
Abstract
Objective:
Mindfulness- and acceptance-based intervention (MABI) is an emerging evidenced-based practice, but no systematic review incorporating meta-analyses for MABIs in stroke survivors has been conducted. The objective of this systematic review was to measure the effectiveness of MABIs on outcomes in people with stroke.
Method:
Three electronic databases, including PubMed, CINAHL, and PsycINFO, were searched to identify relevant studies published in peer-reviewed journals. The methodological quality of the included studies was assessed. Data were extracted and combined in a meta-analysis with a random-effect model to compute the size of the intervention effect.
Results:
A total of 11 studies met the eligibility criteria. Meta-analyses found a small-to-moderate effect of MABIs on depressive symptoms (standardized mean difference [SMD] = 0.39, 95% confidence interval [CI] = [0.12, 0.66]) and a large effect on mental fatigue (SMD = 1.22, 95% CI = [0.57, 1.87]). No statistically significant effect of MABIs on anxiety, quality of life, and mindfulness was found, but there was a trend in favor of MABIs overall.
Conclusions:
This meta-analysis found positive effects of MABIs on depressive symptoms and mental fatigue in stroke survivors, but future high-quality studies are needed to guarantee treatment effects of MABIs on varied outcomes in stroke survivors.
Stroke is a leading cause of long-term disability, with more than 80 million stroke survivors worldwide and 7 million stroke survivors in the United States (Benjamin et al., 2019; Gorelick, 2019). As more people survive stroke with improvements in acute stroke care, risk factor management, and longevity, it is important to support stroke survivors to live well with consequences after stroke with good quality of life in the community (Lakshminarayan et al., 2014).
Studies have found the negative impact of stroke on overall quality of life, mental health, and participation in valued activities, such as greater levels of psychological distress (i.e., depression, anxiety, stress, and negative affect), mental fatigue, and lower levels of quality of life (Gyawali et al., 2020; Johansson & Rönnbäck, 2012; Ramos-Lima et al., 2018). For example, poststroke depression is common (e.g., rates ranged from 18% to 33% based on a recent review) and associated with lower quality of life, higher mortality, and lower recovery (Ayerbe et al., 2013; Medeiros et al., 2020). Mental fatigue, or “pronounced and rapid mental exhaustion even after moderate mental activity involving concentration and attention,” has a substantial impact on the ability to participate in daily life activities, such as social activities and work (Johansson et al., 2015, p. 227).
Accepting the loss of abilities after stroke and managing their own emotions by focusing on the present moment may help stroke survivors better adapt and maintain quality of life (Large et al., 2019; Lawrence et al., 2013). Lower levels of acceptance and mindfulness in stroke survivors have been found to be associated with the presence of symptoms of overall distress, anxiety, depression, and anger, and lower levels of physical and psychosocial quality of life (Shaffer et al., 2016; M. L. van Mierlo et al., 2015; M. van Mierlo et al., 2018). Acceptance is defined as being willing to experience unpleasant thoughts and emotions as they are without attempting to avoid or terminate them (Baer & Huss, 2008). Mindfulness is described as a moment-to-moment awareness of one’s experience in a nonjudgmental and accepting way (Baer & Krietemeyer, 2006). Uncertainty of the recovery process and future health, fear of recurrent strokes, and adjustment to life after stroke have been commonly reported by stroke survivors, which can lead to psychological distress (e.g., McCurley et al., 2019). Stroke survivors and their caregivers report interventions facilitating mindfulness and acceptance to be helpful to prevent and manage psychological distress, accept symptoms and a changed reality, and adjust to limitations after stroke (Large et al., 2019; McCurley et al., 2019).
