
Abstract
The American Medical Association (AMA) is the nation’s largest physician organization and has a prominent voice in health policy in the United States. AMA policies and priorities are set in part by its House of Delegates, in which the US Public Health Service (USPHS) Commissioned Corps participates. The USPHS is a federal uniformed service dedicated to improving health. This article describes the impact of educational USPHS testimony during the policy deliberation process in the AMA House of Delegates. The USPHS has provided invaluable input to the AMA, providing 414 instances of technical advice or information on behalf of subject matter experts at 5 federal agencies during the past 9 years, from 2017 through 2025. The resolution of the proposed AMA policy under debate was aligned with USPHS recommendations a median of 77% of the time. USPHS involvement in the AMA has helped both the AMA and the US government work better together through early information sharing and coordination of activities. The collaboration between the USPHS and AMA is a model partnership to improve health.
Keywords
The American Medical Association (AMA) is the largest physician organization in the United States. It represents the interests of more than 1 million physicians practicing in myriad specialties nationwide. 1 Due to its large size and comprehensive reach, the AMA plays a critical role in shaping health policy at the national and state level. AMA experts recommend reimbursement rates for Medicare procedures to the federal government, set ethics guidelines for physicians, and advocate to preserve physician scope of practice at the state level, among other essential activities. The AMA has official positions on a wide variety of issues touching health and medicine, from future directions for medical education to strategies to reduce obesity rates. 2
The AMA’s largest governing body is the House of Delegates. The House of Delegates comprises more than 700 physician representatives from all geographies and medical specialties. All 50 states, the District of Columbia, 3 US territories, and 143 medical specialty societies are represented. 3 The House of Delegates helps to set AMA policies and priorities, functioning similarly to a unicameral legislature. Proposed policies, called resolutions, are introduced to the House of Delegates for consideration by its members. Resolutions are debated and amended in topic-specific committees at semiannual AMA meetings and, after passing through committee, are presented to the full House of Delegates for voting. Resolutions that are passed by the House of Delegates become official AMA policy and set the strategic direction of the organization. AMA expert committees can also develop policies for consideration, called reports, which are debated and voted on in the same way. 4
The US Public Health Service (USPHS) Commissioned Corps is 1 of 5 federal services with a voting seat in the House of Delegates, along with the US Army, US Navy, US Air Force, and US Department of Veterans Affairs. The USPHS is 1 of 8 uniformed services in the United States; its mission is to protect, promote, and advance the health and safety of the nation. The USPHS comprises approximately 5000 officers, all trained in public health–related professions. Officers serve in diverse roles to promote health: providing medical care to the US military and Native American populations, performing medical and public health research, and leading the administration of federal health programs. 5
The USPHS has been participating in AMA policymaking since the AMA’s inception in 1901, with the US Surgeon General serving as the official AMA delegate. 6 During the past 5 years, however, the USPHS substantially expanded and streamlined its collaboration with the AMA. Currently, the USPHS delegation includes representatives from 9 federal agencies spanning diverse facets of government, from the Centers for Disease Control and Prevention (CDC) to the Indian Health Service (IHS). At each semiannual meeting of the House of Delegates, the USPHS provides technical and educational testimony on a subset of resolutions and reports that are of highest relevance to federal health-related initiatives. The USPHS has commented on the merits and risks of proposed AMA policies as well as shared background information about ongoing federal activities to inform House of Delegates debate. The partnership between the USPHS and AMA ensures that these 2 large entities are aligned in support of better health for all and serves as a model for cross-sector collaboration.
Purpose
This article describes the impact of expert technical and educational testimony provided by the USPHS on AMA policymaking and, through this, on health policy initiatives at the national and state level.
Methods
Written records of USPHS technical and educational testimony provided to the AMA from June 2017 through June 2025 were available for analysis. We examined records from each AMA meeting for the number of items of testimony presented by the USPHS and the number of federal agencies represented. We then evaluated the proceedings of each AMA meeting, 7 which described the number of resolutions and reports submitted and the outcome of each item discussed. We determined the number of AMA resolutions and reports on which the delegation gave testimony at a given meeting and calculated the proportion of those whose ultimate outcomes aligned with USPHS recommendations. We noted items of USPHS testimony that provided background but did not highlight the merits or risks of a resolution or report, but we did not include these items when calculating outcomes. We excluded data from the November 2017 meeting because records of USPHS testimony were missing.
