
Abstract
Behavioral activation is a brief, structured psychotherapy. It focuses on avoidance behaviors as well as activation of healthy behaviors, which together lead to the improvement in depression through increase in positive reinforcement. This study examined this mediation model in a community sample in Japan. The participants were 661 people (323 men and 338 women). Their average age was 36.98 years (SD = 12.91). Mediation analysis supported a partial mediation model and showed that activation and avoidance have direct effects on depression as well as indirect effects through positive reinforcement. The difference between the results of this study and those of the previous studies, which supported a complete mediation model, may occur because of characteristics of the community sample as distinct from previous studies’ undergraduate samples.
Introduction
Depression is one of the most common mental disorders and a major mental health issue. The US-based National Comorbidity Survey Replication (Kessler et al., 2003) reported that the prevalence of depression over a lifetime was 16.2% and that for a 12-month period was 6.6%. An epidemiological study in Japan (Kawakami, 2006) reported that the prevalence of depression over a lifetime was 6.3% and that for a 12-month period was 2.1%. Although Japan tends to have a lower prevalence rate than the United States, researchers argue that it is the most common mental disorder among people living in the country. Depression has resulted in enormous economic losses owing to sufferers’ outright inability to work or need to take leave due to absence from work. According to Sado et al. (2011), the disease burden related to depression in Japan in 2005 was estimated at 2 trillion yen. This cost may be broken down as follows: The direct costs related to inpatient and outpatient medical treatment for depression during this time were 0.18 trillion yen; moreover, the morbidity cost was 0.92 trillion yen, while the mortality cost was 0.88 trillion yen. Accordingly, there is a need for effective treatment. There is also a need to clarify the mechanisms of depression in order to deliver evidence-based healthcare.
According to the behavioral theory of depression, a low rate of response-contingent positive reinforcement (RCPR) leads to depression (Lewinsohn, 1974). Based on this theory, the behavioral treatment for depression, originated by Lewinsohn and his colleagues in the early 1970s, attempted to increase pleasant events and decrease unpleasant events. This behavioral treatment was also incorporated into cognitive therapy (Beck, Rush, Shaw, & Emery, 1979) based on the results of Zeiss, Lewinsohn, and Munoz (1979). However, behavioral treatment attracted attention once again following Jacobson et al.’s (1996) component analysis of cognitive therapy. Martell, Addis, and Jacobson (2001) developed a stand-alone behavioral treatment, which is called behavioral activation. They were heavily influenced by Ferster (1973), who insisted that it is not just that depressed individuals have lost major sources of RCPR, but it is also that they may be inactive due to passive avoidance of aversive situations. In fact, Moulds, Kandris, Starr, and Wong (2007) showed a moderate relationship between avoidance and depression. In addition, behavioral activation emphasizes a functional analysis of contingencies of reinforcement operating for a particular individual, without assuming that engaging in activities that are formally pleasant will reinforce that individual (Martell, Addis, & Dimijian, 2004).
The effect of behavioral activation on depression has been examined in a randomized controlled trial at the University of Washington (Dimidjian et al., 2006; Dobson et al., 2008). The trial showed Martell et al.’s (2001) behavioral activation to be an effective treatment. Richards et al. (2016) compared the cost and outcome of behavioral activation with that of cognitive behavioral therapy (CBT) and reported that behavioral activation is no less effective than CBT while being less costly. In a meta-analysis conducted by Okajima, Kunisato, Nakajima, and Takagaki (2011), Cohen’s d, an indicator of the efficacy of behavioral activation, was 1.55 (95% confidence interval (CI): .70–2.40). According to Cohen (1988), d = .2 reflects a small effect size, d = .5 a moderate effect, and d = .8 a large effect. A more recent meta-analysis (Ekers et al., 2014) showed behavioral activation to be significantly superior to controls and medication. This confirms that behavioral activation is effective for improving depressive symptoms. Despite this evidence, the mechanism of changes in depressive symptoms during behavioral activation still remains unclear.
A few previous studies have examined the mechanism of changes in depressive symptoms under behavioral activation. For example, Yamamoto, Shudo, and Sakai (2016a) used structural equation modeling to show that behavioral activation and avoidance influence depression through RCPR. Carvalho and Hopko (2011) similarly revealed that RCPR mediated the relationship between avoidance and depression. Furthermore, Takagaki et al. (2016) found that score change in activation mediated the relationship between changes in RCPR and depression. All these studies thus support a mediation model.
