
Abstract
People with chronic illnesses are vulnerable to stress and psychopathology during population-level disasters, as a subset of individuals with disabilities. We aimed to examine the relationships between chronic illness, cumulative and specific stressors, and probable depression, probable anxiety, and post-traumatic stress in an under-resourced urban population in New York City during the COVID-19 pandemic. Using cross-sectional survey data collected in April 2020, we utilized bivariate chi-square analyses and multivariable logistic regression models to estimate differences in and adjusted odds of stressor endorsement and diagnostic prevalence between people with and without chronic illness. We also assessed effect modification of the relationship between stressor exposure and psychopathology by chronic illness status. Compared to people without chronic illness, those who reported having a chronic illness experienced increased odds of probable depression, probable anxiety, and post-traumatic stress. They were also more likely to report high cumulative COVID-19-related stress exposure, death of someone close to them due to coronavirus or COVID-19, family problems, feeling alone, supply shortages, and financial problems. Chronic illness was found to be an effect modifier in the relationship between the death of someone close due to coronavirus or COVID-19 and probable depression and between household job loss and probable anxiety.
Introduction
SARS-CoV-2, the virus that causes COVID-19, induces a heterogeneous response among people, ranging from asymptomatic infections to fatal pneumonia and sepsis (Guan et al., 2020). People with a chronic illness are at an increased risk of COVID-19 infection, complication, and death and are at a greater likelihood of experiencing pandemic-related stressors (Centers for Disease Control and Prevention, 2021; Davis, 2016; Goering, 2015; Shakespeare et al., 2021; Turk & McDermott, 2020; Yeo & Sawyer, 2005). In the context of an ongoing global pandemic, and the growing acceptance that COVID-19 will remain a consistent threat, as well as the reality that individuals with chronic illness are at particular risk of severe infection, the relationship between chronic illness and mental health warrants greater attention (Abraham et al., 2020).
There are multiple explanations for why individuals with chronic illness are more vulnerable to COVID-19 than individuals without pre-existing conditions, according to preliminary research. First, it is broadly documented that individuals with a chronic illness experience greater barriers to regular and affordable healthcare, report greater unmet medical need, suffer from systemic socioeconomic marginalization, and have been disproportionately affected by the transition from in-person clinical services to telemedicine (Annaswamy et al., 2020; Boyle et al., 2020; Shakespeare et al., 2021; Turk & McDermott, 2020). Together, these factors enhance their risk of poor COVID-19 outcomes and may increase their experiences of daily stress in the context of the pandemic (Bhatia et al., 2021). Second, individuals with chronic are more likely to live in congregate care settings, such as nursing homes, where approximately 30% of COVID-19 deaths were recorded as of January 2021 (Landes et al., 2020; The New York Times, 2020). These residential settings not only pose increased COVID-19 risk; they have also resulted in greater social stressors as visitation was suspended, facilities experienced staffing shortages, and at times, individuals were confined to their personal living quarters during the pandemic (Abbasi, 2020; Maxouris, 2021). Third, discriminatory rationing of medical equipment and intensive care unit beds and ableism may have increased acute stress for those with chronic illness (Arcieri, 2021; Kattari, 2020; Sabatello et al., 2020). Fourth, studies have documented increased rates of psychological distress and health risks for individuals with chronic illnesses such as asthma, COPD, cardiovascular illness, and diabetes, during the COVID-19 pandemic (de Boer et al., 2021; Higbee et al., 2021; Musche et al., 2021; Viveiros et al., 2021; Yohannes, 2021). Finally, respiratory disease, cardiovascular disease, diabetes, cancer, and other chronic illnesses are associated with an increased risk of severe COVID-19 outcomes due to disease etiology and treatment-related side effects such as immunosuppression, among others (Caramelo et al., 2020; Centers for Disease Control and Prevention, 2021b; Gleason et al., 2021; Li et al., 2020). This added risk of severe illness and mortality may exacerbate pandemic-related stress. Taken together, individuals with chronic illness have experienced unique challenges during the pandemic, and the mental health consequences of these experiences are not well understood (Lund et al., 2020).
