
Abstract
The aim of the present study was to explore the mediating role of patience on the relationship between mindfulness and suicide ideation. To do so, 110 patients with cardiovascular diseases were recruited from the outpatient Clinic of Imam Reza in the city of Shiraz in Iran. These patients completed The Five Facets Mindfulness Questionnaire, Patience Scale, and Suicide Ideation Questionnaire. Data were analyzed using structural equation modeling. Results indicated a significant positive relationship between mindfulness and patience (r = .32, p < .001). There was a significant negative relationship between patience and suicide ideation (r = −.36, p < .001). The results of mediating model showed that patience functioned as a mediator in the relationship between mindfulness and suicide ideation among patients with cardiovascular diseases (β = −.33, p = .005). According to these findings, it can be claimed that mindfulness affects patients’ suicidal thoughts negatively through patience.
Introduction
Research has shown that suicide ideation is more common among patients with physical health problems and specific medical conditions than among the normal population (Druss & Pincus, 2000; Goodwin, Kroenke, Hoven, & Spitzer, 2003; Goodwin, Marusic, & Hoven, 2003). For heart attack patients, the risk for suicide is tripled after getting discharged from the hospital (Rettner, 2010). Individuals with chronic physical ailments such as cardiovascular diseases often experience psychological problems (Rector, Anand, & Cohn, 2006) such as depression and anxiety (Shen et al., 2011), self-harming ideas (Marusic & Goodwin, 2006), death anxiety (Valikhani & Yarmohammadi-Vasel, 2014), and undesirable quality of life (Lossnitzer et al., 2009). In these patients, psychological and physical problems are often intertwined. Accordingly, they experience an overwhelming suffering in their life. Moreover, a high rate of psychological disorders comorbidity with physical illness complicates the understanding of the potential risk of medical conditions for suicide.
Suicidal processes are described as a spectrum that begins with suicide ideation, followed by planning, attempting, and finally, committing suicide (Bertolote et al., 2005). Suicide ideation is considered as a risk factor for suicidality and can be regarded as a useful preliminary measure of suicide attempt (McAuliffe, 2002). It can also be considered as an important parameter in identifying vulnerable individuals who are at risk of suicide attempt as well as a potential target for intervention (Fialko et al., 2006). In addition, cross-national studies have shown that 60% of transitions from suicide ideation to first suicide attempt occurred within a year of the onset of suicide ideation (Nock et al., 2008). Hence, to prevent committing suicide, the first priority is to identify suicide ideation. Therefore, due to the relationship between suicide ideation and suicide attempts and high prevalence rate of suicide ideation in patients with physical illnesses such as cardiovascular diseases (Rettner, 2010), it seems necessary to investigate and determine the related factors among this population. Although the relationship between religion and suicide attempts has received less attention (Dervic et al., 2004), research suggests that spirituality, morality, and religion have undeniable impact on suicide-related behaviors (Dervic et al., 2004; Rasic et al., 2009; Stack & Lester, 1991).
Mindfulness has been described as “the nonjudgmental observation of the ongoing stream of internal and external stimuli as they arise” (Baer, 2003, p. 125). The benefits of mindfulness practices have been recognized by nearly every religious tradition, which date back thousands of years (Fletcher & Hayes, 2005). It is one of the psycho-religious elements in Buddhism that has an important role in mental health. Mindfulness was found to lead to positive psychological health, reduced psychological symptoms, and improved behavioral regulation (Keng, Smoski, & Robins, 2011).
More recently, the so-called third wave of behavioral and cognitive therapies has recently emerged combining techniques from cognitive behavioral traditions with issues those of mindfulness. Approaches, such as Dialectical Behavior Therapy (DBT) and Acceptance and Commitment Therapy (ACT; Fletcher & Hayes, 2005), include mindfulness elements. The core of DBT is the relationship between acceptance and change. Patients are encouraged to accept themselves, their histories, and their current situations and conditions as they are, while working intensively to change their behaviors and environments in an attempt to build a better life. The synthesis of this seeming contradiction is the most important goal of DBT. Mindfulness skills are incorporated within DBT in the context of synthesizing acceptance and change. In addition, ACT embraces mindfulness. Patients enrolled in ACT are instructed to identify an observing self who is capable of watching his or her own bodily sensations, thoughts, and emotions. They are encouraged to see these phenomena as separate from themselves. These suggest that mindfulness training is consistent with cognitive-behavioral treatment procedures in many ways (Baer, 2003).
