
Abstract
Direct relationships between perceived discrimination and eating pathology in ethnic minorities are well-documented. However, theoretical work examining unique risk and resilience factors that strengthen or weaken the relation between these constructs in ethnic minorities is lacking. The current study aims to address this gap by incorporating stress-process and tripartite frameworks to examine social and personal resources as they relate to perceived discrimination and eating pathology. In a sample of Black, Asian, and Latine women (N = 296, M age = 30.82), social support did not mediate the relationship between perceived discrimination and eating pathology. A significant interaction effect was observed for thin-ideal internalization strengthening the relation between perceived discrimination and negative emotional eating. Thin-ideal internalization moderated the relation between perceived discrimination and negative emotional eating in Latine Women, and disordered eating in Black Women. Overall, findings suggest ethnic minority Women have both personal and social resources that may influence the strength of effect on the relation between perceived discrimination on eating pathology.
Keywords
Introduction
Disordered eating includes cognitions, attitudes, and behaviors related to food restriction, binge eating, and purging (APA, 2013), coupled with concerns about weight and shape (Fairburn et al., 2011). Disordered eating exists in both clinical and non-clinical populations (Ciszewski et al., 2020; Kesby et al., 2019) and is associated with a myriad of psychological problems (Thome et al., 2004) such as symptoms of anxiety and depression. While disordered eating does not always warrant an eating disorder diagnosis, elevated levels can place one at risk for developing a diagnosable eating disorder (Pereira & Alvarenga, 2007). A related, but distinct construct to disordered eating is emotional eating. Emotional eating is defined as eating in response to negative (e.g., depression, stress, frustration) and positive (e.g., celebration, happiness) emotions in the absence of physiological hunger (Arnow et al., 1995). While both disordered and emotional eating are considered maladaptive, emotional eating focuses on specific emotional triggers associated with an eating response, while disordered eating ranges from sub-clinical to full-threshold attitudes, cognitions, and behaviors that relate to broad eating, shape, weight, and restriction concerns. Eating in response to negative emotions can be problematic, as elevated levels of emotional eating are associated with increased binge eating behaviors (Ricca et al., 2009) and higher weight concerns (Jordan et al., 2021). While the construct of emotional eating is highly nuanced (Bongers & Jansen, 2016), it is accepted that a positive relationship exists between emotional eating and disordered eating behaviors. Various theories exist in psychosocial risk factors that maintain disordered and emotional eating (Barakat et al., 2023; Reichenberger et al., 2020); one common theory conceptualizes eating pathology as a means to avoid or distract from an aversive emotional experience, such as stress (Heatherton & Baumeister, 1991). Exposure to stress is differentially distributed by race/ethnicity with minoritized individuals reporting greater stress than their white counterparts (McKnight-Eily et al., 2021). Stress-process models suggest that racial/ethnic minorities are disproportionately exposed to stressors related to unfair treatment regarding their social identity (Pascoe & Smart Richman, 2009), regarded as perceived discrimination (Pearlin et al., 1982).
Perceived discrimination, which ranges from subtle day-to-day experiences to significant life events, is related to deleterious eating disorder symptoms in minoritized populations (Kwan et al., 2018). For example, perceived discrimination contributes to eating for reasons other than hunger among African American Women (Johnson et al., 2002), which can be conceptualized closely to emotional eating (i.e., eating in response to negative emotions) (Arnow et al., 1995). Likewise, in a sample of 104 college-aged Black Women, higher race and gender-related stress (Jackson et al., 2005) was positively associated with Body Mass Index (BMI) among students who engaged in emotional eating. Overall, eating disorder symptoms are associated with a variety of stress responses in Black (Longmire-Avital & McQueen, 2019) and Latine (Hoggard et al., 2019) American Women. Similarly, a cross-sectional study found that the “strong Black Woman” schema, a common, high-effort coping mechanism in response to racial-gendered microaggressions, was a significant predictor of emotional eating in 102 collegiate Black American Women (Longmire-Avital & Finkelstein, 2021). Consistent with these findings, a recent meta-analysis found that the relationship between discrimination and eating disorder pathology was characterized by a small-to-medium effect size (Mason et al., 2021).
The relationship between minority specific stressors and health outcomes, such as disordered eating, may be understood utilizing minority stress and stress-process models of coping. Minority stress and stress-process models suggest that minoritized individuals have additional ‘social and personal resources’ that influence the relationship between perceived discrimination and health outcomes (Pearlin et al., 1982), such as disordered and emotional eating. Cheng (2014) found that racial discrimination was related to disordered eating behaviors, with negative self-concept and low self-esteem indirectly mediating these effects in Asian/Asian American Women. Additionally, Salami and colleagues (2019) found an indirect effect of race-related stress on eating pathology via depressive symptoms in Black American Women. All in all, risk factors have been well-documented that exacerbate the effects between perceived discrimination and eating pathology. However, less is known about factors that may protect against the deleterious effects of perceived discrimination. Particularly, less work has examined how perceived discrimination may relate to eating in response to negative emotions; specifically, how coping mechanisms that are at the interpersonal level, such as perceived socials support, may serve as a protective role on the relation between perceived discrimination and eating disorder symptoms in ethnic minority Women.
Perceived social support contains several domains, including tangible, emotional, and positive support (Sherbourne & Stewart, 1991), which may protect against deleterious health outcomes. One study found perceived social support protected against hospital readmission and death among ethnic minority adults who were hospitalized (Chan et al., 2019). Furthermore, a large body of research has documented a significant, negative relation between perceived social support and disordered eating (Yoshikawa et al., 2021). Per the stress-process model, social support can be conceptualized as a mediating role, rather than a moderating role that impacts the relation between stress and health outcomes (Pearlin et al., 1982), as it posits when one experiences systematic stress (i.e., perceived discrimination), they may directly turn to ‘social resources’ (i.e., perceived social support), as a means of coping, rather than relying on individual coping mechanisms (i.e., affect regulation). Thus, social support may mediate the relation between perceived discrimination and negative health outcomes, such as eating disorder symptoms. In drawing conclusions from their recent meta-analysis, Mason and colleagues (2021) recommended that future research should examine perceived social support as a factor that may be associated with perceived discrimination and eating disorder symptoms in diverse samples. To that point, Johnson and colleagues (2022) surveyed a nationally representative sample of 2250 Latines cross-sectionally. Results indicated that discrimination was significantly positively related to binge eating, but surprisingly social support did not interact with discrimination nor binge eating. While this study examined the relation between perceived discrimination and binge eating via perceived social support in Latine individuals, less is known about global disordered eating, which including shape and weight concerns, as well as the inclusion of Black, and Asian Women. In addition to examining the possible role of social support, one’s ethnic identity might also serve as protective against discrimination’s deleterious effects on eating behavior.
Ethnic identity, defined as a sense of closeness and belonging to one’s racial/ethnic identity, serves as a protective factor against various psychological disturbances, such as low self-esteem and poor coping mechanisms (Greig, 2003). Furthermore, ethnic minorities who have a strong connection to one’s cultural background may be protected from Western standards of beauty (particularly for Black and Latine Women) (Brouillard & Hartlaub, 2005), which may in turn relate to less eating pathology. For example, Abrams et al. (2015) posit Black culture promotes more fluid ideals of beauty for Women, such that Black Women with a high level of ethnic identity may not subscribe to the European standard of beauty, and thus might be at a lower risk for developing disordered eating behaviors. Similar conclusions have been drawn about Latine cultures (Warren et al., 2005). These ideas were also supported by a study conducted with a sample of 816 European, African, Latine, and Asian American college student Women (Rakhkovskaya & Warren, 2014), where ethnic identity moderated the relationship between thin-ideal internalization and eating concerns such that the relation was stronger for participants with lower ethnic identity. While information is known about ethnic identity and its protective role on eating pathology broadly, as well as on perceived discrimination (Vines et al., 2017), no study to date has examined ethnic identity, particularly how affirmed one feels in their ethnic identity, on the relation between perceived discrimination and emotional eating, a distinct, but related construct to disordered eating. In contrast to the possible protective effects of ethnic identity and perceived social support, internalization of the thinness may indirectly strengthen the relation between perceived discrimination and disordered and emotional eating.
