
Abstract
Objectives:
Korean American adults have a high rate of gastric cancer in the United States. Although Helicobacter pylori, a major cause of noncardia gastric cancer, is commonly acquired early in life in regions with a high incidence of disease, data on infection history are limited. We assessed current and lifetime H pylori infection and examined gastric cancer prevention practices among Korean American adults.
Methods:
We conducted 14 community outreach events in Connecticut, New Jersey, and New York from June through October 2025. Participants completed a structured survey and underwent 13C urea breath testing. We defined lifetime H pylori infection as prior clinician diagnosis and/or current test positivity. We recorded history, indication, and location of upper endoscopy.
Results:
Of 315 participants, 282 had valid test results. Participants reported prior clinician-diagnosed H pylori infection in 35.1% (n = 99) of cases, and 87.9% (n = 87) of these individuals reported treatment. We identified current infection in 18.4% (n = 52) of participants, including 8.0% (n = 7) of previously treated participants. Overall lifetime infection prevalence was 50.0% (n = 141) and remained similar across categories of duration of US residence. Among participants who reported endoscopy data, 78.4% (n = 225) had undergone esophagogastroduodenoscopy, most commonly for routine screening in the United States.
Conclusions:
Community-based outreach events identified a high prevalence of lifetime H pylori exposure among Korean-born adults, indicating persistent gastric cancer risk acquired before migration. However, high preventive endoscopy use indicates strong community engagement with prevention. Public health efforts can identify individuals at risk of gastric cancer and link them to eradication and surveillance to reduce gastric cancer disparities.
Introduction
Although the United States is generally considered a low-incidence country for gastric cancer, aggregate national statistics obscure substantial heterogeneity in risk.1,2 When data on gastric cancer incidence are disaggregated, noncardia gastric cancer disproportionately affects racial and ethnic minority and immigrant populations, reflecting longstanding disparities in exposure, prevention, and access to care. 2 In parallel, the incidence of gastric cancer has been rising among US adults aged <50 years, further underscoring the need to reexamine prevention strategies for populations historically overlooked by clinic-based approaches. 3
In the United States, gastric cancer prevention is largely opportunistic and clinic-centered, relying on symptom-driven evaluation or incidental testing rather than systematic identification of individuals with elevated lifetime risk. Recent national analyses demonstrate substantial racial, ethnic, and geographic disparities in gastric adenocarcinoma stage at diagnosis and survival in the United States, with disproportionately poorer outcomes among Hispanic and non-Hispanic Black populations than among non-Hispanic White populations. 4 Among adults aged ≥50 years, the incidence of noncardia gastric cancer has been reported to be 1.8- to 7.3-fold higher among racial and ethnic minority populations than among non-Hispanic White populations and up to 14.5-fold higher among Korean Americans than among non-Hispanic White people. 5
These disparities likely reflect the combined influence of early-life Helicobacter pylori exposure, which the World Health Organization classifies as a group 1 carcinogen and the primary cause of noncardia gastric cancer, as well as barriers to prevention associated with migration and access to care. 6 Many immigrants from East Asia and other regions with a high incidence of gastric cancer (hereinafter, high-incidence regions) acquire H pylori infection in childhood, carrying forward a persistent biological vulnerability despite relocation to countries with a low incidence of gastric cancer (hereinafter, low-incidence regions).6,7 Strain-level variation in H pylori (eg, differences in virulence factors such as cytotoxin-associated gene A) has been described across geographic regions and may influence carcinogenic potential; however, population-level risk remains elevated among individuals originating from high-incidence regions. 8 After migration, this risk is often compounded by limited access to primary care, language discordance, health insurance gaps, and the absence of organized screening programs. 9 In countries such as South Korea, national gastric cancer screening programs are government supported, widely used, and culturally normative, contributing to earlier detection and reduced mortality.6,7 Consequently, many Korean immigrants arrive in the United States with established expectations of cancer prevention and surveillance, yet they encounter a fragmented and opportunistic prevention landscape after arrival.
Effective gastric cancer prevention requires more than detection of current infection alone; it also requires identifying individuals with lifetime H pylori exposure, ensuring access to eradication therapy, and facilitating appropriate risk-based surveillance. Community-based outreach is a promising strategy to address structural barriers by delivering services in trusted, nonclinical settings, particularly for immigrant populations who are underserved by traditional health systems. However, data describing H pylori prevalence and preventive care practices in community-based programs are limited, especially among immigrant populations with a high risk of gastric cancer in the United States (hereinafter, high-risk immigrant populations).10,11
To address this gap, we conducted a multistate community-based study among Korean-born adults in the United States to characterize lifetime and current H pylori infection and to describe preventive endoscopy practices within a community outreach framework. By integrating structured survey data with objective diagnostic testing, this study aims to guide migration-informed strategies for equitable gastric cancer prevention among high-risk immigrant populations.
