
Abstract
Communicable disease reporting is essential for public health surveillance, yet underreporting is common. California Title 17 mandates that health care providers report >80 communicable diseases to local health departments, according to the patient’s residence. We conducted a cross-sectional survey assessing health care provider knowledge, attitudes, and practices related to reporting requirements in Alameda County, California. Of 145 health care providers surveyed from April through June 2025, 127 (87.6%) were aware of Title 17 requirements and 105 (72.4%) had submitted at least 1 report. In multivariable logistic regression analysis using Firth penalized likelihood, the following were significantly associated with higher odds of reporting communicable diseases: having an awareness of reporting requirements versus no awareness (adjusted odds ratio [AOR] = 6.91; 95% CI, 1.21-58.36), having >10 years of clinical experience versus <5 years of clinical experience (11-20 years: AOR = 11.07 [95% CI, 2.30-64.68]; >20 years: AOR = 10.89 [95% CI, 2.28-62.59]), and having training in systems of institutional reporting versus no training (AOR = 5.37; 95% CI, 1.56-22.52). Misunderstanding reporting responsibility versus accurately identifying reporting responsibility was associated with lower odds of reporting communicable diseases. Improving clinician training, clarifying reporting expectations, and expanding electronic reporting systems may strengthen public health surveillance.
Keywords
Introduction
Timely communicable disease reporting is vital for effective public health surveillance, response, and prevention.1,2 Robust reporting systems are increasingly urgent as vaccination rates decline—driven by vaccine hesitancy, social media misinformation, rising nonmedical exemptions, COVID-19 pandemic–related disruptions, and variable public health recommendations—and eliminated diseases reemerge. The largest measles outbreaks since US elimination in 2000 have produced >1800 cases nationally in 2026 alone (as of May 2026)—96% among unvaccinated individuals—and modeling suggests that measles and other vaccine-preventable diseases could reestablish endemicity if trends continue.3-5
Communicable disease reporting is inconsistent, with studies documenting up to 90% underreporting and report completeness ranging from 9% to 99% across diseases and jurisdictions. 6 Fewer than half of Tennessee health care providers (hereinafter, providers) had ever reported a disease case to public health in 2017, 55% of Washington physicians understood reporting protocols in 2010, and Indiana provider reporting occurred 65% less frequently than laboratory reporting, with nearly 1-week delays.7-9 Documented barriers to reporting include complex reporting processes (eg, locating forms, determining reporting jurisdiction, manually transmitting reports), the undervaluation of surveillance, a tendency to report only confirmed cases, and unclear responsibilities among clinicians, infection prevention and control (IPC) practitioners, and laboratories.10,11
In California, Code of Regulations Title 17 requires health care providers to report >80 communicable diseases to local health departments. 12 Although noncompliance is a misdemeanor, enforcement is rare and adherence is promoted through education rather than prosecution.12-14 In 2024, this reporting infrastructure enabled the California Department of Public Health to identify the first clade 1b mpox case in the Americas—confirming the clade within 24 hours, tracing 83 contacts without secondary transmission, and detecting community spread by October 2025.15,16
No studies have examined Title 17 reporting among California providers. A 2001 study found 85% concordance between automated electronic laboratory reports and state records but did not assess provider behavior. 17 The Alameda County Public Health Department (ACPHD) addressed this gap through a cross-sectional survey assessing provider knowledge, attitudes, and practices regarding Title 17 requirements and determinants of reporting.
Methods
Study Design and Setting
From April through June 2025, we surveyed 145 Alameda County providers, including physicians, nurse practitioners, physician assistants, nurses, and other clinical staff.
Survey Development and Distribution
The 27-item survey, developed from a literature review and piloted with public health professionals, assessed Title 17 knowledge, attitudes toward reporting, current reporting practice, and demographic and professional characteristics (Supplement). Distribution occurred electronically via REDCap through ACPHD email distribution lists, professional society networks, hospital communications, and direct outreach. The APCHD invited licensed providers in Alameda County to participate regardless of specialty. Participation was voluntary and anonymous. No minimum sample size was prespecified.