Little research has examined the direct effect of mindfulness on suicidality. But numerous studies have investigated the relationship between mindfulness and psychological factors associated with suicide ideation and action. It is assumed that mindfulness enhances well-being and mental health. It reduces depression, anxiety, and even pain (Thompson, 2010). Mindfulness-based intervention is a promising intervention for vulnerable individuals who experience suicide ideation (Williams, Duggan, Crane, & Fennell, 2006). Cognitive inflexibility (Miranda, Valderrama, Tsypes, Gadol, & Gallagher, 2013), perfectionism, and negative cognitive bias (Beevers & Miller, 2004) increase individuals’ vulnerability for suicide. Mindfulness was found to be inversely related to these measures, as it involves flexible attention and attention to the present (Bishop, 2002). Mindfulness is negatively associated with two strong risk factors for suicide including depression (Keune, Bostanov, Kotchoubey, & Hautzinger, 2012; Lamis & Dvorak, 2014) and neuroticism (Hollis-Walker & Colosimo, 2011; Latzman & Masuda, 2013). It also reduces the risk for suicidality through reducing experiential avoidance (tendency to escape or avoid unwanted psychological experiences) which is a pathway leading to suicidal behavior (Luoma & Villatte, 2012) and suicide rumination (Lamis & Dvorak, 2014).
Patience is another psycho-religious construct that has recently been proposed in the psychological literature. Patience is one of the key issues in ethics and is one of the moral concepts emphasized in Islamic ethics (Khormaei, Farmani, & Soltani, 2013) and other religions such as Christianity, Judaism, and Buddhism. Khormaei and Farmani (2015) have defined patience as a moral virtue which refers to persistence, forbearance, restraint, acceptance, and transcendence one can reach in difficult and unpleasant situations. Using this definition, patience is an active process that makes the individual not to complain, have fortitude when confronting with difficult and sometimes impossible to change situations, and be stable in carrying out the activities. Moreover, it makes him or her restraint against inner urges and use hardships and adversities as means to achieve transcendence. It is one of the most important elements of faith that is related to many cognitive, affective, and behavioral characteristics of a person (Khormaei et al., 2013; Khormaei, Zarei, Mahdiyar, & Farmani, 2014). In fact, patience means to postpone desires to achieve a higher purpose (transcendence), endurance under difficult circumstances and fortitude in the face of adversity (forbearance), acceptance of situation and the circumstances in which a person is (acceptance), stability in doing activities (persistence), and interruption or restraint against the wishes and desires (delay; Shekoofefard & Khormaei, 2012; Khormaei et al., 2013).
In Western psychology literature, there is no general agreement on the definition and nature of patience. In a general sense, patience is defined as a psychological attribute that affects an individual’s response to different situations. In this sense, patience is defined as the propensity to delay immediate gratification in favor of future rewards (Fowler & Kam, 2006). Based on this psychological definition, those who are more patient would be more likely to exhibit delayed gratification behaviors (Fowler & Kam, 2006). Stevens and Stephens (2008) have defined patience as the ability to wait for larger, later rewards in situations that waiting for the larger, later options increases the possibility of greater benefits. Another definition of patience is the individual’s propensity to stay calm in the face of failure, misery or suffering (Schnitker, 2012). It is clear that in Western psychology, patience is enacted in mundane activities such as waiting in traffic. In these definitions, the emphasis is on time (Schnitker, 2012). Furthermore, in Western psychology, patience is not regarded as a psycho-religious construct. In animals, patience may be referred to as called self-control or delayed gratification. Patience is often a religious construct by which a person achieves transcendence by enduring suffering. Accordingly, the spiritual aspect of patience in Western psychology has received little attention. In the West, patience is considered as a behavioral and emotional component but patience has a cognitive aspect as well (belief that tragedy is a divine test). Hence, the structure of patience that is recently suggested by Khormaei, Farmani, and Soltani (2015) includes the missing part of patience, that is, the issue of religion or spirituality, faith in God, as well as components of faith and belief.