Methods
Study Design and Setting
We conducted a cross-sectional, community-based study from June through October 2025 across Korean American communities in Connecticut, New Jersey, and New York, regions that include some of the largest Korean immigrant populations on the East Coast. The study team organized 14 outreach events in partnership with faith-based and community organizations, including churches, cultural centers, and nonprofit groups, which served as trusted access points for gastric cancer prevention services. Events were held in accessible community settings and promoted through local networks and Korean-language communication channels to facilitate participation among individuals who may have limited engagement with clinic-based health care services.
Participants
Eligible participants were Korean-born adults aged ≥20 years who were residing in the United States. Participation was voluntary, and individuals were enrolled consecutively at each outreach event. For the purposes of this study, we defined an offer of participation as an individual being physically present at an outreach event during the screening period and having a real, immediate opportunity to participate. Individuals who were exposed to pre-event announcements but were not present during screening periods were not considered to have been offered participation.
Across outreach events, the study team offered participation to approximately 450 adults present during the screening periods, 350 of whom elected to participate, corresponding to a participation rate of 78%. Of these, 315 met eligibility criteria and were included in the study. The study team conducted outreach events across multiple geographic locations and community and faith-based settings selected to reflect socioeconomic diversity in Korean American communities.
A total of 315 eligible participants aged 25 to 85 years participated in study activities. Of these, 287 (91.1%) completed the structured survey and the 13 C urea breath test (UBT). Five UBT results were invalid or missing, yielding a final analytic sample of 282 participants for analyses involving current infection status (Figure).
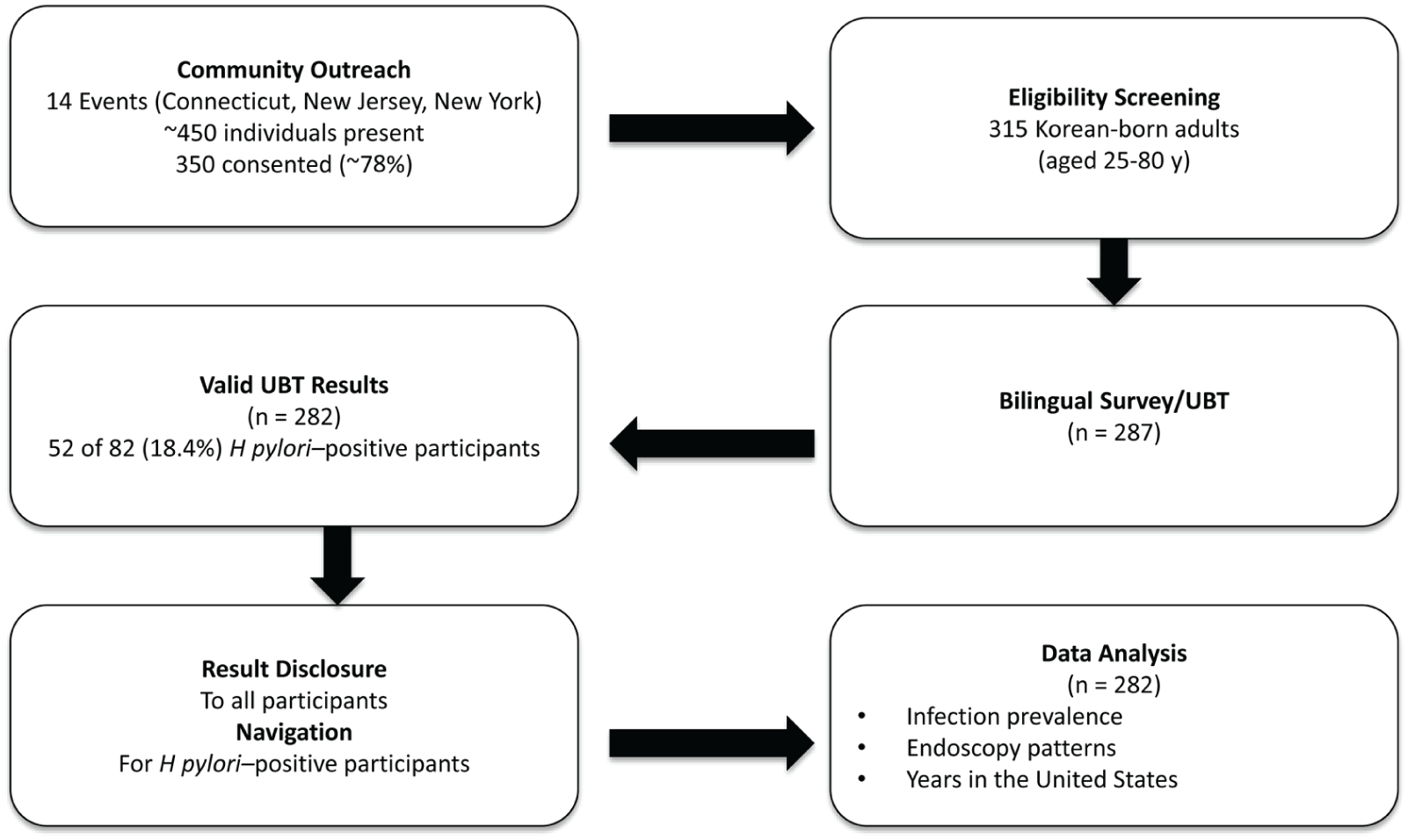
Flow of participants in a community-based gastric cancer prevention outreach and Helicobacter pylori screening program among Korean American participants in Connecticut, New Jersey, and New York, June through October 2025 (n = 287). Participant flow from community outreach events was through screening, eligibility assessment, testing, and analytic cohort inclusion. Approximately 450 adults attended outreach events focused on gastric cancer prevention education, risk assessment, and H pylori screening, of whom 350 consented to participate. After eligibility assessment, 315 participants met inclusion criteria. A total of 287 participants completed survey and urea breath testing (UBT), and 282 had interpretable H pylori test results and were included in the analytic cohort. Of these, 52 participants (18.4%) received a positive test result for current H pylori infection and were provided result disclosure and navigation for follow-up care.
Data Collection and Survey Measures
Participants completed a structured survey administered by trained bilingual staff and available in Korean and English (Supplement). Survey domains included sociodemographic characteristics (age, sex, education, health insurance status, and duration of US residence) and clinical history relevant to gastric cancer prevention. Participants reported prior H pylori infection, diagnostic modality (biopsy, stool antigen testing, or UBT), and history of eradication therapy. We assessed gastrointestinal symptoms, including dyspepsia-related symptoms, to contextualize testing and endoscopy utilization.