Mindfulness- and acceptance-based interventions (MABIs) include mindfulness-based stress reduction (MBSR; Kabat-Zinn, 1990), mindfulness-based cognitive therapy (MBCT; Segal et al., 2002), acceptance and commitment therapy (ACT; Hayes et al., 1999), dialectical behavior therapy (DBT; Linehan, 1993), and other variations facilitating mindfulness (Baer & Krietemeyer, 2006). MBSR employs the formal practice of mindfulness meditation (e.g., body scan meditations, walking and seated mindfulness meditation practices, breathing meditations, and gentle yoga movement), typically involving 2.5-hr group therapy per week for 8 weeks with a 1-day retreat and homework assignments, to enhance moment-to-moment awareness of one’s experience in a nonjudgmental and accepting way and thus reduce negative affect and improve coping (Grossman et al., 2004; Kabat-Zinn, 1990). MBCT was adapted from MBSR, by combining elements of cognitive-behavioral therapy (e.g., understanding the association between thoughts and feelings) with MBSR to teach skills for disengaging from automatic dysfunctional thoughts and promoting behavior change strategies while practicing mindfulness (Segal et al., 2002; Williams et al., 2008). ACT aims to foster greater psychological flexibility, which is defined as the ability to face challenging experiences in an open, conscious manner and change one’s behaviors to participate in valued activities (Hayes et al., 2012). Metaphors, mindfulness exercises, cognitive defusion exercises (i.e., exercises to step back from unhelpful thoughts and emotions to reduce their dominance over behaviors), self-as-context exercises (i.e., observing thoughts and emotions without judgment), clarification of values, and action plans aligned with personal values are used in ACT (Hayes et al., 2012). DBT uses acceptance-oriented strategies (mindfulness and distress tolerance) and change-oriented strategies (emotion regulation and interpersonal effectiveness) aiming for the right balance in terms of acceptance and change (Linehan, 1993). DBT involves filling out diary cards to track emotions, urges, behaviors, and skills and skill coaching for acceptance-oriented strategies and change-oriented strategies, such as skills for effectively communicating with others to cope with inevitable interpersonal conflict and mindfulness skills (Linehan, 1993).
Although these MABIs can vary in terms of intervention duration and structure, all of these MABIs regard negative internal experiences (e.g., emotions, cognitions, and sensations) as a part of life (Baer & Huss, 2008). Accepting these uncomfortable internal experiences with mindfulness practice is suggested to be important to mental health rather than avoiding or suppressing them (Baer & Huss, 2008). As stroke survivors have challenges in managing psychological distress, accepting symptoms and a changed reality, and adjusting to limitation after stroke, MABIs, which promote accepting uncomfortable internal experiences with mindfulness practice, can be effective for enhancing mental health of stroke survivors (Large et al., 2019; McCurley et al., 2019). Studies have found effects of MABIs on reducing psychological distress (e.g., depressive symptoms and anxiety) and mental fatigue and improving quality of life among stroke survivors (e.g., Johansson et al., 2012; Majumdar & Morris, 2019).
Previous systematic reviews incorporating meta-analyses for MABIs have been conducted either for specific outcomes (e.g., smoking cessation and weight loss outcomes by Roche et al., 2019) or for specific populations, such as people with fibromyalgia in Haugmark et al.’s study (2019) and informal caregivers of people with dementia in Collins and Kishita’s study (2019). For example, a recent meta-analysis found moderate to large effects of MABIs on improving quality of life and decreasing symptoms of depression, anxiety, stress, and fatigue among people with multiple sclerosis (Han, 2021a, 2021b). Meta-analyses of MABIs in people with fibromyalgia showed moderate effects of MABIs on depressive symptoms, large effects on quality of life, and small effects of anxiety and mindfulness (Haugmark et al., 2019). To date, no systematic review incorporating meta-analyses for MABIs among stroke survivors has been conducted. This systematic review and meta-analysis, therefore, aimed to assess effects of MABIs on depressive symptoms, anxiety, quality of life, mental fatigue, and mindfulness in stroke survivors.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Liberati et al., 2009) and Cochrane handbook for systematic reviews of interventions version 5.1.0 (Higgins & Green, 2011) were used as a guide for conducting and reporting this systematic review and meta-analysis.