Individuals with chronic illness have also demonstrated high rates of psychological distress (Brady et al., 2017; Lacomba-Trejo et al., 2020; Turvey et al., 2009). One study identified significant risk of suicidality and depression among participants with chronic illness (Gürhan et al., 2019). Researchers have predominantly linked such rates of distress with difficulties in adjusting to a new diagnosis and the stress involved in medical regimens often required of individuals with chronic illnesses (Chapman et al., 2004; Compas et al., 2012; de Ridder et al., 2008; Strine et al., 2008). Additionally, other material and social factors such as difficulty working due to illness, and lack of financial support, play an important role in the mental health outcomes of individuals with chronic illnesses (Cukor et al., 2007; Kullowatz et al., 2007; Moussavi et al., 2007). In light of this context, ongoing investigations into the correlates of mental health as well as the psychological well-being individuals with chronic illness during COVID-19 are needed (McLoone et al., 2022; Mokdad et al., 2005).
The present study examined the relationships between chronic illness, pandemic-related stressors, and mental health symptomatology in a cross-sectional sample of racially and socioeconomically diverse adults enrolled in at least one university-level course living in New York City’s (NYC) largest public university during the COVID-19 pandemic. Survey data was collected in April 2020, when NYC was the epicenter of the pandemic in the United States, and therefore a critical site to examine the associations between exposures related to the COVID-19 pandemic and associations with mental health. Moreover, individuals with chronic illness, enrolled in academic courses specifically faced an additional host of pandemic-related challenges, including inaccessible online learning tools and financial stress (Twardzik et al., 2021; Zhang et al., 2020). We sought to understand if participants with chronic illnesses were at increased likelihood of probable depression, probable anxiety, and probable post-traumatic stress (PTS). We also sought to evaluate how the pandemic’s impact on mental health differed amongst those with chronic illnesses or without, and therefore examined self-reported chronic illness as a potential effect modifier in the relationship between COVID-19-specific stressors and probable anxiety, probable depression, and probable PTS.
Methods
Study Population
Our sample was composed of under-resourced adults, ages 18 years or older, enrolled, at the time of data collection, in at least one course across six City University of New York campuses. Data were collected during one time period from April 8, 2020, to May 2, 2020 (n = 2551), using electronic self-administered surveys.
Survey Distribution and Data Collection
The Intersect Lab at The City College of New York distributed an original survey to six City University of New York campuses from April 8, 2020, until May 2, 2020, to collect demographic information, assess COVID-19-related experiences and stressors, and administer self-report psychological health measures. Participants were informed of the study via an email from their respective campus, which provided the web address of the survey. Participants provided consent by voluntarily participating in the study; participants were not compensated for their participation. Rationale for non-participation was not requested. The study was approved by the Institutional Review Board at City University of New York.
Survey Measures
Demographics
Participant ethno-racial group membership was operationalized using five mutually exclusive categories: non-Latinx white, non-Latinx Black, Latinx, non-Latinx Asian, and non-Latinx Indigenous (including “American Indian or Alaskan Native” and “Native Hawaiian or other Pacific Islander”). Gender was operationalized using three mutually exclusive categories: “male,” “female,” and “other” (including transgender and non-binary). Socioeconomic status (SES) was scored and categorized as high versus low, with the high SES category indicating college education or above, household incomes greater than or equal to $65,000, household savings greater than or equal to $10,000, individual incomes of greater than or equal to $35,000, individual savings of greater than or equal to $5,000, and private health insurance. The computations of the SES index are outlined in the data analysis section below.
Chronic Illness Variable
Participants were asked a multi-select question: “Do you have a chronic illness?” Possible responses included, “Yes, respiratory-related illness (i.e., asthma),” “Yes, cardiovascular (i.e., heart disease),” “Yes, other (i.e., diabetes),” and “No.” These three response options highlight major types of chronic conditions which have been preliminarily explored in relation to COVID-19-induced psychological distress, and constitute major types of illnesses recognized as disabled subpopulations (Centers for Disease Control and Prevention, 2021a; de Boer et al., 2021; Higbee et al., 2021; Musche et al., 2021; Viveiros et al., 2021; Yohannes, 2021). The “Yes, other” response option include all other chronic conditions that are not specified in the previous two response options.
COVID-19 Stressors
COVID-19-related stress was operationalized using the following 13 binary exposures: seeing family in person less, seeing friends in person less, death of someone close due to coronavirus or COVID-19, family or relationship problems, challenges finding childcare, feeling alone, not being able to get food due to shortages, not being able to get supplies due to shortages, losing a job, a member of the household losing a job, having financial problems, having difficulty paying rent, and being forced to leave campus. The total number of stressors endorsed was utilized to quantitatively assess cumulative stress exposure, with a score less than or equal to 4 indicating low stress exposure and a score greater than or equal to 5 indicating high stress exposure, in accordance with a previous dichotomization of this scale to assess the psychological impact of the pandemic (Rudenstine et al., 2021, 2021b, 2022a, 2022c). These stressors have been previously assessed in published research on post-traumatic responses and capture mortality rates and financial hardships, both of which are disproportionately experienced by vulnerable populations in the setting of disasters.
Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9), a clinically validated psychometric tool, was employed to indicate probable diagnosis of depression (Kroenke & Spitzer, 2002). The measure utilizes a cut-off score of 10 and is composed of nine items, each containing a four-point scale that ranges from 0 to 3 (0-not at all, 1-several days, 2-more than half the days, 3-nearly every day) (Kroenke & Spitzer, 2002). The PHQ-9 has demonstrated a high level of sensitivity at 88.0%, test-retest reliability with a correlation of .84, and internal reliability with a Cronbach’s alpha of .89 (Kroenke et al., 2001; Kroenke & Spitzer, 2002). The Cronbach’s alpha for this sample population was found to be .89.
Generalized Anxiety Disorder-7
The Generalized Anxiety Disorder-7 (GAD-7) was used to indicate probable diagnosis of anxiety (Spitzer et al., 2006). Like the PHQ-9, the GAD-7 utilizes a cut-off score of 10 and is composed of seven items, each containing a four-point scale that ranges from 0 to 3 (0-not at all, 1-several days, 2-more than half the days, 3-nearly every day) (Spitzer et al., 2006). The GAD-7 has been clinically validated and has demonstrated a sensitivity rate of 89.0%, strong test-retest correlation of .83, and internal reliability with Cronbach’s alpha of 0.92 (Löwe et al., 2008; “The GAD-7 Scale Was Accurate for Diagnosing Generalised Anxiety Disorder,” 2006). For this sample, the Cronbach’s alpha was 0.92.
Primary Care Post-Traumatic Stress Disorder Screen
The Primary Care PTSD Screen (PC-PTSD) was used to assess probable post-traumatic stress. The clinically validated screen is comprised of 4 binary items and has a documented cut-off score of 2 (Cameron & Gusman, 2003). Each item assesses a different symptom type in accordance with DSM-IV criteria: intrusion (i.e., “that you had nightmares about it or thought about it when you did not want to”), avoidance (i.e., “that you tried hard not to think about it, or went out of your way to avoid situations that reminded you of it”), changes in arousal (i.e., “that you were constantly on guard, watchful, or easily startled”), and negative changes in mood and cognition (i.e., “that you felt numb or detached from others, activities, or your surroundings?”) (Cameron & Gusman, 2003). The PC-PTSD has a sensitivity rate of 91% and a strong test-retest reliability with a correlation of .83 (Prins et al., 2004). The measure was validated against diagnostic interviews for PTSD, with higher scores indicating greater likelihood of diagnosis.
Data Analysis
First, descriptive analyses were performed to assess the demographic characteristics of this sample population and subpopulations of individuals with chronic illness and without. A unique socioeconomic index was created using the following variables: education, health insurance status, household income, household savings, individual income, and individual savings. Study participants were divided into socioeconomic categories based on a median score of 4. Individuals of low SES were defined as having a score of less than or equal to 3, while individuals of high SES were defined as having a score greater than or equal to 4. This computation has been previously used to assess relationships between SES and psychological outcomes during the pandemic (Rudenstine et al., 2022b; Schulder et al., 2022). Second, the prevalence of probable depression, probable anxiety, and probable PTS, as defined by the clinical cut-off scores for each measure, as well as individual stressor endorsement, was estimated among participants with chronic illness. Third, bivariate chi-square analyses were performed to evaluate differences in demographic characteristics, diagnostic prevalence, and individual stressor endorsement between the two subpopulations. Fourth, after controlling for ethno-racial group membership, age, gender, and SES, a multivariable logistic regression model was used to estimate the adjusted odds ratios and confidence intervals for demographic characteristics; clinically significant levels of anxiety, depression, and probable PTS; and endorsement of individual stressors for participants with chronic illness compared to people without. Fifth, given the importance of investigating the relationships between stress, chronic illness, and mental health during the pandemic, chronic illness was evaluated as an effect modifier in the relationships between individual stressors and diagnosis and cumulative stress exposure and diagnosis, using interaction terms to calculate adjusted odds ratios (McLoone et al., 2022). A likelihood ratio test was utilized to compare the goodness of fit of the nested and complex statistical models prior to assessment for effect modification. For variables in which more than half of responses were missing, completed responses were removed from analyses. For variables in which more than half of the responses were completed, missing cells were imputed with the mean of the completed responses.