The AMA meeting format changed during the COVID-19 pandemic. The June 2020 meeting was canceled, and the November 2020, June 2021, and November 2021 meetings were shortened so that meeting agendas included only a subset of the submitted resolutions and reports. For these years, we tabulated the total number of items of USPHS testimony, but we compared resolution and report outcomes with USPHS recommendations for only the subset of items discussed during the meetings.
We used Microsoft Excel version 2402 to analyze data descriptively. For the purposes of this analysis, we defined an item of testimony as any technical or educational input from a subject matter expert at a federal agency provided to the USPHS regarding an item of business at a House of Delegates meeting. It was possible for the USPHS to have multiple items of testimony for the same AMA resolution or report.
Finally, we qualitatively reviewed USPHS testimony to select a convenience sample of testimony illustrative of the delegation’s contributions to AMA policymaking. We used the Standards for Quality Improvement Reporting Excellence (SQUIRE) reporting guidelines 8 and reporting checklist 9 to guide drafting of this article.
This project did not involve human data or participants; therefore, institutional review board review was deemed not necessary per the policy of the Office of Science and Medicine at the US Department of Health and Human Services, Office of the Assistant Secretary for Health.
Outcomes
From 2017 through 2025, USPHS participated in 15 AMA meetings (Table 1). During the 9-year study period, the House of Delegates considered 3236 resolutions and reports, and the USPHS provided 414 items of testimony. Of these, 43 items provided informational background only, while the remaining 371 included comments on the merits or risks of proposed AMA policies. A median of 22 items of testimony were presented