
Abstract
Objectives:
Mercury exposure is a preventable public health concern that arises from multiple environmental, dietary, and occupational exposure pathways and poses disproportionate risks to the fetus during pregnancy. However, routine identification in clinical care is limited. This study aimed to generate practice-informed evidence from primary care clinicians serving populations at risk of mercury exposure to inform the development and implementation of evidence-based guidance on mercury exposure screening in primary care.
Methods:
In April 2025, we conducted a qualitative study using semistructured interviews online or by telephone with 12 primary care clinicians practicing in outpatient and hospital-affiliated settings in New York City. Interviewers examined clinicians’ knowledge of mercury exposure, current screening practices, perceived barriers, and recommendations for practical supports. Informed by the Knowledge-to-Action framework, we analyzed data using reflexive thematic analysis and reported in accordance with consolidated criteria for reporting qualitative research.
Results:
Clinicians described mercury exposure as a recognized but low-priority issue in routine primary care. Screening was rare and largely reactive rather than preventive. Clinicians identified health care system–level barriers, including lack of training, lack of screening guidance, limited access to testing, health insurance restrictions, time constraints, and the absence of decision support for electronic health records. Despite these barriers, clinicians supported standardized, practical screening guidance, often referencing lead exposure screening as a useful model. They emphasized the need for simple risk-based tools, workflow integration, health care provider training, and policy support.
Conclusions:
Aligning public health evidence with clinical systems through evidence-based screening guidance, workflow integration, and supportive policy is essential to advance equitable mercury exposure identification and prevention in primary care.
Keywords
Mercury exposure is a persistent environmental health concern in the United States. Exposure occurs through multiple pathways, most commonly through contaminated fish and seafood but also through cultural practices, consumer products, occupational activities, and environmental sources.1-3 Mercury exposure is associated with neurologic impairment, developmental delays, cardiovascular effects, and other chronic conditions, and emerging evidence suggests that cumulative exposure may contribute to adverse health outcomes later in life.4,5 Although severe poisoning is uncommon, low-level and chronic exposure continues to pose meaningful population-level risks.4-6 Exposure during pregnancy and early childhood is linked to lasting neurodevelopmental effects, and cumulative exposure contributes to adverse health in adulthood.7-9 Risk of mercury exposure is elevated in communities where certain dietary patterns, product use, housing conditions, occupational exposures, and neighborhood environments increase the likelihood of repeated or unrecognized exposure, contributing to persistent disparities and inequities in exposure and health outcomes.10-12 Mercury exposure is, therefore, a preventable public health concern.
Although national biomonitoring data show declining median blood mercury levels, exposure remains detectable in the US population, including women of childbearing age.13,14 Environmental Protection Agency (EPA) summaries of National Health and Nutrition Examination Survey (NHANES) data reported a median blood mercury level of 0.6 µg/L and a 95th percentile level of 3.8 µg/L among women of childbearing age from 2017 through 2018, indicating that a subset of women continues to experience elevated exposure levels.13,14 These national trends demonstrate persistent exposure among subgroups but may still obscure important variation across populations, particularly among groups with repeated or unrecognized exposure. In practice, clinicians may encounter meaningful exposure risk in certain communities even when national averages appear to improve. State-level surveillance highlights this variation: data from the New York State Heavy Metals Registry show that the number of adults with elevated blood mercury levels increased from 2016 through 2020, with 6403 adults reported in 2020 alone. 15 During this period, >23 000 adults were tested. These findings indicate ongoing detection of elevated mercury levels through clinical and occupational surveillance systems, even as national median levels have declined. This context makes New York City a relevant setting in which to examine whether routine primary care screening practices reflect documented environmental health risks.