Search Strategy
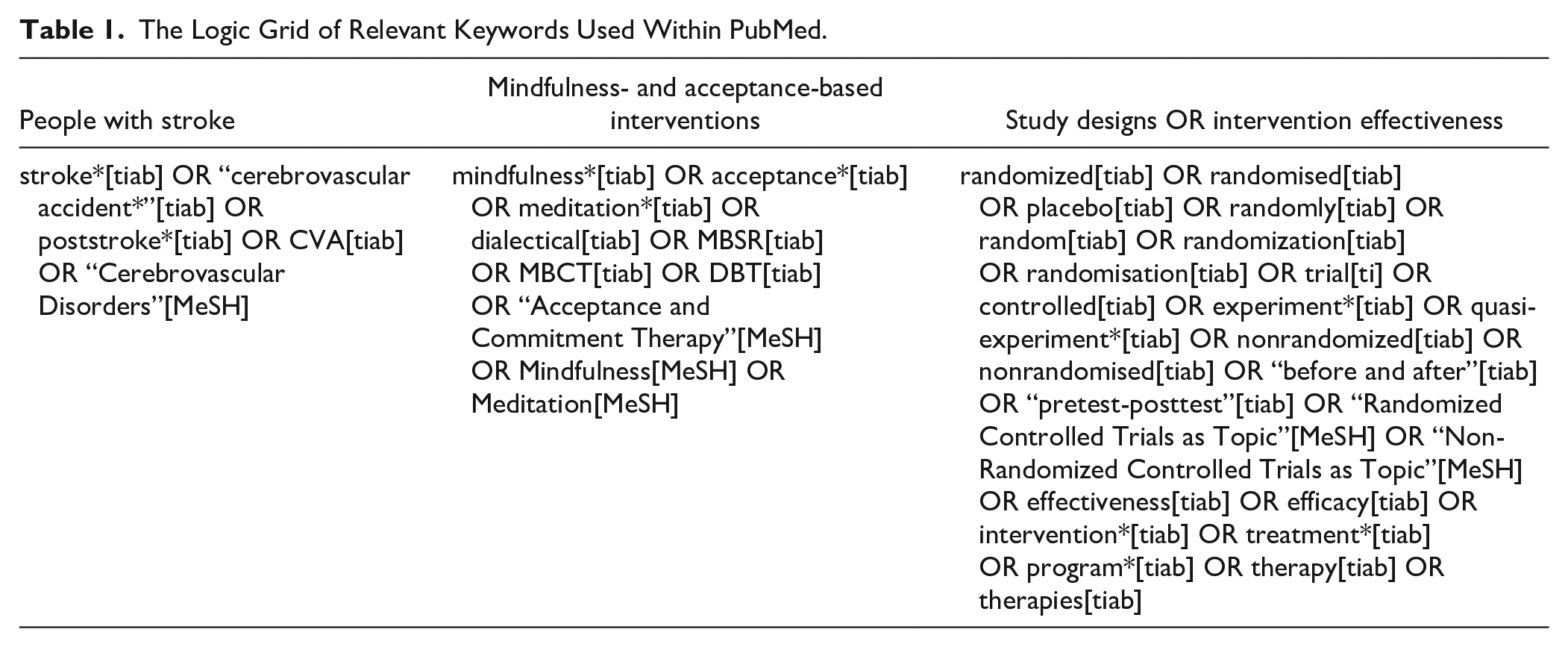
Relevant articles were identified by searching three electronic databases from the date of inception of each database to May 20, 2020, including PubMed (1966–2020), CINAHL (1981–2020), and PsycINFO (1935–2020). Key search terms were combined to identify the relevant literature around the subjects: Stroke, MABIs, and experimental research using randomized controlled trials (RCTs), and quasi-experimental designs to measure the intervention effectiveness. Keywords relevant to outcomes were not entered as search terms to broaden the search, so all the outcomes measured in the literature could be identified as much as possible. The logic grid of relevant keywords used within PubMed is presented as an example in Table 1.
The Logic Grid of Relevant Keywords Used Within PubMed.
Eligibility Criteria
Studies were selected based on the following inclusion criteria: (a) the study must be experimental research using RCTs and quasi-experimental designs (i.e., nonrandomized control group pretest–posttest design and one-group pretest–posttest design); (b) study participants must involve people with stroke regardless of types and severity of stroke; (c) MABIs must be provided to people with stroke; (d) the study must have reported pretest and posttest results in outcomes for people with stroke; and (e) the study must be written in English and published in a peer-reviewed journal article. Studies were excluded if the study: (a) investigated other meditation interventions with focus on exercises and physical activity, such as yoga, Qigong, and Tai Chi; (b) involved stroke survivors 50% less than the total study participants; (c) used self-developed surveys only as outcomes; and (d) the study had no reported data on outcomes for people with stroke.