We evaluated preventive care practices through an assessment of endoscopic history, including prior esophagogastroduodenoscopy (EGD), timing of procedures, primary indication (routine screening, symptom evaluation, or surveillance), and country in which procedures were performed (United States or abroad). We categorized duration of residence in the United States into quartiles (≤15, 16-25, 26-35, and >35 y) to examine migration-related risk patterns. The full survey instrument is provided in the Supplement.
Urea Breath Testing
We assessed current H pylori infection by using UBT. Trained personnel administered tests on-site according to manufacturer instructions. Participants were advised that the recent use of proton pump inhibitors, antibiotics, or bismuth-containing agents could affect test performance; adherence to medication restrictions was self-reported. A Clinical Laboratory Improvement Amendments (CLIA)–certified reference laboratory analyzed breath samples and classified test results as positive, negative, or invalid. For study analyses, we further categorized UBT results as interpretable or noninterpretable. Interpretable results included valid positive or negative test results, whereas noninterpretable results included missing or indeterminate tests. We included only participants with interpretable results in analyses of current H pylori infection.
We selected the UBT to facilitate on-site sample collection and maximize participation, because stool antigen testing requires at-home sample collection and return, which may reduce completion rates in community-based settings. UBT also provides high sensitivity and specificity for detecting active H pylori infection and is widely used in clinical practice.
Definitions of Infection Status
We defined current H pylori infection as a positive 13 C UBT result. We defined prior infection as self-reported clinician-diagnosed H pylori infection by any modality (biopsy, stool antigen testing, or UBT). We defined lifetime infection as evidence of either prior infection or current UBT positivity, and we counted infection once for participants who met both criteria. We recorded treatment history for all participants who reported prior infection to contextualize current infection status.
Endoscopic Practice Measures
We assessed endoscopic practices by self-report. Participants indicated whether they had ever undergone EGD, the number of procedures received, the primary indication for each procedure (routine screening, symptom evaluation, or surveillance), and the country in which each procedure was performed. We also recorded the timing of endoscopy relative to migration to the United States to characterize access to preventive care before and after immigration.
Statistical Analysis
We used descriptive statistics to summarize participant characteristics, H pylori infection prevalence, and endoscopic practice patterns. Continuous variables are presented as means with SDs and categorical variables as counts and percentages.
We examined the current and lifetime prevalence of H pylori infection across quartiles of duration of US residence. We calculated age-adjusted estimates of current infection by using direct standardization to the age distribution of the analytic sample to enable comparisons across quartiles of duration of US residence.