Dietary intake is the dominant pathway for mercury exposure. Methylmercury exposure occurs primarily through fish and seafood consumption, whereas inorganic mercury exposure is more commonly associated with occupational settings and certain consumer products.14,16 Both the EPA and the Food and Drug Administration (FDA) identify consumption of fish and seafood containing methylmercury as the primary source of exposure in the United States.14,16,17 NHANES analyses demonstrate a clear dose–response relationship between seafood intake and blood mercury levels: women consuming fish or shellfish at least twice weekly had approximately 7 times higher geometric mean blood mercury concentrations than women reporting no seafood consumption in the prior 30 days.18-20 Exposure patterns are reflected in the proportion exceeding established reference levels. An EPA analysis of NHANES data from 1999 through 2010 found that a measurable subset of women aged 16 to 49 years had blood methylmercury concentrations exceed-ing 5.8 µg/L, the level corresponding to the EPA reference dose, although the proportion above this threshold declined across survey cycles.13,14 In addition to dietary sources, mercury has been documented in certain consumer products, including some skin-lightening creams.17,21 FDA and Centers for Disease Control and Prevention investigations have identified skin-lightening products containing extremely high mercury concentrations, including levels exceeding 12 000 parts per million (ppm), and FDA testing has documented concentrations as high as 200 000 ppm.17,21 Together, these data suggest that mercury exposure is clinically relevant for prevention but is not systematically addressed in routine care, underscoring the importance of exposure history in clinical assessment, including dietary, occupational, and consumer product–related exposures.
Despite well-established exposure pathways, routine identification of mercury exposure in clinical care is limited.22-24 In the absence of standardized screening guidance, identification depends largely on clinician awareness during brief encounters.25-27 Primary care plays a central role in prevention and is often the most consistent point of contact for people in communities at risk of mercury exposure.28-30 Routine visits offer opportunities for risk assessment and counseling; however, prevention of mercury exposure is not consistently supported by clear guidance, standardized workflows, or decision support.31-33 This gap leaves decisions to individual clinician judgment and results in variability across settings. Lead exposure screening demonstrates how environmental risks can be incorporated into routine care when clear guidance, defined thresholds, reporting requirements, and infrastructure are in place.34-37 In contrast, comparable guidance for mercury exposure screening is limited. Despite documented pathways for mercury exposure, identified populations at risk of mercury exposure, and persistent disparities between groups, mercury screening has not been integrated into routine preventive care, reflecting a gap in policy and implementation rather than feasibility.12,22,23 While lead screening relies on well-defined blood thresholds to guide intervention, mercury exposure assessment is more complex because blood mercury levels may reflect recent dietary intake and decline over time, and interpretation depends on the form of mercury and exposure context.
The absence of evidence-based mercury screening guidance reflects broad gaps in public health and clinical coordination. 26 Uncertainty persists regarding when screening should occur, which populations should be prioritized, how risk should be assessed, and how findings should be linked to public health follow-up.27,33 As a result, identification is inconsistent and largely dependent on clinician judgment. Framing these gaps in mercury exposure screening solely as a knowledge deficit overlooks barriers in the health care system.
This study aimed to generate practice-informed evidence from primary care clinicians serving populations at risk of mercury exposure to inform development of evidence-based screening guidance and implementation strategies relevant to public health policy and practice. Through qualitative interviews with primary care providers in New York City, we sought to (1) characterize clinicians’ knowledge and training related to mercury exposure, current screening and risk assessment practices, and perceived barriers to routine identification and (2) identify facilitators and practical supports that clinicians believe are necessary to enable consistent, equitable screening and follow-up. Guided by the Knowledge-to-Action framework, the study focused on gaps in existing evidence, frontline practice, and implementation supports.38,39 Our findings will inform efforts to strengthen prevention infrastructure and reduce disparities in mercury exposure detection.
Methodology
Study Design and Approach
We conducted a qualitative study using semistructured interviews to examine primary care clinicians’ knowledge, practices, perceived barriers, and facilitators related to mercury exposure screening and risk assessment among socioeconomically vulnerable populations in New York City. A qualitative approach was appropriate given the exploratory nature of the topic, limited guidance on mercury screening in primary care, and the aim to generate in-depth practice-informed insights within a clinically relevant urban context where multiple exposure pathways may occur. Reporting followed the consolidated criteria for reporting qualitative research. 40 The University of New Haven Institutional Review Board reviewed and approved this study (2025-013), and the research team conducted all procedures in accordance with institutional ethical standards.
