
Abstract
Mental health problems among college students are increasingly prominent. The negative effects of emotional distress on college students’ mental health have been supported empirically. It is important to understand the psychological processes underlying this relationship. Using a longitudinal design, the present study aimed to reveal the explanatory mechanism of the association between dimensions of dispositional mindfulness and mental health problems among Chinese college students by testing the mediating effects of experiential avoidance and intolerance of uncertainty. A total of 907 Chinese college students (57% male; Mage = 20.33 years) were invited to complete self-report questionnaires at two time points. Mindful awareness, acceptance and mental health problems (depression, anxiety and stress) were assessed at baseline (T0). Experiential avoidance, intolerance of uncertainty and mental health problems were assessed at the 6 month follow-up (T1). Following structural equation modeling (SEM) analyses, the results show that high levels of mindful awareness and acceptance may diminish mental health problems by decreasing the levels of experiential avoidance among college students. However, only mindful acceptance diminished mental health problems through decreased intolerance of uncertainty. In addition, our study found that mindful awareness and acceptance may have different functions when working alone. Specifically, these two constructs may have different relationships with mental health. Identifying these mechanisms by which dispositional mindfulness is associated with college students’ mental health over time has potential value for the prevention of potential mental health issues and timely interventions.
Keywords
Introduction
Mindfulness is a characteristic associated with reliable and valid global measures of mental health (e.g., Brown & Ryan, 2003; Gu et al., 2015). Buddhist psychology posits that mindfulness helps one perceive what is presented to the senses in a way that is closer to its true nature and not affected by the projection of reality, which helps to free oneself from negative emotions and to reach a lasting state of mental health (Ekman et al., 2005). On the one hand, mindfulness-based interventions was found to reduce many forms of mental health issues, including stress (Burton et al., 2016), anxiety (Peterson & Pbert., 1992) and depression (Kumar et al., 2008). On the other hand, a dispositional tendency toward mindfulness—trait mindfulness—was found to be positively correlated with mental health (Mesmer-Magnus et al., 2017). For instance, Giluk (2009) meta-analytically reported a large negative correlation between trait mindfulness and mental health problems. More recently, trait mindfulness has been shown to be associated with increases in psychological well-being (Tomlinson et al., 2018). Therefore, trait mindfulness may be a protective construct against mental health problems.
However, the roles of different dimensions of mindfulness deserve to be studied further. According to monitor-and-acceptance theory (MAT), attention monitoring and acceptance have different and synergistic effects on some outcomes (Lindsay & Creswell, 2017). Attention monitoring refers to an ongoing awareness of the present sensory and experiences (Lindsay & Creswell, 2017). By enhancing one’s focus on present-moment cues, attention monitoring for positive cues allows positive experiences to be more intense and frequent (Lindsay & Creswell, 2017). However, individuals high in mindful awareness also tend to ruminate on negative internal or external experiences and may be more likely to experience symptoms of emotional disorders. A growing body of studies of mindfulness components in nonmeditating samples supported this idea, suggesting that when unaccompanied by acceptance, attention monitoring is associated with higher levels of affective symptoms, such as depression and anxiety (Bravo et al., 2016, 2018; Lam et al., 2017). A longitudinal study also showed that as time goes on, emotional awareness can highly predict the trend for symptoms of depression, fear, worry and rumination (Zuddas, 2012).
Monitor-and-acceptance theory predicts that monitoring alone would increase affective reactivity, whereas, when combined with acceptance, it would promote health outcomes (Lindsay & Creswell, 2017). However, the results of a recent study provided very little support for the two tested MAT tenets, which suggested that there is no significant interaction between monitoring and acceptance, and the beneficial effects of mindfulness on mental health are largely dependent on acceptance (Simione et al., 2021). Acceptance refers to an objective, nonreactive orientation to the present moment, which allows all experiences to enter and pass without further reaction, whether the experience is pleasant or stressful (Lindsay & Creswell, 2017). In other words, elevated acceptance may help people treat thoughts gently. According to Verplanken and Tangelder (2011), acceptance can reduce the impact of negative thoughts by diminishing their adverse effects. Studies on trait mindfulness also have demonstrated that acceptance can strongly predict a decrease in psychological symptoms and an increase in well-being (Klein et al., 2015; Simione et al., 2021).