However, in all these studies, the samples comprised undergraduate students. Therefore, they have some limitations in generalization to a general population. This study examined behavioral activation model in a community sample in Japan. Hypothesis: RCPR mediates the relationship between behavioral activation strategy (activation/avoidance) and depression symptom severity in a community sample in Japan.
Method
Participants
Participants were recruited by random selection from 7286 registered users of Fastask who were between 18 and 59 years of age. Fastask is an online research department of the Japanese company Justsystems. Those selected received invitation emails to a questionnaire survey. The first 700 to respond affirmatively participated in a computer-based questionnaire survey. A total of 661 Japanese people (323 men and 338 women; average age = 36.98 years, SD = 12.91; range = 18–59) whose informed consent was obtained participated in the questionnaire survey. Because of disapprobation, 39 people were excluded from this study. The rejection rate was 5.57%. Of the 661 participants, 12.93% were married without children and 33.95% were married with children. Moreover, 4.40% worked in the civil service, 39.00% worked for corporations, 5.57% were self-employed, 11.57% were full-time homemakers, 13.43% were part-time workers, and 19.00% were students. The remaining 7.03% of participants indicated “other” types of employment status.
Measures
Behavioral Activation for Depression Scale–Short Form
The Behavioral Activation for Depression Scale–Short Form (BADS-SF; Manos, Kanter, & Luo, 2011; Yamamoto, Shudo, & Sakai, 2015) is a shortened version of the Behavioral Activation for Depression Scale (Kanter et al., 2007), which was created to assess changes in activation and avoidance behavior, consistent with behavioral activation theory. The Japanese version of the BADS-SF is an eight-item (one less than the original scale) self-report measure designed to measure behaviors presumed to be targeted during BA treatment interventions, with two factors: activation and avoidance. Each item is rated on a seven-point Likert-type scale with anchors 0 (Not at All) and 6 (Completely). Scores range from 0 to 48, with higher scores reflecting higher level of behavioral activation and more avoidance behaviors.
Reward Probability Index
The Japanese version of the Reward Probability Index (RPI; Carvalho et al., 2011; Yamamoto, Shudo, and Sakai, 2016b) is a 19-item (one less than the original scale) self-report measure designed to evaluate the magnitude of reward observation as an approximation of RCPR with three factors: amount of rewards, environmental suppressors, and reward skill. Participants rate each item on a four-point Likert-type scale with anchors 1 (Strongly Disagree) through 4 (Strongly Agree). Scores range from 19 to 76, with higher scores indicating higher levels of reinforcement.
Patient Health Questionnaire—9
The Japanese version of the Patient Health Questionnaire—9 (PHQ-9; Kroenke, Spitzer, and Williams, 2001; Muramatsu et al., 2007) assesses the severity of depression symptoms and includes nine items rated on a four-point Likert-type scale with anchors 0 (Not at all) through 3 (Nearly every day). Scores range from 0 to 27, with higher scores indicating increased depression severity.
Procedure
The Research Ethics Committee of Chukyo University approved all methods and study procedures, which were in accordance with the Declaration of Helsinki and its later amendments. Prior to data collection, participants were given a complete description of the study, including the risks and benefits of participation, after which written informed consent was sought.
Data analysis
The mean scores and SDs of BADS-SF, RPI, and PHQ-9 were calculated. Gender differences in activation and avoidance of BADS-SF, RPI, and PHQ-9 scores were examined with a t test. Zero-order correlations were conducted to examine the relationships between measures.
In this study, we conducted mediation analysis using a bootstrapping method with k = 5000 resamples and 95% bias-corrected and accelerated (BCa) CI used to evaluate indirect effects. The bootstrapping method was performed in line with recommendations by Preacher and Hayes (2008). Activation and avoidance scores on the BADS-SF were the independent variables, RPI score was the mediator variable, and PHQ-9 score was the outcome variable, as shown as Figure 1. All analyses were conducted using SPSS 24 and Mplus 6.12.