Per the tripartite influence model of eating pathology (van den Berg et al., 2002), appearance related pressures deriving from peers, family, and media may lead to internalization of body-ideals, such as the thin-ideal internalization. Thin-ideal internalization is operationalized as the level in which one values and prioritizes thinness; if one’s body does not match what one perceives as an idealized body, it can lead to body dissatisfaction, which is established as a primary risk factor for eating disorder symptoms (Griffiths et al., 2018; Talbot et al., 2019). To that end, thin-ideal internalization, operationalized as the extent to which one ‘buys into’ thinness as socially ideal and attractive (Thompson & Stice, 2001), increases the risk of eating pathology. However, appearance and shape ideals may vary across racial/ethnic groups. For example, Awad and colleagues (2015) suggest Black women idealize ‘thick’ or ‘curvy’ bodies, whereas thin-ideal internalization is more prevalent within Asian (Wang et al., 2020) and White (Ahern et al., 2008) women, with Latine women reporting a drive for thinness coupled with appreciation for a curvier body type (Viladrich, 2009). To that end, appearance and shape ideals may vary based on acculturation (Vartanian et al., 2005). For example, Black and Latine American Women with low levels of acculturation (e.g., acculturating to white American culture) might have certain cultural norms that stray away from the thin ideal, and thus might experience lower levels of thin-ideal internalization, whereas Asian and White American Women experience higher levels of thin-ideal internalization due to the thinness expectancy within their cultural norm. To that end, thin-ideal internalization has been supported to exacerbate the relationship between sociocultural risk factors for eating pathology and disordered eating. For example, in a cross-sectional (N = 168, 97% White) sample of college students, thin-ideal internalization moderated the relationship between social media use and body dissatisfaction, such that at high levels of thin-ideal internalization, a stronger relationship between social media use and body dissatisfaction was present (Martinez et al., 2019). Given varying body ideals described above, it is important to examine Black, Latine, and Asian Women’s thin-ideal internalization in relation to perceived discrimination and eating disorder symptoms, separately.
Present Study
While these data suggest that perceived discrimination relates to binge eating, with insignificant, negative, indirect effects of perceived social support in Latine Women (Johnson et al., 2022), no study to date has examined if these effects are different with global disordered eating, which includes shape and weight concerns, nor examined eating in response to negative emotions. Additionally, no study to date has extended this model with including other ethnic minority Women, such as Black and Asian Women. Lastly, no study to date has examined if such resilience factors (i.e., social support and affirmation of ethnic identity) protect against perceived discrimination’s impact on emotional eating, particularly. The present study aims to extend models of risk and resilience factors in ethnic minority Women to address the following research questions: Does perceived social support mediate relationships between perceived discrimination and eating disorder symptoms (i.e., global disordered eating and emotional eating) in a sample of ethnically minoritized Women? It was hypothesized that social support would mediate the relationship between perceived discrimination and disordered and emotional eating, such that perceived discrimination would affect disordered and emotional eating through social support. Second, do ethnic identity and thin-ideal internalization moderate these relations? It was hypothesized that ethnic identity would moderate the relationship between perceived discrimination and disordered and emotional eating, such that at high levels of ethnic identity, a weaker relationship between perceived discrimination and disordered and emotional eating would be expressed. In terms of the thin-ideal, it was hypothesized that it would strengthen the relationship between perceived discrimination; such that, at high levels of thin-ideal internalization, a stronger relationship between perceived discrimination and disordered and emotional eating would be expressed. A third, exploratory aim was established to examine the moderating effect of thin-ideal internalization in Black, Latine, and Asian Women, separately. Given the exploratory nature of this aim, no a-priori hypotheses were generated.
Method
Participants
Participants who self-identified as Women and at or over the age of 18 were recruited via Amazon Mechanical Turk, and identification with an ethnic/racial minority group was required for study enrollment. According to an a priori power analysis at a .80 power level, with a small effect size and .05 significance threshold, 344 participants were desirable. However, participants were recruited until virtually equal groups were established for exploratory analyses (e.g., 100 in each ethnic minority group) as well as creating equal representation among participants. For example, when an adequate number of Black American Women were recruited, the only Latine and Asian Women were recruited, and so forth. Participants were recruited via Mechanical Turk, as it is more likely to pull from a more diverse pool than undergraduate students (Buhrmester et al., 2011). This study was advertised to female workers residing in the United States.
Systematic recommendations for producing robust and reliable data when recruiting via Mturk have been published (Aguinis et al., 2021), and several of these recommendations were implemented in the current study. As such, prior to data collection, the researchers determined the qualifications that would be used to screen MTurk workers. Interested subjects were not made aware of the race/ethnicity inclusion criteria (i.e., Black, Latine, or Asian). Thus, participants could not falsify their race/ethnicity to participate in the study and were immediately screened out if they reported being White/Caucasian. In addition, the present study was only advertised to Female workers, eliminating the possibility of someone falsely reporting their sex. It was also determined a-priori that eligible participants must reside in the United States, as well can read and write in English. The present study was only advertised to “Master Workers”, which are people who have scored at least a 98% approval rating. The sample size was established a-priori, with the plan of collecting data on at least 15% more than the final sample size. Participants were also required to complete a CAPTCHA verification to thwart web robots, and participants who had duplicate IP addresses were screened out. Lastly, five attention checks were utilized throughout the study, such as having to type-back a sentence (e.g., “I went to the store today”). Participants also were assigned a unique worker ID in which they could not take the survey more than once which may have mitigated participants taking the survey repeatedly until they met participant demographic criteria, as well as attempting to take the survey multiple times until they passed the race/ethnicity screening item.
Procedure
Participants signed an online consent form agreeing to participate in a 25–30-min voluntary study about different life experiences and health behavior. Interested individuals were not informed that they must identify with having an ethnically minoritized identity to be eligible for study participation. The present study was only advertised to women. Following consent, the first item was a screening question that asked about their race/ethnicity, where they were asked to choose what racial/ethnic minority BEST described them (i.e., only one race/ethnicity item could be chosen). This rationale was to establish sub-group analyses for aim three. All questionnaires were counterbalanced. The survey averaged taking 21 minutes. Participants received $1.00 monetary compensation for completing the survey. All procedures were approved by the affiliated university’s Institutional Review Board (IRB).
Measures
Sociodemographic Characteristics and Anthropometrics
Sociodemographic variables including racial and ethnic composition and age were assessed. Income was measured by the participant’s estimated yearly total household income. Body Mass Index (BMI) was assessed by self-report of height (inches) and weight (lbs.).
Disordered Eating
The EDE-Q is a questionnaire format of the Eating Disorder Examination Interview (Fairburn et al., 2011). This measure includes 28 items, measuring disordered eating cognitions, attitudes, and behaviors. Item options range from 0 to 6, with greater scores indicating greater endorsement of eating disorder symptomatology. A global score (EDEQ-Global) was calculated by taking the mean score of all subscale items. Scores ≥4 (range: 0–6) on EDEQ-Global are indicative of clinically significant eating, shape, weight, restriction, and global eating pathology concerns, respectively. Higher scores yield higher global disordered eating. A sample item includes, ‘Has your weight influenced how you think about (judge) yourself as a person?’. The EDEQ has shown acceptable internal consistency in ethnic minority populations, with an acceptable α coefficient (.70–89, see Kelly et al., 2012). It also has high test-retest reliability in Black and Latina American women (α = .81 and .79, respectively, see Rose et al., 2013) and in non-clinical populations (Berg et al., 2012). Internal consistency in the current study was excellent in global (α = .96) and good in sub-scale scores (α′s > .80).
Emotional Eating
The Emotional Eating Scale-Revised (EES-R, Koball et al., 2012) was reconstructed from the original Emotional Eating Scale (EES, Arnow et al., 1995) to include a separate boredom factor. The EES-R is a Likert scale measurement that assesses emotional eating in three subscales: Depression, Boredom, and Anxiety/Anger. A five-point scale was used to anchor between “no desire to eat” to an “overwhelming desire to eat”. Total scores were analyzed for the present study and higher scores yield higher endorsement of negative emotional eating. An example item is ‘How much desire do you have to eat in response to ‘anger’? This scale was originally validated in clinical samples, but then later validated for non-clinical populations (Schneider et al., 2012). Internal consistency was reported at 0.93 for the entire scale (Koball et al., 2012), with 2-week test-rest reliability being robust in a sample of predominately Black women (α = .79) (Risica et al., 2021) and internal consistency being excellent in a sample of Chinese undergraduates (α = .93, see Yang et al., 2023). Internal consistency in the current study was excellent (α = .97).
