
Abstract
Posttraumatic stress disorder (PTSD) remains a highly stigmatized disorder despite its prevalence. Given that the origin of stigmatization is rooted in cognitive representations that people hold, stigma may be differentially exhibited by people with varying degrees of cognitive flexibility. Intellectual humility, the recognition of one’s own intellectual shortcomings or flaws, may allow for flexibility in how people navigate knowledge surrounding PTSD, which may reduce stigma and improve interpersonal interactions with individuals with PTSD. The present study investigated whether intellectual humility would negatively predict PTSD stigma and social distance, above and beyond demographic factors and personal or social experience with individuals with PTSD. Participants (N = 421, 67.2% men, mean age = 37.45, SDage = 9.99) completed a multidimensional measure for intellectual humility and the Mental Illness Stigma Scale adapted to assess PTSD stigma. Results confirmed our preregistered predictions. Bivariate correlations demonstrated that overall intellectual humility was negatively correlated with overall PTSD stigma, and overall intellectual humility was negatively correlated with overall social distance. That is, intellectually humble people reported less PTSD stigma and desired closer social distance with individuals with PTSD. Additionally, hierarchical multiple regression revealed that intellectual humility predicted unique variance in PTSD stigma and social distance above and beyond the contribution of demographic factors and personal experience or social relationships with someone with PTSD. These results may provide a useful framework for approaching and minimizing stigma toward PTSD.
Keywords
Introduction
Posttraumatic stress disorder (PTSD) is a commonly stigmatized disorder, and the stigma toward individuals with PTSD (i.e., PTSD stigma) acts as a major barrier toward seeking treatment. Researchers have consistently attributed the origin of stigmatization to cognitive representations that people (perceivers) hold regarding stigmatized targets (Bos et al., 2013; Dijker & Koomen, 2003; Weiner et al., 1988). Additionally, studies show that stigma is linked to knowledge; that is, the more accurate knowledge someone has about PTSD the less stigma they tend to hold against people with PTSD (Hanisch et al., 2016). Beyond volume of knowledge, the willingness to challenge and update one’s knowledge may be key factors to understanding how PTSD knowledge is related to PTSD stigma. For example, researchers have demonstrated that when people improved their mental health literacy, their stigma scores decreased, regardless of income or socioeconomic status (SES; Girma et al., 2013). This development of new knowledge may facilitate stigma reduction in the context of PTSD and may be captured via a construct known as intellectual humility. Intellectual humility, the ability for people to hold their own beliefs firmly yet remain willing to acquire new knowledge or information, (Krumrei-Mancuso et al., 2020; Krumrei-Mancuso & Rouse, 2016) may be able to counter stigma and associated outcomes. People high on intellectual humility may be more willing to expand their knowledge about PTSD, thereby lowering the stigma they hold against people with PTSD. Additionally, this willingness to update one’s knowledge may lead to appreciable behavioral changes relating to interpersonal interactions with individuals with PTSD. Thus, this study examines the relationship between intellectual humility and PTSD stigma and social distance, seeking to offer an empirical account of how intellectual humility may help reduce stigma.
PTSD Stigma
Stigma surrounding mental illness, including PTSD, is one of the major barriers that prevents people with mental illnesses from seeking treatment (Hanisch et al., 2016). In the context of mental illness, stigma is often a result of misunderstanding or misinformation among the general public about people with mental illness and leads to discrimination and stereotyping by society (Day et al., 2007; Rüsch et al., 2005). Furthermore, stigma among the public is not limited to society in general, but also includes professionals in the mental health field (Corrigan, 2000). The Mental Illness Stigma Framework (MISF; Fox et al., 2018) was developed to conceptualize the existing stigma literature and helped guide the current study. Stigma comes in many forms (e.g., public, self, associative, and structural; Pryor & Reeder, 2011). Current research identifies two domains of stigma at the individual level: perspective of people who hold stigmatizing beliefs (i.e., public stigma) and perspective of the person experiencing stigma, or the stigmatized (i.e., internalized or self-stigma; Fox et al., 2018). Utilizing the MISF, the current study focused on perspectives of people who are stigmatizing toward people with PTSD. Public stigma, which is at the core of stigma (Pryor & Reeder, 2011), represents people’s social and psychological reactions toward stigmatized targets (Bos et al., 2013). The consequences of stigma include stereotypes, prejudice, and discrimination against people with mental illness, including PTSD (Corrigan, 2000; Rüsch et al., 2005). Stereotypes, or negative beliefs about a group, which includes labeling people with PTSD as “violent,” “angry,” “dangerous,” or “crazy”, leave people with PTSD aware of the perceptions of people who are stigmatizing toward them. Therefore, people’s own awareness of these labels may lead them to self-stigmatize and/or to be reluctant or hesitant to seek proper treatment (Correll et al., 2021; Mittal et al., 2013; Rüsch et al., 2005). Such stereotypes can lead to prejudice if the person agrees with the belief, and may cause negative emotional reactions, such as feeling afraid of a person with PTSD and keeping a distance from them for fear of that person having a violent outburst. Discrimination is the behavioral response to prejudice and is often a direct negative consequence of public stigma. Discrimination may prevent people with a mental health diagnosis such as PTSD from finding employment, housing, or seeking treatment (Correll et al., 2021; Rüsch et al., 2005).
To make matters worse, some people who are stigmatizing view PTSD as controllable and ascribe some responsibility onto the targets for their disorder (Caldwell & Lauderdale, 2018; Correll et al., 2021). A form of victim-blaming, many people maintain that individuals who have PTSD resulting from combat experience or work-related events (e.g., in law enforcement) are responsible for their trauma because they knowingly signed up for that career (Caldwell & Lauderdale, 2018). This perceived responsibility for the disorder combined with labels and a lack of knowledge about PTSD create a negative public perception of people with PTSD. As the dual-process model of reactions to perceived stigma suggests (Pryor et al., 1999, 2004), people may have both implicit and explicit negative reactions to stigmatized targets. One such reaction may be reflected through interpersonal contact.
