
Abstract
Theoretically, home practice of mindfulness is a critical mechanism underlying the benefits of mindfulness-based intervention (MBI), but rates of adherence to home practice recommendations are low for youth participants in MBI. In the current study, we test the extent to which the first supplement delivered via cellphone to an MBI increases rates of home practice, and to what extent home practice mediates condition differences in key outcomes (mindful attention, psychological distress, depressive symptoms, and difficulties in emotion regulation). Participants were 59 university students who attended at least one session of a 6-week MBI and completed daily diaries assessing home practice and outcomes. Participants were randomly assigned to receive varying intervention support between sessions; we compared those who received no support to those who received support. Results indicated that those who received the MBI plus multi-modal adaptive supplement in daily life reported significantly higher rates of home practice, relative to those who received only the MBI. In addition, there were indirect effects of condition on mindful attention, psychological distress, depressive symptoms, and emotion regulation difficulties through home practice. This study provides preliminary evidence that incorporating supplements to MBI may increase intervention effectiveness by supporting and boosting home practice of mindfulness.
Although mindfulness-based interventions (MBIs) are effective for promoting mental health for young adults, effects are relatively small (Zoogman et al., 2014). One of the best predictors of improvements in well-being during an MBI is the degree to which mindfulness is practiced at home between group sessions (Birtwell et al., 2019; Frank et al., 2021); however, for adolescent and young adult participants in MBIs, rates of home practice are dramatically below recommendations (Quach et al., 2017). Theoretically, technological supplements (e.g., messages with intervention content delivered via cell phone) to MBIs that provide “just-in-time” support during daily life may promote home mindfulness practice, and as a result, bolster intervention effects (Lucas-Thompson et al., 2019). Emerging evidence evaluating the first group-based MBI with a multi-modal adaptive supplement (Lucas-Thompson et al., 2020) relative to a traditional group MBI suggests that young adults randomized to receive the supplemental elements had greater pre-post change in mindful attention and smaller pre-post increases in mental health symptoms (Lucas-Thompson et al., 2023). However, it is unclear what mechanisms drive these condition differences. It was the goal of the current study to evaluate the extent to which the benefits of the supplemented MBI relative to a traditional MBI are mediated by greater rates of home practice.
MBI, Mental Health, and Home Practice
There is a growing evidence base supporting the efficacy of MBIs aimed at adolescents and young adults for promoting mental health. Theoretically, MBIs are particularly effective because they dually support both top-down regulatory processes, such as attention allocation and emotion regulation, as well as bottom-up arousal processes, such as physiological stress responding (Davis & Hayes, 2011). In fact, meta-analytic evidence indicates that these interventions are effective for reducing problems with psychological distress (e.g., depression, anxiety, and stress) for adolescents and young adults (Dawson et al., 2020; Greeson et al., 2014; Miller et al., 1995; Zoogman et al., 2014). Although meta-analytic estimates of the effect sizes for MBIs in adult participants are moderate to large (Khoury et al., 2015), overall effects in younger participants are relatively small (Dawson et al., 2020; Zoogman et al., 2014).
Evidence evaluating the extent to which adolescent and young adult participants in an MBI adhere to home practice recommendations provides a possible explanation for these relatively weaker effects. A robust predictor of improvements from before to after an MBI is the amount of time that participants spend engaging in mindfulness practices between sessions (Goldberg et al., 2020; Lloyd et al., 2018), with both formal (i.e., time intentionally set aside for a longer practice) and informal (e.g., mindfully noticing sensations, thoughts, and feelings across the day) mindfulness practice being important (Birtwell et al., 2019). More specifically, there is evidence that practicing mindfulness increases levels of mindfulness, which then predict improvements in psychological functioning (Carmody & Baer, 2008).
Many MBI curricula encourage participants to establish a consistent mindfulness practice, in order to experience the benefits of mindfulness, and typically provide a specific set of instructions to participants for home practice between sessions (Broderick, 2013; Kabat-Zinn, 1990). However, MBI curricula vary dramatically in terms of what resources are actually provided to participants to support establishing a home practice (Lloyd et al., 2018), and many MBIs provide no structured resources beyond recordings and/or workbooks that participants can use (Broderick & Metz, 2009; Lloyd et al., 2018). In fact, many provide no structured resources, and simply recommend that participants practice at home between sessions. And, MBI participants report that they forget about home practice recommendations – both that they are supposed to practice and what they are supposed to practice (Lucas-Thompson et al., 2020) – between group sessions. Although adult MBI participants are relatively compliant with home practices recommendations (Brintz et al., 2024; Ribeiro et al., 2018), adolescent and young adult participants are not: some estimates suggest adolescent and young adult participants in MBI complete only about 25% of the recommended home practices (Quach et al., 2017). Therefore, efforts to increase home practice for adolescent and young adult participants in an MBI are needed, and if successful, should boost intervention effects.