Many of the studies on trait mindfulness and mental health are cross-sectional (Coffey et al., 2010; Mandal et al., 2012), and the current study explored the relationship between different dimensions of trait mindfulness and mental health problems from a longitudinal perspective. As dispositional differences in mindfulness are associated with mental health, the next step is to identify the underlying mechanisms, which are beneficial for understanding both mindfulness and mental health. However, there has been little exploration of the mechanisms that might explain the relationship between different dimensions of mindfulness and mental distress from a longitudinal perspective.
One factor that may be important to examine in this regard is experiential avoidance. It has long been suggested that avoiding negative affect can influence psychopathology (Hayes et al., 1996), this idea has been repackaged as the construct of experiential avoidance (Chawla & Ostafin, 2007). Experiential avoidance (EA) can be defined as the tendency to avoid distressing thoughts, feelings, memories, and other internal experiences (de la Cruz et al., 2013). EA may have short-term benefits, but a growing body of research has shown that EA will subsequently result in more negative emotions (Briggs & Price, 2009; Gold & Wegner, 1995; Wegner et al., 1987). Moreover, EA has been shown to play a role in the maintenance of emotional disorders such as anxiety (Forsyth et al., 2006) and depression (Starr & Moulds, 2006), as well as leading to more severe symptoms than EA itself will bring (Sloan, 2004).
From the perspective of mindfulness-based interventions, mindfulness may theoretically reduce experiential avoidance. Hayes et al. (1996) cited plenty of evidence to show that many forms of psychopathology involve patterns of experiential avoidance in an attempt to escape private experiences. Mindfulness-based interventions have something in common with modern behavioral therapies such as dialectical behavior therapy (Linehan, 1993), acceptance and commitment therapy (Hayes, 1987; Hayes & Wilson, 1994) by encouraging individuals to give up ineffective experiential avoidance strategies. Additionally, there is empirical support for significant negative correlations between mindfulness and experiential avoidance (Baer et al., 2006). To be specific, mindfulness is a multidimensional construct (Cardaciotto et al., 2008). Thus, different components of mindfulness may have different relationships with experiential avoidance. MAT affirms that attention monitoring will exacerbate affective reactivity (Lindsay & Creswell, 2017). In other words, individuals high in mindful awareness tend to have more emotional responses to troublesome events, associating judgments with negative experiences. Thus, they may be more likely to choose avoidance to solve the problem temporarily. Consistent evidence supports a positive relationship between awareness and experiential avoidance (Pinto-Gouveia et al., 2012). Mindful acceptance is identified as an adaptive alternative to experiential avoidance (Hayes et al., 1999). When an individual refuses to face the unwanted experiences, acceptance encourages the person to diminish this avoidance. That is, acceptance may reduce negative emotions by affecting experiential avoidance. The inverse correlation between acceptance and experiential avoidance has already been identified in both clinical and nonclinical samples (Hayes et al., 2004; Ruiz-Párraga & López-Martínez, 2014). Based on this, we proposed a hypothesis that experiential avoidance might mediate the longitudinal relationship between dimensions of trait mindfulness and mental health.
Intolerance of uncertainty may be another important mechanism for understanding how mindfulness reduces negative emotions. Buhr and Dugas (2012) conceptualized excessive worry as resulting from an “approach-avoidance” dilemma, intolerance of uncertainty and experiential avoidance may fit nicely into this statement. Intolerance of uncertainty may drive people to find specific ways to achieve a higher level of certainty (Ladouceur et al., 1997), and fear of negative experiences may cause people to take avoidance measures to deal with negative emotions (Berman et al., 2010). Oscillating between approach and avoidance behaviors may lead to mental health problems over time (Buhr & Dugas, 2012). Carleton (2016) defined intolerance of uncertainty (IU) as an individual’s dispositional inability to tolerate the negative response resulting from incomplete perceptions of information and maintained by the associated perception of uncertainty. According to Krohne’s (1989) coping theory, people tend to perceive unpredictable situations as threatening, and IU may lead to excessive attempts to obtain threatening information. A model suggested by Mathews and MacLeod (2002) posits that overstating threatening information may generate negative emotions. So theoretically, IU may lead to more negative emotions. The relationships between IU and emotional disorders have been widely studied, and there appears to be mounting evidence that IU may be a transdiagnostic vulnerability factor for many psychological disorders (Dugas et al., 1997; Grenier et al., 2005; Gentes & Ruscio, 2011; McEvoy & Mahoney, 2012).
