
Abstract
Many universities are navigating changes to strengthen their long-term sustainability. Although challenges and negative consequences of institutional change are often most visible, successful efforts can provide valuable lessons. In 2024, the University at Albany launched the College of Integrated Health Sciences after a yearlong, participatory planning process. The new college integrates the university’s long-standing public health programs and academic departments, 40-year partnership with the New York State Department of Health, 60-year-old School of Social Welfare, and newly developed nursing programs. A change consultant guided the planning process, and 3 working groups developed recommendations for the college’s name, organizational structure, and vision, mission, and value statements. The planning process involved multiple strategies to identify student, faculty, and staff priorities and encourage active participation: 5 surveys (626 responses), 3 full-day retreats, 7 consultant-led listening sessions, and 41 working group meetings. Students, faculty, and staff (n = 168) voted on the final recommendations. Most participants reported satisfaction with the mission (75%), vision (79%), and value (85%) statements; 80% reported satisfaction (44%) or neutrality (36%) with the proposed organizational structure. Although the working groups presented 3 name options reflecting constituent priorities, voting did not reveal consensus. Deans of the public health and social work units ultimately recommended a name for the college using phrasing that resonated with the vision, mission, and value statements. The university provost and president adopted all recommendations. This case study demonstrates that effectively navigating change requires transparent, participatory planning and frequent 2-way communication, which will facilitate successful outcomes and establish a strong foundation for the institution’s future.
Higher education is facing unprecedented challenges, and administrators are strategizing new ways to promote the vibrancy and long-term sustainability of their institutions. Trust in higher education and public health has eroded,1,2 and enrollment has declined. 3 By 2041, the number of new high school graduates is expected to decline by 13%, 4 further underscoring the need for higher education to be proactive about its future. Many universities are responding to these issues through increased collaboration, including strategic alliances across internal units and partnerships with external organizations. 5 However, negative aspects of institutional change, such as program closures or layoffs, tend to be more visible than successful instances of change and adaptation. 6 Although institutional change can be met with feelings of resistance, particularly when uncertainty is high, positive engagement is possible when constituents understand the need for change and participate in the process.7,8 Documenting and sharing success stories and lessons learned in navigating change can provide valuable guidance for other institutions.
Academic public health institutions are adapting to this shifting landscape by aligning training with evolving student and workforce needs and emphasizing interdisciplinary learning. 9 Public health and social work are closely aligned through a shared commitment to the social determinants of health, equity, and community engagement. 10 Recognizing this overlap, an increasing number of schools accredited by the Council on Education for Public Health have partnered with social work schools, 11 with many offering dual master of public health and master of social work degrees. Creating partnerships between public health and social work units is becoming a strategic way forward.
In fall 2024, the University at Albany announced its new College of Integrated Health Sciences (CIHS),12,13 a Council on Education for Public Health–accredited college of public health that maintains the university’s long-standing public health programs, academic departments, and its unique 40-year partnership with the New York State Department of Health. CIHS also includes the School of Social Welfare, 14 an institution dedicated to social justice and community-engaged research and practice for the past 60 years. In addition, CIHS has a new nursing unit that offers undergraduate training in partnership with local hospitals and a graduate degree in population health nursing. This case study describes the participatory planning process and lessons learned in establishing CIHS to inform other institutions that might be navigating similar changes.
Purpose
Four considerations motivated the creation of CIHS. First, students must have interdisciplinary training to address modern public health challenges such as climate change, aging, and health equity. 9 Second, the disciplines of public health, social work, and nursing share a commitment to addressing the social determinants of health. 10 Integrating these disciplines will promote innovation and collaboration in teaching and research. Third, a new college affords the opportunity to build modern and in-demand degree programs. In addition to the flagship public health and social work degrees the units will continue to offer, CIHS has implemented several new undergraduate and graduate programs. Finally, while requiring initial financial investments, CIHS will yield structural and financial efficiencies. For example, the units will be located together in a newly renovated building on the main campus. This colocation will eliminate the need for students to travel to multiple campuses for classes and streamline operations for the college (eg, information technology, utilities). The units were previously independent and not in financial difficulty when the administration requested integration, and no layoffs or program closures occurred. Integration was proposed to achieve modern interdisciplinary training goals, create structural efficiencies, and increase enrollment through new and updated programs.
