
Abstract
Cluster B personality disorders, including Borderline, Histrionic, Narcissistic, and Antisocial personality disorders, collectively affect up to 5.5% of the population. These disorders are characterized by strong emotional responses; however, little research compares specific symptomatology with emotion regulation ability. The current study examines the relationship between subscales of the Difficulties in Emotion Regulation Scale and symptomatology across Cluster B disorders in a mixed non-clinical sample. In Study 1 (N = 325), participants completed self-report measures assessing emotion regulation and personality disorder symptoms. Primary findings showed that difficulties with emotion-related impulse control significantly predicted symptoms of all four Cluster B disorders, highlighting its importance in understanding these conditions. Study 2 (N = 530) was conducted to examine more specifically the different facets of impulsivity that are associated with these disorders. This study had participants complete self-report measures on emotion regulation, impulsivity, and personality disorder symptoms and found differential associations between facets of impulse control and Cluster B personality disorder symptoms. Impulse control difficulties also explain a large amount of variance in these disorders. These results suggest the necessity for targeted interventions focusing on impulse control and emotion regulation strategies to enhance treatment outcomes for individuals affected by Cluster B personality disorders.
Introduction
Cluster B Personality Disorders
The DSM-5-TR (APA, 2022) Cluster B personality disorders include Borderline, Histrionic, Narcissistic, and Antisocial personality disorders and up to 5.53% of the population is affected by at least one (Volkert et al., 2018). Borderline Personality Disorder (BPD) is defined by a strong fear of abandonment, chronic feelings of emptiness, and unstable relationships (American Psychiatric Association, 2022). Histrionic Personality Disorder (HPD) is characterized by attention-seeking behavior, shallow, quickly changing emotions, and a belief that relationships are closer than they are. Narcissistic Personality Disorder (NPD) is defined by a sense that oneself is superior to others, a need for constant praise and admiration, and fantasies about success and power. Antisocial Personality Disorder (ASPD) is characterized by a limited (or lack of) concern for others, a disregard for laws or social norms, and a lack of remorse for harmful actions (American Psychiatric Association, 2022).
Characterization of the four Cluster B disorders varies in important ways, but the disorders also share features. It is evident from their designation as the dramatic, erratic, or emotional disorders that Cluster B personality disorders are strongly associated with difficulties with emotion regulation (Kraus & Reynolds, 2001). These disorders are also some of the most difficult to treat and lead to some of the lowest success rates in treatment response; notably, even when pathology improves, residual personality and functional impairment often remain (Bond & Smith, 2023; Kraus & Reynolds, 2001; Leichsenring et al., 2024; Skodol, 2008). Because of these factors, further examining the emotion regulation issues that characterize the disorders can be instrumental in improving the prognosis of those affected.
Emotion Regulation and Cluster B
Emotion regulation is defined as the process of controlling one’s emotions, including when they are felt, and how they are experienced and expressed (Gross, 2014). These processes are typically goal-directed, as individuals frequently attempt to modify their emotional state to better align with situational demands or personal goals (Gross, 2015). One can change many aspects of an emotion, all of which are encompassed in emotion regulation. Namely, regulation may target the expression, duration, or intensity of one’s emotional response. A common conceptualization of emotion regulation characterizes difficulties across six domains: lack of awareness, defined as inattentiveness to one’s emotional responses; clarity of emotional responses, or difficulty identifying specific emotions; non-acceptance of emotional responses, or negative reactions to one’s own emotions; limited access to emotion regulation strategies perceived as effective; difficulties controlling impulses when experiencing negative emotions; and difficulties engaging in goal-directed behaviors when experiencing negative emotions (Gratz & Roemer, 2004).
Within the context of Cluster B personality disorders, emotion regulation is especially relevant. Notably, much of the research on emotion regulation and Cluster B has focused on BPD. Many of these studies suggest that BPD is linked to impulsivity and strong, unpredictable emotional responses (Chapman et al., 2008; Clarkin et al., 2004; Daurio & Taylor, 2022; Selby & Joiner, 2009). When delineating specific aspects of emotion regulation, a study by Glenn and Klonsky (2009) found that BPD was associated with a lack of access to emotional regulation strategies and difficulties with impulse control. However, despite the breadth of research demonstrating the link between emotion regulation and BPD, it is much sparser when it comes to the other Cluster B disorders. Some studies investigated the relationship between all personality disorders and emotion regulation and found difficulties with emotion regulation to be predictive of most personality disorders (Dimaggio et al., 2017; Garofalo et al., 2018).
When looking at specific dimensions of emotion regulation within Cluster B disorders, few studies have examined how different facets predict personality disorder symptomatology; however, certain studies have reported differential emotion regulation predictors for different Cluster B disorders (Borges & Naugle, 2017; Donahue et al., 2014; Glenn & Klonsky, 2009; Gratz et al., 2013; Marissen et al., 2012). BPD has been found to be associated with a lack of access to emotion regulation strategies and poor impulse control (Glenn & Klonsky, 2009), as well as clarity of emotions and control of behaviors when distressed (Gratz et al., 2013); psychopathic traits (many of which are found in ASPD) were found to be associated with a lack of clarity of emotions, a lack of access to emotion regulation strategies, difficulties with impulse control, and nonacceptance of emotional responses (Donahue et al., 2014); a study on NPD found patients to be worse at recognizing emotions (Marissen et al., 2012); and a study on personality disorders in general found all Cluster B personality disorders to be associated with difficulties engaging in goal-directed behavior when distressed (Borges & Naugle, 2017).
Impulsivity and Cluster B
Impulsivity has had numerous definitions over time, but recently it has begun to be examined as a dimensional concept, although those dimensions vary between different models of impulsivity (DeShong & Kurtz, 2013; Few et al., 2015; Lootens et al., 2017; Turner et al., 2017). The definition of impulsivity used here is consistent with the multidimensional theory presented by Whiteside et al. (2005), a five-factor model that seeks to consider personality in addition to pathology when characterizing impulsivity. This concept may be especially relevant in the context of Cluster B personality disorders as impulsivity is consistently shown to be one of the most significant predictors of some or all of these disorders (Chapman et al., 2008; Few et al., 2015; Fossati et al., 2007; Garofalo et al., 2018; Links et al., 1999; Looper & Paris, 2000; Lootens et al., 2017). However, much of this research centers on BPD and ASPD. While there is substantial research examining impulsivity and personality disorders in general, there is limited research comparing specific dimensions of impulsivity in different Cluster B personality disorders (Hahn et al., 2016; Lootens et al., 2017; Tragesser & Robinson, 2009). This research shows that BPD is strongly associated with urgency (Lootens et al., 2017; Tragesser & Robinson, 2009); however, Tragesser and Robinson (2009) found BPD to be most strongly associated with a lack of premeditation. One study (Hahn et al., 2016) found that BPD and ASPD are differential in their association with impulsivity factors and that negative urgency and lack of perseverance were associated with BPD, while sensation seeking and lack of premeditation were uniquely associated with ASPD.
Additionally, some prior work has demonstrated associations between impulsivity and Cluster B personality disorder symptoms using broad trait measures such as the Barratt Impulsiveness Scale (Garofalo et al., 2018); however, such measures do not differentiate between emotion-driven and non-emotional facets of impulsivity. Given that difficulties with emotion regulation have been demonstrated to be foundational to these disorders, it is likely that impulsive behaviors are often contextually and affectively driven, and that more specific assessment of impulsivity may be particularly informative.
Despite the wealth of research showing impulsivity is a central factor of Cluster B personality disorders, there are still inconsistencies in the facets of impulsivity associated with BPD and ASPD, and very little research examining this in HPD and NPD.
The Present Studies
Although a number of studies have examined relationships between emotional regulation, impulsivity, and Cluster B personality disorder symptoms, the present studies aimed to investigate these associations at a more finite level. Specifically, Study 1 aimed to investigate the relationship between different facets of emotion regulation and Cluster B personality disorder symptomatology in a non-clinical sample. Given the findings from Study 1, Study 2 sought to explore the relationship between different dimensions of impulsivity, facets of emotion regulation, and Cluster B personality disorder symptoms. These studies also used a large sample with a wide age range to expand upon previous research that has primarily focused on inpatient or undergraduate samples.
Study 1
Method
Participants
Participants were recruited via social media, word of mouth, an introductory psychology research group, and flyers in cities around the Northeastern United States. Four hundred and seven participants took the survey. There were three attention-check questions embedded in the survey. Participants were excluded from the analysis if they responded to more than one of the attention check questions incorrectly. This resulted in 83 participants being excluded from the sample and an overall sample of 325 participants for analysis. In Study 1, 24.3% of participants were recruited through the university research participant pool.