Perceived Discrimination
One of the most widely used measures for perceived discrimination is the Everyday Discrimination Scale (EDS, Williams et al., 1997). The EDS was developed to capture aspects of global, interpersonal discrimination that are chronic or episodic. EDS consists of 9-items in a 6-point Likert scale format. Total score was derived from a sum of all scores, with higher scores indicating greater perceived discrimination. An example item is, ‘In your day-to-day life, how often have any of the following things happened to you?’ (ranging from never (1) to almost every day (6)). The EDS has been validated across racial and ethnic groups, with internal consistency deemed as adequate (i.e., Black, Latino, Asian Americans, (α > .80) (Kim et al., 2014). Internal consistency in the current study was very good (α = .92).
Social Support
Social support was measured using the Multidimensional Scale of Perceived Social Support (MSPSS), which was designed to measure perceptions of support. This scale is comprised of 12 items (4 items from each subscale). Sample item includes ‘I got the help and support I need from my friends’. The MSPSS is comprised of three subscales: significant other, family, and friends. Scores are derived from the mean of the total raw scores, with higher scores indicating higher levels of social support. Only total scores were calculated. Higher scores indicate greater levels of global perceived social support. The MSPSS has been shown to have good internal and test-retest reliability and good validity (Zimet et al., 1990), and has been validated across racial and ethnic groups (Canty-Mitchell & Zimet, 2000; Edwards, 2004, αs > .70). Internal consistency in the current study was good (α = .89).
Ethnic Identity
The Ethnic Identity Scale-Brief (EIS-B) version was developed as a 9-item brief version of the EIS (Douglass & Umaña-Taylor, 2015). The affirmation subscale is three items and measures the degree to which a person associates with their ethnic-group membership and ethnic-racial identity content (Umaña-Taylor et al., 2004). An example item is the following: ‘I do not like my ethnicity’. The affirmation subscale was reverse coded, with greater scores reflecting greater affirmation of ethnic identity. Existing findings provide support for the validity and reliability of the EIS-B as a brief measure of the multidimensional construct of ethnic-racial identity and indicate that the EIS-B assesses ethnic-racial identity in comparison to the original version of the scale (EIS) at both the full-scale and subscale level (Douglass & Umaña-Taylor, 2015). Internal consistency has been shown to be adequate in Latina, Black, and Asian Americans (α = .84–.89, see Douglass et a., 2015) Internal consistency in the present study was adequate (α = .70).
Thin-Ideal Internalization
The Sociocultural Attitudes Towards Appearance Questionnaire-4th Edition (SATAQ-4) is a widely used and well-validated measure of appearance ideal internalizations and pressures (Schaefer et al., 2019). The thin-ideal internalization subscale is 5-items and was used for the current study, consisting of questions such as, “I think a lot about looking thin” and “I think a lot about having little body fat.” Higher scores indicate greater endorsement of thin-ideal internalization. In addition, the SATAQ-4 also demonstrated excellent convergent validity with measures of eating pathology, body image, and self-esteem (Schaefer et al., 2019), and has been validated in ethnic minority women, such as Black women (Burnette et al., 2020) and Japanese men and women (Yamamiya et al., 2019). In the current study, internal consistency was high (α = .93).
Statistical Analyses
Descriptive statistics were calculated to summarize demographic information including age, ethnicity and race, income, and BMI of participants. Preliminary analyses also included the examination of missing data, normality and homoscedasticity, and collinearity. Missing data were accounted for using list and pairwise deletion. One way-ANOVA were examined on continuous constructs of interest across racial minority groups. Bivariate correlations were calculated and a chi-squared test with standardized residuals was conducted to determine differences in socioeconomic status (SES) across racial minority groups. Mediation and moderation analyses were conducted with the PROCESS macro for SPSS (Hayes, 2013). All models were tested in separate, single models using a bootstrap approach (samples = 5000) to assess the significance. To determine the indirect effect of perceived discrimination on both disordered and negative emotional eating through perceived social support, separately, two mediation analyses were conducted using the bootstrapping method (Hayes, 2013). To measure the moderating effects of ethnic identity and thin-ideal internalization on the relation between perceived discrimination and disordered and negative emotional eating, separate moderation models were conducted in PROCESS (Hayes, 2013). All models had perceived discrimination as the predictor. For models 1 and 2, thin-ideal internalization was the moderator with disordered and negative emotional eating as outcomes. For models 3 and 4, ethnic identity was the moderator with disordered eating and negative emotional eating as outcomes. To measure thin-ideal internalization as a moderator of the relation between perceived discrimination and eating disorder symptomatology across Black, Asian, and Latine Women, separately 6 moderation models were conducted. Twenty-nine participants were excluded from these analyses given that, although they identified as an ethnic/racial minority, the selected their ethnicity as “Other” as opposed to Black, Latine, or Asian. Perceived discrimination was the predictor and thin-ideal internalization was the moderator for all models. Disordered and negative emotional eating were the outcomes across three racial/ethnic groups. PROCESS models (Hayes, 2013) produced regression coefficients, p-values, and confidence intervals for each regression included in all moderation models. To protect from Type-I error, a Bonferroni correction was made at a p < .05 level. Self-reported BMI was entered as a covariate in all PROCESS analyses.
Results
Preliminary Results
Bivariate Correlations on Constructs of Interest.
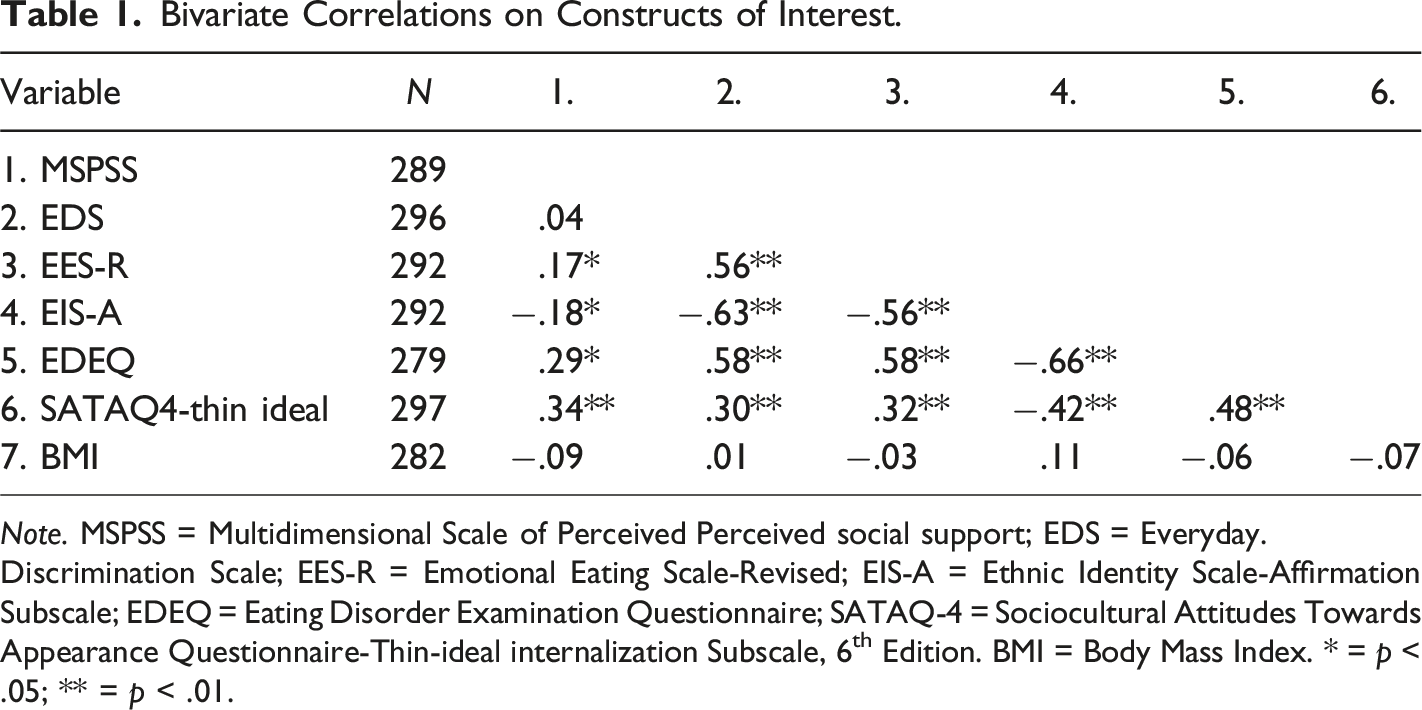
Note. MSPSS = Multidimensional Scale of Perceived Perceived social support; EDS = Everyday.
