
Abstract
The 12-item World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) has been used to assess functional impairments in various disability populations and has been shown to be applicable to the youth population. The purpose of the study was to evaluate the psychometric properties of the World Health Organization Disability Assessment Schedule II–Youth Version (WHODAS-Y). Results of the study revealed a two-factor solution, including the socio-cognitive index and self-care index. The WHODAS-Y measurement appears to be a reliable and valid measure of function impairment in transition-age youth with disabilities in a community setting. This assessment tool can be integrated in vocational rehabilitation practices and guide rehabilitation counselors in identifying needs and facilitators related to education and employment-related services, as well as understanding health care needs in youth with disabilities.
The experience of living with a disability is a global concern. Approximately 1 billion people, or 15% of the global population, are identified has having a disability (World Bank, 2018). The classification of disability varies across different systems but generally involves an impairment in body function or structure that limits the ability to complete tasks or actions, ultimately restricting participation in a range of major life activities or situations (World Health Organization [WHO], 2018). Regardless of the method of classification, persons with disabilities are faced with barriers to accessing health and rehabilitation services in many settings (WHO, 2018). These barriers are often the result of restrictions on the requirements or qualifications for services. With limited resources, governments and collaborating agencies are often faced with the need to prioritize services for those with the most significant needs (WHO, 2018). For example, state vocational rehabilitation (VR) programs in the United States are required to implement an order of selection if unable to serve all those individuals who apply and are eligible for services. An order of selection involves creating a tiered waiting list to determine the order that individuals will receive services with a focus on serving those with the most significant disabilities first followed by persons in other categories of severity (Hager, 2004). Under an order of selection, some individuals on the waiting list, particularly those considered to have the least severe disabilities, may never be served (Hager, 2004). Due to a paucity of empirical research on the prevalence of disability in children and youth (United Nations Children’s Fund, 2013), many countries and communities struggle in developing evidence-based intake procedures and intervention programs capable of supporting the needs of youth with disabilities, particularly at the critical juncture of their transition to adult life (WHO, 2011).
Upon transitioning into adulthood, youth face a complex set of new tasks, responsibilities, experiences, and expectations. To mitigate the difficulties and ambiguities often present in this transition period, the groundwork for transitioning into adulthood is laid at an early age, instilled in the curricula and values of early education, and further expanded upon in high school (Bruner, 1966; Weidenthal & Kochhar-Bryant, 2007). High schools foster a student’s sense of self-awareness by providing a course load aimed at identifying their passions, interests, and strengths, while providing the setting for diverse peer interactions that help to cultivate a varied understanding of society and the world. This developmental period of adolescence is integral to the advent of career awareness and exploration (Niles & Harris–Bowlsbey, 2009). Schools often foster this awareness by integrating a variety of services into the framework of their curriculum, such as employment opportunities, career counseling, and extracurricular activities (Worthington & Juntunen, 1997). Participation in these activities can also help the growth of self-determination, which research has shown aids in the development of independence and greater employment outcomes (Wehmeyer & Palmer, 2003).
In an effort to insure that youth are served by the state VR program, the Workforce Investment and Opportunity Act requires states to set aside 15% of their budgets to provide pre-employment transition services for youth with disabilities who are eligible or potentially eligible for services (Department of Education, 2014). As such, youth with disabilities have a clear pathway to being served by state VR agencies. However, in identifying specific needs of youth, as well as those that are potentially eligible who are not recipients of federal programs such as Supplemental Security Income (SSI) or have an Individualized Education Program through their schools, state VR programs may realize benefits from an instrument that can assess the functional impairment and impact of that impairment on daily living and overall health and functioning.
Reliability and Validity of WHODAS 2.0
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) is a global self-report measurement of functioning and disability (Andrews et al., 2009; Kimber et al., 2015; Üstün et al., 2010). The assessment measures an individual’s level of functioning 30 days prior to the assessment in six major life domains: cognition, mobility, self-care, getting along, life activities, and participation in society (Carlozzi et al., 2015; Gold, 2014; Üstün et al., 2010). It was designed to be a standard measure that was consistent between different health conditions, countries, and cultures (De Wolf et al., 2012; Gold, 2014). It has also been known to be beneficial in population surveys, identifying health outcomes, and assessing treatment effects (Gold, 2014; MacLeod et al., 2016; Üstün et al., 2010). The WHODAS 2.0 has two versions for assessing disability, the full 36-item version and the shortened 12-item version. Both have been tested numerous times to be reliable and valid measures of functioning and disability (Carlozzi et al., 2015; Sjonnesen et al., 2016; Üstün et al., 2010).