Social Distance
An outcome of negative public perceptions of mental illness, including PTSD, is the desire for social distance, or the act of people creating physical distance between themselves and someone with PTSD as a means for comfort or security (Yap et al., 2014). The Social Distance Scale (SDS) addresses people’s willingness to be in proximity to someone with a mental illness, including how willing they would be to live next door to or be coworkers with someone with a mental illness (Link et al., 1999; Yap et al., 2014). People who desire greater social distance from someone with a mental illness are often older in age and have less familiarity, contact, or direct personal experience with someone with a mental illness (Jorm & Oh, 2009). Familiarity, or having knowledge of or experience with a person with mental illness, can occur in varying degrees, ranging from knowledge gained through media depictions of mental illness to actual, first-hand experience such as having a family member or friend who has a mental illness (Corrigan et al., 2001). The connection between acquiring knowledge and ultimately having more familiarity with mental illness has demonstrated an inverse relationship with prejudicial attitudes, such that people who received education about mental illness expressed improvement in attitudes toward people with mental illness (Holmes et al., 1999).
However, there are some mixed findings when predicting social distance among people with personal experience with mental disorders. In one study, people who experienced greater psychological or emotional distress or had higher amounts of self-reported contact with depression demonstrated higher perceived stigma toward people with depression (Griffiths et al., 2008). Although, other studies suggest knowledge of and familiarity with mental illness lowers stigmatizing attitudes and beliefs and negatively predicts social distance; this was also true for people who have direct or personal contact with people with mental illness (Boyd et al., 2010). For example, in a review, researchers identified that people who have contact with individuals with a mental illness or who have personal experience with mental illness are less likely to desire social distance from people with mental illness (Jorm & Oh, 2009). This finding was also true of people with higher levels of mental health literacy; when people have a background, experience, or an understanding of mental health and mental disorders, they are more likely to desire less social distance and have fewer stigmatizing attitudes toward individuals with mental disorders (Jorm & Oh, 2009). When medical students were assessed based on contact with people with mental illness and knowledge of mental illness overall, results indicated that greater knowledge predicted fewer stigmatizing attitudes toward people with mental illness above and beyond the experience of having prior contact (Mas & Hatim, 2002). Similar results were found for the association between knowledge of schizophrenia and desire for social distance; in a study assessing community attitudes toward people with schizophrenia, participants with the greatest knowledge of schizophrenia endorsed the least desire for social distance (Stuart & Arboleda-Flórez, 2001). In a study addressing PTSD specifically, participants who scored higher on measures assessing actual knowledge of PTSD reported an increased willingness to socialize with people with PTSD and less desire for social distance (Krzemieniecki & Gabriel, 2019).
These results strongly indicate that knowledge, and specifically the willingness to update one’s knowledge base, of mental illness negatively predict stigma and social distance. However, it is unclear if these results are generalizable to specific mental illnesses. Existing literature indicates that, overall, contact with someone diagnosed with PTSD (such as knowing someone with PTSD) leads to less stigmatizing attitudes and beliefs compared to people who did not know someone with a PTSD diagnosis. In another study, familiarity specifically in the context of personal experience of PTSD (e.g., having a PTSD diagnosis or experiencing symptoms of PTSD) was associated with increased public stigma via greater perceived danger, anger, and fear toward veterans with a PTSD diagnosis (Caldwell & Lauderdale, 2018). These results could be highlighting an interaction between self-stigma and public stigma, conflated by a person’s own experiences and familiarity of PTSD and their projection of such biases onto others with the same diagnosis.
Demographic and Personal Predictors of PTSD Stigma and Social Distance
Several factors, including gender, education level, SES, race/ethnicity, political orientation, religiosity, and mental health familiarity may predict PTSD stigma and social distance. In a study in which participants appraised veterans with PTSD in various vignettes, men were more likely than women were to assign responsibility and control to individuals with combat-related PTSD (Caldwell & Lauderdale, 2018; Corrigan et al., 2003; Gibbons et al., 2015). Existing literature also suggests that men tend to have a lower level of mental health literacy compared to women, which has been associated with increased public stigma (Cotton et al., 2006; Gibbons et al., 2015; Kaneko & Motohashi, 2007; Swami, 2012). However, gender does not appear to play a role when it comes to social distance (Jorm & Oh, 2009). Researchers have also indicated that education has a significant effect on stigmatization toward mental illness (Girma et al., 2013); people with more education tend to have fewer stigmatizing attitudes toward individuals with mental illness (Kim et al., 2019). The negative correlation between education and social distance appears to be small, and some studies report the opposite (Jorm & Oh, 2009). Political orientation is also a predictor of stigma toward mental illness; people with more conservative ideologies and affiliation are more likely to endorse stigmatizing attitudes and behaviors, including desiring greater social distance, from people with mental illness (DeLuca & Yanos, 2015; Gonzales et al., 2017; Löve et al., 2019). Religiosity was also found to predict stigma toward people with mental illness; participants who practiced greater religious fundamentalism or had higher scores of religiosity endorsed more stigma toward people with mental illnesses (Abuhammad & Al-Natour, 2021; Adams et al., 2018; Al-Natour et al., 2021).