Results
The majority of the sample identified as a person of color. 24.34% were non-Latinx white (n = 570), 12.30% were non-Latinx Black (n = 288), 20.03% were non-Latinx Asian (n = 469), 39.50% were Latinx of any race (n = 925), and 3.84% were of another ethno-racial group, including multi-racial, native Hawaiian and Pacific Islander, and American Indian/Alaskan Native (n = 90). 71.73% of the population identified as a woman (n = 1685), 26.99% identified as a man (n = 634), and 1.28% identified as another gender, including transgender and non-binary (n = 30). With respect to household income, 19.83% reported a household income less than $20,000 (n = 405), 24.83% reported a household income between $20,000 and less than $45,000 (n = 507), 24.83% reported a household income between $45,000 and less than $75,000 (n = 507), and 30.51% reported a household income of $75,000 and over (n = 623).
Prevalence of Chronic Illness Across Sample Demographic Characteristics.
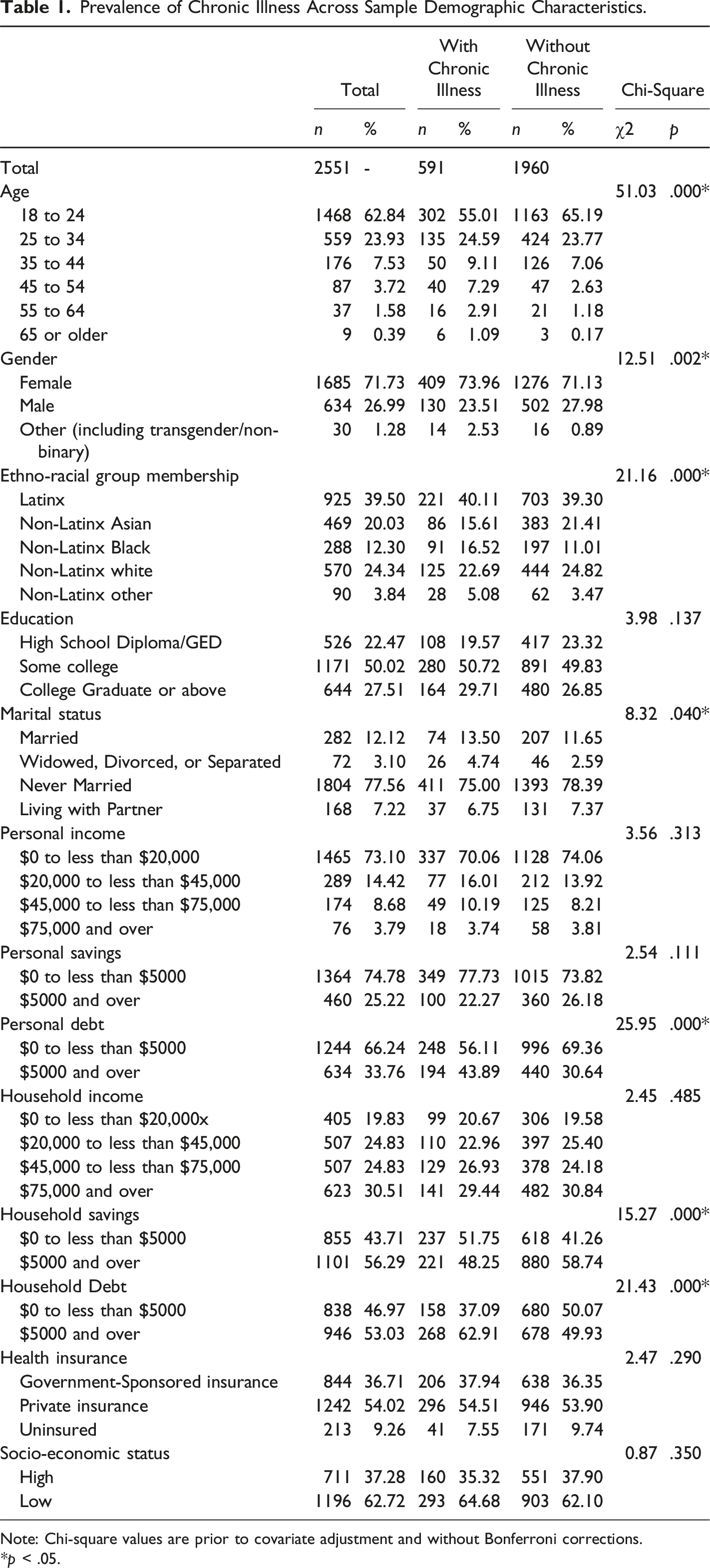
Note: Chi-square values are prior to covariate adjustment and without Bonferroni corrections.