We performed multivariable logistic regression analyses to evaluate independent associations of duration of US residence (categorized), age (categorized), and sex with current H pylori infection. We calculated 95% CIs for regression estimates, and we considered 2-sided P < .05 to be statistically significant. We conducted all analyses by using Stata version 17 (StataCorp LLC) and R version 4.3.2 (R Foundation for Statistical Computing).
The study protocol was reviewed and approved by the Yale University Institutional Review Board (IRB no. 2000039782). We obtained written informed consent from all participants prior to their inclusion in the study, and we conducted all study procedures in accordance with institutional ethical standards.
Results
Lifetime and Current H pylori Infection
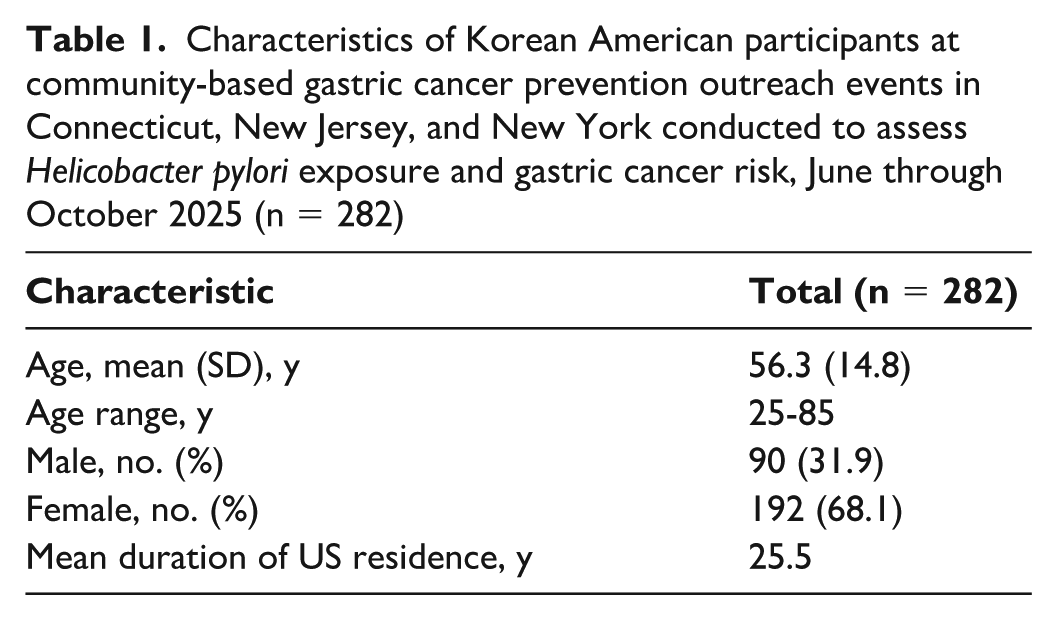
The final analytic cohort comprised 282 participants with valid UBT results. The mean (SD) age was 56.3 (14.8) years (range, 25-85 y), 68.1% (n = 192) were female, and the mean duration of US residence was 25.5 years (Table 1). Of 282 participants, 99 (35.1%) reported a prior clinician-diagnosed H pylori infection (Table 2). Diagnosis was most commonly established by endoscopy with biopsy (73 of 99; 73.7%), and most diagnoses occurred after migration to the United States (91 of 99; 91.9%). Among those reporting prior infection, 87 (87.9%) indicated having received eradication therapy, 2 (2.0%) reported no treatment, and 10 (10.1%) were unsure of their treatment history.