Other potential influences and predictors of stigma include age, race and ethnicity, and SES, although some findings are mixed. Older people tend to desire greater social distance from individuals with mental disorders (Jorm & Oh, 2009; Lauber et al., 2004). In another study, participants were split into age groups, with those in the oldest age group being almost three times more likely to endorse higher social distance when compared to the youngest age group (Stuart & Arboleda-Flórez, 2001). Many studies have found that people in minority groups, including Black-, Hispanic-, and Asian-Americans, are less likely to seek treatment for mental illness and have higher levels of self-stigma (APA, 2017; Wong et al., 2017). Findings regarding SES influencing stigma toward people with mental illness were mixed, although multiple studies supported the positive association between higher SES and more stigmatizing and/or prejudicial attitudes toward people with mental disorders (e.g., Billings, 2020; Foster et al., 2017; Girma et al., 2013). Moreover, people’s knowledge of or contact with someone with a mental illness, including individuals with PTSD, can influence their stigma and social distance (Grant et al., 2016; Jorm, 2012; Jorm & Oh, 2009; Svensson & Hansson, 2016). People with greater knowledge of mental health or specific diagnoses such as PTSD, and people who have had contact or interacted with someone with a mental illness tend to report lower levels of stigma (Correll et al., 2021).
As the evidence indicates, relationships between demographic variables and stigma and social distance exist (Cotton et al., 2006; Gibbons et al., 2015; Kaneko & Motohashi, 2007; Swami, 2012). However, demographic factors’ contributions to stigma and social distance differ widely in terms of how much variance in stigma and social distance they can predict. Therefore, to properly examine the unique contribution of intellectual humility to predicting PTSD stigma and social distance, we wanted to account for demographic factors’ potential influence on the associations based on their established connections to stigma and social distance. In other words, we examined whether intellectual humility can incrementally predict PTSD stigma and social distance above and beyond demographic factors.
Intellectual Humility
Despite notable obstacles to overcoming stigma and social distance associated with PTSD, researchers have recommended that stigma reduction strategies be rooted in theory and targeted to specific elements of the social interaction (Bos et al., 2013; Corrigan & Kosyluk, 2013). As such, it may be fruitful to examine psychological factors that predict decreased stigma as basic research to establish empirical evidence for future interventions. Although stigma is multifaceted (e.g., cognitive, affective, behavioral components; Goffman, 1963; Mak & Cheung, 2008), many researchers posit that cognitive representations are at the heart of stigma formation and preservation (Bos et al., 2013). As such, psychological factors that signal high cognitive flexibility and openness to knowledge formation — essential components of intellectual humility — are particularly important to examine because they could serve as factors to which interventions can be individualized. Intellectual humility, characterized by its epistemological roots (Porter et al., 2021) may seamlessly serve this need. Below, we define intellectual humility and suggest how it might predict PTSD stigma and social distance.
Intellectual humility has been conceptualized in a number of ways; some researchers have focused on intellectual humility’s virtuous properties, while others have described it as a trait in which individuals find the balance between being completely unopen to new ideas and too easily changing their own views to match that of others (Davis et al., 2016; Krumrei & Rouse, 2016). Still, other researchers describe intellectual humility as an openness to acquiring knowledge, hearing other’s viewpoints, and the willingness to update and revise one’s own opinions or views upon gaining more knowledge (Krumrei-Manusco et al., 2020). The present study conceptualizes intellectual humility as a “non-threatening awareness of one’s intellectual fallibility” with four facets (Krumrei-Mancuso & Rouse, 2016, p. 210) that can be represented by four facets.
Independence of Intellect and Ego, the first facet, allows people to remain unthreatened in the face of an intellectual disagreement. For example, a person may feel strongly that someone with PTSD is dangerous. However, when that person possesses a high degree of Independence of Intellect and Ego, they would not feel threatened when this belief is challenged by information that counters or negates it. The second facet is Openness to Revising One’s Viewpoint, which enables people to change their opinion when faced with significant alternative evidence. In the context of stigma, this facet could manifest as people’s willingness to learn new information and updating their preexisting knowledge about people with PTSD. Respect for Other’s Viewpoints, the third facet, allows for civil discourse to occur, despite holding apparent incompatible views. This facet could manifest in a manner where a person would listen and discuss the merits of the various supposed dangers of PTSD, without anger or frustration directed toward their conversation counterpart. Lastly, the fourth facet of intellectual humility, Lack of Intellectual Overconfidence, allows people to avoid intellectual arrogance or hubris. A person who possesses a high degree of this facet may be willing to admit that they do not know all there is to know about PTSD and its implications.
Summary and Hypotheses
PTSD stigma and related interpersonal outcomes (e.g., social distance) is rooted in cognitive representations and knowledge and may specifically be related to one’s willingness to acquire new knowledge or information. As such, intellectual humility may predict PTSD stigma and social distance. In this study, we examined the association between intellectual humility, PTSD stigma, and social distance. We made the following preregistered predictions (https://aspredicted.org/222xm.pdf). First, we hypothesized that intellectual humility would negatively predict PTSD stigma and social distance, such that participants high in intellectual humility would hold less stigma toward individuals with PTSD, and desire closer social distance with people diagnosed with PTSD. Furthermore, we hypothesized that intellectual humility would predict PTSD stigma and social distance above and beyond demographic factors and personal experience and social relationships with people with PTSD.
Method
Sample Size
We used G*Power 3.1.9.2 (Faul et al., 2009) to estimate the necessary sample size for the study. We conservatively estimated a small effect of r = .15. Given the following parameters, alpha at .05 and power at .80, 343 participants are required. However, our budget allowed us to collect data from approximately 500 participants. We thought that a larger sample size would allow us some flexibility around our estimate and enable us to preemptively address anticipated data loss due to data collection using MTurk (Aguinis, 2020).