*p < .05.
Prevalence of COVID-19-Related Stressor Exposure, Cumulative Stress Level, and Probable Diagnosis by Chronic Illness Status.
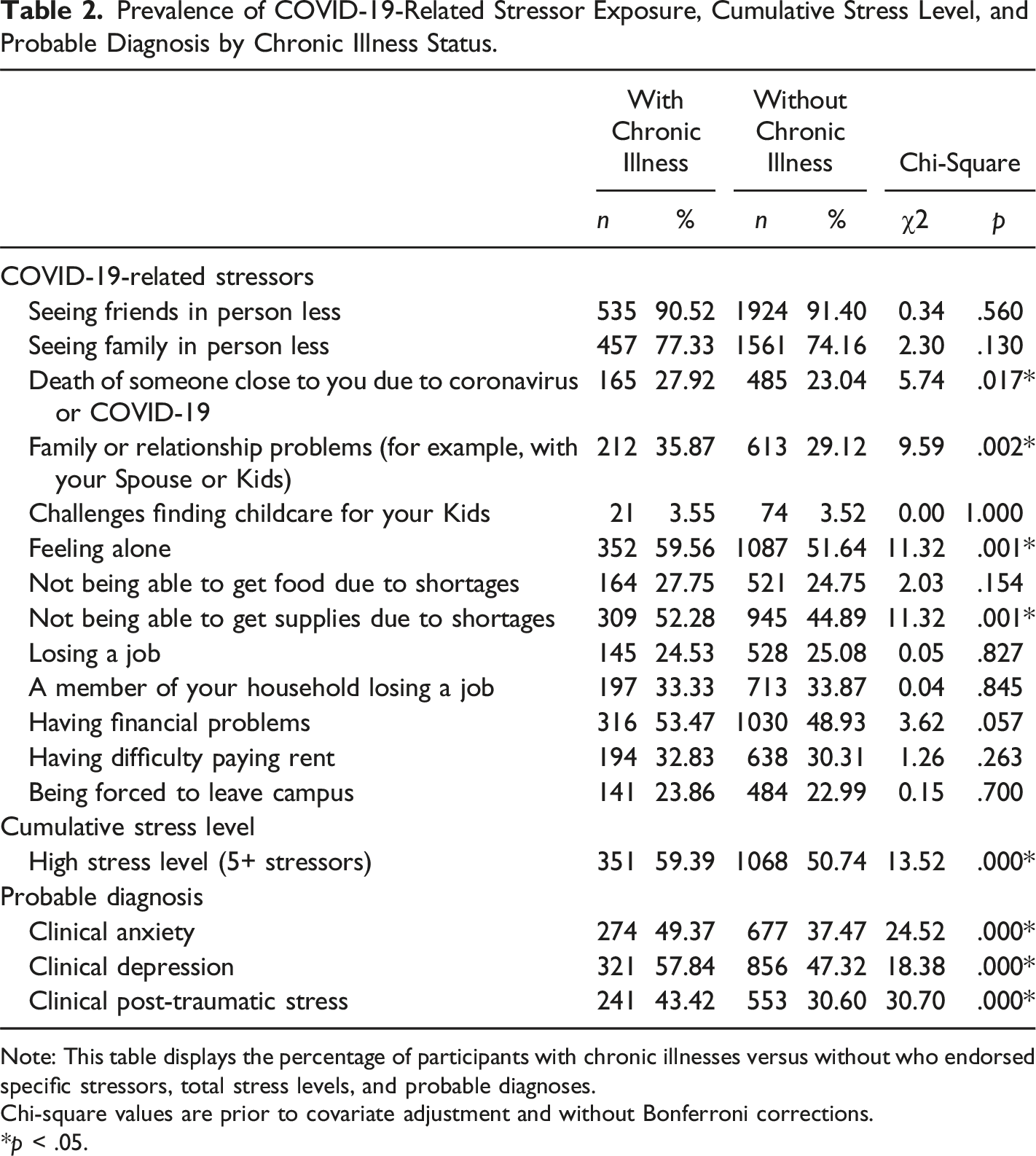
Note: This table displays the percentage of participants with chronic illnesses versus without who endorsed specific stressors, total stress levels, and probable diagnoses.