It is not surprising that very little research has been conducted in relation to patience, as its emergence in psychological literature is new. Research conducted on this issue is presented below: Studies have shown that there is a significant negative relationship between patience and aggression and hopelessness (Shekoofefard & Khormaei, 2012), Neuroticism (Khormaei & Farmani, 2015), depression and anxiety (Kalantari, 2011) and suicidal ideation (Haghjoo, 2013). Other studies have shown that there is a significant positive relationship between patience and hope (Khormaei et al., 2014) and agreeableness, extraversion, and conscientiousness (Khormaei & Farmani, 2015).
It is well accepted that religion acts as a protective factor against suicidal behavior. Studies have shown that spirituality and religiosity are associated with lower approval of suicide (Stack & Lester, 1991). Therefore, they reduce the probability of suicide attempts in the general population (Neeleman, Wessely, & Lewis, 1998; Rasic et al., 2009). Religious affiliation reduces risk-taking behaviors such as impulsivity, aggression, and substance abuse; factors that place individuals at higher risk for suicide (Dervic et al., 2004). The investigation of suicide-related beliefs shows that some issues are common in different religions: on a macro level, different religions, including Judaism, Christianity, Islam, Hinduism, and Buddhism, oppose suicide and place great importance on human life. Suicide implications for life after death play an important role in each religion’s core beliefs regarding suicide (Nelson, Hanna, Houri, & Klimes-Dougan, 2012).
Bring a quality of kindliness to our awareness, perhaps seeing the repeated wanderings of the mind (being mindfulness) as great opportunities to bring patience and gentle curiosity to your experience (Thompson, 2010). Patience is seen as an attitude which is included and enhanced by practicing mindfulness (Shapiro, Carlson, Astin, & Freedman, 2006; Kabat-Zinn, 1994; Fulton, 2009; Goodman & Greenland, 2009; Kabat-Zinn, 1990). In fact, by returning again and again to the breath without judgments, we manage to cultivate patience and gentleness toward ourselves (Thompson, 2010). Hence, based on a review of the literature on the relationship between psycho-religious variables and suicide ideation, in the present study, it was hypothesized that mindfulness can reduce suicide ideation through patience in cardiovascular patients (See Figure 1).
Method
Sample and procedure
A correlational design was employed in this study. A total of 110 cardiovascular patients (Mage = 46.62, SD = 15.45), referring to the clinic of Imam Reza in Shiraz, Iran, were selected using convenience sampling method; 57.8% of participants were male (Mage = 44.95, SD = 14.76) and 42.2% were female (Mage = 49.19, SD = 16.30). Participants were in the age range of 17 to 84. Regarding marital status of the study sample, 80.6% were married while 19.4% of them were single. Furthermore, regarding economic status, 15% of the sample was at low level while 66.4% were moderate and 18.7% were in good economic status.
The authors interviewed cardiovascular patients who referred to the clinic and after obtaining fully informed consent, administered the questionnaires. All patients were informed that participation was voluntary, and they were also informed that the information would be kept confidential. The study was approved by Shiraz University of Medical Sciences ethics committee.
