
Abstract
The purpose of this study was to examine the structure of active social networks of individuals with visual impairments, the social support they receive from their social networks, and their satisfaction from received support. In addition, we examined these factors as predictors of happiness in people with visual impairments. A total of 96 individuals with visual impairments, who ranged in age from 16 to 50, participated in this study. Three self-constructed questionnaires, which included questions related to demographic data, social networks, social support, and happiness, were used in the study. Participants reported being satisfied with received support, and they also appeared to receive more positive than negative support. Findings also demonstrated the merit of social support for the happiness of individuals with visual impairments.
In general, social support, which has been defined in many different ways, refers to the type of assistance/help that individuals receive or expect to receive from those who come into contact with them in any way (Papakonstantinou & Papadopoulos, 2010). Orth-Gomér and Undén (1987) define social networks and social contacts as the structural aspects of social support, and available support as the functional aspect of social support. O’Reilly (1988) suggests that social network is an analytic concept that portrays the linkages between individuals or groups of individuals, whereas social support is one of the network’s functions, which is offered through behaviors and actions of the members of the network and communicated through the network’s structure. The present study accepts that a social network has two main aspects, the structural aspect—the network, and the functional one—social support, including the satisfaction with social support. The social network, as the structural aspect of the social network, can be further divided in various subsystems such as close family environment, kin, close friends, and so forth. The main attribute of these subsystems is their size. As far as the functional aspect of social network is concerned, social support is divided into positive practical support, positive emotional support, negative practical support, and negative emotional support.
The conceptual framework of the present study focuses on the cumulative expression of support. Antonucci (2001) describes the support/efficacy model in which the cumulative expression is a key element. When one or more individuals express their feelings or thoughts of a person being an able, worthy, capable person, and this person perceives this kind of support as being accurate and altruistically motivated, then the person might adopt these same feelings/thoughts. Over time, the person obtains accumulated beliefs of his or her own abilities that will be a great support in facing the challenges of life. In this study, we seek to examine the structure of active social networks of individuals with visual impairments, the social support they receive from their social networks, and their satisfaction from received support. Moreover, the study aims to investigate the relationships among demographic covariates, social support, satisfaction derived from that support, social networks, and their impact on participants’ happiness. In the next three sections, we provide a brief review of the research literature related to social networks, social support, and the relationship between social networks/social support and well-being.
Social Networks
The social networks of people with visual impairments can be divided into formal networks, which consist of professionals and teachers, and informal networks, which consist of parents, siblings, kin, and friends (Cause & Srebnik, 1990; Schwarzer & Buchwald, 2004). The average number of important persons contained in the network of an individual with a visual impairment is 15 individuals—mostly friends and family members—whereas the same number for sighted individuals is 20 individuals (Kef, 1997, 2002, 2005). Another measure of the size of the network, besides important/significant persons, is the range of the active network, which is the measure used in the present study. The active network refers to those persons with whom one feels he or she has a personal relationship and tries consciously to keep contact with, or persons with whom one has had contact within the last 2 years (Roberts, Dunbar, Pollet, & Kuppens, 2009). Previous studies have proven that the average size of the active network of sighted individuals ranges from 100 to 300 persons (Roberts et al., 2009).
Independent factors related to impairment, such as social stigma, play a significant role in the ability of individuals with visual impairments to create and retain new relationships (Sacks & Wolffe, 1998). For example, adolescents with visual impairments seem to have smaller networks in comparison to sighted adolescents (Kef, 2002, 2005). It is generally believed that adolescents with visual impairments have fewer opportunities for acceptance by their sighted peers (Wolffe & Sacks, 1997), higher level of social isolation (Sacks & Wolffe, 1998), and more difficulty retaining friendships in comparison to their sighted peers (Sacks & Wolffe, 1998). It is also more difficult for adolescents with visual impairments to maintain friendships with their sighted peers than with their friends with visual impairments (Wolffe & Sacks, 1997).
Demographic/personal characteristics such as gender, severity of visual impairment, employment status, independent mobility, and ability of self-management are also factors that influence the range of individuals’ social networks. Independent mobility has been defined as the ability to travel safely, comfortably, gracefully, and independently through the environment (Foulke, 1971). Self-management is defined by Lorig and Holman (2003) as taking an active role in decisions that affect an individual’s health and demonstrating responsibility for the day-to-day management of his or her life.