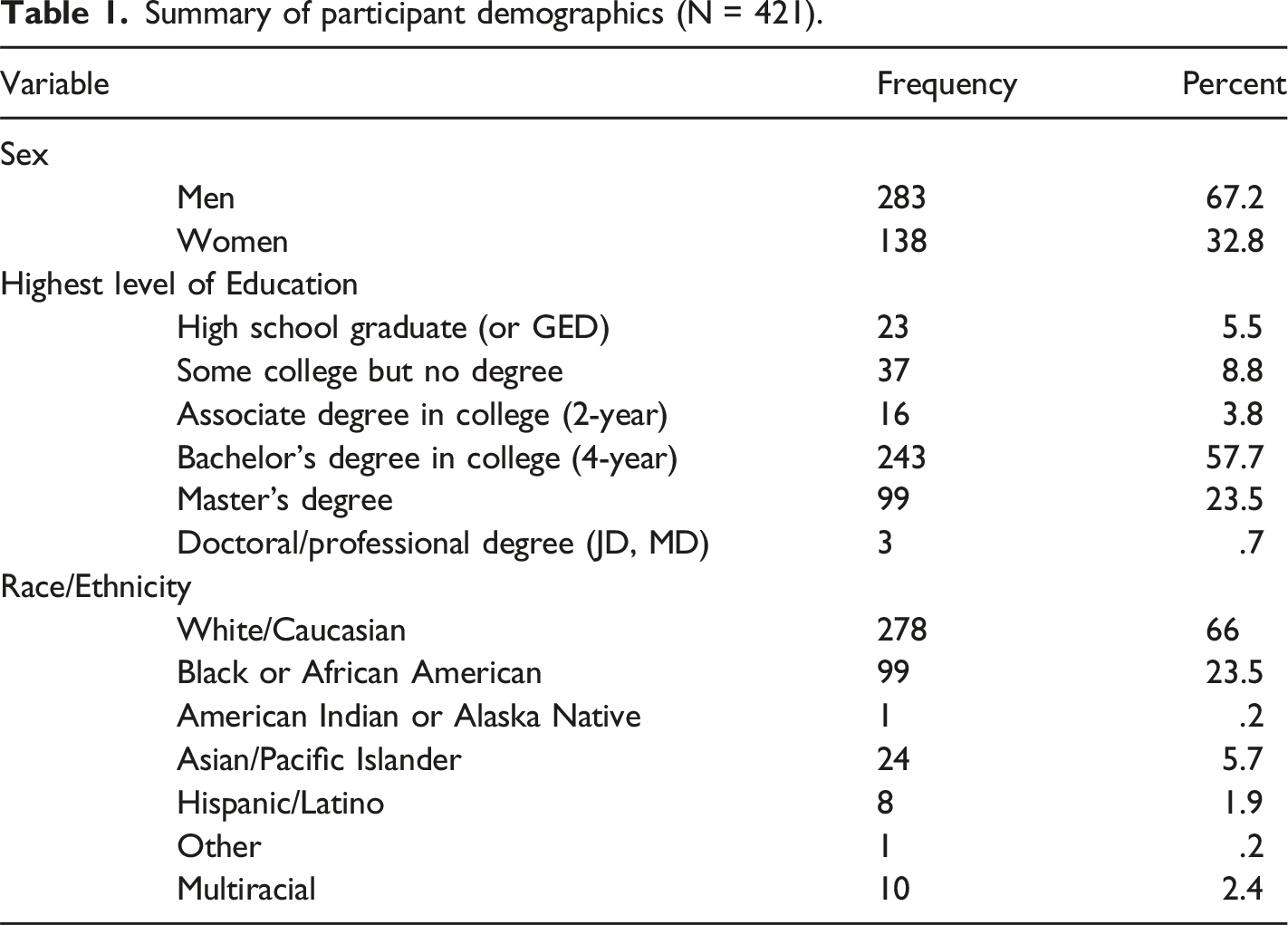
Participants
Summary of participant demographics (N = 421).
Measures
Summary of cronbach’s alphas, means, standard deviations, and correlations for main study measures.
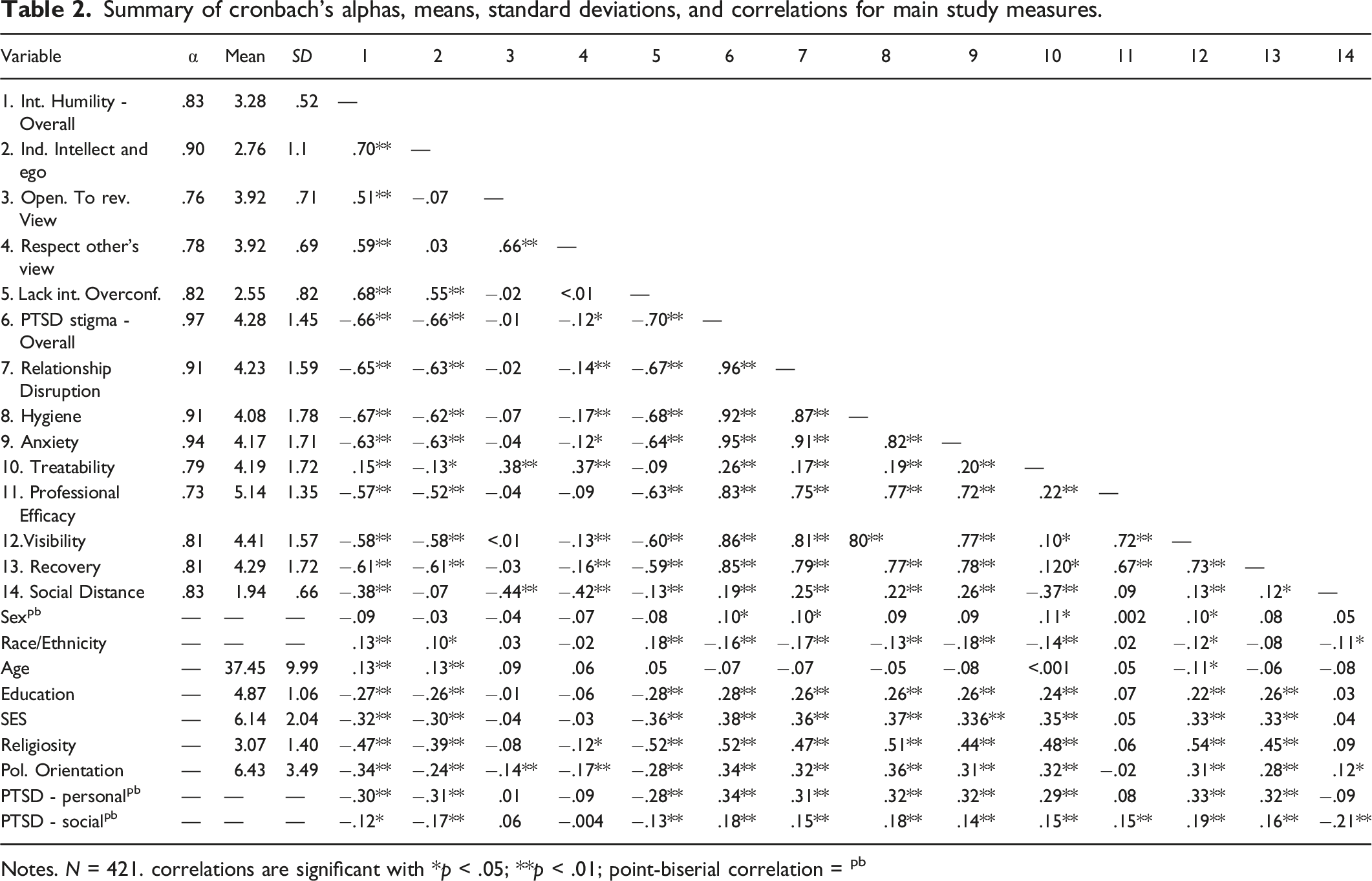
Notes. N = 421. correlations are significant with *p < .05; **p < .01; point-biserial correlation = pb
Intellectual Humility
We used the Comprehensive Intellectual Humility Scale (Krumrei-Mancuso & Rouse, 2016) to measure intellectual humility. The scale consists of four subscales: 1) Independence of Intellect and Ego (5 items), e.g., “When someone contradicts my most important beliefs, it feels like a personal attack.” (R); 2) Openness to Revising One’s Viewpoint (5 items), e.g., “I am willing to change my position on an important issue in the face of good reasons.”; 3) Respect for Other’s Viewpoints (6 items), e.g., “I can have great respect for someone, even when we don’t see eye-to-eye on important topics.”; 4) Lack of Intellectual Overconfidence (6 items), e.g., “For the most part, others have more to learn from me than I have to learn from them.” (R). Participants indicated their (dis)agreement with 22 statements using a Likert scale, with (1) = strongly disagree to (5) = strongly agree as anchors. Higher scores represent higher intellectual humility.
Stigma toward Posttraumatic Stress Disorder (PTSD Stigma)
Stigma toward Posttraumatic Stress Disorder was measured using an adapted version of the Mental Illness Stigma Scale (Day et al., 2007). The scale has seven subscales to measure specific aspects of stigma. We adapted the scale by replacing “mental illness” in the scale items with “PTSD.” Below we list the names of the subscales followed by a sample item for that subscale: 1) Treatability, 2 items: “There are no effective treatments for PTSD.“; 2) Relationship Disruption, 6 items: “I don’t think that it is possible to have a normal relationship with someone with PTSD.“; 3) Hygiene, 4 items: “People with PTSD tend to neglect their appearance.“; 4) Anxiety, 7 items: “I feel anxious and uncomfortable when I’m around someone with PTSD.” 5) Visibility, 3 items: “It is easy for me to recognize the symptoms of PTSD.” (R); 6) Recovery: “Once someone develops PTSD, he or she will never be able to fully recover from it.” 7) Professional Efficacy, 2 items: “Psychiatrists and psychologists have the knowledge and skills needed to effectively treat PTSD.” (R). Participants responded to the items using a 7-point scale, with 1 representing completely disagree and 7 representing completely agree.
Experience with PTSD
