
Abstract
Background
Nonverbal synchrony is a growing area of interest in social anxiety disorder (SAD), but a systematic overview is lacking. This scoping review maps existing research on nonverbal synchrony between individuals with high social anxiety and others to identify characteristics, measurement methods, and knowledge gaps.
Methods
Following PRISMA-ScR guidelines, we conducted a scoping review of four major databases (MEDLINE, Embase, CENTRAL, and PsycINFO), two trial registries (WHO ICTRP and ClinicalTrials.gov), and citation searching. The included studies investigated interindividual nonverbal synchrony (e.g., body movement, physiological, vocal) in individuals with diagnosed or high social anxiety.
Results
From 1,503 records, 12 studies were included in the review. Individuals with high social anxiety showed difficulties in body, vocal, and physiological synchrony, especially when in leadership roles. Body-movement synchrony, measured mainly by motion energy analysis, was the most common approach. Social anxiety severity and therapeutic alliance were key associated indicators.
Conclusions
Individuals with high social anxiety show context- and role-dependent synchrony difficulties. Research in this field is dominated by body movement analysis, revealing a gap regarding other modalities, especially neural measures like inter-brain synchrony. Multimodal, ecologically valid, and culturally diverse research is needed to advance understanding and develop targeted interventions for SAD.
Background
In recent years, the challenges faced by individuals with social anxiety disorder (SAD) in interpersonal engagements have gained attention from the aspect of nonverbal synchrony. Social anxiety disorder (SAD), defined as marked fear or anxiety in social interactions or performance situations (APA, 2013), is a major subtype of anxiety disorders. Cross-national data from the World Mental Health Surveys (28 community surveys) estimate the lifetime prevalence of SAD at 4.0% (12-month prevalence: 2.4%) (Stein et al., 2017). Epidemiological evidence indicates that the global burden of anxiety disorders has increased over recent decades (e.g., increases in incident cases and disability burden from 1990 to 2019; Xiong et al., 2022) and rose further during the first year of the COVID-19 pandemic (Bie et al., 2024). In addition to this growing disease burden, anxiety disorders impose substantial economic costs; for example, 2.08% of global health expenditures have been estimated as allocated to treating anxiety disorders (Bie et al., 2024). For clarity, we use “SAD” to refer to clinically diagnosed social anxiety disorder, “social anxiety” to refer to elevated social anxiety in non-treatment samples defined by questionnaire thresholds, and “SAD/social anxiety” when discussing findings across both groups.
Given that SAD is characterized by heightened fear and anxiety in interpersonal situations, mechanisms that facilitate mutual understanding in social interaction are particularly relevant. The characteristics of social anxiety disorder can be observed across multiple modalities. Behavioral (body movement) synchrony captures the coordination of visible actions such as gestures, postures, or whole-body motions and is often quantified from video (e.g., motion-based indices) at sub-second to seconds-level timescales. Vocal synchrony (acoustic/prosodic entrainment) reflects the convergence in speech-related features, such as pitch, intensity, speaking rate, and turn-taking patterns; these are typically derived from audio recordings. Physiological synchrony refers to covariation in autonomic signals (e.g., heart rate/heart rate variability), which may reflect shared arousal or co-regulation and is often expressed on slower timescales (daSilva & Wood, 2024). Neural (inter-brain) synchrony denotes the alignment of neural activity between individuals measured simultaneously (e.g., hyperscanning) and has been discussed as a potential mechanism for supporting successful social interaction (Czeszumski et al., 2020; Müller et al., 2022). Although related, these forms of synchrony are not interchangeable because they differ in their measurement protocols, temporal dynamics, and the aspect of interaction they most directly index. In the present scoping review, we primarily focus on behavioral (body movement) synchrony, while also summarizing evidence from vocal and physiological (cardiac) synchrony, when available. The fear of negative evaluations from others prompts those with SAD to engage in safety behaviors, such as avoiding eye contact. This hinders their ability to acquire external cues like body language and facial expressions, which leads to lost interaction opportunities in social contexts (Asher et al., 2020). In psychotherapy, the synchrony level between a therapist and client is posited to correlate with the strength of the therapeutic relationship (Tschacher & Meier, 2020). Studies coding interactions between individuals with SAD tendencies and their romantic partners have revealed that those with SAD tendencies engage in negative nonverbal communication more often than those without such tendencies (Wenzel et al., 2005), for example, by exhibiting less eye contact and fewer gestures and smiles. Although data collection on nonverbal activities was formerly challenging, recent advancements in sensing technologies have facilitated the acquisition of high-precision, multimodal data, allowing for the accurate measurement of synchrony phenomena related to heartbeat, body movement, respiratory patterns, and even brain activity using methods like hyperscanning (e.g., Mende & Schmidt, 2021; Tschacher & Meier, 2020).
