
Abstract
Neuropsychological trauma processing techniques based on hippocampal-dependent spatial and episodic memory were trialled with 71 newly recruited officers within one UK police force between March 2018 and February 2019. Results indicate that the skills are teachable within an operational training environment, have a positive impact on feelings of ease about difficult or traumatic work-related incidents, can improve recall of events and may mitigate against the impact of age and trauma exposure on memory. Participants report the techniques to be useable, sharable and operationally relevant to trauma management and personal resilience. Results will inform a larger randomised controlled trial.
Keywords
Introduction
At the Manchester Arena attack on 22 May 2017, 22 people died, many of them children (Kerslake Report, 2018). Over 1,000 Greater Manchester Police (GMP) officers and staff were recorded as having been involved in responding to the incident. Preparedness for – and resilience to – trauma exposure is becoming a pressing public health issue – not least for policing and not least for the hundred new recruits who joined GMP in January 2018. This article reviews a study with that cohort, testing how feasible it is to train police to direct their attention more effectively towards trauma processing with a view to increasing resilience to disorder that emanates from unprocessed trauma exposure on the job.
Literature on the prevalence of post-traumatic stress disorder (PTSD) in contemporary UK policing is scarce, perhaps mainly because (despite its recognition back in 1980) PTSD is not uniformly monitored within occupational settings (Skogstad et al., 2013), and not least in the police service (Green, 2004). Where studies of PTSD prevalence have been embarked upon, sample sizes are a consistent limitation (Lee et al., 2016). Alongside this degree of invisibility, stigma surrounding police traumatisation cannot be ignored (Heffren and Hasudorf, 2014). Even when science steps in to introduce a non-subjective understanding of trauma impact in policing – measuring changes in cognitive function and brain structure as a result of trauma disorder (Baldacara et al., 2017, Miller et al., 2017a, b) – these have not yet been framed in the context of resilience.
Nonetheless, the impact of long-term trauma exposure in policing is becoming increasingly well understood, thanks to tools such as the new self-report diagnostic measure of PTSD and complex PTSD (C-PTSD), the International Trauma Questionnaire (ITQ; Cloitre et al., 2018). Using that ITQ, recent (unpublished) data from Police Care UK and University of Cambridge (2019; Policing: The Job & The Life, n = 16,857) suggest that 12% of trauma-exposed officers and staff likely have C-PTSD and a further 8% PTSD, equating to one in five having some form of trauma disorder. Over 90% of respondents reported trauma exposure in their everyday role and yet fewer than half said they had the opportunity to make sense of what they had experienced.
Such high prevalence of C-PTSD in policing may have been masked up until now by a certain social acceptance of the ‘drip-drip-drip’ effect of trauma exposure on the job, that ‘burn out’ inevitably awaits the long serving. As contemporary policing adapts to fewer resources and changing demand, it is all the more vital to challenge this resigned acceptance. The impact of trauma exposure on the job needs to be addressed directly to help those heading towards burnout and to give those joining the profession the greatest chance of maintaining their resilience.
This is not a new calling. The need for trauma management has long been clear through adoption of military-inspired trauma risk management (see Greenberg et al., 2010) and other interventions such as psychological screening, ‘debriefing’ and ‘decompression’ (Rona et al., 2017) – all with mixed results and some contrary to National Institute of Clinical Excellence (2018) guidance. This article describes a different approach. Our aim is to teach new recruits practical skills to help them adapt to the extraordinary and difficult incidents that lie ahead. To do so, we translate neuropsychological techniques of trauma processing into training materials for the operational police training environment. There are many challenges to this approach. One challenge is a conceptual one; all of us process our life experiences in our own ways with our own limitations – ranging from the legacy of previous trauma to even genetic disadvantage (Brewin et al., 2000; Miller et al., 2017). Randomised controlled trials in policing populations cannot realistically expect to control for all of this variance. This feasibility study is also confined by that limitation and aims instead to ascertain what meaningful outcomes can emerge from training police officers in this way and how these outcomes are received among those starting out in a job like no other.
Neuropsychological models of trauma describe clearly how demanding it can be for the brain to file away extreme experiences, experiences which may, in reality, be commonplace in policing (Brewin et al., 1996). When we are faced with adverse or threatening situations, many areas of our brain and body spring into action and yet there is one particular area of the brain which is integral; the hippocampus (Astur et al., 2006). The hippocampus (deriving from the Greek for ‘seahorse’, due to its shape) enables us to render events as past, contextualising them into the context of ‘been there, done that’. In doing so, the hippocampus helps reset the stress response. There is a sad irony of evolutionary neuropsychology here, and one for which those regularly re-exposed to trauma (such as police) pay the price. Stress toxins released in the brain damage the hippocampus. This results in a potentially vicious cycle of the stress response preventing the very part of the brain needed to manage it (Andersen et al., 2007; Bremner and Elzinga, 2002). A trauma-impaired hippocampus becomes lethargic, making it difficult to perceive threats accurately, to recognise safety cues and reducing situational awareness – ultimately disrupting our ability to respond effectively to adverse situations, rendering us even more vulnerable to trauma (Andero and Ressler, 2012; Miller, 2016; Miller et al., 2017; Pearson et al., 2012; Smith et al., 2015; Teicher et al., 2003).
As bleak an outlook as this may seem for policing, it isn’t all bad news. Trauma processing techniques using spatial processing techniques have already been trialled in a small military case study of veterans with combat-related PTSD with improvements in self-reported trauma impact and treatment outcomes (Kaur et al., 2016). We can see these techniques also subtly adopted in civilian life. When the media report on a major incident (such as a terror attack), they frequently illustrate the event using a map and a timeline. Essentially, these representations mimic successful hippocampal processing, offering readers spatial and episodic context to help make sense of adverse situations. Making sense of difficult or traumatic incidents is arguably an essential component of contemporary policing, if officers and staff are to effectively respond to incidents one after the other and maintain their resilience over a protracted period of time. Tools to support how one makes sense of episodes and incidents are already relevant to policing. Producing maps and timelines are recommended components of the cognitive interview in forensic investigations (Dando et al., 2008; Hope, 2013; Thomas and Hope, 2018). If we appreciate that police officers and staff are themselves perpetual ‘witnesses’ of the (potentially traumatic) incidents they respond to, it seems right to use techniques such as these to help maintain the integrity of their memory and their well-being. This feasibility study endeavours to define how training in trauma processing techniques can help that happen.
Research questions
The study looks to prove the concept that trauma processing techniques (based in neuropsychology) are translatable into a police training environment and assess the extent to which the techniques’ preventative capacity might be tested over time. The study analyses in-session efficacy of trauma processing techniques (including participant feedback) and between-group trauma impact monitoring. Types of trauma exposure and their frequency among new recruits are also investigated.
Ethics clearance and general data protection regulation (GDPR) adherence were granted in 2017 through the University of Cambridge. 1 Project steer was provided by The Police Federation of England & Wales, The College of Policing, Chief Medical Officer and Chief Officers, leads for well-being and clinical lead from University College London.
Participants
A cohort of 101 student officers was selected by GMP to participate in the study based on their availability. Officers had already been randomly assigned to five training classes. Ninety attended the participant recruitment briefing in March 2018, at which 88 provided consent to participate. Consenting officers in the first three GMP training classes were nominally assigned to the trial group and officers from the remaining two classes to the control group. Twenty-seven students withdrew over the course of the 11 months due to force examinations and operational issues, affording the study a trial group of n = 43 and a control group of n = 28.
There were no discernible differences in the urban or rural profile of the trial and control groups’ patrol areas to suggest any risk of trauma exposure bias to the study.
Exclusion criteria comprised self-reported depression, anxiety or PTSD. Participants (including controls) were screened at recruitment using the PTSD Checklist for DSM-5 (PCL-5) self-assessment tool for PTSD (Blevins et al., 2015), hosted as a survey on Qualtrics™ (https://www.qualtrics.com/uk/). No participants were excluded.
Participants were given a unique identification number and were asked to provide basic demographic data and a one-sentence description of previous trauma exposure using The Life Events Checklist (Gray et al., 2004). These data were later used to control for previous trauma impact on training outcomes.
The PCL-5 tool was re-applied on a monthly basis from March 2018 to February 2019 and more detailed assessment using diagnostic clustering of symptoms was undertaken where any participants approached threshold PTSD levels. 2 Most recent PCL-5 scores were also calculated for each participant before training. This was used to monitor well-being of participants attending training sessions and was later used to control for most recent (current) trauma impact on training outcomes.
The trial and control groups were well matched for age, gender, previous trauma and current trauma in all training sessions. Between-group differences in current trauma impact were not significant, and small sample sizes of those with current trauma impact in the control group precluded further group analysis.
Interventions and techniques
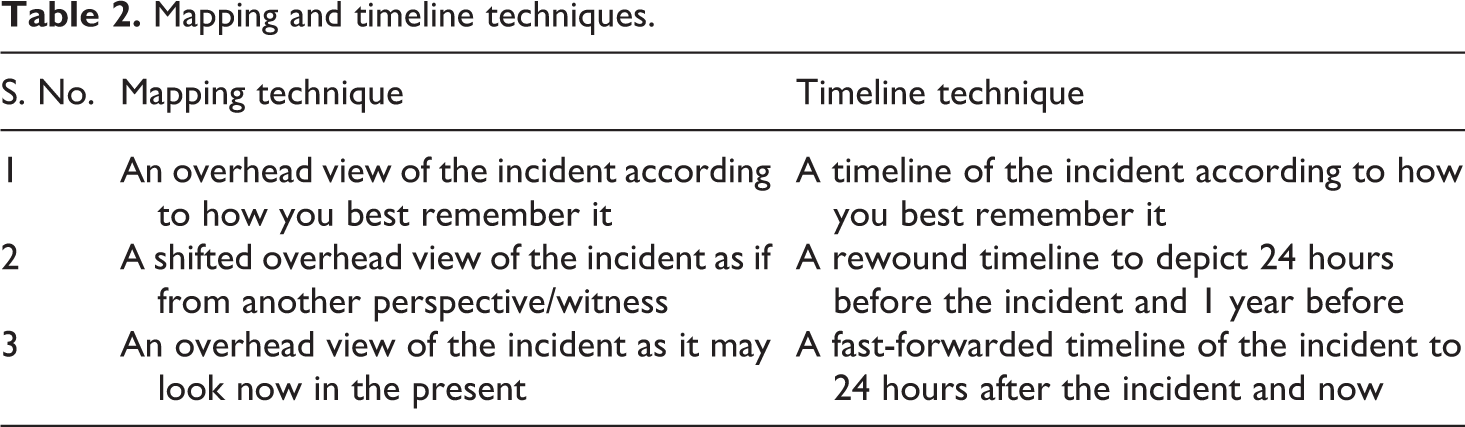
In each session (see Table 1), participants were asked to bring to mind a difficult incident (nothing too traumatic) for the purposes of training 3 and applying the mapping and timeline techniques (see Tables 2 and 3).