We assessed personal experience with PTSD with a single question: “Have you ever been diagnosed with posttraumatic stress disorder (PTSD)?” Participants selected from one of three options: Yes (26.1%); No (71.3%); Prefer not to say (2.6%). We used the item “Has anyone you know ever been diagnosed with PTSD?” to assess social experience with PTSD. Participants selected from one of three response options: Yes (41.6%); No (73.9%); Prefer not to say (4.5%).
Demographic Variables
Participants provided information about their sex, race/ethnicity, age, highest level of education, SES, religiosity, and political orientation. Participants’ sex was determined by their response to the question “What is your sex?“, which had four options (Male, Female, Prefer not to say, Other [space to specify]). Participants’ race/ethnicity was determined by asking participants to select “one or more race/ethnicity that you consider yourself to be” with the following options: White/Caucasian, Black or African American, American Indian or Alaska Native, Asian/Pacific Islander, Native Hawaiian or Pacific Islander, Hispanic/Latino, Other, and Mixed. Socioeconomic status was measured with the MacArthur Scale of Subjective Social Status (Adler et al., 2000). Participants used a ladder to indicate their status to others, 1 indicates worst off relative to others, 10 indicates best off relative to others. Subjective SES has been shown to be a better predictor of psychological functioning than traditional measures of SES (Adler et al., 2000; Rabin & de Charro, 2001).
Political orientation was assessed with a one-item measure (Kroh, 2007): “How would you describe your overall political ideology?” Participants selected from 1–11, where 1 represents completely liberal, 11 represents completely conservative. Religiosity was measured using a single item: “How religious do you consider yourself to be?” (adapted from Abdel-Khalek, 2007). Participants selected from 1–5, 1 represents not at all religious, 3 represents moderately religious, and 5 represents extremely religious.
Procedure
The study was conducted fully online through Qualtrics, a survey management system. Participants clicked on a web link to arrive at the study, where they were met with an information page about the study. Following consent procedures, participants completed the study measures and provided demographic information. The study measures were presented in random order to reduce potential order effects; demographics were provided last. After completion the study sections, participants read a debriefing statement and a statement thanking for their participation. All materials and procedures for this study was approved by our Institutional Review Board (IRB).
