
Abstract
Insomnia is common and associated with both personality traits and psychological distress, yet it remains unclear how stable dispositional characteristics relate to insomnia severity across levels of emotional distress. Guided by hyperarousal and vulnerability–stress perspectives, this cross-sectional study examined Big Five traits, anxiety, depression, and insomnia severity in a community sample of Greek adults (N = 1,349). Participants completed validated measures of personality, psychological distress, and insomnia severity; sex and age were examined as covariates. Women, young adults aged 18–25, and older adults aged 66+ reported higher insomnia symptoms. At the domain level, insomnia severity was positively associated with Neuroticism and negatively associated with Conscientiousness, Extraversion, and Agreeableness, although Extraversion and Agreeableness did not remain independent predictors in multivariate models. Facet-level analyses showed that Neuroticism-related Anxiety and Depression, lower Organization, and lower Energy level uniquely contributed to insomnia severity. Moderation analyses indicated that anxiety, but not depression, attenuated the Neuroticism–insomnia association, which was strongest when anxiety symptoms were low and weaker, though still significant, at higher anxiety levels. Exploratory analyses suggested that this attenuation was unlikely to reflect a simple ceiling or variance-restriction effect. Findings support person-tailored approaches to insomnia assessment and intervention.
Introduction
Insomnia—characterised by persistent difficulties in initiating or maintaining sleep, accompanied by daytime impairment, persistent fatigue and reduced energy levels (APA, 2013)—afflicts between 10% and 40% of adults worldwide (e.g., Zeng et al., 2020). Recent epidemiological syntheses place point prevalence above 32% in Eastern European populations and show that one in five cases persists chronically, with women and older adults being at disproportionate risk (Morin & Jarrin, 2022). Beyond its immediate toll on mood and functioning, chronic insomnia independently predicts cardiometabolic morbidity and reduced life expectancy (Buysse, 2008). Although cognitive-behavioural therapy for insomnia (CBT-i) is effective for many sufferers (Alimoradi et al., 2022), a substantial proportion of the treated individuals remain symptomatic after therapy (Sandlund et al., 2023), underscoring the need to clarify effects associated with psychological distress and individual-difference factors that confer vulnerability. Even under similar conditions—noise, workload, shifts—some individuals remain resilient, suggesting that stable traits influence vulnerability. The present study explores whether such dispositional traits, in interaction with psychological distress, account for individual differences in insomnia severity.
Personality Dispositions as Diatheses for Sleep Disturbance
The Five Factor Model (FFM) of personality posits five broad trait domains—Neuroticism, Extraversion, Openness, Agreeableness and Conscientiousness—which together capture most of the systematic variance in adult personality. Large prospective cohorts and two recent meta-analyses converge on a robust bivariate pattern: high Neuroticism and low Conscientiousness reliably forecast shorter, poorer and more variable sleep (Duggan et al., 2014; Krizan & Hisler, 2019). Neuroticism is marked by emotional lability, rumination, and exaggerated threat appraisal—features commonly observed in individuals suffering from insomnia (Ellis et al., 2021) and conducive to nocturnal hyperarousal (Harvey, 2002). In contrast, conscientious individuals tend to maintain regular routines and exercise behavioural self-control, both protective for sleep regulation (Akram et al., 2023). Extraversion and low Openness appear to confer modest protective effects, while the role of Agreeableness remains equivocal (Conway et al., 2023; Emert et al., 2017; Fabbri et al., 2022; Kim et al., 2015).
Experimental studies demonstrate that neurotic individuals exhibit difficulties in emotion regulation, greater propensity for negative affect (e.g., pronounced worry about sleep, anxiety), and heightened physiological and cognitive hyperarousal, which, in turn, contribute to poorer subjective sleep quality (Zhang et al., 2023). Conscientiousness, by contrast, reflects self-discipline, planning and rule adherence. Epidemiological studies show that conscientious adults tend to follow earlier and more regular bedtimes, avoid evening stimulants, and adhere more consistently to stimulus-control guidelines, promoting healthier and more efficient sleep (Duggan et al., 2014; Emert et al., 2017). Extraversion’s association with positive affect and social connectedness may buffer stress reactions (Fabbri et al., 2022), whereas Agreeableness could foster interpersonal harmony and perceived bedtime safety (Hintsanen et al., 2014; Kim et al., 2015). Nonetheless, the modest size and contextual variability of these effects highlight the need to identify higher-order moderators that determine whether, when, and how personality traits influence sleep outcomes.