Data Extraction and Quality Assessment
Characteristics of the included studies, such as the country of origin, participants, design, description of intervention and control groups, outcomes, and results, were extracted into a table. Reported means and standard deviations (SDs) at each data collection time point and sample sizes of intervention and control groups in the included studies were entered into an excel file. The methodological quality of each of the included studies was assessed using the Effective Public Health Practice Project Quality Assessment Tool (EPHPP) that can be used for studies with a variety of study designs (Thomas et al., 2004). EPHPP includes the following components: (a) selection bias; (b) study design; (c) confounders; (d) blinding; (e) data collection methods; and (f) withdrawals and dropouts. Each component is rated as strong, moderate, or weak. The global rating is strong if there is no weak rating in all components, moderate if there is one weak rating, or weak if there are two or more weak ratings. Studies support that EPHPP shows content and construct validity, excellent inter-rater reliability for the global rating (the intraclass correlation coefficient: 0.77), and fair interrater reliability for the individual component (Cohen’s Kappa: 0.60) (Armijo-Olivo et al., 2012; Thomas et al., 2004).
Meta-Analysis
Reported means, SDs, and sample sizes of intervention and control groups in the included studies were entered into RevMan version 5.3 for meta-analyses and pooled for each of the outcomes. When multiple posttreatment data (e.g., follow-ups at multiple data collection time points) were reported, the immediate posttest data or primary end-point data were used. Authors of the included studies were contacted when the studies did not report the means and standard deviations of groups at each of the data collection time points. Studies were not able to be used in meta-analysis if authors did not respond to the request of data. The I² statistic was used to measure statistical heterogeneity across studies, and I² of 30% to 60% and greater than 60% were interpreted as moderate heterogeneity and substantial heterogeneity, respectively. Either a random-effect model or fixed-effect model with the inverse variance method was used depending on I² for each outcome. The standardized mean difference (SMD) with 95% confidence intervals (CIs) was used as a summary statistic for the size of the intervention effect to account for outcomes measured using difference assessment tools (Higgins & Green, 2011). SMDs lower than 0.4 indicate a small effect, SMDs between 0.4 and 0.7 indicate a moderate effect, and SMDs higher than 0.7 indicate a large effect (Higgins & Green, 2011).