Chi-square values are prior to covariate adjustment and without Bonferroni corrections.
*p < .05.
Odds Ratios of COVID-19-Related Stressor Exposure, Cumulative Stress Level, and Probable Diagnosis for People with Chronic Illness Compared to People without Chronic Illness.
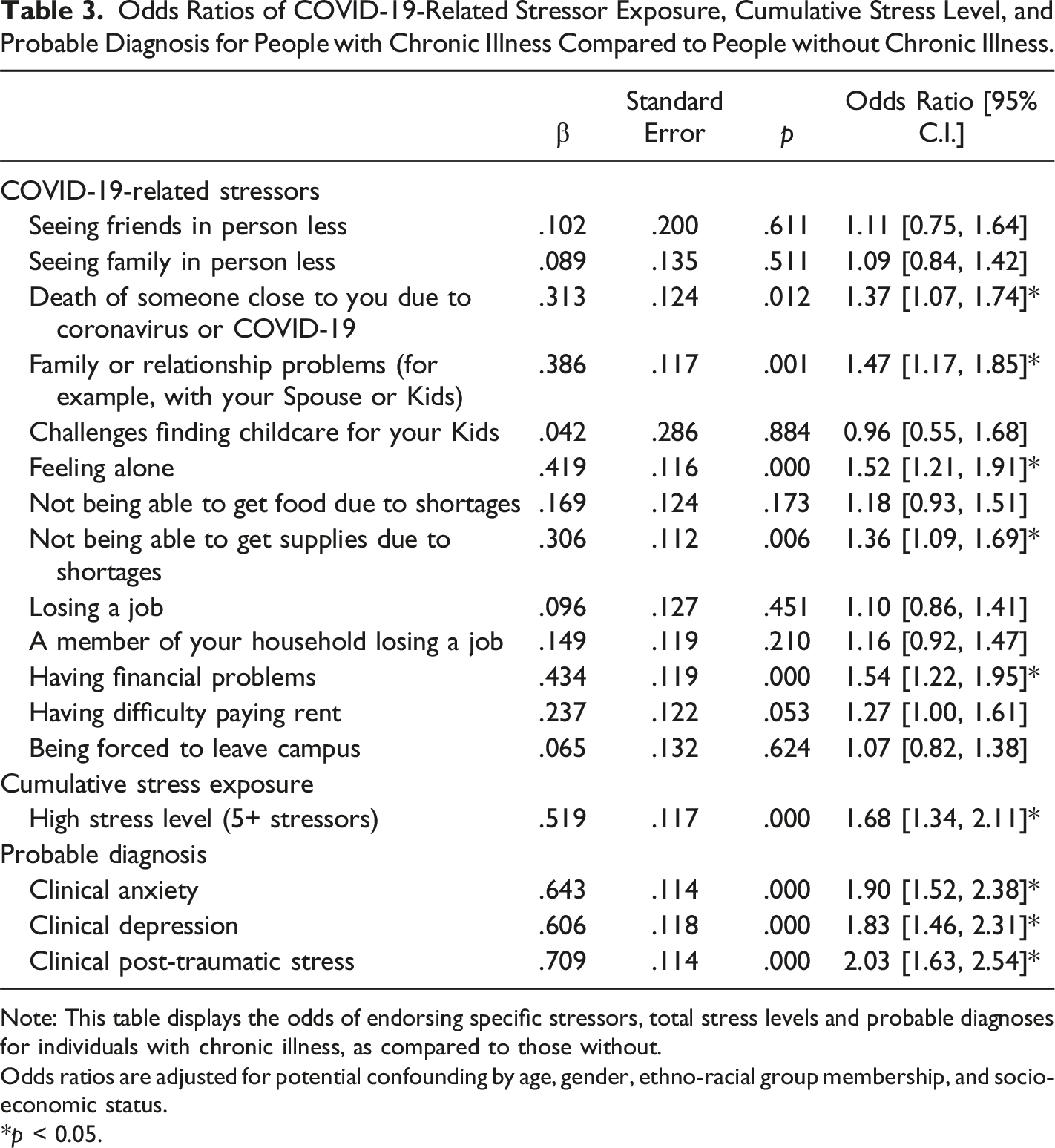
Note: This table displays the odds of endorsing specific stressors, total stress levels and probable diagnoses for individuals with chronic illness, as compared to those without.