Affective States as Modulators of Dispositional Risk
Anxiety and depressive symptoms co-occur with insomnia at rates exceeding chance; population studies place the odds ratio for comorbid anxiety around 3.23 and for depression around 2.83 (Hertenstein et al., 2019). The dominant aetiological account—the hyperarousal model—posits that chronic insomnia reflects sustained cortical and autonomic activation driven by threat monitoring, rumination and dysfunctional beliefs (Dressle & Riemann, 2023). These processes are amplified by anxiety and depressive symptoms, which co-occur with insomnia at rates exceeding two-thirds in some populations. These psychopathological conditions are strongly associated with higher levels of Neuroticism and lower levels of Conscientiousness, Agreeableness, and Extraversion, which may exacerbate vulnerability to both sleep disturbances and affective dysregulation (Lester, 2021; Lyon et al., 2021; Nouri et al., 2019).
Until recently, empirical models treated distress primarily as a mediator explaining why neurotic or unconscientious individuals sleep poorly (Akram et al., 2019). However, accumulating evidence hints that anxiety and depression may instead—or also—moderate the strength of trait–insomnia couplings. Laboratory manipulations of pre-sleep worry show that once state anxiety surpasses a moderate threshold, Neuroticism no longer predicts polysomnographic sleep onset latency, implying a ceiling phenomenon in which intense affective arousal overrides the influence of stable personality traits (Horváth et al., 2016).
Building on vulnerability–stress theory, a two-tier perspective can be advanced. Under sub-clinical affective load, personality traits exert discernible influence: elevated Neuroticism heightens threat appraisal and perseverative cognition, whereas elevated Conscientiousness stabilises circadian and behavioural rhythms. As anxiety or depression escalates, global arousal reaches a ceiling where insomnia becomes widespread, attenuating between-person variance attributable to traits. Methodologically, this non-linear dynamic, demands moderation analyses able to detect trait × state interactions (Hayes, 2022). Individuals high in neuroticism are prone to maladaptive emotional and cognitive responses to sleep-related difficulties—such as persistent rumination and worry—that can intensify and prolong sleep disturbances (Krizan & Hisler, 2019). Moreover, neuroticism has been consistently associated with elevated levels of anxiety and depressive symptomatology (Lester, 2021), both of which are well-established correlates of insomnia (Comas et al., 2023). Taken together, these findings provide both theoretical and empirical support for examining whether anxiety and depression function as moderators in the relationship between neuroticism and insomnia.
The Present Study
Most trait-sleep studies have been conducted in Northern European or North American populations, while evidence from Mediterranean contexts remains sparse. Cultural differences in social rhythm regularity, dietary habits, and collectivistic coping strategies could modify both baseline sleep patterns and the salience of personality in sleep regulation. Moreover, extant research rarely examines personality, anxiety and depression simultaneously within the same moderation framework. By situating these factors within the mechanisms described above, the study offers a rigorous test of whether psychological distress amplifies or obscures the well-documented influence of personality on sleep. In doing so, it addresses a critical gap in the literature and informs precision-tailored interventions aimed at matching CBT-i to the individuals’ dispositional and affective profile.
Demographic factors such as sex and age also intersect with personality and distress in shaping sleep outcomes. Middle-aged women exhibit the highest chronic-insomnia prevalence, a pattern attributed to hormonal transitions, multi-role strain and heightened pre-sleep arousal (Morin & Jarrin, 2022; Tsou, 2022; Zeng et al., 2020). Younger adults report more sleep-onset difficulties (Morin & Jarrin, 2022) and greater evening physiological activation (Sidani et al., 2021), whereas older adults face circadian advance and difficulties maintaining sleep (Patel et al., 2018). These observations underscore the value of including demographic covariates when probing personality and distress effects.
The present study extends prior work in several ways. First, by analysing a large Greek sample it tests whether well-documented trait–insomnia associations generalise to a southern European cultural milieu characterised by later average bedtimes and strong familial networks. Second, the study explicitly models anxiety and depression as moderators rather than mere mediators, thereby adjudicating between additive-risk and ceiling accounts of dispositional vulnerability. Third, it incorporates sex and age as covariates to clarify whether previously reported demographic gradients persist after accounting for personality and distress. Fourth, it adds a facet-level perspective, moving beyond broad Big Five domains to identify the specific lower-order trait components most strongly associated with insomnia severity. This more fine-grained approach helps clarify whether insomnia risk is linked primarily to broad dispositional tendencies or to narrower affective, self-regulatory, and vitality-related personality features.