The Role of Technological Supplements to MBI
Outside of the MBI literature, there is strong evidence for the benefits of just-in-time adaptive interventions as supplements to traditional behavioral interventions. Benefits are driven by delivering intervention content in daily life, tailoring it to individuals, and targeting moments of high need (Smyth & Heron, 2016). These intervention elements can be delivered via text message or smartphone applications, and in general are well-liked by participants (Heron & Smyth, 2010). Overall, there is evidence that they promote skill transfer from an intervention to daily life and, as a result, boost intervention effects (Heron & Smyth, 2010; Smyth & Heron, 2016), particularly if they are integrated with other intervention elements (e.g., a group-based intervention) rather than used as a stand-alone intervention (Heron & Smyth, 2010).
However, these adaptive interventions have not historically been incorporated into MBIs. To fill this gap, we developed the first multi-modal adaptive supplement to an MBI (Lucas-Thompson et al., 2020). This supplement was designed based on an MBI for adolescents, Learning to BREATHE (L2B; Broderick & Metz, 2009) which has been implemented successfully in populations that vary based on age, including in university students (e.g., Mahfouz et al., 2018), most of whom are young adults. Rooted in the philosophy of mindfulness-based stress reduction (Kabat-Zinn, 1990), L2B is well-liked by participants, and predicts reductions in symptoms of depression and stress in adolescent and young adult samples (Bai et al., 2020; Broderick & Metz, 2009; Dvořáková et al., 2017; Eva & Thayer, 2017; Felver et al., 2019; Frank et al., 2021; Fung et al., 2019; Tang et al., 2020).
We created the supplemented MBI, Learning to BREATHE PLUS (L2B PLUS; Lucas-Thompson et al., 2020) to provide support between sessions of L2B. One key goal of L2B PLUS is to promote the establishment of a consistent daily home practice (Lucas-Thompson et al., 2020). In particular, intervention content is delivered throughout the day to promote home practice (e.g., 5 short messages a day, each day other than the day of the intervention meeting). Messages were designed to support both formal and informal mindfulness practices throughout the day. As noted, participants in an MBI report forgetting about home practice between sessions (Lucas-Thompson et al., 2020).
In addition, the behavior change literature indicates that two critical and modifiable predictors of behavior change are motivation to change and self-efficacy for making change (Fisher et al., 2003). For instance, low levels of motivation and/or self-efficacy (i.e., beliefs about one’s own ability to engage in a behavior or meet a goal) are major roadblocks to engaging in behavior change (e.g., establishing a mindfulness practice). However, theoretically, the information-motivation-behavioral (IMB) model that has been widely applied to behavior change emphasizes that motivation and self-efficacy can be increased, and that doing so is critical for creating and also maintaining behavior change (J. D. Fisher & Fisher, 1992; W. A. Fisher et al., 2003); empirically, there is meta-analytic evidence that the IMB model is a good theoretical framework for developing behavioral interventions (Chang et al., 2014). Other theoretical accounts for the mechanisms underlying behavior change similarly emphasize the importance of motivation and self-efficacy. For instance, authors of a recent systematic review of behavior change literature concluded that approach motivation (i.e., towards positive and pleasurable experiences) is a critical factor that underlies individual behavior change, at least until the behavior change has been established (Michaelsen & Esch, 2023); similarly, the health belief model frames self-efficacy as a key cognitive construct underlying health-relevant behavior change (Orji et al., 2012). Theoretical accounts of behavior change in the context of mindfulness have similarly emphasized motivation and self-efficacy, and the importance of applying lessons learned from the broader behavior change literature to the practice of helping individuals to establish a mindfulness practice (Schuman-Olivier et al., 2020). In terms of self-efficacy, positively framed messages are most effective at increasing self-efficacy (Egbert & Omosun, 2017). Therefore, the categories of messages included in L2B PLUS are (1) reminders of what was learned in the last group session and what to practice, (2) messages to increase motivation to practice mindfulness, which emphasize the benefits of regular mindfulness practice, and (3) positively-framed messages to support self-efficacy by emphasizing that participants already have the skills they need to establish a regular mindfulness practice.
Importantly, an initial pilot randomized controlled trial in young adults (the same as utilized in the current study) suggests that, relative to the traditional L2B program, L2B PLUS predicts greater pre-post increases in mindful attention and smaller pre-post increases in mental health symptoms (Lucas-Thompson et al., 2023). Although this evidence is promising, it is empirically unclear what mechanisms underlie outcome differences between L2B PLUS and L2B. As consistent home practice is a theoretical mechanism underlying the benefits of MBI (Lloyd et al., 2018; Vettese et al., 2009), and L2B PLUS was designed to increase rates of home practice, the goal of the current study was to investigate the extent to which differences in home practice mediate these condition differences.