The reliability and validity of the WHODAS 2.0 measures has furthermore been tested with different disabilities across many different countries and cultures (Carlozzi et al., 2015; De Wolf et al., 2012; Smedema et al., 2016; Üstün et al., 2010; Wu et al., 2020). A Canadian study used the 12-item WHODAS 2.0 to assess severity of mental health disorders using a community survey with the adult population (Sjonnesen et al., 2016). Results suggested even though the measure was not mental health specific, the WHODAS 2.0 was a reliable measure for mental health with higher scores indicating more severe disability. The study also found that the 12-item WHODAS 2.0 was sensitive to changes in health during the individual’s lifetime (Sjonnesen et al., 2016). A different study used the 12-item WHODAS for adults with Huntington disease (Carlozzi et al., 2015). The results showed good internal consistency and convergent validity advocating its use for individuals with differing disabilities, in this case specifically Huntington disease.
Andrews and colleagues (2009) assessed the 12-item version to test its reliability as a common measurement of functioning and disability using a sample of Australian residents aged 16–85 years old. Confirmatory factor analysis (CFA) was conducted to verify a second-order, one-factor solution with six first-order factors as the best model fit, which is consistent with the six domains of functioning (Andrews et al., 2009). A more recent study using a sample of adults from a data set of community samples yielded similar results (MacLeod et al., 2016). The analysis consisted of evaluating four different community-based studies of adults in Canada that all used the 12-item WHODAS as a measure of disablement or daily functioning. The results of the CFA indicate verification for a one-factor model (MacLeod et al., 2016). After running a latent class analysis (LCA), the study also revealed four different subgroups of responses including pervasive disability; physical disability; emotional, cognitive, or interpersonal disability; and no/low disability. However, sample size for this population was low so further research is needed to confirm replicability in a larger population (MacLeod et al., 2016). Likewise, most of those studies have focused on adult populations in clinical settings, and as a result, more research is needed to see whether WHODAS 2.0 is applicable to the younger population outside of clinical settings.
Use of WHODAS 2.0 With Adolescents and Youth
The WHODAS 2.0 was designed to assess functioning due to disability with adult populations. Research on the direct application of this measure to youth without consideration of the different response set of youth or the applicability of the items to this population has been limited. As such, WHO does not host a youth version of this scale (WHO, 2020). However, several studies have focused on applying it to measure the disability in youth populations (Andrews et al., 2009; Hu et al., 2012; Kimber et al., 2015). One study aimed to assess the validity and internal consistency of the 36-item version of WHODAS 2.0 in adolescents in China (Hu et al., 2012). Adolescent inpatients and junior high school students ranging from 10 to 19 years old were recruited to participate, with 14.07 years being the median age of the youth. A 35-item version of the WHODAS 2.0 was distributed to the youth, after one item about sexual activity was removed bringing the Cronbach’s alpha to .95 (Hu et al., 2012). These results indicate that the WHODAS 2.0 can be a reliable measure of disability for transition-age youth. However, further research on how it compares with the adult population is needed.
Kimber et al. (2015) used the 12-item version of the WHODAS 2.0 to measure the invariance between adult and youth populations in Canada. Measurement invariance refers to the amount to which the measurement traits of the construct is equal across the different groups of interest (Hu et al., 2012; Kimber et al., 2015). The youth sample included transition-age youth 15–17 years old and the adult sample consisted of individuals 18 years or older. The results showed evidence of a strong invariance between youth and adults, signifying youth and adults interpreted the items of the measure in the same way (Kimber et al., 2015). Therefore, these results suggest that the 12-item WHODAS 2.0 can be applied for use with transition-aged youth in clinical and epidemiological settings.
Purpose of the Study
The 12-item WHODAS 2.0 has been shown to be applicable to the youth population (Tompke et al., 2018). The current study aims to validate the youth version of the WHODAS 2.0 called World Health Organization Disability Assessment Schedule II– Youth Version (WHODAS-Y) in a sample of transition-age youth living in a community setting.