Participant demographic and trauma monitoring data for all training sessions (note small sample sizes for control group with current trauma).
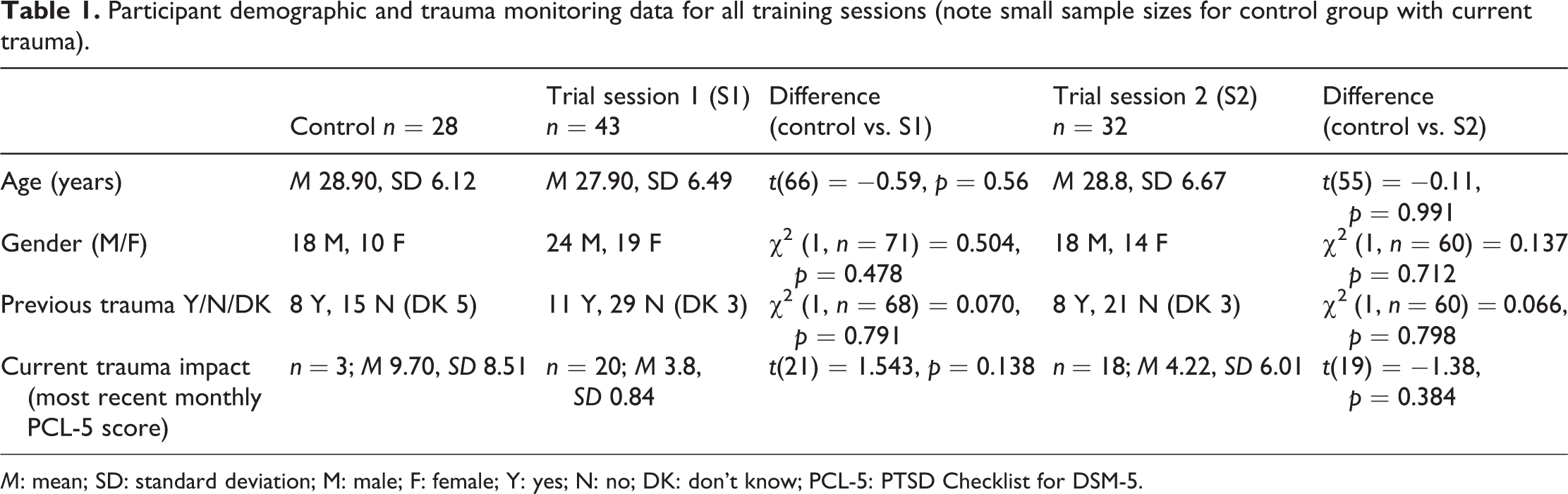
M: mean; SD: standard deviation; M: male; F: female; Y: yes; N: no; DK: don’t know; PCL-5: PTSD Checklist for DSM-5.
Mapping and timeline techniques.
Training session content (all sessions) for trial and control groups May 2018 to February 2019.
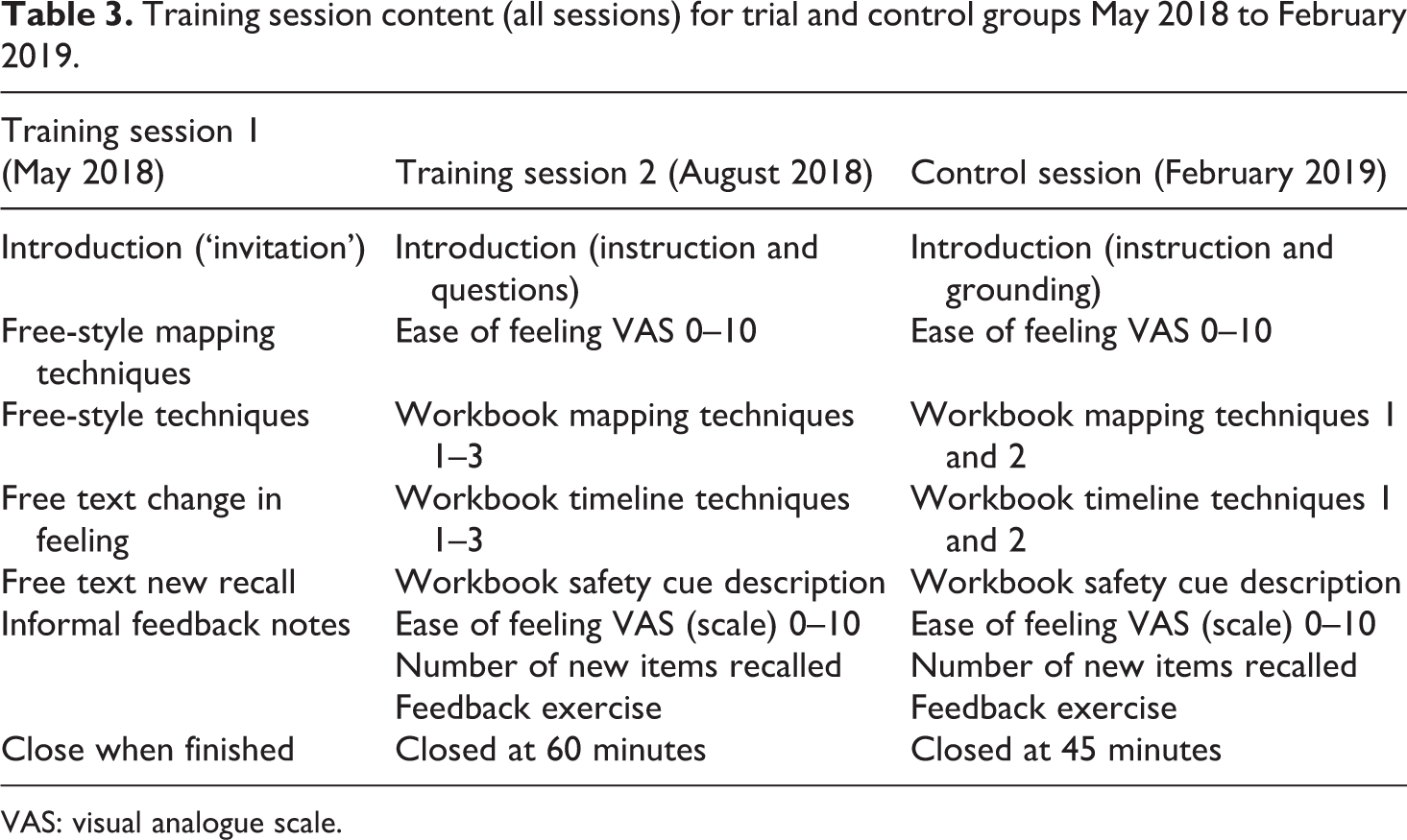
VAS: visual analogue scale.
The first training session for the trial group took place in May 2018, lasting 90 minutes and attended by all 43 participants. This session was deliberately informal and is not dissimilar to the notion of free recall in the cognitive interview (Dando et al., 2008) to be compared later with the more formal training structures of sessions 2 and 3. Participants were invited to produce overhead maps and timelines about the incident, noting down any change in feeling (positive or negative) and/or any newly recalled information. Drawings and notes were then depersonalised and categorised for qualitative analysis (see Figure 1).
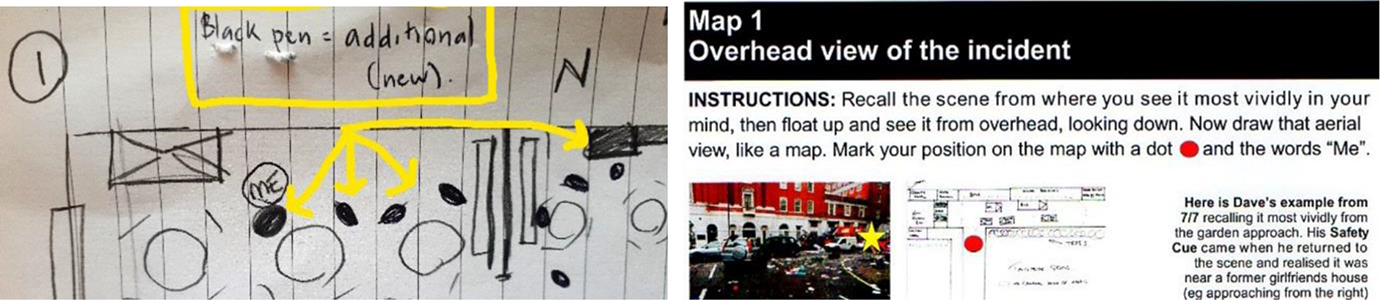
Free recall notes from session 1 and a workbook sample from session 2. The black circular symbols in the first note represents newly recalled persons present at the scene of the chosen incident.
Their second session in August 2018 was a more formal ‘refresher’ session for 90 minutes. Due to exams and a disciplinary incident, only 32 participants of the original 43 attended. Following a ‘recap’ presentation, participants spent 60 minutes completing pre-designed workbooks with step-by-step instructions for producing a range of maps and timelines. Using a visual analogue scale (VAS) from 0 to 10, 4 participants relayed ‘how at ease’ they felt about the incident before and after applying the techniques. Participants were also asked to recall any moment of the incident at which it became clear to them that the stress was over (referred to as a ‘Safety Cue’). Workbooks, VAS score and item totals were collated and depersonalised for analysis.
The third session in February 2019 was for the control group and was attended by 28 participants. This session followed the same format as the first but was a little shorter (45 minutes) after removing some tasks that had previously received negative feedback.