The Current Study
Home practice is an important predictor of improvements in outcomes during an MBI (Lloyd et al., 2018), but rates of compliance with home practice recommendations are very low (Quach et al., 2017). L2B PLUS (Lucas-Thompson et al., 2020) was designed to supplement a traditional group-based MBI (L2B) and, in part, promote home practice by providing intervention content to remind participants about home practice, motivate them to engage in home practice, and encourage self-efficacy for building a new mindfulness habit. L2B PLUS predicts greater benefits for young adult participants in terms of mindfulness and mental health (Lucas-Thompson et al., 2023), but it is unclear the extent to which differences in home practice mediate these condition differences. The goal of the current study was to fill this gap in the literature, by examining daily home practice as a mediator of L2B PLUS vs. L2B differences in mindful attention, psychological distress, depressive symptoms, and emotion regulation. The initial investigation of the benefits of L2B PLUS relative to L2B focused on pre- to post-intervention changes in key outcomes (Lucas-Thompson et al., 2023). In the current study, we focus on testing mediation in the context of intensive repeated measurements, as participants reported home practice, as well as mindful attention, psychological distress, depressive symptoms, and emotion regulation, each day of the intervention period in a daily diary. In addition, given the importance of consistency of home practice to theoretical benefits of mindfulness (Kabat-Zinn, 1990), we utilized these intensive repeated measurements to examine condition differences in consistency (versus erraticism) of home practice.
Method
Participants
Participants were college students enrolled in a midwestern university in the United States who attended at least one session of a six-week MBI (n = 62) and who completed daily dairies over the course of the intervention period (n = 59), because it was at group meeting sessions that participants were provided with the software and instructions to complete daily diaries, the primary measurement strategy for the current study. On average, participants were 21.12 years old (SD = 4.38; range 18-42 years old; 85% were between 18–25 years old). In addition, the sample was predominantly female (71% of those who reported gender; also, 23% male, 3% non-binary, and 2% gender fluid/queer) and non-Hispanic White (73% of those who reported race/ethnicity; also, 2% Native American, 11% Asian/Pacific Islander, 3% Black, 14% Hispanic/Latino, and 3% self-identified an “other” racial/ethnic identity). Finally, participants reported an average annual household income of $65,000-$75,000.
Procedure
All procedures were reviewed and approved by the Colorado State University institutional review board. Participants were recruited through class lists, as well as the university counseling center. Those who were interested completed an online screener to determine eligibility; eligible participants were those who reported experiencing stress and/or anxiety at least occasionally, and who owned a smartphone (see Figure 1 for CONSORT table). Eligible participants then received more detail about the study over email and, if still interested, in a phone call with study staff. After providing informed consent, participants then completed baseline assessments, and then were randomly assigned to conditions that received