
Abstract

In 2009, Howard Koh and Marsha Jacobson wrote about the “special nature” of leading in public health. 1 Problems in public health, they contended, were enormous in scale, stemmed from highly complex causes, played out in the public eye, affected an array of organizations, and required unusually long-term solutions. They observed that the profession tended to learn about leading from other professions, and yet no other profession dealt with such large and complex problems. They called on people working in public health to develop their own models and frameworks for leading, tailored to the special nature of the work.
Today, a substantial number of models, frameworks, and courses exist for people aspiring to lead in public health. 2 However, in responding to Koh and Jacobson’s call, we fear the profession has embraced a performative orientation. Our concern is that leading in public health is being rendered into a set of activities: communicating, partnering, connecting. If someone performs these activities, the logic goes, they are showing leadership. But in our experience, the performance of leadership is not the same as leading. Leading is a way of being, an orientation that makes it possible to respond to new challenges as they arise. By contrast, performing leadership activities is less flexible, less able to deal with new challenges. This discordance between the performance of leadership and leading was laid bare during the COVID-19 pandemic. While the demands on public health during the pandemic were unprecedented, many leaders found they did not have the skills required to respond, especially to the way in which health became polarizing, something that has not happened on such a scale before.
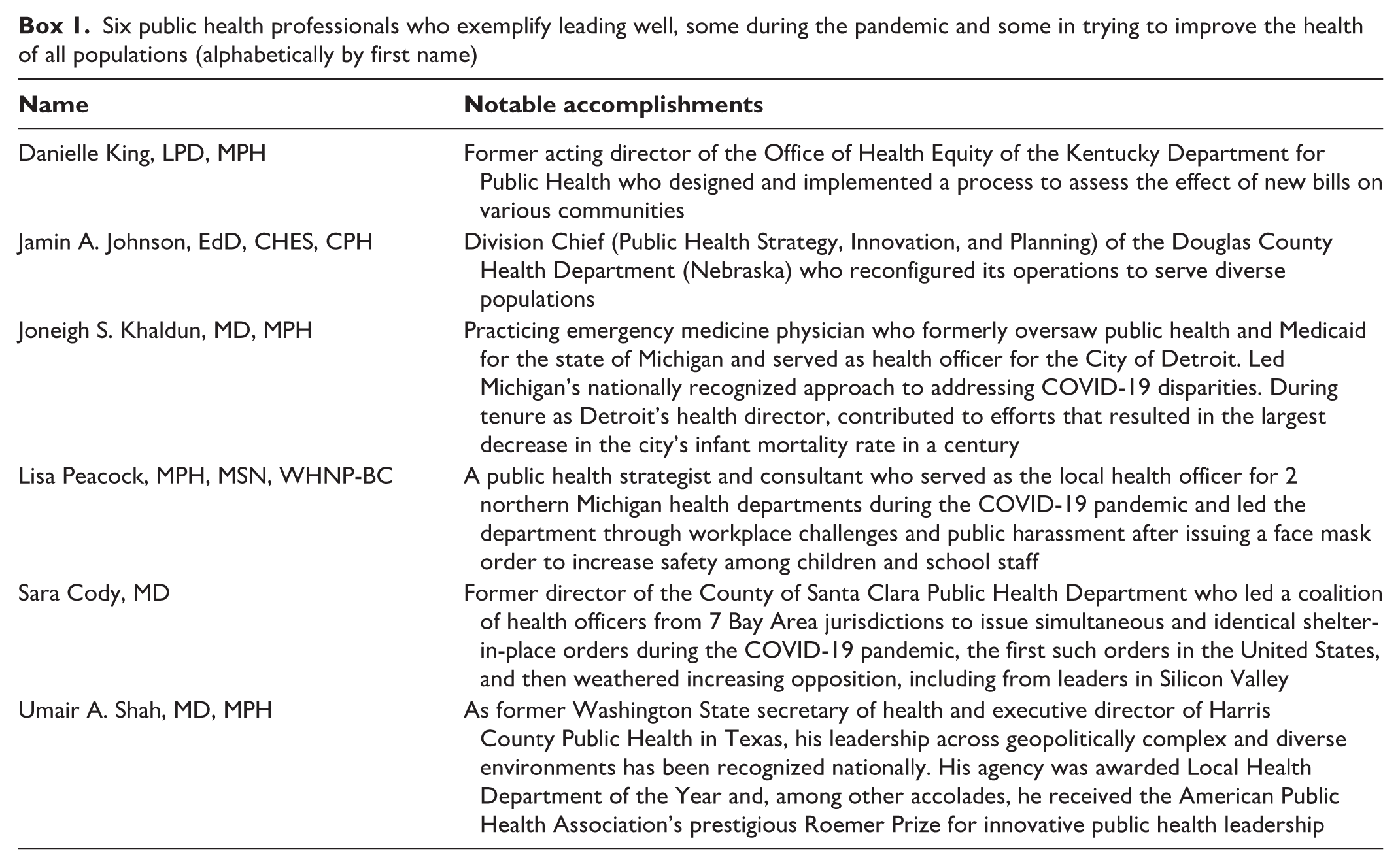
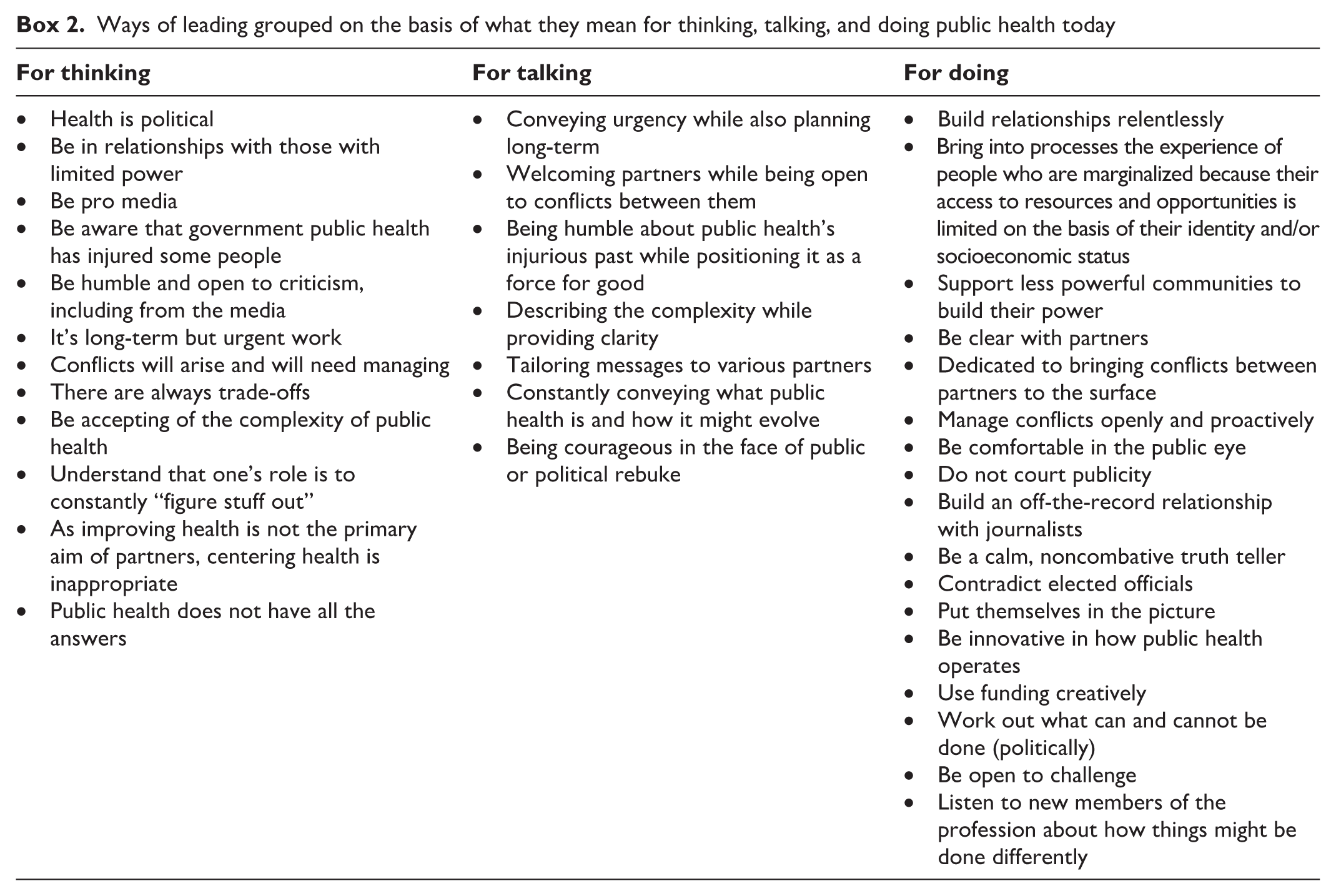
Two of us are leaders in public health who have grappled with new challenges in health and public health all of our careers, early on as leaders of local health departments and now in the nonprofit and philanthropy sectors, both also holding academic appointments (R.B.C. and A.I.). To explore whether our concern had merit, we spoke with 6 colleagues who we believe have