per meeting, ranging from 3 (June 2018) to 50 (June 2022). A median of 4 federal agencies were represented per meeting, with a range of 1 to 5 (both found in multiple years). Federal agencies providing testimony were CDC, the Centers for Medicare & Medicaid Services (CMS), the US Food and Drug Administration, the Indian Health Service, the National Institutes of Health (NIH), and the Office of the Surgeon General. USPHS officers with expertise in correctional medicine also contributed testimony. Four additional federal agencies reviewed AMA resolutions and reports during the study period but did not contribute any written testimony.
Technical and educational USPHS testimony provided as part of the policy deliberation process at semiannual meetings of the AMA House of Delegates, 2017-2025
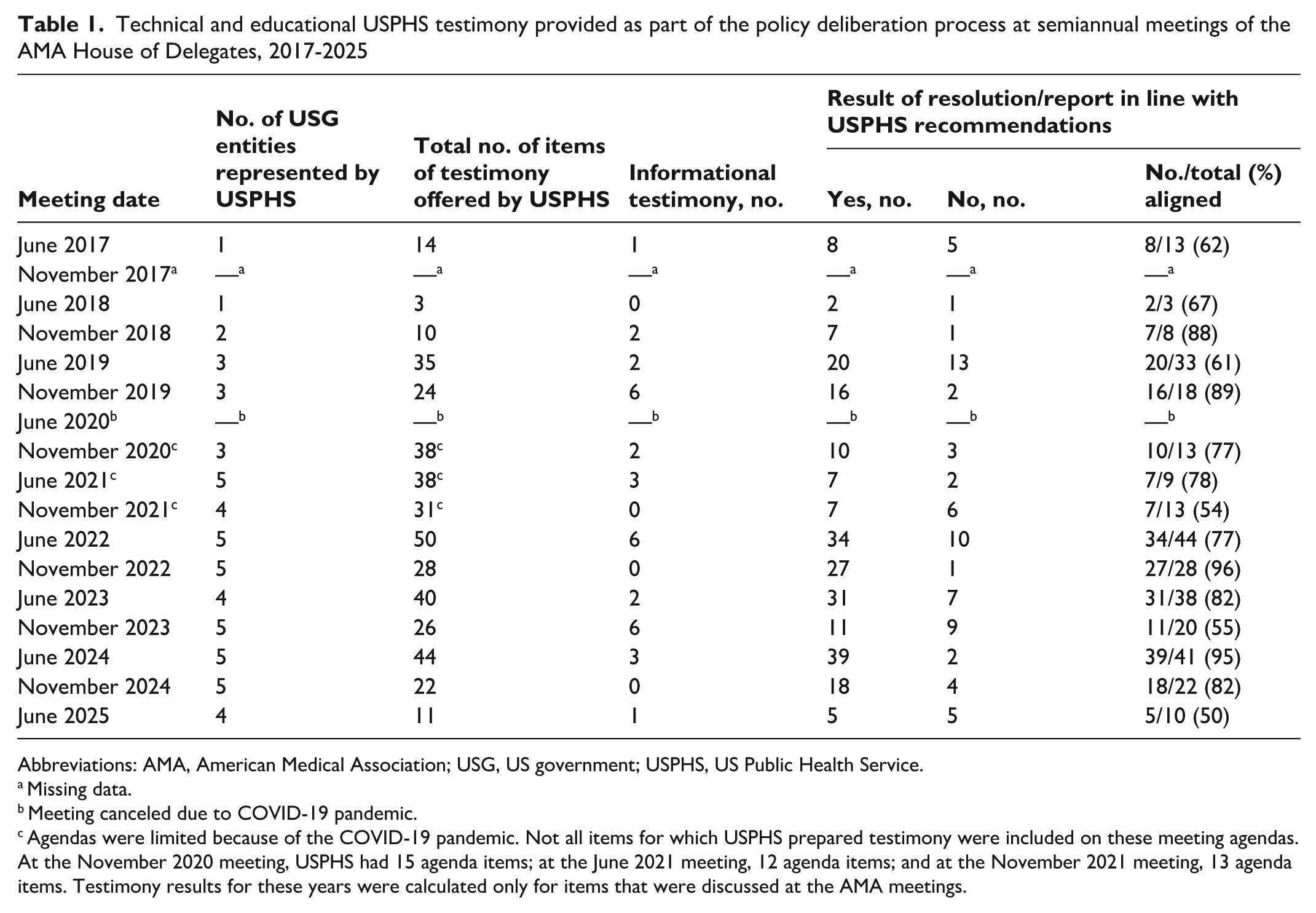
Abbreviations: AMA, American Medical Association; USG, US government; USPHS, US Public Health Service.
Missing data.
Meeting canceled due to COVID-19 pandemic.
Agendas were limited because of the COVID-19 pandemic. Not all items for which USPHS prepared testimony were included on these meeting agendas. At the November 2020 meeting, USPHS had 15 agenda items; at the June 2021 meeting, 12 agenda items; and at the November 2021 meeting, 13 agenda items. Testimony results for these years were calculated only for items that were discussed at the AMA meetings.
USPHS informed AMA policymaking at each House of Delegates meeting. On a per-meeting basis, the resolutions and reports for which USPHS provided testimony were resolved in alignment with the delegation’s recommendations a median of 77% of the time, ranging from 50% (5 of 10 in June 2025) to 96% (27 of 28 in November 2022).
Examples of USPHS testimony and the ultimate results of the AMA resolutions or reports for which USPHS provided input illustrate the diversity of shared expertise (Table 2).