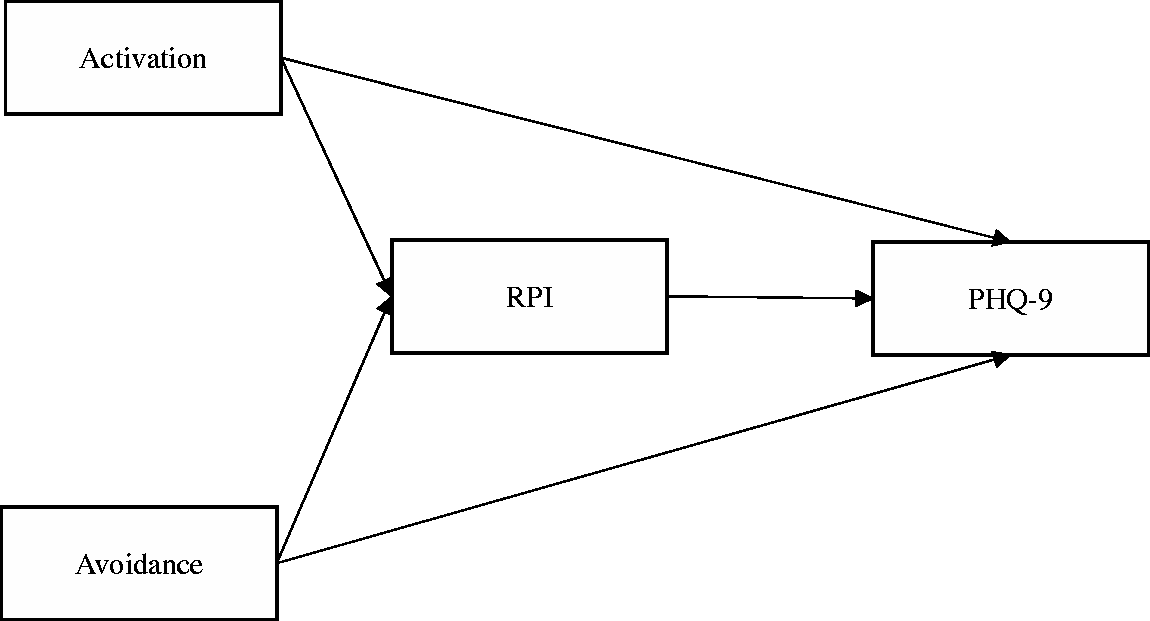
Hypothetical model in this study.
Results
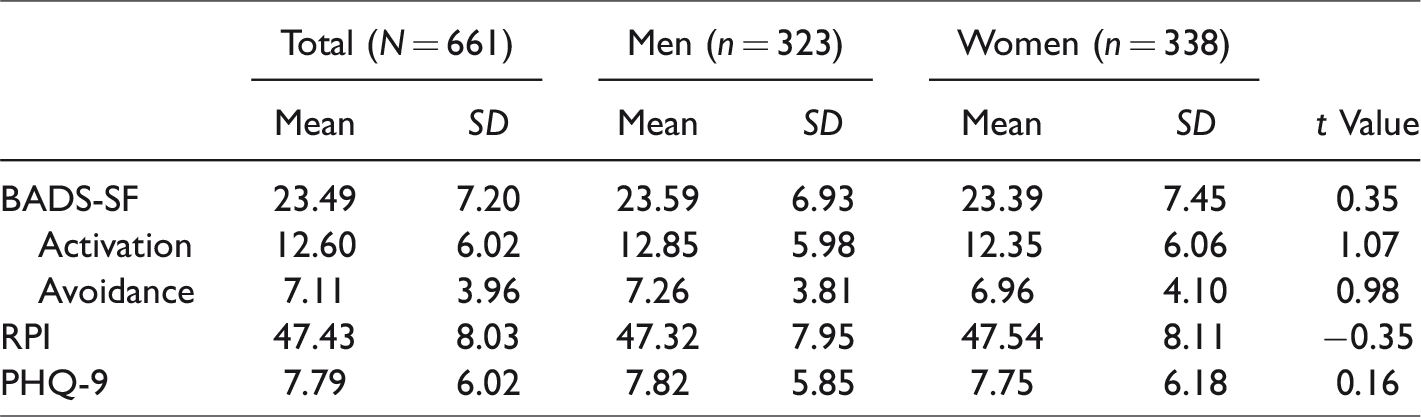
Descriptive statistics are presented in Table 1, and zero-order correlations for each scale are presented in Table 2. There were no significant gender differences; therefore, the subsequent analysis does not consider gender.
Descriptive statistics in this study.
Correlations between measures.
