
Abstract
Objectives:
Little is known about foods associated with sporadic listeriosis, a foodborne bacterial infection. We compared self-reported foods consumed by people with sporadic versus outbreak-associated listeriosis, overall and for certain populations.
Methods:
We analyzed data on cases with ≥1 reported food exposure reported during 2016-2022 in the United States to the Listeria Initiative. We used counterfactual random forests to identify foods associated with sporadic and outbreak-associated listeriosis in certain populations (eg, pregnant women).
Results:
Of 3413 listeriosis cases reported during 2016-2022, 83.5% (n = 2849) were sporadic. Many foods showed no differential association between sporadic and outbreak-associated illness, indicating similar associations or lack thereof with both illness types. While a subset of foods were associated with sporadic versus outbreak-associated listeriosis, these associations varied by population. For example, strawberries (odds ratio [OR] = 2.48; 95% CI, 1.11-5.52) were the only foods associated with sporadic illness among nonpregnant females aged 15 to 49 years. Among adults aged ≥65 years, 10 foods, including deli-counter sliced cheese (OR = 1.78; 95% CI, 1.28-2.47), were associated with sporadic listeriosis.
Conclusions:
Foods associated with sporadic listeriosis differed from foods associated with outbreak-associated illness, with differences observed across population groups and by pregnancy status. These findings highlight variation in exposure patterns and underscore the need for further attribution studies focused on sporadic illness across demographic groups, to inform population-specific prevention messaging.
Listeria monocytogenes is a pathogenic bacteria that causes listeriosis, the third leading cause of death among foodborne illnesses in the United States. 1 About 20% of listeriosis cases result in death and 94% in hospitalization. 2 Reducing listeriosis incidence is a public health priority, and the US government established the goal of reducing the incidence of listeriosis to 0.22 cases per 100 000 population by 2030. 3 According to the Foodborne Diseases Active Surveillance Network (FoodNet), listeriosis incidence was stable during 2016-2023, suggesting a lack of progress toward these goals. 4
Certain populations are more likely than others to experience severe complications, be hospitalized, or die following listeriosis, including immunocompromised people, adults aged ≥65 years, and pregnant women. 5 The incidence of pregnancy-associated listeriosis is disproportionately higher among Hispanic women than among non-Hispanic women.2,6 Thus, population-specific guidance is frequently developed to reduce listeriosis risk in these populations.7-9 However, the development of effective prevention strategies requires an understanding of how food exposures differ for these populations versus similar paired groups.
Exposure to L monocytogenes can be reduced by preventing food contamination and consumption of contaminated food. However, such efforts rely on an understanding of food vehicles associated with listeriosis and the characteristics of the populations that consume them. Because of the greater incidence and risk of severe illness outcomes among certain populations, it is important to understand how transmission and exposures differ between these and other populations so that targeted prevention strategies can be developed.
The Centers for Disease Control and Prevention (CDC) detects outbreaks using whole-genome sequencing (WGS) to assess genetic relatedness and defines a foodborne outbreak as ≥2 people experiencing a similar illness following ingestion of a common food. 10 Illnesses not meeting this definition are considered a sporadic foodborne illness. The food vehicles for most sporadic illnesses are unknown. Outbreak-associated listeriosis accounts for 14% of cases in the United States, and information on how representative outbreak-associated food vehicles are for sporadic listeriosis is limited. 5 Outbreak-associated food vehicles may be more vulnerable to contamination events that contaminate a large amount of product,1,11,12 which might not be the case for food vehicles for sporadic listeriosis. Because outbreak data serve as the primary source of information for listeriosis attribution in the United States, it is important to understand differences in food exposures for sporadic versus outbreak-associated listeriosis. 13 Comparing food exposures for sporadic and outbreak-associated listeriosis within and between paired population groups provides an opportunity to identify population-specific differences in exposure patterns that may inform prevention efforts.