Method
Participants
The study included 436 youth with a disability who received SSI between the ages of 14 to 16 (M = 14.96, SD = 0.86) years at entrance into the study. Demographics were broken down by race, gender, primary disability, and highest level of education. Caucasian was represented the most with 191 (44.4%) participants, where African American followed closely with 188 (43.7%) participants. Within this study, 7.7% (n = 33) identified as being Hispanic while American Pacific Islander, Non-Hispanic reported 2.3% (n = 10) of the sample. The rest of the participants made up less than 10% of the population including Asian, Non-Hispanic (0.5%; n = 2) and other/unknown, non-Hispanic (0.9%; n = 4). Only eight participants had values not reported. In the sample, males encompassed most of the participants (68.1%; n = 293), followed by females (31.6%; n = 136) and finally seven participants who did not disclose gender.
Primary disability type of the participant was one of the demographic questions asked during the baseline survey. Developmental disability was the most prevalent self-identified primary disability with 131 (30.5%) of the participants. Psychiatric disability closely followed with 130 (30.2%) of the participants. Other disabilities included 120 (27.9%) participants. Long-term illness was among the highest with 20 (4.7%) participants, followed by a tie between physical/mobility and sensory disability that had 10 (2.3%) participants a piece. Less than 5% of the population identified with having a primary disability of head injury/traumatic brain injury (1.4%; n = 6) and value not reported ( n = 9).
Participants were asked to specify the highest level of education obtained. Participants surveyed ranged from having some middle school education to completion of high school. The most prevalent reported highest grade completed for 30.5% (n = 131) of the participants was eighth grade followed by 27% (n = 116) reported ninth grade as highest completed. Completion of the 10th grade included 78 (18.1%) of the participants and 72 (16.7%) of the participants reported their highest grade completed as seventh grade or lower. Only 14 (3.3%) participants completed the 11th grade and one person (0.2%) reported the completion of the 12th grade. Some participants chose not to answer (n = 17) and 7 (1.6%) reported other as the highest grade.
Instruments
Functional impairment
The WHODAS-Y was designed based on the WHO International Classification of Functioning, Disability, and Health (ICF; WHO, 2001) to assess the impact of a health condition or disability in terms of functioning. The measure has a total of 12 items representing six domains of daily activities. The internal consistency reliability for WHODAS 2.0 12-item scale has been reported to be .94 (Carlozzi et al., 2015). For this study, 11 items were selected for inclusion. Participates endorsed their agreement with these items on a 5-point Likert-type response scale ranging from 0 (no difficulty) to 4 (extreme difficulty/cannot do). The selection of 11 items was done to reduce response burden across the entire protocol and one item being perceived as not being applicable to the population of interest. That item assesses difficulty in “day-to-day work” and given the population of interest was unlikely to be working as a function of age (less than 16 at admission to study), this item was dropped from further inclusion in the study.
Outcome expectation
The Vocational Outcome Expectancy Scale (VOES) was used to measure youth perception on their own outcome expectancy. Previous research has identified a relationship between overall functioning to outcome expectations of VR services (Tansey et al., 2017). The VOES was developed based from the social cognitive career theory (SCCT) which was an expansion of Bandura’s (1986) social cognitive theory. SCCT introduces the explanation of career development of adolescents and young adults (Lent et al., 1994). The VOES is an 11-item scale that asked participants to rate their level of agreement with vocational outcome statements. Questions include completing the sentence, “completing my vocational rehabilitation program will likely allow me to”: in two factors, positive employment outcomes and negative employment outcomes. Example of positive employment outcomes, “find a job that I can do well” and questions that reflect on negative outcomes or barriers “increase in responsibilities” (Iwanaga et al., 2017). Questions are answered on a 5-point Likert-type scale that range from 1 (strongly disagree) to 5 (strongly agree). The VOES had a Cronbach’s alpha of .92 in this study.
Stages of change for employment
Stages of change for employment were assessed using the 15-item version of the Stages of Change for Vocational Rehabilitation Scale (SOC-VRS; Rehabilitation Research and Training Center on Evidence-Based Practice in Vocational Rehabilitation [RRTC-EBP VR], 2014). Stages of change for employment was identified as an appropriate construct to measure the motivation, and ultimately, a precursor for behavioral intention to go to work and has previously been identified as being related to overall functioning (Tansey et al., 2017). Each item is rated on a 5-point Likert-type response scale ranging from 1 (strongly disagree) to 5 (strongly agree). The scores on the 15 survey items were averaged, with higher scores indicating the greater readiness to obtain employment. The Cronbach’s alpha for the SOC-VRS was computed to be .79 for this study.