Intolerance of uncertainty is a construct pointing to the future, whereas mindfulness is a trait that points to the present. Mindfulness allows people to focus more on the present (Kabat-Zinn, 1990), and negative emotions about the unknown future may also be reduced due to lack of attention. A study on mindfulness-based intervention suggested that mindfulness-based cognitive therapy (MBCT) is an effective way to lower IU in patients with panic disorder (Kim et al., 2016). Recently, many studies have shown that mindfulness is negatively correlated with IU (Kraemer et al., 2016; Mantzios et al., 2015; Nekić & Mamić, 2019). However, an interesting phenomenon is that the two subdimensions of mindfulness do not work the same way. Mindful awareness and acceptance may differ in their relationship to IU. Unlike the relationship between mindfulness as a compound concept (or a form of therapy) and IU, individuals with high levels of awareness may also have high levels of IU. They might be more able to catch their thoughts and emotions in daily life and be more aware of the changes in their body and state of mind (Price & Hooven, 2018). That heightened sensitivity may make unpredictable changes in the future perceived as more threatening and lead to the belief that they cannot handle the unknown future (Mathews & MacLeod, 2002), which results in the inability to tolerate uncertainty. However, individuals high in acceptance may have the ability to free themselves from internal thoughts and emotions by considering them without any possible subjective evaluation, good or bad, positive or negative, worthy or unworthy (Kabat-Zinn, 1990). This kind of ability to be non-judgemental makes the uncertainty less likely to be interpreted as negative and threatening. And these individuals are less likely to develop a cognitive bias to evaluate uncertain situations or events negatively (Dugas et al., 2004), which may associated lower degree of IU (Ladouceur et al., 2000).
The Current Study
Although there is theoretical and empirical support for the association between greater mindfulness and decreased psychological distress, there has yet to be an integrative model to reveal the internal mechanism. Thus, the goal of the current study was to examine the indirect effect of different dimensions of trait mindfulness on mental health through experiential avoidance and intolerance of uncertainty from a longitudinal perspective. After controlling for the effects of gender, age and mental health problems at baseline (T0), we hypothesized that mindful awareness at T0 would be positively associated with experiential avoidance, intolerance of uncertainty and mental health problems 6 months after baseline (T1), whereas acceptance at T0 would be inversely associated with them. Furthermore, both experiential avoidance and intolerance of uncertainty were hypothesized to significantly mediate the longitudinal relationship between dimensions of trait mindfulness and mental health.
Method
Participants and Procedure
Participants were recruited from two colleges in Gansu, China. A total of 1119 college students (59% male; Mage = 19.94 years; SD = 1.38 years) were included in the baseline assessment (T0), and 907 of them (81.05% of the original sample) participated in the assessment 6 months later (T1). Thus, data from 907 college students ranging in age from 17 years old to 24 years old (57% male; Mage = 20.33 years; SD = 1.10 years) were analyzed in the current study. There was no significant difference in age, gender, mindfulness, experiential avoidance or intolerance of uncertainty between the dropout subjects and the final sample (ps > 0.05).
This study was approved by the Ethics Committee of the Faculty of Psychology at the author’s University. Informed consent was obtained from the participants. They were told that their participation was voluntary and were ensured that their privacy would be protected. Both assessments were conducted online. Participants completed questionnaires assessing mindful awareness, mindful acceptance and mental health problems (depression, anxiety and stress) at T0 and assessing experiential avoidance, intolerance of uncertainty and mental health problems (depression, anxiety and stress) at T1. The questionnaire can only be successfully submitted when it is fully completed, so there were no missing values.
Measures
Dispositional Mindfulness
Dispositional mindfulness was measured using the Chinese version of the Philadelphia Mindfulness Scale (PHLMS) (Liang et al., 2018). The original PHLMS (Cardaciotto et al., 2008) is a widely used bidimensional measure of trait mindfulness that assesses its two key components: mindful awareness and acceptance. Each subscale comprises 10 items (for example, “When I walk outdoors, I am aware of subtle smells or the feeling of air touching my face” and “I think I have to control or change my bad mood better”), and each item is rated using a Likert-type scale from 1 (almost never) to 5 (almost always). In the present study, the internal consistency of the scale was good (α = 0.863 and α = 0.871 for mindful awareness and acceptance, respectively).