The size of a network of an individual has been found to be affected by gender. Sighted men seem to prefer a large number of network members in comparison to women, who seem to prefer smaller groups and more intimate relationships (Schwarzer & Buchwald, 2004). Gender is an influential factor in the size of the networks of individuals with visual impairments. Female adolescents appear to have more friends than their male peers and tend to have larger networks (Kef, 1997; Kef, Hox, & Habekothé, 2000).
In addition, the severity of visual impairment appears to play no significant role in the range of visually impaired adolescents’ network (Kef, 1997). Employment status has also been found to be a significant factor, as employed individuals with visual impairments appear to have larger networks than unemployed individuals (Roy, Dimigen, & Taylor, 1998). Moreover, independence in mobility and living situation influences the size of visually impaired adolescents’ network (Kef et al., 2000).
Social Support
Social support is an umbrella term that includes received support and perceived support (Brough & Pears, 2004; Kef, 1997). Perceived support is the belief that social support will be available when needed (Lindorff, 2005; Sarason, Sarason, Shearin, & Pierce, 1987), while received support is the support an individual actually receives or has reported receiving in a specific situation or during a specific period from specific persons (Kef, 1997).
Received and perceived support further subdivide into emotional and practical support (Brough & Pears, 2004; Kef, 1997). In the present study, practical support is defined as informational support (providing alternative perspectives, coping strategies, and information about community resources), as well as the provision of services and materials (Chang & Schaller, 2000) and tangible resources, such as physical aids and transportation (Birch, 1998). Emotional support is defined as affective support (Kahn & Antonucci, 1980) and includes expressions of concern (Brough & Pears, 2004; Chang & Schaller, 2000) or feelings of being accepted, respected, included, and having one’s emotions acknowledged (Chang & Schaller, 2000).
Demographic/personal characteristics such as gender, severity of visual impairment, employment status, self-management skills, and independent mobility are factors that influence the amount of social support an individual receives. Little is known about the relationship between social support and the above-mentioned demographic/personal characteristics of individuals with visual impairments, especially in a wide range of ages. According to Weiner (1991), no correlations between severity of visual impairment of young adults and social support are found. In addition, age is found to influence the kind of social support received (Kef, 1997). For example, practical support for adolescents with visual impairments tends to decrease as their age increases.
Gender also appears to be an influential factor for the amount of social support. Female adolescents with visual impairments seem to have less perceived support from their friends than their sighted female peers. In contrast, no differences were found between visually impaired male adolescents and sighted male adolescents (Huurre, Komulainen, & Aro, 1999).
Employment status has also been found to be a significant factor in social support, as employed individuals with visual impairments appear to have more supportive networks than do unemployed individuals (Roy et al., 1998). In addition, a low level of independence in adults with visual impairment seems to lead to overprotective behaviors from network members as a form of negative social support (Cimarolli, 2006), whereas independence in mobility of adolescents with visual impairment influences the amount of social support (Kef et al., 2000).
Social Network, Social Support, and Well-Being
In line with Ryff and Keyes (1995), in this study, the term well-being is used to refer to the breadth of wellness that includes self-acceptance, personal growth, purpose in life, positive relations with others, environmental mastery, and autonomy. Social support can improve overall physical and psychological well-being (Guerette & Smedema, 2011). Social support can help individuals promote and maintain healthy behavior (Birch, 1998) and enhance psychological well-being (Cimarolli & Wang, 2006; Gencöz & Özlale, 2004; Guerette & Smedema, 2011; Kef, 2002; Reinhardt, 2001a), self-esteem (Guerette & Smedema, 2011; Huurre et al., 1999; Kef, 2002; Sarason, Levine, Basham, & Sarason, 1983), and a sense of control (Cohen & Wills, 1985), whereas it acts as a buffer against the effects of stress (Buunk & Peeters, 1994; Sarason et al., 1983).
