
Abstract
Objectives:
COVID-19 testing is an important strategy to limit the spread of COVID-19 and improve health outcomes. Although health care providers (hereinafter, providers) decide which strategies to implement to improve access to testing, they may not have fully accurate impressions of the barriers faced by patients. We examined patient and provider perspectives on barriers to COVID-19 testing.
Methods:
We surveyed 788 patients and 77 providers working at 5 health care organizations in the United States that served urban American Indian and Alaska Native people from January through May 2021. We asked patients and providers about barriers to COVID-19 testing and possible strategies that could improve access to testing. We compared patient and provider perspectives by using descriptive statistics and logistic regression; percentages were weighted.
Results:
Overall, we observed a high level of congruence among patients and providers regarding perceived efficacy of strategies to increase testing. Difficulty finding transportation to the clinic was the least commonly reported barrier by patients (14%) but was the most frequently cited barrier by providers (73%). The most commonly reported barrier by patients was concern for contracting COVID-19 during an in-person appointment (43%). Two strategies, providing mobile testing units (76%) and offering monetary incentives (57%), were not commonly used but were endorsed by most patients and providers.
Conclusions:
Overall, patient and provider perspectives were highly congruent on perceived barriers to and strategies to facilitate COVID-19 testing. Research on barriers to testing for communicable diseases such as COVID-19 should systematically examine perspectives of both patients and providers to identify potentially effective interventions.
American Indian and Alaska Native (AI/AN) communities have been at the forefront of COVID-19 preventive measures and have achieved high rates of testing and vaccination. 1 Individual and community-level responses highlight the speed and efficiency at which AI/AN people and health care agencies were willing and able to respond to the pandemic. A key component of those responses has been COVID-19 testing; testing is essential for early identification of cases, contact tracing, and isolation, which are crucial for controlling the spread of SARS-CoV-2 and providing early treatment for severe cases. 2
AI/AN communities experience unique facilitators and challenges that can affect their access to COVID-19 testing services. Facilitators include tribal government structures with local decision-making abilities, health care through Indian Health Service or tribal health care organizations, and cultural values that stress the importance of community and caring collectively for elders. 3 Challenges include geographic isolation, insufficient funding of health care and social services, and limited access to health care facilities. 4 Health care leaders, such as administrators and providers, create strategies to reduce barriers to testing; eliciting patient perspectives on barriers and solutions to COVID-19 testing and determining whether they differ from health care providers’ (hereinafter, providers) perspectives can be valuable for designing those strategies.
In this study, we surveyed patients and providers at 5 geographically dispersed tribal health care organizations in the United States that primarily serve AI/AN people living in urban settings to examine barriers to COVID-19 testing and strategies to increase COVID-19 testing. To our knowledge, this is the first study to compare patient and provider perspectives on barriers to COVID-19 testing among AI/AN people. Our findings could be used to reduce barriers among AI/AN populations to obtaining health care, which may otherwise not be obvious to policy decision makers.
Methods
Study Design
We designed Community Organizations for Natives: COVID-19 Epidemiology, Research, Testing, and Services (CONCERTS) to increase COVID-19 testing and vaccination among urban AI/AN people and to address COVID-19–related health disparities in this population. We created and implemented a cross-sectional survey in partnership with 5 health care organizations that primarily serve AI/AN people in urban settings to identify barriers, facilitators, attitudes, and risk factors for COVID-19 testing and vaccination (Supplemental Methods in the Supplement). We distributed links to online questionnaires by mail or email to patients and providers at all organizations. The health care organizations participating in CONCERTS served 5 urban areas: (1) Albuquerque, New Mexico; (2) Anchorage, Alaska; (3) Denver, Colorado; (4) Minneapolis-St. Paul, Minnesota; and (5) Wichita, Kansas. In 2019, from 1269 to 25 043 unique patients visited clinics in these organizations.
The Washington State University Institutional Review Board (no. 18590), the Alaska Area Institutional Review Board (no. 2020-11-044), local health care organization review boards, and the Indian Health Service National Institutional Review Board approved the study. In addition, tribal research review committees at Southcentral Foundation and the Alaska Native Tribal Health Consortium reviewed and approved the study and the dissemination of results. Before starting the survey, participants gave informed consent.
Study Population
We included patients who had been seen at clinics of the 5 health care organizations in the year before the survey; eligible patients were aged ≥18 years, AI/AN, and not diagnosed with dementia or other serious cognitive issues (International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] codes F01-04, G30, or G31). 5 To ensure that we enrolled enough older participants at highest risk of severe COVID-19, we stratified sampling by age (aged 18-54 y [adult group] vs aged ≥55 y [older adult group]).