Odds ratios are adjusted for potential confounding by age, gender, ethno-racial group membership, and socio-economic status.
*p < 0.05.
Chronic illness was an effect modifier in the relationship between the death of someone close due to coronavirus or COVID-19 and probable depression. Participants with chronic illness who experience the death of someone close to them due to coronavirus or COVID-19 have 2.49 [1.13, 5.46] times the odds of probable depression, while people without chronic illness who experience the death of someone close to them due to coronavirus or COVID-19 have 1.30 [1.01, 1.67] times the odds of probable depression. Chronic illness was also an effect modifier in the relationship between household job loss and probable anxiety. Participants with chronic illness who experience household job loss have 2.10 [1.04, 4.22] times the odds of probable anxiety, while people without chronic illness who experience household job loss have 1.25 [.99, 1.57] times the odds of probable anxiety.
Discussion
Using cross-sectional survey data from an urban under-resourced adult population from April 2020, we assessed the relationships between chronic illness, pandemic-related stressors, and mental health. We aimed to utilize these findings as a lens through which to understand the psychological impact of the pandemic on a particular subset of the disability community, as is consistent with disability studies and disability health literature (Centers for Disease Control and Prevention, 2021; Davis, 2016; Gulley et al., 2018; Krahn et al., 2021; Yeo & Sawyer, 2005). This study has four main findings. First, people with chronic illness in our sample were more likely to endorse high cumulative stress exposure than individuals who did not report having a chronic illness. This finding is consistent with past research that shows that individuals with a chronic illness have an increased risk of stressors in the context of population-level disasters (Fox et al., 2010; Stough, 2009). Further, these individuals, like other marginalized populations, have an increased risk of stress exposure more generally, which is a primary contributor to psychological distress (Dohrenwend, 2000; Kessler, 1997). Chronic illnesses, such asthma, diabetes, and heart disease, have a disabling impact, and such conditions may have been related to their experiences of stressors and mental health more broadly (Davis, 2016; Goering, 2015; Yeo & Sawyer, 2005). Thus, these concepts are interrelated and may accumulate burden for affected populations.
Second, participants with chronic illness were more likely to report five individual stressors than those without. These stressors were death of someone close to them due to coronavirus or COVID-19, family problems, feeling alone, supply shortages, and financial problems. To the best of the authors’ knowledge, to date, there is little research examining the differential prevalence of COVID-19-related stressors between individuals with chronic illness and without chronic illness. The increased prevalence of these five stressors among individuals with chronic illnesses compared to those without chronic illness can be understood in the context of the defining attributes of the COVID-19 pandemic. Pandemic-induced changes, such as supply shortages and increased risk of exposure during in-person work, may have more significantly impacted individuals with chronic illness as compared to the general population. For example, the risk of COVID-19 exposure in the context of typical movement throughout NYC to purchase necessary supplies and in-person work presented a greater risk to those with chronic illness than to those without chronic illness. Similarly, the increased risk of COVID-19 exposure in the context of in-person gatherings may have increased psychosocial stressors, such as family problems and feeling alone, among those with chronic illness, especially in the early weeks of the pandemic. Related, a documented increase in domestic violence and decreased mobility during the initial months of COVID-19 resulted in greater daily exposure to and experiences of stressful home environments (Dalise et al., 2021; Lund, 2020; Turk & McDermott, 2020). In this vein, these data are consistent with growing evidence that persons with disability broadly reported experiencing greater social isolation and greater material stressors during the COVID-19 pandemic compared to non-disabled adults (Assi et al., 2022; Boyle et al., 2020; Dalise et al., 2021; Sabatello et al., 2020).
The third key finding in this study is that participants with chronic illnesses experienced increased odds of probable depression, probable anxiety, and probable PTS compared to individuals who did not endorse a chronic illness. Increased psychological distress among people with chronic illness during population-level disasters is well documented (de Boer et al., 2021; Higbee et al., 2021; Musche et al., 2021; Stough, 2009; Viveiros et al., 2021; Yohannes, 2021). These individuals are more vulnerable to COVID-19-related mortality and morbidity, and this increased risk may intensify the fear of viral exposure and ableism upon seeking care (Andrews et al., 2021; Landes et al., 2020; Shakespeare et al., 2021). The greater physical vulnerability to COVID-19 outcomes may thereby increase secondary risks of psychological distress (Bhatia et al., 2021; Lund et al., 2020).
