors impacting those experiencing poverty (Aidoo, 2023). As of the 2020 U.S. Census, the poverty rate for individuals under 18 years old rose 16.1% (Creamer et al., 2022). This upward shift constitutes an increase of 1.1 million children from the previous year and 31.2% of all individuals experiencing poverty. (Creamer et al., 2022) Children experiencing poverty have reduced opportunities to engage in physical activity (PA) and report greater rates of obesogenic behavior (e.g., eating calorie-dense/nutrient-poor food, sedentary lifestyle, poor sleep habits), resulting in a disparity compared to their peers (Hawes et al., 2019). Thus, as Lee and colleagues (2021) highlighted, those looking to remediate the effects of poverty on children need to consider doing so with a preventive focus, as experiencing poverty in childhood often results in adverse health effects into adulthood (e.g., health risk behaviors, general health problems, chronic health problems, and depression).
While some preschool children are meeting the minimum requirement of 60–100 minutes of moderate-to-vigorous physical activity (MVPA) per day, as measured by step count, few meet 24-h movement guidelines (Rico-González et al., 2025), and thus the early childhood obesity epidemic persists (Stierman et al., 2021). Despite substantial efforts and significant resource allocation, PA interventions have resulted in an average increase of only three to 14 minutes of movement per day (Lai et al., 2014; WHO, 2019). To rectify the deficiency in children’s PA levels, they need exposure to interventions that address the underlying mechanisms that predict PA behavior.
Fundamental movement skills (FMS, e.g., body transport and object manipulation skills) and motor competence (MC, e.g., goal-directed movement) are underlying mechanisms supporting PA behavior and developmental trajectories for health in children (Barnett et al., 2022; D'Hondt et al., 2011; Lubans et al., 2010; Stodden et al., 2008). To directly target and improve the results of previous PA interventions, researchers developed an early childhood program called Successful Kinesthetic Instruction for Preschools with Promoting Achievement, Learning, and Success (SKIPping with PALS), further referred to as PALS (Brian et al., 2023). PALS featured a systems approach (e.g., distal) to prevention and remediation through parental, teacher, and child engagement/education. PALS participants showed strong effects for increases in PA behavior and motor skill development (Brian et al., 2023; Campbell et al., 2024).
To better understand why PALS succeeded when many other PA programs failed, parent perceptions and expectations were examined as suspected facilitators for participating (Campbell et al., 2024). Facilitators included access to resources (which were previously unavailable) and understanding the multiple benefits for children’s well-being by teachers and parents (Campbell et al., 2024). These findings align with expectancy-value theory (EVT), which posits that individuals’ beliefs about competence and the value they assign to a behavior are key drivers of motivation and engagement (Wigfield & Eccles, 2000).
The PALS program was grounded in EVT, which hypothesizes that achievement-related choices are motivated by a combination of individuals’ expectations for success (Wigfield & Eccles, 2000) and subjective task value (Eccles, 1983). For example, outcomes (e.g., attending PALS, participating in PA, etc.) could be predicted by the interaction between confidence and valuation. Thus, if one creates a transformative learning environment that focuses on increased confidence built in a fun and engaging environment, children and their families should be motivated to engage with the outcome of interest (Wigfield et al., 2012). Furthermore, as motivation increases, so does valuation; the greater the valuation, the lesser the impact that perceived barriers have upon outcomes (Wigfield & Eccles, 2002; Wigfield et al., 2012).
An abundance of evidence supports theoretically driven pathways within EVT in various educational contexts (Shang et al., 2023; Sin et al., 2022; Wang & Xue, 2022). Within the majority of the extant EVT literature, participants tended to be older youth (Shang et al., 2023) who self-reported feelings of amotivation, low self-expectations/confidence, and structural barriers (Wigfield & Gladstone, 2019), including no family support and a lack of transportation. Thus, intervention strategies tended to target improving motivation through confidence-building and skill improvement (Shang et al., 2023). However, overestimation/confidence can be just as debilitating as low confidence (Lee, 2021).
Overestimation of one’s health can have dangerous consequences in later life (Hamm et al., 2017). Plausibly, parents who have inaccurate expectations for their children may unintentionally promote a maladaptive developmental trajectory for long-term health due to a lack of awareness of the issue at hand (Hamm et al., 2017). For example, if caregivers overestimate their children’s motor skills and/or do not realize that their children are not developing their motor skills with enough proficiency, then attention to motor skill learning may not occur. Given that today’s children are showing a secular decline in motor skills (Brian et al., 2019), obesity rates are rising (Cunningham et al., 2014), and sedentary behavior rates are surging (Jones et al., 2013), promoting a systems-approach to prevention (via learning and improving motor skills) and potentially adjusting parental expectations is warranted. However, little is known regarding caregivers’ perceptions as well as their expectations for and valuation of children’s health-enhancing behavior (e.g., motor skills and PA). Applied to the early childhood context, parents’ expectations and perceptions of their child’s abilities and the importance of PA may play a critical role in shaping children’s participation in PA. However, while these perceptions are likely influential, it remains unclear how accurately they reflect children’s actual behaviors and performance. This warrants further investigation, as discrepancies between perceived and actual ability may have important implications for children’s engagement and outcomes in PA contexts. Thus, the purpose of this study was to explore and describe the alignment between caregivers’ expectations and valuations of PA behavior and motor skill development with actual behaviors of their preschool-aged children.
Method
This study is a secondary analysis of data previously published in Campbell et al., 2024. The purpose of the secondary analysis was to fill the gaps mentioned above regarding alignment between parental perception and the child’s actual behavior. The Institutional Review Board at University of South Carolina approved all procedures. Caregivers provided informed written consent. A collective case study approach (Stake, 1995) with cross-case comparison (Miles et al., 2014) framed the study to explore the relationship between caregiver and child perceptions of PA and actual child PA through multiple lenses and data sources (see below). Each case represented a parent-child dyad with multiple data sources from each member (see below).