Research Team and Reflexivity
The study’s lead investigator (N.B.), a doctoral researcher trained in qualitative methods with experience in public health practice and research, conducted all interviews. Participants had no prior professional relationship with the interviewer. The interviewer aimed to minimize assumptions during data collection and analysis and documented analytic decisions to support reflexivity and transparency. To strengthen interpretive rigor, the interviewer iteratively discussed theme development and interpretation with a senior researcher (P.R.) during the study to ensure that findings were grounded in participant accounts.
Participants and Recruitment
Participants were primary care clinicians, including physicians, nurse practitioners, and physician assistants, who provide direct patient care to New York City residents. We used purposive sampling to recruit clinicians from outpatient clinics and hospital-affiliated settings serving racially, ethnically, and socioeconomically diverse and vulnerable populations. We distributed interview invitations via email and text through professional contacts, and we encouraged participants to share the invitation with colleagues, using a snowball sampling approach. Recruitment continued until we achieved thematic saturation, resulting in 12 completed interviews from April through June 2025.
Data Collection
We conducted the interviews with clinicians online via Microsoft Teams or by telephone, with each interview lasting approximately 15 to 30 minutes. Before participation, clinicians received a study information sheet describing the purpose, procedures, and confidentiality protections, and we obtained written informed consent. We also obtained and documented verbal informed consent before each interview in accordance with institutional review board–approved procedures. We audio-recorded the interviews with permission and transcribed them verbatim. The interview guide