In summary, key outcome measures comprised feeling at ease about the difficult or traumatic event (VAS score of 0 to 10), ability to shift overhead view (i.e. to apply hippocampal-dependent processing associated with effective trauma processing) and new recall. Control variables comprised age, gender, previous trauma exposure (yes or no) and current trauma impact level (PCL-5 score).
Results and analysis
Can the techniques be taught at all in this setting? In-session efficacy of techniques
The training group’s first session, session 1 (n = 43)
Typical of many feasibility studies the more experimental design of session 1 necessitated results to be presented using descriptive statistics, frequencies and qualitative data (see Table 4).
Session 1 frequencies of basic measures of task performance and impact.
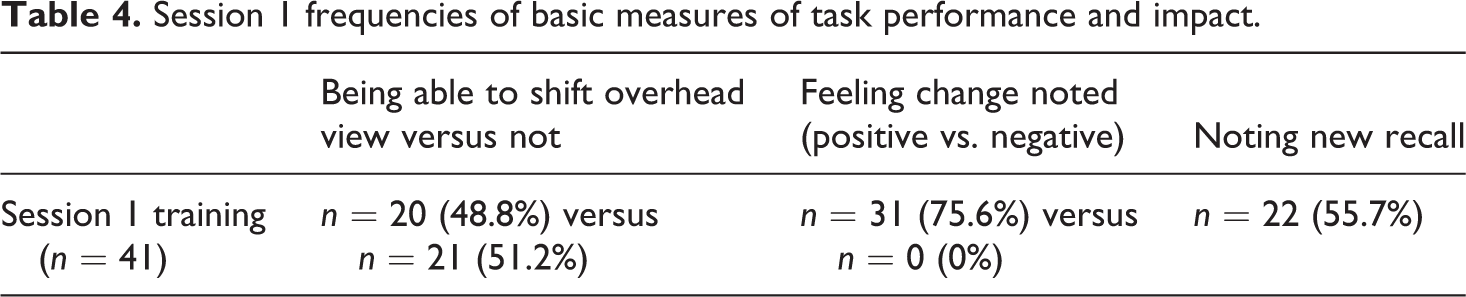
Engagement with participants in this informal session was positive with only two participants failing to complete all requests for maps and timelines, providing a sample size of n = 41. Drawings and notes were categorised for being able to shift overhead perspective, changes in positive or negative feeling and recalling new detail. Being able to shift from one overhead perspective to another is demanding on the hippocampus (Miller et al., 2017) and variation in performance on this measure provided a good baseline by which to gauge the benefits of alternative spatial techniques. Noting positive feeling change and new recall were taken to be basic measures of the techniques’ potential to address the emotional resonance and memory of an incident.
Participants were near equally divided on their ability to shift overhead perspective and noting new detail. Ten individuals reported neither feeling change nor improved recall. Eight of these described having no feeling to speak of and two were using a recent bereavement as their training scenario, their feelings about which were unchanging.
Qualitative analysis of participants’ note-making revealed a shared sense of having a broader context, more objectivity and more acceptance and peace of mind about the incidents from the session. Depersonalisation of space (i.e. being less likely to identify personally with the scene of the incident) was frequently mentioned. In terms of episodic memory, several timelines referred to a sense of time expanding around an incident (where it had previously been contracted). Some participants used rewound timelines to explore cause and effect of incidents, liberating some from a (misplaced) sense of responsibility that ‘[they] should have done something (differently)’. The notion of transience (and being able to ‘move on’ from an incident) accompanied some fast-forwarded timelines.
The training group’s second session (2) and the control group’s session (3)
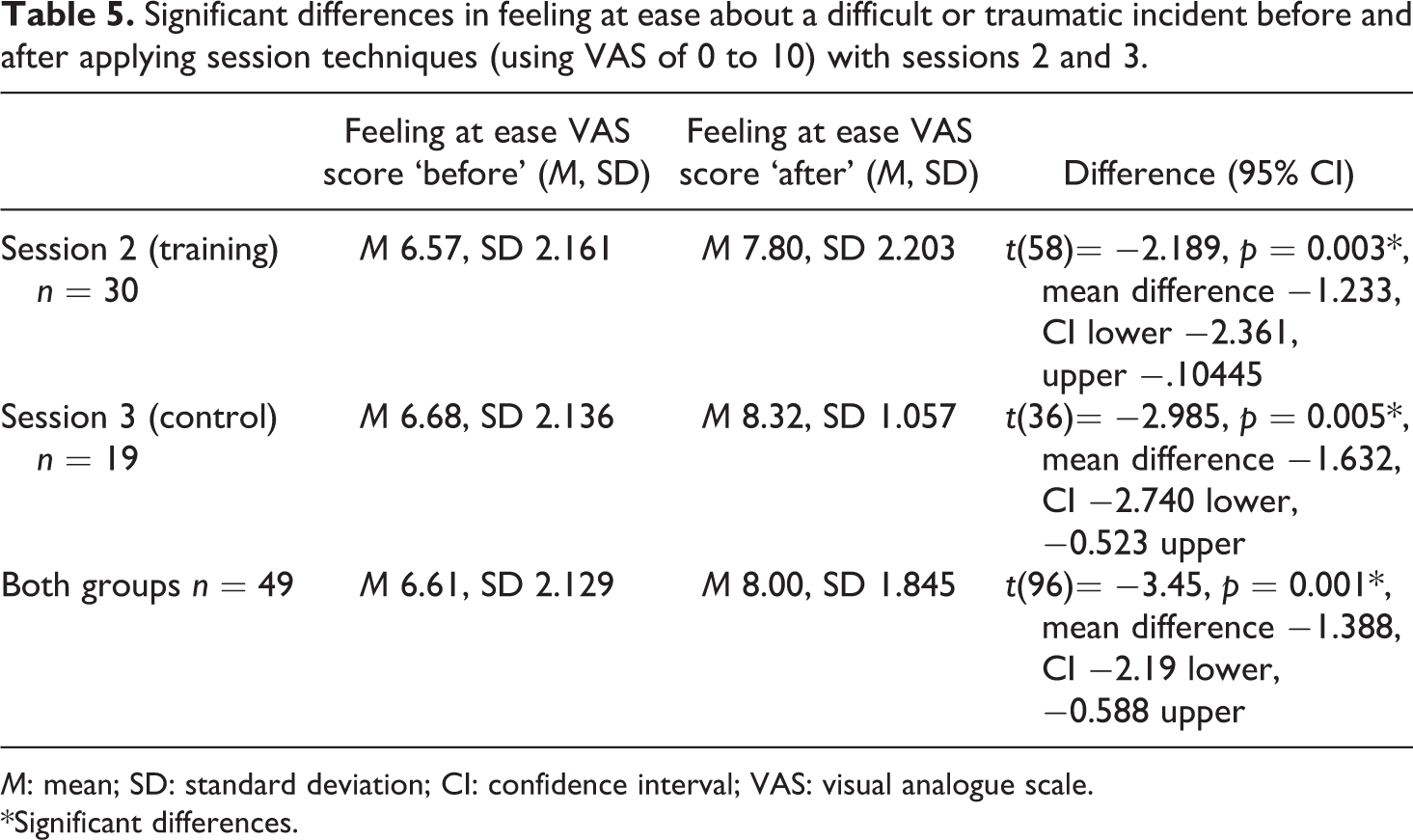
Results from both session 2 (n = 32) and session 3 (n = 28) together enable us to assess the ‘teach-ability’ of the techniques using the workbooks (see Table 5). Comparing these groups gives us a larger sample to work with and an opportunity to assess what difference providing additional training sessions could make (i.e. with the training group), compared to a stand-alone session (control group). Feeling at ease with the incident (VAS) data, performance in hippocampal-dependent processing and quantified new recall were analysed by age, gender, previous trauma exposure and current trauma impact (most recent PCL-5 score).
Significant differences in feeling at ease about a difficult or traumatic incident before and after applying session techniques (using VAS of 0 to 10) with sessions 2 and 3.
M: mean; SD: standard deviation; CI: confidence interval; VAS: visual analogue scale.
*Significant differences.
Feeling at ease with difficult or traumatic incidents
The rationale for statistical analysis here was to use t-tests to compare ease of feeling before and after applying the techniques. There were positive improvements in how at ease participants felt about their chosen incident (using the VAS) after applying the techniques in both the training and control groups. For the two groups combined, the difference was highly significant with an effect size of 0.70 (Cohen’s d).
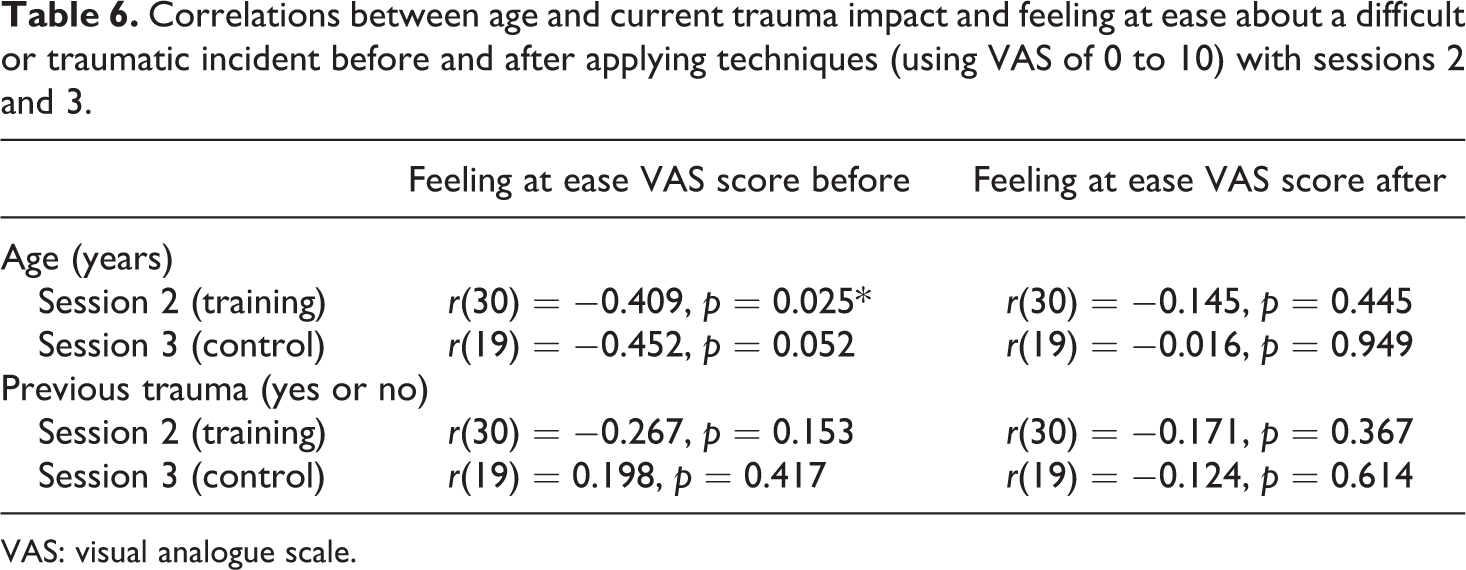
Correlation analysis was undertaken for age and current trauma impact (see Table 6). Age was negatively correlated with how at ease participants felt about the incident before they applied the techniques (VAS score) in both session 2 training group and session 3 control group. These correlations were weaker after applying the techniques in either group.
