
Abstract
The focus of this article is on women with mental health illness and themes pertaining to issues of gender in their mental health experiences and in their treatment by peers and family. Grounded theory methodology was utilized in the data analysis of semi-structured interviews with 20 women with mental health illness. Findings revealed several themes related to gender in the experiences of women with mental health illness. These themes include male leverage, gendered emotions, weight worries, caretaker demands, friendship barriers, higher expectations, and double standard of violence. Implications for rehabilitation counseling will be discussed.
Keywords
Women with serious mental health illnesses face adverse rates of victimization, poverty, homelessness, suicidality, and single parenthood (Jonikas et al., 2003; Mowbray et al., 2003). In addition, women’s subjective experiences of mental health illness appear to commonly differ from men (Ritsher et al., 1997). However, few studies have explored the views of women with mental health illness in their experience of gender (Scheyett & McCarthy, 2006). Rather, other research has focused on the voices of professionals or has taken a “gender-less” view of the experience of mental health illness (Scheyett & McCarthy, 2006). Moreover, much of the research on women with mental health illness is over 15 years old, focused on a specific diagnosis, or explores less severe mental illnesses, such as mild to moderate depression and anxiety disorders. These issues suggest the need for more research on the views of women with mental health illness, with a specific focus on their experiences with gender (Manuel et al., 2012; Ritsher et al., 1997; Scheyett & McCarthy, 2006; Schön, 2010). The present qualitative study was conducted with women with mental health illness to learn about their perceptions of their unique experiences as women with mental health issues, and in their treatment by others. In this article, we will present findings from a grounded theory study of 20 women with mental health illness and clarify the current needs of women with mental health illness in rehabilitation counseling.
Gender Issues in Mental Health Illness
A serious mental health illness refers to major mental health disorders that lead to impairment in functioning in one or more of the following areas: occupational, educational, social, and activities of daily living or self-care (National Institute of Mental Health [NIMH], 2019). Mental health illnesses typically include such diagnoses as schizophrenia spectrum disorders, severe depression, and bipolar disorder.
As described in a discussion of gender issues in mental health from the World Health Organization (WHO, 2019), “Gender determines the differential power and control men and women have over the socioeconomic determinants of their mental health and lives, their social position, status and treatment in society and their susceptibility and exposure to specific mental health risks” (p. 1). Women tend to report issues with stigma and isolation in their mental health experiences, associated with stressors in the expectations of womanhood, such as pregnancy, motherhood, caring responsibilities, and other gender expectations (National Women’s Council of Ireland, 2018). Poor mental health among women can be attributed to barriers to autonomy, reproductive rights, financial wellness, as well as physical, sexual, and psychological safety (Afifi, 2007).
Hence, gender differences have been found in the experience of mental health illness in the areas of prevalence, symptoms, course, onset, and treatment response to mental illness (Teh et al., 2008). National survey data from 2017 indicates that the occurrence of mental health illness is higher among women (5.7%) than men (3.3%) (NIMH, 2019). Symptoms and disorders may differ across men and women, with women having later onset of schizophrenia and bipolar disorder, and twice the rate of depression of men (Baldassano et al., 2005; Nolen-Hoeksema, 2014). Gender differences have also been found for frequency of psychotic symptoms, social adjustment, long-term outcomes, and disability associated with mental health illnesses (WHO, 2019). Sexual abuse and sexual objectification of women appears to contribute to some of the mental health illnesses of women, including depression, eating disorders, substance abuse, and sexual dysfunction of women with mental health illnesses (Carr et al., 2015; Moradi & Huang, 2008). Women with mental health illness face a number of unique challenges with regard to the motherhood identity in particular. They may opt out of, face derailed plans for, or reimagine different ways of embodying this role (Mizock et al., 2019).
Gender differences in treatment factors have also been found. Women appear to be more responsive to treatment in the case of schizophrenia and other psychotic disorders, with greater rates of recovery over the course of their lifetime (Grossman et al., 2008). The timing of remission also tends to be longer for women regardless of diagnosis (Schimmele et al., 2009). In addition, women typically express different treatment needs than men with mental health illness, particularly in the areas of trauma, sexual health, relationships, motherhood, and in forensic settings (Mowbray et al., 2003; Mulvey, 2013). Another study found that women with mental health illness in forensic settings appear to face added levels of social control in the probation and mental health systems within which they interface (Mulvey, 2013). They appear to be held to their criminal charges even when deemed incompetent.
There are gender differences in the experience of specific diagnoses of mental health illness as well. Women have higher rates of depression than men, likely due to higher rates of victimization, gender disparities in income and employment, and reactivity to stress (Nolen-Hoeksema, 2014). Women have a later onset of schizophrenia than men, less symptom severity, fewer negative symptoms, and more positive symptoms (Angermeyer et al., 1990; Vigod & Stewart, 2009). Women appear to have better functioning prior to development of schizophrenia than men, potentially due to women’s gender socialization (Childers & Harding, 1990). Furthermore, women have a later onset of bipolar disorder, with more seasonal and rapid cycling of their mood episodes, as well as problems with delayed detection and treatment (Arnold, 2003).
While some research suggests that women develop mental health illness later in life and have fewer relapses, they are still overrepresented in mental health services, possibly due to help-seeking differences (Schön, 2010). For instance, women are more likely to identify the need for mental health assistance and seek out these services when in need as a result of negative stereotypes of weakness attributed to men who reach out for assistance (Courtenay, 2000). Women are more compliant with care, which may contribute to their tendency to be hospitalized for longer periods (Mowbray et al., 1992). It has been proposed that increased rates of women with mental health illness may be largely due to the effects of women’s disadvantaged social status (Gove, 1980; WHO, 2019).
A handful of key studies to our knowledge to date have been conducted that explicitly explore issues of gender among men and women with mental health illness from their perspective. For example, in a related qualitative investigation to this study (Mizock & Brubaker, in press), a number of gender issues in treatment experiences of women with serious mental illnesses were identified that provided in-depth characterization of these phenomena. Themes included experiences with providers who raised questions as to the legitimacy of their symptoms and concerns in their mental health treatment, termed diminishing dismissals. Another theme was symptom misattribution, the erroneous ascriptions of their mental health symptoms. Mistrust of male providers was described, as well as psychiatric insults—perceptions that mental health providers tend to make stigmatizing diagnoses. The women also experienced doomsday predictions from their providers, negative prognoses of their future. A final theme was diagnostic reordering—the tendency of mental health providers to revise their prior diagnoses in ways that diminished stigma and built trust. This diagnostic process often included renaming borderline personality disorder—overdiagnosed among women (Walton et al., 2015)—as posttraumatic stress disorder—a diagnosis the women tended to find more validating of the role their trauma histories played in their current mental health challenges.