Quasi-experimental studies as well as RCTs were included in meta-analysis. Studies suggest advantages of including quasi-experimental studies in meta-analysis by providing new evidence of improvements in outcomes and finding similar effect estimates among RCTs and quasi-experimental studies (Arditi et al., 2016; Shrier et al., 2007). A separate meta-analysis depending on the existence of a control group (i.e., RCTs vs. one-group pretest–posttest design studies) was conducted in each outcome by following guidance on synthesizing results separately (Valentine & Thompson, 2013). Baseline data were regarded as data for the control group when calculating SMDs of one-group pretest–posttest design studies (Arditi et al., 2016).
Results
Selection of Studies
Figure 1 describes the study selection process. A total of 743 articles were identified through database searching. After removing 219 duplicates, 524 articles were screened based on title and abstract screening. A total of 510 articles were excluded based on title and abstract screening, and 14 articles were assessed for eligibility by reading the full text. Three articles were excluded after reading the full text due to the following reasons: employing a case study design; not reporting outcomes regarding the effects of the intervention; and involving only one participant with stroke among seven participants. A total of 11 studies met the eligibility criteria.
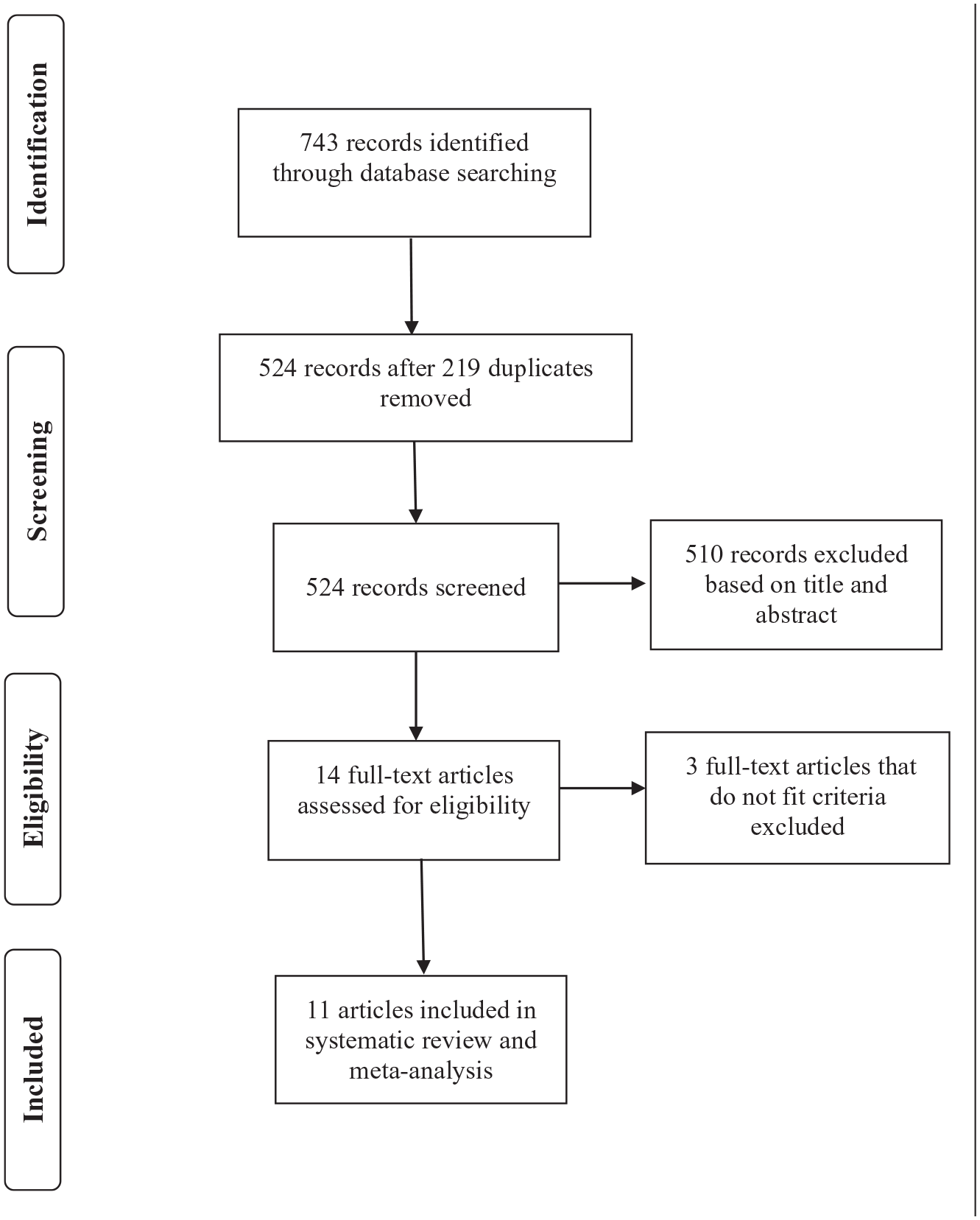
PRISMA flow diagram of study selection process.
Characteristics of the Included Studies
The main characteristics of the 11 included studies are summarized in Table 2. The included studies measured effects of MABIs as RCTs (n = 4), nonrandomized control group pretest–posttest design studies (n = 2), and one group of pretest–posttest design studies (n = 5). MABIs in the included studies involved MBSR (n = 3), MBCT (n = 2), ACT (n = 2), and other mindfulness-based trainings (n = 4). The average sample size for participants in the 11 included studies was 39, ranging from 8 to 134. The mean age of participants was 57.4 years, ranging from 47.4 years to 64 years (SD = 5.5), and the average percentage of male participants was 59.9%, ranging from 35.7% to 90% (SD =16.9). Of the 11 studies, five studies involved stroke patients in inpatient care settings. Type and severity of stroke were not specific inclusion or exclusion criteria in all the included studies except for three studies (i.e., Baylan et al., 2020; X. Wang et al., 2020; Wathugala et al., 2019). The included studies were largely of western origin, including United States (n = 3), United Kingdom (n = 2), Sweden (n = 2), China (n = 2), Switzerland (n = 1), and Indonesia (n = 1). Of the 11 studies, eight studies were published between 2018 and 2020 and three studies were published between 2012 and 2015.
Characteristics of the Included Studies.