Social support also is indirectly related to depression symptomatology. Low levels of social support have been found to be associated with higher levels of depressive symptoms (Guerette & Smedema, 2011). Conversely, individuals who feel that there are persons available to help or that they are already being cared for report less depressive symptomatology, partly due to reduced life stress (Gencöz & Özlale, 2004). Both practical and emotional support has been shown to be important for maintaining health and well-being among older individuals (Thompson & Heller, 1990).
Happiness is defined as a short-term affective well-being (Ryff, 1989). It has been reported that sighted adults who receive a high level of social support have higher self-esteem and are more optimistic about their lives than sighted adults with a low level of social support (Sarason et al., 1983). There is also a positive association between social support and happiness in visually impaired adolescents (Kef, 2002). Social support contributes to the positive adaptation to stressful conditions, such as a chronic physical impairment, by making them feel psychologically more able to cope with these events (Reinhardt, 2001a; Schwarzer & Buchwald, 2004). Received emotional support for elderly individuals with visual impairments is associated with greater life satisfaction and less depressive symptoms. In addition, the receipt of practical support for the elderly and the provision of social support by the elderly can lead to greater life satisfaction (Reinhardt, 2001b). The availability of a stable and trustworthy relationship is of great importance (Mellor & Edelmann, 1988). Women with progressive disabilities seem to be happier than men maybe due to the satisfaction from the support they receive from their networks (Chen & Crewe, 2009).
Apart from the above-mentioned positive outcomes related to social support, some negative effects have also been identified by researchers. Negative social support may take the form of help that is offered inappropriately (Sarason et al., 1987), unwillingly, or unnecessarily. Apart from the obvious negative forms of behavior such as criticism, anger, and hostility (Ruehlman & Karoly, 1991), negative social support may also manifest as insensitivity, overprotection (Chang & Schaller, 2000; Cimarolli & Boerner, 2005), and underestimating, or overrating of the person’s capabilities. Negative social support has been shown to have a negative impact on the well-being of individuals with visual impairments. It can have a harmful impact on mental health (Hirsch & Rapkin, 1986; Reinhardt, 2001a). Cimarolli (2002) reports that negative social support has a negative impact on adjustment to age-related vision loss. Perceived overprotection, specifically, seems to be associated with more difficulties in the process of adjustment for older individuals with visual impairments (Cimarolli, Reinhardt, & Horowitz, 2006). Cimarolli and Boerner (2005) have shown that receiving no support or only negative support is inversely related to well-being.
Predictors of life satisfaction include demographic variables such as employment status (Chen & Crewe, 2009). Unemployed people with impairments are more vulnerable to depression (Turner & Turner, 2004). Individuals’ personal characteristics, such as independence in mobility and gender also play an important role in their well-being according to research related to adolescents with visual impairments (Kef et al., 2000). The more independent individuals are, the higher the well-being they will achieve. Also, female adolescents with visual impairments are more likely to be less happy than male adolescents with visual impairments, and satisfaction with social support is positively associated with well-being (Kef et al., 2000).
Purpose of the Study
The aims of the present study are (a) to examine the structure of active social networks of individuals with visual impairments; (b) to investigate the social support they receive from their social networks and their satisfaction from the received support; (c) to examine the impact of participants’ personal characteristics (age, gender, severity of visual impairment, age at onset, ability of independent mobility, ability of self-management, number of close friends, and employment status) and range of active social networks in social support and satisfaction from the support; (d) to examine the impact of participants’ personal characteristics, range of active social networks, and satisfaction from the support in happiness; and (e) to examine the impact of participants’ personal characteristics in the range of social network.
Method
Participants
The sample consisted of 96 individuals with visual impairments (63 males and 33 females), who ranged in age from 16 to 50 (M = 27.4, SD = 9.89). Of the 96 participants, 74 were adults and 22 participants were under the age of 18. A total of 40 participants were residents of Athens (capital of Greece with a population of about 5 million), 44 participants were residents of Thessaloniki (the second largest city of Greece, with a population of around 800,000 citizens), and 12 participants were residents of Ioannina, which is a provincial city with a population of around 100,000 people.
In all, 47 participants (49%) were either individuals who were blind or had severe visual impairments (visual acuity < 20/400), and 49 (51%) were individuals with low vision (20/200 > visual acuity > 20/400). A total of 45 participants (47%) were congenitally visually impaired, and 51 (53%) were adventitiously visually impaired.