Drawing on the Five-Factor Model, the dynamic hyperarousal framework, and recent insights into psychological vulnerability, the literature review provides a conceptual foundation for examining a nuanced vulnerability–saturation model of insomnia. In doing so, it aims to move beyond static main-effect thinking and towards a more conditional, personalised understanding of why some individuals remain sleepless under stress while others sleep soundly despite similar challenges. Thus, drawing on the integrative hyperarousal model (Riemann et al., 2022), the study conceptualises insomnia risk as a two-tier system: a baseline predisposition (trait layer), where stable personality differences shape habitual cognitive-emotional reactivity, and affective activation (state layer) where situational anxiety or depression adds acute allostatic load. Whether state symptoms amplify or mask trait influences remains an open empirical question with direct clinical relevance. If an additive-risk model holds, interventions should address both personality-related cognitions and current emotional states. Alternatively, if saturation occurs, treatment should align with the individual’s current distress level.
Thus, the purpose of this study was to examine: (a) demographic covariates (age, sex) commonly implicated in sleep research; (b) the associations of each Big Five trait with insomnia severity; and (c) whether anxiety and depression condition the association between Neuroticism and insomnia severity. In supplementary exploratory analyses, we further examined whether specific Big Five facets uniquely contributed to insomnia severity and whether distress-related or demographic factors moderated selected facet-level associations. Building on prior findings, insomnia is expected to relate positively to Neuroticism and negatively to Conscientiousness. Regarding moderation, we tested two competing possibilities: an additive-risk pattern, in which trait–insomnia associations would be stronger under elevated distress, and an attenuation pattern, in which high psychological distress would reduce the relative contribution of stable personality traits.
Method
Participants and Procedure
A convenience sample of Greek adults was recruited between January and March 2025 through social media, word of mouth, and university-affiliated networks. Of the 1,838 individuals who participated, 1,349 (63.2 % female) provided consent and completed the Limesurvey online questionnaire (completion rate = 82%), while 489 were excluded due to incomplete responses or invalid response patterns. Regarding age (18 to 79 years; M = 35.26, SD = 16.41), 37.4% were between 18 and 29 years old (n = 504), 30.1% were aged 30–44 (n = 406), 20.2% were 45–59 years old (n = 272), and 12.3% were 60+ years (n = 167). The institutional review board approved all procedures.
Measures
Insomnia
The Greek translation of the Sleep Condition Indicator (SCI; Espie et al., 2014) consists of eight items rated on a 5-point Likert scale (0–4), assessing both nighttime symptoms and daytime consequences of poor sleep over the past month (e.g., “How satisfied are you with your current sleep pattern?”). Although the SCI is conceptually structured around two core components— sleep pattern and sleep-related impact—it is widely employed in both clinical and research contexts as a unidimensional index of insomnia severity (Marques et al., 2025). In the present study, total scores were computed by summing all items (range: 0–32), with lower scores indicating more severe insomnia.
To verify the factorial consistency of the translated instrument, an exploratory factor analysis (EFA) was conducted which confirmed the anticipated two-factor solution, accounting for 63.3% of the total variance (KMO = .84; Bartlett’s test of sphericity, χ2 (28) = 4011.02, p < .001). In line with prevailing empirical practice, and given the high internal consistency observed (Cronbach’s α = .86), the total SCI score was used as a unidimensional measure of insomnia severity.
Personality
The 60-item Big Five Inventory-2 (BFI-2; Kokkinos & Voulgaridou, 2024; Soto & John, 2017) yields Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness scores (12 items each; 1 = strongly disagree to 5 = strongly agree). Cronbach’s alphas ranged from .73 (Extraversion) to .86 (Conscientiousness and Neuroticism). In addition to the five broad personality domains, facet-level scores were computed following the BFI-2 scoring guidelines. Each domain was decomposed into three facets (four items each), resulting in 15 facet scores (e.g., anxiety, depression, and emotional volatility for neuroticism; organization, productiveness, and responsibility for conscientiousness). Internal consistency for the facet scales ranged from α = .57 to .86.