Experiential Avoidance
Experiential avoidance was measured by self-report with the Acceptance and Action Questionnaire-Second Edition (AAQ-II) (Bond et al., 2011). The Chinese version of the AAQ-II has been shown to be reliable and valid. It consists of seven items (for example, “My painful memories prevent me from having a fulfilling life”) (Cao et al., 2013), and each item is rated using a Likert-type scale from 1 (almost never) to 7 (almost always). The scores of the items were summed to obtain an experiential avoidance score, with higher scores indicating higher levels of experiential avoidance. The internal consistency of the scale in the present study was good (α = 0.968).
Intolerance of Uncertainty
The Chinese Version of the Intolerance of Uncertainty Scale-Short Form (IUS-12) was used to measure responses to uncertainty. The 12-item short version of the IUS has been found to be highly correlated (r = .96) with the full version in two studies with both undergraduate (Carleton et al., 2007) and clinical samples (McEvoy & Mahoney, 2011). The Chinese version of the IUS has been shown to have good reliability and validity (Zhang et al., 2017). This scale comprises 20 items (for example, “I would be frustrated if I didn’t have all the information I needed”), and each item is rated using a Likert 5-level scoring method. Higher scores indicate higher levels of intolerance of uncertainty. In the present study, Cronbach’s alpha was 0.953.
Mental Health Problems
Mental health problems were assessed by the Depression, Anxiety and Stress Scale (DASS) (Lovibond & Lovibond, 1995). The Chinese version of the DASS is considered reliable and valid (Gong et al., 2010), it contains 21 items in three subscales: depression (for example, “My painful memories prevent me from having a fulfilling life”), anxiety (for example, “I worry about occasions where I might panic or make a fool of myself”), and stress (for example, “I feel like I consumed a lot of energy”). Each item rated on a 4-point scale from 1 (never) to 4 (always). The scores for the depression, anxiety, and stress items were summed to obtain depression, anxiety, and stress scores, with higher scores indicating higher levels of depression, anxiety, and stress. In the present study, the Cronbach’s alphas for depression, anxiety and stress subscales were 0.902, 0.886 and 0.897 at T0, 0.923, 0.913 and 0.923 at T1.
Data Analyses
Descriptive statistics and correlation analyses were performed using SPSS 22.0. In addition, AMOS 24.0 was utilized to construct the model and conduct mediating effect analyses.
After controlling for the effects of gender, age and mental health problems at T0, we used mindful awareness and mindful acceptance at T0 as independent variables, experiential avoidance and intolerance of uncertainty at T1 as mediating variables, and mental health problems at T1 as dependent variables, respectively, to construct the hypothetical mediating model. We used structural equation modeling and bootstrapping to test these relation by specifying a sample of 2,000 to examine the significance of the role of the mediators.