In terms of education, 24 participants were university graduates, 17 were current university students, 23 were high school graduates, 27 were high school students, 4 had completed junior high school, and 1 was an elementary school graduate.
In total, 40 participants reported that they could “always” move independently (without needing any support from a guide), 32 reported moving independently “most of the time,” 14 “sometimes,” and 10 “a few times.” A total of 27 participants were employed, and the remaining 69 stated that they were unemployed, retired, or students.
Instruments
Social network, social support, and satisfaction
In the present study, we used a modified version of the social network, social support, and satisfaction from support questionnaire for Greek adults with visual impairments developed by Papakonstantinou and Papadopoulos (2009). Papakonstantinou and Papadopoulos (2009) developed the items for their questionnaire based on the Social Support Questionnaire (SSQ; Sarason et al., 1983; Sarason et al., 1987), the Social Network Map, and Social Network Grid (Tracy & Whittaker, 1990). Instead of four support groups (colleagues with visual impairments, sighted colleagues, employers or supervisors with visual impairments, and sighted employers or supervisors), six support groups were included in the current version of the Papakonstantinou and Papadopoulos questionnaire to assess the total actual social network of individuals with visual impairments and the social support they receive from their social networks. These support groups include (a) close family environment (parents, brothers/sisters, and grandparents), (b) kin (extended family members), (c) friends, (d) fellow-students, (e) teachers, and (f) colleagues, members of unions, neighbors, and therapists.
The first part of the questionnaire assesses the range of the social network by asking the respondents to count the number of people from the six support groups that are considered part of their networks. Participants were instructed not to include a person twice in the network groups and to identify how many close friends or best friends they have in their support networks.
The second part of the questionnaire was designed to evaluate social support received from each of the six support groups. It is composed of 24 items and four subscales: (a) Positive Practical Support, (b) Positive Emotional Support, (c) Negative Practical Support, and (d) Negative Emotional Support. Each item is rated on an 11-point Likert-type rating scale ranging from 0 (none) to 10 (a great deal of support). Prior to asking participants to rate received support, the researcher read aloud two texts, explaining the meaning of positive and negative support, both practical and emotional, while also offering various examples based on findings from previous studies regarding the forms of positive and negative support received by individuals with visual impairments (Chang & Schaller, 2000; Cimarolli & Wang, 2006; Papakonstantinou & Papadopoulos, 2010).
The third section addressed the assessment of satisfaction from support. This part consisted of 12 items. Participants were asked to rate on a range of 0 (none) to 10 (a great deal) how satisfied they were with the social support they received from their social network groups.
The test–retest (2 weeks) reliability coefficients for the range of social networks (r = .97), positive practical support (r = .79), positive emotional support (r = .94), negative practical (r = .97), negative emotional (r = .93), satisfaction with the practical support (r = .74), and satisfaction with the emotional support (r = .89) were relatively high. Cronbach’s alpha coefficients for positive practical support, positive emotional support, negative practical, and negative emotional were computed to be .87, .90, .82, and .84, respectively.
Happiness
The measure of happiness used in this study is similar to the Cantril Scale (Cantril, 1965), which has been used by Kef (2002). It is a single-item scale. Participants responded to the question, “How happy do you feel?” on an 11-point Likert-type rating scale ranging from 0 (none) to 10 (a great deal).
Self-management
Self-management was assessed using a single item. Participants responded to the question “To what degree can you self-manage yourself?” on an 11-point Likert-type rating scale ranging from 0 (none) to 10 (a great deal).
Mobility
Independent mobility was assessed using a single item. Participants responded to the question, “How often do you move independently—without being helped by a human guide—in an outdoor space (either familiar or unfamiliar)?” on a 5-point Likert-type rating scale ranging from 0 (never) to 4 (always).
Procedure
In the present study, the ethical principles of the Declaration of Helsinki (World Medical Association, 2010) were followed. In addition, consent was obtained from the individuals, using the appropriate forms and according to the procedure suggested by the World Medical Association (2010). Students with visual impairments in this study were recruited from mainstream high schools located in Athens, Thessaloniki, and Ioannina. Only those students who accepted to participate and whose parents gave their consent participated in this study. The adults were recruited from the members of the Panhellenic Association of the Blind. We contacted by phone a random selection of 130 individuals with visual impairments in Athens, Thessaloniki, and Ioannina to invite them to participate in the study, and 74 individuals agreed to participate.