Ritsher and colleagues (1997) conducted a study on gender among men and women with mental health illness and utilized a questionnaire to compare their experiences of health care and relationships while managing a mental health illness. Analysis of the questionnaire data was primarily descriptive, and revealed that relationships were an area of strength for women in that they reported more and better quality of relationships than men. Both men and women commonly reported a history of abuse. However, women were more likely to report a history of sexual abuse. Women were more likely to report having a significant other and to have had at least one child. Moreover, women did not receive proper care for reproductive health or health screenings, though they were more likely to report generally good relationships with providers than male respondents.
In another relevant study, Schön (2010) focused on gender differences in the recovery process through 30 interviews with men and women with mental health illness. Schön interpreted recovery as a more embodied process for women in contrast to men. When doing poorly, self-harm and suicidality might occur. When recovery was stronger, women attended to aesthetics and strived to maintain a normal appearance. Recovery signified regaining possession of their whole identity, and sometimes advocating for their care, and defying social norms. Women found that when their partners helped with domestic labor and child care, this was instrumental to their recovery and sense of feeling loved. Women were also more likely to see spirituality as a key facilitator to recovery. In contrast, men in this study experienced their recovery as being less about the body. For men, recovery focused on gaining autonomy and control over the illness to prevent relapse through education and skill development. Men tended to work on their recovery through tools such as medication and new coping strategies, with little use of social support.
Scheyett and McCarthy (2006) conducted relevant study to compare the service needs of men and women with mental health illness through three mixed-gender focus groups. Both men and women shared an interest in recovery and hope, with an interest in providers who are respectful and collaborative. Although, women defined respect in terms of their caring and compassion, while men simply sought information, justice, and independence from their providers. Women differed from men in this study in being particularly concerned with the systemic issues in their treatment, including underfunding, understaffing, and problems with coordination of their care by providers. However, the authors felt that mixing the genders in the focus groups was a limitation and identified a need for future research with in-depth interviews with women with mental health illness.
Study Rationale
Women and men with mental health illness have different experiences of mental health, services, recovery, relationships, and risk factors. However, more research is needed to expand on the findings in the prior studies in this area to generate a broader picture of the unique gender experiences of women with mental health illness. The literature could be enhanced by a study in which women are asked directly about their experiences and perceptions about gender issues in their care and treatment in their key relationships with people in their social network, such as family and peers. Furthermore, discussion of the experiences and perceptions about gender issues is an in-depth manner, which is the rationale for the current study. Hence, the current grounded theory study was conducted with 20 women with mental health illness to update and expand up on the literature to comprehensively characterize the experiences with gender that women with mental health illness have perceived in their general experience, and in their treatment by their peers and family members.
Method
Participants
The sample of 20 women with mental health illness were recruited from a psychosocial rehabilitation center in the Northeast. This sample included 12 participants who identified as straight/heterosexual, four participants who identified as lesbian, two participants who identified as bisexual, one participant who identified as pansexual, and one participant who reported questioning her sexual orientation. The ages of participants ranged from 32 to 66, with an average age of 50 (SD = 10.15). The racial-ethnic makeup of the sample was predominantly White (n = 12), with five biracial participants, one African American participant, one Asian American participant, and one Native American participant. Participants self-reported their diagnoses, with eight participants having a single diagnosis and 12 participants reporting co-occurrence of two or more diagnoses. These diagnoses included major depressive disorder (n = 10), posttraumatic stress disorder (n = 8), anxiety (n = 7), bipolar disorder (n = 5), borderline personality disorder (n = 4), schizophrenia (n = 3), schizoaffective disorder (n = 2), and high functioning autism (n = 1). The sample identified their current marital status as the following: single (n = 11), divorced (n = 4), and married (n = 1). The marital status of four participants was unknown.
Procedure
University institutional review board approval was obtained for the study, and participants signed informed consent forms prior to participation. Participants received a US$25 gift card for participating in the study. Using purposive sampling, participants were recruited to participate in semi-structured interviews (see the appendix) from mental wellness groups at a psychosocial rehabilitation center in the Northeast. This center provides mental health services to individuals with mental health illness from the local community and was chosen as a location for recruitment due to the availability of women with mental health illnesses—of focus in the present study. These services consisted of psychoeducation-based groups in mental wellness and physical health (e.g., wellness recovery groups, art therapy, mindfulness meditation training). Recruitment occurred via flyers posted in the center and announcements made in groups. The selection criteria for choosing participants included the following: (a) female-identified; (b) 18 years or older; (c) self-reported diagnosis of severe depression, bipolar disorder, or schizophrenia spectrum disorder; (d) impairment in social, occupational/educational, and/or activities of daily living (self-care).
The interviews lasted approximately 60 min and took place either by phone or in a private research space within the center from which participants were recruited. Data collection occurred over the course of 2 months. Each interview was audio recorded and transcribed verbatim. Excerpts presented in this article were edited in some cases to remove extraneous words, nonlexical utterances, and other areas of speech to enhance readability while retaining original meaning. Recruitment continued until saturation of themes occurred, representing the theoretical sampling method involving theoretical saturation (Mason, 2010). This sampling method was selected based on the standards of grounded theory methodology (Glaser & Strauss, 1967). Glaser and Strauss (1967) described theoretical saturation as being achieved when “no additional data are being found whereby the [researcher] can develop properties of the category” (p. 61).
The first author created a semi-structured interview guide for the purposes of this study. This interview guide was developed to address gaps in the literature on women with mental health illness. The guide underwent review by several researchers in the area of mental health who served as a content expert panel in the revising of the interview guide. Questions addressed several topics related to the experience of women with mental health illness, including gender differences they have observed in their treatment by the public, family, peers, partners, and in the workplace as a woman with a mental health problem. Although these multiple topics were included in the interview guide, the present article isolated analysis to the topic area of their observed differences in mental health experiences, as well as in their views about gender issues in their treatment as women in comparison with men in peer and family relationships.