Each clinic generated a list of eligible patient participants from their electronic health records (EHRs) and then randomly sampled 200 patients in each age group. We invited each clinic sample group to participate by using a multipronged strategy. We emailed invitations to patients who had an email address documented in the EHR to participate in CONCERTS, which included a link to an online Research Electronic Data Capture (REDCap) survey. 6 We mailed invitations to patients without an email address. Patients received up to 4 reminders (by email or telephone call, depending on the data collection mode) during a 14-day period. We aimed to enroll up to 150 patients per clinic. If we could not achieve this sample size through the first round of emails, letters, and telephone calls, we selected a new random sample of eligible patients from the EHR.
We included providers who were employed full-time or part-time at 1 of the 5 health care organizations for at least 1 year. We included providers who were physicians, physician assistants, nurses, and nurse practitioners. Clinic directors identified eligible providers at each clinic, and we sent identified providers links via email to complete the REDCap survey.
Patients and providers completed questionnaires from January through May 2021 and received $100 in Visa, Mastercard, or Amazon gift cards as compensation.
Measures
We surveyed patients and providers on multiple demographic factors. For patients, we examined the following demographic factors: sex (female, male), current marital status (married or member of an unmarried couple; divorced, separated, or widowed; never married), and education (<high school/no diploma; high school diploma or General Educational Development [GED]; associate, occupational, technical, or vocational degree; ≥college degree).
For patients, we assessed 4 barriers to testing with the following questions: (1) “How easy or difficult is it for you currently to travel to your clinic for an appointment?” (2) “How easy or difficult is it for you to go to the clinic during the hours it is open?” (3) “How concerned are you about the cost of getting a test for COVID-19?” and (4) “How concerned are you about getting infected with COVID-19 during an in-person appointment at your clinic?” We dichotomized the responses for all questions to “somewhat or very difficult/somewhat or very concerned” and “somewhat or very easy/not at all or a little.”
We questioned providers on how often patients in their clinic told them about barriers that they encountered in the past month (eTable in the Supplement) based on barriers assessed among patients: problems getting transportation to the clinic, difficulties attending clinic during open hours, concern about getting a SARS-CoV-2 test because of cost, and concerns about contracting SARS-CoV-2 at the clinic. We dichotomized responses for all questions to “often or sometimes” and “seldom or never.”
We asked patients and providers questions on 10 strategies to increase COVID-19 testing among patients: (1) providing drive-through testing at or near your clinic; (2) increasing social distancing at your clinic; (3) providing mobile testing unit close to home; (4) participating in testing at the same time as your family or friends; (5) receiving an incentive for being tested; (6) providing clinic staff to help you with social services; (7) having testing available at a place in the community that was safe and familiar; (8) having testing that was simple, quick, and easily administered; (9) having test results available on the same day; and (10) having free tests.
For each strategy, we asked patients, “How likely would you be to get tested for COVID-19 if the following strategies were available?” (extremely likely, very likely, moderately likely, slightly likely, not at all likely). For each strategy, we asked providers, “How effective do you think the following strategies would be at increasing SARS-CoV-2 testing at your clinic?” We combined responses into “extremely or very effective,” “moderately or slightly effective,” “not at all effective,” and “already using this strategy.” For participants, we dichotomized responses into “already using this strategy, or extremely or very effective” and “moderately to not at all effective” to estimate risk differences.
Statistical Analysis
We compared patient and provider perspectives on the 4 barriers to testing and 10 strategies to improve access to testing by examining the relative proportion of responses to each barrier or strategy and by estimating the risk difference using logistic regression with robust SEs. We analyzed all data with inverse probability weights to improve the generalizability of our findings. For providers, we generated probability weights to give equal weighting to each clinic. For patients, we gave equal weighting to each clinic and we also corrected for sample selection based on age and sex. We conducted a supplementary analysis in which we compared clinics (Supplemental Analysis in the Supplement). We used Stata version 17.0 (StataCorp) for all analyses.
Results
Characteristics of Patients and Providers
Of the 4603 eligible patients who were contacted for this study, 788 (17%) were enrolled and completed the survey (Table 1). Overall, 60% were female, 93% had ≥high school degree, and 42% were married or a member of an unmarried couple (weighted percentages).