Participants and Setting
Participant Demographic Information
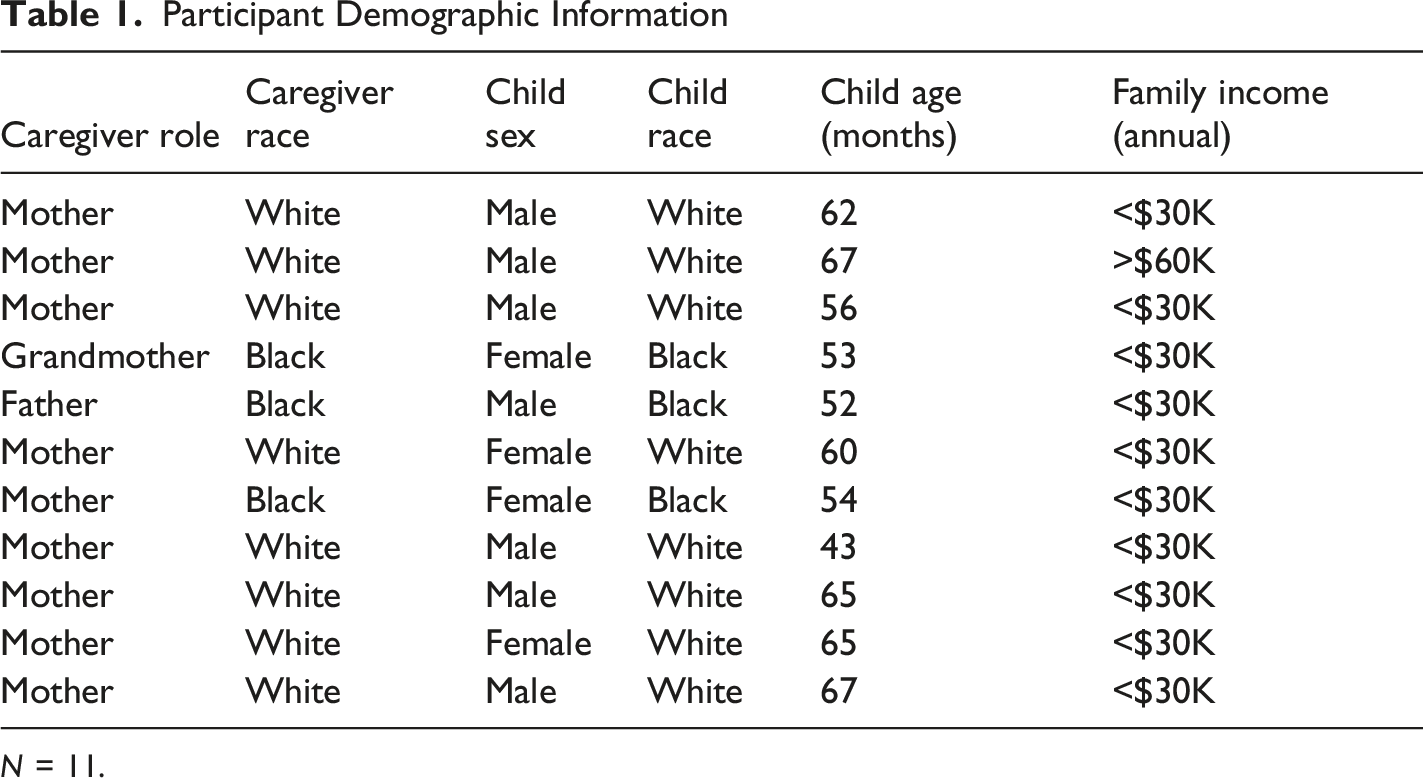
N = 11.
Data Collection Procedures
Each caregiver provided three data points: semi-structured interviews, visual representations of their child’s PA via drawing and talking technique (see below; Angell et al., 2015; Brailas, 2020), and quantitative survey responses. As described in Campbell et al. (2024) via open access, interviews took place in March 2020 after parents had the opportunity to attend six in-person PALS sessions. Semi-structured interviews were conducted over the phone by a member of the research team. Questions focused on exploring caregivers’ definition of PA, perceptions of the amount of time and types of PA in which their child typically engaged, and their perceptions of their child’s skillfulness in locomotor and object control skills. Interviews were transcribed by a member of the research team and checked for accuracy by a second member. A third member of the research team resolved all/any conflicts.