Instruments
Patience Scale
Patience Scale was developed using religious components. Accordingly, patience is a moral virtue and it is the key to deal with difficult and unpleasant situations in life. This scale was developed by Khormaei et al. (2015). It is a 25-item, five-point scale. The scale gives five options scored 1 to 5 (1 = completely false to 5 = completely true). In order to examine the psychometric properties of the Patience Scale, 516 university students were recruited using random cluster sampling method. The results of the factor analysis yielded a five-factor structure. Five factors explained 52% of the variance. These components were named as transcendence (enduring hardships and being tolerant in sufferings and adversities to achieve divine revelation and spiritual growth, e.g., forbearance is a way of getting closer to god), forbearance (enduring sufferings and fortitude in the face of hardships; e.g., if I lose one of my beloved persons, I can tolerate it), acceptance (acceptance of the present, no complaining, and being satisfied with one’s being; e.g., I do not consider what happens to me as divine destiny and I am not satisfied with them), persistence (stability in doing the work; e.g., obstacles and difficulties have not been able to make me away from my goals), and delay (disruption to the wishes and desires, controllability of the internal desires, e.g., I can control myself against temptation). Cronbach’s alpha coefficients were calculated to be .84, .67, .60, .61, and .68 for components of transcendence, persistence, acceptance, forbearance, and delay, respectively. Cronbach’s alpha of .86 was obtained for the total scale (Khormaei et al., 2015). In this study, the Cronbach’s alpha for total scale, and subscales of transcendence, forbearance, acceptance, persistence and delay were calculated to be .82, .79, .65, .57, .47, and .51, respectively.
The Five Facets Mindfulness Questionnaire
The Five Facets Mindfulness Questionnaire (FFMQ; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) is currently one of the most comprehensive scales assessing mindfulness. FFMQ is a 39-item measure consisting of five subscales (observing, describing, acting with awareness, nonjudging of inner experience, and nonreactivity to inner experience). Items are rated on a five-point Likert-type scale ranging from 1 to 5 (1 = never to 5 = always). Cross-cultural studies related to the psychometric properties of FFMQ have shown good and acceptable reliability and validity. For instance, Hou, Wong, Lo, Mak, and Ma (2014) found that the Chinese version of FFMQ had good psychometric properties. In Iran, Heidarinasab, Ahmadvand, and Shaeeri (2013) validated the Iranian version of FFMQ. Test-retest reliability was calculated to be .80. Alpha coefficients for subscales were as follows: observing .71, describing .83, acting with awareness .81, nonjudging of inner experience .73, and nonreactivity to inner experience .55. The total Cronbach’s alpha coefficient was .80. All subscales of the mindfulness scale had a significant and positive correlation with six components of well-being (convergent validity). In another study in Iran, the results of exploratory factor analysis revealed that five subscales of FFMQ explained 45% of total variance (Kalantari, 2011). Cronbach’s alpha coefficient was calculated to be .81, .77, .65, .63, and .62 for components of describing, acting with awareness, nonjudging, nonreactivity to inner experience, and observing, respectively. In the present study, Cronbach’s alpha coefficient was calculated to be .80, .67, .67, .84, .73, and .59 for total scale, observing, describing, acting with awareness, nonjudging, and nonreactivity, respectively. Based on these findings, the Iranian version of FFMQ has good psychometric properties and structural validity similar to the initial version.
Suicide Ideation Questionnaire
Suicide ideation was measured by a self-report questionnaire consisting of three questions. This questionnaire directly measured suicide ideation and its intensity. These three questions were designed on the basis of studies in this area. Participants were asked to answer the following questions: “In the last year, how much did you have thoughts about suicide?” (Never = 0, rarely = 1, sometimes = 3, often = 4); “During your life, how much have you had thoughts of suicide?” (Never = 0, rarely = 1, sometimes = 3, often = 4); and “Have you ever committed attempted suicide?” (Never = 0, once = 1, twice = 2, three times or more = 3). Alpha coefficient was calculated to be .81 for total questionnaire.
Statistical analyses
First, descriptive statistics was used to describe the data. Then, the normality of data was tested. Results showed that all variables were normally distributed. Pearson correlation coefficient was used to examine the relationship between variables. Then, structural equation modeling was used by the application of software Amos 16.0 to test the mediating role. Three latent variables used in the model are as follows: Mindfulness (as the independent variable; using its four subscales as its indicators), suicide ideation as dependent variable, and latent variable of patience (using its five subscales as its indicators) as a mediatory variable. Finally the indirect effect of mindfulness on suicide ideation via the mediator patience was tested with bootstrap method with 5,000 resampling and Monte Carlo with a confidence level of 0.95 (Preacher & Hayes, 2008). To examine the given model fit with data, the following fit indicators were utilized: χ2/df ratio (Byrne, 1989), the comparative fit index (CFI; Bentler, 1990), the goodness of fit indicator (GFI; Hu & Bentler, 1995), and the root mean square error of approximation (RMSEA; Browne & Cudeck, 1993).