included questions designed to examine clinicians’ knowledge and training related to mercury exposure, screening and risk assessment practices, barriers and facilitators to routine identification, and recommendations for practical tools or guidance. The Knowledge-to-Action framework guided development of the interview guide and analytic focus to examine gaps in evidence, clinical practice, and implementation support systems.38,39
Data Analysis
We analyzed transcripts using reflexive thematic analysis following Braun and Clarke’s 6-phase approach. 41 The research team read transcripts repeatedly for familiarization and generated initial codes across the dataset. We then grouped codes into candidate themes aligned with study aims and reviewed and refined them for coherence across participants. We used structured Microsoft Excel–based matrixes to organize codes, themes, and illustrative quotes and to maintain an audit trail. Before analysis, we removed identifying information.
Results
Participant Characteristics
Twelve primary care clinicians (P1-P12) participated: 6 physicians, 4 nurse practitioners, and 2 physician assistants (Table 1). Participants practiced across multiple outpatient settings in New York City, primarily in the Bronx and Queens. Six participants worked in hospital-based clinics and 6 in private family medicine practices. Most participants served racially and ethnically diverse, low-income, uninsured, and immigrant populations, many with limited English proficiency and limited access to preventive services.
Characteristics, mercury exposure–related training, and guideline familiarity among 12 primary care clinicians participating in qualitative interviews conducted in New York City, April 2025
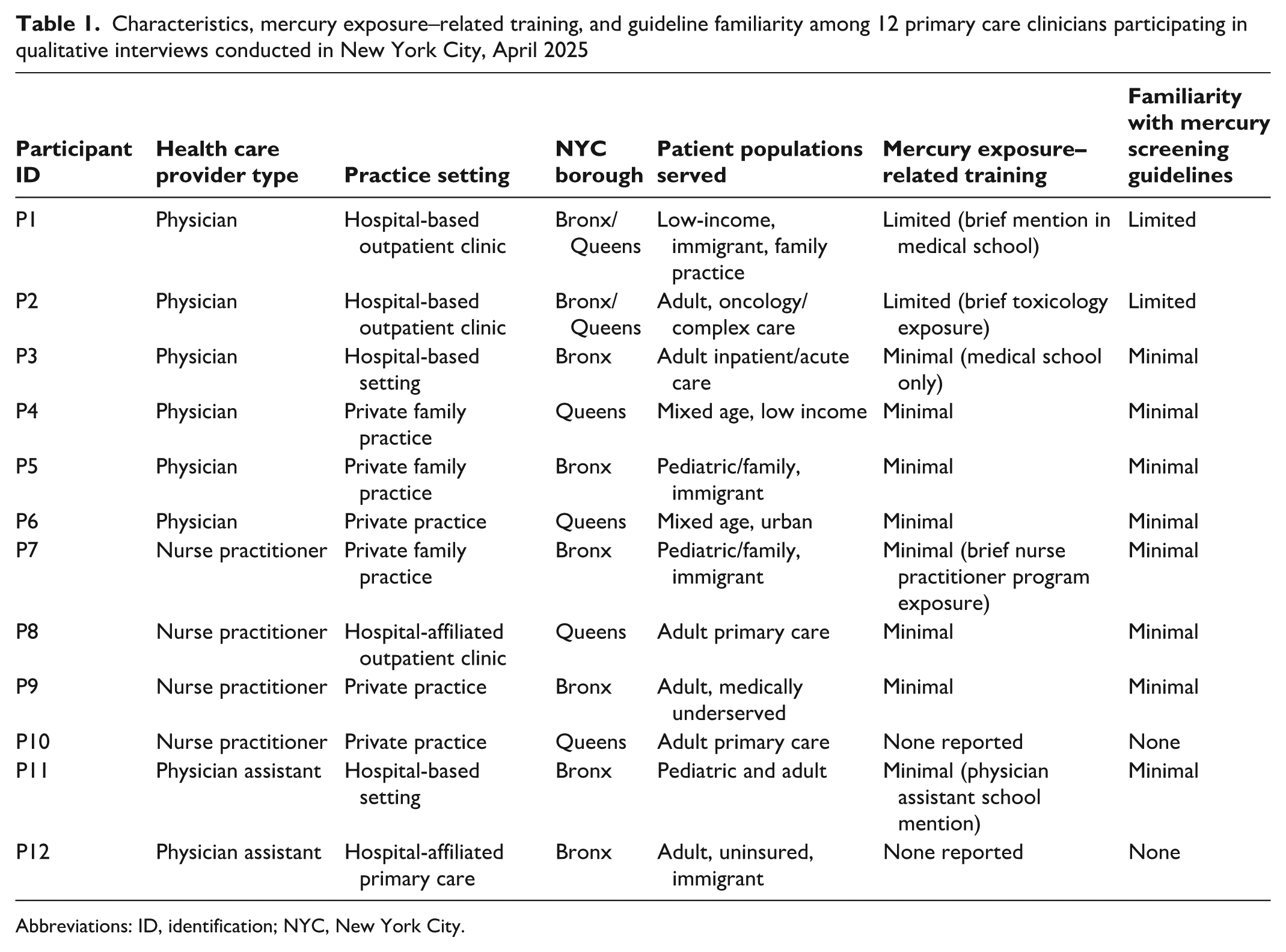
Abbreviations: ID, identification; NYC, New York City.
Across roles and settings, clinicians reported minimal formal training related to mercury exposure or screening and limited familiarity with existing guidance. Key themes and illustrative quotes are summarized in Table 2.