Discrimination Scale; EES-R = Emotional Eating Scale-Revised; EIS-A = Ethnic Identity Scale-Affirmation Subscale; EDEQ = Eating Disorder Examination Questionnaire; SATAQ-4 = Sociocultural Attitudes Towards Appearance Questionnaire-Thin-ideal internalization Subscale, 6th Edition. BMI = Body Mass Index. * = p < .05; ** = p < .01.
Mean Differences
A One-Way ANOVA was conducted to compare the constructs of interest across racial groups. Comparisons were made between Black, Asian, and Latine women. There was a significant difference in negative emotional eating across all subgroups, F (2, 240) = 6.243, p = .002. LSD post hoc results revealed that Black/African American women (M = 80.4, SD = 21.7) reported higher levels of negative emotional eating compared to Asian women (M = 67.0, S = 25.8). A significant difference was also revealed in perceived discrimination across all racial groups, F (2,271) = 5.719, p = .001. LSD post hoc results Black women (M = 37.3, SD = 9.14) reported higher levels of perceived discrimination (M = 37.3, SD = 9.14) than Asian Women (M = 37.3, SD = 9.14). Racial/ethnic groups also differed in ethnic identity, F (2,270) = 5.083, p = .004. LSD post hoc analysis revealed such that Asian Women (M = 7.79, SD = 2.30) reported significantly higher levels of ethnic identity compared to Black (M = 6.78, SD = 2.33 and Latine (M = 6.80, SD = 2.45) women. No significant differences in internalization of thinness, social support, BMI, or disordered eating existed between subgroups (See Table 3 all mean scores of constructs of interest across racial groups). Lastly, chi-squared test revealed no statistically significant association between SES and race/ethnicity, χ2 (249, 12) = 29.1, p = .212.
Social Support
As described in Figure 1, social support did not mediate the relationship between perceived discrimination and disordered eating. Perceived discrimination was not associated with perceived social support. When controlling for perceived discrimination, perceived social support significantly related to disordered eating, such that higher levels of perceived social support were associated with greater disordered eating. When controlling for perceived social support, perceived discrimination significantly related to disordered eating, such that higher levels of perceived discrimination were associated with greater disordered eating. Mediation model of the relation between perceived discrimination (EDS) and global disordered eating (EDEQ). Each pathway includes unstandardized path coefficients of the direct relation of one variable to another. The c path represents the total effect of the IV on the DV. The c’ path represents the direct effect of the IV on the DV after accounting for perceived social support (MSPSS). SEs are identified in parentheses. The indirect effect and confidence intervals are provided in the margin. **p < .01.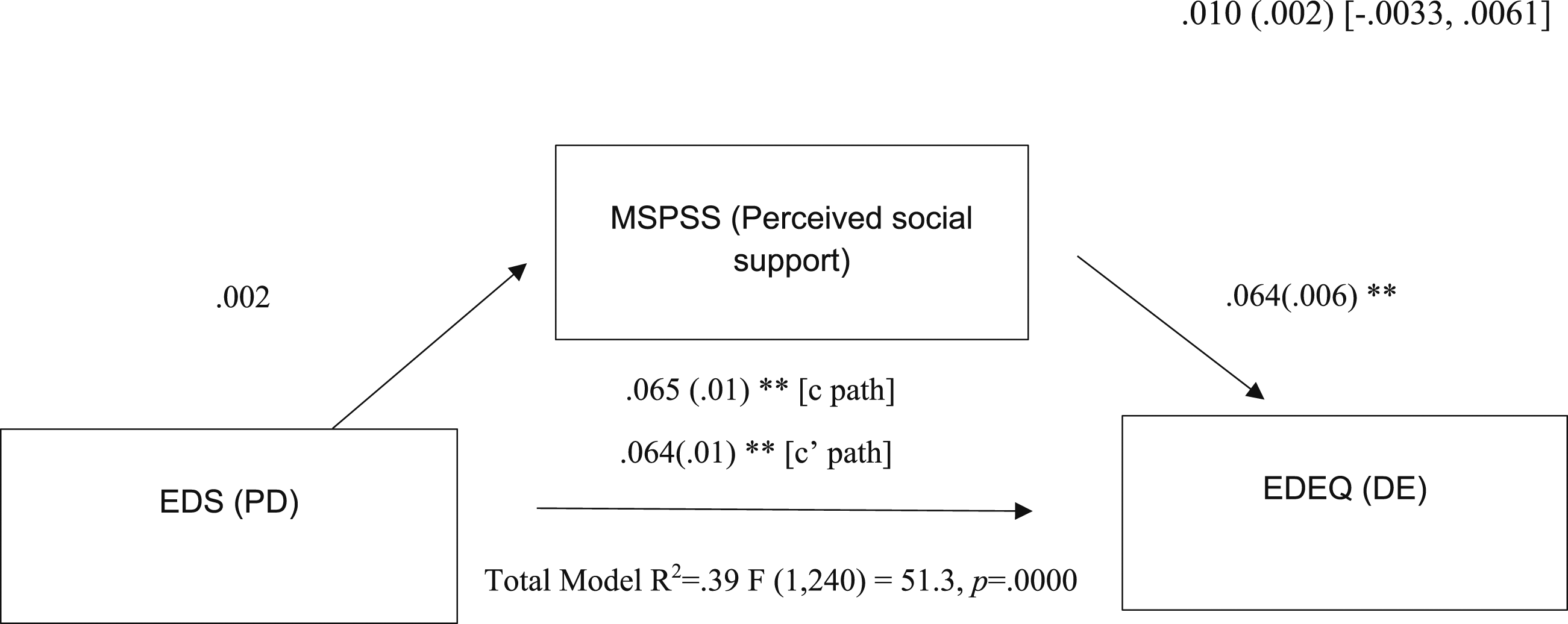
As described in Figure 2, social support did not mediate the relationship between perceived discrimination and negative emotional eating. When controlling for perceived discrimination, perceived social support significantly related to negative emotional eating, such that higher levels of perceived social support were associated with greater negative emotional eating. When controlling for perceived social support, perceived discrimination was significantly associated with negative emotional eating, such that higher levels of perceived discrimination were associated with greater levels of negative emotional eating. Mediation model of the relation between perceived discrimination (EDS) and emotional eating (EES-R). Each pathway includes unstandardized path coefficients of the direct relation of one variable to another. The c path represents the total effect of the IV on the DV. The c’ path represents the direct effect of the IV on the DV after accounting for perceived social support (MSPSS). SEs are identified in parentheses. The indirect effect and confidence intervals are provided in the margin. **p < .01.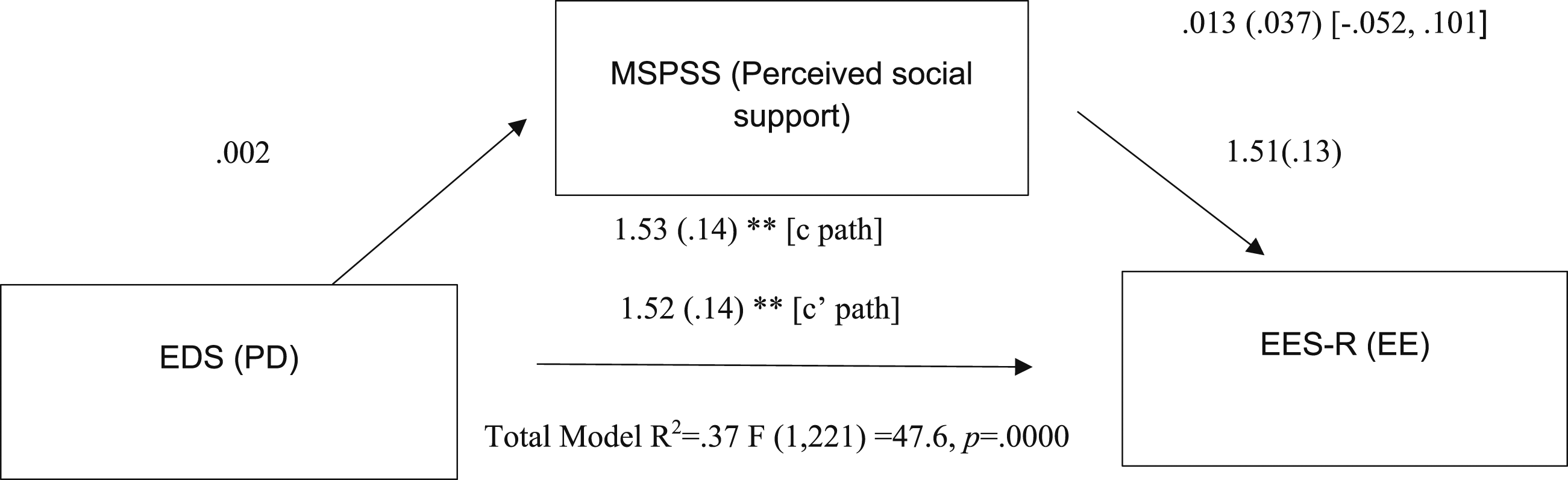
Ethnic Identity and Thin-Ideal Internalization
Means, Standard Deviations, and One-Way Analyses of Variance in Constructs of Interest Across Racial/Ethnic Minority Groups.