Although a previous study suggested that individuals with SAD may exhibit reduced nonverbal synchrony during social interaction (Altmann et al., 2020), the evidence remains scattered and methodologically heterogeneous. Studies differ substantially in (i) the modality and indices used to operationalize synchrony (e.g., movement-, vocal-, and physiology-based measures), (ii) interaction contexts and task demands, and (iii) the populations examined (clinical SAD vs. elevated social anxiety), making it difficult to determine which synchrony characteristics are robust and how they should be measured. This is a critical gap because objective, quantifiable markers relevant to SAD are still limited. Nonverbal synchrony can be measured from observable behavior and physiological signals and may serve as a candidate marker of interpersonal functioning. If reliable and disorder-relevant patterns are established, synchrony measures could support mechanistic research (e.g., interpersonal prediction/co-regulation) and have potential clinical utility, such as complementing the assessment of social functioning/severity and tracking changes over the course of treatment.
Moreover, cognitive-behavioral models of social anxiety emphasize processes such as heightened self-focused attention and the use of safety behaviors in social-evaluative situations, which can undermine effective social performance and interpersonal engagement (e.g., Rapee & Heimberg, 1997). These processes plausibly reduce the responsiveness to a partner’s social signals and may hinder mutual attunement during interactions. This constitutes one pathway through which nonverbal synchrony could be altered in SAD/social anxiety. Empirically, recent studies have begun to quantify nonverbal synchrony in SAD-relevant contexts, including both everyday/experimental interactions and clinical encounters such as psychotherapy sessions, yet their findings remain limited and vary across contexts, modalities, and analytic approaches.
These inconsistencies and gaps motivate the following research questions (RQs): (1) What characteristics/patterns of nonverbal synchrony have been reported in interactions involving individuals with SAD/social anxiety? (2) What sensing technologies, paradigms (interaction contexts/task demands), and analytic methods are used to measure nonverbal synchrony in this literature? (3) How is nonverbal synchrony associated with clinical indicators of SAD/social anxiety (e.g., symptom severity, functional impairment, and treatment processes or outcomes, where available)?
Addressing these questions will clarify the current evidence and methodological landscape, identify key gaps, and inform future mechanistic and clinically oriented research (e.g., assessment and intervention studies). Therefore, we conducted a scoping review to map how nonverbal synchrony has been measured and characterized in SAD/social anxiety, summarize reported patterns and clinical associations, and highlight priorities for future research and clinical translation.
Methods
In preparing this protocol, the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018) statement was used (Supplement File 1). This scoping review also adopted the framework by the Joanna Briggs Institute (JBI) (Peters et al., 2017), which involves following a five-stage approach: Stage 1: Identify the research question; Stage 2: Identify relevant studies; Stage 3: Select studies for review; Stage 4: Chart the data; and Stage 5: Collate, summarize and report the results. The protocol for this study was registered at osf.io (https://osf.io/vqh3d).
Stage 1: Identify the Research Questions
We were interested in the nonverbal synchrony of individuals with social anxiety; therefore, our research questions were as follows: 1. What are the characteristics of nonverbal synchrony in individuals with SAD/social anxiety? 2. How is nonverbal synchrony in individuals with social anxiety measured? 3. What indicators of SAD/social anxiety are reported to be related to nonverbal synchrony in individuals with social anxiety?
Stage 2: Identify Relevant Studies
We used the population, concept, and context (PCC) framework by the JBI for this scoping review (Peters et al., 2017) to define the inclusion criteria as follows:
Participants
Individuals had been diagnosed with SAD based on the APA’s Diagnostic & Statistical Manual of Mental Disorders, 4th or 5th eds. (DSM-IV or DSM-5) or the International Statistical Classification of Diseases and Related Health Problems, 10th or 11th editions (ICD-10, ICD-11). Others were deemed to have a tendency toward SAD through questionnaire scales such as the Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987) or Liebowitz Social Anxiety Scale – Self-Report (LSAS-SR; Baker et al., 2002), the Social Phobia Anxiety Inventory (SPAI; Turner et al., 1989), the Social Phobia Inventory (SPIN; Connor et al., 2000), Mini SPIN (Connor et al., 2001), the Social Phobia Scale (SPS; Mattick & Clarke, 1998), or the Social Interaction Anxiety Scale (SIAS; Mattick & Clarke, 1998).