Key themes and illustrative quotes from qualitative interviews with 12 primary care clinicians regarding mercury exposure screening in New York City, April 2025
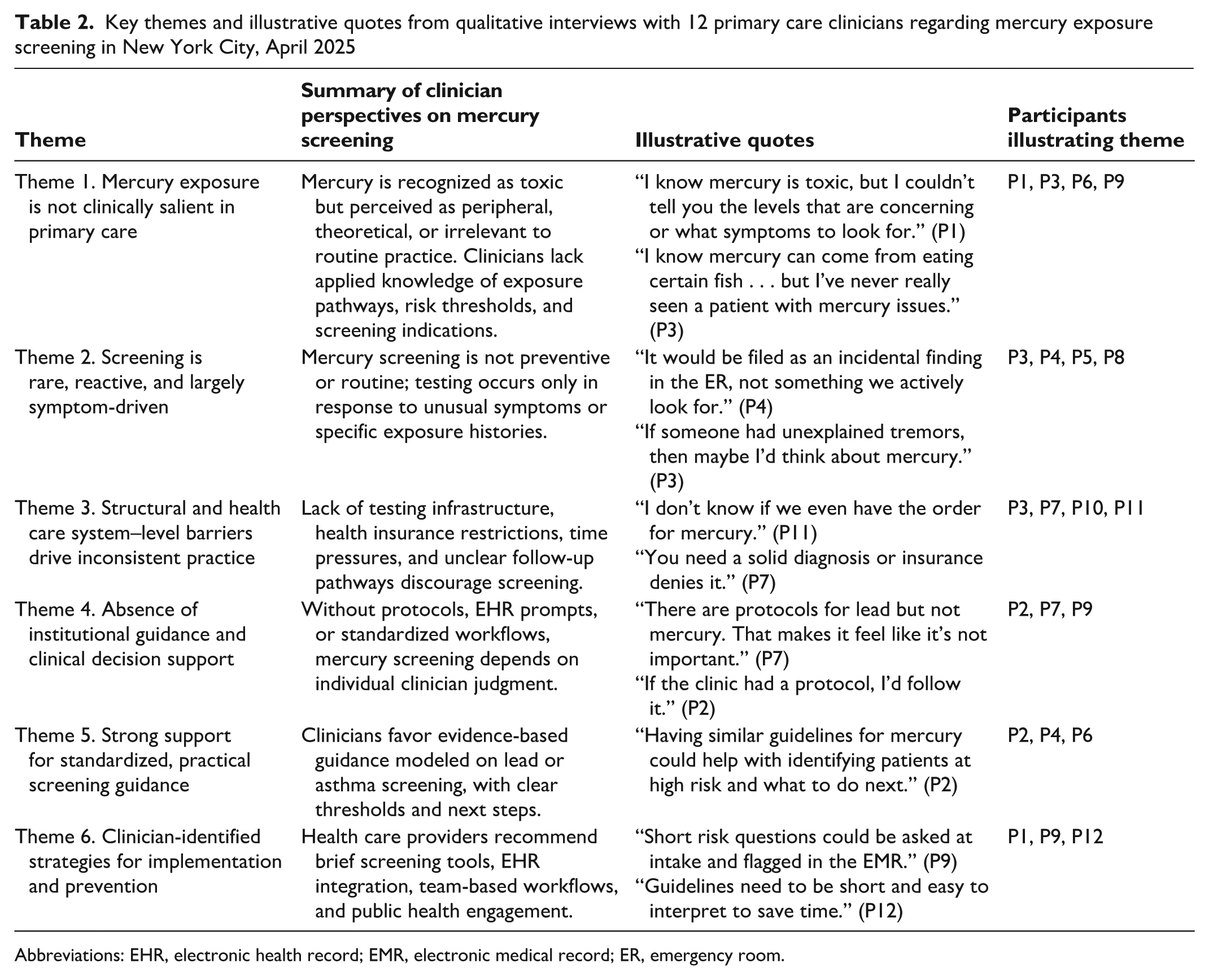
Abbreviations: EHR, electronic health record; EMR, electronic medical record; ER, emergency room.
Theme 1: Mercury Exposure Is Not Clinically Salient in Primary Care
Clinicians consistently described mercury exposure as peripheral rather than integrated into routine care. While most recognized mercury as toxic, they lacked applied knowledge of exposure pathways, populations at risk of mercury exposure, screening thresholds, or follow-up steps. Awareness of mercury exposure pathways was typically limited to fish consumption or industrial exposure and was often attributed to media coverage or brief training references.
Some interviewees interpreted the absence of screening as a sign of limited clinical relevance. As a physician explained, “I know mercury can come from eating certain fish like tuna or swordfish, and maybe from industrial work, but I’ve never really seen a patient with mercury issues in my practice” (P3). In the absence of systematic screening or guidance, clinicians may have limited opportunities to identify mercury exposure even when it is present. Another interviewee noted, “We talk about lead exposure more often; mercury just doesn’t come up unless it’s in the news” (P6).
Several clinicians acknowledged uncertainty about how mercury exposure might present clinically or when screening would be appropriate, with one stating, “I know mercury is toxic, but I couldn’t tell you the levels that are concerning or what symptoms to look for” (P1). Participants also expressed uncertainty about the local epidemiology of mercury exposure. As one remarked, “I’m not sure how common this type of exposure is specifically in New York City” (P9).
