
Abstract
Objectives:
Disease intervention specialists (DISs) provide critical support within the public health workforce. The newly launched Certificate in Disease Intervention (CDI) program is designed to validate their skills. We assessed interest in and feasibility of establishing pathways into DIS certification for undergraduate students in the United States.
Methods:
To qualitatively assess perspectives on undergraduate DIS pathways, we conducted a series of 11 voluntary, semistructured listening sessions with educators who work with undergraduate students who are completing public health training. Interviews took place virtually from January through March 2025. We used data from the 2021 and 2024 Public Health Workforce Interests and Needs Survey (PH WINS) to assess educational backgrounds of DISs.
Results:
Capacity for and interest in establishing DIS pathways varied among participating institutions. Among the 2577 DISs from the PH WINS sample, a weighted estimate of 76.7% of DISs reported having at least a bachelor’s degree. Approximately half (n = 1372) of the sampled DISs reported having any type of additional certification(s).
Conclusions:
Listening session findings suggest some readiness to integrate DIS pathways within some undergraduate educational settings and the need for future implementation support. The educational background of the current DIS workforce suggests that undergraduate pathways into this career may be appropriate and that certification(s) in disease intervention–specific skills are somewhat common but currently lack a DIS-specific pathway. US undergraduate institutions may be equipped to integrate such pathways into their programs but will require support to increase awareness of the DIS field and feasibility of implementation.
The disease intervention specialist (DIS) role was originally developed by health departments in the 1930s in response to the spread of endemic syphilis. 1 While governmental public health agencies (eg, state and local health departments) are still the primary DIS employers in the United States, 2 the DIS role has evolved, now encompassing other infectious diseases such as tuberculosis, HIV/AIDS, and mpox3,4 and professionals with titles such as Communicable Disease Investigator and HIV Prevention Specialist. 5 We refer to this group of professionals as DISs throughout this study. Described as “shoe leather epidemiologists” for their engagement in community fieldwork, 6 DISs conduct empathetic investigations of sensitive issues. Although their work has historically focused on limiting the spread of communicable illnesses, including sexually transmitted infections, 1 their contact-tracing skills were invaluable during the COVID-19 pandemic. 7 DISs come from a wide range of educational backgrounds; most receive substantial on-the-job training, with limited consistency in requirements or role definitions across jurisdictions. 8 They have been classified into broader job classes (eg, health educators, community health workers)8-10 that may not reflect the critical roles they play as described in a job task analysis report. 4
The Centers for Disease Control and Prevention (CDC), the Association of Schools and Programs of Public Health (ASPPH), and the National Board of Public Health Examiners (NBPHE) have designed and will soon launch a Certified in Disease Intervention (CDI) certification program to help standardize and validate the knowledge and skills of DISs. 11 Earning the certification will involve qualifying for and then passing a standardized examination that covers 6 domains comprising essential DIS competencies. 12 Examination qualification requirements include a year of experience as a DIS and additional steps commensurate with educational attainment. 12 Among the potential future certificate earners are undergraduate students with an interest in public health who are considering joining the DIS workforce. To better understand the feasibility of establishing undergraduate pathways to CDI certification, ASPPH granted a subaward to the University of Minnesota Center for Public Health Systems (CPHS) to conduct a formative evaluation of potential future and existing undergraduate educational resources that could be leveraged as educational pathways to be eligible to sit for the CDI examination and enter the DIS workforce. Our preparation for this study included an environmental scan that yielded results relevant to institutions of higher education in the United States developing such pathways (Kirkland C, Dill J, Stabler H, Lazalde G, McDaniel N. Building Disease Investigation Specialist Certification Pathways Within Undergraduate Institutions: Report 1. University of Minnesota Center for Public Health Systems; 2025. Unpublished).