The fourth finding captured the interrelations between chronic illness, mental health outcomes, and two unique stressors. Individuals with chronic illness who experienced the death of someone close to them due to COVID-19 experienced increased odds of probable depression compared to people without chronic illness who also experienced such a loss. This finding could be understood in the context of the increased vulnerability to COVID-19 faced by individuals with chronic illness, as stated above, and the potential fear of one’s own mortality and morbidity associated with learning of the death of a loved one (Caramelo et al., 2020; Centers for Disease Control and Prevention, 2021b; Gleason et al., 2021; Li et al., 2020). Losing a loved one can lead to further losses in social networks and support systems and contribute to community-level grief, exacerbating probable depression outcomes (Lund et al., 2020; McGuire et al., 2018).
Additionally, individuals with chronic illness who experienced household job loss experienced increased odds of anxiety compared to people without chronic illness who experienced household job loss. This finding may be attributed to greater reliance on household members for financial support due to a lack of resources offered by unemployment and Social Security Insurance/Social Security Disability Insurance (Brucker & Houtenville, 2015). Broadly speaking, this subpopulation, on average, are more economically insecure than individuals who do not have a chronic illness and therefore, may have fewer medical expenses (Lund et al., 2020; Shakespeare et al., 2021; Turk & McDermott, 2020). These stressors have been shown to contribute to increased odds of anxiety (Hatch & Dohrenwend, 2007).
This study’s findings are best understood in the context of the differential effect of the pandemic across various subpopulations (Bowleg, 2020). As represented in this study’s sample, people with chronic illness, people of color, and people of low SES are more likely to have coexisting mental illness (Hatch & Dohrenwend, 2007). Considering the intersectionality of identity is critical in understanding the mental health consequences of COVID-19 (Bowleg, 2020). Clinical implications of these findings include ensuring that clinicians assess for psychological distress among individuals with chronic illnesses, and to conceptualize distress as including emotional experiences of stress, alongside material and societal factors. Given the role of material and social stressors in the present analyses, clinical work should account for such realities when providing mental healthcare.
There are several study limitations worth noting. First, the individuals in this study’s sample were enrolled in at least one course at a public university in New York City during the spring semester of 2020. The experiences of individuals in this sample may not be generalizable to the experiences of all university students or the overall United States population. Second, chronic illness was self-reported by participants; therefore, there is risk of misclassification error, in which individuals with chronic illnesses who are undiagnosed or chose not to disclose their illness are wrongly categorized as not having one. Third, the three mental health outcomes (probable depression, probable anxiety, and PTS) were self-reported, albeit using psychometrically validated screening tools that are widely recognized across fields (Cameron & Gusman, 2003; Kroenke et al., 2001; Kroenke & Spitzer, 2002; Löwe et al., 2008; Prins et al., 2004; Spitzer et al., 2006; “The GAD-7 Scale Was Accurate for Diagnosing Generalised Anxiety Disorder,” 2006). Therefore, outcomes in this study refer to estimated burden of probable depression, anxiety, and PTS. Formal diagnoses can only be made by a clinician in the context of a diagnostic evaluation.
Conclusion
Despite the limitations mentioned above, this study provides unique insight into the experiences of under-resourced urban adults with chronic illness during the COVID-19 pandemic. Nevertheless, this study does not intend to generalize individuals with chronic illness but rather validate a shared experience observed within a vulnerable population. Our findings suggest that people with chronic illness were more likely to endorse high cumulative stress exposure, death of someone close due to coronavirus or COVID-19, family problems, feeling alone, supply shortages, and financial problems compared to people without chronic illness and that sample participants with chronic illness had higher odds of probable depression, probable anxiety, and PTS than those without. We also found that having a chronic illness increased the odds of probable depression upon exposure to the death of someone close due to coronavirus or COVID-19 and increased odds of probable anxiety when experiencing household job loss. Building off this work, future studies will consider the importance of other covariates for mental health in individuals with chronic illness, including but not limited to COVID-19 diagnosis, the concern of infection, neighborhood characteristics, and social support.
Footnotes
Author’s Note
This work was written on the unceded ancestral homelands of the Munsee Lenape, Wappinger, and Schaghticoke peoples, to whom we show gratitude for their traditional stewardship of this land.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.