Theme 2: Screening Is Rare, Reactive, and Largely Symptom-Driven
No participants described mercury screening as part of routine preventive care. Instead, clinicians described testing as rare and triggered by unusual symptoms or known exposures. Clinicians reported considering testing primarily in cases of unexplained neurologic symptoms, pediatric concerns, or occupational risk.
One clinician summarized, “Right now, we don’t have anything in place to do that . . . it’s not something we have on our radar” (P1). Another stated, “It would be filed as an incidental finding in the ER [emergency room], not something we actively look for” (P4).
When testing occurred, it was prompted by atypical presentations rather than systematic risk assessment. One interviewee said, “If someone had a weird metallic taste or unexplained tremors, then maybe I’d think about mercury” (P3). Another recalled, “I had a case where a child came from abroad and had both lead and mercury checked, but that was exceptional” (P5).
Theme 3: Structural and Health Care System–Level Barriers Drive Inconsistent Practice
Clinicians emphasized that limited screening reflected structural barriers rather than lack of concern. A central issue was uncertainty about testing infrastructure, including how to order tests and how to interpret results. One participant said, “I don’t know if we even have the order for mercury,” and later asked, “If you get the results and they end up being high, then what do you do next?” (P6).
Absence of health insurance coverage was another barrier to mercury testing. As a clinician explained, “You need to have a solid and valid diagnosis to test for mercury. If not, insurance denies it—that’s the biggest obstacle.” Time constraints further limited clinicians’ ability to assess environmental exposure risks.
Several clinicians described busy primary care workflows with limited opportunity to take detailed exposure histories. One participant stated, “It’s hard to take a full exposure history when you have 15 minutes per patient” (P3).
Theme 4: Absence of Institutional Guidance and Clinical Decision Support
Participants consistently contrasted mercury screening with lead screening, highlighting the absence of protocols, electronic health record prompts, and standardized workflows for mercury screening. One participant noted, “There are protocols for lead but not mercury. That makes it feel like it’s not important” (P7). Another clinician stated, “If the clinic had a protocol, I’d follow it. But without it, mercury just falls through the cracks” (P2).
The lack of electronic health record prompts and order sets further limited uptake. Clinicians reported relying on external resources such as UpToDate when confronted with unfamiliar exposures, underscoring the absence of integrated decision support.
Theme 5: Strong Support for Standardized, Practical Screening Guidance
Despite limited current screening, clinicians supported formal, evidence-based guidance. Several interviewees endorsed adapting models from lead, asthma, or depression screening. One participant stated, “Having similar guidelines for mercury could help with identifying patients at high risk and what to do next if levels are high” (P2). Other interviewees suggested incorporating mercury screening into annual visits or pairing it with lead protocols to improve efficiency.
Participants emphasized that guidelines would need to be accompanied by education. One noted, “Knowledge and awareness would be very helpful for pediatricians, OB/GYNs [obstetricians-gynecologists], and primary care providers” (P6).
Theme 6: Clinician-Identified Strategies for Implementation and Prevention
Participants offered concrete recommendations to operationalize mercury screening in primary care settings, including the development of brief risk-based questionnaires, digital screening tools or calculators, and integration of screening into intake or triage workflows. Several clinicians suggested that medical assistants could administer short screening tools, with automated prompts guiding health care providers when follow-up testing is indicated.
Clinicians also emphasized the importance of public health engagement to complement clinical screening. Suggested strategies included patient education materials, clinic posters, and broad public health communication campaigns to raise awareness of mercury exposure risks. Participants stressed that screening guidance should be concise, easy to interpret, and supported by clear referral pathways to make mercury screening as feasible and routine as lead testing.
Discussion
Across diverse primary care settings, participants viewed mercury exposure as a recognized concern but a low-priority issue. Screening was rare and reactive, shaped by lack of guidance, limited testing access, health insurance barriers, and time constraints. Nevertheless, clinicians consistently supported the development of standardized, practical screening guidance modeled on existing environmental health programs. The findings reveal a clear disconnect between public health evidence on mercury exposure risk and its integration into routine primary care practice.