led well, some during the pandemic and some in trying to improve the health of all populations (Box 1). We asked them to read Koh and Jacobson’s article and reflect on how they lead. We knew that Koh had gone on to write more about leadership but reasoned that the 2009 article was sufficiently well-known to create a common starting point for the conversations. Our colleagues described numerous ways in which they have led. We reflected on their experience and used it to inform our views on thinking, talking, and doing public health today (Box 2).
Six public health professionals who exemplify leading well, some during the pandemic and some in trying to improve the health of all populations (alphabetically by first name)
Ways of leading grouped on the basis of what they mean for thinking, talking, and doing public health today
Thinking
Our colleagues accepted that health is political. Some of this acceptance came from direct experience with elected officials, but, more broadly, they accepted that health is influenced by the availability of resources and opportunities and how the distribution of these resources and opportunities in society comes down to power differentials across groups. As such, there was a general appreciation among our colleagues that core to the work is being in relationship with those who have limited power, including groups that have been traditionally marginalized by having their access to resources and opportunities limited on the basis of their identity and/or socioeconomic status. The rationale for such relationships was partly to better understand their experiences, partly to help them leverage their assets, and partly to advocate on their behalf. Our colleagues were also pro media, seeing it as an important vehicle to depict the circumstances of those who have been marginalized and whose needs have been overlooked by decision makers and wider society. Our colleagues also understood that governmental public health is part of the machinery that has injured (and, in some cases, is still injuring) certain groups, and as such, a need exists to be humble and open to criticism, including from the media.