Characteristics of adult American Indian and Alaska Native patients seen at 5 geographically dispersed health care organizations and surveyed on barriers to COVID-19 testing and strategies to improve access to testing, January–May 2021 a
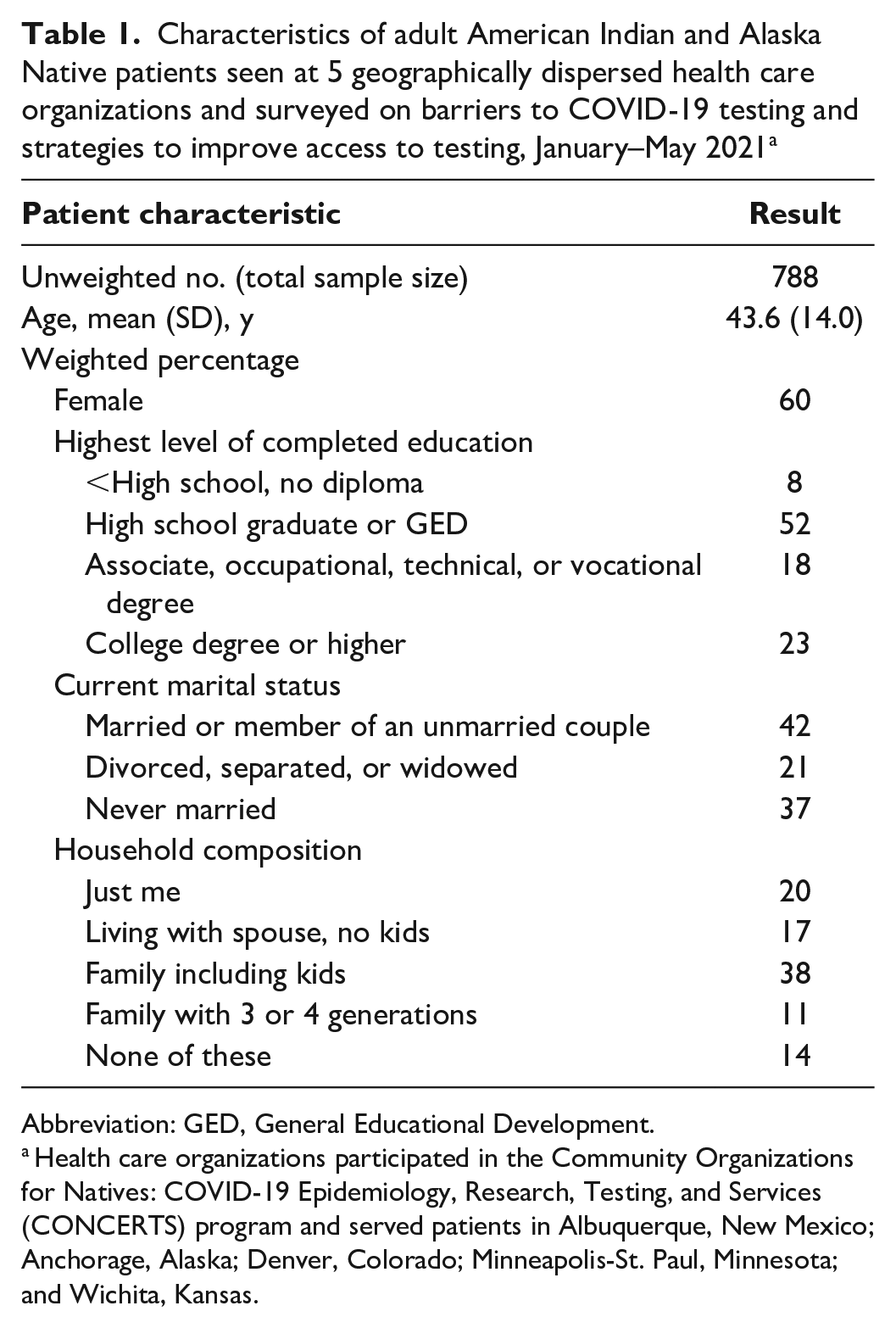
Abbreviation: GED, General Educational Development.
Health care organizations participated in the Community Organizations for Natives: COVID-19 Epidemiology, Research, Testing, and Services (CONCERTS) program and served patients in Albuquerque, New Mexico; Anchorage, Alaska; Denver, Colorado; Minneapolis-St. Paul, Minnesota; and Wichita, Kansas.
Of 77 providers who completed some or all of the questions related to COVID-19 testing, 49% were employed by the Southcentral Foundation (Anchorage). The 4 provider types (physicians, physician assistants, nurses, nurse practitioners) were represented in roughly the same proportions (20%-27%), and 19% of all providers were AI/AN.
Barriers to Testing
Among patients, the most common barrier to testing was concern about contracting COVID-19 during an appointment (43%), followed by difficulty reaching the clinic during open hours (20%) and concern about the cost of testing (19%) (weighted percentages). Only 14% of patients indicated that traveling to the clinic for an appointment was a barrier (Table 2).