Characteristics of Korean American participants at community-based gastric cancer prevention outreach events in Connecticut, New Jersey, and New York conducted to assess Helicobacter pylori exposure and gastric cancer risk, June through October 2025 (n = 282)
Prevalence of Helicobacter pylori infection among Korean American participants attending community-based gastric cancer prevention outreach events in Connecticut, New Jersey, and New York, by sex, June through October 2025 (n = 282)
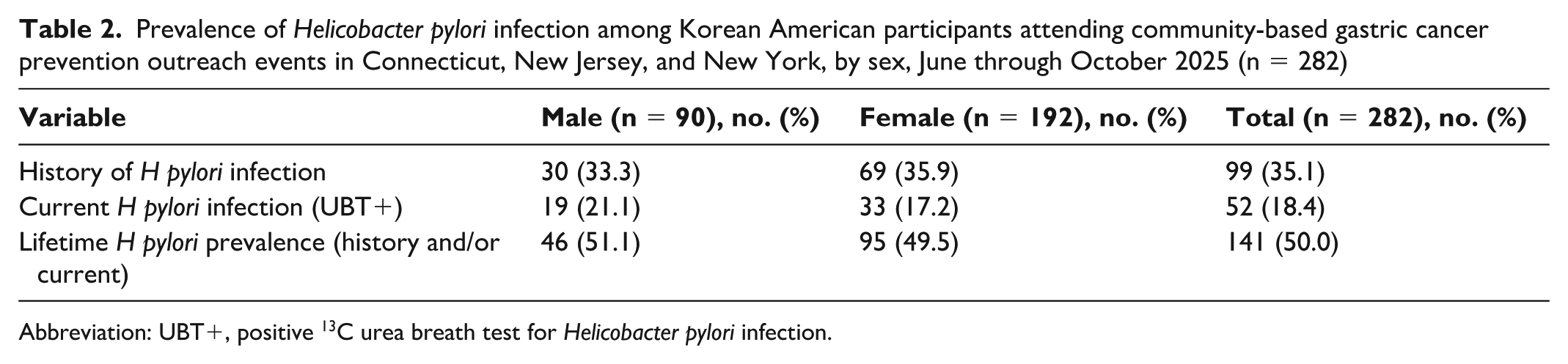
Abbreviation: UBT+, positive 13 C urea breath test for Helicobacter pylori infection.
Of the 282 participants with interpretable H pylori test results, we identified current infection—assessed by positive UBT—among 52 participants (18.4%) (Table 2). We observed UBT positivity in 7 of 87 previously treated participants, 1 of 2 untreated participants, and 2 of 10 participants who were unsure of their treatment history.
We found lifetime H pylori infection in 141 participants (50.0%) after accounting for overlap between prior infection and current UBT positivity (n = 10) (Table 2). Lifetime prevalence was similar among men (46 of 90; 51.1%) and women (95 of 192; 49.5%). We observed current UBT positivity in 19 of 90 men (21.1%) and 33 of 192 women (17.2%).
Current H pylori Infection by Duration of US Residence
Current H pylori infection varied by duration of residence in the United States. Crude UBT positivity was 27.6%, 17.6%, 13.6%, and 16.2% among those with ≤15, 16 to 25, 26 to 35, and >35 years of US residence, respectively (Table 3). After age adjustment using direct standardization, the estimated prevalence of current infection declined with increasing duration of US residence (30.8%, 17.7%, 12.5%, and 12.3%, respectively). Age-adjusted prevalence was highest among participants residing in the United States for ≤15 years and lower among those with a longer duration of US residence, with overlapping 95% CIs across categories. In contrast, self-reported prior and lifetime H pylori infection varied across categories of duration of residence in the United States without a clear pattern.
Prevalence of Helicobacter pylori infection, by duration of US rsidence, among Korean American participants attending community-based gastric cancer prevention outreach events in Connecticut, New Jersey, and New York, June through October 2025 (n = 282) a
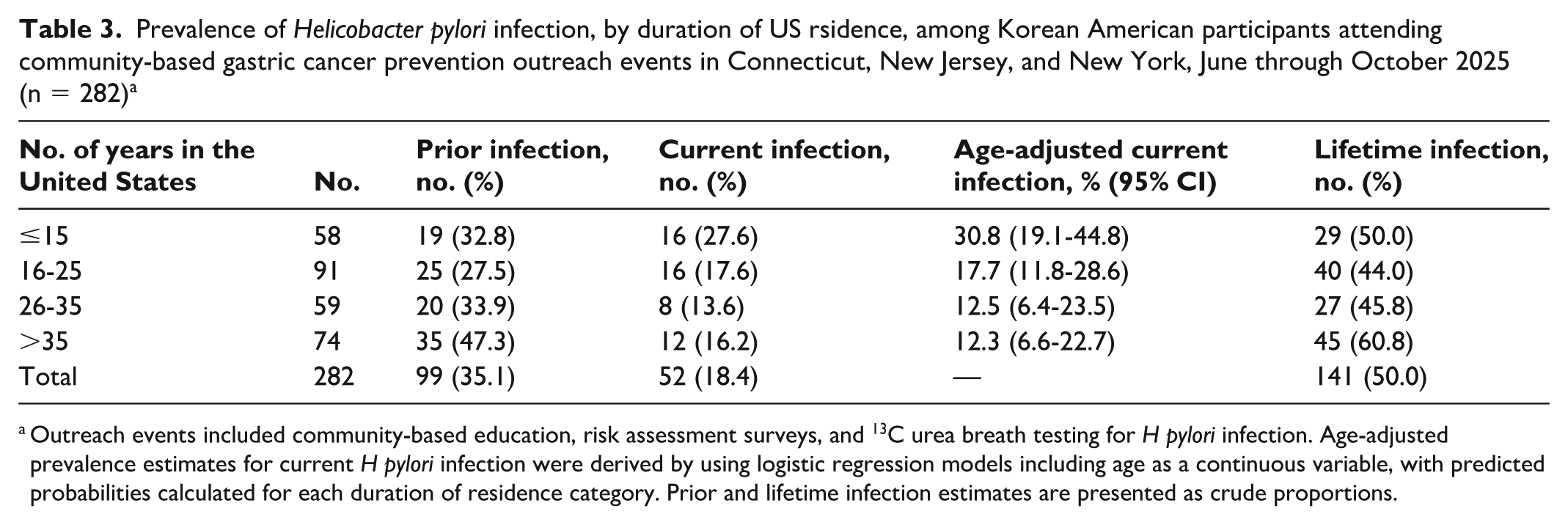
Outreach events included community-based education, risk assessment surveys, and 13 C urea breath testing for H pylori infection. Age-adjusted prevalence estimates for current H pylori infection were derived by using logistic regression models including age as a continuous variable, with predicted probabilities calculated for each duration of residence category. Prior and lifetime infection estimates are presented as crude proportions.