Data Analysis
Methodology
The grounded theory methodological approach was used for data analysis, as developed by Barney Glaser and Anselm Strauss in the 1960s (Corbin & Strauss, 2008; Miles & Huberman, 1994). Grounded theory is a research tradition for developing theory from raw, qualitative interview data from the ground up, rather than the traditional approach of being guided from the top down by applying a theory to the data (Corbin & Strauss, 2008). Grounded theory was used to develop theory from the data depending on the extent to which the data fit the conceptual categories identified by the research team (Suddaby, 2006). In this approach, the interview transcripts are marked with codes that are later grouped into categories (Corbin & Strauss, 2008). These categories can then be used to develop themes and theories from the data.
In addition, we used Charmaz’s (2011) constructivist approach to grounded theory (CGT). In CGT, it is understood that the data analysis process may be affected by the researchers’ pre-existing knowledge of the literature in any area. Hence, the grounded nature of the analysis does not result from the removal of the researcher’s view from the data analysis but requires an attempt to stay rooted in the data in the development of theory. Per Charmaz’s approach, the theory of the gendered treatment of women with mental health illness was depicted visually in a figure described later in this article that displays the relationships between properties of the themes generated from the data analysis.
This study also shared aspects of consensual qualitative research (CQR), a methodology that is informed by the grounded theory approach (Hill et al., 2005). Components of CQR that were a part of the present study included open-ended semi-structured qualitative interviewing, multiple judges throughout the data analysis process, and the use of consensus among the research team in the data analysis process.
Stages
In the present study, two research team members conducted data analysis, including a clinical psychologist and doctoral student in clinical psychology. In the first stage of data analysis, each of the 20 interviews was coded by the research team (both authors), using a line-by-line, open-coding process. During this stage, a representative sample of five interviews were coded first and separately by the research team members, then compared. This allowed the establishment of the initial codebook, or list of codes. The remaining interviews were then coded separately by the coders using the codebook, and compared in intervals of four to five interviews at each meeting until coding was completed.
Coding was an inductive and reductive process with data organized through the identification of common themes and categories, and comparison of similarities and differences in the participants’ narratives (Walker & Myrick, 2006). The coders held weekly meetings to compare and reach consensus on codes applied to each interview transcript, established by equitable discussion from each team member (Hill et al., 2005). The consensus process was repeated throughout the entirety of the data analysis process.
A comprehensive list was created of over 100 codes created from the 20 interview transcripts. Once this codebook was established, the codes were applied to the transcripts using NVivo qualitative analysis software (Corbin & Strauss, 2008). Codes were further aggregated using axial coding to relate codes together under overarching themes.
Next, selective coding took place to further refine the conceptual categories and themes, such as the theme of gender of focus in this article. This stage of data analysis involves identifying a code for selective analysis (gender differences in this study) and returning to the quotes from the data that have been assigned this code. NVivo coding software was used to pull up the list of the quotes that were assigned the code of gender differences. Then, the research team re-read the excerpts within this code, referring back to the interview transcripts from which they were identified to better understand their context and meaning (Heydarian, 2016). This process informed the creation of new themes to capture the complex nuances of concepts within one data code. After developing the themes, the research team created definitions of these themes that captured the concepts involved. Then the transcript excerpts were re-read again within that theme to select two to three representative quotes that were rich in meaning and encapsulated different angles of that theme to represent its scope (e.g., friendship barriers created by stigma vs. concrete transportation challenges to social events). Consensus was used between the researchers at this stage to develop the final themes, definitions, and representative quotes pertaining to the experience of gender.
Data Quality
Data quality was maintained through several qualitative validity strategies. Memos of research meeting notes and themes were recorded and redistributed to the research team during the 2 months of data analysis. Memos (Barbour, 2001) included initial interpretations of the data and representative interview excerpts. Reflexive journaling was also conducted—a diary kept to examine researcher biases and positionality over the course of the research project to minimize and explore these effects on data analysis and interpretation (Lincoln & Guba, 1985). Other validity strategies included the use of a multimember research team in the coding process to enhance data quality (Barbour, 2001). This allowed for cross-checking (Polkinghorne, 2007) of one another’s coding as part of enhancing interrater reliability. Finally, consensus was used to discuss interpretation of themes when occasional disagreements arose regarding coding and data analysis, involving attempts to uphold equitable discussion from each research team member before arriving at a final code (Edwards et al., 2004).
With regard to reflexivity, researcher biases were primarily related to our identities and roles as providers and researchers in the field of clinical psychology who advocate for people with mental health illnesses. Without serving in the role of consumers, the interview questions, interview process, and data analysis are shaped by a power role as researcher-providers, rather than as identified women with the lived experience of a serious mental health illness. Thus, we discussed and examined these biases at each and every stage of the research process to enhance our faithfulness to interpreting the themes and subthemes as they fit the responses of the participants.