No stipulations were applied regarding patients’ age, sex, or race. Individuals for whom SAD is not a primary or secondary diagnosis, and those deemed not to have a tendency toward SAD through the LSAS, LSAS-SR, SPAI, or SPIN scales, were excluded. The cut-off point for the LSAS was set at 30 or more points, based on Mennin et al. (2002); for the SPAI, it was 88 points, referencing Peters (2000); for the SPIN it was 19 points or more, based on Connor et al. (2000); and for the Mini SPIN, it was 6 points or more, referencing Connor et al. (2001). This approach is justified by the dimensional view of social anxiety, where clinical and subclinical manifestations are seen as existing on a continuum (Ruscio, 2010).
Concept
Existing studies on the relationship between nonverbal synchrony phenomena and SAD were reviewed, and the characteristics of nonverbal synchrony among individuals with social anxiety, its measurement methods, and indicators related to SAD were examined. This review was limited to interindividual nonverbal synchrony phenomena (including objectively quantified synchrony and, where applicable, structured subjective ratings related to synchrony/attunement) and excluded studies focusing solely on intraindividual nonverbal synchrony.
Context
In this review, nonverbal synchrony was understood as a phenomenon where “the nonverbal behavior of a person seems to be highly interrelated, coordinated, attuned, aligned, or synchronized with the nonverbal behavior of his/her interaction partner” (Altmann et al., 2020, pp. 574–575). Studies on synchrony in brain function, bodily movements, heart rate, and voice were also included.
Types of Studies
This scoping review considered both experimental and quasi-experimental study designs, including randomized controlled trials, non-randomized controlled trials, and before-and-after studies. Prospective and retrospective cohort studies, case-control studies, and cross-sectional studies were also reviewed for inclusion. The review also considered descriptive observational study designs, including case series, individual case reports, and descriptive cross-sectional studies. Review articles, editorials/commentaries, and study protocols were excluded. This study restricted its search to full-text articles written in English or Japanese. Gray literature (e.g., conference abstracts, dissertations/theses, and preprints) was not searched and was excluded. We searched