Participants were given the option to receive class credit (if they were students at the study’s university) or enter a raffle for one of four $25 gift cards. The mean age of participants was 28.55 (SD = 14.23) years, and the group identified as 39.4% male, 53.8% female, 3.4% nonbinary, 1.8% genderqueer, and 1.5% elected to self-describe their gender. Relevant to note is that some participants reported a prior diagnosis of a Cluster B personality disorder, totaling 5.8% of the sample. Specifically, 3.1% reported a prior BPD diagnosis, 1.5% reported an NPD diagnosis, 0.9% reported an HPD diagnosis, and 0.3% reported an ASPD diagnosis.
Measures
Difficulties in Emotion Regulation Scale
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) is a widely used self-report measure designed to assess emotion regulation problems across multiple dimensions. The DERS consists of 36 items that evaluate six subscales: non-acceptance of emotional responses, difficulties engaging in goal-directed behavior, impulse control difficulties, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional clarity. Items are rated on a scale from 1 (“almost never [0–10%]”) to 5 (“almost always [91–100%]”), with higher scores indicating greater difficulties in emotion regulation. Example items include “When I’m upset, I feel guilty for feeling that way” (non-acceptance) and “When I’m upset, I have difficulty concentrating” (goals). For the current study, the reliability of the DERS was assessed using Cronbach’s alpha and McDonald’s omega total (ωtot).
The total scale score demonstrated excellent reliability with ωtot = 0.964 and α = 0.951. The subscale scores also showed strong reliability: non-acceptance (ωtot = 0.938, α = 0.918), goals (ωtot = 0.910, α = 0.893), impulse (ωtot = 0.939, α = 0.903), awareness (ωtot = 0.846, α = 0.812), strategies (ωtot = 0.936, α = 0.917), and clarity (ωtot = 0.897, α = 0.857).
Personality Diagnostic Questionnaire 4
The Personality Diagnostic Questionnaire-4 (PDQ-4; Bagby & Farvolden, 2004) is a self-report screening measure designed to assess personality disorder symptoms based on DSM-IV criteria. For this study, we utilized the Cluster B section of the PDQ-4, which includes items assessing Antisocial, Borderline, Histrionic, and Narcissistic Personality Disorders. Participants responded to 38 true-false items that reflect the diagnostic criteria for these disorders. Example items include “I often feel that others are envious of me” (Narcissistic), “I have difficulty controlling my anger” (Borderline), “Lying comes easily to me and I often do it” (Antisocial), and “I am uncomfortable in situations where I am not the center of attention” (Histrionic). The scale scores demonstrated acceptable reliability: Histrionic (ωtot = 0.719, α = 0.663), Narcissistic (ωtot = 0.745, α = 0.701), Borderline (ωtot = 0.784, α = 0.738), and Antisocial (ωtot = 0.715, α = 0.652).
Procedure
All procedures were performed in compliance with relevant laws and institutional guidelines and were approved by the Institutional Review Board on June 17, 2022, with approval number HSRO#01060922. Participants completed an online survey administered through Qualtrics, an online survey platform. First, participants were given information about the study and the option to give informed consent, though the words “personality disorder” were not used in the consent form to avoid the risk of bias or stigma. Participants who consented to participate then filled out the demographics form, the DERS, and the PDQ. They were then given the option to choose whether they wanted to receive class credit or to enter the gift card raffle, although only students participating through the introductory psychology research platform could elect to receive class credit. Lastly, participants were then debriefed about the study. In this form they were told that the study investigated the relationship between personality traits and difficulties with regulating emotions; however, the words “personality disorder” were still not used. The survey took about 15 minutes on average.
Analytic Approach
Path analyses for both studies were conducted using lavaan (v.0.6-18, Yves, 2012) in R (v.4.3.0; R Core Team, 2023). Missing data was assessed using the naniar package (v.1.1.0, Tierney & Cook, 2023), reliability measures were obtained using psych package (v.2.4.3, Revelle, 2024), normality measures were obtained with MVN package (v.5.9, Korkmaz et al., 2014) and multicollinearity was assessed using the car package (v.3.1-2, Fox & Weisberg, 2019).
In Study 1, a multivariate multiple regression was run as a path analysis, with the levels of the PDQ scores regressed on to the six subscales of the DERS to ascertain the relationship between different facets of emotion regulation and each of the Cluster B personality disorders. All variables used in the path analysis had less than 5.2% missing data (range: 1.2–5.2%). To account for missing data, Full Information Maximum Likelihood (FIML) estimation was used to estimate missing values. The data was not multivariate normal based on the Henze-Zirkler test, though the skewness (.005-1.33) and kurtosis (-.952 – 1.49) of each measure were within the generally acceptable range. We used the robust maximum likelihood estimator in lavaan, to account for multivariate normality assumption violation. Variance Inflation Factors (VIF) indicated that the predictor variables had an acceptable range of multicollinearity (range 1.65–3.46). To correct for multiple comparisons in the models the Benjamini-Hochberg false discovery rate (FDR) correction was used to correct the p-values. All data and R-code for both studies can be viewed at the Open Science Framework at https://osf.io/6y3zp/?view_only=6ae3c2e495d0403084e1a5ed2b32f2c3. 1
Results
Means, SDs, and Correlations for Study 1 Variables
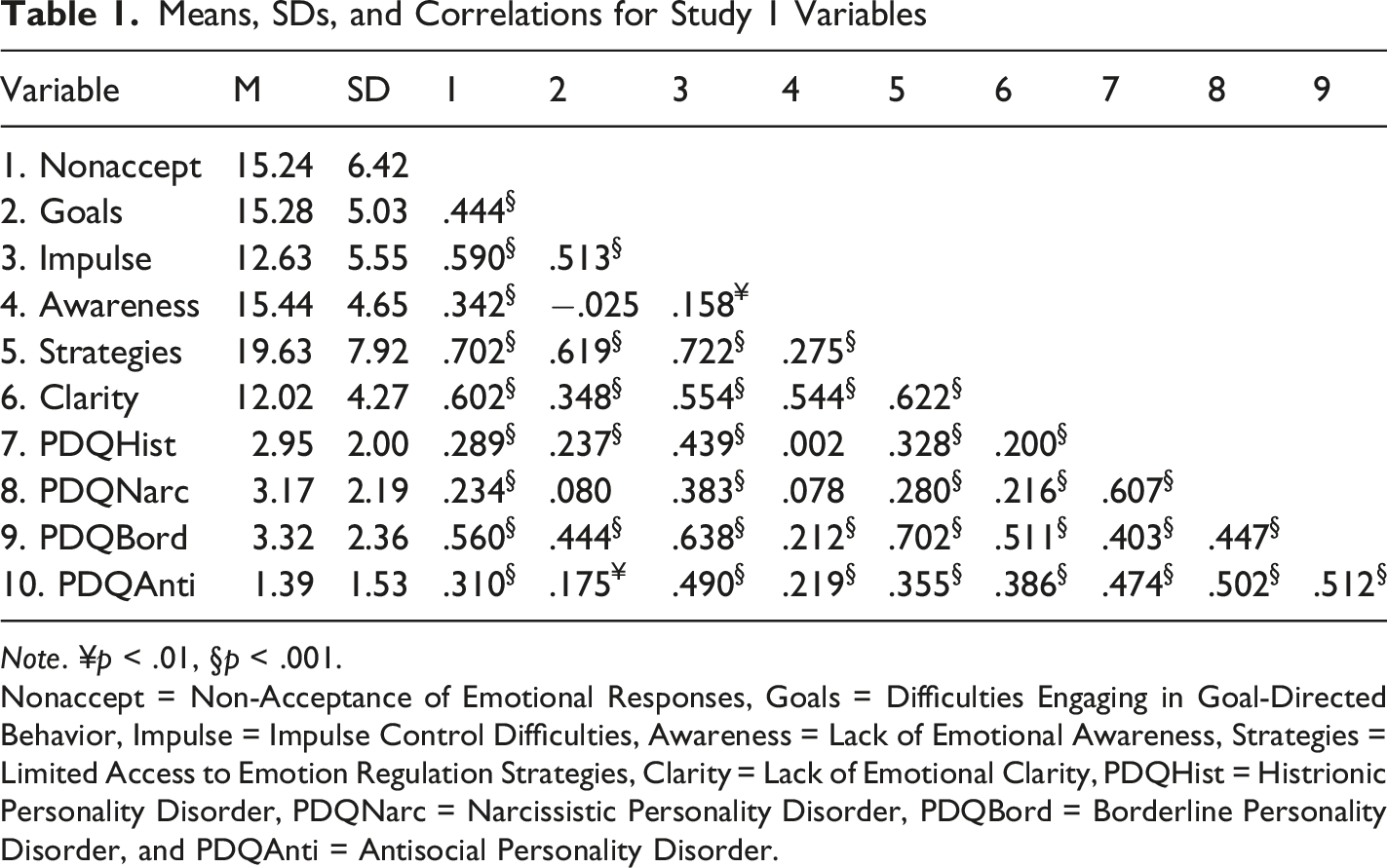
Note. ¥p < .01, §p < .001.