Health care expenditures
Participants were tracked on their health care utilization, as measured by the expenditures for health care for 36 months subsequent to completing the study measures. In addition to total health care expenditures, expenditures were subdivided into those for outpatient treatment costs and those costs associated with prescription medications. The costs identified under health care expenditures were those associated with billing invoices submitted by treating professionals for services provided.
Statistical Analysis
We adopted a random split-half approach and performed exploratory factor analysis (EFA) with first data set (n = 229) and CFA with second data set (n = 207). All analyses were conducted with SPSS 24 and R (RStudio Team, 2015) and lavaan package (Rosseel, 2012). Pearson product–moment correlation coefficients were computed to provide evidence of construct validity for the WHODAS-Y on its relationship with functioning related constructs (i.e., stage of change and outcome expectancy). Internal consistency reliabilities (Cronbach’s alpha) and Pearson product–moment correlation coefficients were calculated on the sample as a whole.
Results
Exploratory and Confirmatory Factor Analyses
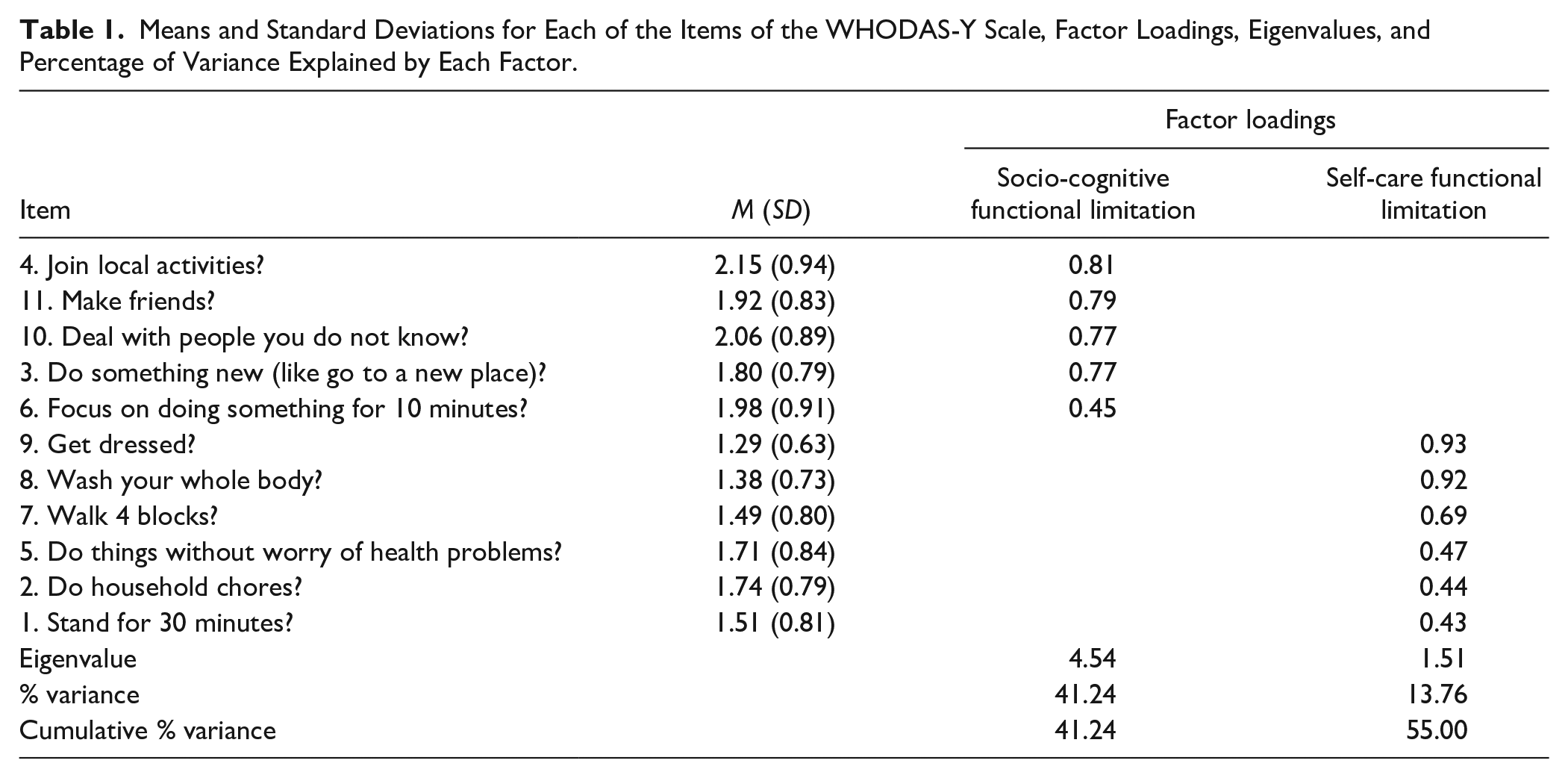
A principal component analysis with oblique rotation was conducted on the first split-half data set (n = 229) to examine the structure of the WHODAS-Y. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was .83 (>.60), and the Barlett’s test of sphericity was significant, χ2 (55, N = 229) = 934.04, p < .001, indicating suitability for factor analysis. The Kaiser–Guttman “eigenvalues greater than one” criterion and Cattell’s scree test (Cattell, 1966; Nunnally & Bernstein, 1994) indicated a two-factor solution, accounting for 