Barriers to COVID-19 testing reported by American Indian and Alaska Native patients and their health care providers at 5 geographically dispersed health care organizations, surveyed in January–May 2021 a
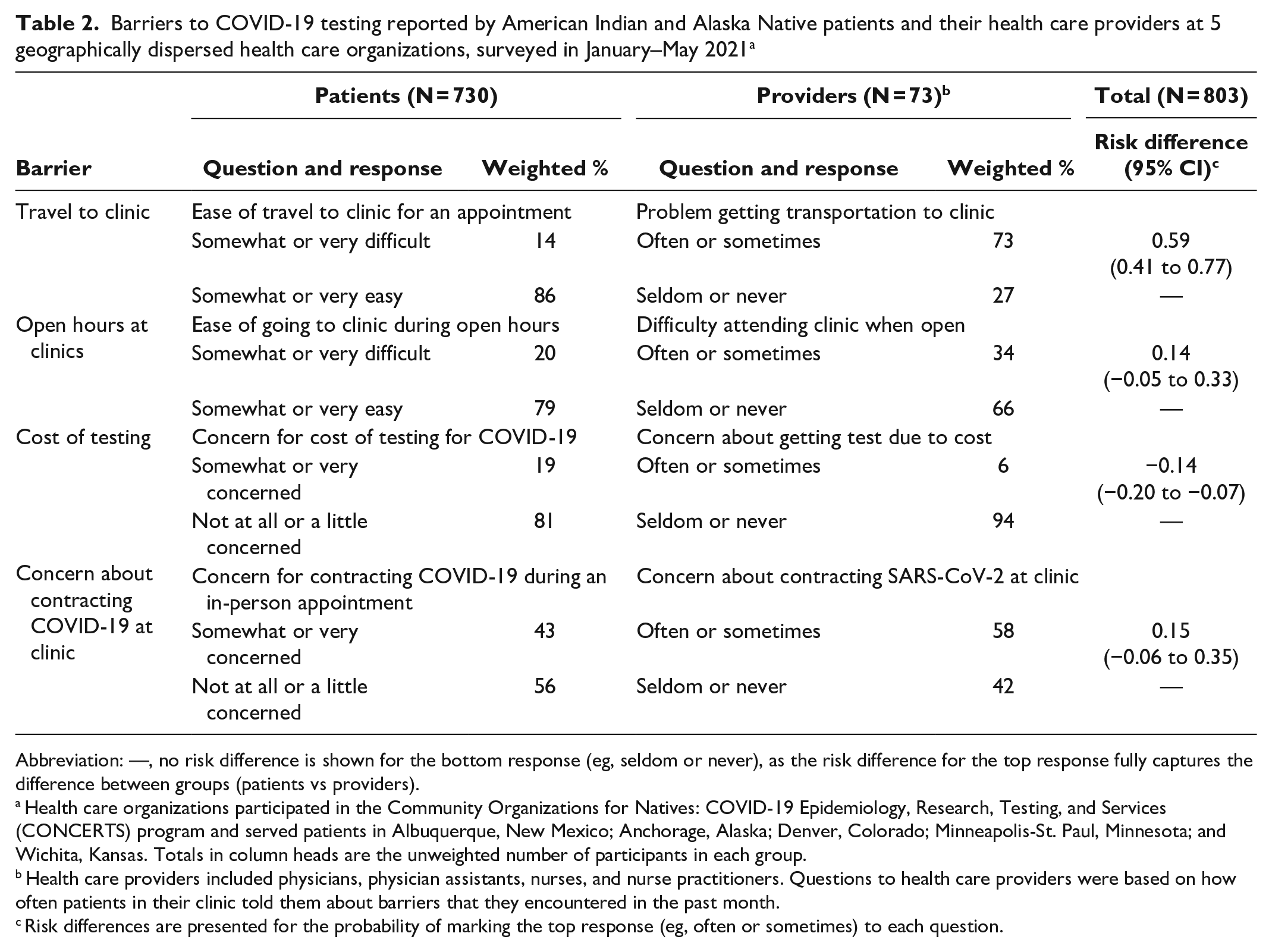
Abbreviation: —, no risk difference is shown for the bottom response (eg, seldom or never), as the risk difference for the top response fully captures the difference between groups (patients vs providers).
Health care organizations participated in the Community Organizations for Natives: COVID-19 Epidemiology, Research, Testing, and Services (CONCERTS) program and served patients in Albuquerque, New Mexico; Anchorage, Alaska; Denver, Colorado; Minneapolis-St. Paul, Minnesota; and Wichita, Kansas. Totals in column heads are the unweighted number of participants in each group.