To explore parents’ perceptions of their child’s physical activity (PA) behaviors, a drawing and talking technique was employed (Angell et al., 2015). This qualitative participant-centered method encourages individuals to express their thoughts and experiences through visual representations, which are then elaborated upon through discussion. The approach is particularly useful for eliciting beliefs, perceptions, and tacit knowledge that may be difficult to capture through verbal methods alone (Backett-Milburn & McKie, 1999). This technique has been shown to facilitate reflection and deepen participant engagement, allowing for more nuanced insights into perceptions and experiences compared to traditional interview methods alone (Angell et al., 2015). Each caregiver was asked to “draw a picture of what it looks like when your child is being physically active” without concern for drawing or artistic ability (Brailas, 2020). After completing the sketch, they described the drawing to the interviewer (Figure 1) Sample parent-generated drawings of child PA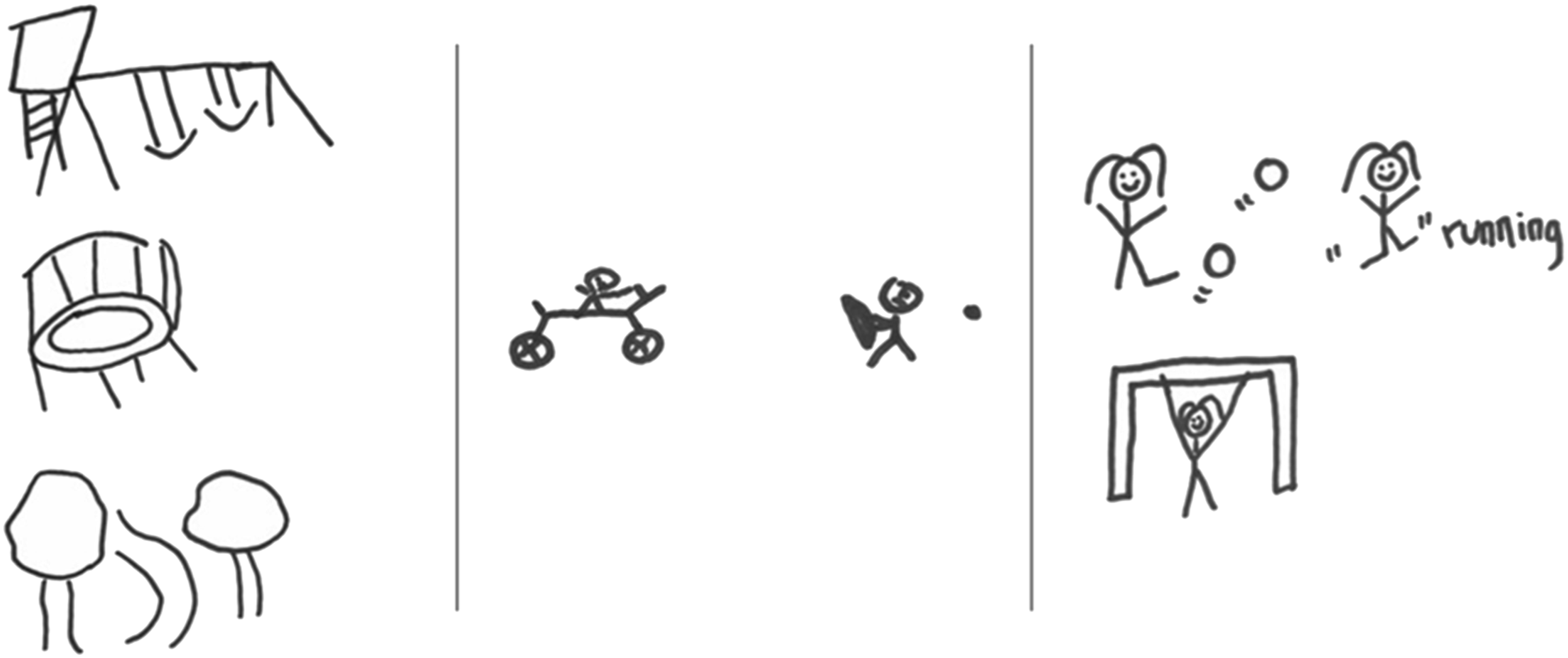
Next, caregivers completed a selection of questions developed by Welk and colleagues (Simpkins et al., 2012; Welk et al., 2003;) regarding parental support of PA behavior and parental PA behavior role modeling. The 15 survey items were psychometrically vetted measures of indirect support for children’s PA behavior (Simpkins et al., 2012; Welk et al., 2003). These items assessed behaviors such as encouragement, facilitation, and parental participation in physical activity, which are thought to influence children’s activity levels through social and environmental pathways. Example items included statements such as, “I encourage my child to be physically active,” “I provide transportation so my child can participate in physical activities,” and “I am physically active myself as a way of setting an example for my child.”
Caregivers responded to each item using a Likert-type scale (e.g., 1 = never to 5 = very often). Items were averaged to create a composite score, with higher values indicating greater levels of parental support and PA role modeling. In prior research, these measures have demonstrated acceptable internal consistency, with Cronbach’s alpha coefficients reported in the range of α = .71–.86 for parental support subscales (Welk et al., 2003) and α = .74–.88 for similar constructs of parental involvement and support (Simpkins et al., 2012). Factor analytic work has supported the multidimensional structure of parental support (e.g., logistical support, encouragement, and modeling), with items loading onto expected factors. Additionally, Simpkins et al. (2012) reported evidence of construct validity through significant associations between parental support and children’s participation in organized and informal physical activity. Where assessed, short-term test–retest reliability has been reported in the moderate range (e.g., r ≈ .60–.80), indicating reasonable temporal stability.
Four sources of data were gathered from each child to capture perceptions of competence, physical activity behavior, Body Mass Index, and motor competence. First, children’s perceived motor skill competence was assessed using the Pictorial Scale of Perceived Movement Skill Competence (Barnett et al., 2016). This instrument uses illustrated scenarios depicting children performing fundamental motor skills (e.g., running, hopping, throwing, catching) and asks participants to indicate which child they are most like and then rate the degree of similarity. Responses are typically scored on a structured four-point scale, with higher scores reflecting greater perceived competence. Item scores are averaged within domains to yield perceived locomotor and perceived object control subscale scores, and in some cases, an overall perceived competence score is calculated. Prior research has demonstrated acceptable internal consistency (α ≈ .70–.85 across subscales) and evidence of construct validity through positive associations with objectively measured motor competence and physical activity (Barnett et al., 2016).