Correlations between age and current trauma impact and feeling at ease about a difficult or traumatic incident before and after applying techniques (using VAS of 0 to 10) with sessions 2 and 3.
VAS: visual analogue scale.
Current trauma impact (participants’ most recent monthly check-in PCL-5 score prior to the training session) was negatively correlated with how at ease participants felt about the incident before they applied the techniques (VAS score) in session 2 training group. Again, this correlation was weaker after applying the techniques. Sample sizes for those with current trauma impact were too small for session 3 control group (n = 3) to replicate the correlation.
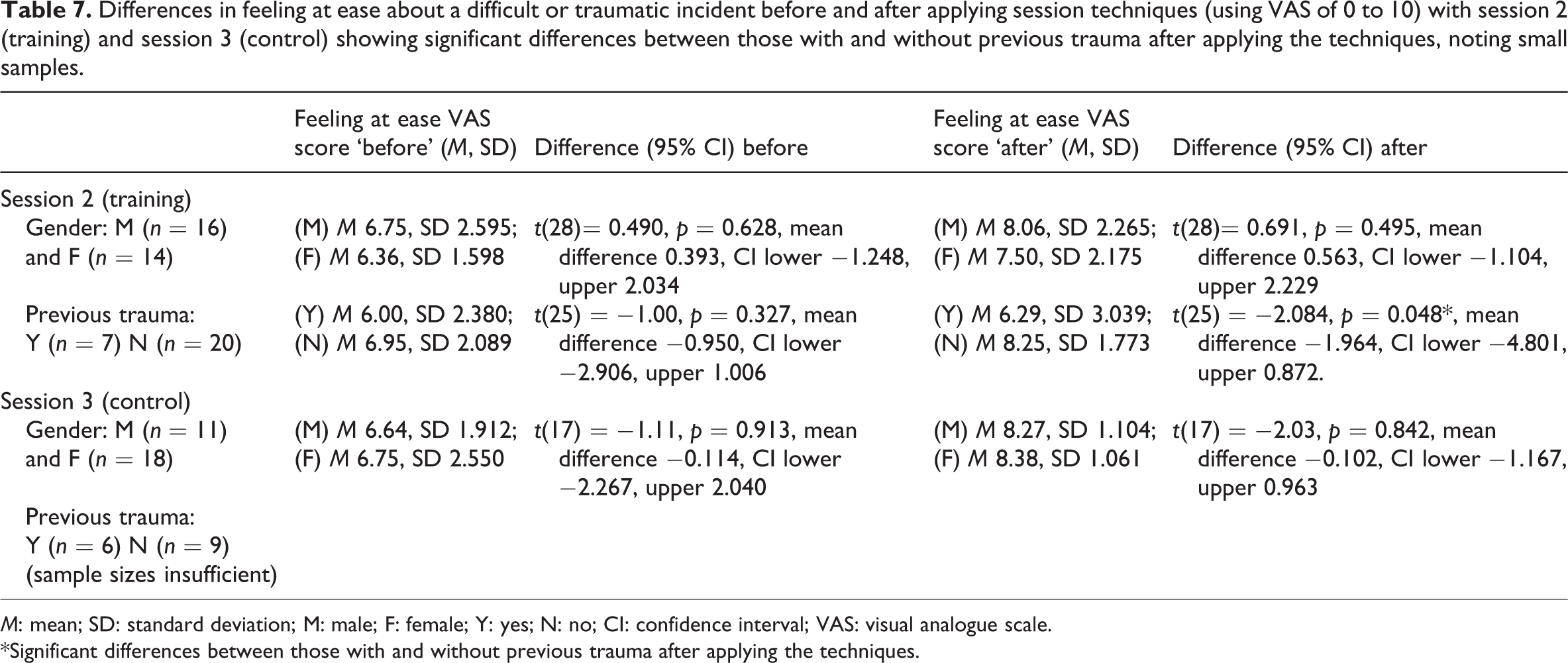
Statistical analysis of differences in feeling at ease (VAS score) by gender and previous trauma status (yes or no) was undertaken using t-tests for both session 2 (training group) data and session 3 (control group) data (Table 7).
Differences in feeling at ease about a difficult or traumatic incident before and after applying session techniques (using VAS of 0 to 10) with session 2 (training) and session 3 (control) showing significant differences between those with and without previous trauma after applying the techniques, noting small samples.
M: mean; SD: standard deviation; M: male; F: female; Y: yes; N: no; CI: confidence interval; VAS: visual analogue scale.
*Significant differences between those with and without previous trauma after applying the techniques.
Gender did not affect how at ease participants felt before or after applying the techniques in either session. In session 2 (training) group, there was a significant difference in ease of feeling after applying the techniques between those with and without previous trauma (p = 0.048) with an effect size d 0.79 but with low power of 0.39, suggesting a larger sample size was required. 5
Task performance
Being able to shift from a ground level view (an ‘egocentric’ view) to an overhead view (an ‘allocentric’ view) is useful for depersonalising an incident in one’s mind (which can help trauma processing (Eich et al., 2011). Being able to then shift the overhead view to one from a different perspective requires hippocampal-dependent processing and, as such, is an acceptable (albeit basic) indicator of hippocampal function (Guderian et al., 2015). If hippocampal integrity is important for trauma resilience, then performance on this task is important to assess. In session 2 training group, age and previous trauma exposure negatively correlated with being able to shift overhead view (see Table 8). Both variables of age and previous trauma had power of 0.99 and effect sizes of 0.73 and 0.65, respectively. Meaning that older participants and those with background experiences of trauma were less able to change their overhead view of the incident from one perspective to another. This was not the case with current trauma impact. Sample sizes for those with current trauma impact were smaller and too small in session 3 control group (n = 3) for correlation analysis.
Correlations between shifting overhead view, age, previous trauma and current trauma impact (most recent monthly PCL-5 score) with sessions 2 and 3.
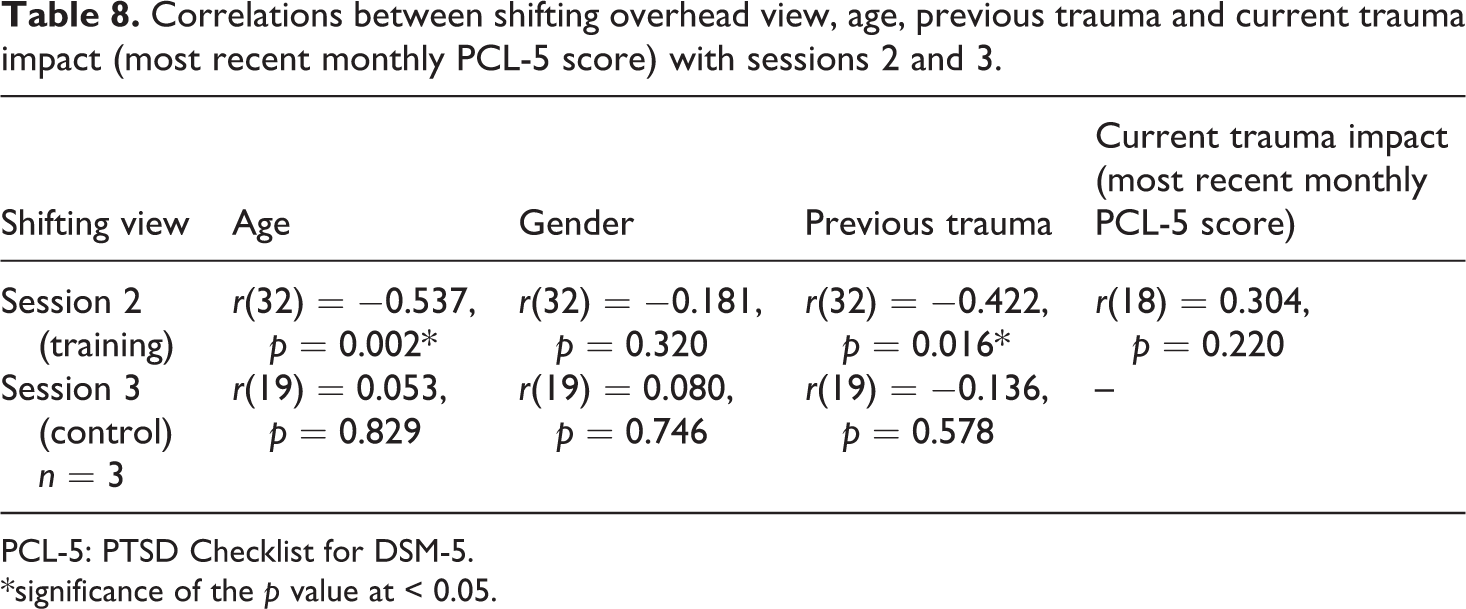
PCL-5: PTSD Checklist for DSM-5.
*significance of the p value at < 0.05.
Gender did not correlate with being able to shift overhead view in either session 2 or 3.
New recall
On average, 62.7% of participants recalled new information after applying either the mapping or timeline techniques to a difficult or traumatic incident. The highest number of recalled items were those recalled after using mapping techniques applied in session 2, the participants from which had received the most training in the study sample (see Table 9).