Health care providers included physicians, physician assistants, nurses, and nurse practitioners. Questions to health care providers were based on how often patients in their clinic told them about barriers that they encountered in the past month.
Risk differences are presented for the probability of marking the top response (eg, often or sometimes) to each question.
The most common barrier that providers heard from patients was transportation (73%), followed by concerns about getting COVID-19 at the clinic (58%). Only 6% of providers reported that they heard concerns about the cost of testing compared with 19% of patients who reported that concern.
Whereas 14% of patients indicated that it was somewhat or very difficult to travel to the clinic for an appointment, 73% of providers indicated that their patients often or sometimes had problems getting transportation to the clinic, a difference of 59 percentage points.
Strategies to Increase Testing
Overall, patients strongly supported all 10 strategies to increase COVID-19 testing (Table 3). The 3 strategies that most patients indicated would make them extremely or very likely to get tested for COVID-19 were drive-through testing (79%); a simple, quick, and easily administered test (86%); and a free test (87%).
Strategies to reduce barriers to COVID-19 testing reported by American Indian and Alaska Native patients and their health care providers at 5 geographically dispersed health care organizations, surveyed in January–May 2021 a
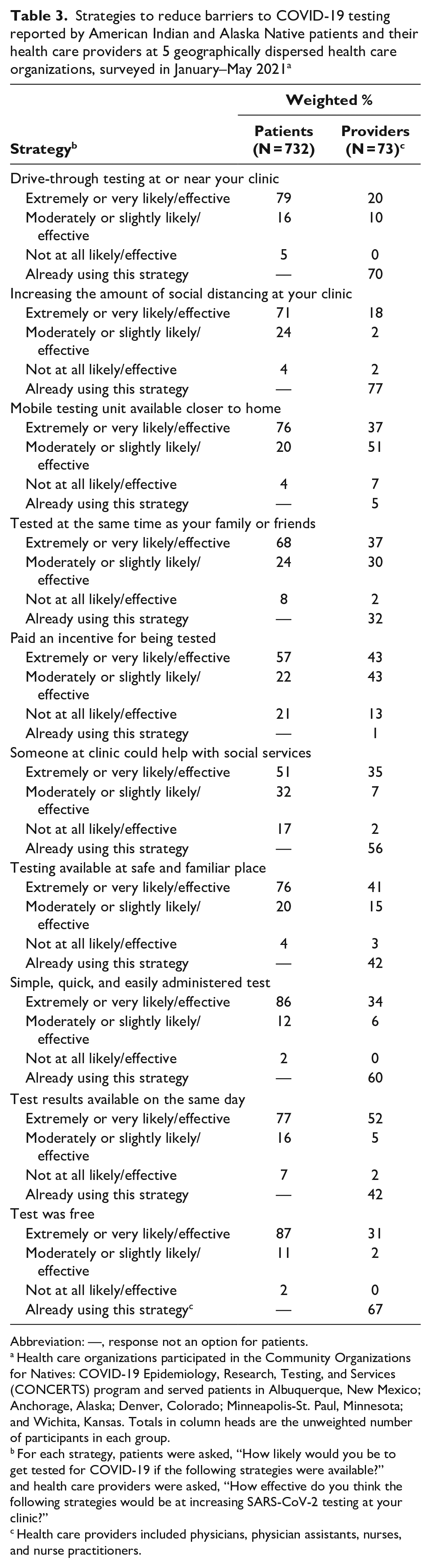
Abbreviation: —, response not an option for patients.
Health care organizations participated in the Community Organizations for Natives: COVID-19 Epidemiology, Research, Testing, and Services (CONCERTS) program and served patients in Albuquerque, New Mexico; Anchorage, Alaska; Denver, Colorado; Minneapolis-St. Paul, Minnesota; and Wichita, Kansas. Totals in column heads are the unweighted number of participants in each group.
For each strategy, patients were asked, “How likely would you be to get tested for COVID-19 if the following strategies were available?” and health care providers were asked, “How effective do you think the following strategies would be at increasing SARS-CoV-2 testing at your clinic?”
Health care providers included physicians, physician assistants, nurses, and nurse practitioners.
Although 67% of providers noted the COVID-19 test was already free at their clinic, a weighted 94% of providers at clinics where the test was not free thought a free test would likely increase testing. Similarly, 70% noted that drive-through testing was already available at their clinic; among providers at clinics that did not have drive-through testing, a weighted 66% of providers reported that drive-through testing would be extremely or very likely to increase testing. Among providers, 60% thought the test at their clinic was simple, quick, and easily administered; however, among providers who did not have this perception, a weighted 85% indicated that such a test would be extremely or very likely to increase testing.