Methods
The university leadership charged the deans of the public health and social welfare units with developing a planning process that would result in recommendations for the new college’s vision, mission, and value statements; organizational structure; and name. The deans chose a participatory planning approach and developed a planning strategy that included students, faculty, and staff from the public health (which includes nursing) and social welfare units, the university faculty senate, and university leadership. Many New York State Department of Health scientists have faculty appointments in the University at Albany public health academic departments, and New York State Department of Health faculty, including the Commissioner of Health, participated. An organizational change consultant facilitated the planning process. The planning spanned a single academic year (2023-2024). This work was determined to be exempt from review by the State University of New York at Albany Institutional Review Board because it did not involve human data or participants.
Working Groups
To launch the planning phase, the deans formed 3 working groups: (1) the Transition Steering Committee (TSC), charged with managing the planning process and providing regular communications with planning partners and constituents; (2) the Vision, Mission, and Values (VMV) Working Group, charged with developing statements that encapsulate the philosophy and belief structure of the new college; and (3) the Name and Organizational Structure (NOS) Working Group, charged with developing phrasing recommendations for the college name and drafting an organizational chart that represents the new college’s structure and is compliant with each unit’s accrediting body. A public health representative and a social welfare representative cochaired the working groups. The TSC was cochaired by the unit deans, and tenured faculty co-led the VMV and NOS working groups as part of their service for the year. Working group membership was voluntary and included faculty, staff, and students from each unit as well as members of the university senate. This membership structure enabled constituents to directly shape the new college features, with senate members providing a broader university perspective. Senate members also reported on the process and facilitated discussions at senate meetings to ensure university-wide transparency. The organizational change consultant facilitated listening sessions with students, faculty, and staff; participated in TSC meetings; and helped organize the process, but the consultant did not advise on the new college components.
Working groups used several strategies to solicit ideas and discuss priorities and used multiple communication methods to provide updates and answer questions. Meetings early in the process emphasized reactions to the changes, with time to share, listen, and process, which was important for validating emotions and building relationships across units. Working groups consulted accrediting bodies, materials from other integrated public health and social work colleges, university communications offices, and ChatGPT. Working groups responded to questions raised by students, faculty, and staff and received suggestions for improving the planning process. Planning methods and key concerns for each group are listed in the Box.