Results
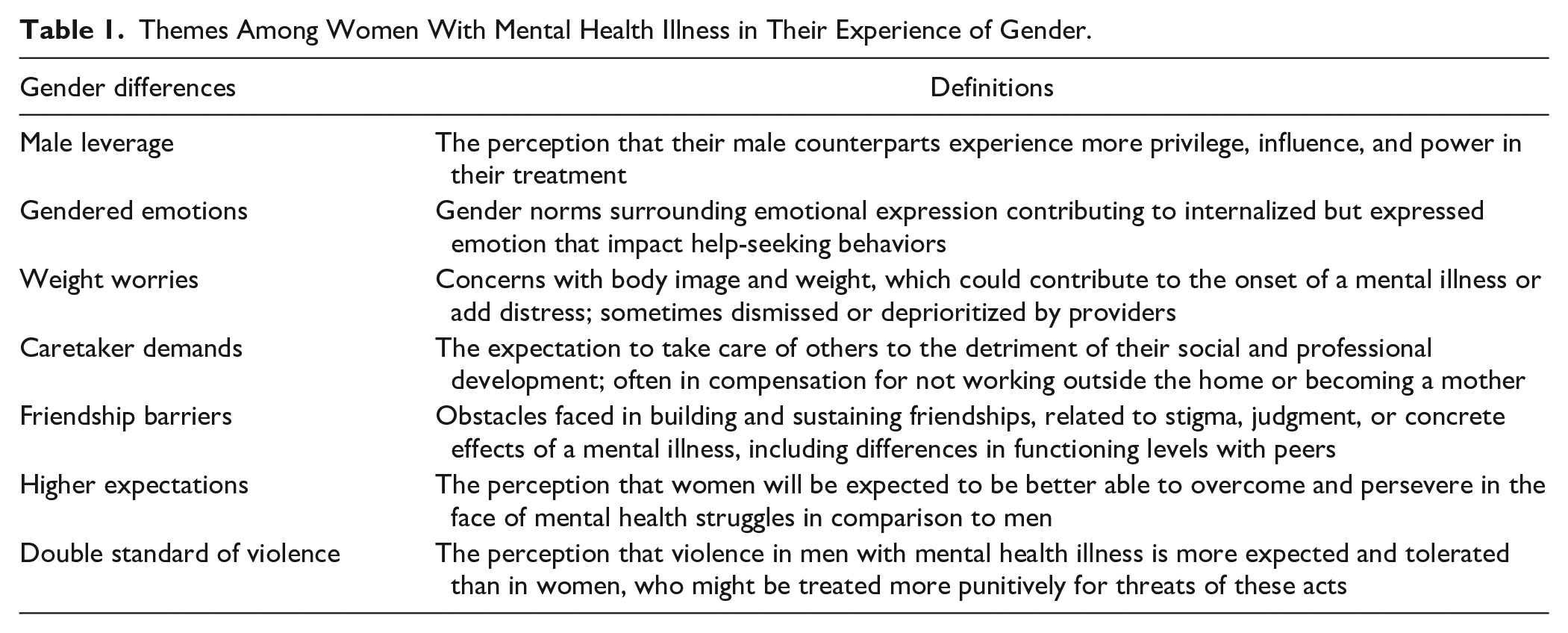
Several gender-specific themes emerged from the grounded theory analysis (see Table 1). Figure 1 displays the relationships between properties of the themes generated from the data analysis capturing our theory of the gendered treatment of women with mental health illness. This figure delineates the themes that represent different outcomes of their gendered treatment (triggering onset, worsening mental health, or a source of resilience). The following section describes these themes in further detail.
Themes Among Women With Mental Health Illness in Their Experience of Gender.
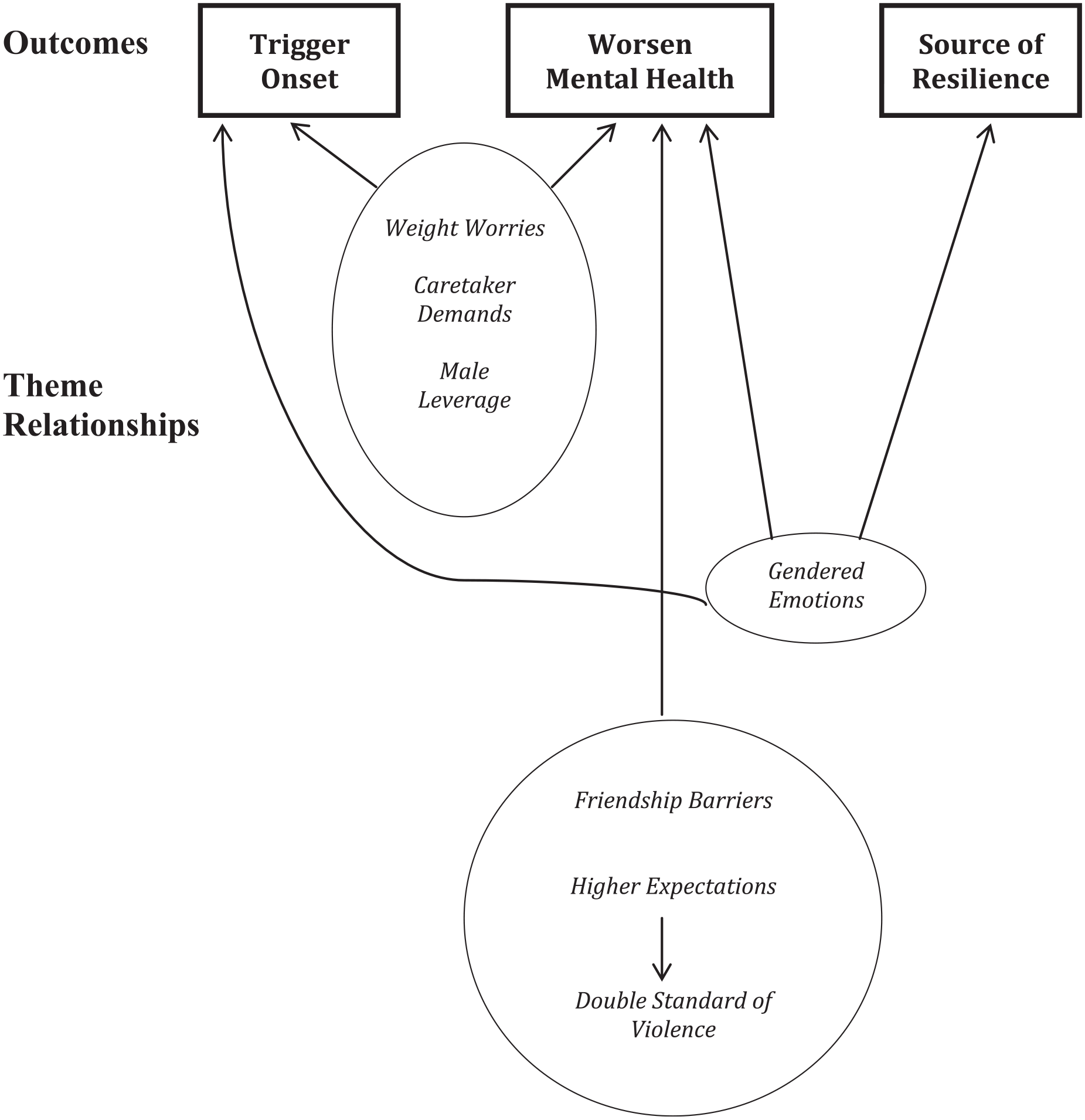
Grounded theory of relationships of gendered treatment themes for women with mental health illness.