Several strategies not commonly used by the clinics in this study had support from patients. Only 1% of providers reported that incentives to get tested were available, yet 57% of patients thought incentives would be extremely or very likely to encourage them to get tested. Although 5% of providers reported that their clinic had mobile testing units that could travel closer to patients’ homes, 76% of patients answered that availability of mobile testing units would make them extremely or very likely to get tested. Similarly, 42% of providers reported that tests were available at a place in the community that was safe and familiar, and 76% of patients stated that this strategy would make them extremely or very likely to get tested. Lastly, 32% of providers reported the availability of getting tested at the same time as family and friends, and 68% of patients felt this approach would make them extremely or very likely to get tested.
Increasing social distancing (risk difference = 0.24; 95% CI, 0.18-0.30) and having someone to help with social services (risk difference = 0.40; 95% CI, 0.32-0.48) were both strategies that were more common among providers as already implemented or endorsed than considered by patients as a way to increase COVID-19 testing (Table 4).
Estimated difference between perspectives of American Indian and Alaska Native patients and their health care providers at 5 geographically dispersed health care organizations on strategies to increase COVID-19 testing, surveyed in January–May 2021 a
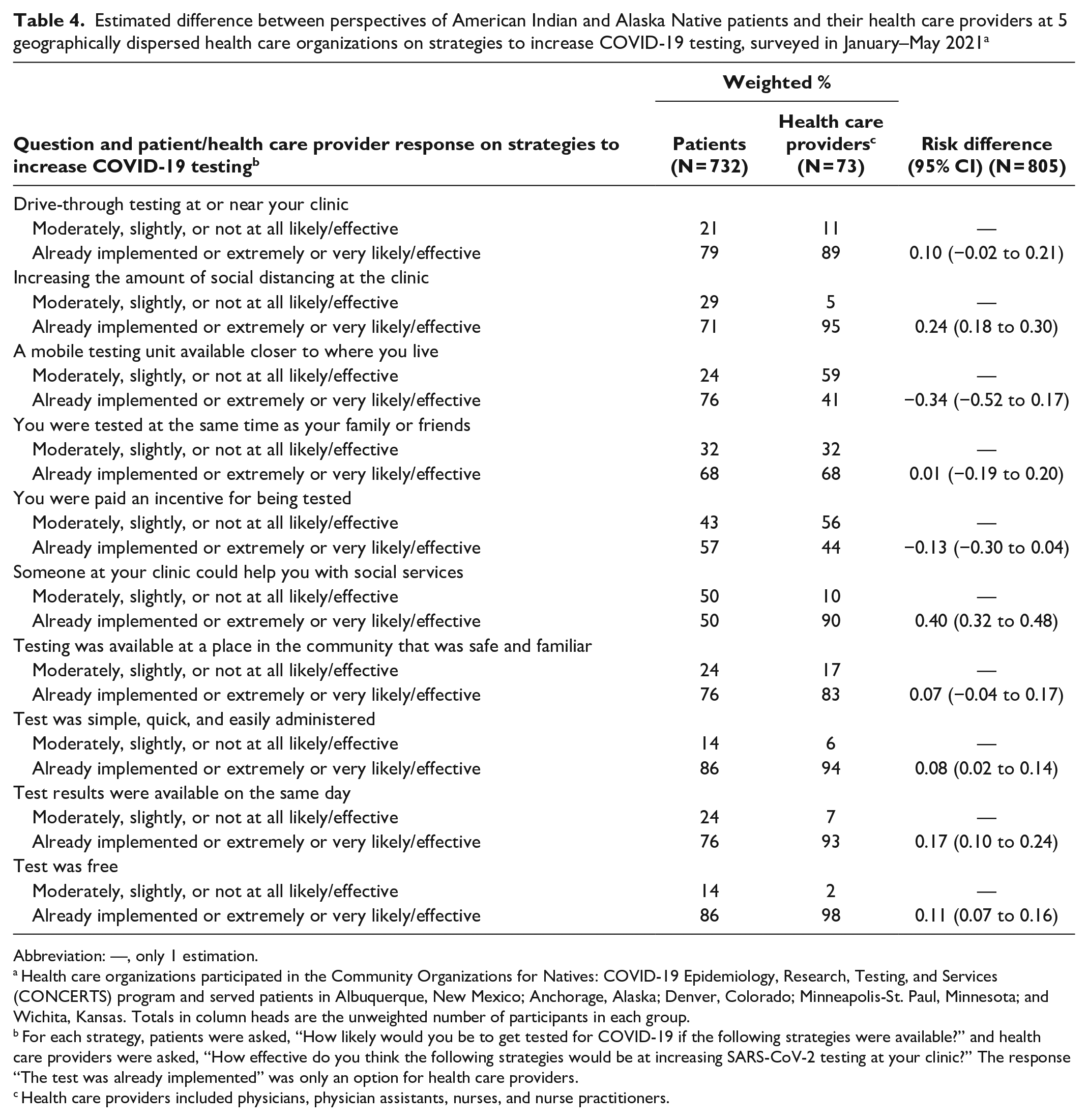
Abbreviation: —, only 1 estimation.