Psychological Distress
Anxiety and Depression were indexed by the respective six-item sub-scales of the Brief Symptom Inventory (Derogatis & Melisaratos, 1983; Loutsiou-Ladd et al., 2008). Respondents rate distress over the past week (0 = not at all to 4 = extremely). Alphas were .84 (Anxiety) and .86 (Depression).
Demographics
Age and sex were self-reported.
All instruments were administered in Greek. The BFI-2 was administered using the Greek version reported by Kokkinos & Voulgaridou (2024), and the BSI anxiety and depression subscales were based on the Greek psychometric evidence reported by Loutsiou-Ladd et al. (2008). For the SCI, a translation and back-translation procedure was conducted by independent bilingual translators, with discrepancies resolved through discussion to ensure semantic and conceptual equivalence. Accordingly, the BFI-2 and BSI subscales relied on Greek versions with prior psychometric support, whereas the SCI was psychometrically evaluated in the present sample through internal consistency analysis and exploratory factor analysis.
Statistical Analysis Plan
Data were screened for outliers and missing values (< 2% per variable) prior to analysis using SPSS 29.0 and the PROCESS macro v4.3 (Hayes, 2022). All variables met univariate normality assumptions (|skew| < 2, |kurtosis| < 7). Pearson correlations were conducted to examine zero-order associations among study variables. Hierarchical multiple regression analyses were performed to predict insomnia severity.
In addition to the primary domain-level analyses, supplementary models examined personality at the facet level to provide a more fine-grained understanding of the associations. Facet-level predictors were entered in the final step of the regression models after controlling for demographic variables and psychological distress.
Moderation analyses were conducted using PROCESS Models 1 and 2 to examine whether anxiety symptoms, depressive symptoms, sex, and age moderated the association between Neuroticism and insomnia severity. Exploratory facet-level moderation analyses were additionally conducted for the Neuroticism facets that demonstrated unique associations with insomnia severity in the hierarchical regression analyses. To reduce overparameterization and limit Type I error inflation, moderators were examined in separate models.
To further evaluate the attenuation pattern observed in the moderation analyses, additional exploratory analyses examined the variability of insomnia severity across low, moderate, and high levels of anxiety and depression. Mean scores, standard deviations, and variances of insomnia severity were compared across distress groups, and Levene’s tests were conducted to evaluate homogeneity of variances.
Significant interactions were further probed via simple-slope analysis and Johnson–Neyman regions of significance with 5,000 bias-corrected bootstrap samples. Effect sizes were interpreted according to Cohen (1988) guidelines.
Results
Means, Standard Deviations, Cronbach’s α (Diagonal, in Parentheses), and Zero-Order Correlations Among Study Variables
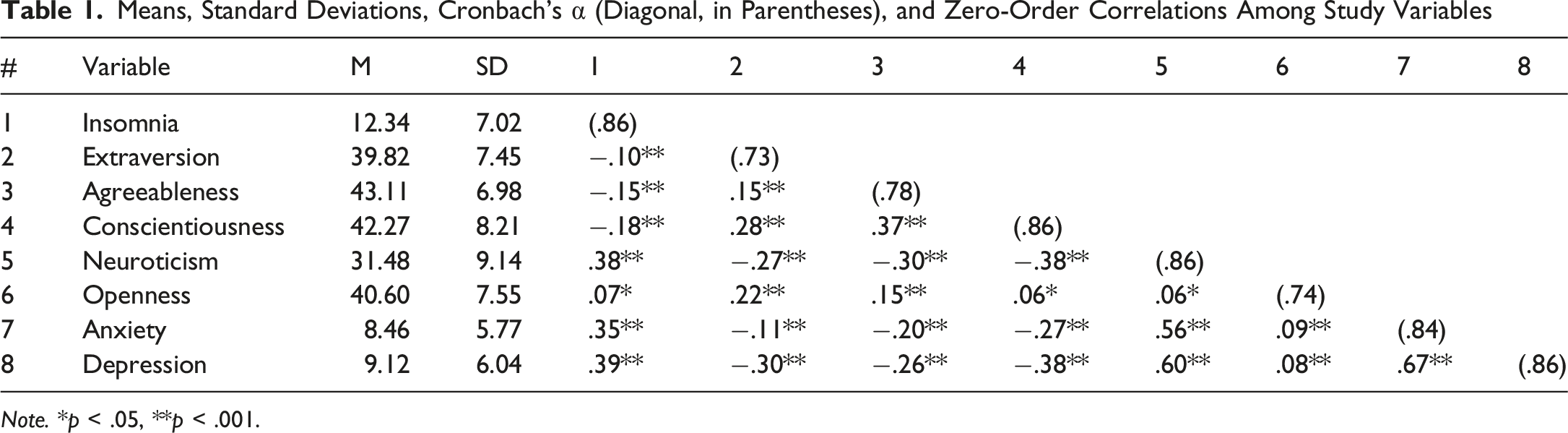
Note. *p < .05, **p < .001.