Second, children’s physical activity was measured via average daily step count using the Movband 4 (Engage Moves, LLC). Children wore the device during waking hours over multiple consecutive days, and daily step counts were recorded. Data were screened for valid wear time (e.g., minimum hours per day and minimum number of valid days), and step counts were averaged across valid days to estimate typical daily physical activity. In addition to mean daily steps, variability (e.g., standard deviation across days) can be examined when relevant. Objective monitors such as the Movband have demonstrated strong agreement with other accelerometry-based devices and acceptable reliability for step-based estimates in youth, with intraclass correlation coefficients (ICCs) commonly exceeding .80 under standardized conditions (Mayorga-Vega et al., 2023).
Third, anthropometric data were collected to calculate body mass index (BMI; kg/m2). Body mass was measured using a calibrated Seca digital scale, and standing height was assessed with a Tanita portable stadiometer following standardized protocols (e.g., shoes removed, proper posture alignment). Two measurements are often taken and averaged to improve accuracy when feasible. BMI was calculated as weight (kg) divided by height squared (m2), and values can be further interpreted using age- and sex-specific BMI percentiles or z-scores based on established growth reference standards (e.g., CDC growth charts).
Finally, children’s motor competence was assessed using the Test of Gross Motor Development–Third Edition (TGMD-3; (Webster & Ulrich, 2017). The TGMD-3 evaluates fundamental movement skills across two domains: locomotor skills (e.g., run, gallop, hop, horizontal jump) and ball skills/object control (e.g., two-hand strike, dribble, overhand throw, catch). Each skill consists of multiple performance criteria (typically 3–5 per skill), which are scored dichotomously (1 = criterion present, 0 = criterion absent) across two trials. Scores for each criterion are summed across trials to produce a skill score, which is then summed within domains to yield locomotor and ball skill subscale scores. The TGMD-3 has demonstrated strong psychometric properties, including high inter-rater reliability (ICCs often >.90), internal consistency (α ≈ .85–.95), and evidence of construct and criterion validity across diverse child populations (Webster & Ulrich, 2017).
Interviewers were members of the research team who were either graduate students in exercise science, health, or physical education or possessed a doctoral degree in an allied health field. Three separate members of the research team analyzed the data and generated themes through a content analysis. Each member of the data analysis team possessed a doctoral degree in health education or physical education and experience working with children in the health and physical education setting; however, no members of the research staff who analyzed the transcripts were involved in data collection and held no relationship with the participants in this study, allowing for objective, independent analysis.
Data Analysis
Data analysis was conducted using a qualitative content analysis approach within a cross-case study design informed by (Miles et al., 2014) and proceeded in two phases: (1) within-case analysis through the development of 11 caregiver/child dyad descriptive case study narratives and examination for emergent patterns, followed by (2) cross-case comparison to identify similarities and differences across cases and construct themes. The inductive nature of the analysis was derived from coding the interviews and analyzing them within the context of the quantitative results, with an emphasis on generating meaning through triangulation of multiple information sources. The use of qualitative content analysis, with an emphasis on interpretive coding and meaning making, is consistent with the researcher’s constructivist epistemological approach.
Phase 1 Caregiver/Child Dyad Case Narratives
Interviews were audio-recorded, transcribed verbatim, and analyzed alongside child physical activity and motor competence assessment data. Two researchers summarized and synthesized the collective data into 11 individual descriptive case study narratives: one for each caregiver/child dyad. Each case provided a rich description of the family context, with attention to factors such as caregiver health problems, child disability, and family size. The within-case content analysis narrative then focused on the caregiver’s description and perceptions of PA in general as well as their perceptions of their child’s PA behavior and patterns (e.g., abilities, types, amount), the child’s self-perception of motor competence, and the child’s actual PA and motor competence. Data triangulated across the multiple sources of quantitative and qualitative data within each case were used to develop a summary of the accuracy of the caregiver’s awareness and perceptions of PA and alignment with their child’s actual PA behavior (Patton, 2002; Stake, 1995). Finally, a summary of the unique and salient features of each case was generated by two independent researchers. Verification of the case narrative accuracy and comprehensiveness was conducted by a third researcher.
Phase 2 Cross-Case Analysis
Using the finalized case narratives from Phase 1, two researchers conducted a cross-case content analysis to collectively examine similarities and differences across the cases. Open coding procedures (Strauss & Corbin, 1998) were used to identify recurring patterns, similarities, and differences across cases. Codes were iteratively grouped into broader themes through constant comparison. Emergent themes were reviewed and verified by a third researcher who ensured accuracy and consistency of the data and codes. Analytic decisions and discrepancies were discussed during regular research team debriefing sessions until consensus was reached. Several strategies were used to establish the trustworthiness of the qualitative findings, including data triangulation across interviews and assessment measures, research triangulation through independent coding and verification by multiple researchers, and peer debriefing.
Results
The iterative cross-case comparison by the research team resulted in five key themes as described below:
Theme 1: Caregivers Value PA
Caregivers across all cases indicated that they deeply valued PA, and specifically for their children. Caregivers were asked to rate how important it was for their child to be active on a scale from 1 (not important) to 7 (the most important thing). Scores ranged from 5 to 7. Caregivers also reported that, in comparison to other things that children may do, it was “very” or “extremely” worthwhile for their child to be involved in PA (range = 5–6). Although most of the children had step counts below the daily recommendation, their caregivers wanted them to be active and reported encouraging them to play outside and supporting involvement in sports.
Many caregivers talked about the importance of being active with their children to invest in, connect with, and spend time with them. For example, participant 1 stated, “It initiates family time,” and participant 11 explained, “It’s really given us a bonding time.”
Others noted: “The boys enjoy it. I mean they enjoy my interaction with them and kind of making them feel special about me taking time out of my day just for them” (participant 3). “It’s always fun to be involved with what your kids do and show them that, you know, you care about them, that you’re aware with what goes on in their lives” (participant 5).