In multivariable analysis adjusting for age and sex, the pattern of higher current H pylori infection among participants with a shorter duration of US residence remained similar; however, associations were not statistically significant, and 95% CIs overlapped across categories.
Preventive Endoscopy Practices
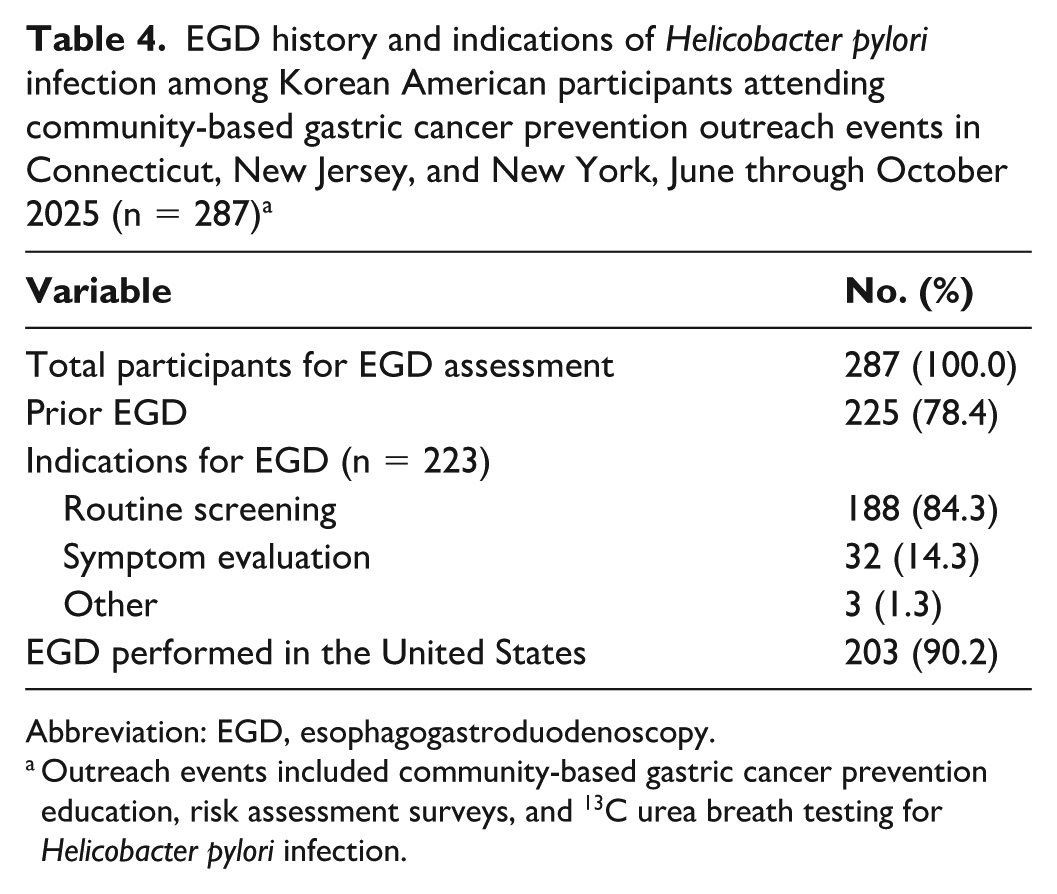
Of 287 participants with available endoscopy data, including 5 participants without valid UBT results, 225 participants (78.4%) reported having undergone at least 1 EGD (Table 4). Two participants lacked data on indication; of the remaining 223 participants, routine preventive screening was the most commonly reported indication (188 of 223; 84.3%), followed by evaluation of upper gastrointestinal symptoms (32 of 223; 14.3%). Three participants (1.3%) reported other indications, such as follow-up of prior gastric findings. Most reported EGDs were performed in the United States (203 of 225; 90.2%), with the remainder occurring in Korea or other countries.