Examples of technical and educational USPHS testimony and AMA resolution outcomes of the policy deliberation process at semiannual meetings of the AMA House of Delegates, 2017-2025
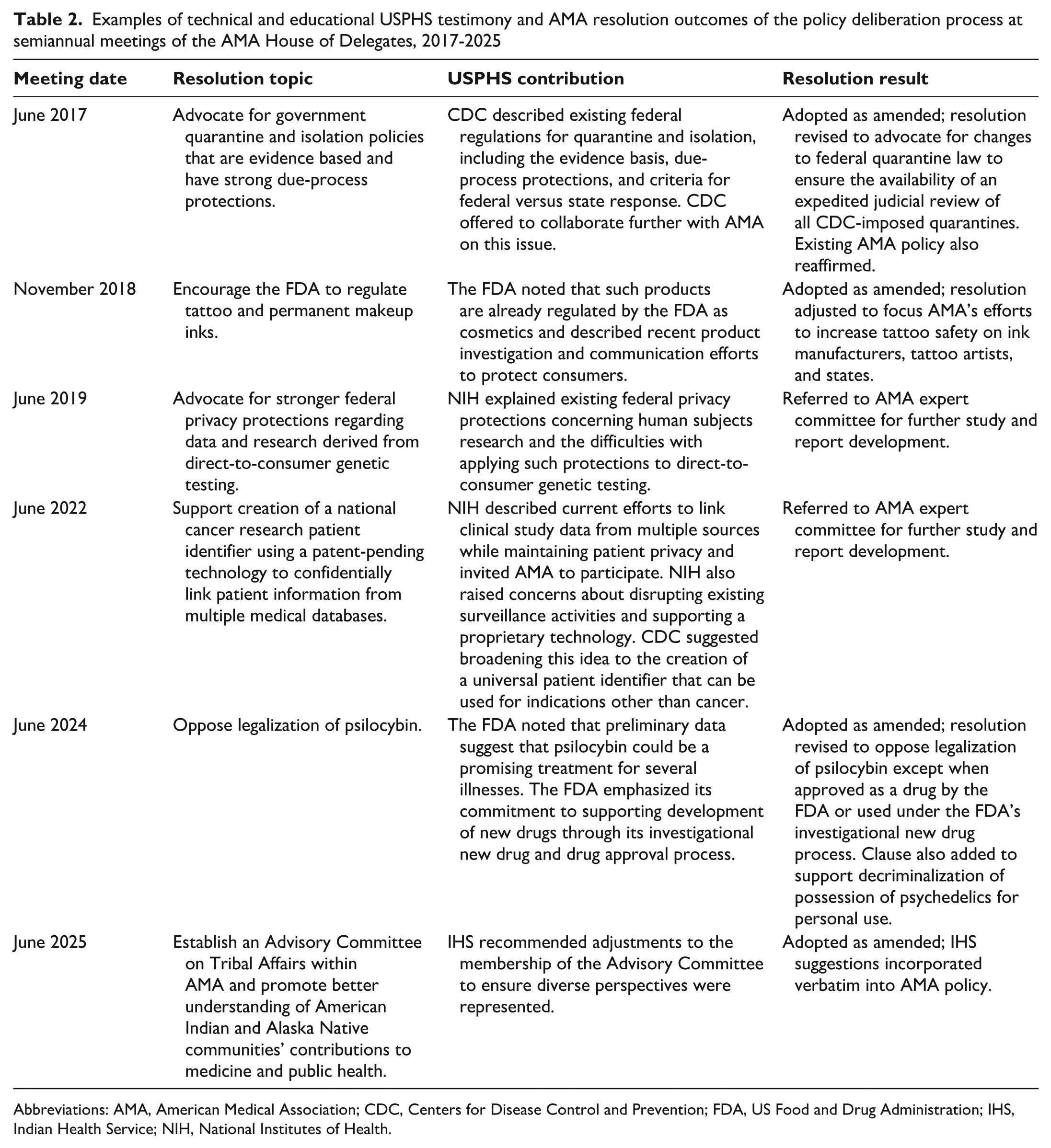
Abbreviations: AMA, American Medical Association; CDC, Centers for Disease Control and Prevention; FDA, US Food and Drug Administration; IHS, Indian Health Service; NIH, National Institutes of Health.
Lessons Learned
The partnership between the USPHS and the AMA House of Delegates has been beneficial for both organizations. The US government and the AMA frequently collaborate on large-scale issues that are vital to health. USPHS participation in the House of Delegates provides opportunities to inform the AMA policy development process with the highest level of national expertise, discuss strategies to meet common goals, and explore opportunities for alignment of priorities. Conversely, the AMA gains early insight into which of their initiatives are likely to be successful or feasible for the US government before committing resources toward them. This early insight saves time and energy for both organizations.