varying elements of L2B vs. L2B PLUS: (1) L2B only, (2) L2B + online library of practices (conditions 1 and 2 were combined because of limited use of the online library by those who had access to it); (3) L2B + intervention messages; (4) L2B + just-in-time stress supports (intervention content tailored to people’s current experiences); or (5) full L2B PLUS (library, intervention text messages, and just-in-time stress support). The initial investigation of L2B PLUS focused primarily on conditions 1 + 2 (traditional L2B) versus the other three conditions (L2B PLUS), but also provided evidence for similar patterns of pre-post change in outcomes between conditions 3, 4, and 5 (masked for review). Therefore, in the current study, we also focused on L2B (conditions 1 and 2) versus L2B PLUS (conditions 3-5), consistent with past research and also to maximize power. Participants attended group sessions (not stratified by condition, that is, participants assigned to multiple conditions were in group together) held via video conference for 1–1.5 hours, for each of the six sessions of L2B (Broderick, 2013). Intervention and assessment by study condition & CONSORT table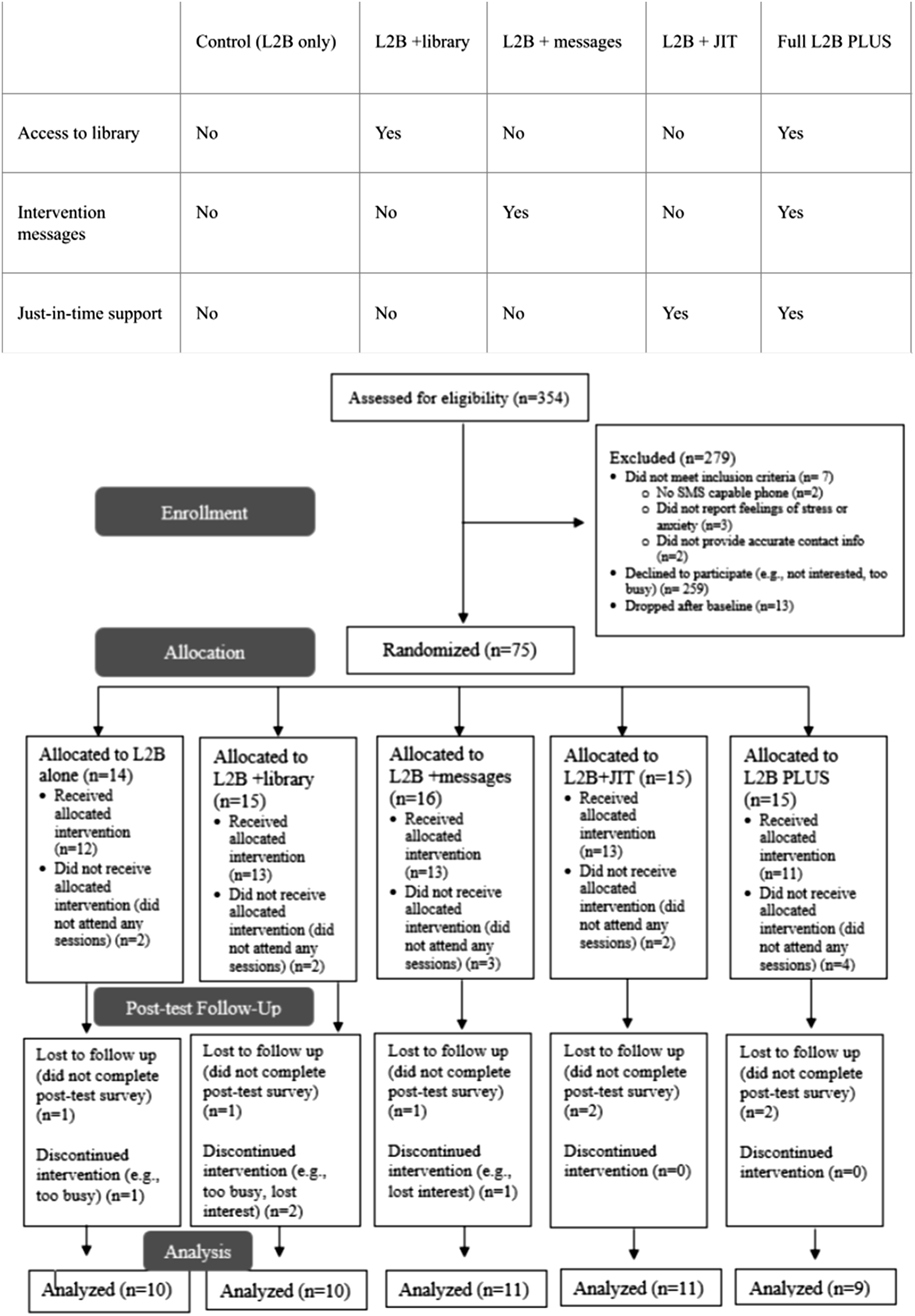
L2B PLUS intervention elements as well as daily diaries were delivered/collected via TigerAware (a mobile phone application) (Morrison et al., 2018a; 2018b), on all days of the week except the day on which the L2B group session occurred. Participants in conditions 3 and 5 received intervention messages 5 times per day, with no two being the same (for a total of 150 unique messages across the intervention period). There were three different types of messages, all of which were based around the previous week’s L2B theme. The first message category focused on reminders of key messages of the previous week’s L2B theme, as well as what to practice (e.g., “You can bring your attention back to the present moment any time by focusing on your body or your breath.”). The second message category focused on motivational content, reminding users of reasons they might benefit from home practice of mindfulness (e.g., “Noticing how your body feels can help you be aware of stress before it is overwhelming”). The third and final message category focused on supporting self-efficacy, reminding users that they already have all of the necessary skills to establish a regular mindfulness practice (e.g., “Now that you know how to do a body scan, you have the skills to focus and recenter whenever you need to.”). Then, participants in conditions 4 and 5 received two ecological momentary assessments of levels of stress and mindful attention each day. When participants reported low levels of mindful attention (i.e., levels of 5 or lower on a scale from 1 = not at all mindful to 10 = very mindful) or high levels of stress (i.e., levels of 6 or greater on a scale from 1 = not at all stressed to 10 = very stressed), they received a brief message designed to support practicing mindfulness, particularly during stressful periods (e.g., “You’re going through a lot. Where do you feel it in your body? Noticing the way our body feels is practicing mindfulness.”). Like the intervention messages, these just-in-time support messages were specific to the content that participants had just covered in the previous week’s L2B group session.
Measures
Primary measures were drawn from daily diaries sent to participants in all conditions each day of the intervention period.