Methods
State and local health departments in all US jurisdictions conducted listeriosis surveillance by interviewing people with listeriosis or their surrogates using the standard Listeriosis Initiative case report form (hereinafter, LI form). 14 They then submitted this information to CDC through the Listeria Initiative (LI), a national surveillance system. 15
The LI form collects information on demographic characteristics, pregnancy status, clinical outcomes, laboratory, and food history data for foods consumed in the month before illness onset, including data on 150 food exposures representing 10 categories (cheese, other dairy products, seafood, dips/spreads, deli meats, other meat/poultry, fruit, vegetables/other produce, deli salads, and other foods). Food exposure is reported using a 4-point Likert scale, where 1 = ate, 2 = likely ate, 3 = likely did not eat, and 4 = did not eat. Food exposure among pregnant women is considered the exposure for their fetus. For listeriosis cases in which an isolate was available, WGS was performed. CDC used the WGS data to identify genetically similar cases, which were assigned outbreak cluster codes. 16 We defined cases with a cluster code as outbreak associated and all others as sporadic.
We analyzed listeriosis case reports from 2016 through 2022 for laboratory-confirmed cases with ≥1 reported food exposure reported.
Statistical Analysis
We performed all statistical analyses in R version 4.4.2 (R Core Team). We characterized missingness using the funModeling package and singly imputed missing data using the randomForestSRC package to grow 1000 unsupervised trees during 2 iterations.17-19
We used counterfactual random forest (CFRF) to quantify the association between specific food exposures and having a sporadic versus outbreak-associated illness. Briefly, we constructed individual random forest models for each exposure and estimated the counterfactual outcomes of each subject. We used these to quantify odds ratios (ORs) and 95% CIs and set significance at P < .05 by comparing the counterfactual and actual exposures. Because CFRF estimates associations using counterfactual contrasts that condition on all other reported exposures and covariates, this approach reduces, but does not eliminate, the influence of correlation. CFRF also estimates associations by using a joint multivariable modeling framework rather than repeated univariate hypothesis tests, so results are interpreted as differential exposure patterns and do not require multiple-comparison correction.
We adjusted food exposures for age, ethnicity, race, state of residence, pregnancy status, and year of illness. In addition to overall data, mutually exclusive subsets analyzed were the following (a total of 9 separate CFRFs were implemented):
Nonpregnant women and men aged ≥65 years and nonpregnant females and males aged <65 years
Pregnant and nonpregnant adolescent and adult females aged 15 to 49 years
Hispanic and non-Hispanic people
Pregnant Hispanic and pregnant non-Hispanic females
We converted the 4-point Likert scale used on the LI form to 2 levels by classifying “ate” or “likely ate” as exposed and “did not eat” or “likely did not eat” as unexposed. We used the CFRF results to calculate the odds of an illness being sporadic (as opposed to outbreak associated) if an ill person reported consuming a given food after controlling for all other exposures in the CFRF.
Ethics Statement
CDC reviewed this activity, deemed it not research, and conducted the research consistent with applicable federal law and CDC policy (see, eg, 45 CFR part 46.102[l][2], 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Results
Demographic Characteristics
During 2016-2022, a total of 3413 listeriosis cases with ≥1 reported food exposure were reported. The listeriosis incidence was higher in the eastern United States than in other regions (Figure 1).