Sex and Age Effects
Because Levene’s tests indicated heterogeneity of variances across demographic groups (p < .05), a two-factor Aligned-Rank-Transform ANOVA (ART-ANOVA) was conducted on ranked SCI scores, with sex (male vs female) and age group (18–25, 26–45, 46–65, 66+) entered as between-subject factors. The analysis revealed a significant main effect of sex, F (1, 1338) = 4.82, p = .028, whereby women reported higher insomnia severity than men. A robust main effect of age group also emerged, F (3, 1338) = 7.68, p < .001, indicating that younger participants (18–25 years) and older adults (66+ years) experienced more pronounced insomnia symptoms than the other cohorts. Tukey-adjusted pairwise contrasts confirmed that each of the two older groups differed significantly from the 18–25 and 26–45 groups (all adjusted ps < .01), whereas the two younger groups did not differ from each other. The sex × age interaction was non-significant F (3, 1338) = 0.25, p = .864, suggesting that the age-related rise in insomnia severity was comparable for men and women. The ART-ANOVA approach was preferred over traditional parametric alternatives (e.g., Welch ANOVA) as it allows for the examination of interaction effects in factorial designs under violations of homogeneity of variance.
Correlations
Pearson correlations (Table 1) indicated that insomnia severity correlated positively with Neuroticism (r = .38), Anxiety (r = .35), Depression (r = .39) and, weakly with Openness (r = .07), and negatively with Extraversion (r = −.10), Conscientiousness (r = −.18) and Agreeableness (r = −.15).
Facet-Level Analyses
To extend the domain-level findings, we conducted additional analyses at the facet level of the BFI-2. Correlational analyses indicated that insomnia severity was positively associated with all Neuroticism facets, particularly Depression (r = .38) and Anxiety (r = .32), and negatively associated with Conscientiousness facets, including Organization (r = −.17), Productiveness (r = −.16), and Responsibility (r = −.12). Among Extraversion facets, only Energy level was significantly related to insomnia (r = −.19), whereas Sociability and Assertiveness were not. Internal consistency estimates and zero-order correlations for all BFI-2 facets are presented in Supplemental Table S1.
A hierarchical regression analysis was then conducted to examine whether these facets uniquely predicted insomnia severity beyond demographic variables and psychological distress. In Step 1, age was a significant predictor, whereas sex was not. In Step 2, both anxiety (β = .128, p < .001) and depression (β = .172, p < .001) were positively associated with insomnia severity, explaining 17.4% of the variance.
In Step 3, the inclusion of personality facets led to a significant increase in explained variance (ΔR2 = .041, p < .001), with the final model accounting for 21.5% of the variance. Among the facets, Neuroticism-related Anxiety (β = .129, p < .001) and Depression (β = .119, p = .004) emerged as significant predictors, whereas Emotional Volatility was not. From the Conscientiousness domain, only Organization was a significant negative predictor (β = −.100, p = .001). Additionally, Energy level, a facet of Extraversion, was negatively associated with insomnia severity (β = −.066, p = .019) (see Supplemental Table S2).
Moderation Analysis
A hierarchical multiple regression analysis was conducted to establish which covariates would enter the subsequent moderation analysis. The final model—including Neuroticism, BSI depressive symptoms, and BSI anxiety symptoms—was significant, F (5, 1343) = 63.33, p < .001, and explained 19% of the variance in self-reported insomnia (R2 = .19, adj. R2 = .19). Within this model, Neuroticism remained the most robust predictor (β = .20, t = 6.13, p < .001), followed by BSI depressive symptoms (β = .20, t = 5.62, p < .001) and BSI anxiety symptoms (β = .11, t = 3.08, p = .002). Sex and Openness to Experience were no longer significant once these variables were included, underscoring the primacy of the three focal predictors for the moderation stage.
