
Abstract
Objective:
COVID-19 exacerbated health inequities for American Indian/Alaska Native (AI/AN) populations. Tribal public health departments and Tribal Epidemiology Centers are critical in addressing these challenges, particularly among people on or near tribally owned land. In this study, we described an example of the value of Tribal Epidemiology Centers and tribal public health departments and estimated the prevalence of post–COVID-19 condition (PCC), defined as symptoms persisting ≥90 days postinfection, in a tribal community.
Methods:
This retrospective cohort study evaluated the prevalence of PCC and functional limitations among adults diagnosed with COVID-19 on the Tule River Reservation from July 2020 through February 2023. Tule River Indian Health Center, Inc staff conducted telephone surveys to assess symptoms at 30 and 90 days postinfection and functional outcomes using the Post–COVID-19 Functional Status scale. We stratified prevalence rates by age and sex and compared functional limitations before and after infection.
Results:
We estimated PCC prevalence at 21% (15 of 76). We also found that 37% (24 of 65) of survey participants reported more functional limitations after COVID-19 infection than before.
Conclusions:
Our study highlights the need for further research and inclusion of AI/AN communities in PCC research and new vertical policy solutions such as those used for diabetes. AI/AN communities have had inequitably higher rates of COVID-19 and appear poised to also have inequitably higher rates of PCC.
Keywords
COVID-19, the disease caused by the SARS-CoV-2 virus, exacerbated long-standing health inequities among American Indian/Alaska Native (AI/AN) populations, who experienced disproportionately more mortality than other groups, with more than 14 223 COVID-19 deaths since 2020.1-3 Before the pandemic, life expectancy for the AI/AN population was 7 years shorter than for the non-Hispanic White population, a gap that grew to 11 years in 2021. 4 In addition, COVID-19 morbidity rates among AI/AN people were higher than for other demographic groups, 5 worsening numerous other health inequities, such as rates of diabetes, substance use, and mental health, all of which are magnified through social determinants of health, such as low educational attainment and high rates of unemployment and poverty.6,7
Post–COVID-19 condition (PCC), also known colloquially as “long COVID,” has emerged as a pressing public health issue, with a substantial portion of people experiencing lingering symptoms well beyond their initial infection. 8 In the general US population, an estimated 31% of adults who had COVID-19 developed symptoms of PCC. 9 However, research on the prevalence of PCC in AI/AN communities is limited, despite the disproportionate prevalence of COVID-19 in these populations. Similar studies did not disaggregate for AI/AN people 10 or they defined PCC differently, which limits comparison. 11
To alleviate these problems, AI/AN people can be served by tribal public health departments (TPHDs) and regional Tribal Epidemiology Centers (TECs), especially AI/AN people living on or near tribally owned land. A TPHD is a public health entity operated by a tribal government or organization that is responsible for delivering health services such as disease prevention, health promotion, and safety initiatives to its community. 12 As sovereign entities, tribes have public health authority, which can be operationalized by a TPHD or other entity per tribal orders. The reauthorization of the Indian Health Care Improvement Act designated TECs as public health authorities (25 USCA §1621m[e][(1]) 13 under the Health Insurance Portability and Accountability Act (HIPAA). 14 As public health authorities, TECs may be granted access to public health information held by the US Department of Health and Human Services for public health activities. 15 A recent journal supplement highlighted several successful examples of the efforts of TPHDs and TECs,16-18 while other articles noted impediments to their work, especially data access and funding.19,20
In this study, we describe another example of the value of TECs and TPHDs, through a study to estimate the prevalence of PCC in a tribal community. The Tule River Indian Health Center, Inc (TRIHCI), which serves 1800 adults, was granted public health authority by the Tule River Tribe in March 2020. 21 TRIHCI staff used patient data to develop and implement a COVID-19 contact-tracing system from June 2020 through February 2023. This system was funded by temporary federal COVID-19 emergency relief funds.