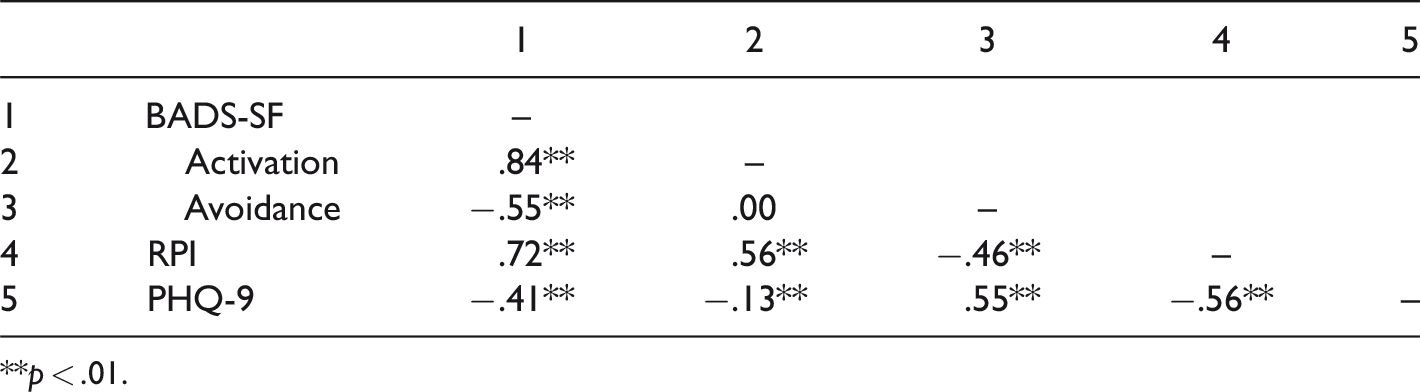
**p < .01.
Mediation analysis using a bootstrapping method with k = 5000 resamples and 95% bias-corrected and accelerated (BCa) CI was conducted to examine behavioral activation model in a community sample in Japan. Figure 2 shows the mediation model, where the weight of β in the relationship between the independent variables, the mediator variable, and the outcome variable, was observed. The indirect effect of activation on PHQ-9 through RPI was significant (indirect effect = −.28, p < .001, 95% CI: −.23 to −.34); the direct effect of activation on PHQ-9 was also significant (direct effect = .15, p < .001, 95% CI: .07 to .23). Moreover, the indirect effect of avoidance on PHQ-9 was significant (indirect effect = .23, p < .001, 95% CI: .19 to .28), as was the direct effect of avoidance on PHQ-9 (direct effect = .48, p < .001, 95% CI: .35 to .61). R2 of RPI and PHQ-9 were .53, and .44, respectively.
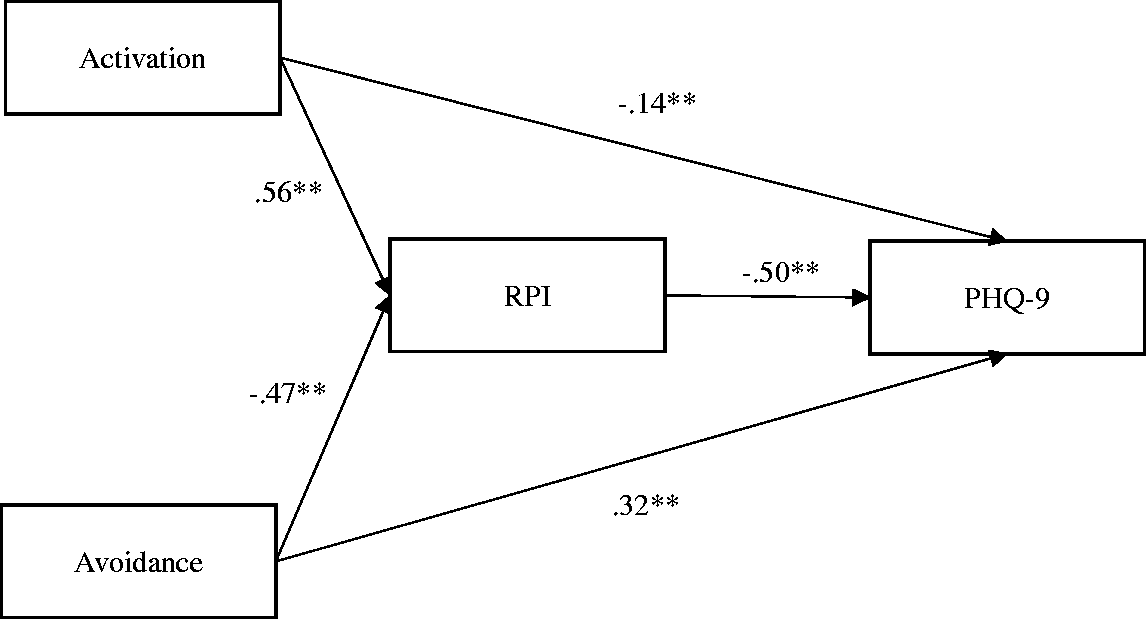
The result of mediation analysis. **p<.01
Discussion
According to the behavioral activation theory, depression arises as RCPR for healthy behaviors decreases (Lewinsohn, 1974). When RCPR decreases, healthy behaviors will be deactivated. Therefore, behavioral activation seeks to increase contact with RCPR by activating healthy behaviors. More recently, the behavioral activation theory proposed by Martell et al. (2001) emphasized the role of avoidance in depression. Depressive individuals may be inactive due to passive avoidance of aversive situations. Thus, these two processes are primary pathways to depression. Therefore, modern behavioral activation includes simple behavioral activation techniques and techniques for identifying and overcoming avoidance (Kanter, Busch, & Rusch, 2009).