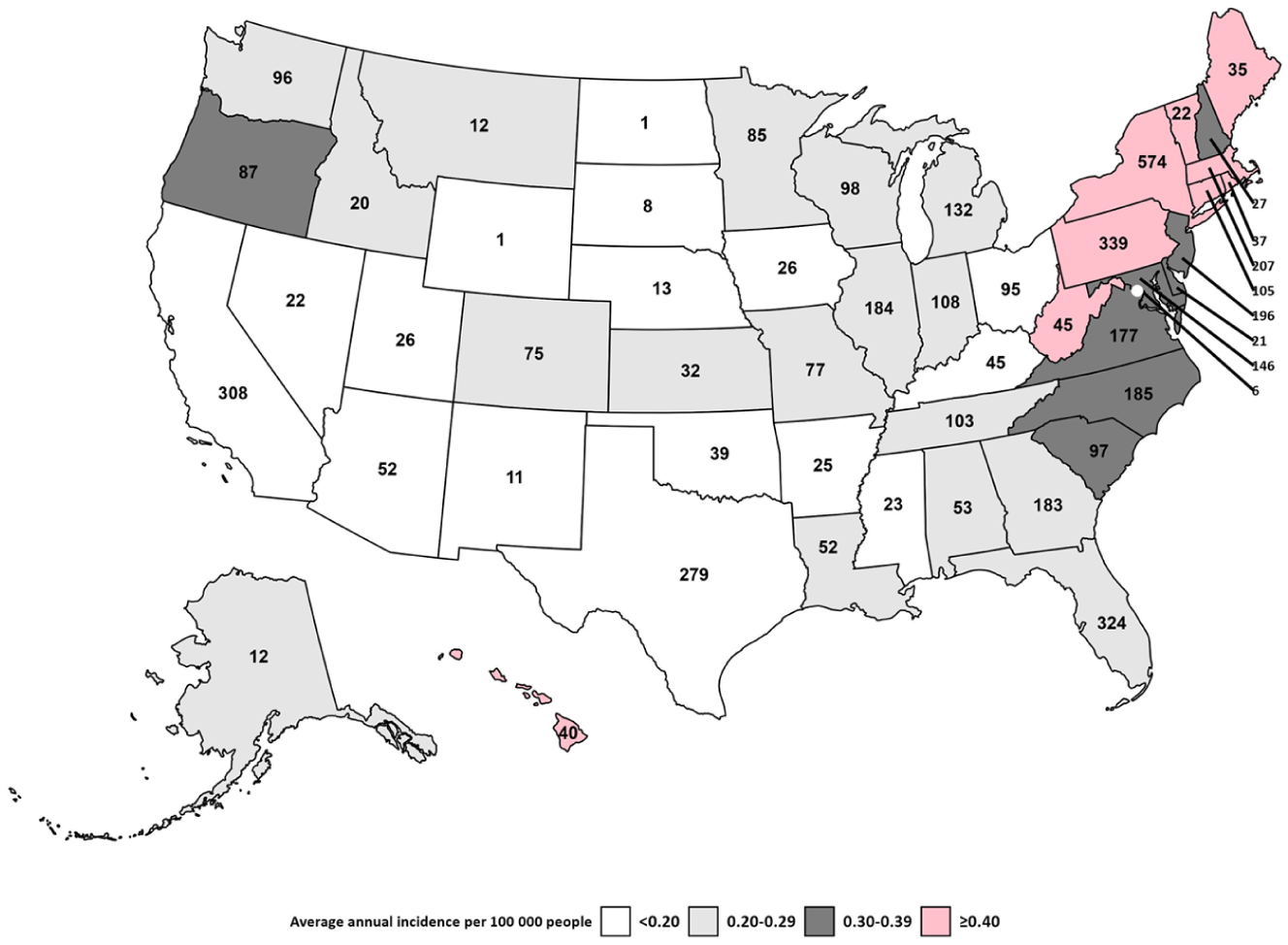
Average incidence per 100 000 people and number of listeriosis cases in each US jurisdiction reported to the Listeria Initiative, 2016-2022. Data source: Listeria Initiative, Centers for Disease Control and Prevention. 15
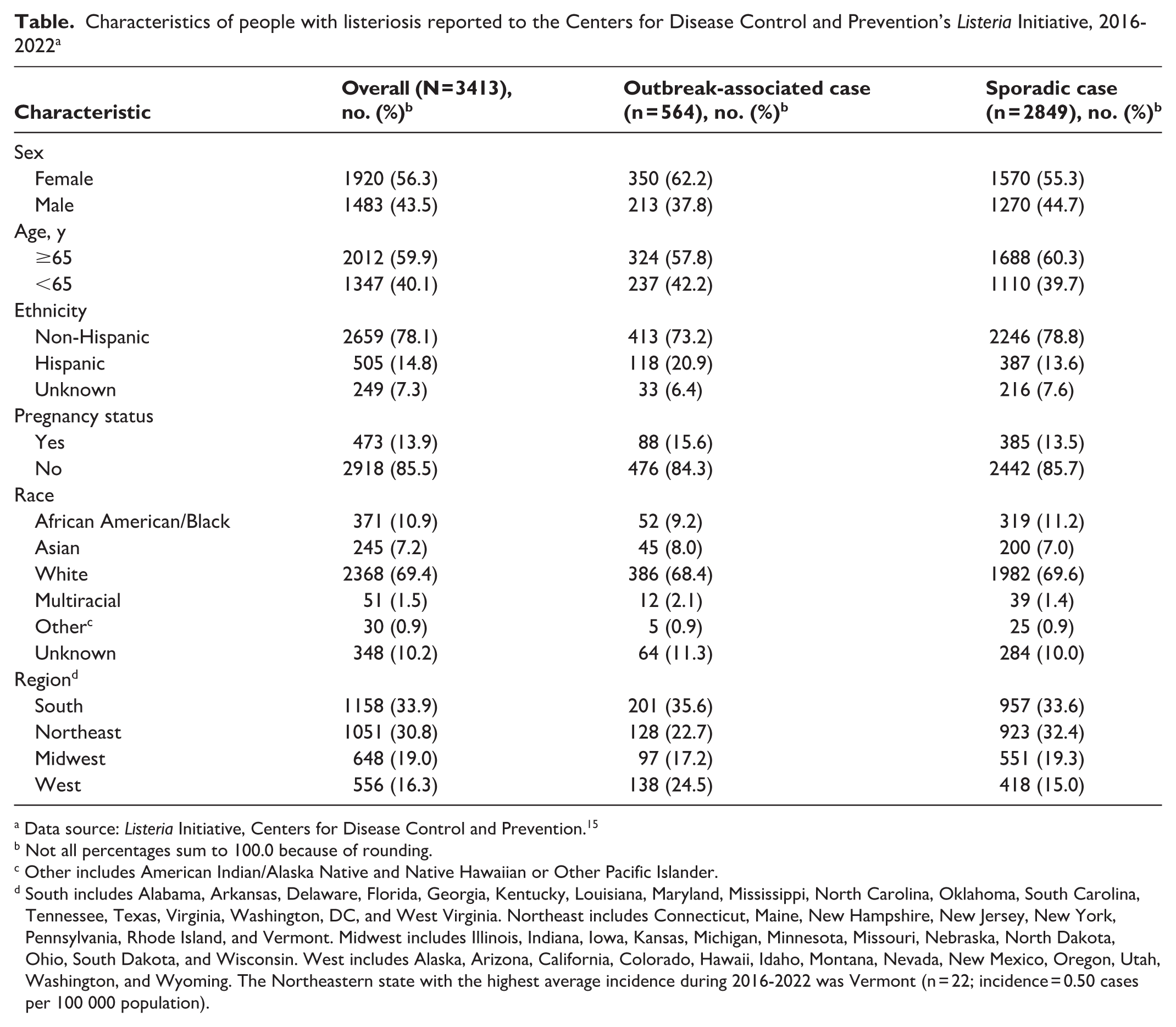
Among people with sporadic listeriosis (83.5%; 2849 of 3413), 59.2% (n = 1688) were aged ≥65 years, 13.5% (n = 385) were pregnant, and 13.6% (n = 387) were Hispanic (Table). Among people with outbreak-associated listeriosis (564 of 3413; 16.5%), 57.4% (n = 324) were aged ≥65 years, 15.6% (n = 88) were pregnant, and 20.9% (n = 118) were Hispanic. Rates of self-reported food exposures for people with sporadic and outbreak-associated listeriosis are in eTables 1 to 3 in the Supplement.
Characteristics of people with listeriosis reported to the Centers for Disease Control and Prevention’s Listeria Initiative, 2016-2022 a
Data source: Listeria Initiative, Centers for Disease Control and Prevention. 15
Not all percentages sum to 100.0 because of rounding.
Other includes American Indian/Alaska Native and Native Hawaiian or Other Pacific Islander.
South includes Alabama, Arkansas, Delaware, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, Washington, DC, and West Virginia. Northeast includes Connecticut, Maine, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. Midwest includes Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. West includes Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. The Northeastern state with the highest average incidence during 2016-2022 was Vermont (n = 22; incidence = 0.50 cases per 100 000 population).