This project began as a joint effort by staff at TRIHCI and the California TEC (CTEC), which is located within the California Rural Indian Health Board, Inc. We used Tule River’s data to conduct a survey on PCC, which has been recently defined as an “infection-associated chronic condition (IACC) that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.” 8
Our study serves 2 goals. First, it fills a gap in the literature by estimating the prevalence of PCC in a rural AI/AN reservation community. We hope these data will be considered in resource allocation decisions and program design, such as within the Indian Health Service and in PCC research. Second, the study shows the potential of TPHDs and TECs to carry out responsive, informed public health interventions when they have adequate funding and data access, which temporarily occurred during the COVID-19 pandemic.
Methods
This retrospective cohort study included all adult patients at TRIHCI with COVID-19 diagnosed from July 2020 through February 2023. TRIHCI staff collected individual-level COVID-19 data through their independent contact-tracing system; they used their own system because TRIHCI was not granted access to the state system. Patients were able to participate if they were aged 18 years or older, were listed in TRIHCI’s records with a telephone number, resided on the Tule River Reservation, and were diagnosed with COVID-19 either through a laboratory test or a presumptive diagnosis by our medical staff based on symptoms and/or recent exposure history. During the peak of the pandemic, presumptive diagnoses were necessary due to the high case volume.
This study received approval from the TRIHCI board of directors, an elected board of tribal members who oversee the tribe’s health center, and, subsequently, from the internal review board of the California Rural Indian Health Board, Inc (institutional review board no. 2022-011) on November 9, 2022. An extension was granted on October 16, 2023. Clinic staff read a consent form by telephone to respondents, who gave their verbal consent to participate before starting the interview. Data were aggregated and anonymized.
TRIHCI staff received training in survey administration, confidentiality, and patient interaction from CTEC because they did not have previous research experience. A TRIHCI staff member, who is a part of the community, interviewed patients via telephone and entered the responses into an online form created by using Qualtrics software (Qualtrics XM Platform, used 2022-2024). This staff member made calls to 503 eligible patients from August 2023 through May 2024. Patients were called at least once; if they were not reached on the first call, they were called again. The entire survey was completed in a single call. Although a proxy could complete the survey if a patient was incapacitated or deceased, no proxies participated. We offered no financial incentive for participation.
The survey consisted of 3 sections: PCC symptoms at 30 and 90 days, functional limitations before and after COVID-19 infection, and opinions on the Tule River Public Health Authority’s COVID-19 orders (shared with the tribe but not reported here).
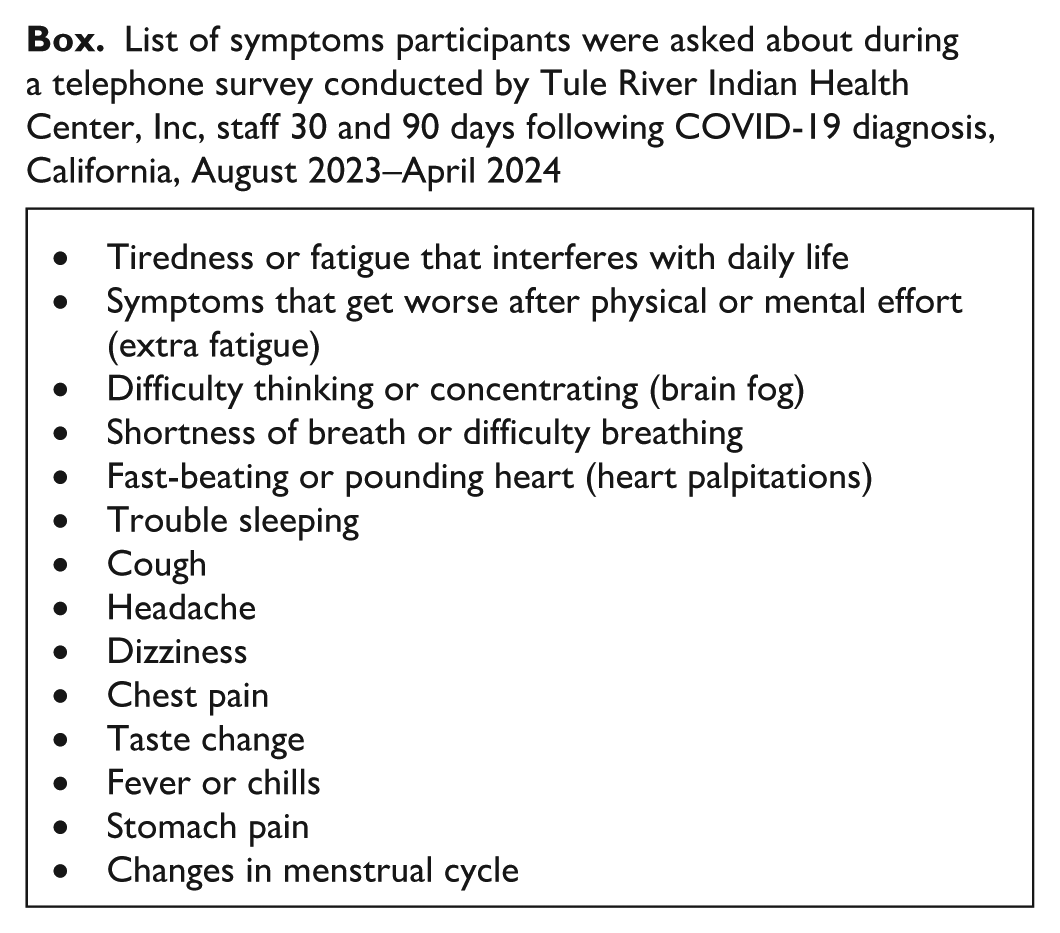