A researcher read the questions to the participant and then wrote down the answers. Each participant took part in the process separately in a quiet room, and no other person, except for the participant and a researcher, was in the room each time.
Statistical Analyses
Descriptive statistics were computed to provide a description of the demographic characteristics of the participants. Stepwise regression analysis was used to answer the research questions.
Results
Descriptive Statistics
The mean of the range of active social network total for the participants in this study was 59.08 (SD = 32.09). The mean for close family (Group 1) was 6.35 (SD = 3.69), 14.50 (SD = 11.66) for kin (Group 2), 15.09 (SD = 12.24) for friends (Group 3), 10.04 (SD = 10.71) for classmates/university colleagues (Group 4), 5.82 (SD = 4.69) for teachers (Group 5), and 17.24 (SD = 17.23) for colleagues, members of unions, neighbors, and therapists (Group 6). The mean of the range of active social network total was 59.08 (SD = 32.09).
The mean of the positive support in total (practical and emotional) was 7.29 (SD = 1.79), while the mean of the negative support was 2.71 (SD = 1.90). The results are presented in Table 1.
Social Support Received by Each Group.
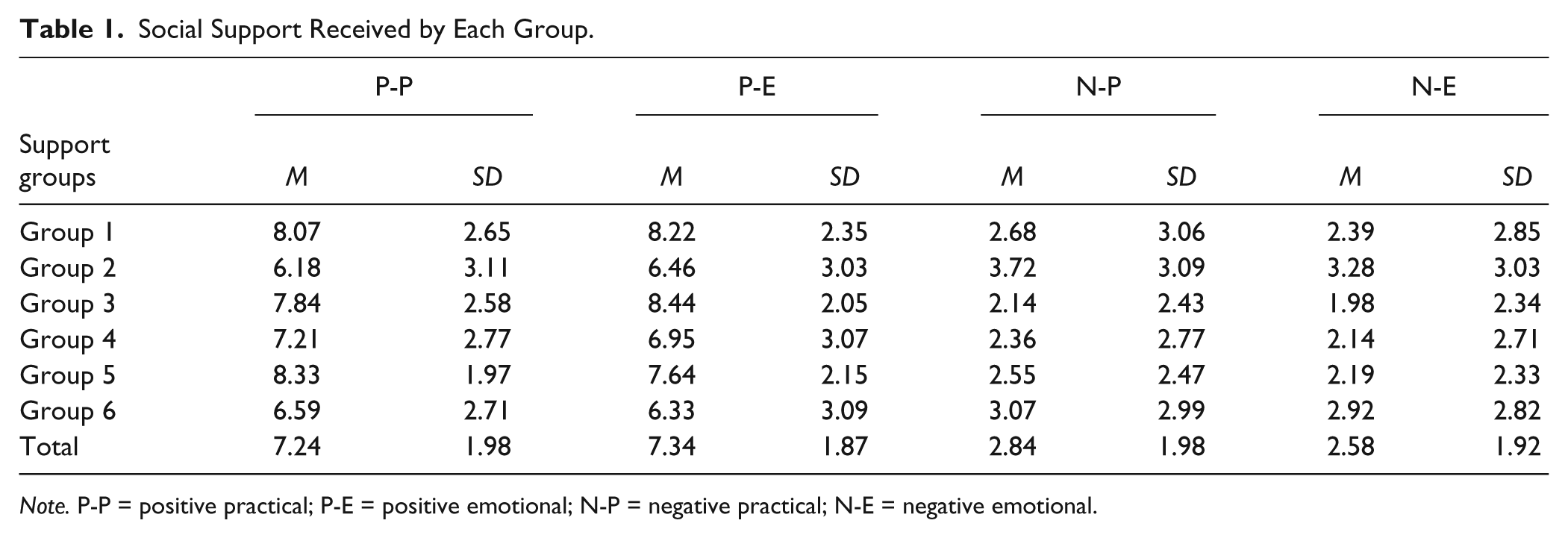
Note. P-P = positive practical; P-E = positive emotional; N-P = negative practical; N-E = negative emotional.