MEDLINE, Embase, CENTRAL, and PsycINFO from database inception to January 31, 2026. To capture the most recent publications, we performed an updated (rolling) search using the same strategy up to the final search date (January 31, 2026). Furthermore, ongoing trials were sought in the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) and ClinicalTrials.gov (Supplement File 2). In addition, we conducted backward and forward citation searching; reference lists of the included studies were screened, and forward citation searching was performed using Web of Science (cited-reference search) to identify studies citing the included articles.
Stage 3: Select Studies
The original literature search was conducted on December 19, 2023. We selected studies following the PRISMA flow diagram. We used the PCC framework, and the process was carried out independently by two researchers (AY and AM). The two authors compared their lists, and any differences in opinion were resolved by discussion and, where this failed, through arbitration by a third researcher (NN).
Stage 4: Chart the Data
Data extraction was carried out by one researcher (AY) using standard data extraction forms including country, journal, diagnosis, sample, age, methods, study type, control, measured outcomes, and conclusion. Another researcher (AM) confirmed the data extraction. If necessary, we contacted the authors of these studies for clarifications.
Stage 5: Collate, Summarize, and Report the Results
We presented the results of the search in a PRISMA flow diagram. We organized the extracted data described above as a qualitative synthesis.
Results
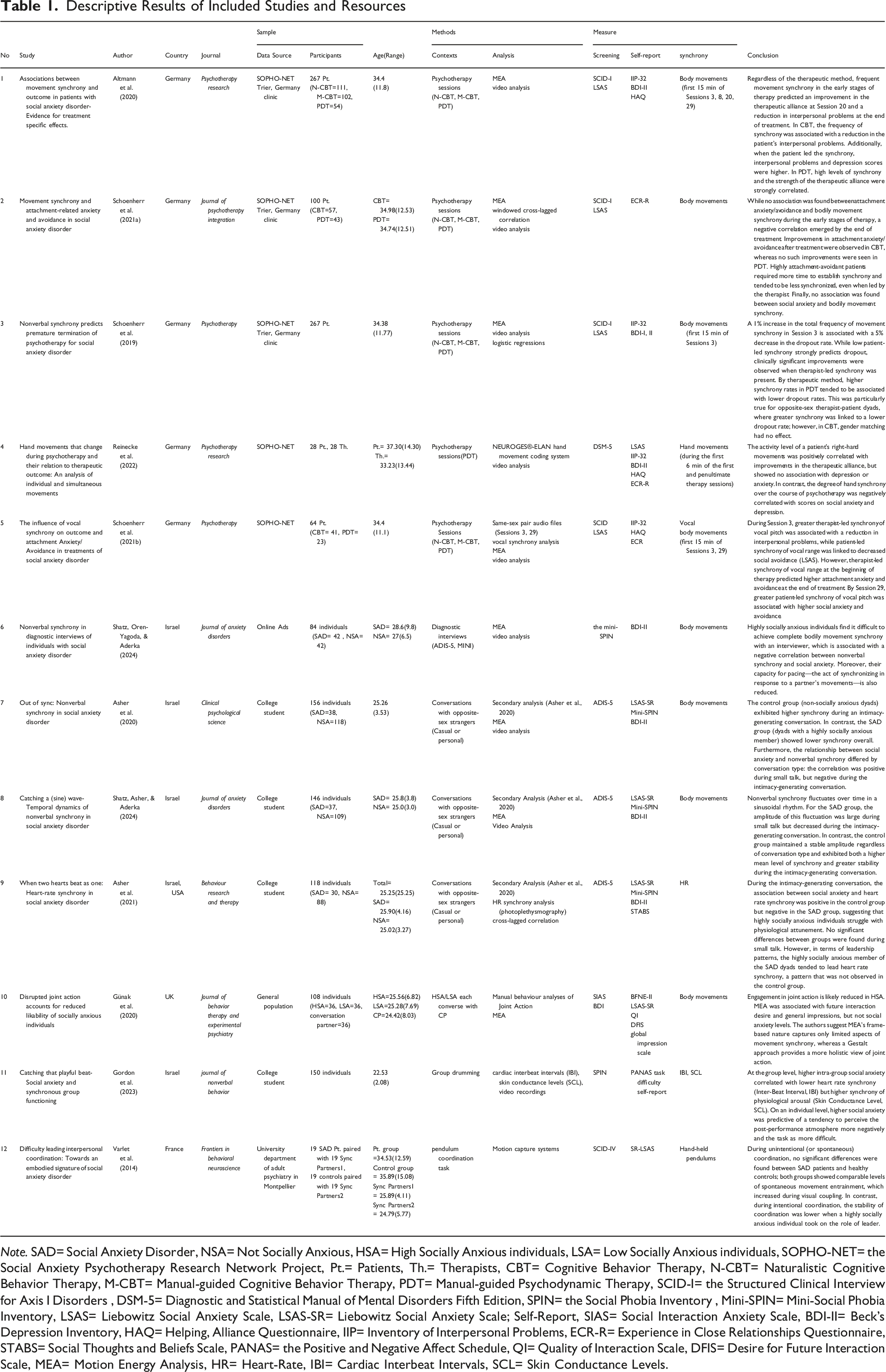
The literature search identified 1,503 records. After removing 519 duplicates, 984 records remained for screening. During the screening of titles and abstracts, 971 records were excluded, leaving 13 reports for eligibility assessment. Of these, two more were excluded because they focused on the wrong population (Supplement File 3). Additionally, one article identified through citation searching was added. Ultimately, 12 studies were included in the review. Figure 1 presents the PRISMA-ScR flow diagram, including reasons for exclusion at each stage. Data were subsequently extracted from the twelve studies (Nos. 1–12) in accordance with the review questions and protocol (Table 1). PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers), **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. From: Page MJ, McKenzie JE. Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: https://www.prisma-statement.org/ Descriptive Results of Included Studies and Resources Note. SAD= Social Anxiety Disorder, NSA= Not Socially Anxious, HSA= High Socially Anxious individuals, LSA= Low Socially Anxious individuals, SOPHO-NET= the Social Anxiety Psychotherapy Research Network Project, Pt.= Patients, Th.= Therapists, CBT= Cognitive Behavior Therapy, N-CBT= Naturalistic Cognitive Behavior Therapy, M-CBT= Manual-guided Cognitive Behavior Therapy, PDT= Manual-guided Psychodynamic Therapy, SCID-I= the Structured Clinical Interview for Axis I Disorders , DSM-5= Diagnostic and Statistical Manual of Mental Disorders Fifth Edition, SPIN= the Social Phobia Inventory , Mini-SPIN= Mini-Social Phobia Inventory, LSAS= Liebowitz Social Anxiety Scale, LSAS-SR= Liebowitz Social Anxiety Scale; Self-Report, SIAS= Social Interaction Anxiety Scale, BDI-II= Beck’s Depression Inventory, HAQ= Helping, Alliance Questionnaire, IIP= Inventory of Interpersonal Problems, ECR-R= Experience in Close Relationships Questionnaire, STABS= Social Thoughts and Beliefs Scale, PANAS= the Positive and Negative Affect Schedule, QI= Quality of Interaction Scale, DFIS= Desire for Future Interaction Scale, MEA= Motion Energy Analysis, HR= Heart-Rate, IBI= Cardiac Interbeat Intervals, SCL= Skin Conductance Levels.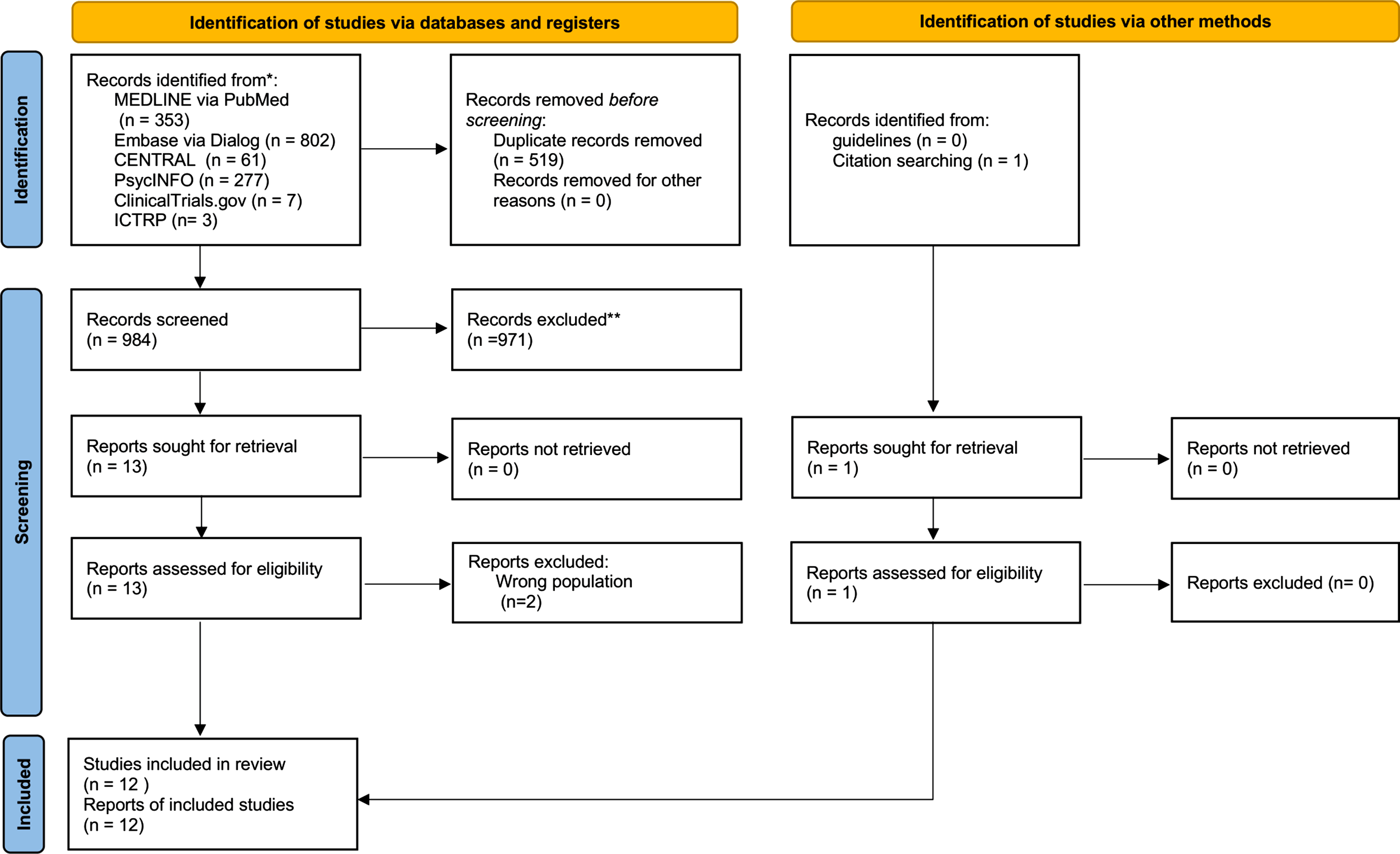
Study Characteristics
Publication years ranged from 2014 to 2024. The review identified six experimental studies, five individual counseling studies (four studies combining CBT and PDT, and one PDT-only study), and one diagnostic interview study. Six studies targeted patients diagnosed with social anxiety disorder, whereas six recruited individuals with high social anxiety. The studies were conducted in Germany (n = 5), Israel (n = 4), Israel and the United States (n = 1), UK (n = 1) and France (n = 1). Recruitment sources included university campuses (n = 5), the Social Anxiety Psychotherapy Research Network Project (SOPHO-NET) (n = 2), a combination of SOPHO-NET and German psychiatric departments (n = 3), French psychiatric departments (n = 1), and online advertisements (n = 1). Diagnostic measures for social anxiety disorder included the ADIS (n = 3), the SCID plus an LSAS score ≥30 (n = 4), the SPIN (n = 2), the SIAS (n = 1), the DSM-5 (n = 1), and the SCID-IV (n = 1). All participants were adults.