Results
Pearson correlation coefficients between variables (n = 110).
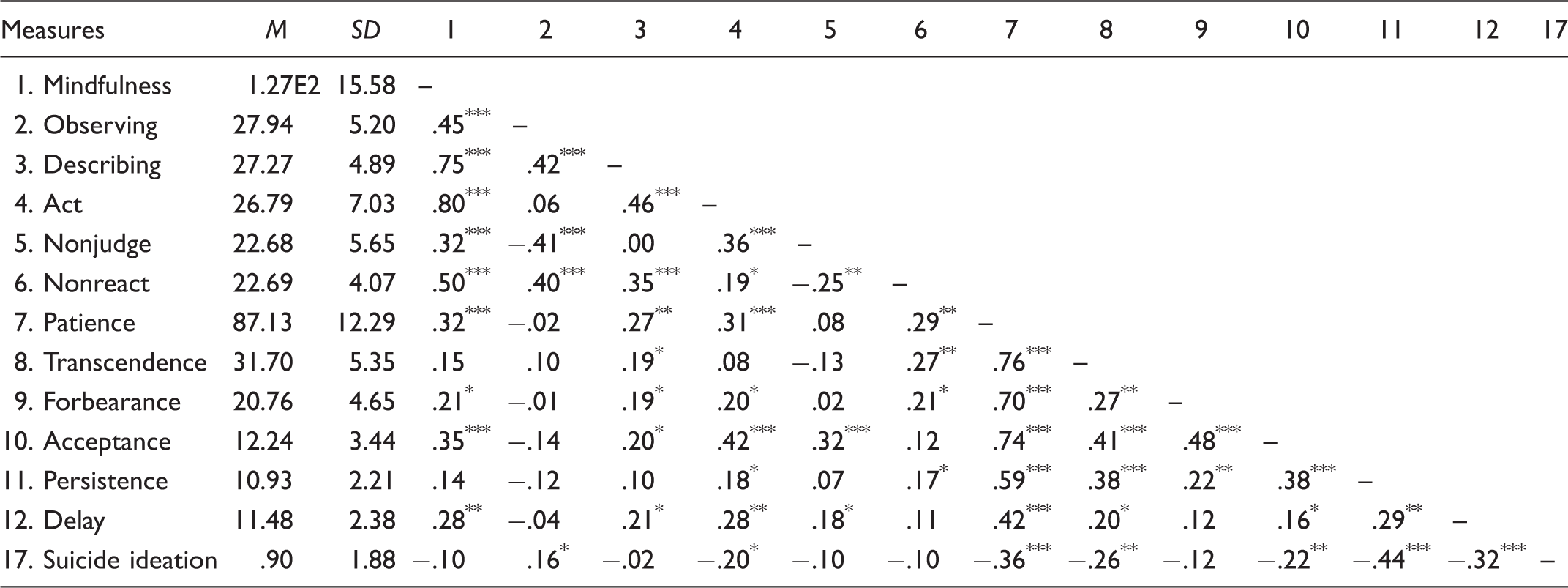
p < .05, **p < .01, ***p < .001.