Using these predictors, a PROCESS Model 2 moderation analysis tested whether BSI anxiety symptoms and BSI depressive symptoms jointly moderated the Neuroticism–insomnia association. The combined model accounted for 19.8% of the variance (R2 = .198). Main effects remained significant for Neuroticism (B = 0.17, SE = 0.03, p < .001), Depression (B = 0.21, SE = 0.04, p < .001), and Anxiety (B = 0.12, SE = 0.04, p = .001).
A modest but statistically significant Neuroticism × Anxiety interaction emerged (B = −0.08, SE = 0.04, p = .045; ΔR2 = .002), whereas the Neuroticism × Depression interaction was not (B = −0.04, p = .352; ΔR2 = .001). Simple-slope analysis showed that the positive association between Neuroticism and insomnia was strongest at low Anxiety (−1 SD; b = 0.33, SE = 0.04, p < .001), moderate at the mean (b = 0.25, SE = 0.03, p < .001), and weakest at high Anxiety (+1 SD; b = 0.17, SE = 0.04, p < .001). Thus, Anxiety attenuates—but does not reverse—the Neuroticism–insomnia link, while Depression does not further moderate this relationship. The interaction pattern is shown in Figure 1. Neuroticism as a function of psychological distress (anxiety and depression). Note. The combined interaction predicts insomnia. The slopes indicate that (i) at lower levels of depression with low or average anxiety, (ii) at average levels of depression with low, average or high anxiety, and (iii) at higher levels of depression with low or average anxiety, the relationship between neuroticism and insomnia is stronger
Exploratory facet-level moderation analyses were conducted for the Neuroticism facets that uniquely predicted insomnia severity. Because these analyses involved multiple interaction tests and conceptually overlapping constructs, findings should be interpreted cautiously. The results indicated that higher levels of depressive symptoms were associated with weaker facet–insomnia associations for both the Anxiety facet (b = −0.080, SE = 0.039, p = .042) and the Depression facet (b = −0.060, SE = 0.025, p = .015). Specifically, the associations between these facets and insomnia were weaker at higher levels of depressive symptoms.
In addition, age significantly moderated the association between the Anxiety facet and insomnia severity (b = 0.059, SE = 0.024, p = .014), such that the positive association between the Anxiety facet and insomnia severity was stronger among older participants. No significant moderation effects emerged for sex or for the interaction between the Depression facet and age. Full facet-level moderation results are presented in Supplemental Table S3.
Variance Check for the Ceiling-Effect Interpretation
To further examine whether the attenuation of the Neuroticism–insomnia association at higher levels of distress reflected a ceiling or variance-restriction effect, additional exploratory analyses compared the variability of insomnia scores across low, moderate, and high levels of anxiety and depression.
Results indicated that mean insomnia severity increased across distress groups; however, the variability of insomnia scores did not decrease at higher levels of anxiety or depression. In contrast, standard deviations and variance estimates remained relatively stable or slightly increased across groups. Levene’s tests further indicated significant heterogeneity of variances for both anxiety and depression groupings (ps < .01), suggesting that the attenuation pattern was unlikely to be explained solely by statistical variance restriction.
Accordingly, the findings do not provide strong support for a strict ceiling-effect interpretation and instead suggest that alternative mechanisms associated with elevated psychological distress may contribute to the weakened association between Neuroticism and insomnia severity.
Discussion
This study examined how personality traits relate to insomnia severity and whether these associations depend on levels of state anxiety and depression. Three principal findings emerged.
Demographic analyses converged with epidemiological norms by revealing higher insomnia severity in women and, more robustly, in older adults, over 66 years. Women appear more vulnerable to insomnia due to a complex interplay of psychological, biological and social factors, such as hormonal changes, especially during menopause and menstruation (Kennedy et al., 2022; Tandon et al., 2022), along with higher prevalence of depressive and anxiety symptomatology (Bandelow & Michaelis, 2015; Kennedy et al., 2022) and social pressures, including juggling various roles and cultural expectations (Tsou, 2022). Likewise, regarding the elderly, this trend is due to age-related biological changes, such as lower melatonin production and disruptions in circadian rhythms, along with higher rates of physical and mental health issues (Mookerjee et al., 2023; Patel et al., 2018).