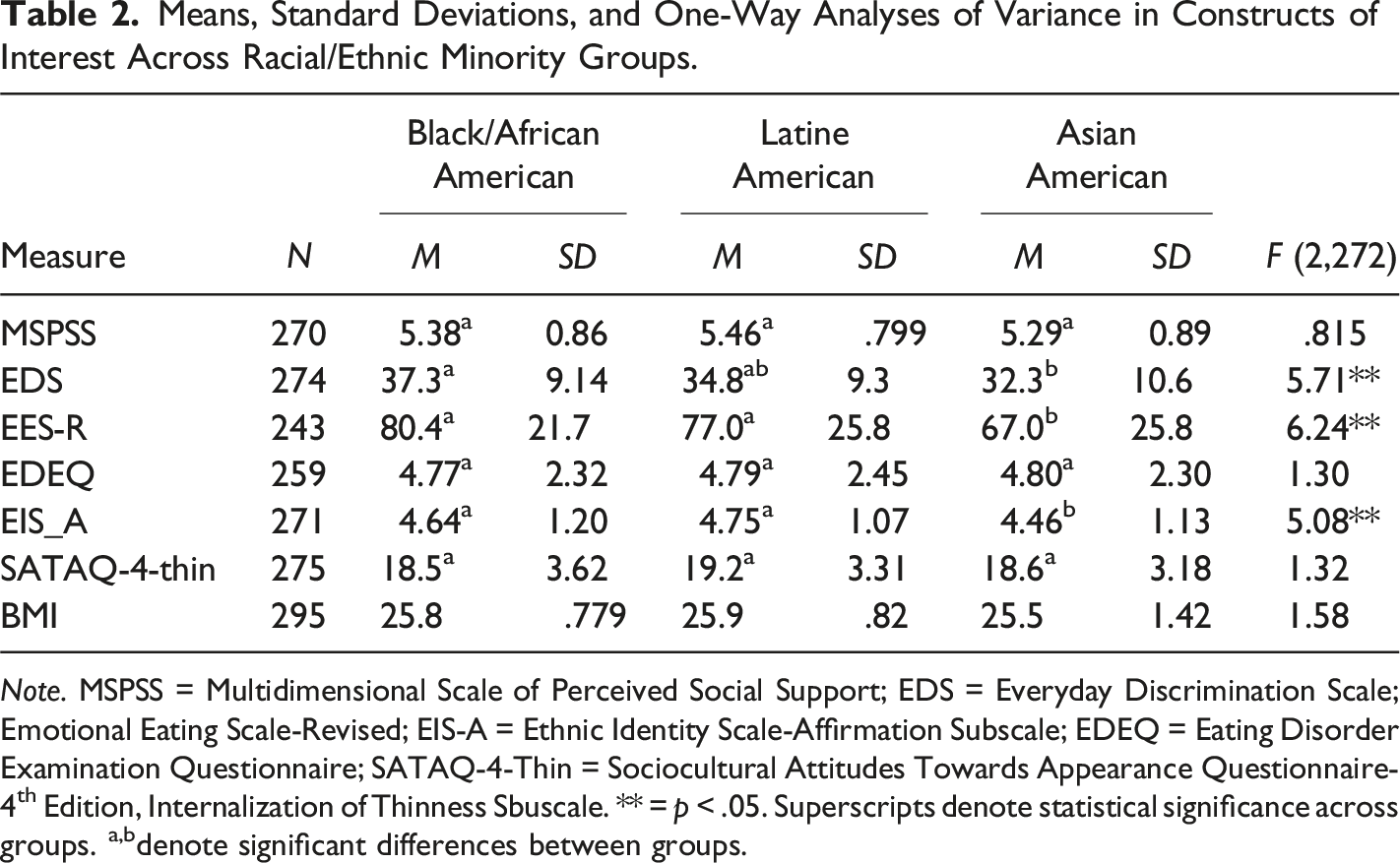
Note. MSPSS = Multidimensional Scale of Perceived Social Support; EDS = Everyday Discrimination Scale; Emotional Eating Scale-Revised; EIS-A = Ethnic Identity Scale-Affirmation Subscale; EDEQ = Eating Disorder Examination Questionnaire; SATAQ-4-Thin = Sociocultural Attitudes Towards Appearance Questionnaire-4th Edition, Internalization of Thinness Sbuscale. ** = p < .05. Superscripts denote statistical significance across groups. a,bdenote significant differences between groups.
Ethnic Identity as a Moderator on the Relation Between Perceived Discrimination and Eating Disorder Symptoms.