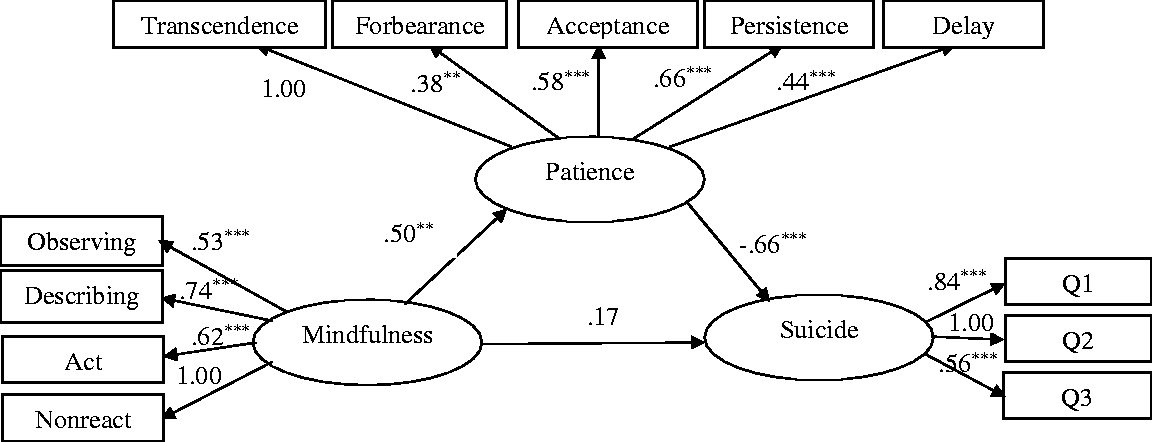
Structural equation modeling was used to examine the mediating role of patience in the relationship between mindfulness and suicide ideation. The results are presented in Figure 2. The results showed a good fit for the data (χ2 = 71.845, df = 47, χ2/df = 1.528, p = .011, GFI = .90, CFI = .93, RMSEA = .07). The structural equation modeling results indicated that mindfulness had a strong positive direct effect on patience (β = .50, p = .005). The effect of patience on suicide ideation was significant, strong, and negative (β = −.66, p < .001), but the direct effect of mindfulness on suicide ideation was not significant (β = .17, p = .204). Therefore, it can be inferred that patience mediated the relationship between mindfulness and suicide ideation (β = −.33, p = .005). Mindfulness can influence suicide ideation negatively through patience. Our findings suggest that patience fully mediated the relationship between mindfulness and suicide ideation.
The theoretical graph of mediating role of patience on the relationship between mindfulness and suicide ideation. Mediating role of patience on the relationship between mindfulness and suicide ideation. Indirect effect of mindfulness on suicide ideation through patience was significant (β = −.33, p = .005). This model fit the data: χ2 = 71.845, df = 47, p = .011, goodness of fit indicator = .90, comparative fit index = .93, root mean square error of approximation = .07. **p < .01, ***p < .001.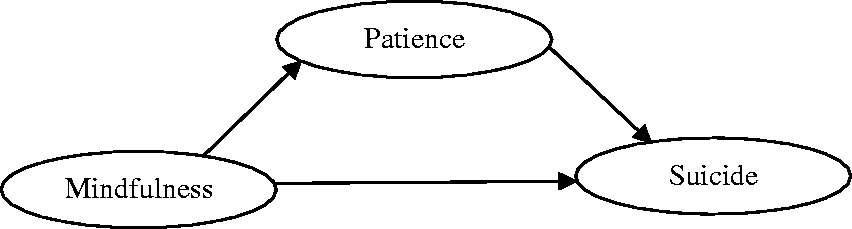
Discussion
This study aimed at investigating the mediating role of patience on the relationship between mindfulness and suicide ideation. As hypothesized, structural equation model results showed that patience mediated the relationship between mindfulness and suicide ideation. The findings also showed that patience was significantly and negatively related to suicide ideation and significantly and positively associated with mindfulness.
The structural equation modeling results also showed that patience can strongly and negatively influence suicide ideation. This means that patience and suicidal thoughts are intricately related. This finding is consistent with the findings of Haghjoo (2013), whose results showed that the components of patience can negatively predict suicide ideation among university students. Moreover, her results are also consistent with the results of several studies showing that religion and spirituality are negatively associated with suicidal behavior (Hovey, 1999; Neeleman et al., 1998). Various studies have shown that religiosity and spirituality act as important protective factors against suicidal behavior and are considered as effective coping strategies in suicide prevention. Suicide is considered as a violation of most, if not all, religious principles. Accordingly, religious affiliation causes people not to approve suicidality (Nelson et al., 2012). Therefore, it can be claimed that suicide is considered as a serious sin and violation of religious principles and for many religious people, as suicide act will be punishable in the hereafter and many of them are fearful that hell will be the consequence for suicide behavior. Accordingly, this belief may have significant implications for individual’s likelihood of engaging in this behavior. In addition, there are some individuals who do not believe in a particular religion and there are religious people who do not consider fear of hell or guilt as reasons for not committing wrong behaviors such as suicide; those individuals believe that suffering and catastrophes are divine tests, and thus have fortitude in face of these difficult conditions (Izad, 2010). They also consider these tragedies as a chance not a threat and use hardships and adversities as means to achieve transcendence and get closer to god. They do not complain about these problems and also show endurance during suffering times in order to achieve god’s approval (Khormaei & Farmani, 2015).