Data From All Cases
Consumption of 9 foods was significantly associated with increased odds of an illness being outbreak associated, while consumption of 15 foods was significantly associated with sporadic listeriosis (Figure 2; eTable 4 in the Supplement). The largest odds of sporadic illness were associated with the consumption of ready-to-eat salads (OR = 2.11; 95% CI, 1.21-3.70) and sandwiches (OR = 2.06; 95% CI, 1.11-3.84). Consumption of Oaxaca (OR = 0.33; 95% CI, 0.15-0.77) and Middle Eastern–style (OR = 0.48; 95% CI, 0.24-0.98) cheese was most strongly associated with outbreak-associated illnesses. Other foods associated with sporadic illness included 6 fruits (eg, apples, blueberries, cantaloupe) and multiple deli and ready-to-eat products. Only 1 fruit (apricot) but no deli or ready-to-eat products were associated with outbreak-associated listeriosis.
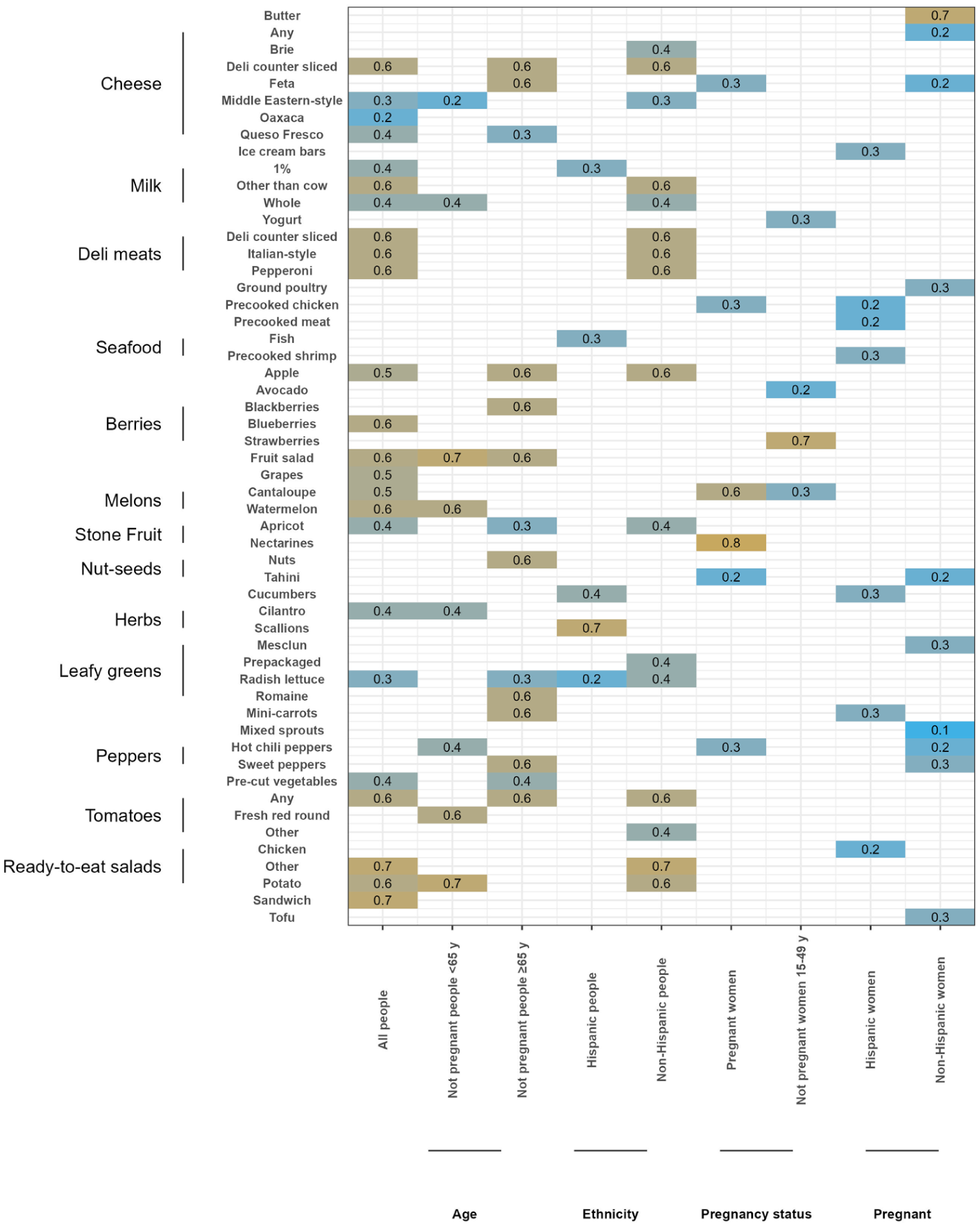
Association between food exposures and whether an illness was outbreak associated or sporadic among listeriosis cases reported to the Listeria Initiative, United States, 2016-2022. Data source: Listeria Initiative, Centers for Disease Control and Prevention. 15
Age
We found no overlap in the foods associated with an illness being sporadic versus outbreak associated for people aged ≥65 and <65 years. Consuming queso fresco, precut vegetables, radish lettuce, and apricots was associated with outbreak-associated listeriosis among people aged ≥65 years (Figure 2; eTable 5 in the Supplement), while consuming Middle Eastern–style cheese, whole milk, cilantro, and hot chili peppers was associated with outbreak-associated listeriosis among people aged <65 years (Figure 2; eTable 6 in the Supplement).
Consuming fruit salad was associated with sporadic listeriosis among adults aged ≥65 years (OR = 1.5; 95% CI, 1.1-2.1) and <65 years (OR = 1.9; 95% CI, 1.1-3.6). Among people aged ≥65 years, consuming 9 additional foods was associated with sporadic listeriosis: feta cheese, any deli-counter sliced cheese, apples, blackberries, mini carrots, any tomatoes, romaine lettuce, sweet peppers, and nuts (Figure 2; eTable 7 in the Supplement). Among people aged <65 years, consuming watermelon, red round fresh tomatoes, and potato salad was associated with sporadic listeriosis.
Pregnancy