Data Analysis Plan
We began by conducting bivariate correlations to provide an overview of the relations between study variables. Then, we conducted a series of hierarchical multiple regression analyses to assess intellectual humility’s ability to predict PTSD stigma and social distance. This analytic approach allowed us to examine the unique contribution of intellectual humility in predicting PTSD stigma and social distance, above and beyond the effects of demographic and personal relationship with PTSD. In hierarchical multiple regression, we entered the predictor variables in two steps: 1) demographic variables (i.e., sex, race/ethnicity, age, education, socioeconomic status, religiosity, political orientation); 2) personal and social experience with PTSD; 3) the four facets of intellectual humility (Independence of Intellect and Ego; Openness to Revising One’s Viewpoint; Respect for Other’s Viewpoints, and Lack of Intellectual Overconfidence). To include the categorical variables of sex and race/ethnicity in the model, sex was dummy coded from four categories into men as 1 and other responses as 0; race/ethnicity was dummy coded from its 8 categories into White as 1 and other responses as 0. We ran separate models for each outcome (seven subscales of the stigma scale and social distance).
Prior to conducting the regression analyses to test our hypotheses, we examined whether multicollinearity was an issue because the four facets of intellectual humility were correlated. The highest variance inflation factor (VIF) value was 1.75, which is lower than the conservative benchmark of 5 (Tabachnick & Fidell, 2007), suggesting that multicollinearity was not an issue. Additionally, the histogram of standardized residuals, P-P plots, and residual scatter plots supported normality, linearity, and homoscedasticity assumptions. The range for Cook’s Distance scores (0–.10) indicated that there were no outliers.
Results
Bivariate Correlations
We briefly summarized the main trends of the associations here. See Table 2 for the complete correlations between study variables. Generally, intellectual humility and its individual facets were negatively correlated with the various subtypes of stigma and social distance, such that higher intellectual humility predicted less stigma against people with PTSD and closer distance between the self and someone with PTSD. The strongest relationships between subscales were observed between the intellectual humility component of Independence of Intellect and Ego and the PSTD stigma subscales of Relationship Disruption, Hygiene, Anxiety, Treatability, Visibility, Recovery, all rs between −.52 and −.63, ps < .001; and, Lack of Overconfidence and Relationship Disruption, Hygiene, Anxiety, Treatability, Visibility, Recovery, all rs between −.59 and −.69, ps < .001. Additionally, Openness to Revising One’s Viewpoint and Respect for Other’s Viewpoints had the strongest correlations with Social Distance, r = −.44 and −.42, p < .001, respectively.
Hierarchical Multiple Regression
Results of final hierarchical regression models.
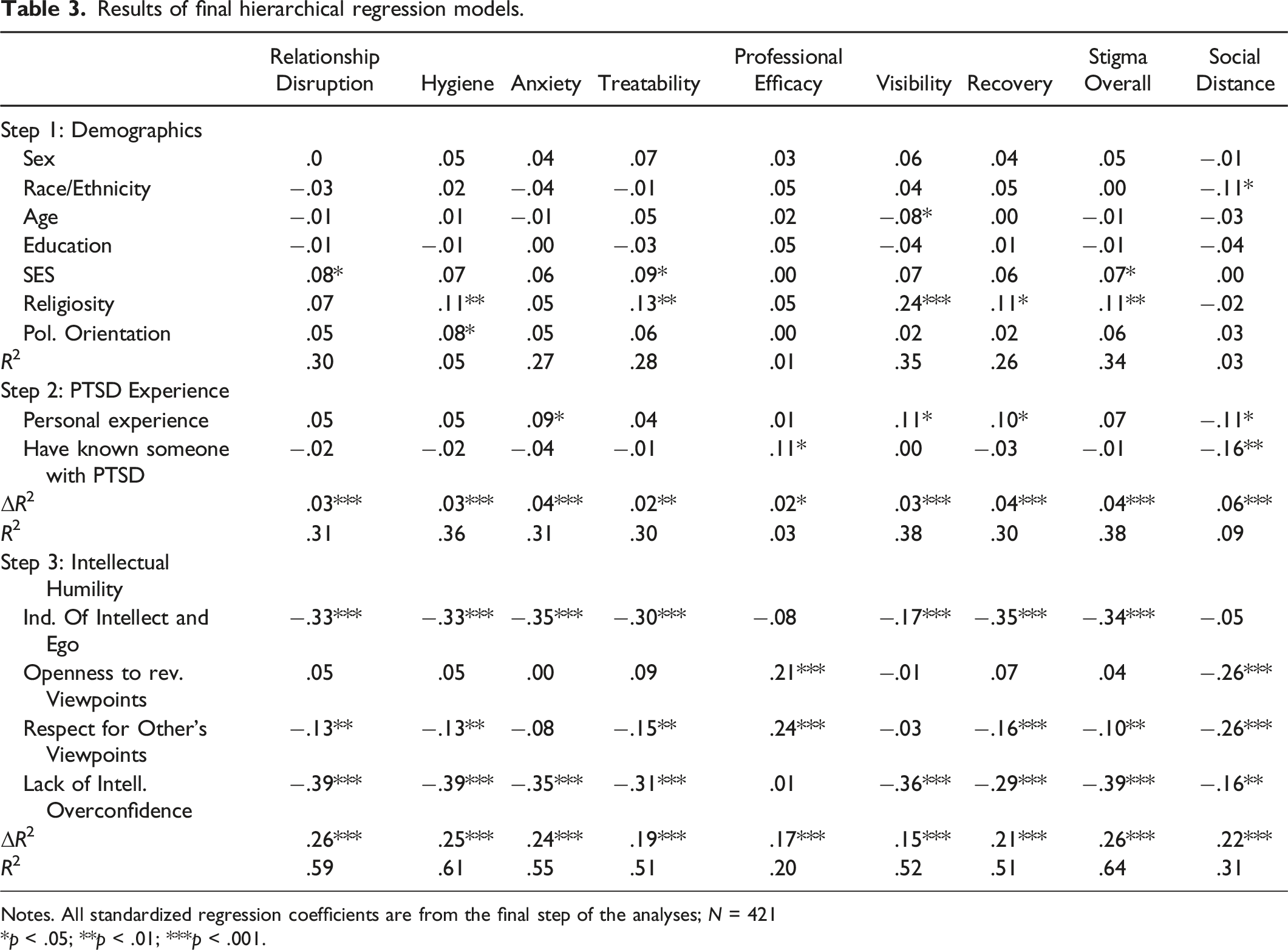
Notes. All standardized regression coefficients are from the final step of the analyses; N = 421
*p < .05; **p < .01; ***p < .001.