EGD history and indications of Helicobacter pylori infection among Korean American participants attending community-based gastric cancer prevention outreach events in Connecticut, New Jersey, and New York, June through October 2025 (n = 287) a
Abbreviation: EGD, esophagogastroduodenoscopy.
Outreach events included community-based gastric cancer prevention education, risk assessment surveys, and 13 C urea breath testing for Helicobacter pylori infection.
Discussion
Community-Based Insights Into Gastric Cancer Prevention
In this community-based study of Korean-born adults living in the United States, we observed a high prevalence of lifetime H pylori exposure and widespread participation in preventive endoscopy. Together, these findings highlight 2 interrelated components of gastric cancer prevention in high-risk immigrant populations: persistent biological risk acquired early in life and sustained engagement with preventive health behaviors after migration. Nearly half of participants demonstrated evidence of lifetime H pylori infection, consistent with early-life exposure in high-incidence settings, while more than three-quarters reported having undergone upper endoscopy, most often for routine screening rather than symptom evaluation. This coexistence of risk and preventive engagement underscores the importance of strategies that integrate infection control with accessible, culturally concordant care.1-5
Population-based studies in Korea have reported H pylori seroprevalence rates of approximately 50% to 60% in adults, with higher rates observed in older cohorts and declining prevalence in more recent generations.12,13 Although these estimates are based on serologic testing rather than active infection (eg, UBT), they provide a useful approximation of cumulative exposure in the country of origin. In comparison, the prevalence of current infection in our cohort, assessed using UBT, was substantially lower—particularly among individuals with longer duration of US residence—suggesting that infection patterns reflect both early-life exposure in the country of origin and subsequent environmental and health care–related factors after migration.
By examining both lifetime H pylori prevalence and engagement with preventive care in a community-based setting, this study identified gaps in gastric cancer prevention that may not be recognized when studies focus on only current infection or clinic-based health care use.
Early-Life Exposure and Gaps in Primary Prevention
The relatively low prevalence of current H pylori infection observed in this cohort likely reflects substantial testing and treatment after migration, suggesting meaningful engagement with the US health care system. However, the high prevalence of lifetime exposure indicates that most infections were acquired well before diagnosis and eradication. Although H pylori infection is typically acquired in early childhood, our study did not directly assess the timing of acquisition. This interpretation is based on established epidemiologic patterns rather than direct measurement in this cohort. Because prolonged untreated infection drives progressive gastric mucosal injury and the development of premalignant conditions such as atrophic gastritis and intestinal metaplasia, delayed diagnosis and treatment may reduce the potential benefit of eradication for primary prevention.6,7 These findings highlight a critical gap in current US prevention approaches: the absence of systematic early testing for immigrants arriving from high-incidence regions, when eradication may yield the greatest long-term benefit.
Patterns by duration of US residence further support this interpretation. Age-adjusted prevalence of current infection was highest among participants with shorter durations of US residence and declined with longer durations of US residence, whereas lifetime infection prevalence was stable. This pattern suggests that access to testing and eradication increases over time after migration, reinforcing the importance of early migration-aware prevention strategies that do not rely solely on opportunistic clinical encounters.
Taken together, these findings suggest limitations of predominantly clinic-centered prevention strategies for gastric cancer in low-incidence settings. Reliance on symptom-driven testing or episodic care may delay identification of H pylori exposure until years or decades after initial infection, when opportunities for primary prevention may already be reduced.
Preventive Endoscopy as a Community-Embedded Practice
The high prevalence of endoscopic screening in this cohort reflects strong preventive engagement rather than atypical health care use. Population-based studies have shown that Korean Americans are more likely than other Asian populations to undergo upper endoscopy before gastric cancer diagnosis and that prior endoscopy is associated with earlier stage at diagnosis and improved survival. 14 Health care provider–patient ethnic concordance further increases the likelihood of prior endoscopy. Our findings extend this literature by demonstrating high participation in a community-based context, likely facilitated by dense social networks, culturally embedded screening norms, and access to linguistically concordant gastroenterologists in the Connecticut, New Jersey, and New York region.
In this setting, endoscopy appears to function as a culturally embedded preventive practice that parallels Korea’s national gastric cancer screening program. 15 These observations illustrate how migration may transmit not only disease risk but also durable prevention behaviors when supported by appropriate community infrastructure. From a public health perspective, community-based platforms may help reinforce preventive behaviors that are already culturally valued in populations at high risk of gastric cancer.