Outcome Measures
The primary objective of this study was to examine the relationship between awareness of communicable disease reporting requirements and whether respondents had ever submitted a report, categorized as yes (to ACPHD or another public health authority) or no (including unsure)—termed reporters and nonreporters. Combining responses of unsure with responses of no reduced potential outcome misclassification. Covariates included provider role, specialty, clinical setting, years of clinical experience, population(s) served, IPC involvement (eg, participation in IPC programs, committees, or surveillance activities within health care institutions), and prior training or guidance on communicable disease reporting from one’s health care facility. Secondary objectives identified determinants of reporting and opportunities to improve Title 17 adherence.
Statistical Analysis
Descriptive statistics summarized characteristics, knowledge, attitudes, and practices. We used multivariable logistic regression to assess associations among provider characteristics, reporting knowledge and attitudes, and prior communicable disease reporting, with Firth penalized likelihood to account for the small sample size and potential separation, reported as adjusted odds ratios (AORs) with 95% CIs. We considered P < .05 to be significant. We used R version 2024.04.2 (R Foundation for Statistical Computing) for all analyses.
Ethics Approval
The Alameda County Health Research Review Committee deemed the project public health practice and quality improvement and, therefore, considered it exempt from human subjects research review.
Results
Respondent Characteristics
Of 145 respondents, 114 (78.6%) were physicians (Table 1). Common specialties included emergency medicine (n = 41; 28.3%), internal medicine (n = 37; 25.5%), and pediatrics (n = 27; 18.6%); 9 (6.2%) each were infectious disease physicians or family medicine physicians. Other specialties included obstetrics/gynecology (n = 3), IPC (n = 3), geriatrics (n = 2), and preventive medicine/public health (n = 2).
Characteristics and communicable disease reporting knowledge, attitudes, and practices among health care providers in Alameda County, California, April–June 2025 (N = 145) a
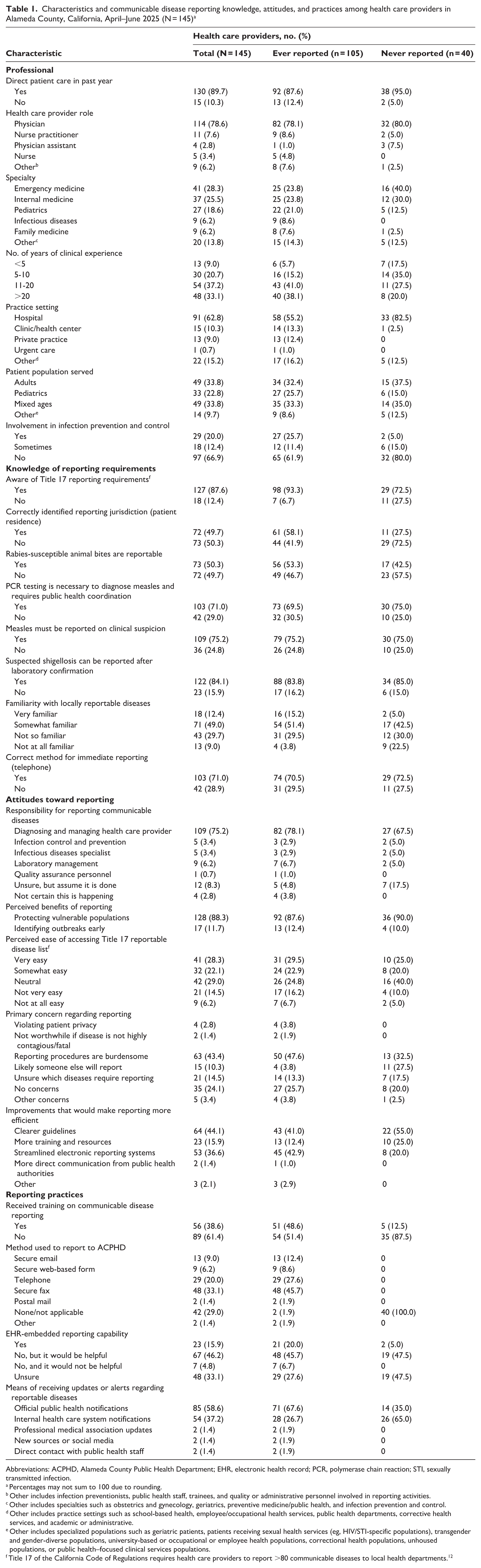
Abbreviations: ACPHD, Alameda County Public Health Department; EHR, electronic health record; PCR, polymerase chain reaction; STI, sexually transmitted infection.