In all models, facets of intellectual humility accounted for additional variance for all subscales of PTSD stigma and social distance above and beyond variables entered in Steps 1 and 2 (demographic and personal experience with PTSD). Three of the four intellectual humility facets were largely responsible for this trend. The facets of Independence of Intellect and Ego, Respect for Other’s Viewpoints, and Lack of Intellectual Overconfidence consistently and negatively predicted most types of stigma measured, indicating that more intellectual humility was associated with less stigma.
Discussion
Supporting our preregistered hypotheses, we found that facets of intellectual humility were negatively correlated with PTSD stigma and social distance. Specifically, we found that various facets of intellectual humility negatively predicted all eight subtypes of stigma measured (i.e., relationship disruption, hygiene, anxiety, treatability, professional efficacy, visibility, and recovery). These findings suggest that people who have high levels of intellectual humility will have lower stigmatizing attitudes and beliefs toward people who have PTSD. This pattern was also true for social distance; people who had greater intellectual humility desired less social distance from people with PTSD (i.e., indicating that highly intellectually humble people were more comfortable being close to someone with PTSD than people with low intellectual humility). Also, it is important to note that intellectual humility predicted incremental variance in PTSD stigma and social distance above and beyond personal and demographic variables and personal and social experience with PTSD.
Of note, three facets of intellectual humility were mostly responsible for the trends in predicting PTSD stigma and social distance. People who may be willing to have their beliefs challenged without feeling threatened or personally attacked (i.e., Independence of Intellect and Ego), can remain respectful through disagreements (Respect for Other’s Viewpoints), and do not hold their knowledge as unimpeachable (Lack of Overconfidence) may be particularly less likely to stigmatize against people with PTSD and desire closer distance to people with PTSD. The value of these facets, which allow people to productively explore and attain knowledge, align with research that indicate that when people had more knowledge of mental illness, they scored lower on stigma scales (Corrigan et al., 2001; Holmes et al., 1999; Krumrei-Mancuso et al., 2020). Additionally, these facets may allow people to possess greater empathy and/or willingness to revise their knowledge, which is associated with lower desire for social distance from people with mental illness (Krumrei-Mancuso & Rouse, 2016; Krzemieniecki & Gabriel, 2019).
Our findings were consistent with existing literature regarding the potential impact that intellectual humility has on stigmatizing attitudes and social distance. Previous research identified that, beyond any demographic predictors of stigma, mental health literacy and one’s willingness to update their knowledge or beliefs predicted lower levels of stigma and desire for social distance (Grant et al., 2016; Hanisch et al., 2016; Svensson & Hansson, 2016). Therefore, these findings are theoretically congruent with the current findings about intellectual humility’s relationship with PTSD stigma and social distance, especially when people scored high on Openness to Revising One’s Viewpoints, Respect for Other’s Viewpoints, and Lack of Intellectual Overconfidence. These facets are strong predictors of one’s willingness to seek, receive and update their knowledge, and understand their current knowledge or opinions are fallible.
Moreover, the results indicated that intellectual humility was a predictor of PTSD stigma and social distance even beyond the effects of personal experience or social relationships with someone with PTSD. The current literature identifies personal experience with or contact with people who have mental disorders, including PTSD, as a predictor of someone desiring closer social distance (Boyd et al., 2010; Jorm & Oh, 2009; Mas & Hatim, 2002). Some existing research found people who have personal experience with mental illness (e.g., they have a mental illness themselves) reported lower empathy for others who have mental illness (Cusi et al., 2011). In another study, researchers found that people who experienced PTSD had more stigmatizing beliefs and attitudes toward veterans with combat PTSD (Caldwell & Lauderdale, 2018). However, the findings are mixed, as other researchers argue that having personal experience or contact with someone with mental illness would increase their mental health literacy and thereby lessen the amount of stigmatizing attitudes they possess. In the current study, intellectual humility predicted PTSD stigma and social distance above and beyond participants having any personal or social experiences with PTSD, suggesting that mental health knowledge and one’s willingness to update one’s knowledge is a unique and powerful predictor of PTSD stigma in itself. That is, intellectual humility may be leveraged and incorporated into a strategy to reduce stigma and decrease social distance for people who have and have not had direct relationships/experiences with people with PTSD.
In addition to our main findings about intellectual humility, a few demographic variables consistently predicted PTSD stigma prior to the inclusion of intellectual humility in the model. For example, men indicated more stigma than women. There was less stigma as age increased, and more stigma as SES, religiosity, and conservativism increased. Additionally, relatively consistently, personal experience with PTSD positively predicted PTSD stigma, such that someone indicating that they have had a personal PTSD diagnosis reported more PTSD stigma. However, once intellectual humility was included in the model, these demographic and personal effects generally went away. The exception to this is religiosity, which continued to predict hygiene, treatability, visibility, and recovery even after intellectual humility was added to the model. Overall, these results demonstrate that intellectual humility can robustly predict PTSD stigma and social distance.