Nonaccept = Non-Acceptance of Emotional Responses, Goals = Difficulties Engaging in Goal-Directed Behavior, Impulse = Impulse Control Difficulties, Awareness = Lack of Emotional Awareness, Strategies = Limited Access to Emotion Regulation Strategies, Clarity = Lack of Emotional Clarity, PDQHist = Histrionic Personality Disorder, PDQNarc = Narcissistic Personality Disorder, PDQBord = Borderline Personality Disorder, and PDQAnti = Antisocial Personality Disorder.
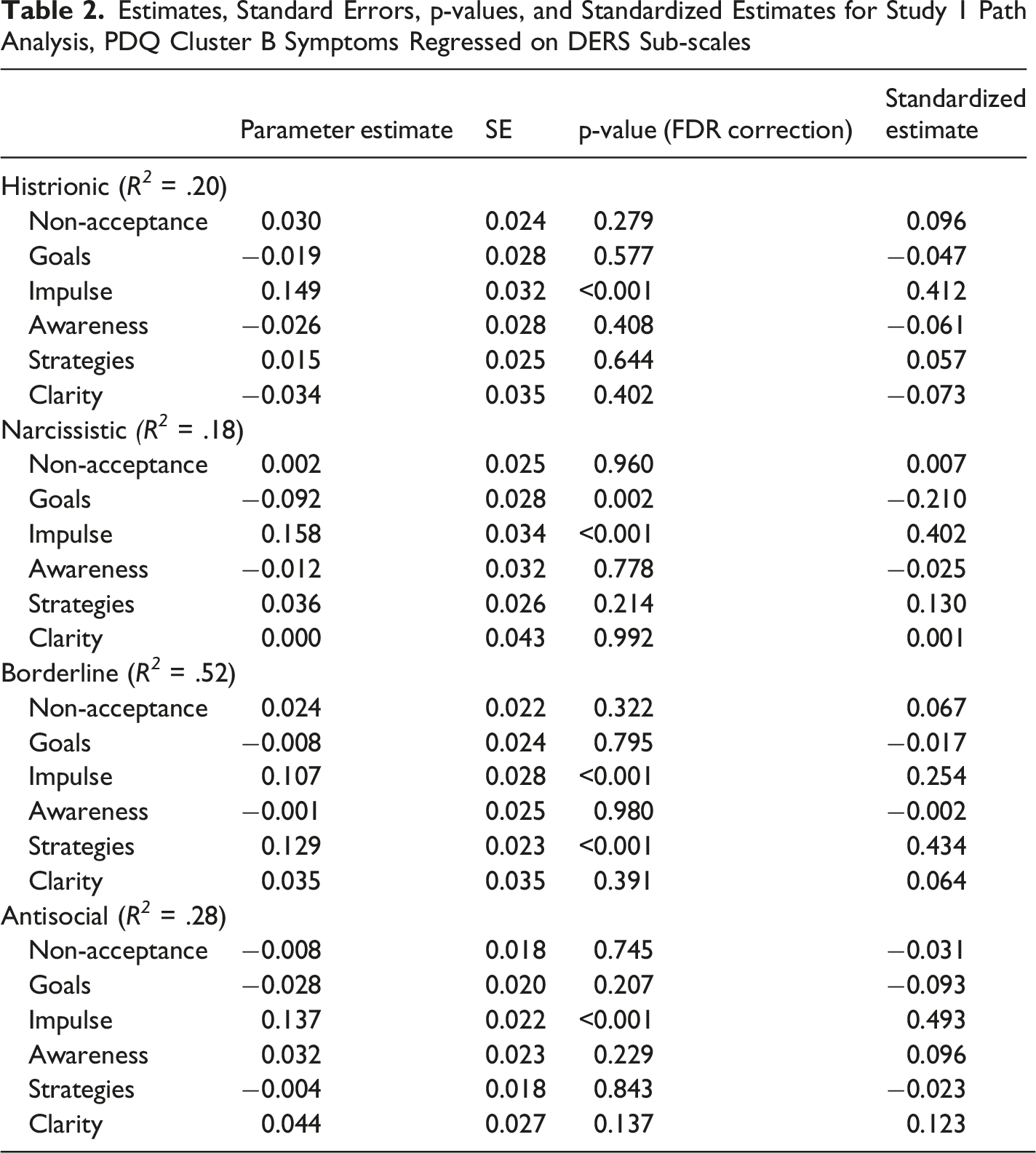
Significant pathways between DERS subscales and the four Cluster B groups are presented in Figure 1, and full model parameters are listed in Table 2. Histrionic personality disorder symptoms were positively associated with Lack of Impulse Control. Narcissistic Personality Disorder symptoms were negatively associated with Difficulties Engaging in Goal-Directed Behavior and positively associated with Lack of Impulse Control. Borderline Personality Disorder symptoms were positively associated with Limited Access to Emotion Regulation Strategies and Lack of Impulse Control. Finally, Antisocial Personality Disorder symptoms were positively associated with Lack of Impulse Control. Notably, Lack of Impulse Control was significantly associated with all four disorders. Study 1 model 1 significant pathways. Note. Only significant paths are shown (p < .05), path estimates are standardized Estimates, Standard Errors, p-values, and Standardized Estimates for Study 1 Path Analysis, PDQ Cluster B Symptoms Regressed on DERS Sub-scales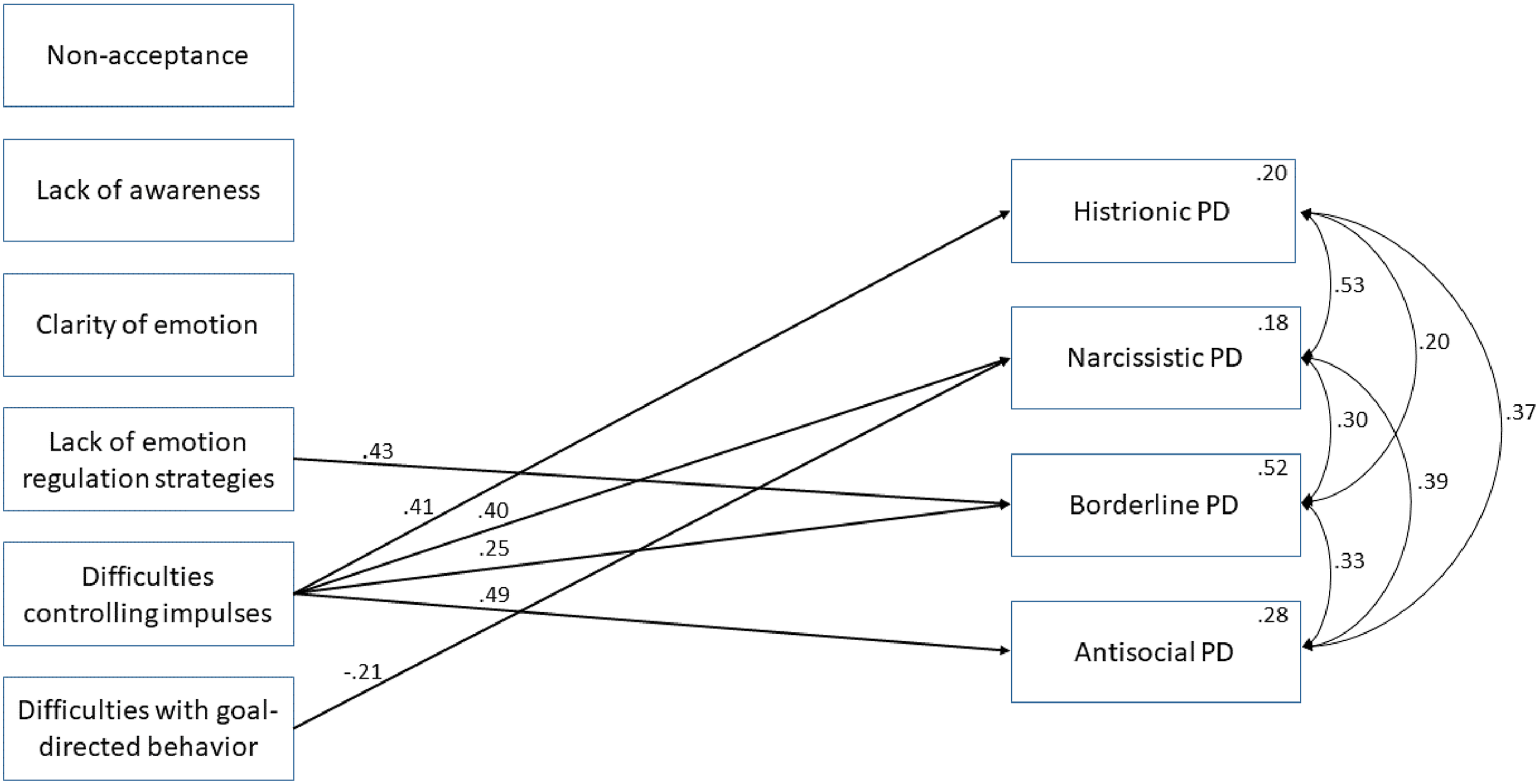
Study 1 Discussion
Study 1 aimed to explore the relationship between Cluster B personality disorders and emotion regulation difficulties. The pattern of results suggests some differential associations between specific emotion regulation dimensions and types of Cluster B Personality Disorders. Consistent with the link between Cluster B and emotion regulation difficulties (Dimaggio et al., 2017; Garofalo et al., 2018), all four disorders were significantly associated with at least one DERS subscale. The association between a lack of access to emotion regulation strategies and BPD is likely due to the disorder’s core feature of a cycle of dysregulation that is difficult to escape because of a lack of skills to deal with it (Berlin et al., 2005). Difficulties with goal-directed behavior is likely significantly negatively associated with NPD because the disorder is characterized by a preoccupation with success and achievement (Kraus & Reynolds, 2001). This could present an opportunity for developing adaptive strategies for behavior change.