Participants could choose from a list of symptoms (Box), which we developed from a list of PCC conditions developed by the Centers for Disease Control and Prevention. 22 To discourage participant fatigue and encourage survey completion, we limited the list to the 14 most commonly mentioned symptoms from other studies.10,11,23-27 An open-ended response for “other” was offered to capture other symptoms not on the list.
List of symptoms participants were asked about during a telephone survey conducted by Tule River Indian Health Center, Inc, staff 30 and 90 days following COVID-19 diagnosis, California, August 2023–April 2024
We evaluated functional limitations by using the Post–COVID-19 Functional Status scale, which has been validated in other studies.28-30 This ordinal scale assesses a broad spectrum of functional outcomes, concentrating on limitations in daily activities and lifestyle changes. Participants self-reported their limitations based on a 5-grade severity scale; the higher the score, the greater the severity of limitations (Table 1). Our analysis excluded grade 5 (death) because no proxies for deceased patients participated. At the time of the survey, each respondent assessed their physical limitations before and after COVID-19 infection according to this scale. Because the questions were presented exactly as defined in the validated Post–COVID-19 Functional Status scale, they did not incorporate the 30- or 90-day postinfection time frames used in other parts of the survey. As a result, participants reported their functional limitations at the time of the survey in reference to their pre–COVID-19 status.
Descriptions of each grade in the Post–COVID-19 Functional Status scale 30

Statistical Analysis
We began our analysis by using z tests and Pearson χ2 tests to compare the age and sex distribution of the participants with the distribution of all eligible patients who had COVID-19 in TRIHCI’s contact-tracing system. We then calculated the prevalence of symptoms at 30 days and 90 days post–COVID-19 infection, stratified by age group and sex. We weighted prevalence estimates by using the poststratification method to adjust for differences in age distribution between the eligible TRIHCI patient population and the sample population for each period (30 and 90 d). Then we performed a binomial test to determine if the weighted prevalence of having PCC symptoms at 90 days in our sample population was significantly different than 31%, the prevalence reported for the general US population in a survey that used a similar definition of PCC. 9 Next, we calculated the distribution of symptom types experienced by participants. Finally, we assessed changes in functional limitations by comparing participants’ self-reported limitations before and after COVID-19 infection, categorizing whether limitations remained the same, increased, or decreased. This question did not specify a time frame postinfection but, rather, reflected patients’ general perception of changes in functional status following COVID-19 infection. To examine whether a significant shift occurred in functional limitations before and after COVID-19 infection, we used McNemar–Bowker and binomial tests. We used an α level of .05 to determine the significance for all tests.