Male Leverage
Participants in the study perceived gender differences in their mental health experiences, and in their treatment by others, particularly in the area of power. Therefore, the first theme was entitled, male leverage, an outcome of their gendered treatment that could trigger the onset of a mental health illness and also worsen their mental health. This theme refers to women’s perceived differences in gender privilege and influence of men in contrast to women with mental health illness that could impact their treatment by others. For example, one woman stated, The men seem to have been given some of the power in certain times. . . men have a louder, volumized voice and aren’t as timid or feel more empowered to say whatever they want.
This participant perceived men with mental health illness to experience more empowerment and agency in various settings than women. Several participants also noticed the intersection of race and gender in their experiences of gender differences in power and privilege in their treatment. When asked whether there was a difference between how men and women with mental health illness were treated, one participant of color stated the following: I think men are always taken more seriously. I remember when I was a lot younger there was like a million studies that concluded that men’s health issues are taken more seriously than women. And my mom and I looked at each other and I said, “Well give me a million dollars! I could have told them that!” . . . Men in general have more privilege, and the lighter their skin is, the more that is true.
This participant spoke about her perception of overlapping privileges of gender and race, and her sense that men, particularly White men, tend to have greater unearned advantages associated with their social standing, benefiting them in mental health settings.
Another participant also noted this issue of male leverage. She described feeling treated differently from her White male friend with mental health illness. She stated, “He could get away with anything and people look at him and then they just let him go. If they look at me, they won’t let me do anything.” Other participants confirmed the power associated with masculinity, in which they found men benefited in some way in contrast to women, amplified by the presence of other sources of power and influence, such as race.
Gendered Emotions
Another theme in the experience of gender among women with mental health illness was captured in the term, gendered emotions. This outcome of their gendered treatment took all forms in that it could trigger the onset of a mental health illness, worsen their mental health, but also represent a source of resilience. This theme refers to ways women felt gender norms affected them differently than their male counterparts with respect to emotional expression. For example, they described being more internalized than externalized in their emotional experience and expression. One participant captured this experience with the following statement: I think one of the things that might be woman-like would be the amount of shame. You know, the toxic shame. Yeah, and shame is a killer. The more internalized—I think women are more internalized and men can be more externalized, so they might not carry that shame to the point of being a life-threatening situation.
Although this participant implied that both men and women might experience shame, she perceived women to be particularly susceptible to this internalizing experience surrounding their mental illness, associated with a sense of failure as a woman for having a mental health illness.
In contrast, the participants also felt they had more freedom of emotional expression. One participant noted the potential source of strength in the differences in gendered emotions among men and women.
Sometimes I think it’s easier for women to have mental illness than men because at least we’re used to being told we can cry and we can be, you know, emotional . . . I feel like I have enough of a macho streak in me just from growing up and having to be tough. I can’t imagine being a man and having so much bottled up. I don’t know how they’re living and walking.
This participant noticed differences in the gender norms associated with emotional expression, impacting different experiences of mental health illness for men in comparison to women. Gendered emotions represented women’s perception of a challenge and also a source of strength in managing their experiences with mental health illness.
Furthermore, the women felt gendered emotions could have consequences for help-seeking behaviors. For example, one participant spoke about the effects of gender socialization on men and women with mental health illness.
I think it’s harder for men. I think they’re more stigmatized. Men are supposed to be tough and brave and strong all the time and not have emotion. I mean, that’s the cultural message, although it’s gradually changing. Some brave men are, well there’s an advertisement on television right now with a black man saying—whatever the percentages of people—you know, one third of people will have mental illness or contact with mental illness in their lifetimes. It’s time for men to speak up and get help. I mean, that’s a great ad. That’s a really good ad. I mean, my father killed himself. I had no idea he was that depressed.
This woman expressed her sense of the devastating effects that men may face with regard to the outcomes of gendered emotions and stigma for men with mental illness. She located this difference in experience as originating in cultural scripts and roles that differ for men and women. She spoke to how public service campaigns are beginning to target men and men of color who may face multiple levels of stigma that pose barriers to help-seeking.
Weight Worries
Another gender-specific theme was the presence of weight worries, an outcome of women’s gendered treatment that could trigger the onset of a mental health illness or worsen their mental health. When asked what gender issues they faced in their experience of mental illness, the participants described feeling particularly targeted by traditional beauty ideals and size-ism. Thus, weight worries referred to the unique concerns women perceived with regard to body image and weight management that could contribute to the onset of a mental illness or add distress. This theme was demonstrated in the following quote: [It all] started with an eating disorder . . . I was a little on the heavy side growing up. And then all of a sudden I just wanted to lose all this weight. And it was like an obsession almost . . . [and] I just became really depressed after high school.
For this participant, her mental health problems began with an eating disorder, which developed into severe depression. Hence, her internalization of cultural size-ism contributed to her mental health illness.
Another participant described the intersection of her weight worries and mental health problems.
I was diagnosed with the eating disorder, which is mostly binge eating and some restricting. I started dieting [at a] very young and that’s a tough one. So, I guess I was diagnosed with the eating disorder at age 15, but I kind of knew before that that I had it. It got bad at age 15. And it’s—I’m doing better with it but old habits die hard. It is very slow to, like, pick out that really entrenched behavior that goes so far back, and it’s a big struggle and a source of a lot of shame and frustration.
For this participant, the symptoms of her mental illness manifested in a variety of mental health problems, including with food. Her severe depression and anxiety disorders manifested in problem eating behaviors and obsessions about her size, leading to co-occurring eating disorders.
Caretaker Demands
In the theme of caretaker demands, participants spoke about how they differed from men with mental health illness in being expected to nurture others. Like weight worries and male leverage, his theme represented an outcome of their gendered treatment that could trigger the onset of a mental health illness and also worsen their mental health. For example, one participant spoke of this theme in her experience in her childhood. She survived a range of abuse and neglect as a child of parents with mental and physical illnesses.
My mom died of a severe asthma attack, so we don’t know whether I got PTSD due to the crap [sexual abuse] my step-dad pulled, or whether I got it because I was my mom’s primary caretaker when I was little, too.