Number of new items recalled after applying mapping and timeline techniques (sessions 2 and 3).
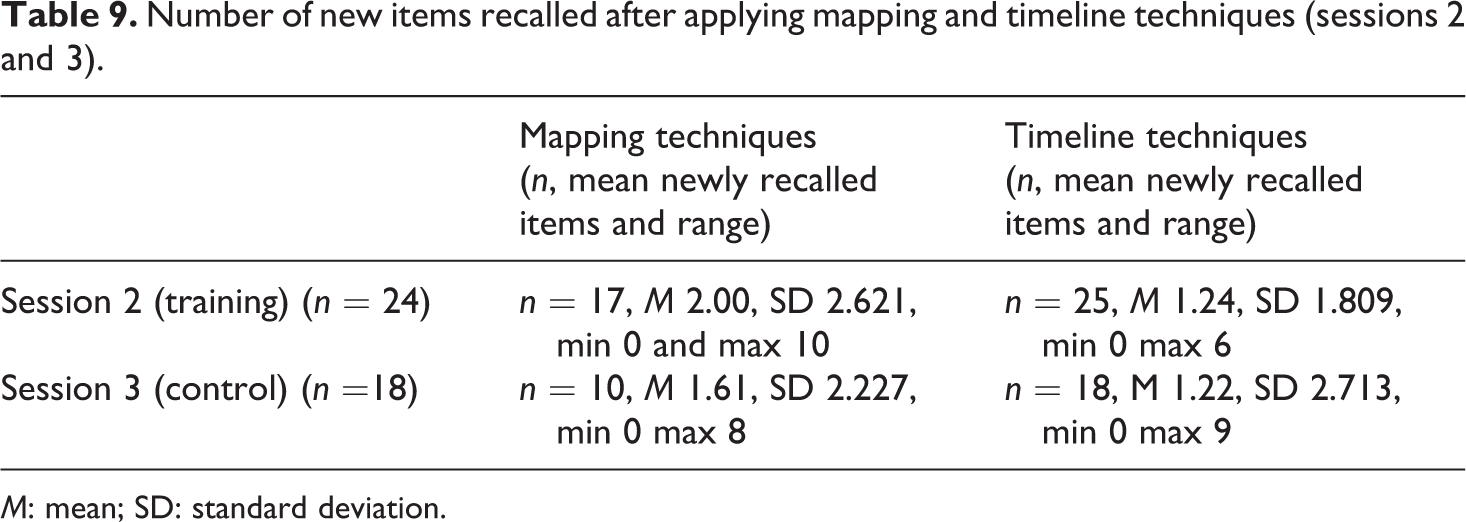
M: mean; SD: standard deviation.
Previous trauma exposure negatively correlated with the ability to recall new memory items about a difficult or traumatic incident in session 2 training group (but this did not reach significance in the smaller session 3 control group session, see Table 10). Neither age nor gender correlated with participants being able to recall new information. There was no correlation between current trauma impact and recall. Sample sizes for those with current trauma impact were too small for session 3 control group (n = 3) to replicate the correlations.
Correlations between recalling new memory items about a difficult or traumatic incident, age, previous trauma and current trauma impact (most recent monthly PCL-5 score) with sessions 2 and 3.
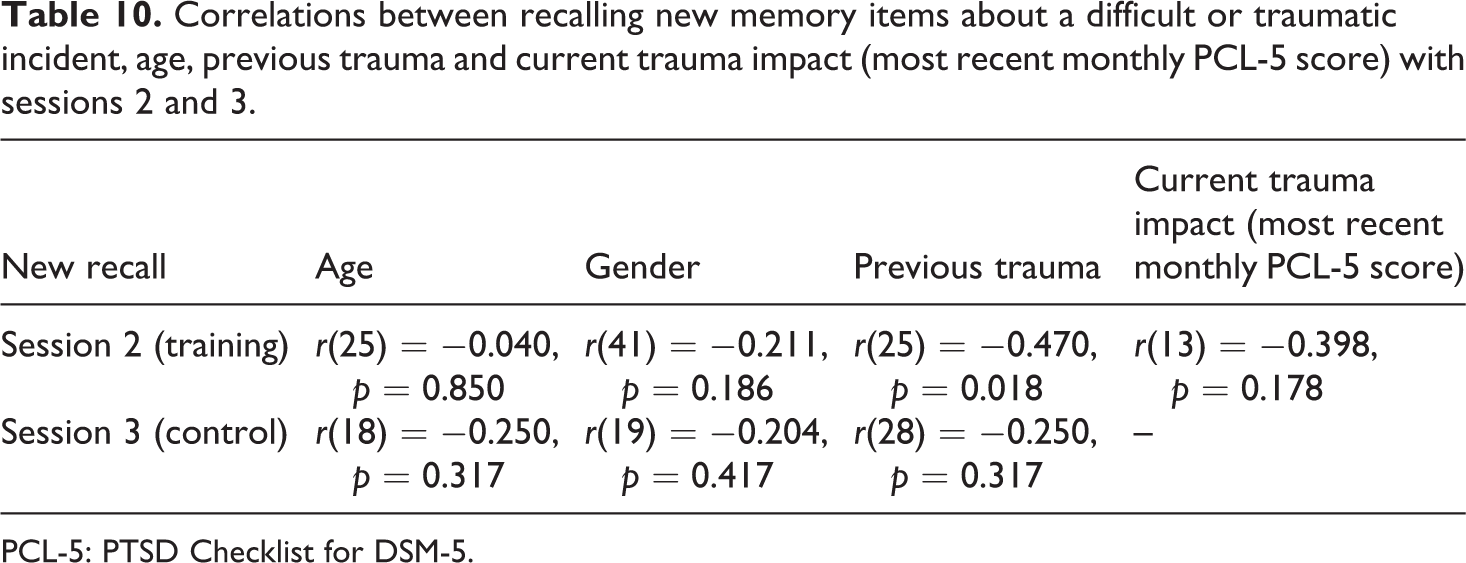
PCL-5: PTSD Checklist for DSM-5.
Task engagement
In session 2, fewer participants (n =26) completed the third timeline task (of ‘fast-forwarding to one year after the event’), compared to an average of 30 participants completing other timelines. In the feedback exercise (n = 27), none of the participants considered this timeline to be the most useful. The third map task (of ‘how the scene may look now’) was not completed by 50% of participants (16 participants). Verbal feedback suggested that in response policing, ‘fast-forwarding’ past jobs to the present day was less relevant or less meaningful than rewinding recall. Both fast-forwarding techniques were subsequently deprioritised for session 3 (control group) training.
Feedback exercise
Feedback on participants’ preferences and advocacy for different tasks was collected in session 2 training and session 3 control group. Forty-seven participants told us from which spatial perspective they naturally recalled events. The majority (65%) recalled from a ground level (egocentric) view and 19% from an overhead position (an allocentric view). Participants were asked to rank the techniques they found most useable. The validity of the ranking data was somewhat compromised due to consistent participant errors in ranking (likely due to fatigue, poor instruction from the research team or a combination of both). Nonetheless, crude analysis 6 across both groups provided some evidence of preference for ‘ground level to overhead view’, followed by ‘my ground view to another ground view’ and finally ‘my overhead view to another overhead view’.
Timelines that centred on the most vivid memories of the event from start to finish were most popular for 60% of participants. ‘Rewinding’ to the events leading up to the incident also featured among the top-ranked timelines. Longer rewinds and ‘fast-forwarding timelines’ to the present day were not ranked highest by any participant. Safety cue descriptions were provided in session by 97% of participants (n = 69 of 71), suggesting the concept as meaningful to all those recalling traumatic incidents, including the control group.
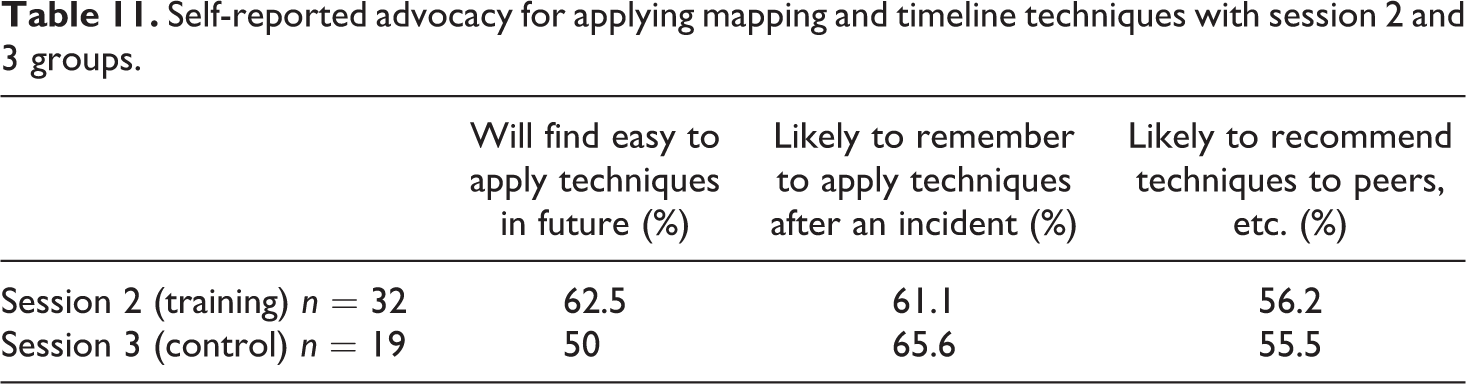
Results regarding advocacy were positive and comparable across both groups, despite the comparatively shorter time spent on techniques in the control group (see Table 11).
Self-reported advocacy for applying mapping and timeline techniques with session 2 and 3 groups.
Both groups fed back on evaluative statements (Table 12) regarding how the difficult incident ‘felt’ to them (see Figure 2). The highest scoring statements were those that referred to objectivity and perspective. There were few remarkable, clearly explicable group differences.
Participants from session 2 and 3 groups ‘strongly’ or ‘somewhat’ agreeing with evaluative statements about applying the techniques to difficult or traumatic incidents.