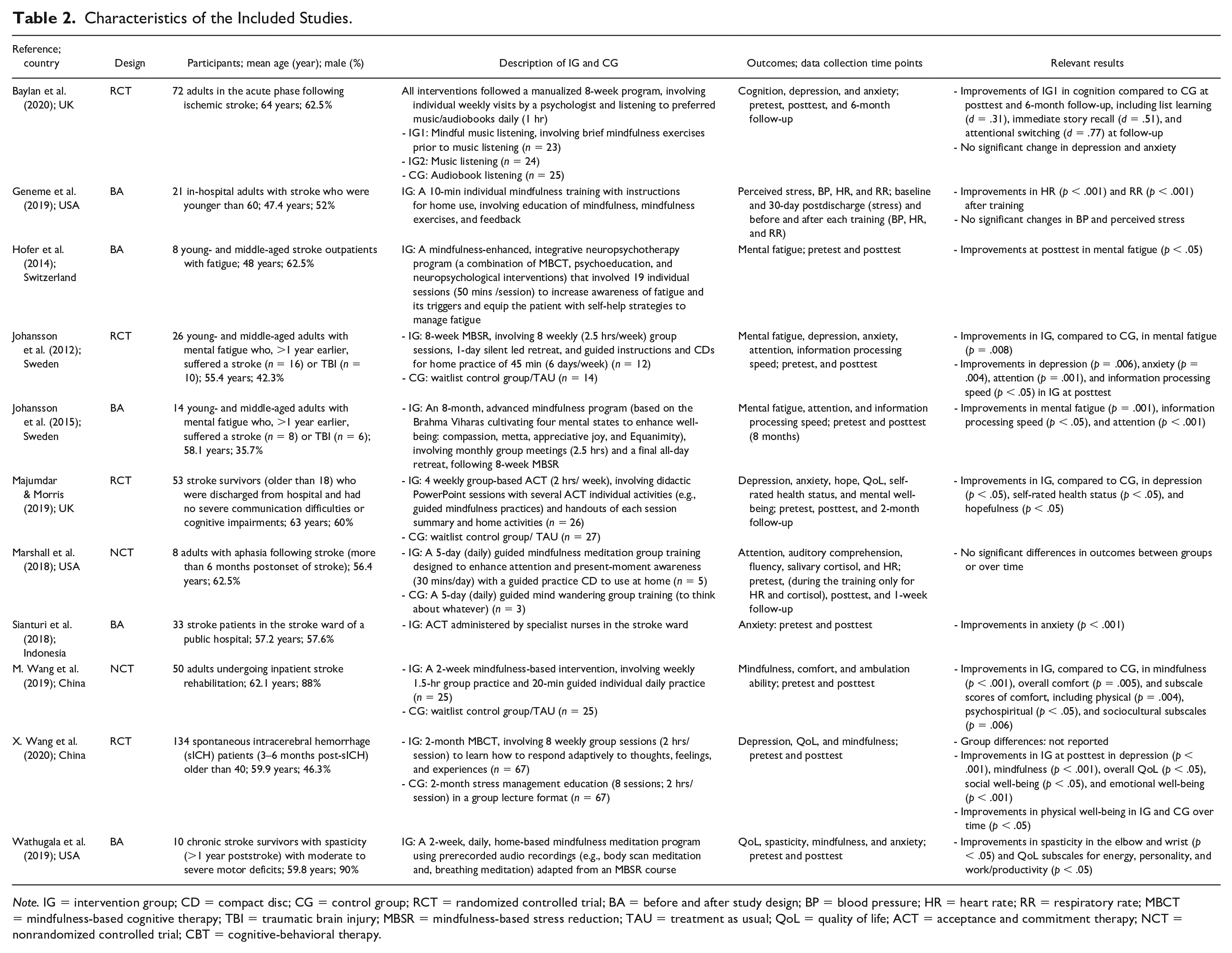
Note. IG = intervention group; CD = compact disc; CG = control group; RCT = randomized controlled trial; BA = before and after study design; BP = blood pressure; HR = heart rate; RR = respiratory rate; MBCT = mindfulness-based cognitive therapy; TBI = traumatic brain injury; MBSR = mindfulness-based stress reduction; TAU = treatment as usual; QoL = quality of life; ACT = acceptance and commitment therapy; NCT = nonrandomized controlled trial; CBT = cognitive-behavioral therapy.
The following section describes results of meta-analyses regarding effects of MABIs on depressive symptoms, mental fatigue, anxiety, quality of life, and mindfulness in people with stroke and synthesized findings in terms of characteristics of the interventions for each outcome.