This participant described how caretaker demands could have contributed to the actual onset of her mental illness altogether.
In other cases, family members expected the women to take on caretaker roles to compensate for her inability to maintain a career or become a parent as a result of her mental health illness. For example, one participant described how her family pushed her into this role early on: I had to go get a hamburger for my brother before he went to work when I didn’t want to. And once I was in the bathroom and my mother made me get out to make my brother go in. She got him a political job, and she didn’t do [that] for me. And she helped—went with him to get a car. She kind of supported him in different ways . . . I think the whole thing, how I was socialized, I think I was supposed to take care of my parents in their old age. I think that’s the role I was supposed to have. So, I don’t think my mother cared really, if I had social relationships and stuff like that.
In this interview, the participant described her social and professional development was limited by caretaker demands, which worsened her mental health, and further limited her ability and hope to work outside the home, develop a career, and form connections with others. She felt that caretaker demands contributed to her psychological distress, and these problems further cemented her in a caretaker role, without a career, home, or family of her own.
Friendship Barriers
The theme of friendship barriers emerged when participants were asked about their unique experiences of mental health illness as women. This referred to unique obstacles women with mental health illness face in building and sustaining friendships, which could potentially worsen their mental health. Friendship barriers could include experiences such as peer judgment and feeling taken advantage of. One participant also spoke about how stigma posed barriers to peer relationships.
I try to stay private about it. I’ve chatted about my depression now and again with a couple of different people in the building, mostly female, and, I always end up feeling sort of patronized later. Or condescended to or looked at in this “poor you” way. Like, pitied, you know?
Women often appeared devastated by these friendship barriers and the social isolation that could result.
Another issue with developing friendships included differences in functioning levels with other women with mental health illness. A Chinese participant described this experience: Well, I have Chinese friends that are from a church I go to in Chinatown. So, they are working. Well . . . a couple of them have mental problems but they could hold a job. They could drive. They could do everything. So that has been pretty good with them, the relationship. As for other races, they do have mental illness, and I’m friends with them. But their mental illness combined with mine, sometimes it’s kind of harder too. So I like being with people that doesn’t have a mental illness, [who are] more well than me.
In this excerpt, we see that friendships could be further complicated by negotiating other variables, including racial-ethnic identity and functioning level. Having a shared sense of cultural community seemed to serve as a point of commonality. However, this woman also appeared to avoid friendships with peers, due to differences in functioning level and possibly internalized stigma, which was not uncommon for other participants as well.
Higher Expectations
The theme of higher expectations refers to ways women felt they were held to a higher standard than men with mental health illness, which could potentially worsen their mental health. The women spoke about perceiving more judgment from others, while sensing that men may be given more permission and acceptance around having a mental health illness. One participant with severe depression explained this problem.
They do see women differently, because it’s like they sometimes accuse me of being manipulative when I really wasn’t. And I kind of felt like if I were a guy, they wouldn’t say I was being manipulative. And I don’t know if I’m right about that, but I’ve heard other people have said—they’ve sort of corroborated that experience. Like, when you’re a woman and you have a miscommunication, they say, “Oh, you’re being manipulative. You should have known better.” And I’ve definitely had people say to me, “You should have known better.”
This participant underscored the scrutiny that women face surrounding their social intentions and the higher standards she feels they are held to in contrast to their male counterparts.
Another participant noticed this gender issue in the public portrayal of several celebrities: Sometimes I’m jealous of certain people. I don’t know if they’re CEOs and then you’ll find out they’re bipolar. But there’s Demi Lovato, and she went into rehab and she’s been successful, and I think she’s an alcoholic or something, but it’s just interesting. And then, I don’t know, maybe Brittany Spears got a bad rap. I mean, it sounds like her thing [losing custody] was so traumatic. And I’m not saying it was wrong, I think other people had to take care of her children, but . . . it just seemed like people thought she was way out of it. Out there. And maybe didn’t—kind of mocked her for being mentally ill. Maybe now a guy going through the same thing wouldn’t get the same treatment. Or it’d been like, “Oh, that’s what artists do . . .” It’s okay for men to have more setbacks. But, like in my family, I think my brother judges himself a lot less than I do, that it’s okay for him to have setbacks.
This example demonstrated how this participant, like the others, found the media both reflected and shaped expectations of mental health experiences of men versus women, which is then re-enacted in the family sphere.
Double Standard of Violence
Several participants noted that women with mental health illness are held to a higher standard around violent behavior, which could potentially worsen their mental health. The theme, double standard of violence, refers to women’s sense that male-initiated violence was interpreted as more acceptable than female violence, with women receiving harsher punishment for acting out. An example of this theme was described in the following quote: Certain females, the guys, they have a tendency to yell and scream and aren’t called on it. But if a woman would yell and scream, she would be called on it in a second . . .
In this excerpt, the participant noticed women being treated more harshly for acting out or when feeling unsafe, while she found this behavior was more expected and, perhaps, somewhat tolerated in men by comparison.
Another woman applied the double standard of violence among men versus women with mental health illness to the case of Aileen Wuornos. Wuornos was a woman with mental health illness and sexual assault survivor who murdered a number of men who picked her up for hitchhiking and sex work. The participant observed the following in the case of Wuornos: They put a woman to death, you know . . . If a woman defends herself from a batterer, she’ll go to jail. And a guy can batter a woman and they don’t spend near the amount of jail time. So, I think women are treated more harshly. When they create—do a crime that might be connected to their mental illness, I think they get harsher sentences. And I don’t think Aileen should have—maybe life in prison—but she shouldn’t have been put to death. She was—you could see right before they did it—that she was totally removed from reality.
This participant spoke about how women with mental health illness may find that they are receiving more punitive treatment as a result of the double standard of violence among men and women. This participant felt that while Wuornos appeared actively psychotic and delusional at the time of her execution, she still received the death penalty.