Contrary to the findings of Borges and Naugle (2017), DERS Lack of Impulse Control was significantly associated with all four Cluster B personality symptom scores. Findings were consistent, though, with Glenn and Klonsky (2009), who also found lack of access to strategies and poor impulse control to be significantly associated with BPD. This could be explained, in part, by differences in samples, as the Borges and Naugle (2017) study used exclusively undergraduate students who were, on average, younger and had a higher proportion of women than the current study. Since difficulties controlling impulses were significantly associated with all disorders in the current study, these findings also suggest that impulse control may be the dimension of emotion regulation that is most important when it comes to Cluster B disorders. These results provide implications for future interventions for these disorders, suggesting that treatments for these disorders should continue to target impulse control (Conrad et al., 2017).
The significant association of impulse control with all the disorders suggests this variable should be assessed more specifically to delineate between the different disorders’ problems with impulse control, as there may be different mechanisms at play with each. To that end, impulse control can be considered a multidimensional concept (Whiteside & Lynam, 2001). Today, one popular conceptualization of impulsivity is a five-factor model consisting of urgency (both positive and negative), (lack of) premeditation, (lack of) perseverance, and sensation seeking. Urgency refers to the inability to resist impulses, driven by either positive or negative emotions. Lack of premeditation refers to the inability to consider the consequences of a behavior before carrying it out. Lack of perseverance refers to difficulties with focusing on tasks that are boring or complex. Finally, sensation seeking refers to the impulse to seek out exciting or stimulating experiences (Whiteside et al., 2005). To follow up on the results of Study 1, Study 2 was conducted to examine the relationship between Cluster B personality disorders and impulsivity as well as replicate and extend the results of Study 1.
Study 2
Method
Participants
To further delineate the relationship between different facets of impulsivity, emotion regulation, and Cluster B personality disorder symptomatology, participants were recruited via social media, online advertisements, word of mouth, an introductory psychology research group, and flyers in cities across the Northeastern United States to complete an online assessment battery. Participants were again given the option to receive class credit or enter a raffle for one of four $25 gift cards. One thousand and seventy-eight individuals started the survey. Of these participants, we removed 191 who did not complete any survey items on the main study variables of interest. In Study 2 there were four attention checks. Participants were excluded from the sample if they answered more than one of the attention check questions incorrectly. This resulted in 354 cases being removed. Finally, three participants were removed because they were younger than 18 years old for a final sample of 530 participants. In Study 2, 22.7% of participants were recruited through the university research participant pool.
The mean age of participants was 30.74 (SD = 14.28) years, and the group identified as 38.7% male, 54.9% female, 4.7% non-binary, 1.1% genderqueer, and .6% elected to self-describe their gender. Relevant to note is that some participants reported a prior diagnosis of a Cluster B personality disorder, totaling 12% of the sample. Specifically, 4% reported a prior BPD diagnosis, 3.6% reported an NPD diagnosis, 2.3% reported an HPD diagnosis, and 2.1% reported an ASPD diagnosis.
Measures
Difficulties in Emotion Regulation Scale
In Study 2, the total scale score demonstrated excellent reliability with ωtot = 0.958 and α = 0.947. The subscale scores also showed strong reliability: Non-Acceptance (ωtot = 0.932, α = 0.900), Goals (ωtot = 0.878, α = 0.864), Impulse (ωtot = 0.905, α = 0.878), Awareness (ωtot = 0.839, α = 0.806), Strategies (ωtot = 0.913, α = 0.884), and Clarity (ωtot = 0.880, α = 0.847).
Personality Diagnostic Questionnaire 4
The reliability scores on the PDQ4 for Study 2 indicated good reliability: Histrionic (ωtot = 0.885, α = 0.860), Narcissistic (ωtot = 0.917, α = 0.895), Borderline (ωtot = 0.902, α = 0.873), and Antisocial (ωtot = 0.932, α = 0.910).
SUPPS-P Impulsive Behavior Scale
The Short Version of the UPPS-P Impulsive Behavior Scale (SUPPS-P) is a 20-item self-report measure designed to assess five distinct facets of impulsivity: Negative Urgency, Lack of Perseverance, Lack of Premeditation, Sensation Seeking, and Positive Urgency (Cyders et al., 2014). Prior research has demonstrated this shorter version of the UPPS-P to have sound psychometric properties across a variety of populations and cultures/languages (Fournier et al., 2025) and was selected to minimize participant burden. Each subscale consists of four items, and respondents rate their agreement with each statement on a four-point Likert scale ranging from 1 (agree strongly) to 4 (disagree strongly). Example items include “I have trouble controlling my impulses” (Negative Urgency) and “I generally like to see things through to the end” (Lack of Perseverance).
The SUPPS-P scale scores demonstrated good reliability: Negative Urgency (ωtot = 0.813, α = 0.765), Lack of Perseverance (ωtot = 0.767, α = 0.723), Lack of Premeditation (ωtot = 0.851, α = 0.822), Sensation Seeking (ωtot = 0.764, α = 0.698), and Positive Urgency (ωtot = 0.848, α = 0.836).
Procedure
To begin the survey, the same procedures were followed as in Study 1. The DERS and the SUPPS-P were presented in a random order, and then the PDQ was presented. Participants were then given the option to choose whether they wanted to receive class credit, if relevant, or to enter the gift card raffle. Lastly, participants were then debriefed about the study. In this form, they were told that the study investigated the relationship between personality traits and difficulties with regulating emotions; however, the words “personality disorder” were not used. The survey took about 23.6 minutes to complete on average.
Analytic Approach
The analytic approach was similar to that in Study 1. Two path analyses were run, one regressing the DERS subscales on PDQ Cluster B personality groups as a replication of Study 1, and a second path analysis regressing the DERS subscales and the SUPPS-P onto the PDQ Cluster B personality groups. Percent missing across path analysis variables ranged from 1.3 to 6.9%. To account for missing data, Full Information Maximum Likelihood (FIML) estimation was used. The data was not multivariate normal based on the Henze-Zirkler test, though the skewness (−0.139 –0.524) and kurtosis (−1.536 to −0.184) of each measure were within the generally acceptable range. We used the robust maximum likelihood estimator (MLR) in lavaan, to account for the multivariate normality assumption violation. Variance Inflation Factors (VIF) indicated that the predictor variables had an acceptable range of multicollinearity in both path analyses (DERS path analysis VIF range 1.50 – 3.40; DERS and SUPPS-P analysis VIF range 1.20 – 3.41). To correct for multiple comparisons in the models, the Benjamini-Hochberg false discovery rate (FDR) correction was used to correct the p-values.