Results
Of the 503 eligible patients called, 78 patients consented to participate. One patient terminated participation before starting the survey, and 1 patient started the survey but did not complete it. Thus, we conducted and analyzed responses for 76 surveys, for a response rate of 15% (76 of 503).
A z test found no significant difference in sex distribution between the sample and the eligible patient population (z = 1.55; P = .12). However, a χ2 test showed a significant difference in age distribution (χ21 = 15.4; P < .001), with the sample having a younger mean age (34 y) than the eligible patient population (41 y).
At 30 days post–COVID-19 infection, 62% (47 of 76) of patients reported having symptoms of PCC, 37% (28 of 76) did not, and 1% (1 of 76) reported “don’t know.” The weighted prevalence of having PCC symptoms after 30 days was 59%. By sex, 77% (20 of 26) of men and 54% (27 of 50) of women had symptoms after 30 days (Table 2). By age group, the percentages reporting symptoms at 30 days were 68% (21 of 31) of patients aged 18 to 29 years, 52% (11 of 21) aged 30 to 39 years, 65% (11 of 17) aged 40 to 49 years, and 57% (4 of 7) aged ≥50 years; no group had a significantly higher or lower rate than another.
Prevalence of symptoms of post–COVID-19 condition 30 days and 90 days post–COVID-19 infection, by age and sex, TRIHCI patients, California, August 2023–April 2024 a
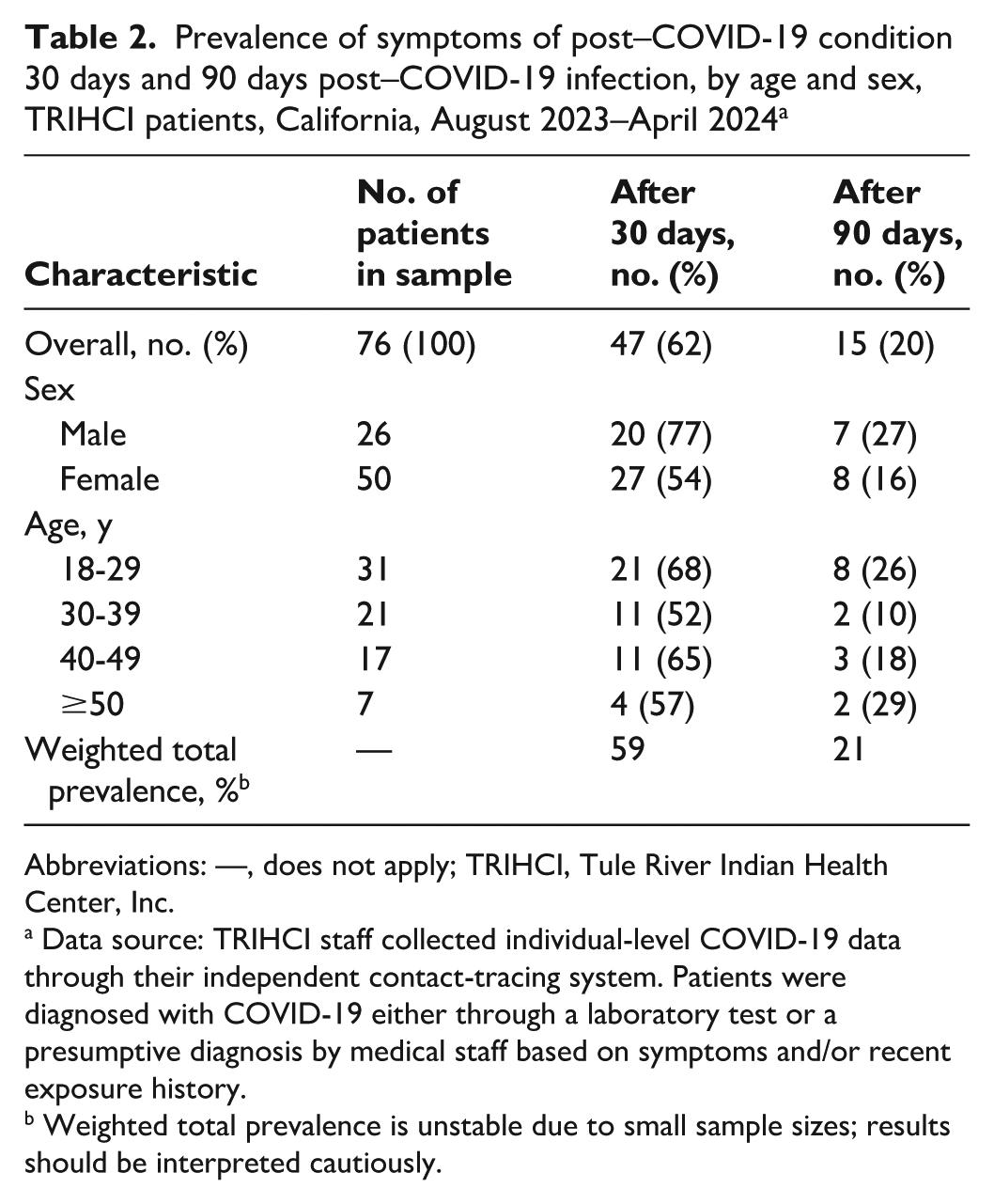
Abbreviations: —, does not apply; TRIHCI, Tule River Indian Health Center, Inc.