Discussion
Women with mental health illness noted a number of different gender issues in their mental health experiences and treatment by others. Many of these gender themes are seen in the experience of women and men in general but had unique implications for women with mental health illness. The grounded theory of the gendered treatment of women with mental health illness depicts our delineation of these themes and their properties and relationships (see Figure 1). Specifically, these experiences of their gendered treatment could contribute to different outcomes, including the onset of mental health illness or worsen mental health, or they might offer unique resources and sources of resilience. For example, the participants felt that differences in male leverage could impact their treatment by others and bar women with mental health illness from voicing her concerns. Male leverage referred to the perception of women with mental health illness that their male counterparts experience more privilege, influence, and power in their treatment. This finding suggests that women with mental health illness may be particularly attuned to issues of gender privilege as a result of their experience with the double oppression of sexism and mental illness stigma (Logie et al., 2011).
While women with mental health illness felt gendered emotions led to more internalizing symptoms of the mental health illness, they also found it came with a greater freedom of emotional expression. Gendered emotions refers to gender norms surrounding emotional expression of women with mental health illness, contributing to internalized but expressed emotion that impact help-seeking behaviors. Other research has identified gender differences in emotional expression and reactivity as they uniquely contribute to women’s mental health (Nolen-Hoeksema, 2014). As a result of gender socialization, women are more likely than men to ruminate on negative emotions like sadness, but they are also more likely to benefit from greater expression of positive emotions (Chaplin, 2015; Nolen-Hoeksema, 2014). Our study highlighted that women with mental health illness could appreciate their emotional strengths and feel compassion for the emotional repression of many men with mental health illness. These results suggested that women with mental health illness may experience another source of coping as a result of gendered emotions, including the ability to detect an emotional problem and reach out for help. Thus, the experience of gendered emotions could pose both risk as well as resilience to women with mental health illness.
However, the participants felt their internalizing of emotions might manifest in eating problems, reflecting the cultural body ideals that led to obsessions with weight. These weight worries could also contribute to the development of a mental health illness, as in the example of the woman whose obsession with her size led to severe depression. Weight worries involved these types of eating problems that could contribute to the onset of a mental illness or add distress, which was at times dismissed or deprioritized by providers. Weight worries might also be reflected in the symptoms of a mental illness, such as disordered eating or exercise behaviors. The participants sensed that these weight worries were often misunderstood or minimized by others in their lives.
It is well known that there are gender disparities in the prevalence of eating disorders with higher incidence among women as a result of sociocultural factors (Hoek & van Hoeken, 2003). While eating disorders such as bulimia and anorexia are not typically considered mental health illness, the relationship between weight worries and mental health illness onset could represent by a diathesis–stress relationship (Meehl, 1962). In other words, the distress about one’s weight could trigger the expression of mental health illness when there was a predisposition (diathesis). It is important to note here that the media and other sociological factors impose beauty standards on women that add considerable strain. The present findings suggest that these sociocultural pressures might also be a contributing factor for women with mental health illness.
Similarly, given women’s socialization to take care of others, the participants felt particularly affected by caretaker demands from family and men in their lives. Caretaker demands included the experience of women with mental health illness that they will be expected will take care of others to the detriment of their social and professional development, often in compensation for not working outside the home or becoming a mother. The participants highlighted the impact of caretaking expectations on the recovery process, as they found caretaking responsibilities often worsened their mental health.
This theme of caretaker demands may reflect a particular contribution of the present study. Much of the caregiver literature on women with mental health illness has focused on the caregiving of family members for people with mental health illness, who are often female given gender differences in role expectations (Sharma et al., 2016). In contrast, our study identified caretaker demands of women with mental health illness for others in their family. Sometimes these caretaker demands were seen as compensation for functional limitations to work outside the home or become mothers of their own children, leading them to be identified as caretakers for elder family members and male partners. The caretaker expectations could begin at a young age and limit their social and professional development, posing isolation and further distress that contributed to the onset of their mental illness.
Women in the study also experienced friendship barriers associated with stigma, concrete challenges posed mental health illness, or functioning differences with their peers. Friendship barriers referred to obstacles women with mental health illness face in building and sustaining friendships, related to stigma, judgment, or concrete effects of a mental health illness, including differences in functioning levels with peers. Social issues were particularly painful given their socialization to focus on connection and gain vital sources of support from other women. Little research has been conducted on the relationships of women with mental health illness beyond a sexual risk-taking framework. This finding made a unique contribution to the literature regarding the particular challenges they face in peer judgment and social isolation. Thus, stigma may interfere with the social support that women with mental health illness draw upon in managing the challenges of a mental health illness, worsening symptoms and interfering with recovery.
In addition, women with mental health illness felt they were held to higher expectations than men in their interpersonal behavior—expected to persevere in the face of mental health struggles, particularly surrounding issues of motherhood. The theme of higher expectations included the perception of women with mental health illness that they will be expected to be more capable of overcoming mental health struggles in contrast to men. These expectations may occur as a result of some of their strengths in emotional expression captured in the gendered emotions theme.
These higher expectations also extended to double standard of violence among men and women. This theme referred to women’s perceptions that violence in men with mental health illness is more expected and tolerated than women. In comparison, women might be treated more punitively for threats of these acts. Other research has discussed the double standard of aging for men and women in general, where men are seen as attractive as they age and women are not (Berman et al., 1981). Our findings extended this research into the area of mental health illness and suggested that this double standard may add greater stress and strain, potentially worsening the effects of the mental health illness for women who act out.
Rehabilitation Counseling Implications
A number of implications for rehabilitation counseling study emerged from these findings. With regard to women’s perceptions of male leverage, it should be noted that while one’s perceptions of gender differences in treatment may not always be reality, rehabilitation counselors should validate each individual’s experience of gender, whether real or imagined. There are differences in the treatment and privilege of men and women in the broader culture, which may be enacted by treatment staff. Rehabilitation counselors should be mindful of gender differences in perceptions and expectations that women with mental health illness may bring to their mental health care.
Women can be helped to understand the impact of gender socialization on emotional expression as well, with women experiencing greater internalizing emotions that lead to directing pain inward. Practitioners might ask questions of women with mental health illness such as, “What are your strengths and challenges in dealing with difficult emotions as a woman with a mental health challenge?” Rehabilitation practitioners can explore and challenge the shame, self-stigma, and self-harm that can result from the tendency to internalize distress. On the other hand, women may feel less stigma surrounding their expression of emotions, which can serve as a source of resilience and rehabilitation in counseling settings. Practitioners might coach women in enhancing distress tolerance or using expressive means to channel difficult emotions such as writing, drawing, or movement.