55% of the total variance. Component 1 is composed of five items (labeled socio-cognitive index), and Component 2 is composed of six items (labeled self-care index). The magnitude of the factor loadings was satisfactory; loadings on target factors ranged from .43 to .93. The correlation between socio-cognitive functional limitation and self-care functional limitation was moderate to high (r = .59, p < .001) (Figure 1; Table 1).
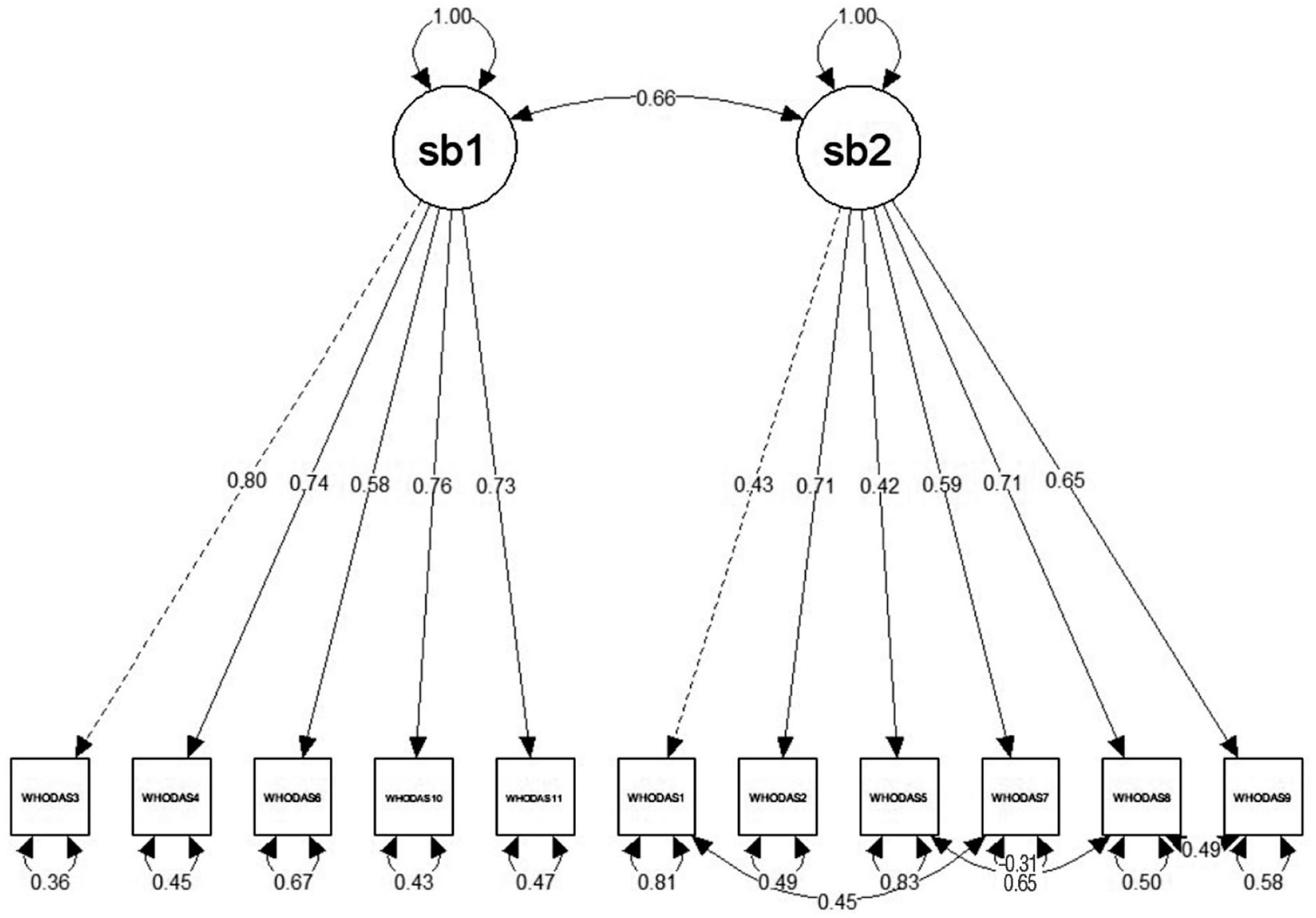
Confirmatory factor analysis results of the two-factor WHODAS-Y.
Means and Standard Deviations for Each of the Items of the WHODAS-Y Scale, Factor Loadings, Eigenvalues, and Percentage of Variance Explained by Each Factor.
To study the stability of the EFA, CFA was conducted on the second data set (n = 207), analyzing the items for socio-cognitive and self-care functional limitation, respectively. The initial model indicated a poor fit for the model: χ2(43, N = 207) = 171.52, p < .001; χ2/df = 3.98, comparative fit index (CFI) = 0.85; and root mean square error of approximation (RMSEA) = 0.12, 90% confidence interval (CI) = [0.11, 0.16]. An examination of modification indexes suggested that three pairs of error terms should be correlated: (a) Item e8 (“Wash your whole body?”) with Item e9 (“Get dressed?”); (b) Item e1 (“Stand for 30 minutes?”) with Item e7 (“Walk for 4 blocks?”); and (c) Item e5 (“Do things without worry of health problems?”) with Item e8 (“Wash your whole body?”). The re-specified model indicated an acceptable fit for the model, χ2(40, N = 207) = 80.24, p < .001; however, χ2/df = 2.01 is less than 3, CFI of 0.951 is greater than 0.95, and RMSEA of 0.07 (90% CI = [0.05, 0.09]) is below the value of 0.08; all these indexes meet the criteria of good model fit (cf. Weston et al., 2008). All items in the two-factor model significantly loaded their respective factors ranging from 0.58 to 0.80 for socio-cognitive functional limitation factor and from 0.42 to 0.71 for self-care functional limitation factor.