Data Analytic Plan
Descriptive Statistics for Key Study Variables
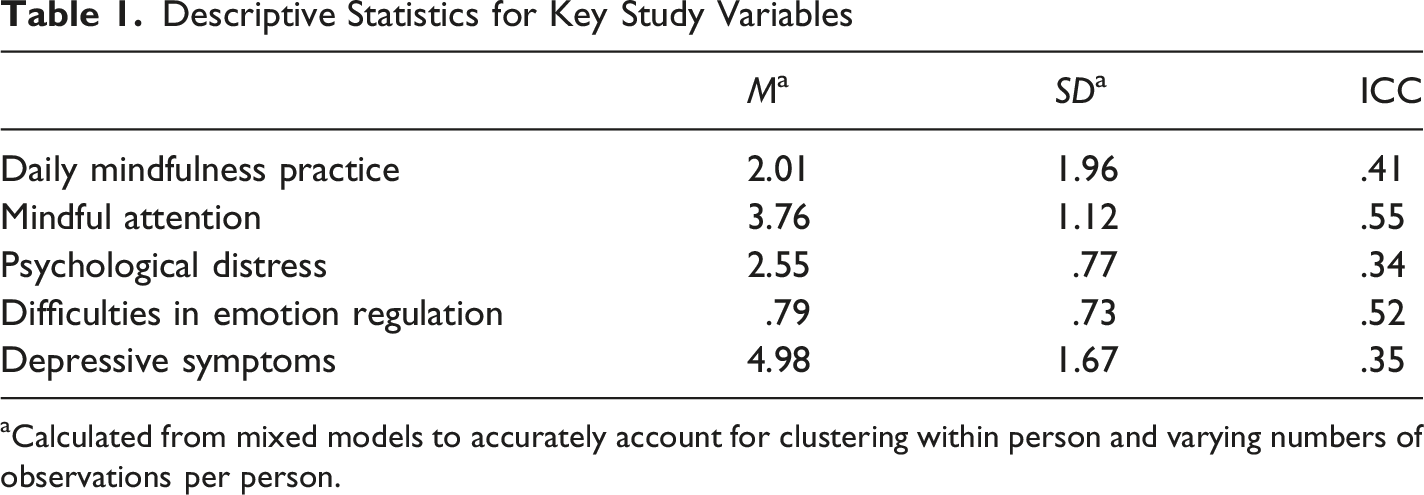
aCalculated from mixed models to accurately account for clustering within person and varying numbers of observations per person.
Next, we tested for baseline equivalence in outcomes (mindful attention, psychological distress, and difficulties in emotion regulation) based on condition using ANOVAs; when there were baseline differences in these variables, we included them as covariates in our final models.
To test our primary hypotheses, we first estimated direct effects of condition (L2B PLUS vs. L2B alone) on the mediator (daily mindfulness practice) and each of the dependent variables (levels of mindful attention, psychological distress, difficulties with emotion regulation, and depressive symptoms) in mixed effects models in Stata 15. Then, we ran cross-level mediation models to estimate the indirect effects of condition on outcomes through daily mindfulness practice. In Krull & MacKinnon’s terminology (Krull & MacKinnon, 2001), we specifically conducted a 2→1→1 mediation model, as we estimated the indirect effects of a level 2 effect (condition) on level 1 variables (mindfulness, psychological distress, and depressive symptoms) through a level 1 variable (mindfulness practice). We used the ml_mediation package (Ender, 2014) in Stata 15 to estimate indirect effects. Because this research question was focused on condition differences (a time-invariant, between-person variable), the raw values of scores on the mediator and dependent variable across all assessments were utilized in these analyses (i.e., raw values were not decomposed into between-person and within-person elements). In addition, we ran heterogeneous mixed-effects location scale models (Hedeker et al., 2009) using MIXREGLS (Hedeker & Nordgren, 2013) to model not just random intercepts (mean associations, or ‘location’) but also random variances both between (heterogeneity) and within (erraticism) people (‘scale’).
Although we focused on L2B versus L2B PLUS differences, we conducted supplementary analyses to examine potential difference in practice and outcomes based on original condition (L2B, L2B + text messages, L2B + just-in-time support (JIT), and L2B + texts + JIT) using the same analytic strategy discussed above.
Results
Means and standard deviations of key variables are presented in Table 1. Fifty-nine participants contributed a total of 1250 daily diaries, with an average of 21.2 observations provided by each participant (range: 1–52). Across those 1250 days of daily diaries, 16% included reports of no home practice of mindfulness, 30% of one mindfulness practice, 25% of two mindfulness practices, and the remaining 29% of more than two mindfulness practices that day. There were no baseline differences in mindful attention (p = .43, ML2B = 3.23, SD L2B = 0.72; ML2BPLUS = 3.04, SD L2BPLUS = 0.72), psychological distress (p = .08, ML2B = 32.25, SD L2B = 3.99; ML2BPLUS = 31.07, SD L2BPLUS = 3.95), depressive symptoms (p = .47, ML2B = 43.75, SD L2B = 8.86; ML2BPLUS = 45.16, SD L2BPLUS = 7.31), or difficulties in emotion regulation (p = .55, ML2B = 2.98, SD L2B = 0.71; ML2BPLUS = 2.82, SD L2BPLUS = 0.63); therefore, we did not include baseline levels of these characteristics in our primary models.