Results
Means, SDs, and Correlations for Study 2 Variables
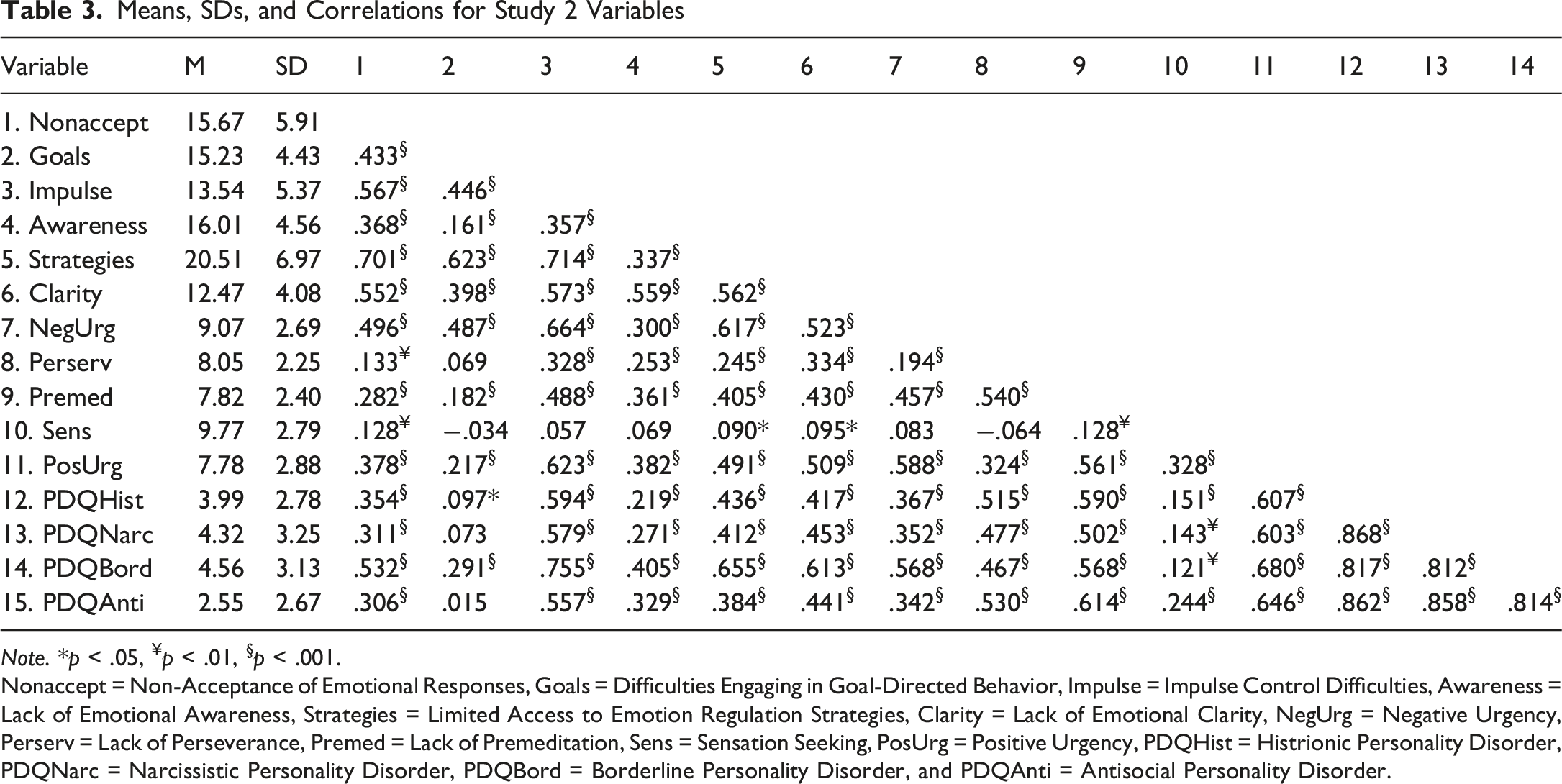
Note. *p < .05, ¥p < .01, §p < .001.
Nonaccept = Non-Acceptance of Emotional Responses, Goals = Difficulties Engaging in Goal-Directed Behavior, Impulse = Impulse Control Difficulties, Awareness = Lack of Emotional Awareness, Strategies = Limited Access to Emotion Regulation Strategies, Clarity = Lack of Emotional Clarity, NegUrg = Negative Urgency, Perserv = Lack of Perseverance, Premed = Lack of Premeditation, Sens = Sensation Seeking, PosUrg = Positive Urgency, PDQHist = Histrionic Personality Disorder, PDQNarc = Narcissistic Personality Disorder, PDQBord = Borderline Personality Disorder, and PDQAnti = Antisocial Personality Disorder.
Model 1 - PDQ Cluster B Symptoms Regressed Onto the DERS
We replicated the significant pathways found in Study 1 in this model. However, in this sample, we also observed additional significant predictors of the four Cluster B groups. Significant pathways between DERS subscales and the four Cluster B groups are presented in Figure 2 and full parameters are presented in Table 4. Histrionic personality disorder symptoms were negatively associated with lack of emotional awareness and difficulties engaging in goal-directed behavior, and positively associated with lack of emotional clarity, limited access to emotion regulation strategies, and lack of impulse control. Narcissistic Personality Disorder symptoms were negatively associated with difficulties engaging in goal-directed behavior, and positively associated with lack of emotional clarity, limited access to emotion regulation strategies, and lack of impulse control. Study 2 model 1 significant pathways. Note. Only significant paths are shown (p < .05), path estimates are standardized Estimates, Standard Errors, p-values, and Standardized Estimates for Study 2 Model 1 Path Analysis, PDQ Cluster B Symptoms Regressed on DERS Sub-scales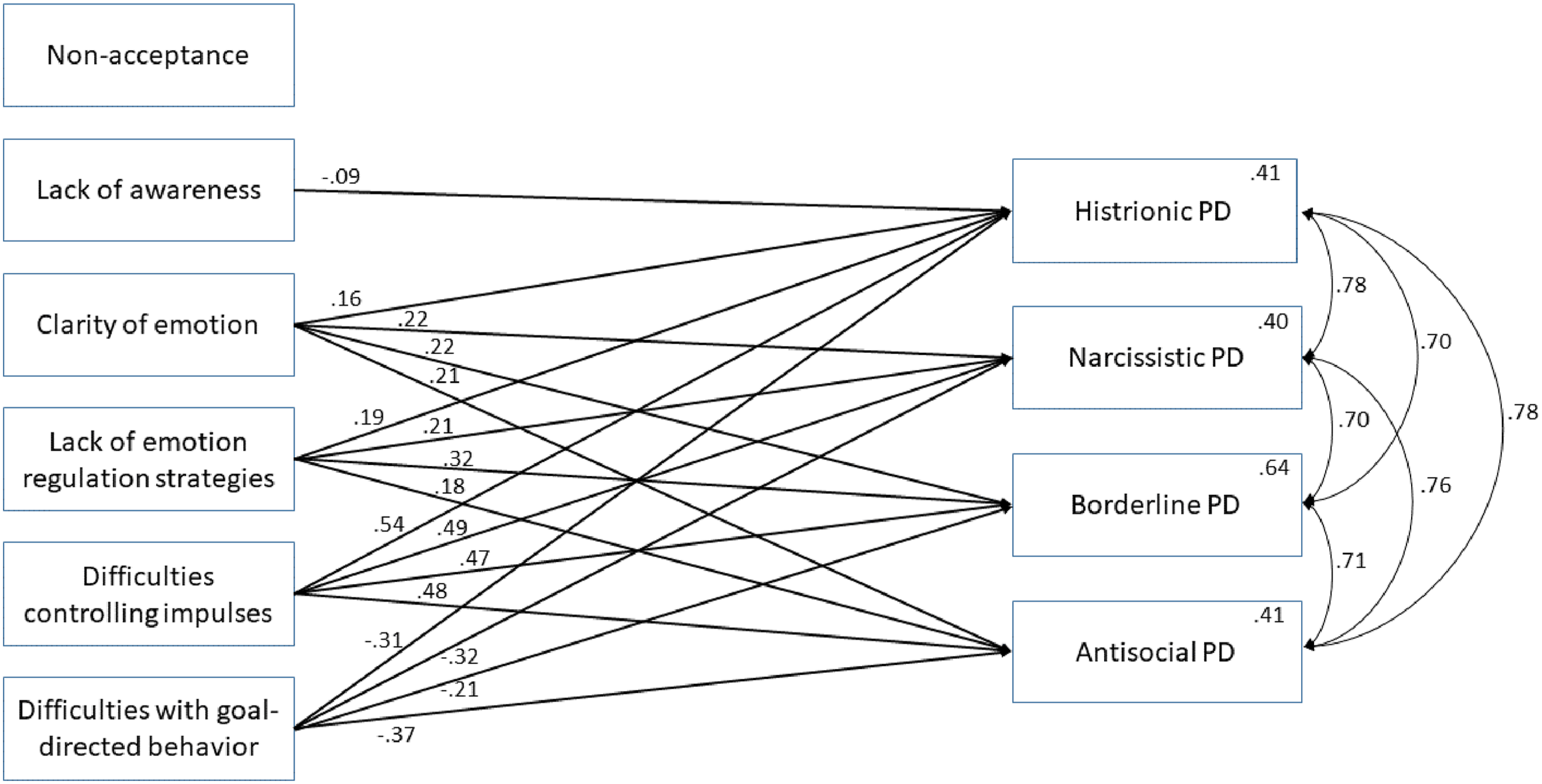
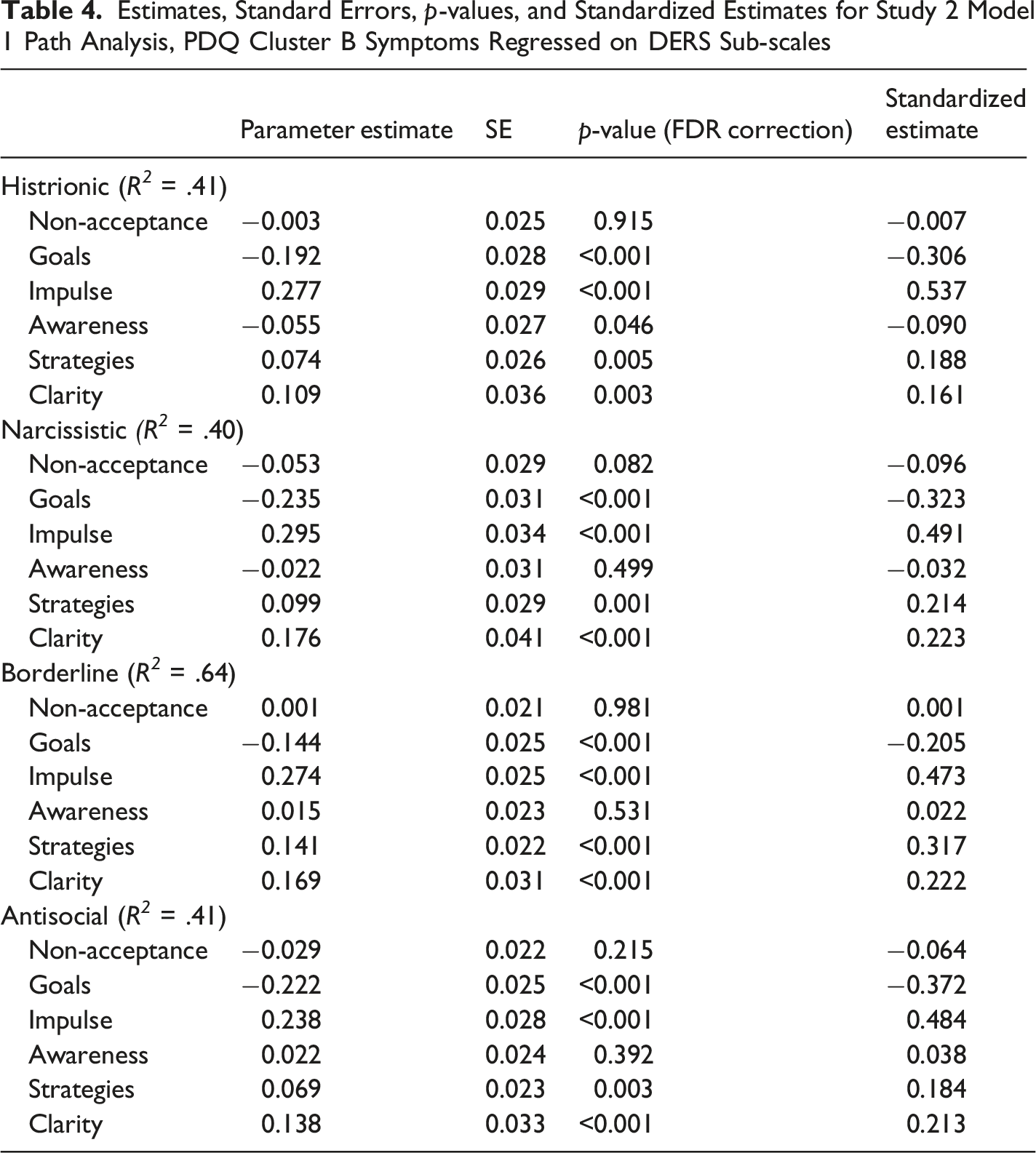
Borderline Personality Disorder symptoms were negatively associated with difficulties engaging in goal-directed behavior, and positively associated with lack of emotional clarity, limited access to emotion regulation strategies, and lack of impulse control. Antisocial Personality Disorder symptoms were negatively associated with difficulties engaging in goal-directed behavior, and were positively associated with lack of emotional clarity, limited access to emotion regulation strategies, and lack of impulse control.