Data source: TRIHCI staff collected individual-level COVID-19 data through their independent contact-tracing system. Patients were diagnosed with COVID-19 either through a laboratory test or a presumptive diagnosis by medical staff based on symptoms and/or recent exposure history.
Weighted total prevalence is unstable due to small sample sizes; results should be interpreted cautiously.
At 90 days post–COVID-19 infection, 20% (15 of 76) of participants had symptoms of PCC, 66% (50 of 76) did not, and 14% (11 of 76) reported “don’t know.” A binomial test showed that the weighted prevalence of having PCC symptoms at 90 days post–COVID-19 infection in our sample population (21%; 95% CI, 15%-27%) was lower than the prevalence for the general US population (31%) (P = .04). By sex, 27% (7 of 26) of men and 16% (8 of 50) of women reported symptoms after 90 days (Table 2). By age group, the percentage of patients reporting symptoms at 90 days was 26% (8 of 31) aged 18 to 29 years, 10% (2 of 21) aged 30 to 39 years, 18% (3 of 17) aged 40 to 49 years, and 29% (2 of 7) aged ≥50 years. We found no significant differences in prevalence between any age or sex group.
Of participants who reported having PCC symptoms, the top 3 symptoms were shortness of breath or difficulty breathing, difficulty thinking or concentrating (brain fog), and tiredness or fatigue that interferes with daily life at both 30 days and 90 days post–COVID-19 infection. Other frequently reported symptoms were fever and chills and a fast-beating or pounding heart (Table 3).
Symptoms of post–COVID-19 condition reported by survey participants 30 and 90 days after COVID-19 diagnosis, TRIHCI patients, California, August 2023–April 2024 a

Abbreviation: TRIHCI, Tule River Indian Health Center, Inc.