Our colleagues were clear that improving the public’s health was long-term work, and yet they also understood they needed to operate with urgency. This contradictory way of thinking was important to hold on to when partnering with organizations, such as business and health care, that tend to have a more black-and-white and short-term way of thinking. Such partnering is further complicated by the understanding that bringing diverse partners together would surface conflicts between them. They did not shy away from this but thought proactively about how to manage such conflicts to the benefit of the public’s health. At the same time, they understood that trade-offs need to occur, both foreseen and unseen, that may harm relationships with or between partners or even, at times, the health of some populations.
Rather than see these processes as chaotic, they were accepting of the complexity of public health and the need to constantly look for patterns and opportunities within it. In that regard, they understood their role was to constantly “figure stuff out.” At the same time, they understood that improving health was not the primary aim of the diverse partners they convened and worked with and so centering health was inappropriate, if not presumptuous and self-important. Finally, they rejected the idea that leading in public health could be frustrating, believing that the experience of frustration is an indicator that you (erroneously) want others to believe you have all the answers and should just do as you say.
Talking
In one way or another, our colleagues described how they tried to share how they think through how they talk, especially in those moments when contradictions are the norm: conveying urgency while also planning long-term, welcoming partners while being open to conflicts between them, being humble about governmental public health’s injurious past while positioning it as a force for good, and describing complexity while providing clarity (Box 3). On a more tactical level, some of our colleagues described the need to tailor messages to various partners, such as being clinical with health care leaders, nontechnical with business leaders, and message oriented with political leaders.