Model 2 - PDQ Cluster B Symptoms Regressed Onto the DERS and SUPPS-P
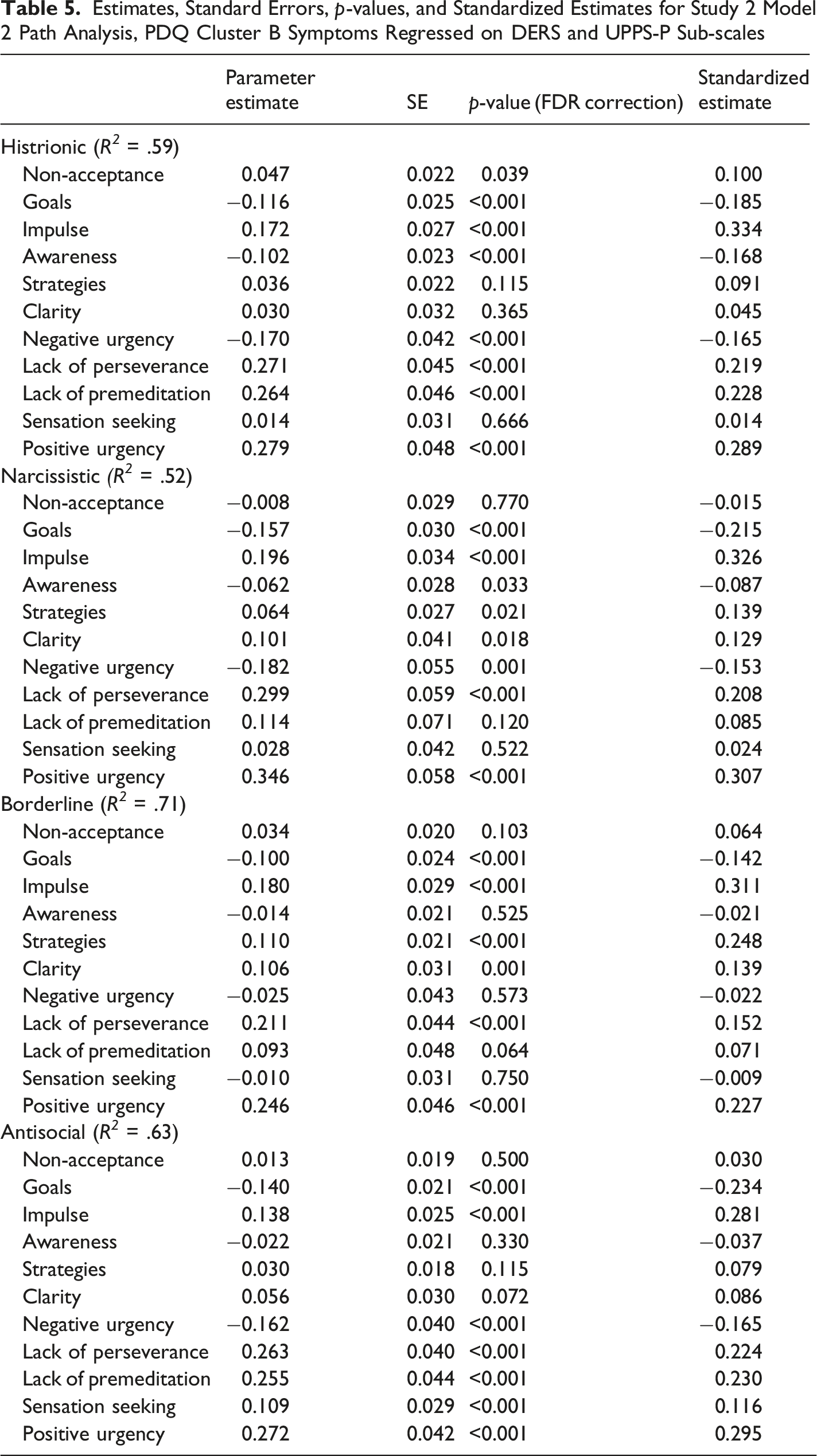
In Model 2, we looked at the relationship between different facets of impulsivity while continuing to control for facets of emotion regulation. Significant pathways between DERS subscales, SUPPS-P subscales, and the four Cluster B groups are presented in Figure 3, and full parameters are presented in Table 5. In this model, Histrionic Personality Disorder symptoms were negatively associated with lack of emotional awareness, difficulties engaging in goal-directed behavior, and negative urgency, and positively associated with non-acceptance of emotional responses, lack of impulse control, lack of perseverance, lack of premeditation, and positive urgency. Narcissistic Personality Disorder symptoms were negatively associated with difficulties engaging in goal-directed behavior, lack of emotional awareness, and negative urgency, and positively associated with lack of emotional clarity, limited access to emotion regulation strategies, lack of impulse control, lack of perseverance, and positive urgency. Borderline Personality Disorder symptoms were negatively associated with difficulties engaging in goal-directed behavior, and were positively associated with lack of emotional clarity, limited access to emotion regulation strategies, lack of impulse control, lack of perseverance, and positive urgency. Antisocial Personality Disorder symptoms were negatively associated with difficulties engaging in goal-directed behavior and negative urgency, and were positively associated with lack of impulse control, lack of perseverance, lack of premeditation, sensation seeking, and positive urgency. Study 2 model 2 significant pathways. Note. Only significant paths are shown (p < .05), path estimates are standardized Estimates, Standard Errors, p-values, and Standardized Estimates for Study 2 Model 2 Path Analysis, PDQ Cluster B Symptoms Regressed on DERS and UPPS-P Sub-scales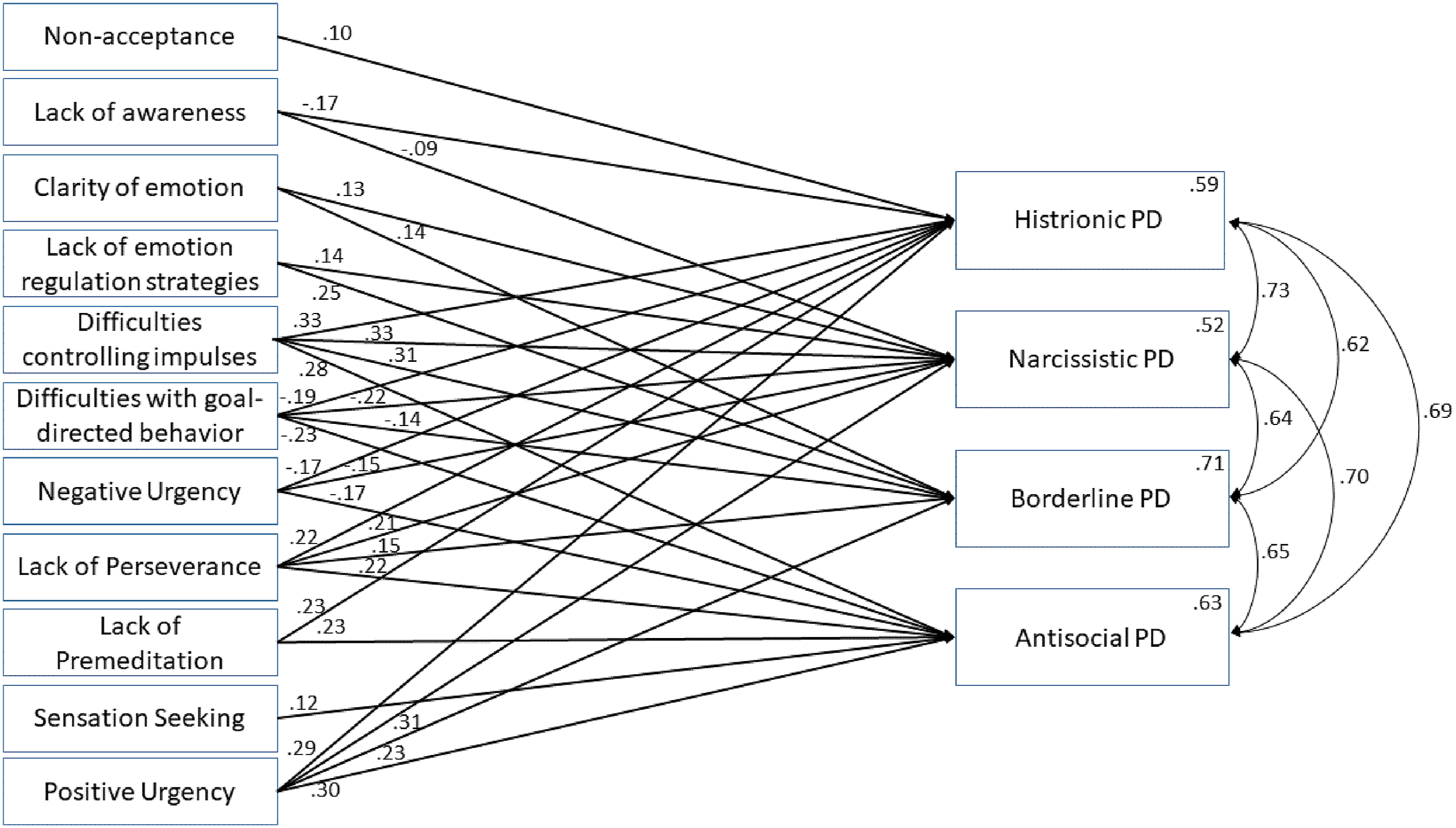
Study 2 Discussion