Few education programs cater to the preparation of DISs in undergraduate programs. 2 Our February 2025 search of the grey literature yielded information about relevant coursework from CDC and a training academy hosted by the University of South Florida School of Public Health.13,14 While many DISs hold associate’s or bachelor’s degrees—often in public health, biology, or the social sciences—most of their preparation occurs through practical, job-specific training provided by public health agencies.2,3 Recently, national organizations have sought to standardize DIS training, recognizing the critical role DISs play. 4 For example, a research team analyzed one university’s curriculum to assess how its Council on Education for Public Health (CEPH)–accredited programming aligned with DIS competencies described in a 2018 job task analysis report by the Public Health Accreditation Board. 2 The study found strong alignment between the bachelor of science in public health core curriculum and the job task analysis, reflecting potential suitability for undergraduate pathways into the DIS workforce. 2 Other studies have investigated undergraduate education in public health more broadly, highlighting increasing public health–focused training at the undergraduate level compared with the graduate level and tension between degrees that prepare students for careers such as DISs and more general curricula.15,16
Additional literature highlights partnerships between health agencies and colleges to deliver DIS-relevant needs. The Idaho Department of Health and Welfare and Idaho State University expanded agency capacity through enhancing undergraduate curriculum in sexually transmitted infection prevention, harm reduction, and care. 17 Several schools availed themselves of resources in local public health programs early in the COVID-19 pandemic, partnering with local health departments to fill contact-tracing roles.18-20 DIS roles can provide an entry point into the governmental public health workforce for those with an educational background relevant to public health and/or with lived experience that can guide their approach to the work, with experts recommending on-the-job training for remaining skill gaps. 2 These examples and findings suggest potential appropriateness of DIS pathways for undergraduates.
Many undergraduate institutions offer public health coursework; in 2020, US colleges and universities conferred more bachelor’s degrees in public health than master’s degrees in public health. 16 Existing resources supporting undergraduate training in public health may facilitate some programs’ alignment with CDI competencies. This alignment could benefit the public health workforce by closing gaps between public health training and entry-level public health careers. These considerations guided our study’s 2 goals: (1) characterize educational attainment of the DIS workforce and (2) assess institutional (ie, student, faculty, and staff) interest in, and feasibility of, establishing educational pathways to the DIS workforce in undergraduate institutions.
Methods
From October 2024 through May 2025, the University of Minnesota Center for Public Health Systems team used a multimethod approach to assess current facilitators and barriers of DIS pathway development at undergraduate institutions and the educational background of current DISs. We first conducted an analysis of educational attainment and professional certification among DISs using the 2021 and 2024 Public Health Workforce Interests and Needs Survey (PH WINS), an online survey of governmental public health workers in the United States that was fielded from September 2021 through January 2022 and from September 2024 21 through January 2025. 22 Analyses described the educational backgrounds of the current DIS workforce. Second, we conducted qualitative listening sessions with representatives from undergraduate-serving institutions and analyses of notes taken during the sessions. Qualitative analyses focused on understanding how CDI pathways might now or in the future fit within undergraduate education. We then reviewed findings from both parts, assessing how pathways might align with the educational attainment of those currently in the public health workforce. The University of Minnesota Institutional Research Board (IRB) determined this study was exempt from review on November 20, 2024, because it did not meet the definition of human subjects research per the US Department of Health and Human Services and US Food and Drug Administration’s definitions of such (IRB ID: STUDY00023935).
Quantitative Approach
For the quantitative component of this study, we drew on the 2021 and 2024 PH WINS data to generate a baseline (ie, pre–CDI launch) understanding of DIS-specific educational backgrounds. PH WINS is a nationally representative survey that characterizes individual workers in state and local health departments. We used job classification and educational attainment survey items to describe the educational background of those employed as DISs in local and state health agencies. Our sample included 2577 individuals who indicated “disease intervention specialist/contact tracer” as the role that best aligns with their work.
Participants reported their educational attainment by indicating degrees and certifications attained. We assessed the proportion of those with a bachelor’s degree or higher when considering formal degrees. In reporting certifications, participants selected options from a list reflecting common certifications (eg, physician board certification, nurse certification, certified community health worker) and/or could select the “other” option, which provided space for naming this other certification. We developed search parameters based on our literature review and CDI examination content to describe these “other” certifications and whether they aligned with DIS skills. Search queries scanned and initially classified the text, and then we confirmed the appropriateness of the classifications. If participants reported having a DIS-specific certification (eg, disease intervention specialist), they were classified as DIS certified. The research team categorized those with certifications that aligned with 1 or more of the other DIS-related terms as having DIS-related other certificates. We used Microsoft Excel and Stata version 18.5 (StataCorp) for these analyses.