Results
Descriptive Statistics and Correlation Coefficients
Descriptive Statistics and Correlations Between Variables.
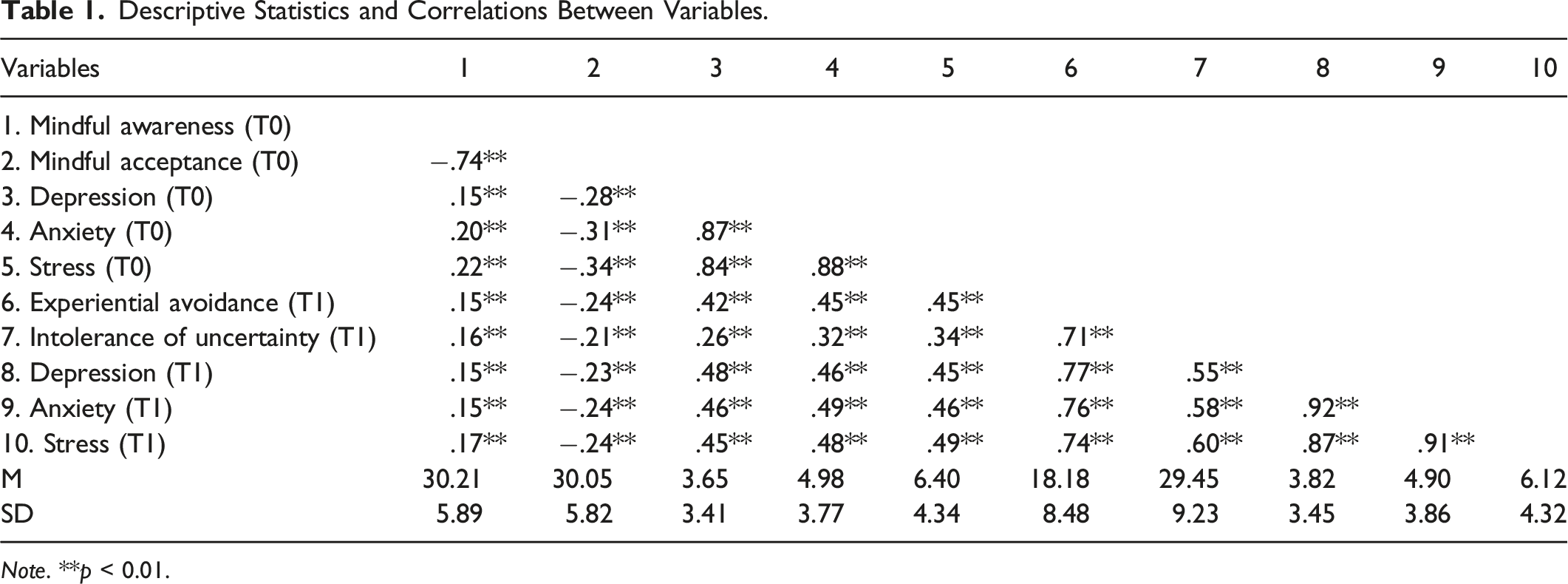
Note. **p < 0.01.
Testing for the Mediation Model
The measurement model (see Figure 1) consisting of mindful awareness at T0, mindfulness acceptance at T0, experiential avoidance at T1, intolerance of uncertainty at T1, and mental health problems at T1 revealed an acceptable fit to the data: χ2 = 255.1, df = 44; RMSEA = .073; CFI = .98; and TLI = 0.96. The root mean square error of approximation (RMSEA; Steiger, 1990; Steiger & Lind, 1980), comparative fit index (CFI; Bentler, 1990), and Tucker–Lewis index (TLI; Bentler & Bonett, 1980; Tucker & Lewis, 1973) are three model fit indices that are widely applied. RMSEA assesses how far a hypothesized model is from a perfect model, CFI and TLI compare the fit of a hypothesized model with that of a baseline model (Xia & Yang, 2019). Hu and Bentler (1999) suggested that an RMSEA smaller than .06 and a CFI and TLI larger than .95 indicate relatively good model—data fit in general. The RMSEA is not completely satisfactory, probably because of the small degree of freedom. Browne and Cudeck (1992) suggested the RMSEA of about .08 or less indicate reasonable error of approximation. The RMSEA too often falsely indicates a poor fitting model when the cutoff values are used to assess the fit of the properly specified models with small degree of freedom (Kenny et al., 2015). Structural equation model.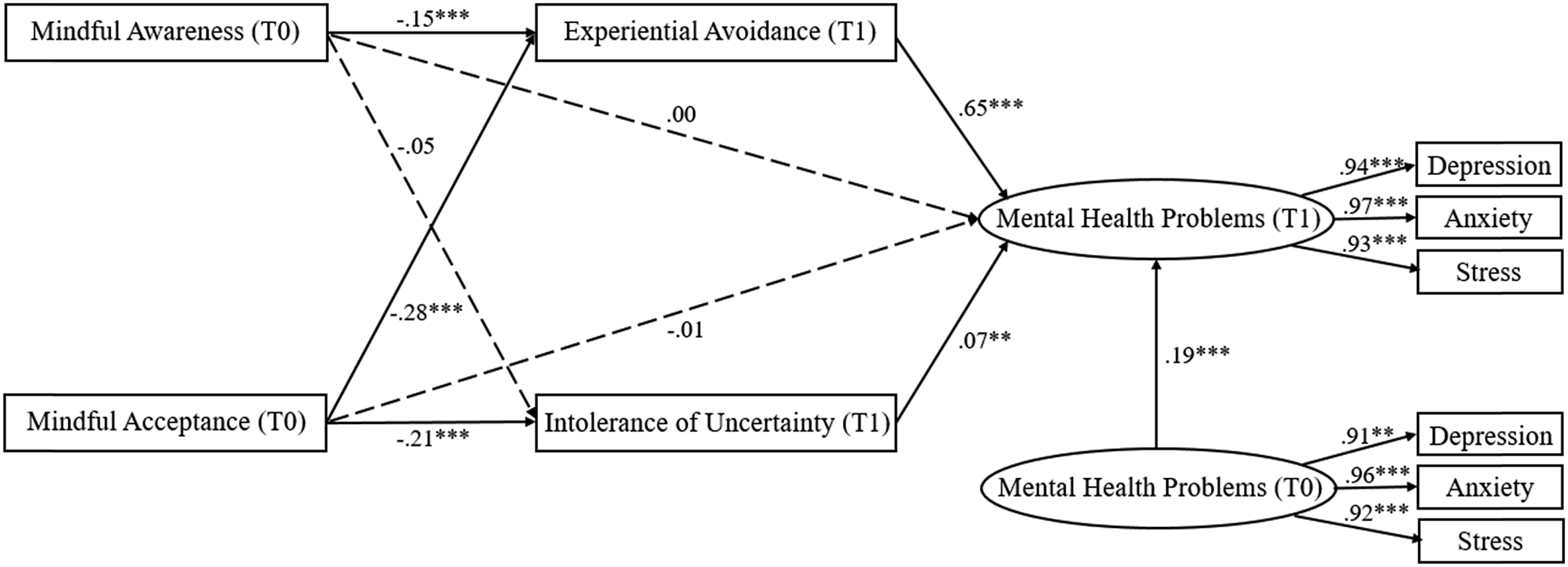
Bootstrapping procedures in AMOS were used to test the significance of the mediated model. Mindful awareness at T0 exerted a significant indirect effect on mental health problems at T1 through experiential avoidance at T1 (indirect effect = −0.052, 95% CI = −0.084 ∼ −0.017), but the indirect effect through intolerance of uncertainty at T1 did not reach significance. The relationship between mindful acceptance at T0 and mental health problems at T1 was mediated by both experiential avoidance at T1 (indirect effect = −0.105, 95% CI = −0.144 ∼ −0.068) and intolerance of uncertainty at T1 (indirect effect = −0.009, 95% CI = −0.018 ∼ −0.002). Different from the results of correlation analysis, mindful awareness negatively associated with experiential avoidance.
Discussion
The aim of the current study was to provide further evidence of the longitudinal relationships among dimensions of trait mindfulness, experiential avoidance, intolerance of uncertainty and mental health. Consistent with prior studies (Baer et al., 2006; Hayes et al., 2004; Klein et al., 2015; Kraemer et al., 2016; Pinto-Gouveia et al., 2012; Simione et al., 2021), higher levels of mindful awareness at baseline were associated with higher experiential avoidance, intolerance of uncertainty and mental health problems 6 months later, whereas mindful acceptance at baseline was negatively associated with those constructs. The mediating role of experiential avoidance and intolerance of uncertainty in the relationship between dimensions of mindfulness and mental health was also examined.