We found no overlap in the types of foods associated with an illness being outbreak associated for pregnant and nonpregnant women. Among pregnant women, consuming feta cheese, hot chili peppers, precooked chicken, and tahini was associated with outbreak-associated listeriosis. Among nonpregnant adolescents and women aged 15 to 49 years, consuming yogurt, cantaloupe, and avocado was associated with outbreak-associated listeriosis (Figure 2; eTable 8 in the Supplement).
For both pregnant and nonpregnant adolescents and women aged 15 to 49 years, fruits were associated with an increased risk of sporadic listeriosis. Sporadic illness was associated with consuming nectarines (OR = 4.8; 95% CI, 1.4-16.9) and cantaloupe (OR = 1.8; 95% CI, 1.1-3.1) among pregnant women and with consuming strawberries (OR = 2.5; 95% CI, 1.1-5.5) among nonpregnant women.
Ethnicity
Consuming radish lettuce was associated with increased odds of an illness being classified as outbreak associated for both Hispanic and non-Hispanic people. Among Hispanic people, consuming 1% milk, cucumbers, and fish was associated with outbreak-associated listeriosis. Among non-Hispanic people, consuming Brie, Middle Eastern–style cheese, whole milk, prepackaged leafy greens, other unspecified tomatoes, and apricots was associated with outbreak-associated listeriosis.
We found no overlap in foods associated with sporadic listeriosis among Hispanic and non-Hispanic people. Scallions were the only food associated with sporadic listeriosis among Hispanic people. Consuming any deli-counter sliced cheese, other unspecified milk types, apples, any tomatoes, deli sliced meat, pepperoni, Italian-style meats, other unspecified ready-to-eat salads, and potato salad was associated with sporadic listeriosis among non-Hispanic people (Figure 2; eTable 9 in the Supplement).
Ethnicity Among Pregnant Women
We found no overlap in foods linked to outbreak-associated listeriosis among pregnant Hispanic and non-Hispanic women. Among pregnant Hispanic females, consuming ice cream bars, cucumbers, mini carrots, precooked shrimp, precooked chicken, precooked meat, and chicken salad was linked to outbreak-associated listeriosis (Figure 2; eTable 10 in the Supplement). Among non-Hispanic pregnant women, consuming feta cheese, any unspecified cheese, sweet peppers, hot chili peppers, mesclun, mixed sprouts, tofu, tahini, and ground poultry was linked to outbreak-associated listeriosis (Figure 2; eTable 11 in the Supplement).