Health care organizations participated in the Community Organizations for Natives: COVID-19 Epidemiology, Research, Testing, and Services (CONCERTS) program and served patients in Albuquerque, New Mexico; Anchorage, Alaska; Denver, Colorado; Minneapolis-St. Paul, Minnesota; and Wichita, Kansas. Totals in column heads are the unweighted number of participants in each group.
For each strategy, patients were asked, “How likely would you be to get tested for COVID-19 if the following strategies were available?” and health care providers were asked, “How effective do you think the following strategies would be at increasing SARS-CoV-2 testing at your clinic?” The response “The test was already implemented” was only an option for health care providers.
Health care providers included physicians, physician assistants, nurses, and nurse practitioners.
Discussion
In this study, we assessed patient perspectives on barriers to COVID-19 testing and strategies to improve testing and provider awareness of these perspectives among 5 health care organizations that primarily serve urban AI/AN people. Among barriers, the largest gap in perspective between patients and providers was difficulty finding transportation to the clinic, which was an uncommon barrier reported by patients but a common barrier reported by providers, who claimed to have heard about this barrier from patients. Conversely, a higher percentage of patients than providers reported concerns about the cost of testing. Two strategies—monetary incentives to test and mobile testing units—were endorsed by many patients but not often indicated by providers as an option available at their clinics.
Some discrepancies on barriers to and strategies of COVID-19 testing between patient preferences and provider awareness point to the importance of patient engagement in the health care system. Patient engagement can be effective in improving the delivery of health care services and improving health care governance through various pathways, including unidirectional feedback and codesign of care processes. 7 Our work similarly highlighted that patient perspectives can lead to improved care by providing better information for provider decision-making than simply relying on informal feedback from patients and casual provider observations.
A study of First Nations, Inuit, and Métis people living in Toronto, Canada, reported that cumulative COVID-19 testing rates among the study group were 10.2% higher than local age-adjusted city and provincial rates. 8 These higher testing rates were credited to effective mobilization by Indigenous community groups who overcame barriers to testing. However, future endeavors must solicit patient perspectives to intentionally act on their feedback. As noted by Bombard et al, 7 patients can be frustrated if their requests are denied or if decisions about clinic policy about which they are giving their perspectives have already been made, rendering their input meaningless and symbolic. In a rapidly evolving situation, such as during the initial outbreak of COVID-19, providers should move quickly to elicit patient feedback when appropriate to design and enact optimal policies and to strengthen patient–provider relationships.
Our data cannot address the reasons for the observed discrepancies between patients and providers. One possible explanation is that some barriers or strategies were important to some patients who faced them, meaning that, even if only a minority of patients faced those barriers, providers would be likely to hear from the affected minority. For example, transportation issues could be critical for a minority of patients who experience them. Alternatively, patients may feel more comfortable voicing their concerns about some barriers than others.
The association between economic conditions and difficulties in accessing COVID-19 testing was consistent with another study that found the ability to pay for treatment and the ability to work after a positive test result were important considerations for whether respondents, particularly Black or Latino people, would test for COVID-19. 9
Free testing, drive-through testing, and simple, quick, and easily administered tests were strongly endorsed by most patients and by providers at clinics where those strategies were not available. Two strategies, notably mobile testing units and monetary incentives, were not commonly used policies but were endorsed by most patients and providers. AI/AN communities have implemented monetary incentives for COVID-19 vaccination, 10 which have been shown to increase COVID-19 vaccination rates in other populations 11 and have increased testing for other viruses, including HIV. 12 More research is warranted to understand the desirability, feasibility, and effects of incentives and mobile testing programs in AI/AN populations.
Despite 63% of patients in our study receiving a COVID-19 vaccine, which would presumably decrease the demand for testing by some amount among those who were vaccinated, we believe the barriers and strategies that we assessed are unlikely to be affected by general demand for testing or be contingent on a patient’s own vaccination status.