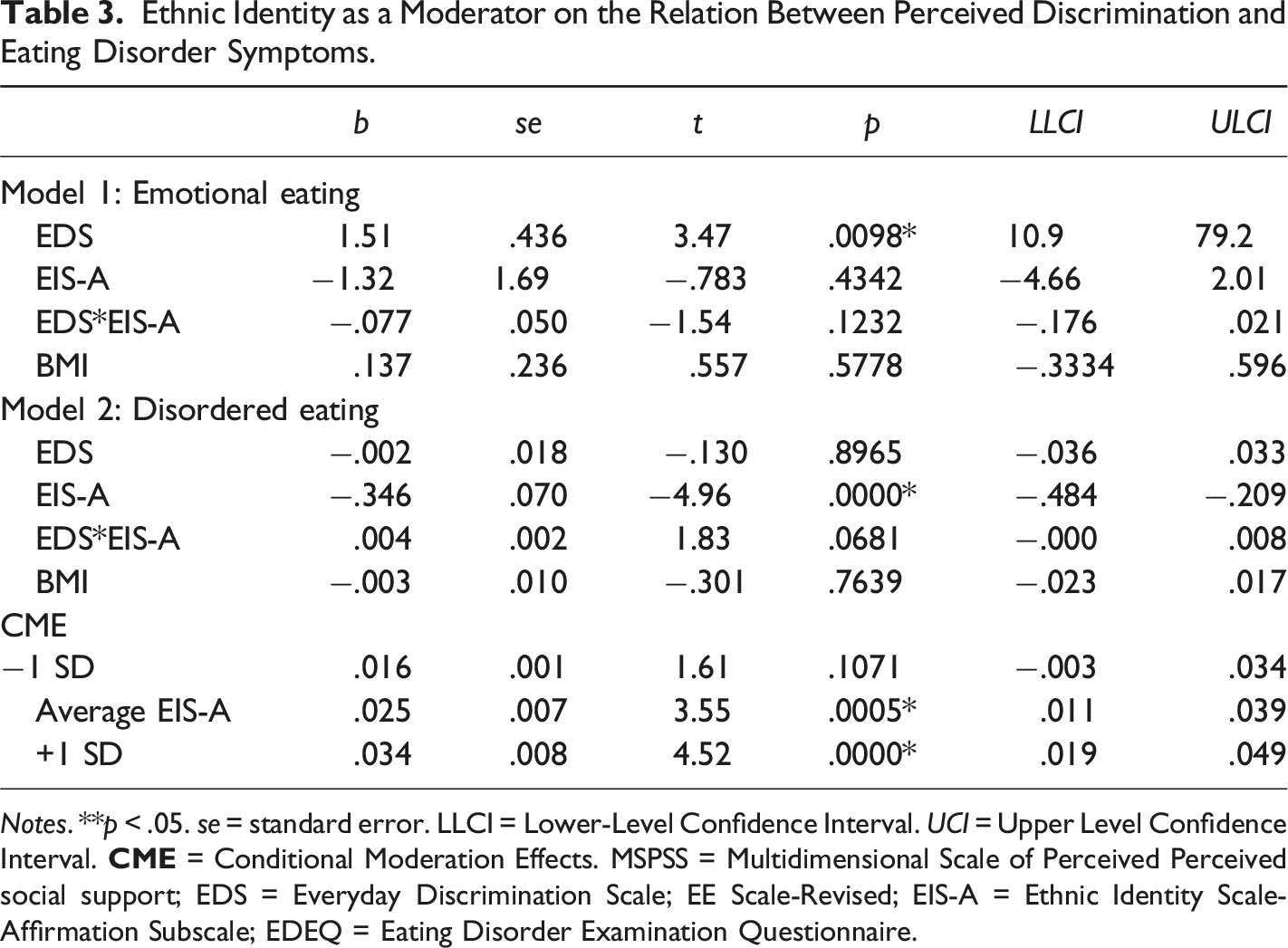
Notes. **p < .05. se = standard error. LLCI = Lower-Level Confidence Interval. UCI = Upper Level Confidence Interval.
Thin-ideal internalization was not a significant moderator in the relationship between perceived discrimination and disordered eating. When controlling for thin-ideal internalization, perceived discrimination significantly related to disordered eating, such that higher levels of perceived discrimination were associated with greater disordered eating. When examining negative emotional eating as the outcome, the interaction between perceived discrimination and thin-ideal internalization was significant. Meaning, that regardless of one’s thin-ideal internalization, higher perceived discrimination was related to higher negative emotional eating. However, the relationship between perceived discrimination and negative emotional eating was strongest at the highest level of thin-ideal internalization.
Thin-Ideal Internalization Across Racial Groups
Thin-Ideal Internalization as a Moderator on the Relation of Perceived Discrimination and Eating Pathology.
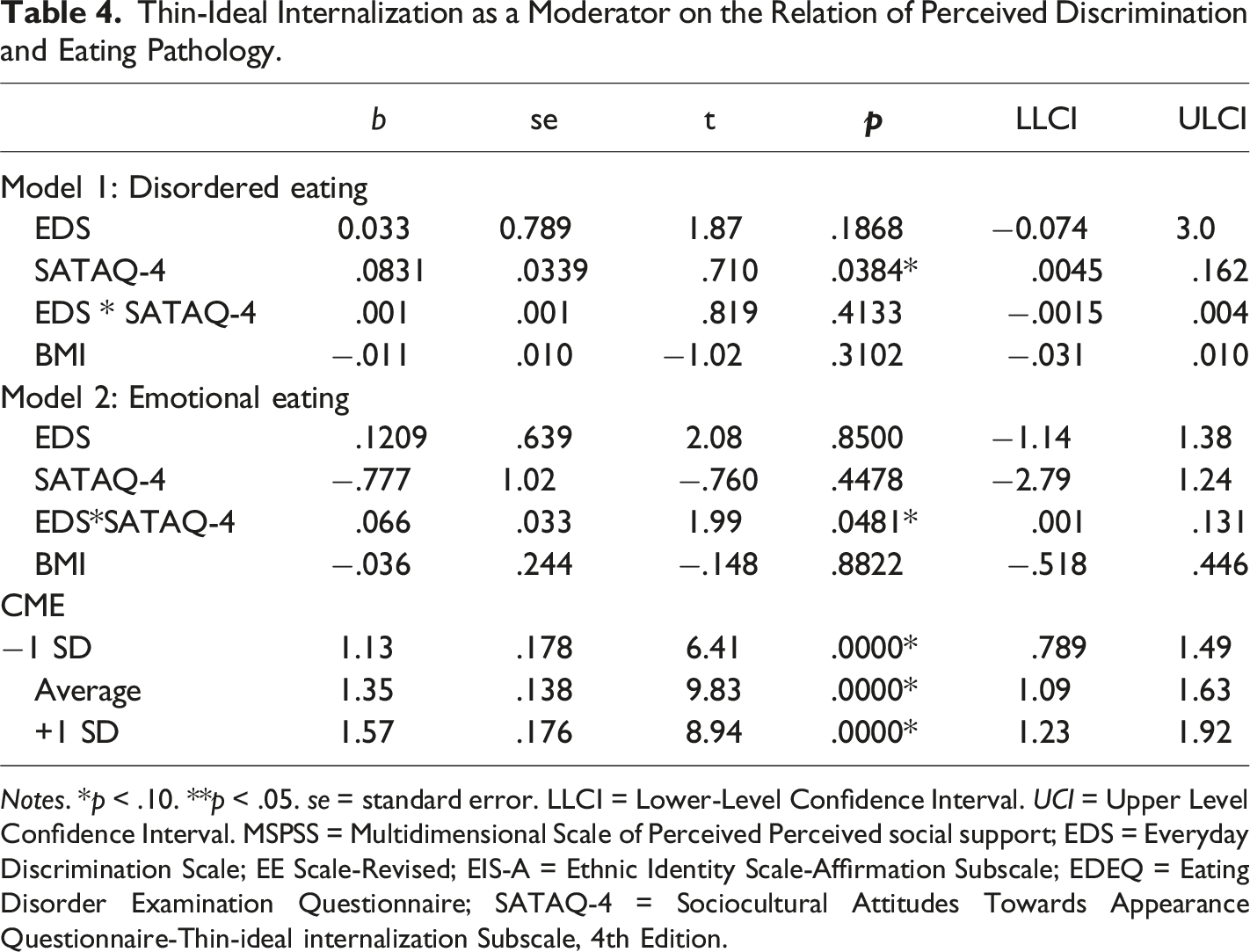
Notes. *p < .10. **p < .05. se = standard error. LLCI = Lower-Level Confidence Interval. UCI = Upper Level Confidence Interval. MSPSS = Multidimensional Scale of Perceived Perceived social support; EDS = Everyday Discrimination Scale; EE Scale-Revised; EIS-A = Ethnic Identity Scale-Affirmation Subscale; EDEQ = Eating Disorder Examination Questionnaire; SATAQ-4 = Sociocultural Attitudes Towards Appearance Questionnaire-Thin-ideal internalization Subscale, 4th Edition.
Sub-group Analysis of Thin-Ideal Internalization as a Moderator on the Relation Between Perceived Discrimination and Emotional Eating.