Data source: TRIHCI staff collected individual-level COVID-19 data through their independent contact-tracing system. Patients were diagnosed with COVID-19 either through a laboratory test or a presumptive diagnosis by medical staff based on symptoms and/or recent exposure history.
Respondents were allowed multiple answers, so percentages do not total to 100.
Of the 76 completed surveys, 65 had data for the Post–COVID-19 Functional Status scale; 11 participants skipped the questions or responded “don’t know” (Figure). Of 65 participants, 37% (n = 24) reported worsened function post–COVID-19 infection (limitations increased), 58% (n = 38) reported no change, and 5% (n = 3) reported improved function (limitations decreased). The McNemar–Bowker test showed significant asymmetry in changes to functional limitations before and after COVID-19 infection (χ210 = 20.0; P = .03), suggesting that changes in function were not evenly distributed. Specifically, the direction of change skewed toward increased limitations, with more participants reporting worsening functionality rather than improvement. Although more participants reported no change in function than worsened function (38 vs 24), a 2-tailed exact binomial test indicated no significant difference between the 2 groups (24 of 62; expected proportion, 0.5; P = .053).
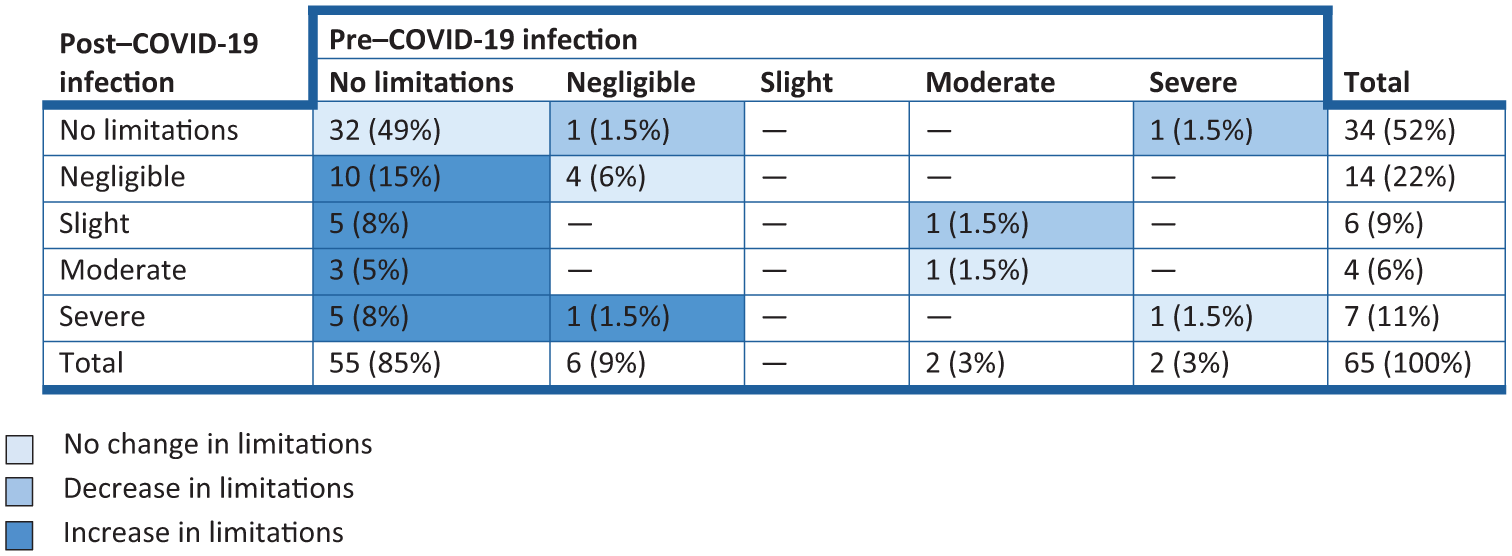
Change in scores for Post–COVID-19 Functional Status scale 30 post–COVID-19 infection, Tule River Indian Health Center, Inc (TRIHCI) patients (n = 65), California, August 2023–April 2024. Values indicate the number (percentage) of survey respondents; totals may not add to 100 due to rounding. Dash indicates that no patients reported that combination of pre– and post–COVID-19 functional status. TRIHCI staff collected individual-level COVID-19 data through their independent contact-tracing system. Patients were diagnosed with COVID-19 either through a laboratory test or a presumptive diagnosis by medical staff based on symptoms and/or recent exposure history. The survey question did not specify a time frame postinfection; responses reflect patients’ general perception of changes in functional status following COVID-19 infection.