The general goal of this study was to evaluate behavioral activation model in a community sample in Japan. Mediation analysis revealed that a partial mediation model was supported. Both activation and avoidance influenced depression through RCPR. These results supported our hypothesis. Our results were consistent with previous research, such as Takagaki et al. (2016) and Carvalho and Hopko (2011).
Our results and those of previous studies showed the importance of RCPR; thus, therapists should activate healthy behaviors that lead to RCPR and decrease avoidance behaviors that reduce RCPR, although they should not simply activate pleasurable activities and remove unpleasant events—it is important for therapists to judge not behavior’s form but its function. Those who conduct research in this area find it difficult to measure RCPR directly. Accordingly, many researchers use indices of reward as proxy measures for RCPR. Carvalho and Hopko (2011), for example, examined the relationship between reward—as measured by daily diary entries—and depression, and found that reward mitigated depression. Yamamoto, Shudo, and Sakai (2014), who used a similar method in their study, found reward to be a critical factor in mitigating depression. These findings suggest that RCPR is an important factor in mitigating depression.
However, Takagaki et al. (2013) and Yamamoto et al. (2016a) suggested that activation and avoidance have no direct effect on depression, using samples of undergraduate students. Thus, our results were somewhat different from those of previous studies. This might have been caused by the differences between community and undergraduate samples. First, undergraduate students live in homogeneous environments (Vredenburg, Flett, & Krames, 1993); for example, almost all undergraduate students in a testing period undergo stressful events uniformly. Second, there is a reduced likelihood that psychiatric disorders other than depression are present in undergraduate students (Vredenburg et al., 1993). Third, it is also less likely that undergraduate students have undergone drug treatment that may influence that data (Vredenburg et al., 1993). In contrast, people in a community sample live in heterogeneous environments and are more likely than undergraduates to have psychiatric or physical disorders and to have undergone drug treatment. Therefore, they have more factors that affect depression. Fourth, Sweeney, Shaeffer, and Golin (1982) suggested that the relationship between avoidance and depression may largely be due to an unmeasured third variable. Therefore, our results might be influenced by other factors that we did not measure.
Finally, we discuss the clinical implications of the study. We tested the behavioral activation model on a community sample, and the results supported the partial mediation model. The finding that behavioral activation and avoidance affect depression via RCPR is consistent with the literature, but we were quite interested to note that avoidance in particular had a moderate direct influence on severity of depression. Clinical practitioners should continue to regard avoidance as a serious risk factor, as they have done until now, but they should also understand that avoidance is not always mediated by RCPR. With such an understanding, practitioners will be able to assess clients more accurately and further refine their interventions.
Limitations and conclusion
We examined a behavioral activation model in which RCPR mediates the relationship between behavioral activation strategies (activation and avoidance) and depression using a community sample in Japan. Mediation analysis supported a partial mediation model. In this sense, this result supported our hypothesis. However, previous studies provide support for a complete mediation model. This difference might be caused by differences in sample characteristics between community and undergraduate samples, as suggested.
Finally, we need to point out some limitations to our research. First, we conducted the study at one point in time. Therefore, we were unable to determine causal relationships between factors. Second, this study is an analog study. To examine the different results between community and undergraduate samples, further examination with a clinical sample will be needed. Third, we need to examine other factors which mediate the relationship between avoidance and depression, because the direct path coefficient from avoidance to depression was relatively strong. Fourth, the study was an online study. Accordingly, readers should be aware that the participants may not be representative of the general population.