Planning methods and key issues addressed by working groups involved in planning the College of Integrated Health Sciences, University at Albany, State University of New York, 2024
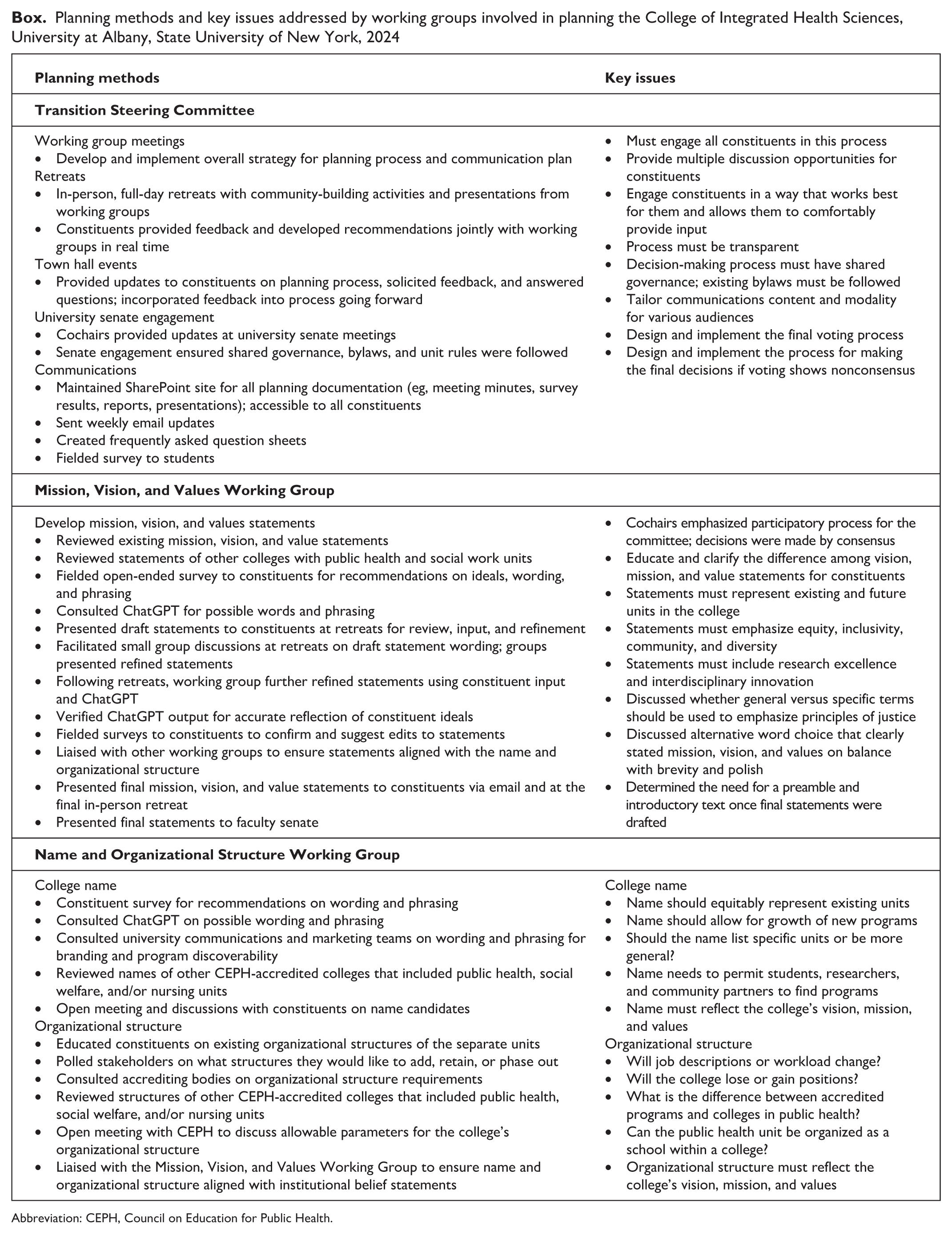
Abbreviation: CEPH, Council on Education for Public Health.
Evaluating the Planning Process
The working groups monitored the implementation of planning activities to determine whether the process achieved the following goals: (1) provide multiple opportunities for discussion, (2) obtain input from constituents (ie, collect data), (3) engage all constituent groups, and (4) develop and deploy communication strategies. This process evaluation enabled the identification of areas for improvement and successes to build on in real time.
Constituent Vote
At the end of the planning year, students, faculty, and staff anonymously rated their satisfaction with the final iterations of the mission and vision statements, including 7 value statements, an organizational structure chart, and 3 college name options, using a 5-point scale (1 = extremely dissatisfied, 2 = somewhat dissatisfied, 3 = neutral, 4 = somewhat satisfied, 5 = extremely satisfied). The TSC tabulated frequencies for all respondents according to constituent type (student, faculty, staff; public health; social welfare).
Outcomes
Planning Process Outcomes
The planning process goals, activities, and outcomes are outlined in Table 1. Working groups and students, faculty, and staff engaged intensively in discussion, and all constituent groups participated in the planning process. The planning process prioritized communication between working groups and constituents. The working groups implemented multiple approaches to promote discussion: 7 listening sessions led by the consultant, 41 regular working group meetings (16 TSC, 10 VMV, 15 NOS), 3 full-day retreats in person, targeted conversations on specific topics (3 open meetings, 4 town hall events), 4 coffee hours with the provost, and participation in 3 university senate meetings to review and discuss the process. Student, faculty, and staff ideas and priorities were anonymously collected in 5 unique surveys (626 responses) and documented in 46 files from discussion activities (eg, meeting minutes, recordings, transcripts). Working group composition, participation at full-day retreats, and survey responses showed representation from all constituents. The working groups developed and deployed multiple communication strategies throughout the year, including in response to needs expressed by constituents. Meeting transcripts and minutes captured the emotional tone of the discussions, ranging from positive feelings of interest and curiosity to negative emotions, including worry and resistance, especially in the early stages of the planning process.