Overall, we found a high level of congruence between patient and provider perspectives. This congruence demonstrates that providers at these clinics had a strong grasp on what their patient populations needed to access COVID-19 testing and suggests that communication between patients and providers was strong. We had predetermined the assessed strategies, and providers reported that many of the strategies were already in use, consistent with the overall dynamic and exceedingly rapid and resourceful response to the COVID-19 pandemic by AI/AN communities and providers. When surveys were conducted (January–May 2021), COVID-19 testing was widely available both at the clinics that partnered for this study and at nearby testing sites operated by other health care systems, but, in general, patients did need to go to a testing facility. We were not able to assess whether barriers to testing specifically at the clinics of the 5 included health care organizations led patients to seek care elsewhere. The US government did not implement its policy of providing free at-home tests until January 2022; as of November 2021, data from the Centers for Disease Control and Prevention showed that, among respondents who took a COVID-19 test in the previous 30 days, fewer than 10% had taken an at-home test. 13 Although our 5 partner organizations no longer prioritize providing COVID-19 testing to patients, the lessons from COVID-19 are important for implementing effective responses to future pandemics or other health care challenges. In addition, with changes in testing costs, we may observe similar barriers as new variants of COVID-19 emerge.
Limitations and Strengths
Our study had several limitations. First, we did not ask patients and providers about an exhaustive list of potential barriers to testing, especially barriers specific to AI/AN concerns. Additional barriers or strategies that we did not explore may be valuable to other practitioners and researchers in efforts to enhance patient care. Second, because of the period when our study was designed and implemented, we did not inquire about at-home COVID-19 testing; thus, our results are not pertinent to at-home testing. In addition, barriers to disease testing at clinics may differ when at-home testing is widely available. Third, the large sample size and the lack of resources to analyze write-in data prevented us from collecting patient- or provider-generated ideas on barriers to testing or strategies to reduce barriers to testing. Fourth, this study captured data on just a 6-month window of the pandemic, so we cannot know how such barriers changed over time. Fifth, our response rate (17%) was low with unknown selection biases (unknown characteristics between respondents and nonrespondents), although this response rate was similar to that of a 2021 study of COVID-19–related discrimination in diverse populations. 14 Survey respondents likely differed substantially from nonrespondents, thereby limiting generalizability to populations who are not represented by the sample and chose to participate in this study.
A major strength of our study was that CONCERTS participants constitute the most comprehensive and geographically inclusive sample of urban AI/AN populations during the COVID-19 pandemic. Thus, our findings, although not representative of the entire diversity of perspectives and experiences of AI/AN people, are likely to be relevant to other AI/AN populations.
Conclusions
Although patient and provider perspectives on barriers to and strategies to facilitate COVID-19 testing at health care organizations that serve urban AI/AN people were overall congruent, some discrepant views emerged, including the view on transportation-related barriers to COVID-19 testing and the strategies of having mobile testing and monetary incentives. These discrepancies highlight areas warranting close attention by health care organizations seeking to make changes. Discrepancies in perspectives about barriers to traveling to testing suggested an outsized influence on subsequent policy. More research is needed on mobile testing and monetary incentives, programs that are rarely used but endorsed by patients and providers as potentially effective. Research on barriers to testing for communicable diseases such as COVID-19 should systematically examine perspectives of both patients and providers to identify potentially effective interventions.
Supplemental Material
sj-docx-1-phr-10.1177_00333549251341242 – Supplemental material for Barriers to COVID-19 Testing Among American Indian and Alaska Native People: Comparing Perspectives of Patients and Providers
Supplemental material, sj-docx-1-phr-10.1177_00333549251341242 for Barriers to COVID-19 Testing Among American Indian and Alaska Native People: Comparing Perspectives of Patients and Providers by Austin Henderson, Krista Schaefer, Richard Maclehose, Spero M. Manson and Dedra Buchwald in Public Health Reports®
Footnotes
Acknowledgements
The authors thank the research participants who shared their thoughts and intentions about COVID-19 testing. The authors also acknowledge Odile Lallemand, MPH (Institute for Research and Education to Advance Community Health, Washington State University), Katie Nelson, MS (Center for Nutrition and Health Impact), and Carolyn Noonan, PhD (Institute for Research and Education to Advance Community Health, Washington State University), for their boundless energy, incomparable organizational skills, and enthusiasm. We also thank the staff and leadership of our health care organization partners, Southcentral Foundation, Denver Indian Health and Family Services, Indian Health Board of Minneapolis, First Nations Community Healthsource, and Hunter Health Clinic, for their collaboration, insights, responsiveness, and, most importantly, trust.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institutes of Health (U54MD011240-05S1, contact principal investigator, D. Buchwald).
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.