Others appreciated the value of PA for the general benefits related to the child’s health and well-being: “I think it’s very important just so you aren’t like, sedentary for health reasons and also it just makes you feel better” (participant 10). “I think that for kids, it’s a developmental need. I think that without it kids do not grow or function the way they should” (participant 1).
While the reasons varied, valuing PA was a theme that spanned all 11 cases. However, the degree to which caregivers modeled PA themselves varied. Only six caregivers reported being physically active regularly for the past six months. These contradictory findings pose a discrepancy between values, perceptions of PA behavior, and actual PA behavior.
Theme 2: Vague Definition of PA
Caregivers seemed to lack a clear understanding of what constitutes PA. Caregivers across all 11 cases defined PA very broadly and included almost anything that is movement related. Examples included: “Just getting up and going. Not sitting around being a lump” (participant 11). “I would say physical activity is any form of moving your body” (participant 8). “Running, climbing. I guess just doing something active like going outside with the ball, baseball. Something besides sitting down” (participant 9).
Approximately half of the caregivers mentioned the concept of elevating one’s heart rate. When asked to give examples of PA, about half listed walking first, and the others mentioned more intense activities such as running, hiking, or mountain climbing. They named a mix of locomotor activities (e.g., run, bike), play (e.g., trampoline, swing), and sport (e.g., baseball, soccer). Some, however, gave examples that would arguably not be considered PA, including swinging on swings (participant 10), bowling (participant 7), and “just busy throughout the day” (participant 5). These findings revealed an inconsistent definition of PA and a misalignment between PA as measured by health professionals and researchers and how it is conceptualized by the average person. Caregivers seemed to know that sedentary behavior is negative; they recognized many benefits of PA, including health and family connectedness, and they wanted their children to be active. Despite this value placed on PA, caregivers did not know exactly how to define it, which is an important factor in assessing the quantity and quality of PA.
Theme 3: Overestimation of PA Behavior/Movement
One clear finding across cases was that caregivers overestimated their child’s movement/PA behavior in relation to recommended standards (Table 2). This contrast was reflected in caregivers’ descriptions of their child’s PA during the interviews. Examples of their perceptions of daily PA included: “Aw man, like all day he’s just running and running, 5-6 hours” [per day] (participant 5). “He is active from the time he wakes up until, like, he goes down, so probably 10 hours a day” (participant 10). “I have two boys, so, honestly, I would think at least 6 hours a day. They're pretty busy. Mine are pretty busy” (participant 3). Caregiver Perceptions of Child PA Compared With Actual PA aEstimated time equivalent was calculated based on suggested evidence that 10,000–14,000 steps/day is associated with 60–100 min of MVPA in preschool children.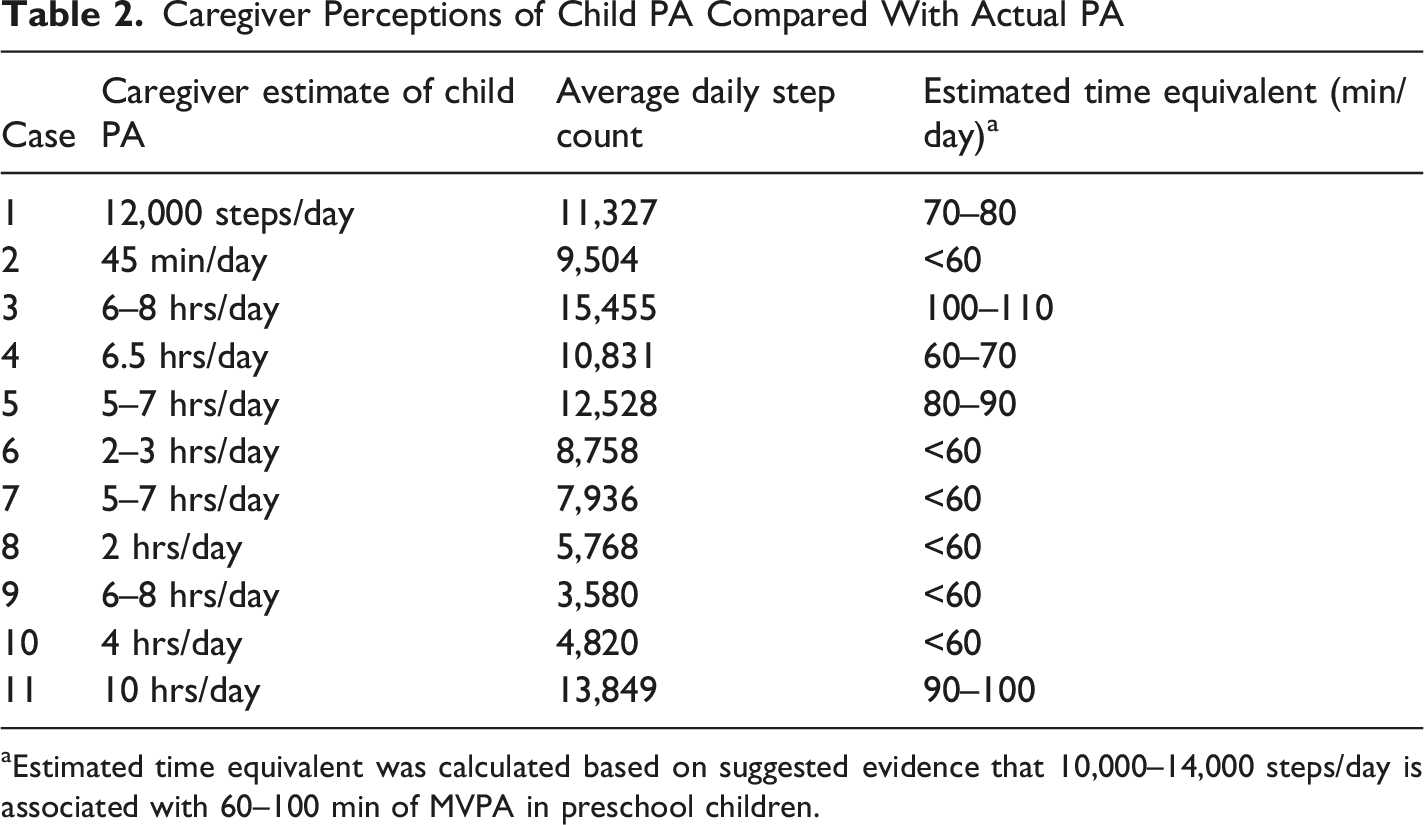
Child step-counts were low-to-average, with only about half reaching the equivalent of 60–100 min per day. This mismatch seems to be related to caregivers’ vague conception of PA and the child’s general energy level. Case 7 illustrates this phenomenon, where the caregiver estimated that her child engages in 5–7 hrs/day of PA on the average weekday. Her drawing depicted a child running, and the caregiver stated that 50% of the child’s daily PA was depicted by the picture, “cuz we play tag, and we’re always running in circles”. This would indicate approximately 3 hours of engaged caregiver-child PA, which was not the reality reflected in the overall case narrative.