Planning goals and activities for the College of Integrated Health Sciences, University at Albany, State University of New York, 2024
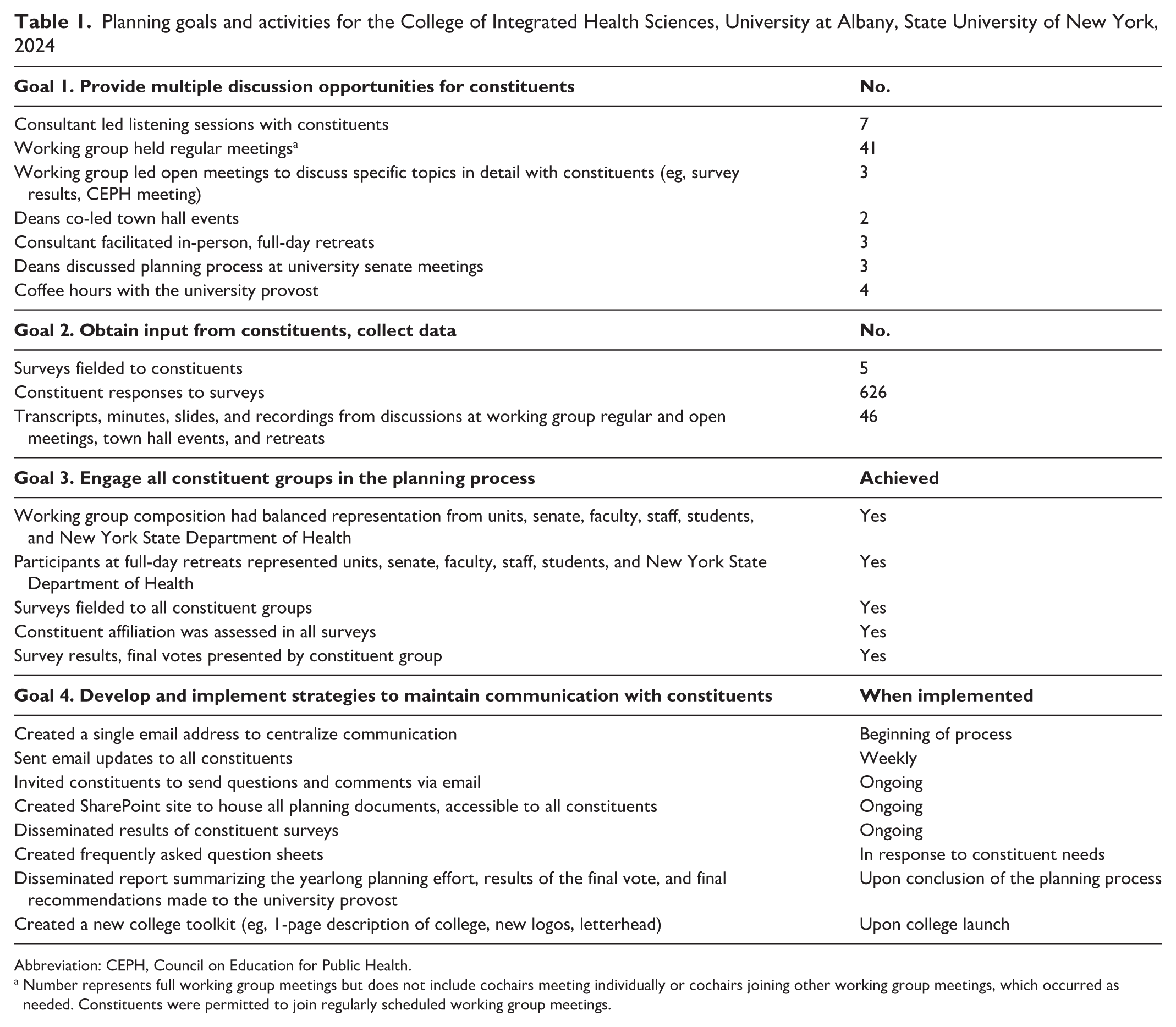
Abbreviation: CEPH, Council on Education for Public Health.