No foods were associated with sporadic listeriosis among pregnant Hispanic females, while only butter was associated with sporadic listeriosis among pregnant non-Hispanic females.
Discussion
This analysis used a novel application of CFRF to listeriosis data to identify foods associated with sporadic versus outbreak-associated listeriosis. Because sporadic listeriosis likely arises from multiple independent contamination events, observed associations should be interpreted as differences in reported exposure patterns.
Differences Between Outbreak-Associated and Sporadic Food Exposures
Our findings support that foods associated with sporadic listeriosis may differ from those associated with outbreak-associated listeriosis. 20 These differences could stem from differences in food production, processing, or distribution for foods associated with sporadic and outbreak-associated illnesses. The differences in foods associated with sporadic and outbreak-associated listeriosis may also reflect challenges in detecting outbreaks. For example, advancements in WGS and surveillance (eg, WGS, increased state participation in the Listeria Initiative) have facilitated outbreak identification and traceback, causing an increase in the number of outbreaks identified each year and a decrease in the average size of each outbreak. 12 We used recent data to minimize this effect. Food vehicles associated with sporadic listeriosis may also represent missed outbreaks. In addition, food associations reported here may not be the actual food vehicles that led to illness but, rather, foods that are consumed or prepared along with them. Additional research is needed to better characterize these differences and enhance our understanding of these distinctions.
Differences in Foods Associated With Sporadic and Outbreak-Associated Listeriosis by Populations
Effective prevention requires a comprehensive understanding of how foods associated with listeriosis vary among populations with different listeriosis risks. While certain foods were consistently linked to sporadic or outbreak-associated illness across multiple populations, some associations were population specific. These differences are particularly relevant for prevention planning because annual listeriosis attribution estimates in the United States are derived from national outbreak data rather than population-specific or sporadic illness data.13,21 Moreover, because most listeriosis cases in the United States are sporadic, prevention strategies that rely primarily on outbreak-based attribution may not fully capture exposure pathways relevant to sporadic illness, particularly for foods that are difficult to link to outbreaks (eg, short shelf-life items). 20 Recognizing these limitations, the US Interagency Food Safety Analytics Collaboration prioritized improved attribution of sporadic listeriosis. 22 Incorporating population-specific patterns of sporadic exposure alongside outbreak-based evidence may help inform prevention efforts for certain communities and food commodities and support progress toward Healthy People 2030 listeriosis reduction goals. 23
It is well-established in the social science literature that demographic characteristics, including age and ethnicity, are associated with diet and food consumption practices.24-28 Similarly, biological changes during pregnancy can alter food preferences, and dietary recommendations, including recommendations to reduce listeriosis risks, are age and pregnancy dependent.8,29-31 We would therefore expect food exposures to differ based on age, ethnicity, and pregnancy status. By identifying how exposures differ between paired populations that are at higher or lower risk of listeriosis, we can tailor food safety prevention efforts to specific foods and the populations consuming them. Doing so will allow for development of culturally competent outreach and education tailored to these populations and identification of novel interventions to reduce L monocytogenes contamination in the supply chains serving these populations.
Targeted Efforts to Reduce Listeria Contamination of Foods Associated With Sporadic Illness
Although fruit, prepackaged leafy greens salads, deli products, and other fresh produce have been linked to outbreaks and recalls, these items were also significantly associated with sporadic listeriosis. Given that sporadic illness accounts for about 85% of listeriosis in the United States, focusing on preventing and mitigating L monocytogenes contamination in foods associated with sporadic listeriosis may have the greatest effect on reducing overall incidence. Such efforts will require targeted studies to identify where contamination is most likely to occur in the supply chain as well as critical control points for managing L monocytogenes. Specifically, many of the outbreak-associated foods, such as cheeses, ice cream, and tahini, have long shelf lives, and individual packages are often consumed by multiple people and during multiple meals, increasing the potential for both L monocytogenes growth and for wider human exposure. Because more people are affected over time, illnesses linked to these foods may be more likely to be linked to outbreaks. Conversely, many of the foods linked to sporadic listeriosis in our study have short shelf lives (eg, stone fruits), which may limit the ability of contaminated products to infect large numbers of people, thereby reducing opportunities for outbreak detection and subsequent identification of the implicated food vehicle.