Similarly, another caregiver (participant 5) estimated that his child engages in 5–7 hrs of daily PA, stating that 70% of that activity is “walking and bouncing around.” In most cases, caregivers described their child as naturally active and energetic. This seemed to be one of the driving forces for encouraging their child to be active and was reflected in the perceptions of how much PA their children engaged in on an average day. Other examples of these perceptions included: “He has a tendency to just run around and play…he don’t know what sit down means. He’s just energetic, full of energy and fun” (participant 5). “He’s full speed ahead. He’s very athletic” (participant 3). “She’s always running somewhere; she never slows down” (participant 4).
While most caregivers overestimated their child’s PA levels, they were accurate in identifying their child’s activity level relative to other children in the study (e.g., within-sample variability), apart from two cases (participants 7 and 9). However, the overestimation effect was consistent across all cases.
Theme 4: Lack of Awareness of Motor Skill Competence
In addition, there seemed to be a general assumption among caregivers that all children, including their own, naturally know how to perform FMS. Some caregivers were surprised to learn through the PALS program that this was not the case. For example, one caregiver noted: Maybe that the children, although they’re ready to do things physically, aren’t or don’t have the proper motor skills to do them. I guess because you just think that it would be something normal…I mean, I guess the perception of you just thinking, well running is just running. It doesn’t really matter how you run or are you just acting naturally, know how to do those things (participant 6).
While it is true that children generally receive more practice opportunities (devoid of instruction) for locomotor skills (e.g., running, hopping, jumping) organically in the environment, object control skills seem to suffer without intentional instruction and opportunities for practice. (Abusleme-Allimant et al., 2023; Chen et al., 2024) In this sample, the caregivers rarely referenced motor skills or development at all when describing their children’s activity, nor did they differentiate between locomotor skill and object control skill competence. Instead, they conflated movement/PA with skill development, as if skills flowed naturally from an active lifestyle. However, the quantitative data painted a very different picture.
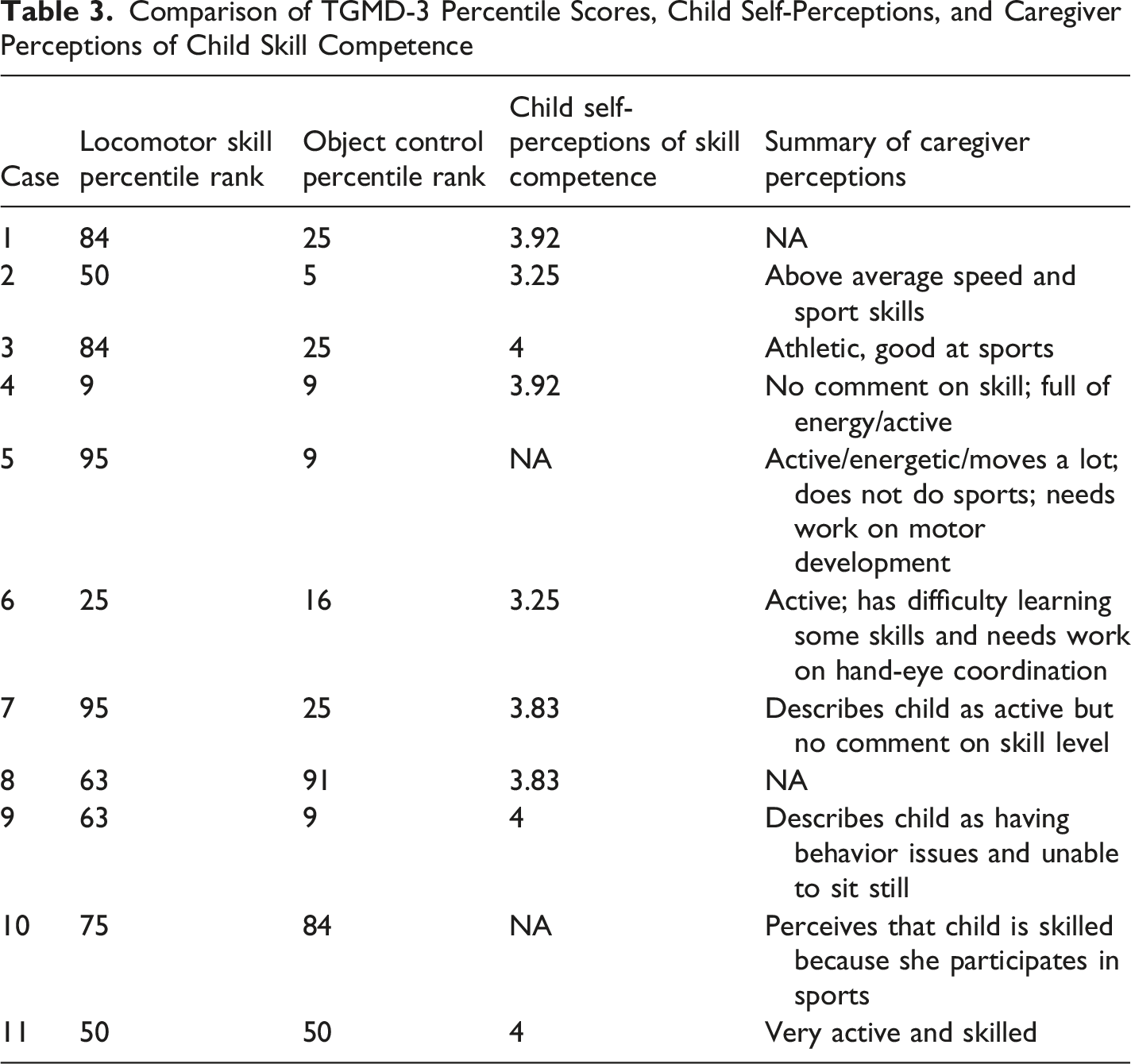
TGMD-3 locomotor skill percentile ranks ranged from 4th to 95th percentile (M = 47.60, SD = 32.44), and seven of 11 children scored above the 50th percentile. These scores somewhat accurately reflect caregivers’ perceptions that their children are active, or at least about as active as the average preschool-aged child, if practice of basic locomotor skills occurs naturally through active play. However, object control percentile ranks told a different story, ranging from the 5th–91st percentile (M = 31.64, SD = 30.38), with only two children scoring above the 50th percentile. These scores are not consistent with caregivers’ perceptions that their child is “athletic” or “good at sports”. This discrepancy may reflect parents’ tendency to equate locomotor skill proficiency with overall activity levels or daily movement, conflating two conceptually distinct constructs.
Only two caregivers noted that their child may need to work on developing their motor skills. Both children scored below the 50th percentile for object control skills, though neither was the lowest, and one of them scored below the 50th percentile for locomotor skills. The other scored the highest (95th percentile rank) for locomotor skills, reflecting a mismatch between parents’ perceptions and actual behavior.
The only other caregiver who noted that his child needed to work on developing his motor skills acknowledged that this was something he realized only after participating in the PALS program. He was surprised by this because “at that age a lot of people just say, they’ll figure it out, just let them do it” (participant 5).