The mean of participants’ satisfaction with practical support was 7.56 (SD = 2.11) and emotional support was 7.31 (SD = 2.49). The mean of satisfaction total was 7.44 (SD = 2.00). The average score for the feeling of happiness was 8.04 (SD = 2.05).
Stepwise Regression Analysis
The analysis of positive practical support produced an adjusted R2 of .154 (F = 9.374, p < .01). Significant individual predictors of positive practical support were age (B = −.062, SE = 0.019, t = −3.278, β = −.315, p < .01) and ability of independent mobility (B = −.978, SE = 0.378, t = −2.588, β = −.249, p < .05). Regarding the positive emotional support, the analysis yielded an adjusted R2 of .051 (F = 5.954, p < .05). Significant individual predictor of positive emotional support was age (B = −.045, SE = 0.019, t = −2.440, β = −.248, p < .05).
Concerning the negative practical support, the analysis yielded an adjusted R2 of .034 (F = 4.274, p < .05). Significant individual predictor of negative practical support was “the number of close friends” (B = −.114, SE = 0.055, t = −2.067, β = −.212, p < .05). Regarding the negative emotional support, the analysis yielded an adjusted R2 of .046 (F = 5.422, p < .05). Significant individual predictor of negative emotional support was “the number of close friends” (B = −.122, SE = 0.052, t = −2.329, β = −.237, p < .05).
The analysis of the satisfaction from practical support was observed to have an adjusted R2 of .108 (F = 12.133, p < .01). Significant individual predictor of satisfaction from practical support was age (B = −.074, SE = 0.021, t = −3.483, β = −.343, p < .01). Regarding the satisfaction from emotional support, the analysis yielded an adjusted R2 of .071 (F = 8.055, p < .01). Significant individual predictor of satisfaction from emotional support was age (B = −.072, SE = 0.025, t = −2.838, β = −.285, p < .01).
The older participants indicated that they received less positive practical and emotional support and were less satisfied with practical and emotional support received compared with the younger participants. Moreover, the greater the independent mobility, the less positive practical social support the individual received. Furthermore, a greater number of close friends was associated with less negative practical and negative emotional social support.
Concerning happiness, the analysis yielded an adjusted R2 of .298 (F = 20.543, p < .01). Significant individual predictors of happiness were self-management (B = .365, SE = 0.111, t = 3.289, β = .287, p < .01) and satisfaction from practical support (B = .455, SE = 0.083, t = 5.476, β = .478, p < .01). Therefore, higher levels of self-management and satisfaction from practical support indicated a greater sense of happiness.
Regarding the range of social network, the analysis yielded an adjusted R2 of .143 (F = 16.517, p < .01). The significant individual predictor of the “range of social network” was employment (B = 27.528, SE = 6.733, t = 4.064, β = .390, t = 4.064, p < .01). The range of social networks of the employed participants was more extended than the networks of unemployed participants.
Discussion
The active network refers to those persons that one feels he or she has a personal relationship with and tries consciously to keep contact with, or persons with whom one has had contact within the last 2 years (Roberts et al., 2009). In this study, the average number of people in participants’ active social networks was 59 individuals. However, the size of networks varied greatly with the smallest network consisting of 8 persons and the largest of 170 persons. Previous studies have demonstrated that the average size of active networks of sighted individuals ranges from 100 to 300 persons (Roberts et al., 2009). Thus, there appears to be a noticeable difference in the size of the active networks of individuals with visual impairments and the active networks of sighted individuals. However, the way social networks, and in general people, evaluate each other plays a significant role on the size and the density of networks (Carter & Feld, 2004). For example, people who are perceived in a negative manner tend to have smaller networks than people who are positively evaluated, as they are actually discouraged from being sociable (Carter & Feld, 2004).