Qualitative Approach
We conducted listening sessions with representatives from undergraduate-serving institutions. To recruit participants, we used ASPPH’s institutional research and National Center for Education Statistics (NCES) Integrated Postsecondary Education Data System (IPEDS) data 23 to identify US schools and programs offering undergraduate public health majors. With ASPPH guidance, we selected recruitment representatives from undergraduate institutions that varied in geography, CEPH accreditation, and minority-serving institution (eg, Historically Black Colleges and Universities, Tribal Colleges and Universities, Hispanic-serving institutions) status.24,25 The participants were typically undergraduate public health program directors and/or faculty who taught undergraduate public health courses. In addition to this purposeful sampling, other participants were recruited using snowball sampling. ASPPH and CPHS distributed invitations via email and included details on the study, a $25 gift card incentive, and a scheduling link. Interested individuals scheduled a session time and received 2 subsequent reminder emails and an information sheet from CPHS before their session.
Listening sessions occurred from January through March 2025. We used a semistructured guide to facilitate discussion intended to gather exploratory perspectives on potential DIS pathways. Participants discussed perceptions of their institution’s resources for undergraduate students and feasibility of implementing CDI pathways. Listening sessions were neither recorded nor transcribed at the request of our funder. Informed consent was verbally provided by all parties involved in listening sessions. Therefore, to increase rigor, at least 2 project team members took notes during each session and conducted postsession debriefs to compare notes. Two members of the research team (C.K., G.L.) collated and analyzed all notes using inductive and deductive coding. 26 Inductive coding consisted of descriptive coding and thematic analysis.27,28 We organized results into themes. We completed all analyses using NVivo version 14 (Lumivero). After all listening sessions were completed, participants received a $25 gift card as a thank you for completing a listening session.
Results
Quantitative Findings
Our analytic sample included 2577 participants from the 2021 and 2024 PH WINS who identified as DISs. Among DISs, a weighted estimate of 74.5% and 81.6% reported having a bachelor’s degree or higher in 2021 and 2024, respectively. Approximately half (53.2%) of the combined sample reported having at least 1 certification; the most commonly reported certificates were clinical certifications (23.7%) and “other” certifications (16.7%) (Table 1). Fewer than 1% of DISs (0.7%) reported having a DIS-specific certification (ie, training resulting in a certification in disease intervention or similar). Among DISs with any certification, 39.5% also had a bachelor’s degree or higher, which was substantially more than participants without at least 1 certification (37.4%).
Certifications among disease intervention professionals in the 2021 and 2024 Public Health Workforce Interests and Needs Survey (N = 2577) a

Abbreviations: CDC, Centers for Disease Control and Prevention; DI, disease intervention; PrEP, preexposure prophylaxis; STD, sexually transmitted disease; STI, sexually transmitted infection.
Listening Session Findings
We conducted 11 voluntary listening sessions with representatives from 11 undergraduate institutions (15 participants total) (Table 2). We organized results into 6 themes across 2 overarching domains: (1) barriers and facilitators and (2) feasibility of establishing CDI pathways.