Number represents full working group meetings but does not include cochairs meeting individually or cochairs joining other working group meetings, which occurred as needed. Constituents were permitted to join regularly scheduled working group meetings.
Vote Outcomes
Constituent satisfaction with final recommendations of the working group is summarized in Table 2 (n = 168; public health, n = 110; social welfare, n = 58; faculty, n = 65; staff, n = 37; students, n = 66). Overall, most respondents reported satisfaction with the mission (75%), vision (79%), and value (85%) statements for the new college, with high degrees of satisfaction across all respondents. Discussion activities revealed that the units shared a common commitment to health equity. This common ground facilitated conversation and the operationalization of shared beliefs.
Satisfaction with final recommendations made by the working groups for the College of Integrated Health Sciences, University at Albany, State University of New York, 2024
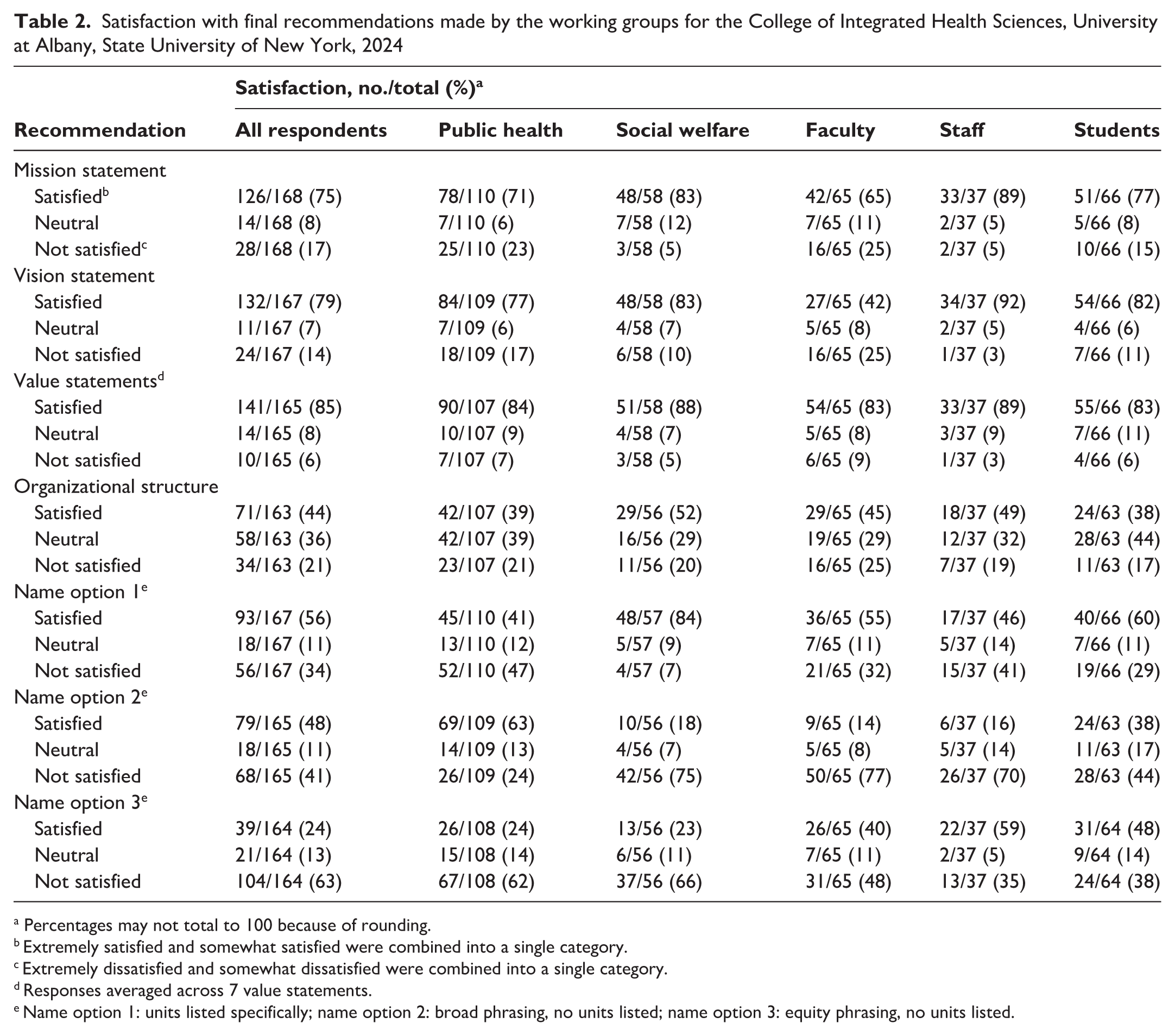
Percentages may not total to 100 because of rounding.
Extremely satisfied and somewhat satisfied were combined into a single category.
Extremely dissatisfied and somewhat dissatisfied were combined into a single category.
Responses averaged across 7 value statements.
Name option 1: units listed specifically; name option 2: broad phrasing, no units listed; name option 3: equity phrasing, no units listed.
For organizational structure, 80% reported satisfaction (44%) or neutrality (36%) with the proposed organizational structure for the new college (Table 2). Social work respondents reported higher satisfaction with the proposed organizational structure than public health respondents (52% vs 39%), while public health respondents reported neutrality more often than social work respondents did (39% vs 29%). Both groups reported low degrees of dissatisfaction with the organizational structure. Unlike the college name and mission, vision, and values statements, the accreditation requirements provided some parameters on what the organizational structure could include. Where possible, student, faculty, and staff priorities were incorporated into the structure to maintain existing unit components and build new offices for the college.