This study demonstrates that although mercury exposure is recognized as a public health concern, clinicians serving socioeconomically vulnerable urban populations rarely address it in routine primary care. Preventive care did not incorporate mercury screening and typically considered it only in response to unusual symptoms or known exposure.
Perceptions that mercury exposure is uncommon may reflect the absence of routine screening infrastructure. Without standardized risk assessment, testing pathways, or decision support, exposure is clinically invisible. Viewed through a Knowledge-to-Action lens, the limited integration of mercury exposure screening into routine primary care reflects an implementation gap in which public health evidence is not translated into routine clinical systems.38,39 This gap may persist even where health care provider–facing guidance on mercury exposure assessment exists, suggesting that available resources are not consistently integrated into routine primary care workflows. 42
The contrast between lead and mercury screening highlights this gap. Lead exposure is routinely addressed because defined thresholds, guidance, and workflows support consistent practice,36,37 whereas mercury exposure lacks comparable infrastructure and is therefore addressed inconsistently. Clinicians in our study frequently described uncertainty regarding testing workflows, result interpretation, and follow-up pathways, reinforcing how the absence of standardized infrastructure may limit implementation of mercury screening in routine care.
Clinicians expressed strong support for practical, risk-based mercury screening guidance integrated into existing workflows. Suggested strategies included brief exposure history questions addressing dietary, occupational, and consumer product–related risks, as well as integration of screening prompts into clinical workflows, clear referral pathways, and alignment with public health reporting and health insurance coverage. Participants also emphasized the need for alignment across public health, health systems, and payers to support implementation. Existing environmental and public health guidance provides a foundation for evaluation of suspected mercury exposure, but our findings suggest that these resources are not consistently translated into routine primary care workflows. Variation in state-level surveillance and reporting approaches may also contribute to differences in implementation pathways across jurisdictions.
Together, these findings indicate that gaps in mercury exposure detection reflect health care system–level and policy limitations rather than clinician unwillingness to assess or address mercury exposure. Addressing these gaps will require concise evidence-based guidance, integration into electronic systems, reimbursement alignment, and implementation research to support sustained adoption in real-world primary care settings.
Limitations
This study had several limitations. First, it included a qualitative sample of primary care clinicians from New York City, and findings may not be generalizable to other regions or health care systems. Second, data were based on self-reported clinician perspectives and may reflect recall bias or social desirability influences. Third, the study focused exclusively on clinician experiences and did not include patient perspectives, public health officials, or direct observation of clinical workflows, which may limit understanding of how barriers to mercury exposure screening are experienced and operationalized across the health care system and care settings. Fourth, the analysis addressed mercury exposure broadly and did not distinguish among specific exposure pathways or assess clinical outcomes. The aim was to identify gaps in screening infrastructure and implementation readiness rather than to evaluate the effectiveness of certain mercury screening approaches or interventions. However, thematic saturation was achieved, and the study was conducted in a setting with documented mercury exposure risks, supporting the relevance and transferability of the identified implementation gaps. Future research across diverse geographic contexts, including coastal, riverine, and industrial regions, can build on these findings to further inform screening strategies.
Conclusion
This study shows that primary care clinicians lack the guidance, infrastructure, and implementation supports needed to address mercury exposure routinely. Screening was uncommon and largely reactive, shaped by unclear identification of groups at risk of mercury exposure, absence of standardized guidance, limited access to testing, health insurance coverage limitations, reimbursement barriers, and limited clinical decision support.
Clinicians expressed strong willingness to strengthen practice through practical, risk-based screening approaches modeled on established environmental health programs. Advancing equitable mercury exposure identification will require coordinated efforts to define priority populations, integrate screening into clinical systems, align reimbursement with prevention, and support health care provider education, consistent with a Knowledge-to-Action approach.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support of the University of New Haven Institutional Review Board, the Marvin K. Peterson Library, and the Writing Center in the completion of this project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The qualitative data generated during this study are not publicly available due to confidentiality considerations and the potential risk of participant identification. Deidentified excerpts are included in the article to support transparency and analytic rigor.