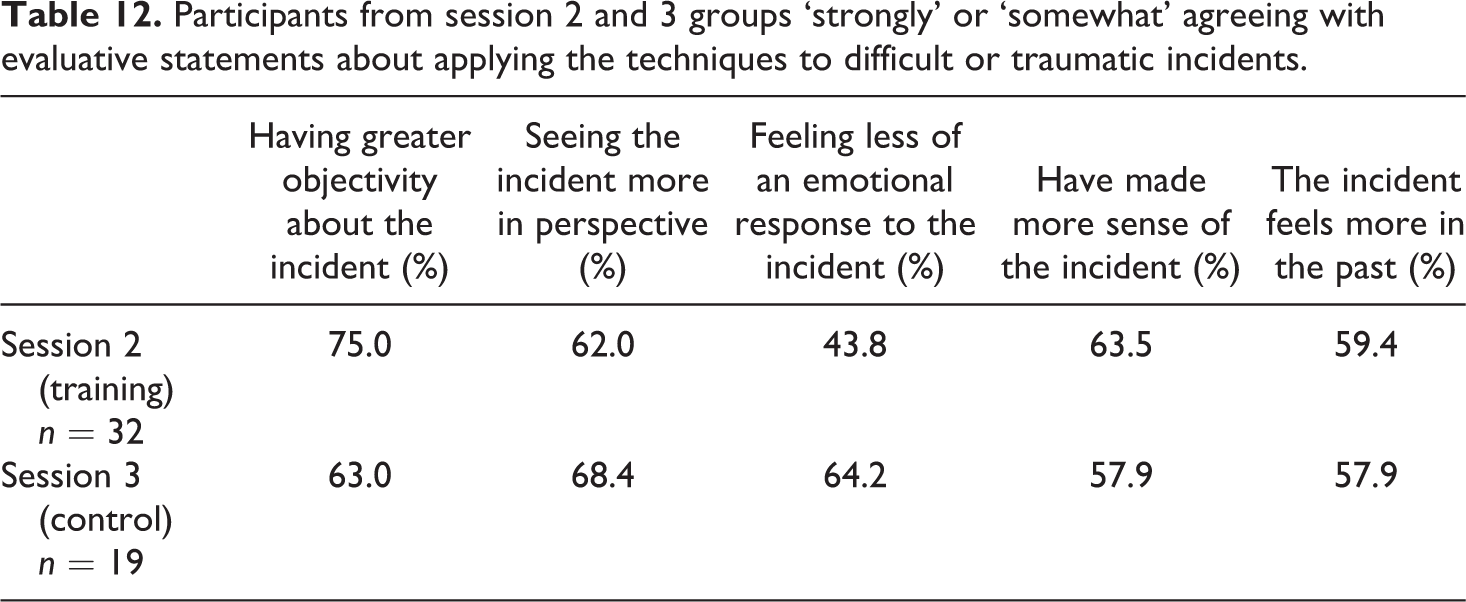
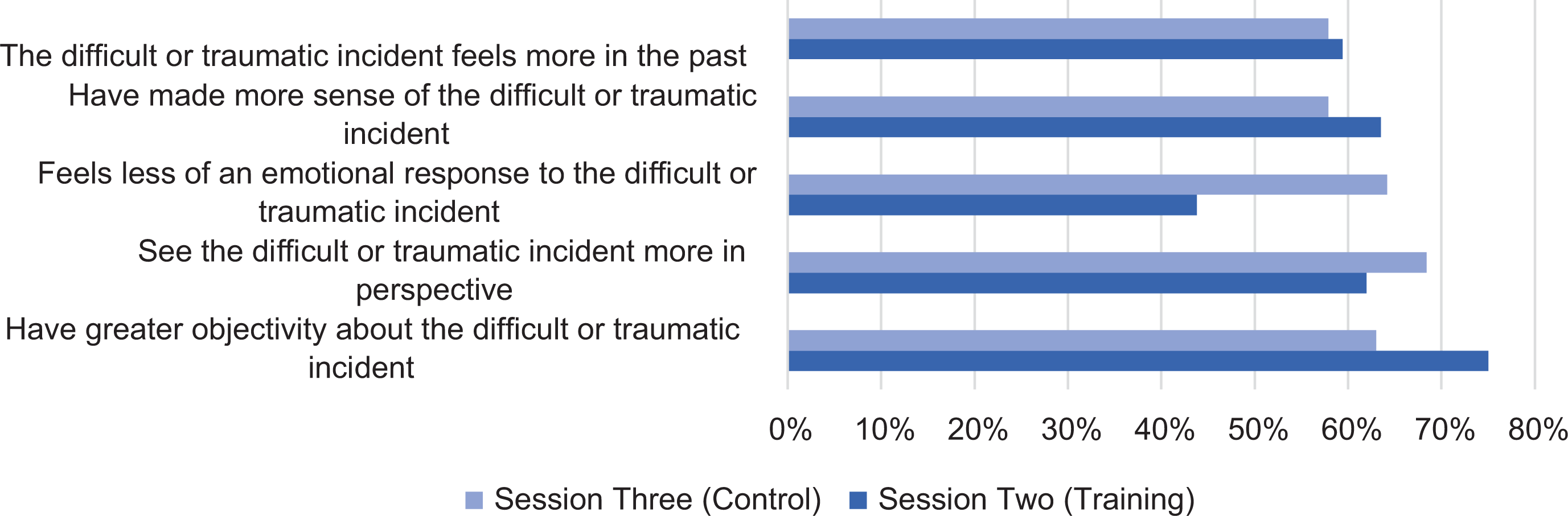
Participants from session 2 (n = 32) and session 3 (n = 19) groups ‘strongly’ or ‘somewhat’ agreeing with evaluative statements about applying the techniques to difficult or traumatic incidents.
How feasible is it to test the impact of the techniques between people and over time? Between-group trauma impact monitoring
Results compare monthly trauma impact between groups over time and consider whole population trauma impact. This includes assessing total trauma impact scores for participants (indicating traumatic load over the fieldwork period), different clusters of recognised PTSD symptoms and coding of the types of traumatic events experienced by officers.
Monthly check-in frequency and trauma impact scores were assessed between the trial group and the control group, revealing peaks and troughs in checking in, but fairly consistent trauma impact, gradually increasing from September 2018 when recruits’ full policing duties began (see Table 13).
Monthly check-in frequencies (with a trauma) and mean PCL-5 trauma impact scores for both groups.
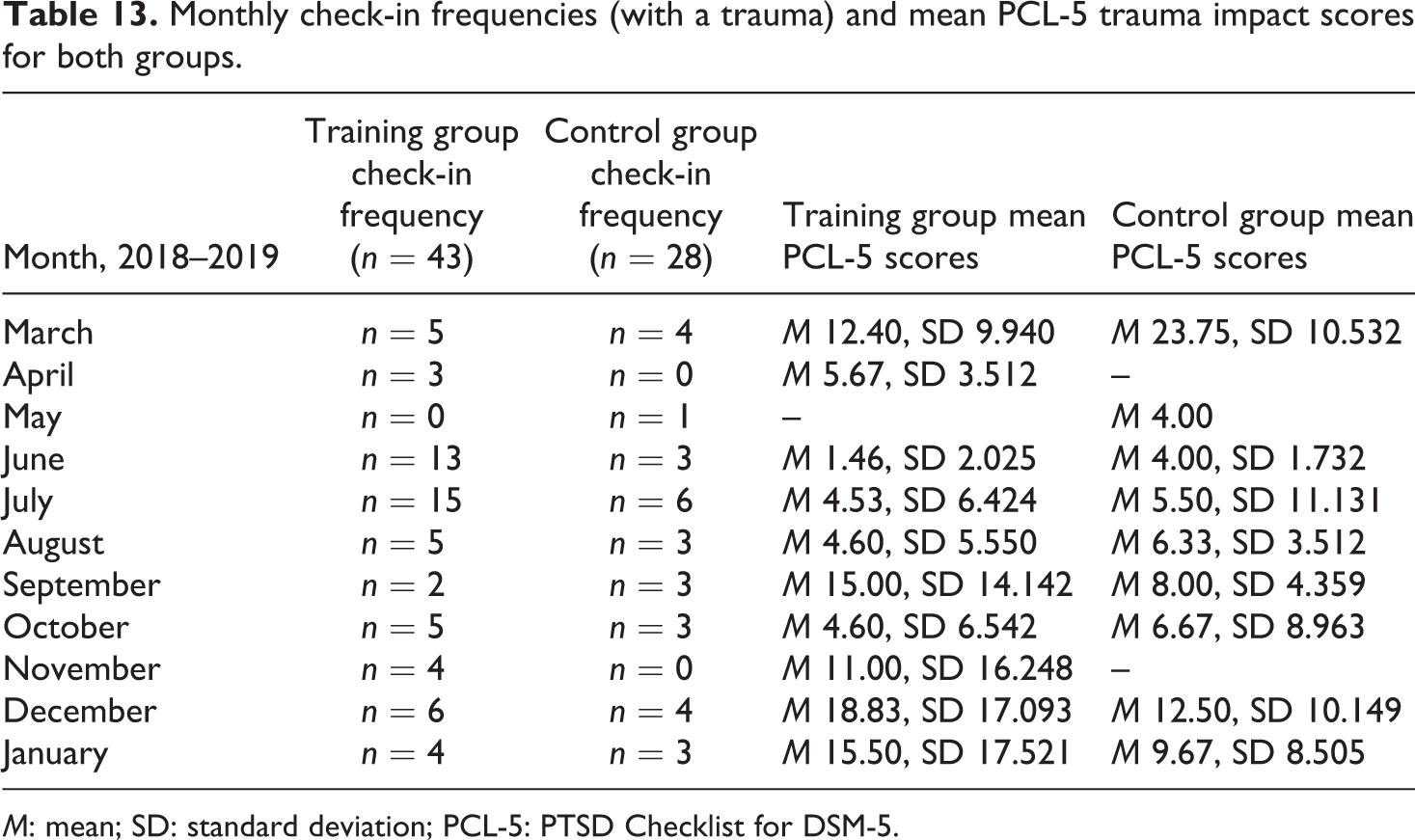
M: mean; SD: standard deviation; PCL-5: PTSD Checklist for DSM-5.
A total trauma impact score was calculated (by summing PCL-5 scores) to establish an approximate trauma ‘load’ throughout the trials. There were no significant differences in trauma load between the groups (see Table 14).