Limitations and Future Directions
The current project has some limitations that should be considered alongside its implications. One such limitation is that our sample does not reflect the demographics of the general population. We had an uneven distribution of men and women in the sample (67% men) and the sample was not evenly distributed across race and ethnicity, with 66% of the sample identifying as White. This unrepresentative distribution could limit the extension of these findings to the general population because minority participants may have unique experiences with intellectual humility or PTSD and mental illness that is not captured by the current data. Moreover, 80% of our sample is college educated, and higher education levels have been shown to be predictors of stigma and social distance. Future studies can stratify recruitment to obtain a representative sample, and researchers may also wish to oversample communities of color to address disparities within these populations.
Relatedly, in our analyses, we controlled for the potential contribution of demographic factors in predicting PTSD stigma and social distance as a strategy to isolate and highlight the unique contribution of intellectual humility. In other words, we examined intellectual humility’s incremental ability to predict PTSD stigma and social distance above and beyond the potential influence of demographic factors. In doing so, we did not examine intellectual humility as a potential mediator or moderator of the relationship between demographic factors and PTSD stigma and social distance. For example, men’s lower level of mental health literacy may be associated with increased public stigma (Cotton et al., 2006; Gibbons et al., 2015; Kaneko & Motohashi, 2007; Swami, 2012), therefore, intellectual humility may be a factor in men who have higher mental health literacy and therefore are less stigmatizing. Additionally, Leary et al. (2017) found that intellectual humility was associated with lower dogmatism, which is often associated with extreme political and religious beliefs. Thus, this relationship might explain a negative association between public stigma and intellectual humility. The interplay between intellectual humility, demographic factors, and PTSD stigma and social distance were beyond the scope of the current study, as it only presented demographic factors as control variables. However, the circuitry between these factors serves as exciting future directions for research.
Additionally, our study used a simple strategy to detect and exclude potential “bot” responses collected through MTurk. Although this is an effective way to identify potential “bot” responses (Chmielewski & Kucker, 2020; Dennis et al., 2018), we did not use other strategies to screen out other potential contributors to poor data quality, such as careless responding (Aruguete et al., 2019). We considered using attention checks, but research shows that they could violate participants’ trust and may lead them to intentionally provide low quality responses (e.g., Fowler et al., 2022). We acknowledge that our data may potentially include low quality responses and we encourage future researchers to replicate and extend our findings using MTurk and/or participants recruited through other strategies. Furthermore, we asked participants about PTSD without asking about their prior knowledge about PTSD (whether they know what PTSD is, and the extent of such knowledge). This omission represents a notable limitation of the data collected regarding personal experience with PTSD.
Another limitation of this research is the use of the Mental Illness Stigma Scale (Day et al., 2007) to directly assess PTSD stigma. This approach deviated from the traditional approach of using vignettes to examine mental health stigma (e.g., Jorm et al., 1997). We acknowledge that the vignettes approach has important advantages such as its ability to enable researchers to draw causal conclusions (Aguinis & Bradley, 2014). However, a noted drawback is its issue with realism (Hughes & Huby, 2004). Because of our intrinsic interest in PTSD stigma specifically, we modified the Mental Illness Stigma Scale to directly measure participants’ stigma directed at people with PTSD in various forms. We did not use a vignette because we were not interested in comparing PTSD stigma with other types of stigma and we wanted participants’ responses to reflect their real experiences without potentially conflating that experience with a vignette driven experience (Hughes & Huby, 2004). Additionally, we acknowledge that questions about a specifically labeled illness can engender different responses compared to another labeled illness or non-labeled illness (e.g., Abdullah & Brown, 2020). These limitations represent opportunities for future research, such as whether intellectual humility can predict stigma for some mental health illnesses but not for others, or whether it predicts stigma toward specific mental health illnesses but not for mental health generally.
The current study also included a behavioral indicator (i.e., social distance), but lacked a true behavioral measure. Interpretations regarding intellectual humility’s impact on behaviors should be done parsimoniously. Similarly, we tested our hypotheses using bivariate correlations and hierarchical multiple regression using cross-sectional and survey-based data. Causality cannot be determined based on this approach. Additional evidence, specifically experimental evidence in which intellectual humility is manipulated would allow for a true test of its effect on stigma and social distance.
In an effort to reduce stigma surrounding people who experience PTSD, and potentially for people with mental illness in general, identifying strategies to increase people’s intellectual humility may be useful. Specifically, identifying ways to improve knowledge regarding PTSD and other mental illness to ensure accurate information is being shared is essential, as research suggests that more knowledge predicts less stigma. Some researchers suggest that encouraging investigative behaviors, such as investigating misinformation, fact checking, and actively seeking alternative opinions or information, is one way to increase knowledge and discernment accuracy (Koetke et al., 2022). A core facet of intellectual humility is the willingness to update one’s own knowledge; by promoting the participation in investigative behaviors and spreading accurate information, intellectual humility may be increased by increasing people’s use of the core facets in their everyday lives and eventually leading to a reduction of public stigma.
Conclusion
Stigma remains an important deterrent for people with PTSD from pursuing necessary care. Stigma largely stems from (incorrect/incomplete) cognitive representations and knowledge about PTSD. In our study, we demonstrated that intellectual humility, which is represented by cognitive flexibility and a willingness to seek and update knowledge, even when it counters established beliefs, negatively predicted PTSD stigma and social distance above and beyond demographic and personal factors. These findings suggest that intellectually humility can be targeted and leveraged to help reduce stigma — to modify representations of PTSD by the public and by those afflicted by the disorder.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this research was supported by a Texas A&M-San Antonio Research Council Grant.
Ethics Approval
The questionnaire and methodology for this study was approved by the Institutional Review Board at Texas A&M University-San Antonio (Protocol #2020-04).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Data Availability Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author.