Many of the foods associated with sporadic listeriosis, such as deli products and prepackaged leafy greens, also lack a kill-step between distribution and consumption and have been shown to be at increased risk of cross-contamination during preparation and at retail, as evidenced by multiple recalls and outbreaks.32-34 Overall, our findings and the existing literature suggest that food safety interventions for ready-to-eat foods and foods typically eaten raw (eg, fruit) are important for reducing listeriosis incidence. Research is needed on L monocytogenes dispersal and dynamics along the farm-to-fork continuum and how to improve control of L monocytogenes in the produce supply chain.
Limitations
This study had several limitations. First, a lack of evidence of an association for a given food in this analysis does not mean that the food is not a vehicle for listeriosis. Second, some outbreak cases may be prioritized for interview sooner than others following illness and may therefore be less affected by recall bias, whereas people with sporadic listeriosis may provide less detailed information on type of food or brand than people who have outbreak-associated illnesses. Third, these data represent people with invasive listeriosis and may not account for people with milder illness who are not captured by the Listeria Initiative. Fourth, food exposure data were collected using a standardized 1-month recall period, consistent with the LI form, which introduced several limitations. The form does not capture all foods nor does it distinguish between fresh and frozen foods, which also limits the level of detailed food information that can be assessed.
Fifth, because food exposures were self-reported, the reported foods cannot be confirmed as the true vehicles of infection. Results should be interpreted as reported exposure patterns rather than confirmed sources of transmission. Similarly, as a case–case analysis, this study evaluated differences in exposure patterns between sporadic and outbreak-associated listeriosis rather than identifying causal food vehicles. Thus, the findings of this study may not represent all food associations relevant to listeriosis and are intended to inform hypothesis generation rather than causal inference. Sixth, while use of a uniform exposure window (1 month) reduces differential information bias across populations and ensures comparability of exposures and attribution, it may result in the inclusion of foods consumed outside the true exposure window for some cases or the exclusion of relevant exposures for others. Seventh, other demographic and medical conditions are associated with increased listeriosis risk, including immunocompromised status. However, data on these comorbidities are not consistently collected by the Listeria Initiative and could not be considered here. Lastly, outbreak size may also have influenced the representation of foods associated with outbreaks, with foods from large outbreaks having a higher likelihood to be linked to outbreak-associated listeriosis than foods from small outbreaks (eg, cantaloupes). However, outbreak size could not be controlled for because it was colinear with the outcome in this study.
Conclusion
Foods associated with sporadic listeriosis differed from those associated with outbreaks, and we found differences across population groups and pregnancy status. Because most listeriosis cases in the United States are sporadic, these findings suggest that follow-up research is needed to better characterize foods associated with sporadic illness among certain populations and to support the development of culturally competent, population-specific public health and food safety strategies. Studies that examine critical control points within supply chains producing foods consumed by or linked to particular populations may further inform these efforts. Interventions, including population-specific prevention messaging, should consider foods disproportionately associated with sporadic listeriosis among populations at highest risk of listeriosis.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261454960 – Supplemental material for A Case–Case Study of Sporadic and Outbreak-Associated Listeriosis Exposures: Listeria Initiative Food History Data, 2016-2022
Supplemental material, sj-docx-1-phr-10.1177_00333549261454960 for A Case–Case Study of Sporadic and Outbreak-Associated Listeriosis Exposures: Listeria Initiative Food History Data, 2016-2022 by Angella S. Namwase, Ethel V. Taylor, Amanda Conrad, LaTonia Richardson, Erica B. Rose, Beau B. Bruce and Daniel L. Weller in Public Health Reports®
Footnotes
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This work was written by US government employees and funded accordingly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions of this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.