Means, Reliability, and External Correlates
Mean of the average item scores for the socio-cognitive functional limitation and self-care functional limitation factors were 2.02 (SD = 0.65) and 1.55 (SD = 0.54), respectively. Internal consistency reliabilities (Cronbach’s alpha) for the social cognitive functioning and self-care functional limitation were calculated on the sample as a whole. Internal consistency of the socio-cognitive functional limitation, self-care functional limitation, and total WHODAS-Y were found to be .81, .77, and .85 respectively. The socio-cognitive functional limitation factor was negatively associated with stages of change (r = −.16, p < .01) and outcome expectancy (r = −.17, p < .001), and the self-care functional limitation factor was negatively associated with stages of change (r = −.13, p < .01) and outcome expectancy (r = −.20, p < .001). The total WHODAS-Y score was negatively associated with stages of change (r = −.16, p < .01) and outcome expectancy (r = −.21, p < .001). The total WHODAS-Y score was not associated with Medicaid outpatient treatment expenditures (r = −.131) but was negatively associated with total health care expenditure (r = −.15, p < .05). The socio-cognitive functional limitation factor was not associated with either outpatient treatment expenditures (r = −.002) or prescription expenditures (r = −.067). However, the self-care functional limitation factor was negatively associated with Medicaid outpatient treatment expenditures (r = −.23, p < .01) and total health care expenditure (r = −.22, p < .01) (Table 2).