Our findings also showed that mindfulness did not have a significant relationship with suicide ideation. So far, little research has investigated the direct relationship between mindfulness and suicide ideation. Nevertheless, studies have shown that mindfulness has a negative relationship with substance abuse, impulsivity, anger, depression, anxiety, stress, pain, aggression, and neuroticism (Brown & Ryan, 2003; Greeson, 2009; Keune et al., 2012; Walsh, Balint, Smolira, Fredericksen, & Madsen, 2009), and a positive relationship with self-acceptability, emotional regulation, and extroversion (Dekeyser, Filip, Mia, Sara, & David, 2008; Jimenez, Niles, & Park, 2010). Therefore, our findings are not consistent with some prior studies. Several explanations can explain these conflicting findings: Given that very little research has been conducted on mindfulness and suicide ideation, the functional mechanism explaining the effect mindfulness on suicide ideation differs from that of other psychological variables such as depression. Accordingly, some other factors are needed to explain suicidal ideation by which mindfulness influences suicidal ideation. This is explained in detail in the model of this study discussed below. Moreover, the sample of the present study consisted of patients with heart diseases, including individuals who experienced serious damages in such a way that just mindfulness alone may not influence their suicide ideation behavior. However, future research should further study the relationship between mindfulness and suicide ideation in clinical and nonclinical populations.
The most important finding of the present study was the confirmation of the mediating role of patience on the relationship between mindfulness and suicide ideation. Mindfulness did not have a direct impact on suicide ideation; it influenced suicide ideation through patience. It can be claimed that faith in extraterrestrial beings is related to suicide ideation prevention as confirmed by many studies (Kay & Francis, 2006; Nelson et al., 2012). It is possible that mindfulness practice is related to their threshold of enduring hardships through increasing forbearance, persistence, delay, and acceptance. By increasing acceptance, mindfulness leads to fewer complaints about problems and hardships. It also reinforces religious individuals’ belief in achieving transcendence that can change the way they view hardships and causes them to consider hardships as divine tests (Izad, 2010). In fact, mindfulness is negatively related to suicide ideation creating useful coping strategies such as forbearance, acceptance, persistence, and delay (components of patience). These factors may relate to how a person chooses more adaptive responses instead of suicidal behaviors in the face of difficulties and diseases. This kind of response is not only passive and negative but also gives a new meaning to life.
Our study has some limitations which can guide future research. One of the limitations of the present study was that it relied on self-report data and correlational analyses which does not reveal the casual relationship among studied variables. Therefore, in order to test the casual relationship between patience and suicide ideation, an experimental manipulation of mindfulness or a longitudinal design is needed. One other limitation is the sample size was small, as data were collected at one place. Further, because of sampling patients with cardiovascular diseases, the results cannot generalize to other populations or religions. In addition, future research should focus on recruiting a homogenous group in terms of having similar ages and only one kind of cardiovascular disease.
Implications for practice
This study establishes some practical recommendations. As mindfulness training is used for the prevention of suicide-related behaviors, especially those who are physically ill such as cardiovascular patients, we should also pay attention to the religion and spirituality of the patients. Therefore, paying attention to the religious affiliation of patients may increase the efficiency of mindfulness particularly for suicide behaviors. Patience education can possibly reduce recurrent suicide ideations, as it has a major effect on reducing or managing mental disorders (Kalantari, 2011).
Footnotes
Acknowledgments
The authors would like to thank the officials and cardiologists in the clinic of Imam Reza in Shiraz city and the patients who participated in this study.