Supporting a substantial literature, high Neuroticism and low Conscientiousness were associated with poorer sleep (Conway et al., 2023; Duggan et al., 2014; Fabbri et al., 2022; Krizan & Hisler, 2019). Neuroticism likely operates through perseverative cognition and autonomic rigidity (Ottaviani et al., 2016) and its significant association with insomnia may be related to this trait’s elevated emotional reactivity, cognitive hyperarousal, and stress vulnerability (Zhang et al., 2023). Notably, Neuroticism alone accounted for a sizeable amount of the variance that is typically attributed to the full Big-Five set, underscoring its centrality in hyperarousal models of insomnia (Dressle & Riemann, 2023; Riemann et al., 2022). Conscientiousness, in contrast, promotes adaptive health behaviours—regular bedtimes, impulse control, self-regulation, and adherence to sleep-restriction guidelines (Akram et al., 2023; Duggan et al., 2014; Emert et al., 2017).
The modest protective effect of Agreeableness and Extraversion on sleep disturbances emerged at the bivariate level; however, these traits did not retain unique predictive effects in the multivariate models. This pattern likely reflects shared variance with neuroticism and psychological distress, suggesting that their associations with insomnia may be indirect rather than independent. Although prior research has linked agreeableness and extraversion to better sleep through enhanced emotion regulation, lower interpersonal stress, and greater positive affect (Allen et al., 2016; Fabbri et al., 2022; Hintsanen et al., 2014), the present findings indicate that these effects may be subsumed under broader affective vulnerability processes when examined alongside distress variables.
When anxiety and depression were entered into the model, depression emerged as a stronger independent predictor of insomnia, whereas anxiety exerted a smaller incremental influence; together, the full model explained nearly one-fifth of the total variance. Contrary to the additive-risk expectation, anxiety and depression weakened the Neuroticism–insomnia link. One possible interpretation is that elevated psychological distress may reduce the relative contribution of stable personality traits to insomnia severity by increasing generalized hyperarousal across individuals.
To further evaluate this interpretation, additional analyses examined the variance of insomnia scores across levels of anxiety and depression. Contrary to a strict ceiling effect explanation, the findings did not indicate reduced variability in insomnia severity at higher levels of distress; instead, variability remained stable or slightly increased. This suggests that insomnia severity does not converge toward a uniform saturation point under conditions of elevated distress. Thus, the attenuation of the Neuroticism–insomnia association appears unlikely to reflect a purely statistical ceiling effect.
However, severe affective symptoms may engage alternative mechanisms (e.g., circadian misalignment, anhedonia, autonomic hyperactivity) that render trait pathways relatively less influential (Kalmbach et al., 2023; Palagini et al., 2023). In this sense, the observed attenuation of the neuroticism–insomnia association may still resemble patterns reported in stress reactivity research, where personality predicts cortisol responses primarily under mild to moderate stress conditions (Bibbey et al., 2013). Clinically, these findings suggest that screening solely for personality in highly distressed individuals may understate insomnia risk. Extending these domain-level findings, additional analyses at the facet level provided a more fine-grained understanding of the personality–insomnia association. Specifically, only certain facets uniquely contributed to insomnia severity when controlling for demographic variables and psychological distress. Within neuroticism, anxiety and depression emerged as significant predictors, whereas emotional volatility did not, suggesting that the link between neuroticism and insomnia is primarily driven by stable tendencies toward worry and low mood rather than general emotional instability.
In addition, the protective role of conscientiousness appeared to be specifically linked to organization, highlighting the importance of self-regulatory processes such as planning, structure, and routine in promoting better sleep. Productiveness and responsibility did not retain unique effects, suggesting that not all aspects of conscientiousness are equally relevant to sleep outcomes.
Αmong extraversion facets, only energy level was associated with insomnia severity, indicating that reduced vitality or fatigue may be more critical for sleep disturbances than broader social or assertive tendencies. Overall, these findings underscore the importance of moving beyond broad personality domains and examining more specific trait components when investigating sleep-related outcomes.
Moderation analysis qualified these main effects by showing that the Neuroticism–insomnia association was strongest at low levels of state anxiety and progressively attenuated as anxiety rose— a pattern suggestive of attenuation under conditions of elevated distress rather than the additive-risk assumption that dominates diathesis-stress thinking (Drake et al., 2014; Liu, 2015). The nonsignificant interaction with depression indicates that transient anxious arousal, rather than reduced positive affect, is the short-term state that obscures trait-based differences. Such a dynamic may help explain why previous clinical studies, which often enroll participants with high distress, have sometimes found weaker personality effects than large longitudinal surveys that include many sub-clinical cases (Rojo-Wissar et al., 2021).