Implications for Population-Level Prevention
Together, these findings support a migration-informed approach to gastric cancer prevention that integrates H pylori testing, timely eradication, and risk-based endoscopic surveillance in community-aligned care pathways. Current US prevention strategies are largely reactive and clinic centered, limiting their reach among immigrant populations with elevated lifetime risk of gastric cancer.
These considerations should be balanced with epidemiologic observations suggesting inverse associations between H pylori and certain conditions, including esophageal adenocarcinoma and selected immune-mediated diseases.16,17 However, the overall clinical and public health rationale for eradication in high-risk populations remains supported by the substantial global impact of gastric cancer and the established causal role of H pylori.
Community-based screening platforms may help address this gap by shifting prevention earlier in the life course, decoupling risk identification from clinic-based entry points, and aligning intervention timing with underlying biologic risk rather than symptom onset. Programs that combine H pylori testing with culturally concordant education, navigation to eradication therapy, and linkage to risk-appropriate endoscopic surveillance may reach populations with limited engagement in preventive gastric cancer care through clinic-based approaches alone.15,18
Community-based screening should be viewed as an entry point into the health care system, with individuals who test positive referred to primary care for confirmatory testing and treatment, consistent with current US practice.
Asymptomatic H pylori positivity alone does not constitute an indication for endoscopy under current US guidelines. Rather, management is based on noninvasive testing and clinical context, with endoscopy reserved for individuals with additional risk factors.
Although this study focused on Korean-born adults, the findings are likely relevant to other immigrant populations from high-incidence regions who carry early-life H pylori exposure and face similar structural barriers to prevention. As the US immigrant population grows, community-aligned strategies that address early-life infection risk may play an increasingly important role in reducing persistent disparities in gastric cancer outcomes.
Limitations
This study had several limitations. First, participants were recruited through voluntary community outreach and may not be representative of all Korean-born adults or Korean Americans in the United States. Individuals who participate in community health programs may be more health engaged than the general population. However, outreach was conducted across multiple geographic locations and diverse community settings selected to capture socioeconomic heterogeneity, and the study was designed to characterize the delivery of prevention rather than to estimate population-level prevalence.
Second, women were overrepresented among participants, a pattern commonly observed in community-based preventive health programs. Cultural norms, caregiving responsibilities, and work-related constraints may have limited participation among men. 19 We observed similar sex-based participation patterns in our prior Korean American hepatitis B screening program, which involved more than 7000 participants. 20 Analyses were stratified by sex or adjusted for sex, as appropriate.
Third, prior H pylori infection and treatment history were self-reported and subject to recall bias, and medication use that could affect UBT could not be independently verified. Although UBT is highly sensitive and specific, false-positive results may occur because of other urease-producing organisms. Fourth, small sample sizes within some duration of US residence categories limited precision in age-adjusted estimates. Fifth, the cross-sectional design precluded assessment of temporal relationships or long-term clinical outcomes. In addition, findings from Korean American communities in a single US region may not be fully generalizable to other immigrant populations or geographic contexts.
Conclusion
Effective prevention of gastric cancer in immigrant populations requires strategies that address early-life H pylori exposure, migration history, and barriers to preventive care. In this community-based cohort, a high prevalence of lifetime infection coexisted with strong participation in preventive endoscopy, highlighting both missed opportunities for earlier primary prevention and opportunities to strengthen risk-based secondary prevention.
These findings support ethnicity- and migration-informed prevention approaches that extend beyond clinic-centered care. Community outreach programs that integrate H pylori testing, timely eradication, and linkage to appropriate endoscopic surveillance in trusted settings may represent a practical and scalable strategy to identify lifetime gastric cancer risk and reduce persistent disparities in the United States.
Supplemental Material
sj-docx-1-phr-10.1177_00333549261460001 – Supplemental material for Community-Based Helicobacter pylori Screening to Identify Gastric Cancer Risk Among Korean-Born Adults in the United States
Supplemental material, sj-docx-1-phr-10.1177_00333549261460001 for Community-Based Helicobacter pylori Screening to Identify Gastric Cancer Risk Among Korean-Born Adults in the United States by Chul S. Hyun, Sung Hwi Hong, Xuehong Zhang, Jae Il Shin, Sara Soonsik Kim and Loren Laine in Public Health Reports®
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korean American Community Foundation. The funding organization had no role in the study design; data collection, analysis, or interpretation; manuscript preparation; or the decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Deidentified programmatic data supporting the findings of this study are not publicly available due to privacy considerations.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.