Study 2 aimed to follow up on Study 1 by attempting to replicate the relationships between Cluster B personality disorders and facets of emotion regulation in a separate sample, and more specifically examine different facets of impulsivity while controlling for emotion regulation. The relationship between Cluster B personality disorders and emotion regulation is complex and interconnected. In terms of replication, Study 2 Model 1 indicated the same relationships between the DERS subscales seen in Study 1; however, many additional significant pathways were found. The results of both studies strongly suggest that impulsivity related to strong emotions is an important factor for all four disorders. We discuss the impulsivity findings in more detail below.
In Study 2, limited access to emotion regulation strategies continued to predict greater Cluster B symptomatology for BPD but was now also significantly associated with the other three disorders, though the largest standardized effect was still for BPD. While difficulty using effective emotion regulation strategies is a well-known feature of BPD (Fitzpatrick & Kuo, 2022), it may underlie many of the behaviors associated with the other Cluster B disorders as well. This is because these individuals try to manage their strong emotional experiences in maladaptive ways, such as someone with ASPD becoming violent when upset or someone with HPD using their sexuality to gain attention to reduce anxiety related to not being noticed. The consistency of these associations across both studies supports prior work emphasizing the importance of teaching more effective emotion regulation strategies to individuals with these disorders.
Lack of emotional clarity was not a significant predictor in Study 1, with standardized estimates being relatively small, but it did significantly predict symptomatology for all four disorders in Study 2, where the standardized estimates were larger. Studies show that emotional clarity facilitates healthy cognitive regulation of emotions, potentially mitigating the maladaptive emotional states typically associated with these disorders (Vine & Aldao, 2014). Additionally, poor emotional clarity not only contributes to the symptomatology of Cluster B disorders but also exacerbates interpersonal dysfunctions common in these individuals (Kraus & Reynolds, 2001).