The impact of weight worries on the development of mental health problems can also be clarified for women with mental health illness to validate their experience. Women are more likely to gain weight due not only from the side effects of medications, but also from childhood trauma, pregnancy, and menopause (Goodrich et al., 2016). Thus, these women face multiple levels of stigmatization as women with mental health illness who are overweight (Mizock, 2012). Potentially due to this pressure on the body, women with mental health illness have higher enrollment in some weight loss programs in mental health settings (Goodrich et al., 2016). Programs like the Health at Every Size (HAES) model can be tailored to this population and adopted in rehabilitation counseling settings to better address their needs without reifying cultural pressures surrounding thinness (Mizock, 2012). HAES promotes size acceptance, positive physical activity, and healthy eating to end weight stigma and redirect focus from weight loss to overall health (Burgard, 2009). Given that women may feel dismissed by others in this area, it is important for rehabilitation counselors to acknowledge size pressures from the broader culture and address their concerns about size, while maintaining a sociocultural perspective of the impact of misogyny on weight concerns. Rehabilitation counselors can learn from the HAES model and redirect the focus of women with mental health illness from weight loss to feeling healthy.
With regard to caretaker demands, women can explore and evaluate these roles with their rehabilitation counselors to understand their development and association with gender. Counselors could ask questions like, “Have there been expectations of you as a woman in your culture for taking care of others? What has that been like for you? Has this had an impact on your mental health in any way?” For some women, caretaking for their family, particularly in the absence of a career or parenthood, might be a source of pride and meaning. Hence, individual meanings of this role should be unpacked, and rehabilitation counselors can explore the positive meaning or strain that women might experience in caretaker roles. Counselors can help women to understand the impact of this role on the development of their mental illness or source of resilience offered by it. They can support women in advocating for changes in this role depending on their needs and values. This support could occur by helping women to identify any rehabilitation goals they might like to set in this area, and mapping steps toward achieving them to help increase their independence. In addition, counselors could encourage women to communicate about their desires in this area to relevant parties, practiced via role-plays and other forms of communication skills teaching.
Rehabilitation counselors can help women understand the different expectations and double standards women experience regarding their mental health and behaviors in contrast to men, particularly regarding violence. Counselors might ask questions to this point such as, “Do you feel that you are treated differently or face different expectations as a woman with a mental health challenge than men? At home? In mental health services? In other settings?” Counselors can help women with mental health illness to gain an awareness of how men and women might differ in their experience of unearned social advantages, and uniquely impact their mental health and treatment experiences. Rehabilitation practitioners might even use Table 1 as a discussion tool in sessions with women with mental health illness to raise awareness of gender-specific experiences of mental health illness.
It may be difficult for women to navigate these double standards and unfair, gendered treatment as a result of the implicit values of their providers. However, some research suggests the best way for women with mental health illness to get their needs met in various systems is to form strong relationships with their providers who can advocate on their behalf (Mulvey, 2013). Rehabilitation practitioners can educate team members on inpatient units to recognize their different sociocultural attitudes and treatment toward women when they act out due to these double standards to prevent punitive treatment of women in this area.
Clearly, interventions are needed to allow women with mental health illness to explore the effects of gender on mental health illness and boost empowerment and recovery. The Women’s Empowerment and Recovery-Oriented Care (WE-ROC) intervention has been developed and piloted to address this need (Mizock, 2019). WE-ROC is currently being refined for future implementation. This intervention is a manualized, 10-session group based on the results of the present study and other related research. The curriculum addresses issues of stigma, relationships, and gender identity for women with mental health illness, to name just a few of the topics. Rehabilitation counselors might consider implementing this group or drawing from the manual to inform rehabilitation counseling sessions with women with mental health illness to address many of the issues raised in the findings in this article. The manual includes a range of therapeutic strategies and exercises, including discussion questions, worksheets, activities, visualization exercises, and other tools and resources.
Limitations and Future Research
The present study includes several limitations that suggest directions for future research. Further research can be conducted to evaluate these findings using quantitative measurement beyond the Northeast regional sample in the present group. Additional investigation of the experiences of men’s perceived gender differences is needed as well.
Another research limitation had to do with the nature of the methodology and data that were collected. Female participants in this study often described their perceptions of gender differences in their treatment, and perceptions are not necessarily facts. Qualitative researchers tend to embrace the subjectivity of participants and intersubjectivity created between interviewer and participant. They are less concerned with facts than learning about the stories and viewpoints of the people being interviewed, and how they shape their experience (Josselson, 2013). Our findings were based on the participants’ perspectives rather than outsider observation or quantitative measurement. However, these perceptions can be considered with caution given the limitations in evaluating the perceptions of the lived experience of one group of people by another (i.e., of males by females).
Finally, while multiple data quality measures were utilized in the present study to enhance methodological rigor, the process of member-checking findings with participants would enhance data quality and could be used in future research in this area. More research is needed to further identify the current issues and clinical needs of women with mental health illness with regard to relationships and dating, work experiences, parenting issues, strengths and resilience, as well as meaning-making. More research is needed to develop effective interventions to meet the needs of women with mental health illness, and this research is underway with the aforementioned Women’s Empowerment and Recovery-Oriented Care group intervention for women with mental health illness (Mizock, 2019).
Conclusion
Women perceive many differences in their experience of a mental health illness in contrast to men and experience unique gender issues in their treatment. The present study found key issues in women’s experience of gender in their care to range from mental health symptoms to family treatment to community roles and expectations. Gender socialization and associated gender norms pose challenges to women with mental health illness, although their uniquely gendered experience also offered sources of coping and empowerment. Specifically, women with mental health illness felt they were afforded less power and privilege in their care and being held to a higher standard and punished more harshly when deviating from this standard, particularly in the area of violence. Moreover, women with mental health illness tend to express concerns about their size, barriers to forming friendships, and expectations to caretake others as key issues in their lives. Rehabilitation counselors can help women to recognize and manage the role of gender in their mental health experiences to enhance recovery and social support through therapeutic discussion, goal-setting, and collaborative advocacy in the systems and relationships within which they interface. Rehabilitation counselors can also contribute to activism and policy change to raise awareness of the impact of gender socialization on mental health and prevent its deleterious effects on mental health.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research stipend from Fielding Graduate University.