Approximately half of the respondents reported satisfaction with name option 1 (both units listed; 56%) and name option 2 (broad phrasing with no units listed; 48%) (Table 2). However, satisfaction differed by unit: social welfare respondents favored option 1 (84%), whereas public health respondents favored option 2 (63%). Only 24% of respondents were satisfied with option 3 (equity phrasing with no units listed). This pattern was consistent across students, faculty, and staff. Discussion transcripts and minutes revealed that participants generally expressed shared naming priorities (eg, represent existing units, allow for growth of new programs, reflect the vision, mission, and value statements), yet it was difficult to translate these shared priorities into consensus on the phrasing of a name.
To address this lack of consensus, the deans proposed a name that was an amalgamation of the broad phrasing option and wording that aligned with the vision, mission, and value statements: the College of Integrated Health Sciences. The public health and social welfare deans provided this name, along with the VMV group statements and organizational structure recommendations, to the university leadership with a report summarizing the yearlong planning effort including results of the final vote. Leadership adopted the recommendations and the college launched in fall 2024.
Lessons Learned
Institutions navigating change should engage in a participatory planning process. Students, faculty, and staff have expertise in unit strengths and needs, and incorporating their experiences and priorities into planning provides important insights and builds trust in the process. Any process involving multiple groups is unlikely to achieve full consensus on all issues, but open discussion is preferable to top-down decision-making. 8 Those whose perspectives are not fully represented in the final outcomes may be more willing to accept decisions when the process is transparent, collaborative, and includes diverse viewpoints. The change consultant played a crucial role by implementing strategies to strengthen engagement across units, working with the TSC to refine processes, and serving as a neutral liaison. High levels of satisfaction across outcomes indicated that this investment in participatory planning was effective and worthwhile.