Another caregiver described her child as having above-average speed and sport skills, yet the child scored in only the 16th percentile overall on the TGMD-3 (locomotor percentile rank = 50, object control percentile rank = 5). Again, this illustrates a substantial lack of awareness of motor development or the ability to detect errors in object control skills.
The children themselves perceived that they were highly skilled in general. Self-perceptions of skill competence ranged from 3.25–4.00 on a 1–4 scale, again a mismatch between perception and reality.
Comparison of TGMD-3 Percentile Scores, Child Self-Perceptions, and Caregiver Perceptions of Child Skill Competence
Two unique cases did not align with this trend. In one case (participant 8), the child had a relatively low step count but relatively higher TGMD scores. In the other (participant 10), the child had the highest TGMD score compared to others in the study, but was also obese and had the second lowest daily step count. It is unclear what drove these differences that were outside of the norm.
Theme 5: Types of Physical Activity Engagement
While all families described their children engaging in a variety of physical activities, most fell into one of two groups: outdoor activity-focused (six cases) or sports-focused (three cases). In sport-oriented cases, caregivers indicated that their child enjoyed playing sports such as kickball, baseball, football, and basketball, and in all three of these cases, the child participated on an organized softball/baseball team. The caregivers also talked about their own love for sports. They did mention other activities, including playing outside, running, and riding bikes, but playing organized sports was dominant during the interviews. Sport-oriented families reported spending a significant amount of time each week at the ball field, and in two of the three cases, the caregivers estimated that sports contributed to several hours of daily PA. One caregiver who estimated that her child participated in 4 hours of PA daily stated: “Well, my daughter plays softball. So obviously that is physical activity” (participant 10).
This child averaged only 4,820 steps daily; thus, the hours spent at softball did not result in the child meeting daily PA guidelines. A second “sport-oriented” caregiver estimated that her child participated in 6–8 hrs of daily PA. In that case, the child averaged 15,455 daily steps, which met the daily PA guidelines but did not align with the 6–8 hrs reported by the caregiver. This case was somewhat unique in that the family was both sports-and-outdoor-oriented and reported spending a lot of time playing outside and riding bikes. These examples represented a common confounding of sports participation (which can include sedentary and low-intensity moments) and sustained PA.
Caregivers from sport-oriented families also reported that their child was athletic or good at sports. However, in two of the three cases, the child scored below the 50th percentile on the TGMD-3, and one of the three had the lowest object control score (5th percentile) compared to all other children in the study. Thus, the caregivers’ perceptions of their child’s motor competence did not align with their actual motor competence.
Outdoor activity-oriented caregivers talked about their children participating in PA more broadly and emphasized activities such as playing on the playground, riding bikes, walking, and running. Some discussed activities, such as hiking, fishing, and hunting, as primary physical activities. For example, when describing the picture she drew, one caregiver said: So, we actually live in a rural area, so I drew a trail going off into the woods that we normally walk down with some trees, and I drew the trampoline cuz it's right next to the trailhead. Usually, we’ll go on walks, and then we'll come back and let the kids jump on the trampoline and play on the playground (participant 8).