The association between difficulties pursuing goals during strong emotional states differed across studies. In Study 1, only Narcissistic Personality Disorder symptoms are negatively associated with difficulties with goal-directed behavior; however, in Study 2, reduced difficulties with goal-directed behavior during emotional states were associated with all four personality disorders, which had relatively similarly sized standardized estimates. One would think that strong emotions would interfere with goal-directed behavior in individuals high in Cluster B personality disorder symptoms. When looking at the individual correlations, we do see that some disorders were positively related to difficulties with goal-directed behavior. This unexpected finding in the path models may be explained by the greater role impulsivity has in Cluster B disorders. That is, impulsive behavior may be directed toward meeting immediate needs, and this in turn may be interpreted by these individuals as goal-directed behaviors, albeit only short-term goals. Thus, these individuals may have difficulty meeting long-term goals due to their symptoms, but during periods of high emotionality, they may be adept at focusing on short-term goals, which may be at odds with their long-term goals (e.g. an individual with BPD engaging in self-harming behaviors to gain attention of a loved one in the immediate future, but the same behavior drives the person away over time).
Lack of emotional awareness was not associated with any Cluster B disorders in Study 1, but was negatively associated with Histrionic Personality Disorder in Study 2 Model 1, where an increased lack of emotional awareness was associated with decreased Histrionic symptoms, albeit with a relatively small standardized effect. This suggests that lack of emotional awareness may not be a significant characteristic of Cluster B disorders. Finally, we see that non-acceptance of emotional responses was not predictive in either Study 1 or Model 1 of Study 2. This suggests that the tendency to be distressed about experiencing strong emotions is not a particular feature of these personality disorders, at least not as conceptualized by the DERS.
While the pathway relationships from Study 1 were replicated in Study 2, there were additional significant pathways that emerged in Study 2. A few factors may contribute to the differences between models. For instance, the sample in Study 2 had a higher percentage of participants who reported a past Cluster B diagnosis, and the participants reported higher mean scores and greater variability on the PDQ scale. Additionally, in Study 2, the model accounts for a higher amount of variance, and the reliability estimates were stronger. Overall, these differences in sample characteristics likely contribute to the variations across Study 1 and Study 2 Model 1.
In both Study 1 and 2, difficulty with impulse control, as measured by the DERS, is significantly associated with all four Cluster B disorders, with relatively large effect sizes. When adding the UPPS subscales in Model 2 to better understand the relationship between impulsivity and Cluster B disorders, the associations with the DERS impulsivity items remained strong, suggesting that the impulsivity-related questions specific to emotion regulation capture unique aspects of Cluster B symptoms beyond the UPPS facets of impulsivity. For example, despite the conceptual overlap between the DERS impulse control scale and negative urgency, the DERS impulse control scale remains significantly associated with all four disorders in Study 2 Model 2 after the addition of the SUPPS-P; however, it is associated less strongly than in Study 2 Model 1. This is likely because some of the variability overlaps with the UPPS negative urgency scale. This may also explain why UPPS negative urgency is unexpectedly negatively associated with Cluster B personality disorder symptoms, while the associations with emotion regulation are taken into account, as a lot of the variance is likely being accounted for by both. These findings taken together further highlight the critical role that impulse control, specifically in the context of emotion regulation, plays in Cluster B disorders.
With regard to other aspects of impulsivity, symptom counts for all four Cluster B disorders were significantly associated with at least one subscale on the SUPPS-P. This is somewhat consistent with the Study 1 finding that DERS lack of impulse control was a significant predictor of each personality disorder score and is in line with expectations because all the disorders are characterized by erratic behavior patterns (Kraus & Reynolds, 2001). Furthermore, positive urgency and lack of perseverance were both significantly predictive of all four disorders. The associations with positive urgency emphasize the importance of rash behavior even in the context of positive emotional states for each of these Cluster B disorders and, unlike negative urgency, do not seem to be adequately assessed by the DERS. Although most treatment approaches for Cluster B personality disorders focus largely on improving skills to cope with negative emotional states, it has been suggested that impulsive behaviors in the context of positive emotional states may also be a valuable target for intervention across a number of psychological disorders (Um et al., 2018). Similarly, the associations between Cluster B disorder symptoms and lack of perseverance may reflect an underlying diminished persistence or motivation toward goals that is not necessarily explicitly addressed in the Cluster B diagnostic criteria. However, therapeutic approaches designed to improve this aspect of impulse control could have a significant impact on one’s ability to effectively implement skills developed during treatment and, therefore, may represent an important assessment and treatment consideration for those with Cluster B personality disorders beyond the more overt behaviors that tend to garner attention. Moreover, each of the Cluster B disorders involve a combination of internalizing and externalizing symptomatology (Eaton et al., 2010; Hahn et al., 2016). Past research has found lack of perseverance to be generally characterized as reflecting internalizing behavior, while sensation seeking and lack of premeditation are thought to reflect more externalizing types of behaviors. Positive and negative urgency have both been described as a mix of externalizing and internalizing symptoms, but with positive urgency tending more towards externalizing characteristics and negative urgency being more balanced (Hahn et al., 2016; Miller et al., 2003). The fact that both positive urgency and lack of perseverance were associated with all four Cluster B symptom variables in the current study does contrast with past research that characterized ASPD symptomatology as primarily externalizing (Eaton et al., 2010). Overall, the addition of the SUPPS-P to the model doesn’t entirely remove the impact of the DERS impulse control subscale, which again underscores that the emotional impulsivity being measured by the DERS may be a distinct and particularly relevant facet of impulsivity relative to what is assessed by the SUPPS-P.
The sensation seeking facet of the SUPPS-P was predictive of only ASPD in the current study. This may be because people with ASPD find it especially reinforcing to engage in these behaviors due to the chronic baseline levels of under-arousal associated with the disorder (Coren, 1999; Lootens et al., 2017). Similarly, lack of premeditation was only predictive of HPD and ASPD, which highlights the importance of lack of forethought for these two disorders. Given the large amount of variance explained by this framework, future treatment research should focus on targeting these differences in emotion regulation and impulsivity.
Conclusions
Limitations of Study 1 include collecting limited demographic information, such as only gender identity and not biological sex, and not collecting race or ethnicity. Another limitation is having a relatively younger, more undergraduate sample because, while participants were as old as 82 years of age, the mean was still just 28.45 years. One limitation of Study 2 is having a relatively young, white, American sample, with a significant portion of undergraduate participants, which may not be representative of the broader population. Both of the present studies are limited by their online nature, which may not be conducive to participant completion and seriousness (Aust et al., 2012). It should also be noted that the PDQ is primarily a screening measure for personality disorder symptomatology. Thus, the assessment may be limited in scope and it is possible that the binary response format may inflate symptom counts (de Reus et al., 2011). Another potential limitation is that for Study 1, the histrionic and antisocial factors of the PDQ4 had lower internal reliability scores, with Cronbach’s α in the .60s. This was also true for the SUPPS sensation seeking factor in Study 2. This may limit the generalizability of the findings and attenuate some of the associations, though it should be noted that all McDonald’s omega scores, a more sensitive measure of internal consistency for self-report measures (Dunn et al., 2014), were all above .7, which is considered acceptable. Finally, there was a difference in the relative rates of participants reporting prior personality disorder diagnoses between the two samples, with a greater number reporting a diagnosis in Study 2. This may be due to the increase online recruitment in Study 2, which included recruiting from online spaces where people with these diagnoses are more likely to actively participate (e.g., r/BorderlinePDisorder). Future research should attempt to replicate and extend the present study while taking a more dimensional approach to measuring personality and personality dysfunction that is in line with the model proposed in the DSM-5-TR.
Overall, these findings suggest that difficulties with impulsivity make up a large part of the emotional difficulties that those with these disorders face. This indicates that treatments for patients with these symptoms should be designed to target impulsivity and tailored to the specific facets associated with their diagnoses. Finally, by further investigating these areas, some difficulties can be assuaged for people who struggle with these difficult-to-treat disorders.
Footnotes
Ethical Considerations
All procedures were performed in compliance with relevant laws and institutional guidelines and were approved by Rochester Institute of Technology’s Institutional Review Board on June 17, 2022, with approval number HSRO#01060922.
Consent to Participate
All participants provided written informed consent electronically prior to beginning the study.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Rochester Institute of Technology College of Liberal Arts Student Research Grant awarded to Finn Cohen.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.