People with visual impairments are more likely to face social stigma than individuals without disabilities and as a result are considered to be at “the negative end of a continuum of social regard” (Carter & Feld, 2004). Generally, they are viewed as a vulnerable social group and, as a result, perceived in a negative framework (Carter & Feld, 2004). As a result, students with visual impairments have limited chances to be accepted by their sighted peers and to be socially integrated without barriers (Wolffe & Sacks, 1997). Thus, people with visual impairments are under great pressure to present themselves as individuals without impairments (Chen & Crewe, 2009).
In the present study, the factors that influence the range of social network were investigated. One of the strongest individual predictors of the range of a social network was “employment.” Employed participants tended to have more extended social networks than those of unemployed participants. This finding is consistent with previous research that employment status appears to play a significant role, as employed individuals with visual impairments were found to have larger and more supportive networks than the unemployed individuals with visual impairments (Roy et al., 1998).
A previous study (Kef, 2002) with participants with visual impairments came up with a reduced range of social networks than was found in the current study. We believe there were two primary factors for this difference. First, we recorded the active network of the participants with visual impairments, while Kef (2002) asked participants to mention the persons that are important to them. Moreover, in Kef’s study, none of the participants was employed as the study was focused on adolescents with visual impairments. In the present study, 27 participants were employed, and as a result, these participants’ social networks were more extended.
The range of social networks was not a significant predictor of the amount of social support, and happiness, reported by participants. For example, Group 6 was the largest participant group, and as a result, the total range of personal network was greater than that of the other groups. However, in many cases these individuals were less likely to provide support to the participants. On the other hand, the greater the number of close friends someone had, the less the negative practical and negative emotional social support experienced. As a result, it is the quality and not the quantity of relationships that influences perceptions of support. Kef (2002) arrived at the same conclusion and suggested that the functional aspects of networks (quality and content of relationships, including such aspects as social support, balance of support provided and support received, intimacy, and satisfaction with support) have critical influence on the adjustment and well-being of the adolescents with visual impairments. Flaherty, Gaviria, and Pathak (1983) suggested that there is not enough evidence in the literature to connect the amount of received support with the number of people that composes an individual’s supportive network. It is the quality of the relationships in a social network that appears to be the determining factor and not the size. Reinhardt (2001a) concluded that the amount of received support reflects, in part, the number of kin and non-kin members in an individual’s social network (Reinhardt, 2001a).
The results of the present study support the finding that individuals with visual impairments seemed to feel satisfied with their received support, especially practical support. Findings also revealed that participants received more positive than negative support. The positive and negative practical support was found to be more or less equal to positive and negative emotional support, respectively (see Table 1). A more in-depth analysis of the results implies that the participants received more positive social support (practical and emotional) from their family and friends but less from kin and persons of Group 6 (colleagues, members of unions, neighbors, and therapists). This finding is in contradiction to that of Reinhardt (2001a) but again may be an artifact of the inclusion of persons with visual impairments who are employed in the study. Similarly, individuals reported receiving the most negative support from their kin and the persons of Group 6, and the least negative support from their friends. These results are in line with the results of previous studies (Kef, 1997, 2002) and show how crucial the role of friends and family is for individuals with visual impairments. Adolescents with visual impairments appear to receive a lot of social support especially from their parents and peers (Kef et al., 2000).
The satisfaction derived from practical social support seems to increase the sense of happiness. Conversely, it could be hypothesized that happiness results in a better social adjustment, which, in turn, increases practical support. These are in line with previous research that indicated that there is a connection between social support and happiness, as there is a correlation between receiving support and feeling happy (Kef, 2002).
The analysis revealed that older persons received less positive social support and felt less satisfied with the support they receive compared with younger persons. According to Kef (2005), the satisfaction that persons with visual impairments feel from the received emotional and practical social support appears to be high both in their adolescence and in young adulthood. The majority of adolescents with visual impairments feel satisfied and, in some cases, very satisfied with the total social support from their social networks (Kef et al., 2000). Reinhardt (2001b) suggested that, in addition to family support, friendship relationships in later life and support stemmed from these relationships are significant enough and influence positively a person’s life. Taking the importance of social support in psychosocial adjustment into consideration, we expect that older people are the group at risk for developing psychosocial problems.