Another caregiver drew a picture of her child playing outside with nerf guns. When she described her child’s PA, she said: “He’s outside practicing his tee ball, running around, fishing, helping us pick up outside” (participant 11).
Like some of the other “outdoor” families, she mentioned that her child participates in an organized sport, but she emphasized outdoor activities over sports. For these families, the rural environment in which they lived seemed to be a backdrop for the types of PA they did. In four cases, the caregivers connected a love of being outdoors as the catalyst for being active. Many of these families equated being outside with PA, regardless of the intensity of the outdoor activity.
Discussion
The purpose of this study was to explore and describe the alignment of caregivers’ expectations and valuations of PA behavior with the motor skill development of their preschool-aged children. Caregivers are critical choice agents and drivers of children’s behaviors (Ceka & Murati, 2016). The findings of the present study highlight several important aspects about caregivers’ perceptions of their children’s PA and FMS, with clear implications for family and community programming.
Caregivers universally valued PA for their children. This finding aligns with existing literature, particularly EVT, which posits that people are motivated to engage in activities in which they value and believe they can succeed (Faith et al., 2012; Hesketh et al., 2017; Oliver et al., 2010). Many caregivers viewed PA as essential not only for their children’s health and well-being but also as a medium for family bonding. Family structured and unstructured play is vital to and can produce spillover effects for impoverished children’s social, emotional, cognitive, and physical development, fostering creativity, resilience, and cooperation (Milteer et al., 2012). Regular PA also strengthens parent-child bonds by offering opportunities for meaningful engagement and seeing the world from the child’s perspective (Coyl-Shepherd & Hanlon, 2013; Milteer et al., 2012). Family and community engagement programs like PALS can leverage this family-oriented and systems approach to increase PA and foster motor development for children that permeates beyond the school setting (Brian et al., 2023). However, despite a strong valuation of PA, caregivers were often unaware that their children’s daily activity levels fell below the recommended guidelines. This gap between perception and reality suggests that caregivers may benefit from education about what constitutes sufficient PA. Physical education and community programs within the school setting could play a crucial role in providing caregivers with concrete examples of activities that will help meet PA recommendations.
The WHO recommends that children aged 3–5 years engage in at least 180 min of daily PA (WHO, 2019). Within our study, step counts indicated that only about half of the children engaged in the equivalent of 60–100 min of daily PA. Yet, many caregivers overestimated their children’s PA behavior each day, with 4–6 hrs being a common response. This reflects a misunderstanding of what qualifies as PA behavior in terms of duration. Activities like participating in sports or simply playing outside were often viewed as outlets providing an adequate amount of PA behavior, even though those activities often do not result in children meeting the recommended step count measures. These findings track with/support the current literature that caregivers of inactive children have an inaccurate perception of their child’s PA levels (Scott-Andrews et al., 2021).
Caregivers also seemed to conflate being active and full of energy with being athletic but lacked an awareness of their child’s skill competence. The common assumption was that children naturally develop motor skills through PA. While this is true of locomotor skills like running, jumping, and skipping, object control skills, such as catching, throwing, and striking require more structured practice and instruction (Brian et al., 2023). A few caregivers noted that they were surprised to learn this fact through participation in the PALS program. These findings support the need to design PA intervention programs with a systems approach, including education for parents and caregivers. Even when caregivers value PA for their children, without knowledge of motor competence, they may not provide intentional, targeted opportunities to facilitate skill development.
Collectively, the TGMD-3 locomotor skill scores of participants in this study reflect a slightly higher level of competence as compared to estimates for children in the U.S. (Kwon & O’Neill, 2020). However, this group of children performed much lower than the national average for object control skills, with only two children scoring above the 50th percentile. Data on PA behavior and skill competence of children ages 3–5 is limited, particularly as it relates to socioeconomic and familial factors, but one study found an inverse relationship between family income and motor performance measured by the TGMD-2, particularly locomotor skill competence (Kwon & O’Neill, 2020). Results from the current study did not allow for a comparison between families who experience poverty and those whose income is above the poverty threshold. However, data highlight the environment as a facilitator for locomotor skill development, as access to the outdoors and the rural setting served as a backdrop for PA engagement. While some families focused on organized sports as the primary source of their children’s activity, their children did not appear to be more competent or more active. The assumption that organized sports result in skill competence or more PA time was frequently inaccurate. In contrast, PA-oriented families emphasized outdoor play and unstructured activities, which were often more in line with sustained physical movement, though there was no correlation between any type of PA and daily step counts.
Given the explanatory nature of this context-specific sample within this collective case study with a cross-case analysis approach, these findings should be interpreted with caution. The results suggest that physical education and community engagement programs may benefit from broadening their focus beyond organized sports to include a wider range of PA options, particularly those that can be performed independently or with family. In rural settings, where outdoor unstructured play may be more feasible, schools might consider integrating activities that support lifelong engagement in PA. Early caregiver education and family engagement may also play a role in shaping perceptions of physical activity, supporting a more holistic understanding of active lifestyles. Additionally, while locomotor skills may develop through general participation in PA, object control skills may require more structured opportunities for practice and instruction. These changes ensure that our conclusions are more appropriately aligned with the data presented and avoid overstating broader implications.
Footnotes
Author Note
The authors declare no conflicts of interest. The datasets generated and analyzed during the current study are not publicly available and cannot be shared beyond approved research team due to ethical restrictions and participant confidentiality agreements. Brian and Campbell are co-lead authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Duke Endowment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.