Indication of cumulative traumatic load between groups through trial period (total PCL-5 scores).
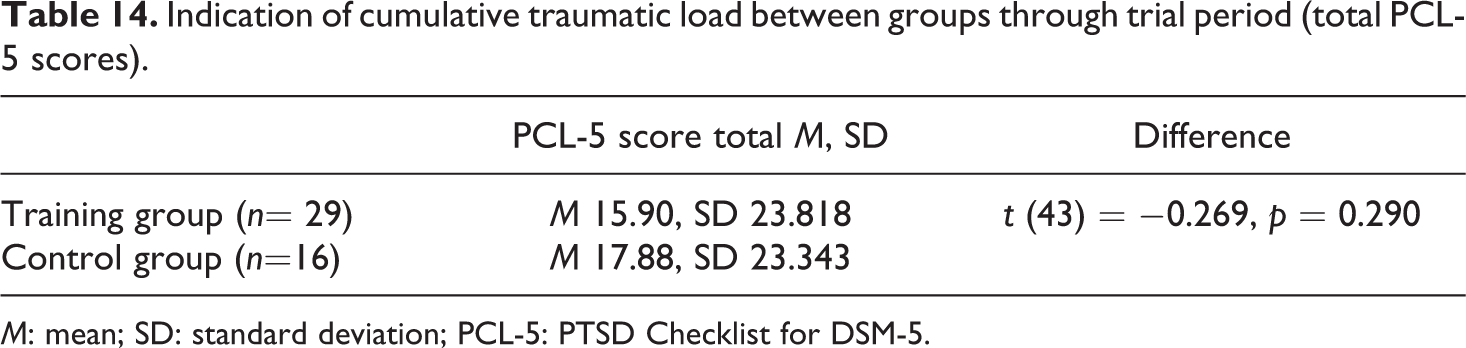
M: mean; SD: standard deviation; PCL-5: PTSD Checklist for DSM-5.
PCL-5 scores were analysed by diagnostic cluster to assess whether there were any symptoms that were particularly common to the policing sample as a whole (see Table 15). A repeated-measures analysis of variance revealed no significant between-group differences, f (42) = 0.072, p = 0.790. Summary t-tests were undertaken in across the sample population (n = 45) which revealed ‘avoidance’ to be less of an issue than ‘negative alterations in mood’, t (88) = 2.28, p = 0.028, and ‘arousal’, t (88) = 1.26, p = 0.048.
Frequency of PTSD symptom clusters using the PCL-5 with both groups.
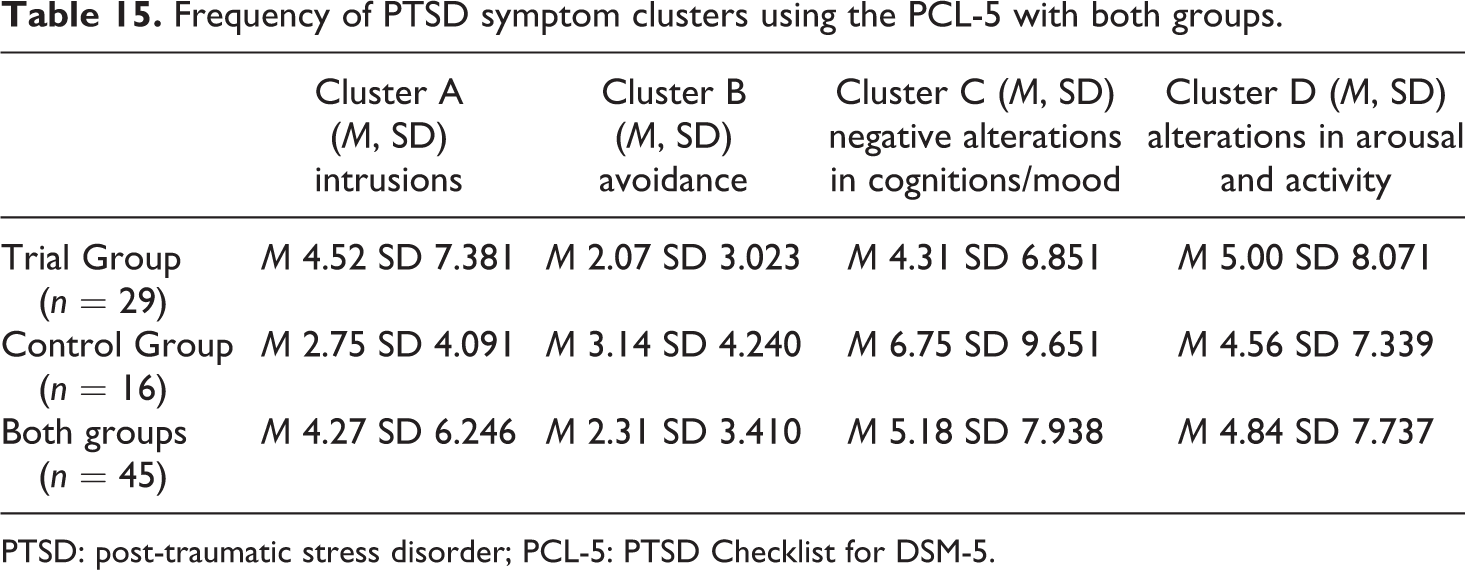
PTSD: post-traumatic stress disorder; PCL-5: PTSD Checklist for DSM-5.
Trauma exposure coding was undertaken using basic thematic analysis (Currie et al., 2014; Skinner et al., 2019) to see whether it was possible to detect any typical ‘first trauma exposures’ 7 in new recruits. Themes were extracted from monthly check-ins from March onwards 8 (n = 71) and the difficult or traumatic incidents participants selected in session 2 training (n = 32) and session 3 control group training (n = 28). Themes from 158 separate recorded incidents were categorised as death, extreme violence, suicide and road traffic collisions and a total of 214 exposures were coded to these themes (see Table 16).
Frequency of coded trauma exposures using categories of ‘death, extreme violence, suicides and road traffic collisions’, taken from recruits’ monthly check-in and training sessions data.
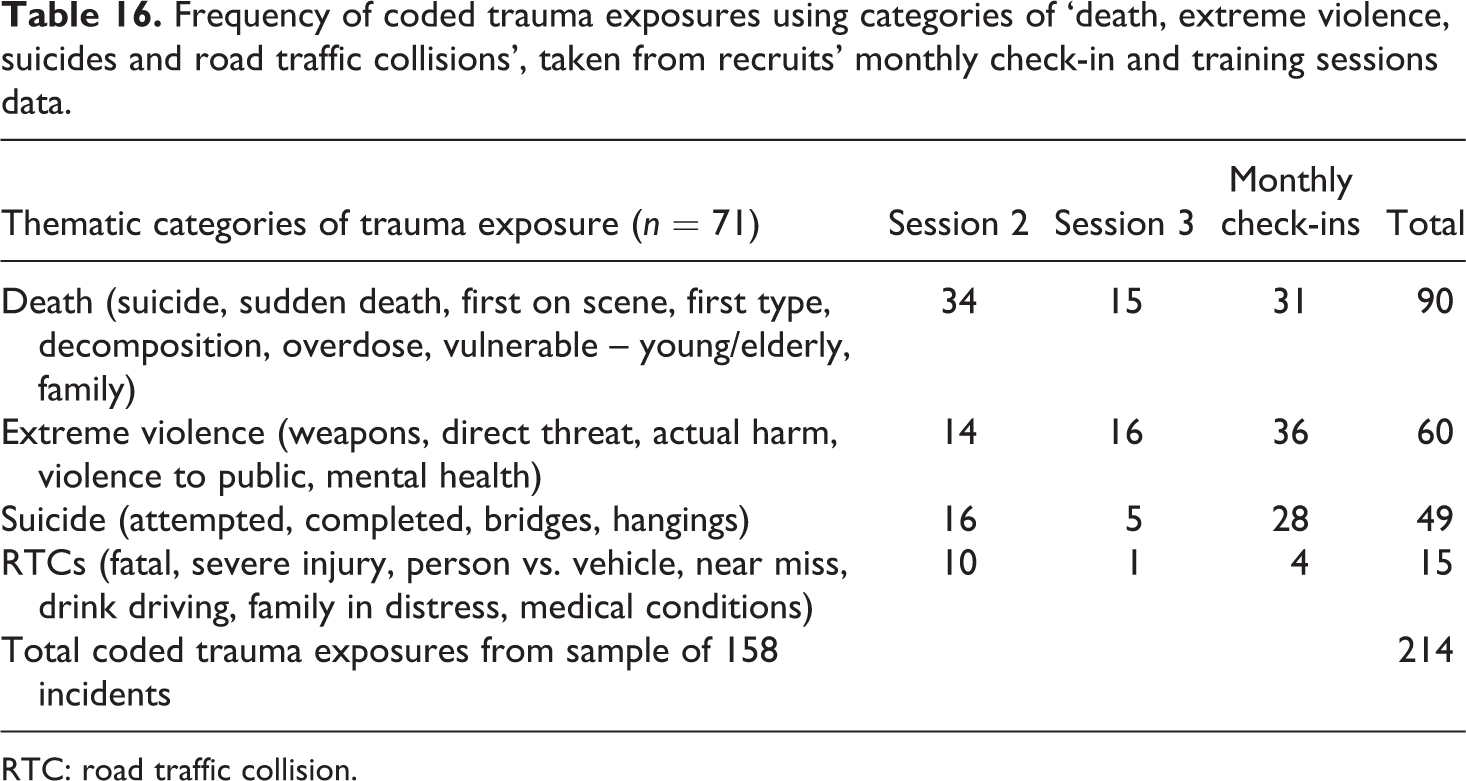
RTC: road traffic collision.
Discussion
In summary, findings suggest that techniques are clearly beneficial in training sessions, the training should account for individual differences, applying the techniques requires some effort, and that some types of trauma exposure in newly recruited police are more common than others.
Research questions for the feasibility study were as follows: can the techniques be taught at all in this operational policing setting, how feasible is it to test the impact of the techniques over time and what types of trauma exposure might new recruits expect in their first few months?
To answer these questions, we reflect on this feasibility study’s findings and its limitations in scientific assessment, processes, management and resources (Tickle-Degnen et al., 2013).