From the longitudinal perspective, experiential avoidance and intolerance of uncertainty mediated the relationship between mindful acceptance and mental health problems, which supported our study hypothesis. The receptive stance of mindfulness encourages individuals to stay in contact with their thoughts, attend to the information they provide flexibly and accept anything that occurs within or outside of themselves (Hayes et al., 1999). Therefore, mindful acceptance is supposed to diminish experiential avoidance, allowing individuals to be less consumed by negative thoughts and cognitive biases, which ultimately reduce related negative emotional distress. College students who are naturally higher in mindful acceptance might also take a more curious, open and accepting attitude toward their experiences (Keng et al., 2011). Then even when confronted with negative experiences, they perceive them as less threatening. Such individuals are prone to develop the ability to tolerate the uncertainty brought about by the content of these experiences (Kraemer et al., 2016), resulting in less negative emotional reactivity to depressive, anxiety-provoking and stressful situations.
Regarding another component of trait mindfulness, there was evidence of significant indirect effects of mindful awareness on mental health through experiential avoidance (EA), but the direction was inconsistent with our hypothesis. Correlation analysis showed a significant positive correlation between mindful awareness and EA as expected. However, we did not observe that awareness can lead to increased EA, resulting in higher levels of mental health problems in the structural equation model. Correlation analysis describes the relationship between mindful awareness and EA, while the structural equation model involves the relationship between mindful awareness, mindful acceptance and EA at the same time. A possible explanation is that there is some connection between the three when calculating, and the negative effect of mindful acceptance on EA is too strong, resulting in a reversal of the relationship between mindful awareness and EA in this structural equation model. According to the result of the correlation analysis, high levels of mindful awareness alone may associated with the increase of EA. Perceiving or even ruminating about negative experiences may lead to people’s unwillingness to have unpleasant thoughts and emotions, when people try to avoid negative emotions, they will inevitably think of them, which instead evokes the emotional experience of negative experiences.