Percentages may not sum to 100 due to rounding.
Other includes infection preventionists, public health staff, trainees, and quality or administrative personnel involved in reporting activities.
Other includes specialties such as obstetrics and gynecology, geriatrics, preventive medicine/public health, and infection prevention and control.
Other includes practice settings such as school-based health, employee/occupational health services, public health departments, corrective health services, and academic or administrative.
Other includes specialized populations such as geriatric patients, patients receiving sexual health services (eg, HIV/STI-specific populations), transgender and gender-diverse populations, university-based or occupational or employee health populations, correctional health populations, unhoused populations, or public health–focused clinical services populations.
Title 17 of the California Code of Regulations requires health care providers to report >80 communicable diseases to local health departments. 12
Most respondents (n = 130; 89.7%) had provided direct communicable disease care within the past year; 91 (62.8%) worked in hospitals (Table 1). The number of years of clinical experience varied across respondents: <5 years (n = 13; 9.0%), 5 to 10 years (n = 30; 20.7%), 11 to 20 years (n = 54; 37.2%), and >20 years (n = 48; 33.1%). Forty-seven respondents (32.4%) cited IPC involvement; 56 (38.6%) received reporting training. Most (n = 127; 87.6%) were aware of Title 17 requirements; 105 (72.4%) had submitted at least 1 report.
Multivariable Analysis of Determinants of Reporting
Being aware of Title 17 (AOR = 6.91; 95% CI, 1.21-58.36; P = .03), having 11 to 20 years of clinical experience (AOR = 11.07; 95% CI, 2.30-64.68; P = .002) or >20 years of clinical experience (AOR = 10.89; 95% CI, 2.28-62.59; P = .002), and having prior reporting training (AOR = 5.37; 95% CI, 1.56-22.52; P = .01) were significantly associated with higher odds of reporting communicable diseases (Table 2).
Multivariable logistic regression analysis of determinants of communicable disease reporting among health care providers in Alameda County, California, April–June 2025 a
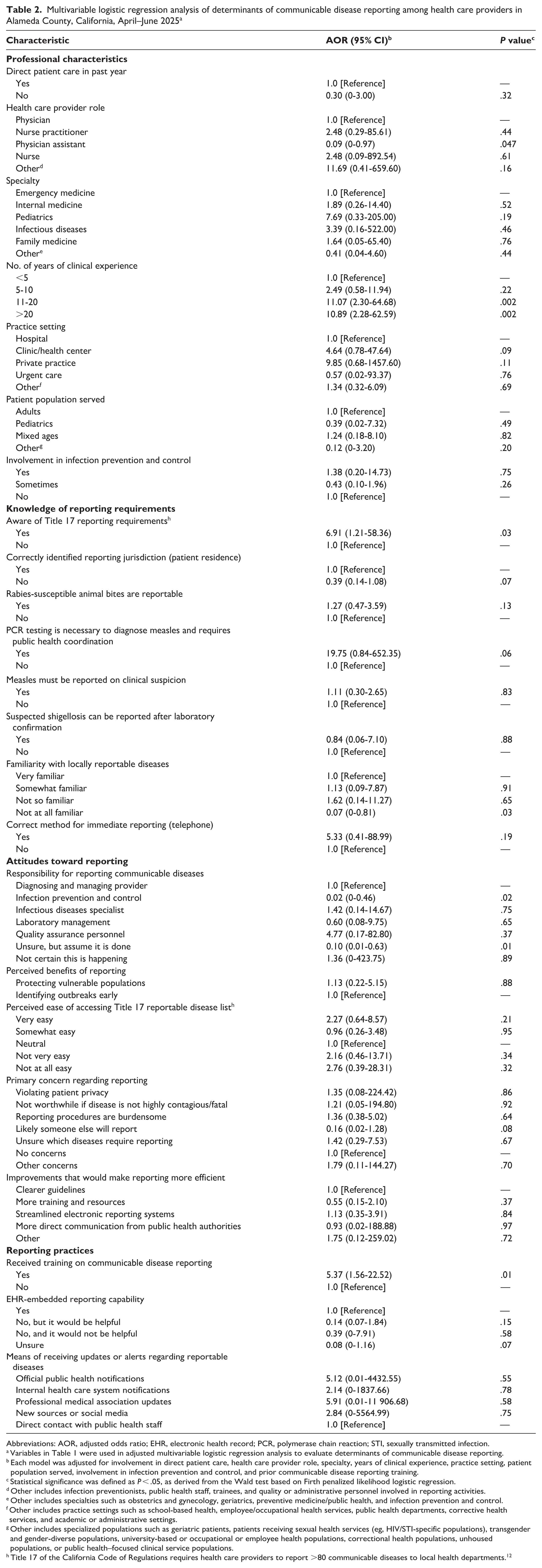
Abbreviations: AOR, adjusted odds ratio; EHR, electronic health record; PCR, polymerase chain reaction; STI, sexually transmitted infection.