Implications for Practice
The findings of the present study suggest implications for the programs of inclusion and rehabilitation addressed to individuals with visual impairments. In particular, this study confirms the connection between social support and happiness for individuals with visual impairments, as the satisfaction derived from practical support seems to increase the sense of happiness. Thus, rehabilitation counselors and teachers should take into consideration the importance of social support in the psychosocial adjustment of persons with visual impairments.
In addition, the findings show the crucial role of family and friends for individuals with visual impairment in comparison with other support groups (kin, fellow-students, etc.). Rehabilitation counselors should focus their efforts to bring these two groups from the individuals with visual impairments entire social network into the rehabilitation process so that they can understand the process and their role in it (Rogers, Schmitt, & Scholl, 1997).
The findings of this study may also assist rehabilitation counselors in identifying the impact of negative social support on psychosocial adjustment of individuals with visual impairments. Cimarolli (2006) stated that addressing overprotective care can reduce the distress of young and middle-aged adults with visual impairments. Professionals must learn to balance care and flexible support, independence, and receiving support, to positively influence individuals with visual impairments, their families, and the other members of their networks in living, educational, working, and leisure contexts (Kef, 2002). Practitioners can improve outcomes in the rehabilitation efforts by understanding and mediating the risk of hurdles associated with emotional, psychological, and social challenges that result or are exacerbated because of negative or absent social support (Kef, 2002).
The results of this study support the conclusion that older people are the group at risk for developing psychosocial problems as they appear to receive less positive social support and feel less satisfied with the support they receive in comparison with younger persons. As a result, rehabilitation counselors should pay attention to the needs of older individuals with visual impairments. Counselors may need to inform older persons with visual impairments about services designed to increase social networks and try to integrate these activities into rehabilitation plans, to learn about community programs, and to assist older persons with visual impairments into accessing them (Rogers et al., 1997). Further, rehabilitation counselors should encourage individuals to discuss with their friends their specific support needs. This would be a particularly salient recommendation for those older individuals with visual impairments who lack family support.
This study also contributes to the development and design of vision-related rehabilitation services. Such services could include programs involving support groups for individuals with visual impairments that would address issues associated with increasing positive and decreasing of negative forms of social support. Further, such programs should also promote support groups for family members and friends and other individuals with visual impairments to help them with challenges and to benefit from their experiences (Rogers et al., 1997). These programs should aim at raising awareness about the forms of social support and the health impact of lack of support on individuals with visual impairments and at encouraging family members and friends to provide the positive support to individuals with visual impairments (Rogers et al., 1997).
Moreover, the findings of the present research might be helpful to rehabilitation educators. For instance, self-management appears to be a significant predictor of the sense of happiness. Thus, the improvement of daily living skills should be an integral part of the aims of any rehabilitation program for individuals with visual impairments. Evidence in the literature has also supported the relationship between social support and social skills (Guerette & Smedema, 2011). It seems that the training for social skills acquisition supports social interactions and the realization and maintenance of social relationships and friendships (Guerette & Smedema, 2011).
Limitations
A limitation of the present study is grouping teens with adults. There are differences in the way each group develops and maintains social networks, and these differences may have increased variability in social networks when viewed cross-sectionally. Another limitation of this study is that only convergent validity of the questionnaire was examined, while other kinds of construct validity, such as discriminant validity, should be examined as well. Another possible limitation of this study is the use of stepwise regression analysis. Hoyt, Leierer, and Millington (2006) indicated that “the main critique of stepwise methods is that they yield a so-called optimal predictor set that is very unlikely to generalize to future samples.” Moreover, they recommend that rehabilitation researchers avoid using these procedures.
Future Research
In future research, it would be useful to examine the forms of support, since there are only a few similar studies. The knowledge of forms of support can contribute to the design of specific programs aiming to the informing and sensitizing of the sighted individuals. Such a program will need to focus on encouraging positive forms of support and eliminating negative ones.
Also recommended is a future direction of research to focus on seeking additional factors that could contribute to the provision of additional positive social support to individuals with visual impairments by their networks and to the expansion of the range of these networks. In addition, future research should include employment of individuals with visual impairments as a moderator of relations between social networks at work, social support, and work satisfaction.
To further confirm the above-mentioned findings, this study could be applied to other types of impairments, in order to draw more global conclusions in terms of social support, networks, and well-being of people with impairments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.