Examples of leading in public health when contradictions are the norm
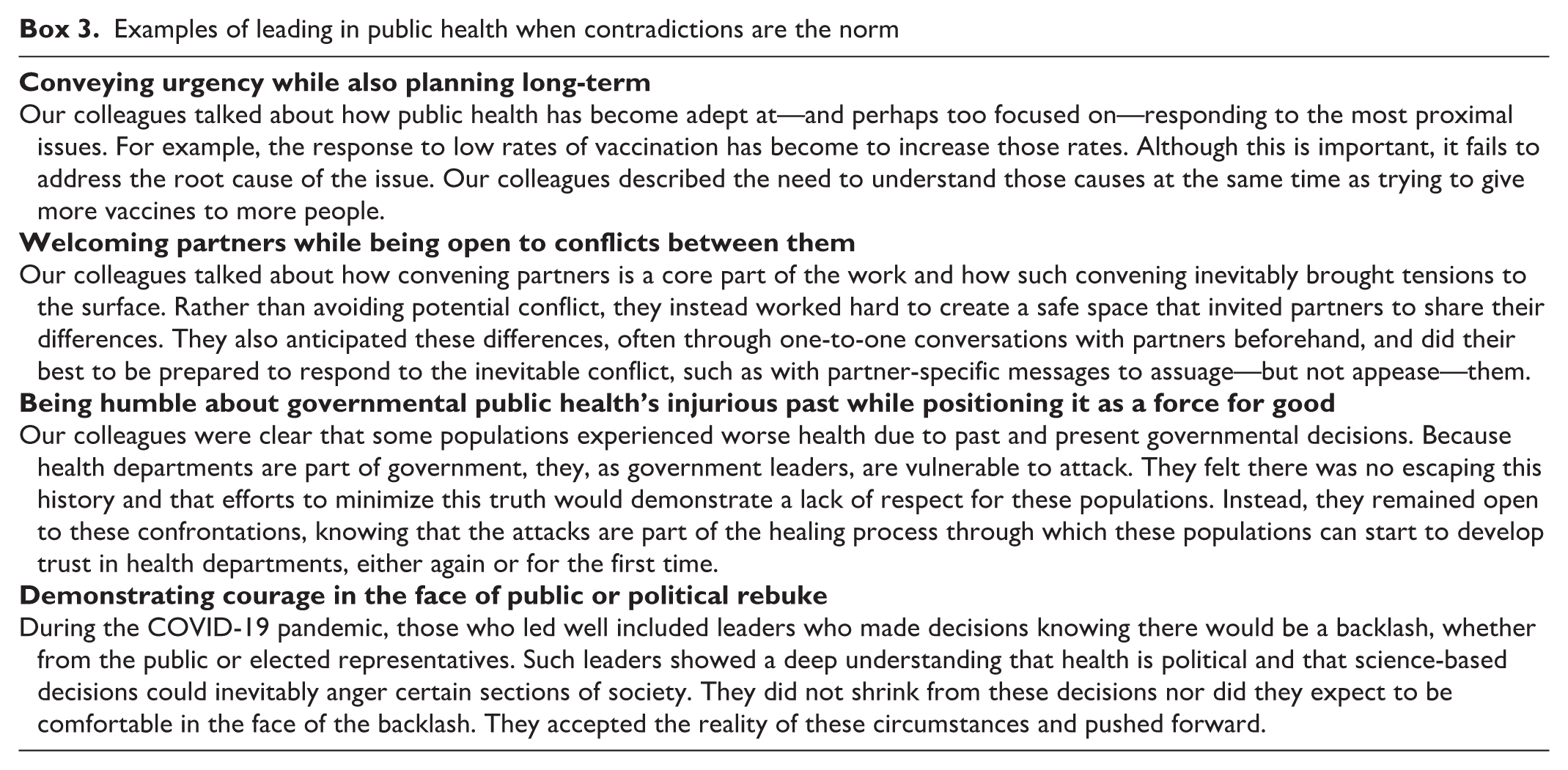
More broadly, our colleagues reflected on the need to constantly convey what public health is and how it might evolve and transform. This need came to the fore during the pandemic, when health issues were politicized and polarizing, resulting in the undermining of common population-level interventions. Some of our colleagues reflected that public health is in transition, caught between what it was and what it needs to become. This transition made talking about public health all the more important, and yet, some of the leaders suggested that the profession is “missing its moment” by being fearful of public or political rebuke. They felt courage was needed. A courageous discourse allows for rebuttal of misinformation about public health, while silence often reinforces flawed narratives. Social unrest and politicization are opportunities to advance an accurate social narrative about public health, not shy away, our colleagues contended.