Exploratory facet-level moderation analyses further suggested that narrower affective components of Neuroticism may not relate to insomnia uniformly across individuals. Specifically, depressive symptoms attenuated the associations between both the Anxiety and Depression facets and insomnia severity, whereas age strengthened the association between the Anxiety facet and insomnia. Although these findings should be interpreted cautiously given their exploratory nature, they suggest that the role of personality-related vulnerability in insomnia may vary depending on broader emotional and developmental context.
Findings advocate a tiered CBT-i approach. Among individuals high in Neuroticism but currently low in distress, interventions that foster worry reappraisal, enforce stimulus control, and strengthen conscientious sleep-hygiene habits could forestall the escalation of insomnia (Baglioni et al., 2023; Espie, 2022). When anxiety or depression is pronounced, therapy should prioritise emotion-regulation and mood management, as trait-focused techniques may yield diminishing returns. Such tailoring resonates with the Research Domain Criteria emphasis on trans-diagnostic mechanisms (Gunzler et al., 2020).
Several limitations warrant caution. The cross-sectional design precludes causal inference. Although moderation analyses identify conditional associations between personality, psychological distress, and insomnia severity, they cannot establish whether personality traits contribute to later insomnia, whether insomnia increases psychological distress, or whether reciprocal processes are involved. In addition, reliance on self-reported sleep may introduce bias, as such reports can be shaped by subjective beliefs, impaired memory recall, social desirability, or insincere responding (Stanley & De Brigard, 2019). Cultural factors may also moderate the observed patterns; for example, Greece’s relatively collectivistic tendencies could accentuate the social-emotional facets of insomnia. Future longitudinal and experience-sampling studies are therefore needed to clarify the temporal ordering of these effects and examine their cultural specificity.
Prospective studies should test whether personality predicts incident insomnia and whether affective states moderate these prospective effects. Neuro-physiological indices of arousal (e.g., heart-rate variability, actigraphy, polysomnography) could illuminate underlying pathways (Dikeos et al., 2023). The study did not assess several sleep-relevant covariates, including physical health status, medication use, caffeine intake, evening screen exposure, blue-light exposure, shift work, or diagnosed sleep disorders. These factors may influence insomnia severity and may also covary with personality and psychological distress. Consequently, the observed associations should be interpreted as psychological correlates of insomnia severity rather than as fully adjusted estimates of personality-related risk.
Finally, the online convenience sampling strategy may have produced selection bias. Recruitment through social media and university-affiliated networks may have overrepresented younger, more educated, digitally engaged, and psychologically minded participants. This may limit generalizability to the broader Greek adult population. In addition, self-selection into a sleep-related study may have attracted individuals with greater interest in, or concern about, sleep problems, potentially influencing the observed levels of insomnia and psychological distress.
Intervention research might compare CBT-i augmented with personality-tailored modules versus standard protocol. For individuals showing high Neuroticism but relatively low current distress, trait-tailored intervention may focus on preventive cognitive-behavioral strategies, such as reappraising sleep-related worry, reducing threat monitoring at bedtime, strengthening stimulus control, and building stable routines that support regular sleep-wake rhythms. For individuals with elevated anxiety or depression, however, insomnia treatment may need to prioritize emotion-regulation and mood-focused components, including relaxation training, behavioral activation, cognitive restructuring of rumination and catastrophic thinking, and integration of CBT-i with interventions targeting anxiety or depressive symptoms.
The current work enriches vulnerability–stress models by showing that anxiety and depression mask rather than amplify Neuroticism-related insomnia risk. Personality exerts its greatest influence when affective arousal is moderate, suggesting a window for preventive, trait-oriented interventions. Integrating dispositional and state constructs promises finer-grained, personalised approaches to insomnia treatment.
Supplemental Material
Supplemental material - Big Five Personality Traits and Insomnia Severity in Adults: The Conditional Role of Anxiety and Depression
Supplemental material for Big Five Personality Traits and Insomnia Severity in Adults: The Conditional Role of Anxiety and Depression by Constantinos M. Kokkinos and Athanasios Koutsospyros in Psychological Reports
Footnotes
Acknowledgements
The authors gratefully acknowledge Assistant Professor Dr. Ioanna Voulgaridou for providing statistical advice. The authors remain solely responsible for the analyses, interpretations, and conclusions reported in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.