There were significant differences in daily mindfulness practice across the intervention period between L2B PLUS versus L2B alone participants, such that L2B PLUS participants reported completing significantly more daily mindfulness practices than those in L2B alone (Figure 2, a paths). There were no direct effects of condition on mindful attention, psychological distress, difficulties in emotion regulation, or depressive symptoms (Figure 1, c’ paths). However, greater daily mindfulness practice was associated with significantly greater levels of mindful attention and significantly lower levels of psychological distress, difficulties in emotion regulation, and depressive symptoms (Figure 1, b paths). Finally, the indirect effects of condition on mindful attention, psychological distress, difficulties in emotion regulation, and depressive symptoms were all significant (Figure 1). Indirect effects of condition on outcomes through daily mindfulness practice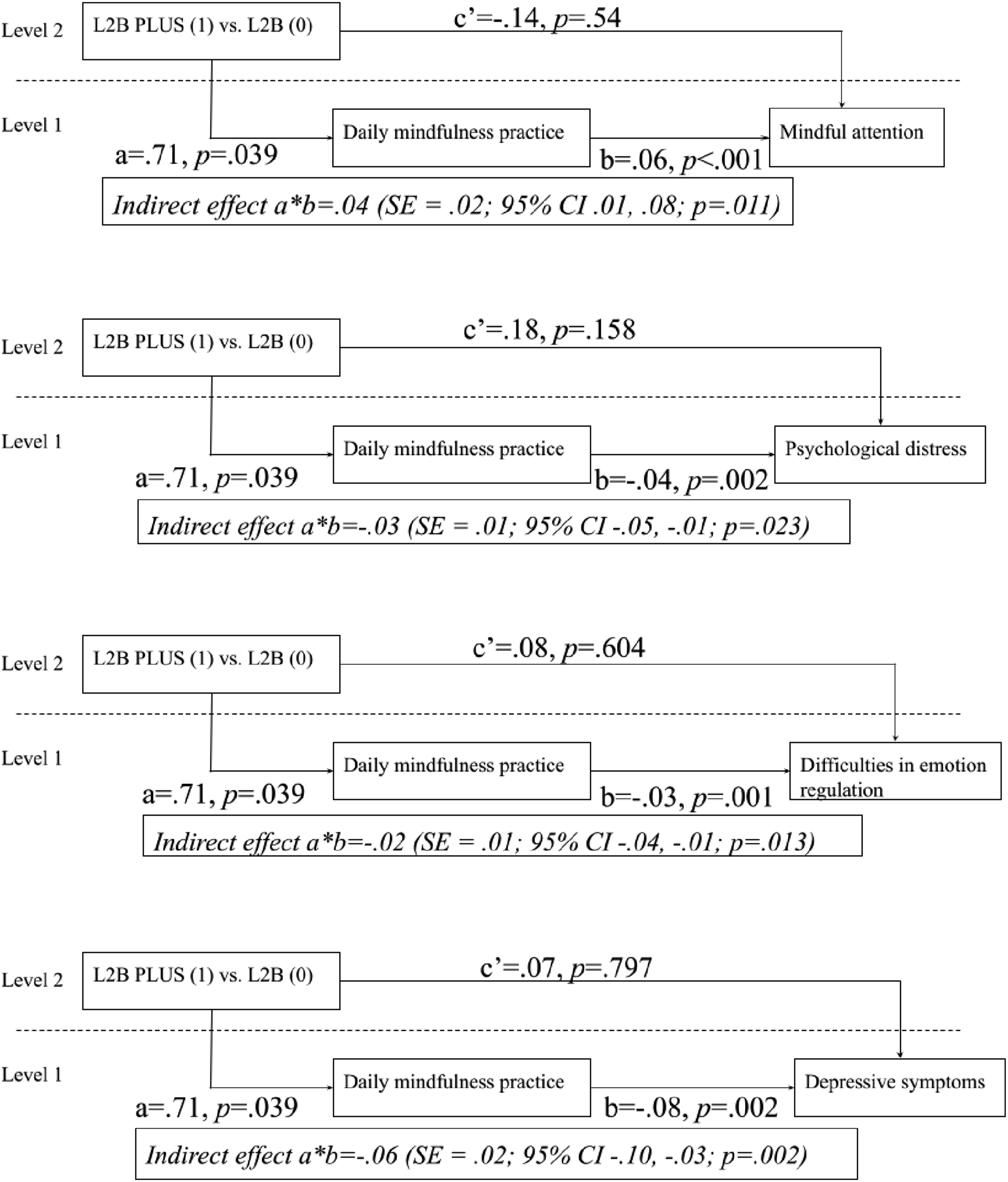
In addition, there were condition differences in not just the levels of daily mindfulness practice, but also variances. Of note, there was significant variability in the consistency of daily mindfulness practice (b = .43, SE = .10, p < .001), and participants who had higher mean rates of practice were significantly more erratic in their rates of practice (b = .82, SE = .07, p < .001). Although there were no significant condition differences in consistency of mindfulness practice (b = .18, SE = .17, p = .28), these location scale models indicated that participants in the L2B PLUS group were significantly more heterogeneous (i.e., dissimilar from each other) in their rates of daily mindfulness practice than those in the L2B alone group (b = 1.40, SE = .43, p < .001).