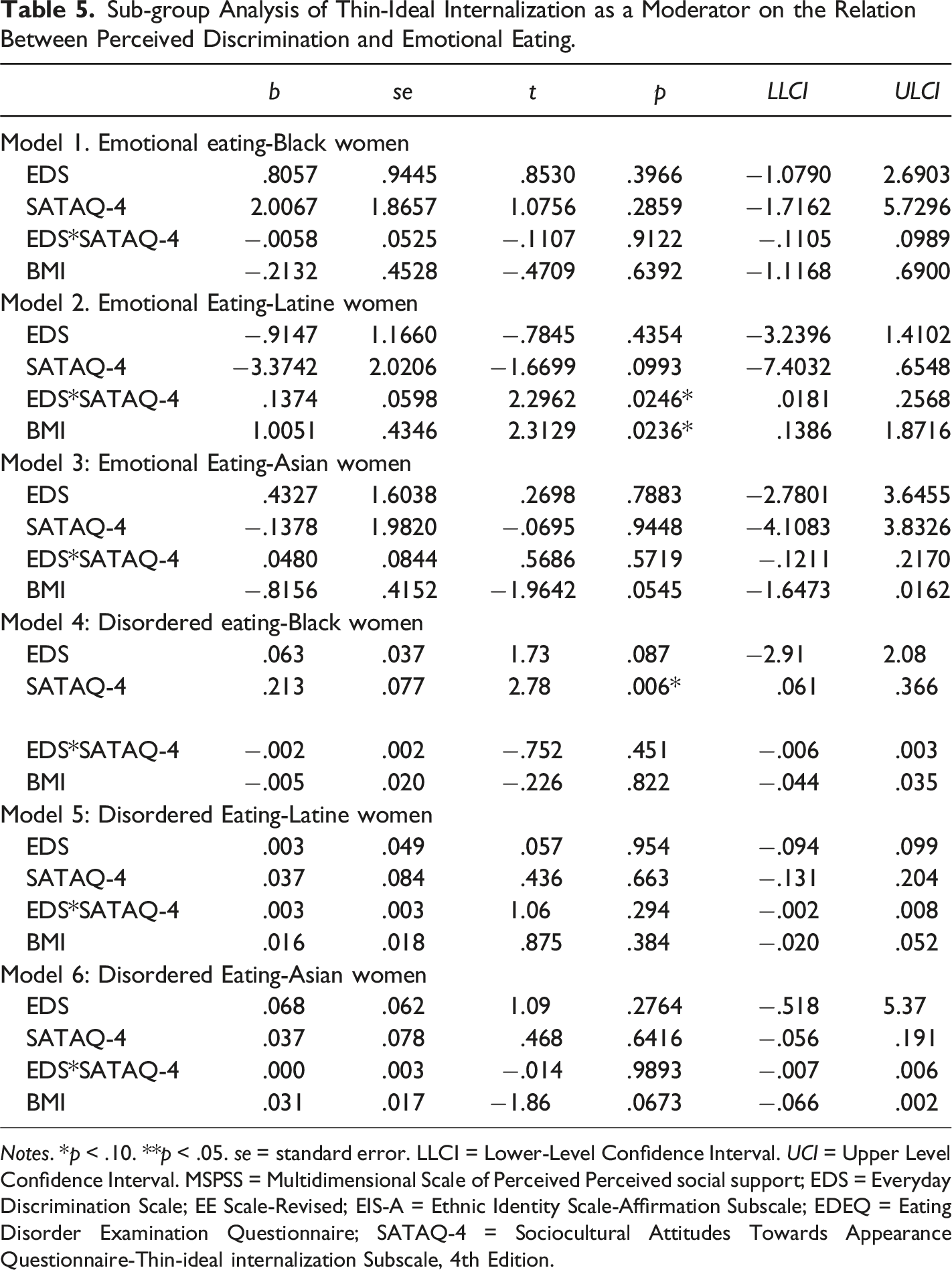
Notes. *p < .10. **p < .05. se = standard error. LLCI = Lower-Level Confidence Interval. UCI = Upper Level Confidence Interval. MSPSS = Multidimensional Scale of Perceived Perceived social support; EDS = Everyday Discrimination Scale; EE Scale-Revised; EIS-A = Ethnic Identity Scale-Affirmation Subscale; EDEQ = Eating Disorder Examination Questionnaire; SATAQ-4 = Sociocultural Attitudes Towards Appearance Questionnaire-Thin-ideal internalization Subscale, 4th Edition.
Discussion
Previous research has documented a strong link between perceived discrimination and disordered eating risk (Mason et al., 2021). The current study builds on this finding by examining how resources that are acquired in both social (i.e., perceived social support) and personal contexts of risk and resilience (i.e., thin-ideal internalization and ethnic identity) may influence such relationships in a cross-sectional sample of 296 ethnic minority women. Surprisingly, perceived social support did not mediate the relation between perceived discrimination and eating disorder symptomatology; in fact, a positive relation was observed between perceived social support and disordered and negative emotional eating. Significant interaction effects were observed for thin-ideal internalization moderating the relation between perceived discrimination and negative emotional eating, as well as ethnic identity moderating the relation between perceived discrimination and disordered eating. Exploratory analyses revealed thin-ideal internalization moderated the relation between perceived discrimination and negative emotional eating in Latine women. Overall, findings suggest ethnic minority women have personal resources that may influence the strength of relationship between perceived discrimination on eating pathology.
Significant differences were observed in racial/ethnic minority groups across constructs of interest. In terms of eating pathology, Black women reported significantly greater negative emotional eating than both Latine and Asian women, whereas there were no significant differences in global disordered eating. These findings pair interestingly with previous studies that have examined racial/ethnic differences in eating pathology, which suggests that Black women experience lower dietary restraint and shape/weight overevaluation than their White counterparts (Burke et al., 2021). Other studies have found mixed results in heterogeneity among emotional eating across ethnic minority groups (we need to cite this). Nonetheless, Black women scored significantly higher on negative emotional eating, which may be due to distress with the ‘Strong Black Woman’ stereotype as previously mentioned. Golbolt and colleagues (2022) found that in a semi-structured interview with 11 Black college-aged women, disorganized eating patterns were associated with emotional stress of being labeled a ‘Strong Black Woman’. As such, Black women may experience greater eating to cope with stress (e.g., emotional eating, overeating) rather than dietary restraint. In summation, there are mixed results in terms of disordered and emotional eating across racial/ethnic minority groups, and these present data lends to that notion. In terms of disordered eating, EDE-Q global scores in Black, Asian, and Latine women (M = 4.77, 4.79, and 4.90, respectively) were above the <4.0 clinical cutoff. This may be due to a ceiling effect produced by potential issues in construct validity in capturing the full spectrum of disordered eating behavior, cognitions, and attitudes in minoritized women, which may produce elevated scores (Kelly et al., 2012; Nagata et al., 2018). However, Meule & colleagues (2021) recommend not using cut-off scores altogether, such as in underrepresented groups in eating disorder research (e.g., ethnic minorities), as their eating, shape, and weight concerns bound my certain cultural expectations or norms may not be reflected on the EDE-Q (Alexander et al., 2024; Kalantzis et al., 2024). Lastly, elevated scores may be due to genuine severity in eating disorder behaviors, cognitions, and attitudes, as clinical status was not examined in the current sample, such as a previous or current diagnosis of an eating disorder.
Black women also scored significantly higher on perceived discrimination than both Latine and Asian women; these data align with epidemiological studies that suggest greater prevalence of discrimination due to systemic racism in Black than both Latinx, Asian, and mixed-race individuals (Harris et al., 2006; Whitcomb et al., 2021). However, it is important to note that perceived discrimination was measured globally, and not regarding their racial/ethnic identity, per say (See Limitations and Future Directions), which may implicate the differences in reporting perceived discrimination. Lastly, Asian women reported significantly greater ethnic identity than both Black and Latine Women. These data contrast previous work examining racial/ethnic differences in ethnic identity affirmation, which greater ethnic identity affirmation was Black American college students in comparison to Asian and Latinx college students (Brittian et al., 2013). However, these analyses were not separated out by gender identity. As such, it is possible that there are both gender and racial differences in ethnic identity affirmation. Lastly, there were surprisingly no significant differences in thin-ideal internalization across racial groups, contrasting previous findings suggesting differing idealized internalizations across ethnic minority groups (Burke et al., 2021), such that Black Women endorse significantly less thin-ideal internalization than Asian and Latine Women. However, recent qualitative studies examining sociocultural pressures in Black Women reveal that desire for a thinner body type may be more prevalent in Black Women who are socialized in White dominated social settings, which may contribute to more similar levels of thin-ideal internalization to other ethnic minority groups who have similar thin-ideal pressures (e.g., Asian Women) (Watson et al., 2019). Lastly, BMI was not related to any of the constructs of interest. Given the emerging evidence that BMI, particularly self-report, may not be predictive of various physical and mental health problems in ethnic minority populations (Wagner & Heyward, 2000) as well as different proportions of fat mass to lean muscle mass (Duerenberg et al., 1998). All in all, these data suggest that Black, Asian, and Latine Women may have heterogeneous experiences with ethnic identity, discrimination, and emotional eating, which lend to the importance of examining these groups distinctly in the eating disorder literature.