Measurements of Nonverbal Synchrony
Across the included studies, nonverbal synchrony in individuals with high social anxiety was assessed via body movement, vocal, and physiological indicators (heart rate, skin-conductance response). The measurement contexts fell into three categories: clinical settings (during therapy or diagnostic interviews), conversations with opposite-sex strangers (light or intimacy-generating conversation, and light conversations with same-sex or opposite-sex strangers), and collaborative tasks (pendulum movement, drumming). Six studies explored synchrony in clinical contexts (Altmann et al., 2020; Reinecke et al., 2022; Schoenherr et al., 2019, 2021a, 2021b; Shatz, Oren-Yagoda, & Aderka, 2024), four in conversational contexts (Asher et al., 2020, 2021; Günak et al., 2020; Shatz, Oren-Yagoda, & Aderka, 2024), and two in collaborative-task contexts (Gordon et al., 2023; Varlet et al., 2014). Nonverbal synchrony was most quantified via video-based body movement analysis; nine studies employed motion energy analysis (MEA). One study recorded hand movements with a hand-held pendulum monitored by a motion-capture system, and another used the NEUROGES®-ELAN hand-movement coding system. Vocal synchrony was examined in one study, and heart-rate synchrony (photoplethysmography) in another, and cardiac interbeat interval (IBI) synchrony and skin conductance level (SCL) synchrony (via electrocardiography and electrodermal activity, respectively), together with behavioral drumming coordination, were assessed in one further study (Gordon et al., 2023).
Measures of Symptoms
Self-report instruments included measures of social-anxiety symptoms (LSAS, SR-LSAS, Mini-SPIN), interpersonal problems (Inventory of Interpersonal Problems-32; Horowitz et al., 1988), therapeutic alliance (Helping Alliance Questionnaire; Alexander & Luborsky, 1986), emotional state (Positive and Negative Affect Schedule; Watson et al., 1988), depressive symptoms (Beck Depression Inventory; Beck et al., 1961), attachment anxiety and avoidance (Experiences in Close Relationships; Brennan et al., 1998), social thoughts and beliefs (Social Thoughts and Beliefs Scale; Turner et al., 2003), Brief Fear of Negative Evaluation Scale revised (BFNE-II; Carleton et al., 2007), and Quality of Interaction Scale (QI; Berry & Hansen, 1996). Although many studies assessed symptoms, depression, anxiety, and alliance, none measured process factors such as self-focused attention, negative self-evaluation.
Discussion
This scoping review synthesized the existing research on nonverbal synchrony between individuals with SAD/social anxiety. Twelve studies met our inclusion criteria; seven relied on primary data and five on secondary analyses, indicating that research in this area is still in its early stages. Overall, individuals with SAD/social anxiety showed difficulties in nonverbal synchrony in specific contexts and roles. Body movement analysis predominated as the measurement approach, and synchrony was chiefly related to social anxiety severity, therapeutic alliance, and interpersonal problems. The findings are discussed below according to the research questions.
Nonverbal Synchrony in Social Anxiety Is Context-dependent and Role-Sensitive
The reviewed studies suggest that disrupted nonverbal synchrony in individuals with SAD/social anxiety is a context- and role-contingent difficulty when evaluative concern intensifies or when the individual is required to assume a high social load role (e.g., leader). Across conversational paradigms, several findings suggest that synchrony may be preserved or even compensated for in relatively low-demand interactions (e.g., small talk). In contrast, it becomes more disrupted when the interaction requires intimate self-disclosure and thus heightens the fear of negative evaluation. Asher et al. (2020, 2021) indicate that synchrony is more likely to deteriorate in contexts involving closer interpersonal engagement, which is consistent with the notion that perceived social threat disrupts synchrony. Shatz, Asher, and Aderka (2024) also report on context-dependent changes that are compatible with a compensatory account. Specifically, some individuals with SAD/social anxiety may attempt to maintain synchrony in low threat settings, but show reduced synchrony when intimacy and evaluative demands increase.