Supplementary Analyses
We conducted supplementary analyses to determine which specific combination of intervention messages and/or just-in-time support predicted daily mindfulness practice and outcomes. First, we found that there were no significant differences in daily practice between L2B + texts and L2B + texts + JIT relative to L2B alone (ps >.09). However, participants who received L2B + JIT practiced significantly more often than those in L2B alone (estimate = 1.24, SE = .42, p = .003). There were no significant direct effects of subcondition on mindful attention, psychological stress, depressive symptoms, or difficulties in emotion regulation (ps >.22). In addition, indirect effects from L2B + JIT (relative to the other groups) to practice to outcomes were all non-significant (ps > .26).
Discussion
The goal of the current study is to investigate the extent to which, relative to the standard group L2B, L2B PLUS multi-modal supplement increases rates of home practice, which then promote greater mindfulness as well as lower psychological distress, depressive symptoms, and difficulties with emotion regulation difficulties. Results indicated that, compared to participants in L2B alone, participants in L2B PLUS practiced significantly more but were also more dissimilar from each other in rates of practice, and that there were significant indirect effects of condition on outcomes through rates of daily practice. These results provide initial support both for the benefits of L2B PLUS for home practice as well as the benefits of home practice for mindfulness, mental health, and emotion regulation in the context of an MBI.
In the same sample as utilized for the current study, there is evidence that L2B PLUS predicts greater pre-post benefits for mindfulness and mental health than L2B alone (Lucas-Thompson et al., 2023). L2B PLUS was designed to increase rates of home practice (Lucas-Thompson et al., 2020), in part because of arguments that home practice is a mechanism underlying MBI benefits (Lloyd et al., 2018; Vettese et al., 2009), and that the amount of time participants engage in mindfulness during sessions predicts gains in outcomes during an MBI (Goldberg et al., 2020). The results of the current study suggest that providing support in daily life via reminders, motivational messages, self-efficacy messages, and/or just-in-time support for practicing mindfulness during stress increases rates of home practice relative to the standard group program without these resources.
In addition, the results of the current study are consistent with arguments that home practice is one mechanism underlying the benefits of MBI (Lloyd et al., 2018; Vettese et al., 2009) as well as evidence for pre-post benefits of L2B PLUS relative to L2B alone for mindfulness, mental health (Lucas-Thompson et al., 2023), and mindfulness stress buffering (Lucas-Thompson et al., 2024). There were significant indirect effects of condition on mindful attention, psychological distress, depressive symptoms, and difficulties in emotion regulation through rates of reported daily practice. A systematic review indicates that there is marked variability in the resources that are provided to MBI participants, and many MBIs provide no or very few structured resources (Lloyd et al., 2018). It is likely not surprising, then, that rates of compliance with home practice recommendations in MBI are often very low (Quach et al., 2017). Providing intervention content and just-in-time support in daily life seems to benefit target outcomes of MBI (mindfulness, mental health, and emotion regulation) through increases in home practice by providing these supports; essentially, L2B PLUS is likely supporting skill transfer from the group program to daily life better than L2B alone. This evidence for the benefits of this multi-modal supplement is also in keeping with the larger evidence that just-in-time adaptive elements promote skill transfer and, as a result, boost intervention effects (Heron & Smyth, 2010; Smyth & Heron, 2016).
Interestingly, though, participants in the L2B PLUS condition were more heterogeneous (i.e., dissimilar from each other) in their rates of daily practice than were those in the L2B condition. There weren’t significant condition differences in erraticism, suggesting that L2B PLUS participants had higher but similarly inconsistent levels of practice as those in L2B alone. Together, these findings suggest that there is additional work to do to refine L2B PLUS to support a consistent mindfulness practice from day to day; it is also possible that rates of home practice are inconsistent, in part, because we measured practice during the early stages of habit formation. For instance, it can take several months to establish a new habit (Wood, 2019). It will be critical for future research to examine condition differences in consistent mindfulness practice over a longer period of time, during potential habit maintenance rather than formation. Also, the greater heterogeneity in the L2B PLUS vs. L2B alone condition suggests that there are unique subgroups of individuals who respond differently to the L2B PLUS intervention components, a possibility that should be explored in future research. A key benefit of just-in-time adaptive interventions is the tailoring of intervention content to individuals (Guan et al., 2024; Smyth & Heron, 2016); therefore, future research should aim to better understand the heterogeneity in mindfulness practice in this group to inform appropriate and effective tailoring of L2B PLUS to individuals. For instance, this pattern may reflect individual differences in responsiveness to the L2B PLUS intervention, differences which may be a function of genetic, physiological and/or psychological characteristics. The vantage sensitivity framework posits that differences in sensitivity to environmental stimuli may be at the root of individual differences in responses to psychological interventions (de Villiers et al., 2018). There is also evidence that dose-response relationships are moderated by the extent to which individuals engage with a health intervention (Lippke et al., 2016), and that both engagement in digital interventions and appraisals of intervention content are predicted by personality (Khwaja et al., 2021). Therefore, this greater heterogeneity in the L2B PLUS group could be caused by individual differences in responses to or engagement with the PLUS components, as well as individual differences in feelings about or reactions to the digital content that was delivered. An important step for future research is to evaluate the factors that underlie these group differences in heterogeneity in order to continue to refine the PLUS components.