In terms of the first research question, social support did not mediate the relation between perceived discrimination and eating outcomes, countering previous studies utilizing stress-process with other varying health outcomes (Kim et al., 2015). It is possible that the type of perceived social support may be key in coping with discriminatory events, such as in-group social support. In a study conducted by Marshburn and colleagues (2022) on African Americans, findings revealed that participants reported more emotional closeness to Black friends and non-Black friends of color relative to White friends. Since racial/ethnic background of perceived social support was not evaluated, it is possible that individuals who experienced high amounts of perceived discrimination receive outgroup perceived social support, to which sufficient emotional support may not be met. Thus, more severe outcomes in eating pathology might be observed. In relation to Johnson & colleagues (2022), a small, negative relationship was found between social support and binge eating, which counter our current findings (i.e., a positive relationship between social support and eating pathology). However, social support was found to be an insignificant predictor of the relation between perceived discrimination and binge eating, which aligns with the insignificant findings. Overall, the relationship between social support and eating disorders varies and may depend on a myriad of factors, such as remission of an eating disorder (Kim et al., 2023). As such, participants may have social support that simultaneously places pressure on appearance ideals (e.g., thin-ideal internalization), which then may lead to greater eating pathology overall. Overall, perceived social support should be a continued pursuit within underrepresented groups in eating disorder research, particularly examining in-group versus out-group, as well as facets of social support.
Our hypotheses about ethnic identity were partially supported. While no moderation effects were present, these data suggest a negative relationship between ethnic identity and eating pathology, such that greater ethnic identity is related to lower disordered and negative emotional eating (Rakhkovskaya & Warren, 2014). These findings align with previous literature suggesting ethnic/racial identity, particularly affirmation, as a protective factor on mental health outcomes broadly (Vines et al., 2017) and eating pathology, specifically (Rodgers et al., 2018). In terms of bivariate correlates, ethnic identity was negatively related to social support, such as greater levels of ethnic identity affirmation were related to less social support. These findings contrast previous studies, which have found a positive link between ethnic identity socialization and parental social support (Hughes et al., 2006). To that end, it is possible that social support from in-group versus out-group differently relates to one’s ethnic identity. Additionally, greater levels of ethnic identity were related to less perceived discrimination, which supports previous data that found negative associations between ethnic identity affirmation and perceived discrimination (Atari & Han, 2018). Furthermore, it is possible that ethnic identity affirmation buffers against the psychological distress associated with perceived discrimination (Ahemed et al., 2011). Overall, ethnic identity affirmation may be a salient construct in examining its relations with discrimination and mental health outcomes in ethnic minority women.
Internalizing the thin ideal strengthened the relationship between perceived discrimination and eating pathology, which was consistent with our hypothesis. Moreover, participants with high levels of thin-ideal internalization reported a stronger relation between perceived discrimination and negative emotional eating than those with average and low levels of thin-ideal internalization. This finding aligns with previous literature, which suggests thin-ideal internalization is a risk factor for developing eating pathology (Wang et al., 2020). Although thin-ideal internalization was associated with a greater risk for negative emotional eating, there was a non-significant relationship between thin-ideal internalization and disordered eating. It is possible that the relation between perceived discrimination and disordered eating may be strengthened by more generalized body dissatisfaction (Cohrdes et al., 2021) or other body image-related constructs, as opposed to internalizing the thin ideal in racial minority Women.
Lastly, exploratory aims were generated based upon each racial/ethnic group’s cultural norm about body image. More specifically Latine and Black Women value internalizing curvier or ‘thicker’ bodies whereas Asian Women may internalize the thin-ideal (Damstetter & Vashi, 2015; Awad et al., 2015). Findings showed that thin-ideal internalization did not moderate relationships between perceived discrimination and eating disorder symptomatology among Black and Asian Women. Additionally, thin-ideal internalization did not moderate the relationship between perceived discrimination and disordered eating among Latine Women. However, among Latine Women, thin-ideal internalization strengthened the relationship between perceived discrimination and negative emotional eating. Interestingly, although thin-ideal internalization was not associated with negative emotional eating in the overall sample, it was in the sample of Latine Women, such that greater levels of negative emotional eating was related to greater levels of thin-ideal internalization. It is possible that thin-ideal internalization is a risk factor for negative emotional eating in Latine women.
Limitations
The present study does not go without limitations. Firstly, these data were collected utilizing MTurk, which has been historically known to threaten validity. To minimize these concerns, several recommendations were followed (Aguinis et al., 2021). Nevertheless, results should still be interpreted with the recruitment method in mind. It is important to note that Burnette (2022) raises significant concerns in using MTurk as a data collection method for eating disorder research. However, a response to Burnette (2022) outlined methodology to curb these concerns (e.g., add CAPTCHA, exclude responses from the same IP address) that prevent participants who use commercial data centers to complete multiple surveys for financial gain. It is noted that both methods were used in the current study. Secondly, these data were cross-sectional, and several models were run, which increased the chances of a Type-I error; however, it is important to note that multiple corrections were made to reduce this risk. Temporal precedence was not determined; thus, inference on temporal patterns or causality cannot be made. Future research should examine the mechanisms of these relations longitudinally. In addition, the current study did not assess a myriad of other marginalized identities (e.g., gender identity) and experiences that could potentially impact these relationships. Future studies should examine stress-process models of these constructs under the framework of gender diversity, as intersecting, minoritized identities (e.g., Transgender Black Women), may experience elevated discrimination (Jefferson et al., 2013). Additionally, we utilized a force-choice for race/ethnicity in order to examine group differences across group differences. As such, individuals who identify as mixed-race and/or identify with intersectional racial/ethnic identities (e.g., Afro-Latine) were not fully captured in these results. Future research should attenuate to including multiracial individuals, who may experience mixed-messaging of appearance-related pressures (Sims, 2012), as well as examine Arab/Middle Eastern Americans, who may also be at risk for disordered eating (Kalantzis et al., 2024). Being able to read and/or write fluently in English was also a requirement. As such, recent immigrants to the United States may not have been represented in these data. Future work should establish these relations in non-Western cultures, as well as people who recently immigrated to the United Staes. Also, the present study examined perceived discrimination globally, and not perceived racism per se. It is possible that participants reported unfair treatment/discrimination due to other marginalized identities. For example, given the strong, positive relation between weight status and global discrimination (Jackson et al., 2014), it is possible that participants in a larger body were reporting discrimination deriving from their weight-status marginalization, and not their racial/ethnic status, per say. Social support was also measured globally and was positively associated with eating pathology. To that end, future research should capture specific facets of social support (e.g., minoritized vs. majority support, in vs. out group support) and their relation to eating pathology outcomes, as varying types of social support may implicate eating disorder outcomes differently (Leonidas et al., 2014). Lastly, future studies should integrate more elements from the tripartite influence model (e.g., appearance comparisons, body dissatisfaction) in tandem with minority stress theory (e.g., in-group discrimination) in ethnic minority women.
Conclusion
Egbert and colleagues (2022) showed that, when race and ethnicity data were reported, white participants comprised approximately 70% of the samples described in the International Journal of Eating Disorders. The present study extends previous theoretical work, with a focus on ethnic/racial minority Women, to examine how the relationship between perceived discrimination and eating pathology is mitigated by various personal and social resources. The current study adds to the body of evidence that thin-ideal ideal may serve as a protective factor on the relation between perceived discrimination and disordered eating in ethnic minority Women. Overall, perceived discrimination had a strong, positive relation to eating disorder symptomology regardless of level of thin-ideal internalization. Higher levels of perceived social support were associated with greater levels of eating pathology. These data should be considered for clinicians and practitioners working with ethnically diverse Women, particularly to assess these populations’ levels of perceived social support, internalization of the thin ideal, and ethnic identity in relation to eating disorder symptoms. Particularly, clinicians should consider inquiring about individuals’ unique experiences with their culture’s body standards, as well as how strongly they identify and/or are affirmed in their ethnic identity.
Footnotes
Author Contributions
Maria A. Kalantzis (
Abby L. Braden (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
All data, materials, and code are available upon request.