The USPHS delegation has provided invaluable technical advice to the AMA to strengthen its policies, avoid unintended consequences, and address real-world conditions in US health care. USPHS technical testimony can educate the House of Delegates on the most appropriate agency or feasible mechanism to consider when approaching a given issue. For example, a resolution was proposed to advocate for leveraging nonemergency medical transportation funds available through Medicaid to transport patients to healthy grocery destinations, such as farmers markets or food banks. 10 During debate, delegates noted that many Medicaid beneficiaries experience food insecurity and that increasing access to healthy food results in improved health outcomes. Other delegates raised concerns about the costs and logistics of such an initiative. USPHS presented testimony on behalf of CMS, reminding the AMA of the federal statutory requirement that Medicaid medical transportation dollars be used only for transportation to medical services. The USPHS also relayed that states could choose to cover nonmedical transportation via Medicaid under a different mechanism, suggesting a more feasible path to achieve the resolution’s objective, and offered to connect AMA leaders with CMS subject matter experts for further discussion if needed. Ultimately, the AMA decided to reaffirm existing policy rather than pass this resolution.
USPHS has provided important information and served as an inflection point in the debate on proposed policies. For example, NIH scientists noted the paucity of research on the efficacy of sobering centers for substance abuse recovery, after which the House of Delegates opted not to advocate for their expanded use. 11 USPHS educational testimony has provided unpublished information on ongoing federal initiatives. For example, an AMA resolution to promote public health data sharing with tribes and tribal epidemiology centers was retooled after hearing about initiatives already in process at CDC. 12 USPHS has also encouraged the AMA to look at existing issues in new ways. For example, when considering the dangers of social media for teenagers, the Surgeon General himself recommended that the AMA evaluate not only evidence of harm but also evidence of the safety of social media for this age group. 13 In many cases, content from USPHS technical and educational testimony, such as suggested clarifying amendments, has been adopted verbatim into AMA policies, resulting in improved technical accuracy, feasibility, and organizational alignment.
USPHS has also contributed timely information on important potential health risks, after which the AMA opted against some proposed policies that may have been detrimental to public health. When a proposed resolution was under debate that promoted vaping as a safe alternative to smoking, USPHS voiced concerns from multiple US government agencies; ultimately, the House of Delegates did not adopt this measure. Shortly thereafter, an outbreak of lung injury associated with electronic cigarettes occurred; had the AMA been actively promoting vaping, the number of cases in this outbreak might have been higher. 14 During the COVID-19 pandemic, the AMA considered a resolution to warn patients being treated for opioid use disorder of the risk that medications for opioid use disorder could contribute to respiratory depression and severe COVID-19 outcomes. USPHS voiced concerns from multiple US government agencies that this warning could cause patients with opioid use disorder to discontinue their medications; a relapse of substance use would cause a much greater increase in the risk of severe health outcomes. Again, this resolution was ultimately not adopted by the House of Delegates. 11
The findings of this analysis were subject to several limitations. First, we examined only 9 years of USPHS testimony, so data are representative of the recent past and may not fully reflect the interactions between the USPHS and the AMA throughout the organizations’ histories. Second, the House of Delegates is a complex body with many participants, and it is not possible to attribute the outcomes of AMA resolutions and reports that aligned with the recommendations of USPHS solely to USPHS efforts. However, because USPHS testimony is cited verbatim in many of the AMA meeting summaries and in amendments to resolutions that were ultimately adopted as policy, it is likely that USPHS input made important contributions to eventual outcomes.
This article provides just a few examples of how the partnership between USPHS and AMA has been invaluable for public health in the United States. Promoting early and frequent dialogue between the US government and the AMA helps these 2 organizations communicate on key priorities and emerging health issues and identify opportunities for alignment to improve health for all. The AMA can understand the capabilities and constraints of the US government, government activities in progress, and gaps that could be filled. The US government can anticipate future priorities of the AMA and position itself for collaboration when appropriate. As a result, both organizations can optimize their initiatives for success, ultimately benefiting the US population through coordinated efforts to improve clinical medicine and public health. This cooperation is an excellent example of cross-sector collaboration to achieve better health for all. Similar partnerships could be pursued at the state level between state health departments and medical societies.
Footnotes
Acknowledgements
The authors give special thanks to the past and present members of the USPHS, the AMA Work Group, who collect and prepare USPHS testimony for delivery to the AMA; to the dozens of civilian subject matter experts throughout the US government who have shared their knowledge and insights; and to USPHS chief physician officers and surgeons general who have supported and encouraged this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.