Doing
Foundational to the doing was relentless relationship building—with partners, with the media, with less powerful members of society, and with people who had experienced unfairness. However, when engaging those who experience powerlessness and unfairness, our colleagues felt that, although having relationships was important, it was not enough. Leveraging relationships was key. For example, although public health can learn from those with experience of being marginalized, it would be better to bring them into processes for understanding problems, designing solutions, and evaluating their experiences in culturally responsive ways. And, although the field of public health can advocate for the less powerful, the longer-term solution is to support communities to build their power.
In terms of building relationships with partners, some of our colleagues reflected on public health’s tendency to be passive, as illustrated by the term “neutral convener” often used in the field. Instead, our colleagues tended to be clear with partners about the urgency of the work and the need for long-term solutions. This more active orientation positions the point of view and perspective of public health as important rather than impartial. This stance gave them confidence to bring conflicts between partners to the surface and manage such conflicts openly and proactively. With regard to the media, our colleagues were clear that it was important to be comfortable in the public eye but not to court publicity lest it dented one’s credibility. They acknowledged that working with the media can be hard—especially given the “gotcha” nature of some outlets—but that it could be aided by building an off-the-record relationship with journalists (eg, by serving as not only a source but also a support in helping them write about complex issues). When on the record, our colleagues talked about the need to be a calm, not combative, truth teller, including when that might mean contradicting elected officials.
Our colleagues also talked about the need for change across the field of public health. They were aware that public health would always involve a technical, evidence-based element, but recent events illustrated that the public needed to see a more human, relatable version. Some of our colleagues put themselves in the picture, partly to put a face to public health but also to illustrate how the profession’s recommendations affected them as much as every other member of the public.
Our colleagues described the need to be innovative in how public health operates, for example, using funding creatively to shift from simply ameliorating disparities to overcoming the structural unfairness that creates them (or finding ways to do both at the same time). Given the political nature of structural work, they also described the need to work out what they can and cannot do, rather than making assumptions based on the norm in the field. Finally, they talked about being open to challenges, especially from new members of the profession, often racial and ethnic minority populations and younger people who tend to have different experiences and worldviews than people who have traditionally worked in public health. They discussed the need to resist indoctrinating them into “how things are done” and instead listen to them to explore how things might be done differently.
Overall Reflections
These conversations provide a critical view into what it means to lead in public health. The ways to think, talk, and do offer a more tangible, real-world insight than the increasingly performative descriptions of leadership that are taking hold. We believe the recent focus on leadership (a set of activities to be performed) rather than leading (a way of being) left some leaders in the profession exposed during the COVID-19 pandemic. Without a prescriptive set of activities to be followed, they were silent when they needed to speak up, placating when they needed to stand their ground, and obsequious when more irreverence would have been appropriate. To be clear, this is a criticism of the profession, not the individuals.
The focus on leadership rather than leading is leaving the profession ill-equipped to adapt. What public health is today is inadequate to deal with the challenges it faces, whether it is the new challenges, such as pandemics or politics, or the old challenges that public health has struggled to overcome, such as noncommunicable diseases and disparities in health. Change does not come from a model, framework, or philosophy presented as a set of activities to be performed (leadership) but from a way of being that makes it possible to respond to new challenges (leading).
Leading is a practice, shaped by deep intention and wholeheartedness. It is the launchpad of innovation and transformation for contemporary public health. The founding of public health focused on root causes and systems. Transforming public health practice could be well facilitated by the examples and lessons of our colleagues. We do not present these ways as a series of activities to be copied but as a glimpse into the kinds of considerations that public health leaders (regardless of their position and title) must contemplate as they grapple toward a version of the profession and practice that can respond to unfairness, establishing a society that is healthier for all and reversing the pattern of poor health outcomes that continue across the United States.
Footnotes
Acknowledgements
We thank our colleagues for making the time for the conversations, sharing their experience, and reviewing this article prior to submission. The views expressed in the article are ours and should not be attributed to any of them or their employers, whether current or previous. All colleagues interviewed gave written consent to be in the conversations that informed this commentary.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was made possible by a grant from the California Endowment (20233247).