Correlation.
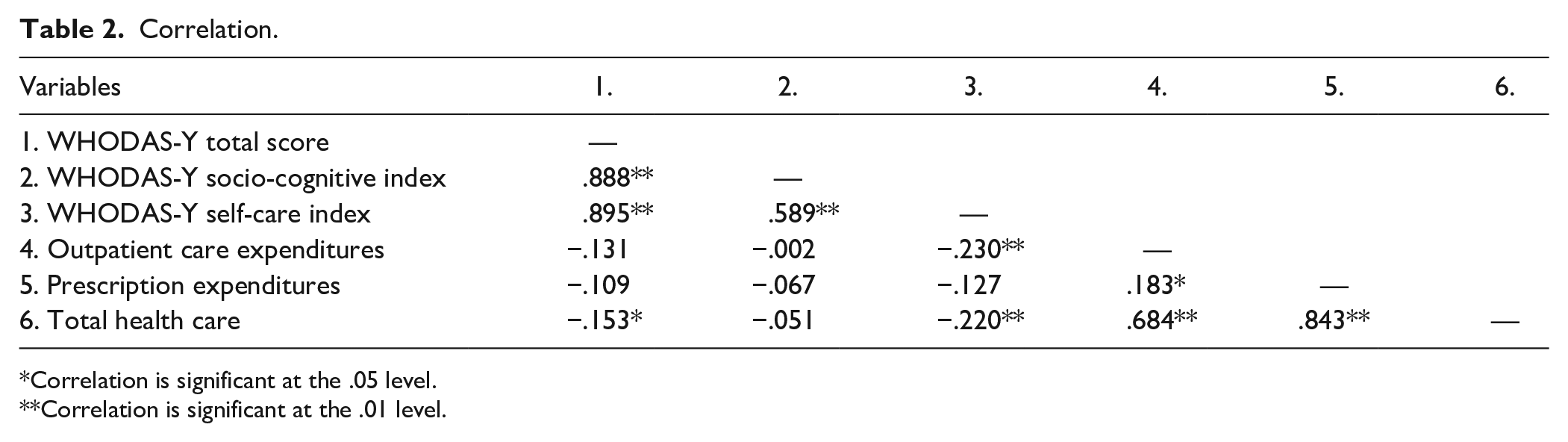
Correlation is significant at the .05 level.
Correlation is significant at the .01 level.
Discussion
The results of the study suggest that WHODAS-Y is a reliable and valid measure of functional impairment for transition-aged youth in a community setting. The development and validation of this measure was intended to provide VR service providers with a common metric to assess function in the context of planning transition services. It can assist VR agencies in the program planning, evaluation, and implementation of Pre-ETS services for transition-aged youth seeking employment or higher education by providing an objective, quantified measure of functional limitations of service recipients. Such a measure may also benefit researchers working with state VR programs by providing a reliable and valid assessment that can be incorporated into methodology aimed at identifying factors associated with employment outcomes (Tansey et al., 2017).
The WHODAS-Y measurement accounted for 55% of the variance and indicated a two-factor solution, which is a departure from hospital-based setting research but consistent with community-based samples (Kücükdeveci et al., 2013; Kulnik & Nikoletou, 2014; MacLeod et al., 2016). The two-factor solution produced two components consisting of five items in the socio-cognitive functional limitation category and six items in the self-care functional limitation category. These results indicate most functioning limitations due to disability fall into one of the two categories outlined by the factor analysis. Categorization can help with improving employment services such as job coaching, post-secondary education, and work experiences for transition-aged youth with disabilities.
The results from this study are consistent with other similar prior research conducted on the WHODAS 2.0 measurement (Andrews et al., 2009; Hu et al., 2012; Kimber et al., 2015). Tansey et al. (2017) also found that comparable results, revealing that functional disability as measured by WHODAS 2.0, were negatively associated with both outcome expectancy and stages of change, consistent with the current study. Results from both studies suggest that lower scores on the WHODAS measure are correlated with higher scores on outcome expectancy and stage-of-change scales. Higher scores on those scales point toward increases in VR engagement and readiness to work. Therefore, applied use of these scales may be helpful for understanding initial engagement and readiness to participate in employment-related services by transition-aged youth with disabilities.