Discussion
In our study sample of 76 adults residing in a rural AI/AN reservation community, the estimated prevalence of PCC, defined as symptoms experienced at least 90 days after testing, was 21%. This prevalence is similar to the 22% prevalence estimated in a non–peer-reviewed report from the Ho-Chunk Nation Department of Public Health, although that report defined PCC as symptoms persisting for longer than 6 weeks (42 d). 11 Compared with other US studies and surveys during the pandemic,9,11,24,27 such as the Centers for Disease Control and Prevention’s Household Pulse Survey, which estimated that 31% of adults who had COVID-19 had symptoms of PCC, 9 our estimate was significantly lower (95% CI, 15%-27%; P = .03). An explanation for our lower PCC prevalence estimate is that our study period differed from the study periods in other studies, and more recent studies usually show lower rates of PCC prevalence. Furthermore, most comparable studies did not disaggregate for AI/AN people, 10 which limits comparison. Although our prevalence rates differ from rates in other sources, the most common PCC symptoms we identified were similar, namely, fatigue, shortness of breath, and brain fog.10,11,24-27
In our sample, 37% of survey participants (24 of 65) reported more functional limitations after COVID-19 infection than before. This rate was substantially higher than estimates from the Household Pulse Survey, a comparable survey of the general US population, which found that only 4.3% of adults nationwide had limitations attributed to PCC. 9 In California, the Household Pulse Survey reported an even lower estimate of 3.7%. 9
In addition to our epidemiological findings, our study highlighted the valuable role TPHDs can play in delivering timely, data-informed public health responses and emphasized the importance of recognizing TECs as public health authorities in the public health system. Our dataset was generated due to the work of TRIHCI contact tracers, who closely monitored patients with COVID-19 on the reservation for nearly 3 years. Our local staff enabled us to identify a robust dataset from a specific community, unlike other larger studies, which examined data on AI/AN people as a subset or did not publicly report findings specific to AI/AN people, often grouping them into an “other” category or excluding them altogether due to small sample sizes. Unfortunately, our data collection stopped after the end of the federal emergency declaration from lack of funds. If properly funded, tribal public health capacity could create better metrics for the communities they serve and for the public health system overall.
The absence of tribal data and public health capacity may already be seen in federal PCC-related activities; to date, these activities make little mention of AI/AN communities. Neither a 2024 report by the US Department of Health and Human Services on the federal response to PCC nor the National Institutes of Health’s major PCC research program, ReCOVER, names any specific funding to the Indian Health Service or for AI/AN communities.31,32
Data from those 2 projects will likely be vital in upcoming policy decisions about addressing PCC. For AI/AN communities, COVID-19 infections and their lingering effects may be added to the list of other health issues, such as alcohol abuse, substance use, and diabetes, as a top priority. Data will be needed to determine the best type of policy response, such as incorporating PCC into a program to address many issues simultaneously (ie, a horizontal program) or creating a stand-alone PCC program to focus on a single issue (a vertical program), such as the successful Special Program for Diabetes for Indians.3,33
Ultimately, policy solutions will have to consider the broader effects of PCC in tribal communities. The prevalence and severity of PCC has implications for overburdened tribal health care providers, who could experience more visits per patient because of PCC. Workplaces and schools could experience more absences from the 15% to 38% of their employees or students who contract COVID-19 and go on to have long-term symptoms than from those who do not. People with PCC may lose work or income and increase spending on health care. 34 Including TPHDs and TECs as part of the response to PCC can help get communities’ priorities heard and address many health inequities.