Variables in Table 1 were used in adjusted multivariable logistic regression analysis to evaluate determinants of communicable disease reporting.
Each model was adjusted for involvement in direct patient care, health care provider role, specialty, years of clinical experience, practice setting, patient population served, involvement in infection prevention and control, and prior communicable disease reporting training.
Statistical significance was defined as P < .05, as derived from the Wald test based on Firth penalized likelihood logistic regression.
Other includes infection preventionists, public health staff, trainees, and quality or administrative personnel involved in reporting activities.
Other includes specialties such as obstetrics and gynecology, geriatrics, preventive medicine/public health, and infection prevention and control.
Other includes practice settings such as school-based health, employee/occupational health services, public health departments, corrective health services, and academic or administrative settings.
Other includes specialized populations such as geriatric patients, patients receiving sexual health services (eg, HIV/STI-specific populations), transgender and gender-diverse populations, university-based or occupational or employee health populations, correctional health populations, unhoused populations, or public health–focused clinical service populations.
Title 17 of the California Code of Regulations requires health care providers to report >80 communicable diseases to local health departments. 12
Physician assistants had significantly lower odds of reporting communicable diseases than other provider types (AOR = 0.09; 95% CI, 0-0.97; P = .047) (Table 2). Believing that IPC staff were primarily responsible for reporting (AOR = 0.02; 95% CI, 0-0.46; P = .015) and being unsure who was responsible but assuming that reporting occurred (AOR = 0.10; 95% CI, 0.01-0.63; P = .01) were also associated with lower odds of reporting communicable diseases. Being unfamiliar with locally reportable diseases predicted significantly lower odds of reporting communicable diseases (AOR = 0.07; 95% CI, 0-0.81; P = .03). No other variables remained significant after adjustment.
Knowledge and Attitudes
Most respondents (n = 103; 71.0%) identified the telephone as the appropriate method for immediate reporting; 72 (49.7%) recognized that reports should be directed to local health departments based on patient residence rather than location of care or laboratory testing (Table 1). Half of respondents (n = 73; 50.3%) knew that all rabies-susceptible animal bites must be reported. Most (n = 109; 75.2%) recognized that measles must be reported immediately upon clinical suspicion and confirmed via public health–coordinated polymerase chain reaction testing (n = 103; 71.0%). Most (n = 122; 84.1%) knew that shigellosis can be reported after laboratory confirmation.
Half of respondents (n = 73; 50.3%) found the Title 17 disease list very or somewhat easy to access (Table 1). Most respondents (n = 109; 75.2%) identified diagnosing providers as primarily responsible for reporting; 9 (6.2%) designated laboratory management and 5 (3.4%) cited IPC practitioners as responsible while 12 (8.3%) were unsure but assumed that reporting occurred.
Most respondents (n = 128; 88.3%) identified protecting populations at increased risk of infectious disease transmission (eg, people in congregate living settings) as the primary reporting benefit (Table 1). Barriers to reporting included burdensome reporting procedures (n = 63; 43.4%)—time constraints, duplicative data entry, and lack of streamlined electronic reporting systems—uncertainty about which diseases require reporting (n = 21; 14.5%), and the assumption that someone else will report cases (n = 15; 10.3%).
Current Practice and Suggested Improvements
Respondents received reporting updates through official public health (n = 85; 58.6%) or internal health care (n = 54; 37.2%) notifications. Twenty-three respondents (15.9%) had electronic health record (EHR)–based reporting, although 67 of 74 respondents (90.5%) without such tools indicated that they would be helpful (Table 1).