An additional important area for future research to explore is the extent to which these differences in engagement and, therefore, outcomes are driven by particular components of the L2B PLUS intervention. Although not a focus of the current study, in part because of relatively small sample sizes in the individual PLUS sub-conditions, supplementary analyses did indicate that it was those in the L2B + JIT group who had significantly greater practice rates than those in L2B alone; there were no significant differences in practice between the other sub-conditions and L2B alone. However, the indirect effects from sub-condition to practice to outcomes were not significant. It is possible that this pattern reflects limited power to detect mediation given the small sub-condition cell sizes; it is also possible that it is the combination of JIT and intervention messages that has the strongest indirect effect from practice to outcome. This latter argument is in keeping with evidence that those randomized to the full PLUS program experienced greater decreases in mental health symptoms than those randomized to individual elements (Lucas-Thompson et al., 2023). However, that differences in practice relative to L2B alone were most evident in the group that received only JIT messages could reflect that participants benefit from the most from targeted support during stress, which is described by adolescents are being a primary underminer of mindfulness practice (Moran et al., 2026). In adolescent samples in particular, there is evidence that stressors predict lower levels of mindful attention (Lucas-Thompson et al., 2022, 2023, 2024). Adolescents in particular seem to struggle with mindfulness practice during stressful periods; thus, just-in-time support for practicing under stress should theoretically improve overall rates of home practice. However, those in the L2B + JIT group also received the fewest intervention prompts each day; therefore, it is also possible that this pattern suggests important information about an ideal daily dosage for PLUS intervention content, which other groups may exceed. Again, additional investigation in larger samples of the active ingredients of the PLUS program that is the most helpful for establishing a consistent daily practice routine will be important in future research.
Despite the practical and scientific contributions of the current findings, there are important limitations to note. First, the sample was relatively small, and lacked heterogeneity in race, ethnicity, and socioeconomic status; in addition, all participants were students at a university who self-enrolled in a mindfulness-based course described as targeting stress management. The latter characteristic of the current study likely reduces generalizability to adolescent populations who may have less intrinsic interest in mindfulness for stress management. It is important in future research to test differences in L2B PLUS and L2B in larger, more diverse samples, including in broader samples of adolescents, who have varying degrees of interest in or motivation to practice mindfulness. In addition, participants self-reported all primary outcomes for the current study. It is possible that part of the observed condition difference in home practice rates was due to demand characteristics, if L2B PLUS participants felt stronger pressure to report high rates of home practice than L2B participants. However, all participants received the same home practice messages at each group session of the intervention. In addition, rates of mindfulness practice were relatively low overall, suggesting that participants felt comfortable reporting low rates of practice in general. Nonetheless, the assessment of home practice was also a potential limitation of the current study, with a focus on overall number of mindfulness practices each day rather than other operationalizations, such as the minutes of time spent in practice, measuring practice separately by formal and informal mindfulness practice, and/or measuring the ways that people use mindfulness (Li et al., 2016). There is evidence that the amount of time that participants spend in both formal and informal mindfulness practice is important for overall program benefits (Birtwell et al., 2019; Goldberg et al., 2020), so it will be critical in future research to aim to replicate the findings in the current study using different and more nuanced measures of home practice.
In conclusion, the results of the current study add to the growing literature suggesting that the multi-modal supplement to L2B is an important extension to the traditional L2B, and that the delivery of intervention content and just-in-time support in daily life is translated into greater home practice, better gains in mindful attention, better mental health, fewer emotion regulation difficulties, and better abilities to remain mindful during stressful periods and thereby use mindfulness as a buffer against mental health challenges during stress (Lucas-Thompson et al., 2020, 2023, 2024). In addition, these results add to the literature about the role that home practice plays in MBI, and suggest that greater home practice is related to higher levels of mindful attention and lower levels of mental health problems and emotion regulation difficulties. Although it is important to replicate these results in larger, more diverse samples with more-nuanced assessments of home practice, these findings make an important contribution to the literature on the science and practice of MBI, and indicate that multi-modal supplements delivered in daily life will likely benefit program participants.
Footnotes
ORCID iDs
Ethical Considerations
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Colorado State University (protocol #1898).
Consent to Participate
Informed consent was obtained from all participants in the study.
Author Contributions
Conceptualization: 1-7; Methodology: 1, 8; Funding Acquisition: 1, 8; Project Administration: 1; Data Acquisition: 1, 2, 5; Analysis: 1; Writing – Original Draft Preparation: 1; Writing – Reviewing & Editing: 1-8.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by internal funding from Colorado State University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the first author upon request.
Clinical Trial Registration
This trial was not registered because of the pilot nature of this study.