Characteristics of undergraduate public health institutions represented among participants (n = 11) in listening sessions describing undergraduate pathways to disease intervention careers, United States, 2025
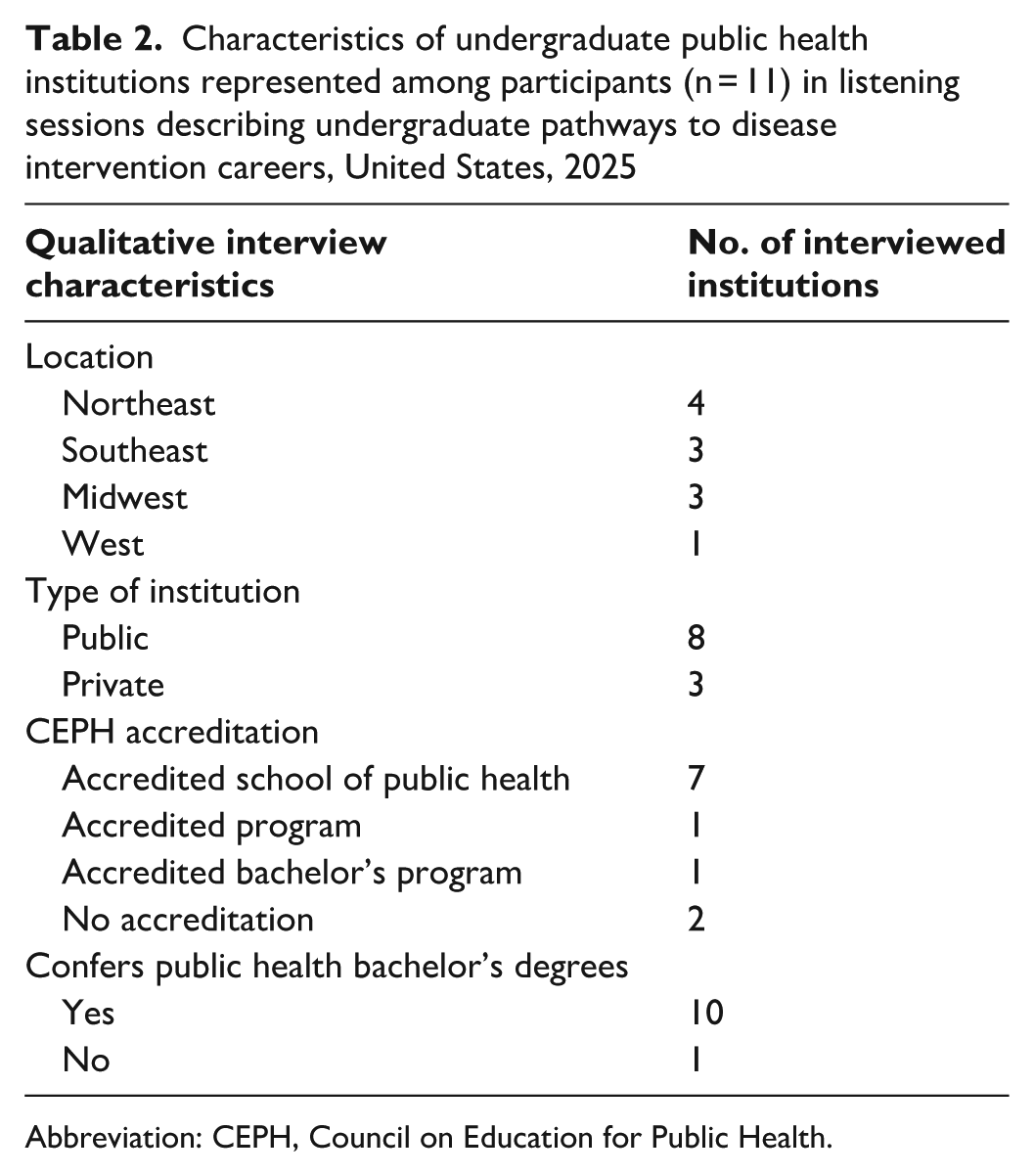
Abbreviation: CEPH, Council on Education for Public Health.