A relationship between scores on the WHODAS-Y self-care functional limitations and Medicaid expenditures for outpatient treatment and for total health care expenditure was also observed. Specifically, as WHODAS-Y scores on the self-care factor increased, suggesting greater functional limitations, the expenditures in both areas were found to decrease. However, it should be noted that the responses on the WHODAS-Y represented a population that, in general, had limited concerns with personal self-care. As such, the inverse relationship between severity on the WHODAS-Y may be associated with a nonlinear distribution of expenditures. The exact nature of the distribution warrants further study with individuals without disabilities and those with signification functional limitations to fully appreciate the nature of the distribution. The WHODAS-Y, in particular, the self-care functional limitation factor, may have utility to inform decisions related to eligibility for VR services and to project future outlays for Medicaid outpatient treatment expenditures and prescription drug costs for youth with disabilities. As a quantifiable metric of the daily functioning of youth with disabilities, it may provide further clarity into the severity of disability for consideration by those states implementing an Order of Selection for services. Likewise, the potential of the WHODAS-Y to project health care expenditures may support efforts to model changes in health care based that incorporate patient characteristics into those analyses.
Limitations
There are some salient limitations that should be considered when interpreting this study’s results and generalizability. Participants were limited to youth receiving SSI and ages 14 to 16 years, so it may be difficult to generalize to the entire transition-age youth population. Also, less than half of the youth enrolled in WI PROMISE completed the baseline survey. Those who volunteered to take the survey were possibly more engaged in the PROMISE program, and their responses may have been skewed toward youth that were higher functioning and more involved in the transition process, so may not be completely representative of the population as a whole. Another limitation of the study was a limited number of gift cards were available through a drawing for survey completion. This opportunity was only available as an incentive during the last month the survey was open. The drawing was added as a method to increase the number of survey responses. The inclusion of 11 items on the WHODAS-Y is a limitation in that it limits the relatability of findings of this measure to other common measure of functional limitations such as the WHODAS-2.0 and the 12-item version of that scale. Furthermore, reducing the existing scale by one item may have led to the lower reliably coefficient compared with previous research. Finally, the survey was all self-report, so a possible opportunity for response bias may have been present.
Conclusion
In conclusion, the WHODAS-Y measurement seems to be a reliable and valid measure of function impairment in transition-age youth with disabilities receiving SSI in a community setting. The use of this measure may assist in identifying self-reported functional impairment toward using this information to identify needs related to education and employment-related services. Effective modeling of needs, barriers, and facilitators may increase the utility of employment for transition-age youth by identifying specific interventions that are most likely to facilitate transition to work and may inform VR agencies of the characteristics of this underserved population. For example, with those youth expressing relatively no self-care limitations, who may have higher overall health care expenditures than peers with modest impairments in this area, interventions such as health literacy training may be appropriate to minimize their utilization of tertiary care services and achieve greater awareness of their daily health and well-being. As an integrative approach, understanding and measuring clients’ functional limitations (or functioning), in conjunction with understanding clients’ strengths, abilities, and interests, would help VR counselors have a holistic case conceptualization, leading more successful rehabilitation outcomes. Likewise, this measure may also prove useful in understanding health care needs as observed by health care expenditures and potential interventions to improve overall health and function. However, further research is needed to determine if this measure can be applied effectively and efficiently as a tool to help monitor and improve services for youth with disabilities.
Footnotes
Acknowledgements
The views expressed herein do not necessarily represent the positions or policies of the Department of Education, the Wisconsin Department of Workforce Development, or their federal or state partners. No official endorsement by the U.S. Department of Education or the Wisconsin Department of Workforce Development of any product, commodity, service, or enterprise mentioned in this publication is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared the potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The views expressed in this paper do not necessarily represent the positions or policies of the Department of Education or its federal partners. No official endorsement by the U.S. Department of Education of any product, commodity, service or enterprise mentioned in this publication is intended or should be inferred.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this paper were developed under a cooperative agreement with the U.S. Department of Education, Office of Special Education Programs, associated with PROMISE Award #H418P140002. Selete Avoke served as the project officer.