Interactional asymmetry in collaborative tasks also affects synchrony. In particular, Varlet et al. (2014) suggest that synchrony disruptions are most apparent when individuals with SAD/social anxiety must take the lead, implying that performance evaluation and responsibility for coordination can destabilize synchrony even when the task is explicitly cooperative. This role dependence implies that the responsibility for coordination can destabilize synchrony even in explicitly cooperative tasks (Varlet et al., 2014). In clinical assessment contexts, Shatz, Oren-Yagoda, and Aderka (2024) describe reduced “pacing” during diagnostic interviews, which is consistent with the idea that highly evaluative, asymmetric interactions can hinder interpersonal synchronization.
Clinical interaction studies suggest that evaluative pressure is modulated by relationship-specific safety and support. For instance, Altmann et al. (2020) and Schoenherr et al. (2019, 2021a) indicate that higher synchrony early in treatment is associated with more favorable relational/process outcomes (e.g., stronger therapeutic alliance, fewer interpersonal difficulties), implying that a supportive therapeutic relationship may buffer the negative effects of evaluation that are more typical in interactions with strangers. To integrate these cross-context comparisons, we propose an “individual–relationship–context” framework in which synchrony difficulties depend on the interplay of (i) heightened evaluative concern (e.g., intimacy, diagnostic scrutiny), (ii) socially demanding roles (e.g., leadership), and (iii) relational conditions that either mitigate or amplify threats. These findings suggest that reduced synchrony is not a uniform marker but varies systematically by context and role, highlighting the need to consider specific contexts in future mechanism-focused research and clinical assessment.
Measurement Approaches Based on Bodily Movement, Vocal, and Physiological Indicators
Across the included studies, measurement approaches showed both convergence and heterogeneity. Most included studies relied on video-based body movement synchrony, with nine of the twelve studies utilizing Motion Energy Analysis (MEA) to quantify frame-by-frame pixel changes as an index of whole-body movement (Altmann, 2013). This preference suggests that the field favors an accessible, non-invasive approach that can be applied across various contexts, including conversations, diagnostic interviews, and psychotherapy sessions. The remaining studies employed alternative methods, such as structured behavioral ratings, vocal synchrony indices, or physiological coupling measures.
Quantitative findings also indicate that measurement choice can shape conclusions. For instance, Günak et al. (2020) found that observer-rated joint action showed an indirect effect on likability (b = −0.55 to −1.89), whereas MEA-based synchrony was not associated with the corresponding outcome (p = 0.789). This divergence suggests that automated movement covariation and human-rated coordination may capture different aspects of social interaction. Physiological measures also showed modality-specific patterns. Gordon et al. (2023) noted that group-level social anxiety was negatively associated with heart-rate timing synchrony indexed by interbeat intervals (p = 0.001), but positively associated with skin conductance level synchrony (p = 0.036). These opposing patterns imply that different physiological channels may reflect distinct processes, such as coordination and stress contagion.
Several studies used directional or time-lagged indices that go beyond symmetric correlation-based metrics. For example, in diagnostic interviews, pacing was significantly reduced in participants with SAD (p = 0.004, partial η 2 = 0.095), whereas leading was not significantly different (Shatz, Oren-Yagoda, & Aderka, 2024). Such indices may be particularly informative in asymmetric, evaluative interactions because they distinguish responsiveness from initiative. Finally, despite the recent emergence of inter-brain synchrony (InBS) research in social neuroscience, no included study assessed InBS in SAD or social anxiety. Overall, the operationalization of synchrony varies across modalities and contexts. These measurement choices, including modality and directionality, may shape conclusions and should be reported more transparently in future research.
Social Anxiety Indicators and Clinical Outcomes Associated With Nonverbal Synchrony
The included studies suggest that nonverbal synchrony relates to both symptom severity and clinically relevant relational or process outcomes. In non-clinical and experimental interactions, higher social anxiety severity was consistently associated with greater difficulty in achieving synchrony (Asher et al., 2020; Reinecke et al., 2022; Shatz, Asher, & Aderka, 2024). This pattern indicates that synchrony difficulties scale with symptom severity. In psychotherapy contexts, several studies suggest prognostic value. Schoenherr et al. (2019) reported that a 1% increase in early-session synchrony was associated with a 5% reduction in early dropout risk (hazard ratio = 0.95, p < 0.05). Altmann et al. (2020) also reported that body-movement synchrony predicted improvements in therapeutic alliance and interpersonal problems (IIP) (β = 0.20–0.30). These findings support the view that body synchrony can function as a process-relevant marker in treatment.