The first domain, barriers and facilitators, included 2 themes. The first theme focused on alignment between CDI domains and institutions’ course offerings. Participants discussed how curricula aligned with CDI domains; participants from institutions with greater overlap expressed more optimism about implementing undergraduate DIS pathways than those with less overlap. However, most participants hesitated to confirm alignment because NBPHE and national partners had not yet finalized detailed definitions of domains and experiential learning requirements. The CDI domain Collaboration was consistently reported as covered, often integrated across multiple courses. Coverage of the CDI domain Field Services and Outreach varied. Reported coverage of the CDI domains Interviewing and Case Management Activities, Outbreak Response, and Emergency Management ranged from partial coverage to unknown or no coverage. Participants rarely mentioned curricula incorporating the CDI domain Planning and Case Analysis. The CDI domain Surveillance and Data Collection was most often found in epidemiology-focused programs. All participants reported experiential learning within programs. Requirements varied widely, from a 50-hour volunteer practicum to a 140-hour internship in placement sites including health departments, nonprofit organizations, hospitals, and state agencies. Barriers to these DI-related work experiences included difficulty securing host sites, limited paid opportunities, and privacy and safety concerns. Nine participants noted general overlap with existing curricula, particularly in epidemiology courses.
The second theme in the Barriers and Facilitators domain addressed student and faculty interest. Some participants anticipated strong student interest in DIS pathways, while others expected little student interest. Participants reported faculty engagement as critical for success. At some institutions, participants indicated that faculty could be amenable to providing examination preparation and supplemental coursework, whereas other participants anticipated minimal involvement.
The second domain, Feasibility of Establishing CDI Pathways, included 2 themes. The first theme, institutional capacity, focused on partnerships and funding. Participants described challenges forming partnerships with external organizations, particularly in geographically isolated areas or where institutions lacked capacity to manage internships, even when agencies wished to collaborate. Participants mentioned past alumni donations and grants as potential funding sources. One participant reported having no funding streams that could support a DIS pathway. Participants reported that institutional capacity paralleled alignment with existing curricula, as discussed in the first domain.
The second theme in the Feasibility domain addressed recruitment considerations. Participants suggested targeting students interested in health fields and promoting CDI credentials as complementing existing degrees. They described students learning about public health through peers or after changing their degree paths. Participants described recruitment strategies that included outreach to students in nursing, premedicine, exercise science, and health education programs and building connections with communities served by DISs. Some participants proposed recruiting from high schools through expanded programming and dual-credit opportunities. Despite enthusiasm for recruitment, participants acknowledged challenges such as limited institutional involvement due to structural constraints, lack of funding, degree timing–related constraints for DI training, and concerns about promoting pathways that lacked financial support and known career trajectories.
Discussion
This study’s findings provide a preliminary understanding of the educational background of DISs and the readiness of undergraduate institutions to support educational pathways aligned with the forthcoming CDI credential. PH WINS data indicate that most DISs have a bachelor’s degree or higher, suggesting that undergraduate education may serve as a viable foundation for building standardized DIS career pathways. Few DISs reported currently holding DIS-specific training, which likely reflects the limited pre–CDI examination availability of such trainings (Kirkland C, Dill J, Stabler H, Lazalde G, McDaniel N. Building Disease Investigation Specialist Certification Pathways Within Undergraduate Institutions: Report 1. University of Minnesota Center for Public Health Systems; 2025. Unpublished). Similarly, a low proportion of DISs reported having certifications that align with DIS competencies, signaling an opportunity for the CDI credential to fill an important gap in professional recognition and skill validation. Listening session findings complement this finding, highlighting both enthusiasm and uncertainty among undergraduate program representatives about the implementation of CDI pathways, given current resource constraints, curricular structures, and limited institutional awareness.
The PH WINS analysis suggests a workforce with education preparation but limited formal accreditation in DI-relevant skills. Approximately three-quarters of DISs had a bachelor’s degree or higher, while fewer than 5% had certifications that overlapped with CDI domains. This finding reinforces the idea that the DIS workforce has a strong educational base but lacks consistent professional infrastructure to support skill validation and potential career path development. As CDI certification is introduced, these data provide a baseline against which to assess the uptake and impacts of credentialing. In addition, the finding that many DISs hold other certifications, including some related to health education or community health work, suggests potential overlap and opportunities for cross-training or credit recognition to potentially streamline pathways into CDI certification.