Results of the current study suggest that mindful awareness and acceptance may have different functions when working alone. Specifically, these two constructs may have different relationships with mental health. Previous research have found the differences between mindful awareness and acceptance, for example, mindful acceptance may be the driving factor in the relationship between mindfulness and food susceptibility, awareness alone is not sufficient for promoting healthier appetite regulation (Keirns et al., 2022); mindful acceptance is fairly consistently related to positive outcomes (Baer et al., 2006; Cardaciotto et al., 2008), while awarenessare is unrelated to problem areas or even linked to increased problems (Baer et al., 2006). Results of the current study may also help explore the differences between mindful awareness and acceptance, and inform mindfulness-based interventions for mental health problems by clarifying which facet of mindfulness is more important.
Moreover, the findings in the current study did not support the indirect effect of intolerance of uncertainty (IU) in terms of the relationship between mindful awareness and mental health. Potential explanations can be provided from two aspects. On the one hand, correlation analysis revealed an independent positive correlation between mindful awareness and IU, but the path coefficient between them in the structural equation model did not reach the level of significance. Consistent with the above, this may be because the negative relationship between mindful acceptance and IU has an effect on the relationship between mindful awareness and IU when calculated in a complex model. On the other hand, awareness points to the present (Bishop et al., 2004), encouraging individuals to focus on current experiences rather than be preoccupied with past or future events (Roemer & Orsillo, 2003). However, IU generally points to the future (Carleton, 2012; Dugas et al., 1997). Therefore, awareness may not have much effect on people’s ability to tolerate uncertainty in the future.
Some of these findings are consistent with previous studies suggesting experiential avoidance as a mechanism of action for mindfulness (McCluskey et al., 2020). Our study can provide a more specific view of the relationship between mindfulness, experiential avoidance and mental health. Both mindful awareness and acceptance confer their benefits through the decrease of mental health problems by reducing experiential avoidance and providing a more comprehensive understanding of the internal mechanism.
Overall, these results indicated the vital role of mindfulness, as a trait, in reducing college students’ depression, anxiety and stress at long-term levels. To protect students from mental distress, mindfulness-based interventions could potentially be used in colleges and universities to provide a coping strategy to reduce students’ depression, anxiety and combat stressors (Bamber & Kraenzle Schneider, 2016). These findings may also provide inspiration and direction for school teachers, researchers, and policy-makers to design and launch school-based programs to improve college students’ mental health (Napoli et al., 2005), for example, reducing students’ experiential avoidance and intolerance of uncertainty by improving their dispositional mindfulness (McCluskey et al., 2020).
Our study has some limitations. First, the participants were college students in China. Researchers should be cautious when generalizing the results of this study to students of different ages and ethnic groups. Additionally, by using nonclinical college samples, inferences about these relationships among individuals with diagnosable depression, anxiety and stress disorders are limited. Future research might discuss the relationship between mindfulness, experiential avoidance, intolerance of uncertainty and mental health in clinical samples to better infer the role of mindfulness components in psychotherapy and more serious forms of mental health problems. Second, our study was conducted online so the circumstances and state of the participants when completing the questionnaire were unknown. The reliability and validity of the questionnaire may be better if measured offline. Third, due to the longitudinal design, incidents that may affect the results might have happened during the 6 month interval, but we did not have enough information to follow. Finally, we did not investigate the short-term and long-term effects of mindfulness-based interventions on improving college students’ mental health. Future studies may explore the potential mechanisms of mindfulness-based interventions for this population.
Footnotes
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by F.S. Y.S and X.W. The first draft of the manuscript was written by F.S. X.W. supervised the process and acquired foundation for this study. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China [Grant No.31800929] and the Fundamental Research Funds for the Central Universities [Grant No. 2020NTSS42].
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Biomedical Research Institutional Review Board of Beijing Normal University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standard.
Availability of Data and Material
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Informed Consent
Informed consent was obtained from all individual participants included in the study.