Respondents prioritized clearer guidelines (n = 64; 44.1%) and electronic systems (n = 53; 36.6%) to improve reporting efficiency over additional training (n = 23; 15.9%) or more public health communication (n = 2; 1.4%) (Table 1).
Free-text responses emphasized automation and EHR integration (eg, automated laboratory reporting, EHR-triggered alerts, embedded electronic case reporting [eCR] forms) to reduce manual entry. Respondents also highlighted unclear reporting responsibility, suggesting that laboratories, IPC practitioners, or dedicated staff—rather than frontline clinicians—complete reports, and they called for clearer guidance, accessible materials, streamlined forms, and receipt confirmation.
Discussion
Despite broad awareness of Title 17 requirements among all providers, more than one-quarter of respondents in our study had never reported a communicable disease—a gap better explained by experiential and structural factors, including clinical experience, prior training, and procedural familiarity, than by disease-specific knowledge. These findings suggest that reporting depends less on recalling criteria than on institutional reinforcement of workflow processes.
Thirty-nine percent of respondents received training on reporting communicable diseases at their health care institutions, which was positively associated with reporting. Systems-level interventions—onboarding modules, refresher trainings, and EHR-integrated guidance emphasizing reporting to local health departments according to patient residence—may prove more effective than knowledge campaigns, particularly for early career providers.
Role ambiguity appears to be an important barrier to reporting communicable diseases. When compared with most respondents who identified diagnosing providers as principally responsible for reporting notifiable diseases, those deferring to laboratory or IPC staff or assuming that reporting occurred elsewhere had significantly lower odds of reporting communicable diseases. Title 17 mandates that providers and laboratories report independently, creating redundancy intended to maximize surveillance completeness that diffuses responsibility. 12 Formalizing IPC as the reporting lead—with frontline clinicians identifying suspected cases—may clarify accountability while leveraging IPC’s established public health relationships. 18 Laboratory-initiated eCR can reduce clinician reporting burden for routine reportable conditions—such as laboratory-confirmed infections that require limited clinical interpretation—while reserving clinician involvement for cases requiring immediate clinical context. 19
Electronic reporting remains underused: 16% of respondents reported access to EHR-based tools, while >90% of respondents without access to EHR-based tools indicated that they would find such tools helpful. EHR-embedded templates, automated alerts, and mobile prepopulated forms reduce procedural burden while improving timeliness and completeness.6,20-25 Such targeted strategies have improved reporting efficiency elsewhere and could be adapted locally.
This study gains importance given California’s role in the West Coast Health Alliance, which was formed in September 2025 to coordinate regional responses to infectious disease threats. 26 California’s rapid mpox response demonstrated what robust reporting achieves: strengthening provider adherence remains essential as vaccination rates decline and previously controlled diseases threaten to reemerge.
Limitations
This study had several limitations. First, self-reported data were subject to recall and social desirability bias. Second, the cross-sectional design limited causal inference. Third, the small convenience sample represented <2% of licensed physicians in Alameda County. 27 Wide 95% CIs indicated imprecision; AORs should be interpreted as directionally informative rather than precise effect estimates. Nonetheless, the heterogeneous sample offers useful quality improvement insights and can inform future research directions.
Conclusion
Improving communicable disease reporting requires institutionalizing clear processes, defined roles, and routine training. Targeted education for early career clinicians, explicit assignment of reporting responsibilities to designated clinical and administrative staff, and streamlined eCR workflows may strengthen surveillance and outbreak detection.
Supplemental Material
sj-pdf-1-phr-10.1177_00333549261457422 – Supplemental material for Experiential and Structural Determinants of Communicable Disease Reporting Among Health Care Providers in Alameda County, California
Supplemental material, sj-pdf-1-phr-10.1177_00333549261457422 for Experiential and Structural Determinants of Communicable Disease Reporting Among Health Care Providers in Alameda County, California by Tyler Martinson, Sana M. Khan, Dustin T. Heaton, Munira Shemsu, Nicholas J. Moss and Kavita K. Trivedi in Public Health Reports®
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The survey instrument used in this study is provided as supplemental material. Deidentified survey data may be made available from the corresponding author upon reasonable request, in accordance with institutional policies and public health data governance considerations.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.