Findings
Officers’ ease of feeling about difficult or traumatic incidents seemed to immediately benefit from training sessions. The observation that no participants reported a negative change regarding how at ease they felt about the incident is a good indication that the techniques did no harm in session. Qualitative responses from participants provided unexpected insights into the positive impact of the sessions, with many reporting a helpful sense of depersonalisation (‘it wasn’t all about me’), an appreciation of transience (‘it’s over’) and of time expanding around the incident (allowing individuals to notice much more about it than their contracted sense of immediate panic at the time). It is important to note that one cannot be clear at this stage if this improvement in ease of feeling may have longer term impact on trauma resilience.
The study also shed light on how officers’ personal differences might disrupt their engagement with the training, but not the outcomes. For example, age had a negative impact on ease of feeling about a difficult or traumatic incident before using the techniques, but the effect disappeared once they had applied them. Officers also differed greatly in their ability to apply the most challenging technique, the shifted overhead view. This observation goes some way to prove the concept that hippocampal-dependant spatial processing of trauma may require a ‘boost’ to ensure that all individuals have the best chance of committing difficult or traumatic incidents to memory. Some variation in participants’ hippocampal-dependent processing emanated from age and previous trauma exposure. Given neuropsychological evidence that age and trauma exposure impair hippocampal function (even in non-clinical populations), this is not surprising (Miller et al., 2017). Previous trauma was also a factor in participants’ ability to recall new details about the event and this makes sense if we acknowledge established evidence that trauma impairs episodic memory function (Kesner et al., 2008).
There is some evidence to suggest that individual variation in applying spatial processing techniques can be mitigated against by practicing them. In this study, the training group (who had had more practice applying the mapping techniques by their second session than the control group had) exhibited markedly more recall from using mapping techniques. In another study about lie detection (Vrij et al., 2017), researchers found it was the deliberate effort applied to constructing an overhead depiction of a scenario that distinguished deception from honesty. Those telling the truth would naturally recount their experiences from a ground level position (as 67% of participants in our study reported). Encouraging individuals to shift from ground level to overhead views may be more of a challenge for some, but studies like these are pointing to flexible spatial processing as being a key marker of integrity in recall and a precursor for successful trauma processing.
Limitations
With regard to scientific assessment, in-session data collection was underpowered. Significant differences in feeling at ease with an incident were not expected immediately in session. Lack of an in-session control group means that any positive effect of merely spending time reflecting on an incident in a protected setting remains unquantified. A distraction task or a timed rumination exercise may provide future studies such control data. Similarly, more sophisticated forensic experimental measures of recall may be useful (rather than simply itemising new details) if or when studying the implications of the techniques for forensic investigation.
Under-reporting of trauma impact among newly recruited police was a potential cultural bias in the process (Fielding et al., 2017; Soomro and Yanos, 2018). However, given the plethora of personal, environmental and genetic conditions that may also influence trauma impact reporting (Brewin et al., 2000; Miller et al., 2017), the risk such bias posed was deemed minimal. What is more, traumatic load across groups and classes was comparable, which suggests some stability of reporting in the sample population.
Managing missing values online and in-session presented problems in this model. Operational demands (especially during exam periods) conflicted with pressure on participants to check in on a monthly basis. This may account for missing data in check-ins. Such demands may also have had a negative effect on attention span in session. Post hoc analysis illustrated check-ins being more frequent when officers had less trauma impact to report (see Figure 3). This relationship may infer a risk to validity in any study which consistently relies on participants’ capacity (and inclination) to reflect on their well-being in times of acute stress.
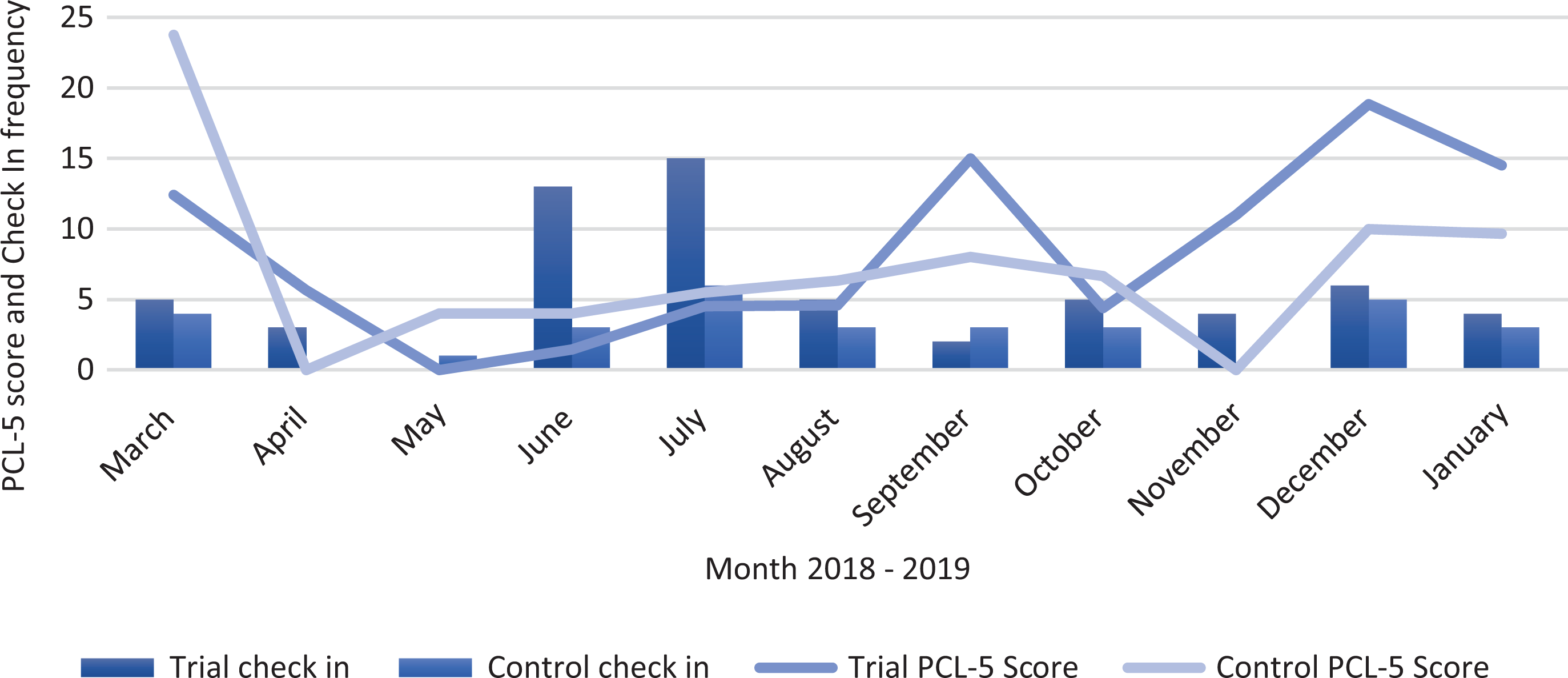
Monthly check-in frequencies and trauma impact scores for trial and control groups.
PTSD cluster data indicated that across the sample, negative alterations in mood and arousal may be more common in police recruits than avoidance. Initial comparison with a larger PTSD data set (the unpublished The Job and The Life Survey from 2019, n = 16,857) suggests that these symptoms may be comparable in healthy officers (with a mean of 15 years in service), with 43% reporting heightened sense of threat (arousal) and only 28% reporting avoidance.
The study population was originally planned to be n = 30, but recruitment was increased threefold following the Manchester Arena attack. The research team was grateful for the training support commandeered from experienced individuals from other forces and networks. Their input included translation of the techniques into policing-relevant scenarios using everyday operational language and providing real-life examples of their practical application. The officers also provided additional welfare support during sessions, which any large-scale study needs to seriously consider when inviting trauma-exposed individuals to re-familiarise themselves with incidents some would rather forget.
Conclusion
To conclude, we first ask, whether the techniques be taught at all in an operational policing setting? This feasibility study strongly suggests they can. Even the most demanding of techniques were consistently deemed useful, and engagement levels with techniques such as the Safety Cue were unprecedented. Qualitative feedback communicated high advocacy for the techniques even after one session, in both training and control groups. In-session controls would help future research better quantify and validate the direct impact of the techniques. (It is worth noting that using GPower™ software, a sample size of n = 447 would be needed to replicate the significant improvement in ease of feeling about a traumatic incident with a medium effect size.)
Secondly, we ask, how feasible is it to test the impact of the techniques between people and over time? The answer to this question is encouraging, albeit more complex. Between-group analysis of trauma impact over the 11 months was hindered by the small window of time during which the new recruits were actually out on full responsive duty (i.e. from September to the end of January). The immediacy of the techniques’ positive impact in session does suggest them to be a simple, cost-effective intervention. Uptake and engagement are important factors to consider if replicating this research. Group differences in check-in data showed individuals in the control group reported initial high trauma impact, then refrained from reporting, until gradually resuming. However, over the course of the study, the trial group reported slightly higher levels of trauma impact overall. Checking in patterns were consistent in both groups, suggesting that differences in workload did not account for these divergent behaviours. Whether training groups inferred ‘permission’ to report trauma impact more than control groups should be considered with respect to potential bias.
Together, these observations (accompanied by the understood limitations of controlling for personal, environmental and genetic conditions) suggest that to demonstrate statistically significant group differences in trauma impact as a direct result of training in these techniques, studies would need to be conducted on larger scale over a larger period of time. Future studies would also do well to include officers and staff with longer years’ service and experience than the newly recruited. Considering existing literature on police-related PTSD, studies like this that address the stigma of self-reporting trauma impact, which encourage self-assessment and demonstrate the successful operational application of neuropsychological techniques to improve trauma processing, can go far in meeting the very real challenge of traumatic stress in contemporary policing.
Footnotes
Acknowledgements
The authors would like to thank Professor Chris Brewin (University College London), Greater Manchester Police, Kevin Maddick and Lee Jackson (Durham Constabulary), Ewen Sim (Lancashire Constabulary) and Prof Neil Greenberg (King’s College London).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Police Care UK, registered charity in England and Wales (1151322) and Scotland (SC0047767).