Early identification of common ground among constituent groups is crucial and serves as a foundation for strengthening engagement and providing a scaffold for subsequent planning work. For example, articulating ideals for the VMV group illustrated a shared commitment to social justice and health equity across units. From there, the development of belief statements proceeded readily while fostering a collegial and positive emotional tone. Process data showed the VMV group had the fewest meetings of all working groups, suggesting that this common ground facilitated the work and led to high satisfaction. The VMV group ideals were incorporated directly into the organizational structure through the enhancement of diversity, equity, and inclusion and community engagement offices. However, different concerns influenced satisfaction with the name. Most participants reported dissatisfaction with the equity-themed name, despite its mapping directly to language in the mission statement. A major constituent priority was that the name should ensure discoverability of existing units, yet consensus was not reached on phrasing and word ordering for a name that listed the units explicitly. Planning efforts should strive to identify shared priorities and build on them where possible, while continuing to listen and adapt.
Listening and frequent communication are essential in planning and serve 2 key functions. First, constituents need to be kept informed on the process to participate in decision-making. Students, faculty, and staff are busy and need engagement through several mechanisms, and messages need to be tailored. The TSC disseminated weekly email updates on the planning process to all, with separate messages sent to students, faculty, and staff to address various concerns. For example, students had questions about how the new name would appear on diplomas and transcripts, whereas faculty and staff had questions related to accreditation. Second, listening and consistent communication build trust. 8 Early on, some participants shared that they believed that decisions had already been made for the college and that the collection of unit perspectives was illusory. This mistrust was addressed through listening sessions, 2-way discussions, and frequent and transparent communication.
Sustaining student engagement was at times difficult to achieve. Although students were invited to all activities and received frequent tailored communications, participation in some activities was lower among students than among faculty and staff. Establishing a dedicated student-led working group could improve their participation.
The financial benefits of integrating disciplines are beginning to be realized. For example, the public health unit has moved from its rented satellite space to university buildings, which enabled funds that previously covered rent to be reallocated to support new graduate student assistantships. This cost-neutral reallocation represents a substantial gain because it will enhance recruitment and retention of talented students. In addition, 4 nursing programs have been launched, along with a fully online master of public health program in epidemiology and a master of science program in bioinformatics and artificial intelligence methods. The online master of social work program in social welfare has doubled in enrollment, and there is high demand for the bachelor of science in nursing program. The integration has also led to new faculty and staff positions and the promotion of some current staff into new roles (eg, college-level development officer, college-level communications director). Although a detailed economic analysis was beyond the scope of this planning process, our findings suggest that investments in CIHS are beginning to yield returns.
Conclusion
To navigate the changing landscape of higher education, universities can adopt institutional reorganization as a strategy to address enrollment declines, make efficient use of increasingly limited resources, and promote modern workforce training. Since its launch, CIHS has developed bylaws, revised memoranda of understanding with local partners, coordinated building renovations and office moves, and implemented plans to elevate college visibility, while maintaining a constituent-driven institutional culture. Institutions facing change should adopt a transparent, participatory approach with frequent opportunities for listening, discussion, and communication. Challenges are inevitable, but taking the time to engage with campus constituents will build trust and establish a strong foundation for the institution’s future growth.
Supplemental Material
sj-pdf-1-phr-10.1177_00333549261455322 – Supplemental material for Managing Institutional Change Through Participatory Planning: Creating the College of Integrated Health Sciences at the University at Albany, State University of New York
Supplemental material, sj-pdf-1-phr-10.1177_00333549261455322 for Managing Institutional Change Through Participatory Planning: Creating the College of Integrated Health Sciences at the University at Albany, State University of New York by Allison A. Appleton, Eric R. Hardiman, Janine M. Jurkowski, Victoria M. Rizzo and Erin M. Bell in Public Health Reports®
Footnotes
Acknowledgements
The authors thank the University at Albany College of Integrated Health Sciences students, faculty, staff, and community for participating in this planning process. We also thank the working group members for their commitment and service in planning for the college.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this article are not publicly available. Data may be made available upon reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.