Limitations
Our study had several limitations. First, the age distribution differed between eligible participants and survey participants. Because older people are more likely than younger people to experience PCC symptoms,9,11,27 the younger age distribution in our sample (34 y) may have led to an underestimation of PCC prevalence relative to the broader patient population (41 y). Second, participants may have had recall bias: participants were asked about PCC symptoms for 2 periods (30 and 90 d after infection) up to 3 years after COVID-19 infection. This bias could have led to patients misreporting the timing, severity, or presence of symptoms, thereby compromising the accuracy of the findings. Third, public awareness of PCC through media or community discussions may have influenced symptom reporting, leading to overreporting due to suggestibility or underreporting if symptoms were seen as common or insignificant. Overreporting and underreporting could distort the true prevalence and presentation of PCC, affecting the validity of the findings. Fourth, participants may have been confused about the difference between PCC symptoms and preexisting or unrelated health conditions. This misattribution could result in either overestimating the prevalence of PCC or mischaracterizing its symptom profile, thereby reducing the specificity and accuracy of the data collected. Fifth, our sample included some people with presumptive COVID-19 (ie, they did not have a confirmed positive COVID-19 test), which raises the possibility that some participants may have had other respiratory illnesses. As a result, the study might have misclassified some participants as having PCC, weakening the internal validity of the findings. Sixth, the survey was conducted by a single staff member who had competing priorities at a resource-limited clinic. Balancing clinic needs and survey implementation might have led to fatigue and limited capacity for outreach, potentially contributing to sampling bias and an inability to reach as many participants as intended. Finally, the low response rate (15%) could reflect both limited staffing and hesitancy among tribal communities to share private health information as a result of historical breaches of trust. This factor increases the risk of selection bias and limits the generalizability of the findings.
Future research could improve accuracy by incorporating control groups, ensuring a representative sample, especially among elders, and using a longitudinal design to reduce recall bias. Seroprevalence studies could also provide more precise estimates of PCC prevalence. It is important to note that historical ethical violations have fostered deep mistrust of medical research, posing challenges. Working through these concerns requires culturally responsive approaches, transparency, and community collaboration to uphold ethical standards and rebuild trust.
Conclusions
AI/AN communities have had inequitable rates of COVID-19 and appear poised to experience the ill effects of PCC on functional limitations in a similarly disproportionate way. Staff members of a TPHD and a TEC used tribally owned data to estimate the prevalence of PCC among AI/AN adults with a COVID-19 diagnosis at 21%. This study adds to the growing literature on the prevalence of PCC, especially among a rural tribal population. Although the prevalence of PCC in our study was lower than rates found in other studies, we found a large percentage of patients who reported worsened function post–COVID-19 infection (37%; 24 of 65).
The effects of PCC in total can further strain an already limited tribal health system. TPHDs and TECs can be vital partners if they are adequately funded and have data access. We hope to see the inclusion of AI/AN communities in PCC initiatives, such as those sponsored by the National Institutes of Health and the US Department of Health and Human Services, in the future.
Footnotes
Acknowledgements
The authors thank the Tule River community for generously sharing their time and experiences and the Tule River Indian Health Center, Inc Board of Directors and staff members, especially Ms. Lorina Carabay, for their support in fostering connections within the community to facilitate this survey.
Data Availability
The data supporting this study are not publicly available due to privacy concerns. The dataset is derived from a small community and sharing it, even in a deidentified format, poses a risk of identifying individuals.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the California Rural Indian Health Board, Inc, and Tule River Indian Health Board, Inc, cooperative agreement UiBiIHS0014-15-00.