Listening session participants expressed broad conceptual support for undergraduate pathways into DIS careers while emphasizing challenges that could limit the success of pathways. Participants frequently shared curricular alignment as facilitators. Many institutions noted that existing public health courses cover CDI domain–relevant topics such as field services, outbreak response, and case investigation but highlighted gaps, particularly those related to experiential learning requirements. Institutions described limited capacity to offer internships or field placements that meet the CDI experience threshold, reflecting broader constraints in workforce training partnerships between academia and public health agencies. We noted faculty and student interest as key considerations, finding that while some participants believed that DIS pathways would appeal to students seeking applied public health careers, others noted limited awareness of the DIS field.
We identified several structural barriers to pathway implementation. Participants acknowledged funding limitations, administrative hurdles to adding new programs, and uncertainty about employer demand for certification as potential barriers. Importantly, many participants noted that while undergraduate institutions could help prepare students for the CDI examination, the sustainability of these pathways would depend on the stability of DIS positions in governmental public health and employer recognition of the CDI credential. Findings underscore the need for stronger coordination among academia, public health agencies, and national partners to ensure that new educational investments meet workforce needs and opportunities.
Limitations
This study had several limitations. First, listening session participants represented a small and potentially nonrepresentative sample of US undergraduate institutions that may not reflect the full diversity of institutional capacities or student interests. Second, the qualitative data also reflect a single point in time, prior to the launch of the CDI credential. Perspectives may evolve as institutions gain familiarity with certification requirements. Third, although the PH WINS analysis offered valuable national data, limitations are inherent in survey research, including potential nonresponse bias. Fourth, the classification of DISs likely overrepresents individuals hired as contact tracers during the COVID-19 pandemic in 2021 when demand was highest for these roles and may underrepresent workers performing DIS functions under other titles. Finally, our method for identifying DIS-related certifications relied on textual responses and may have introduced further misclassification, because many participants who reported “other” certifications were neither standardized nor elaborated upon in text responses.
Conclusions
This study provides timely insight into the educational and institutional foundations needed to support the emerging DIS certification. Findings suggest that undergraduate public health programs may have some curricula aligned with CDI domains. However, addressing gaps in experiential learning requirements, faculty awareness, and funding may require targeted support and partnerships. This evidence can guide ASPPH, CDC, NBPHE, and practice-based partners including health departments and professional organizations in developing technical assistance resources, institutional toolkits, and communication strategies to help universities explore CDI-aligned curricula. Moreover, findings from PH WINS data can be used to establish a baseline for monitoring trends in educational attainment and certification among DISs, enabling the evaluation of the CDI program’s long-term effects on workforce development and professionalization.
Future research should explore the interplay among DIS educational preparation, certification, and employment outcomes. Studies linking certification status with job satisfaction, retention, and career advancement could clarify whether CDI pathways enhance workforce stability and quality. In addition, mixed-methods research involving students and employers could provide valuable perspectives on demand and the perceived value of CDI credentialing.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261459006 – Supplemental material for Multimethod Analysis of Potential Disease Intervention Career Pathways at US Undergraduate Institutions
Supplemental material, sj-docx-1-phr-10.1177_00333549261459006 for Multimethod Analysis of Potential Disease Intervention Career Pathways at US Undergraduate Institutions by Gabriela Lazalde, Chelsey Kirkland, Hank Stabler, Nicole McDaniel and Janette Dill in Public Health Reports®
Footnotes
Acknowledgements
The authors acknowledge the assistance of those who contributed to improving the content of this article, including Heather Krasna, PhD (Columbia University Mailman School of Public Health), and the ASPPH team of Beth Handler, MPH, Melissa Meadows, MPH, Sara McDowell, MPH, and Emily Burke, EdD.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the Certified in Disease Intervention (CDI) program was provided through CK20-2003 Improving Clinical and Public Health Outcomes Through National Partnerships to Prevent and Control Emerging and Re-Emerging Infectious Disease Threats from the Centers for Disease Control and Prevention (CDC) of the US Department of Health and Human Services (HHS) as part of financial assistance award NU50CK000612 funded by CDC/HHS. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS, the US government, or the Association of Schools and Programs of Public Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.