However, these findings also indicate that higher synchrony is not universally beneficial. Altmann et al. (2020) reported that greater patient-led synchrony at Session 8 was associated with worse end-of-treatment IIP and depressive symptoms (p < 0.05). Vocal synchrony results point in a similar direction. Schoenherr, Strauss, Stangier, and Altmann (2021) found that higher vocal synchrony was positively associated with attachment anxiety and avoidance at treatment end (β = 0.25–0.32). Taken together, these results suggest that the meaning of synchrony depends on who drives it and in which modality it is expressed. Therapist-led synchrony may facilitate a secure therapeutic environment, whereas patient-led or excessive synchrony might reflect maladaptive emotion regulation or over-accommodation.
In addition to social anxiety severity, depressive symptoms in some studies were found to covary with synchrony. This raises the possibility that synchrony reflects broader interpersonal and affective functioning, rather than SAD specific mechanisms alone. Importantly, no included study directly tested whether core cognitive mechanisms in SAD, such as self-focused attention, negative self-evaluation, or fear of negative evaluation, explain synchrony disruptions. Future work should integrate multimodal and directional synchrony analyses with designs that can test mechanisms and track changes during the course of treatment.
Limitations and Future Directions
Several limitations should be noted. First, generalizability is constrained by our search being limited to English- and Japanese-language literature and by the included studies being concentrated in Western and Middle Eastern contexts. The direct comparison of findings is also hindered by the equivalent treatment of clinical and laboratory settings. Conceptually, the review is limited by the absence of studies examining cognitive mediators such as metacognition, and whether the observed patterns are specific to SAD remains unclear given the lack of clinical control groups (e.g., other anxiety or depressive disorders). Finally, no included studies assessed inter-brain synchrony (InBS). Future research employing hyperscanning techniques (e.g., EEG or fNIRS) should test whether individuals with social anxiety exhibit altered synchrony in neural circuits related to social cognition or threat processing (Saul et al., 2022). Identifying such neural patterns, alongside cognitive and behavioral measures, will be essential to refine pathophysiological models of SAD and to explore whether interventions designed to enhance multimodal synchrony can directly improve treatment outcomes.
Conclusion
This review mapped the characteristics, measurement methods, and associated indicators of nonverbal synchrony in individuals with high social anxiety, highlighting current knowledge gaps. Difficulties in physical, physiological, and vocal synchrony arise from factors related to symptom severity, relational dynamics, and context, especially when socially anxious individuals assume leadership roles. While MEA is the predominant measurement technique, advances in multimodal, ecologically valid, and culturally inclusive research are essential for deepening understanding and improving interventions. In particular, incorporating neural measures is crucial.
Supplemental Material
Supplemental material - Nonverbal Synchrony Between Individuals With Social Anxiety and Others for a Scoping Review
Supplemental material for Nonverbal Synchrony Between Individuals With Social Anxiety and Others for a Scoping Review by Ayaka Yanagida, Akira Matsumoto, Shunsuke Taito, Masahiro Banno, Hitomi Oi, Takayuki Iwayama, Shun Nakajima, Hiroku Noma, Ayako Saneyoshi and Nanako Nakamura-Taira in Psychological Reports
Supplemental Material
Supplemental material - Nonverbal Synchrony Between Individuals With Social Anxiety and Others for a Scoping Review
Supplemental material for Nonverbal Synchrony Between Individuals With Social Anxiety and Others for a Scoping Review by Ayaka Yanagida, Akira Matsumoto, Shunsuke Taito, Masahiro Banno, Hitomi Oi, Takayuki Iwayama, Shun Nakajima, Hiroku Noma, Ayako Saneyoshi and Nanako Nakamura-Taira in Psychological Reports
Supplemental Material
Supplemental material - Nonverbal Synchrony Between Individuals With Social Anxiety and Others for a Scoping Review
Supplemental material for Nonverbal Synchrony Between Individuals With Social Anxiety and Others for a Scoping Review by Ayaka Yanagida, Akira Matsumoto, Shunsuke Taito, Masahiro Banno, Hitomi Oi, Takayuki Iwayama, Shun Nakajima, Hiroku Noma, Ayako Saneyoshi and Nanako Nakamura-Taira in Psychological Reports
Footnotes
Consent to Participate
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Contributions
A.Y. conceptualized the study, conducted the literature search, and wrote the original draft. A.Y. and A.M. performed the literature screening. N.N. supervised the project. All other authors contributed to the critical review and editing of the manuscript. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI Grant 23H01043.
Declaration of Conflicting Interests
S.N. has received research funding unrelated to the present study from Nomura Real Estate Development Co., Ltd., S’UIMIN Inc., Tsukuba City (Ibaraki, Japan), and Mitsubishi Electric Corporation. N.N. has received research funding unrelated to the present study from Mitsubishi Electric Corporation. The other authors declare no competing interests.
Data Availability Statement
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.