Effects of MABIs on Depressive Symptoms
A meta-analysis of 3 RCTs (N = 213 participants) revealed a small-to-moderate effect of MABIs on depressive symptoms compared to control groups (SMD = 0.39, 95% CI = [0.12, 0.66]; see Figure 2). The included three RCTs tested the effects of MABI groups on depressive symptoms, compared to either a treatment as usual control group (Johansson et al., 2012; Majumdar & Morris, 2019) or an attention control group providing stress management education (X. Wang et al., 2020). MABIs in the included studies involved 8 weekly group-based MBSR sessions (2.5 hrs/session) with a 1-day retreat in Johansson et al. (2012); 4 weekly group-based ACT sessions (2.5 hrs/session) in Majumdar and Morris (2019) and 8 weekly group-based MBCT sessions (2 hrs/session) in X. Wang et al. (2020). Two studies involved group sessions accompanied by home practice, by providing guided instructions and CDs for 45-min home practice for 6 days per week in Johansson et al. (2012) and handouts of home activities in Majumdar and Morris (2019). Depression was measured using self-reported questionnaires, including the Comprehensive Psychopathological Rating Scale (CPRS; Svanborg & Asberg, 1994) by Johansson et al. (2012), the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) by Majumdar and Morris (2019), and the Center for Epidemiological Studies—Depression Scale (CES-D; Radloff, 1977) by X. Wang et al. (2020).
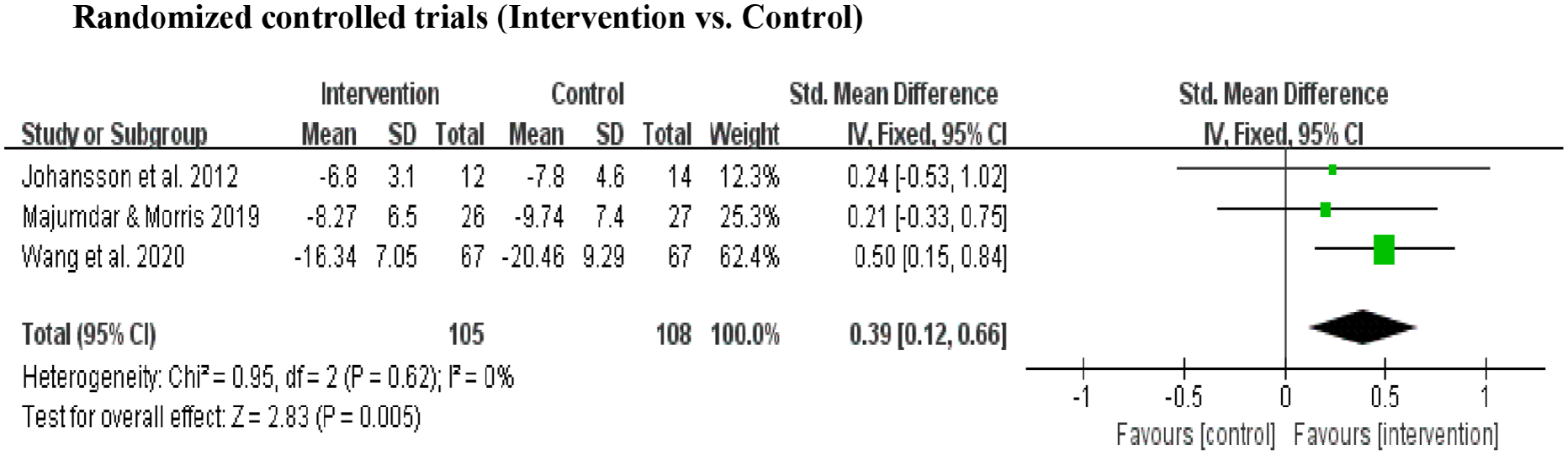
A forest plot showing effects of MABIs on depressive symptoms of people with stroke.
Effects of MABIs on Mental Fatigue
A meta-analysis of 2 one-group pretest–posttest design studies (N = 22 participants) found a large effect of MABIs on mental fatigue at posttest compared to pretest (SMD = 1.22, 95% CI = [0.57, 1.87]; see Figure 3). MABIs in the included studies involved: a monthly group-based, advanced mindfulness program that involved eight sessions (2.5 hrs/session) to enhance well-being with a 1-day retreat following 8-week MBSR by Johansson et al. (2015); and a mindfulness-enhanced program that involved individual 19 sessions (50 min/session) of a combination of MBCT, psychoeducation, and neuropsychological interventions to increase awareness of fatigue and its triggers and equip the individual with self-help strategies to manage fatigue in Hofer et al. (2014). Mental fatigue was measured using the Mental Fatigue Scale (MFS; Johansson et al., 2010) in both studies, which is a multidimensional self-reported questionnaire involving affective, cognitive, and sensory symptoms, duration of sleep and day-time variation.
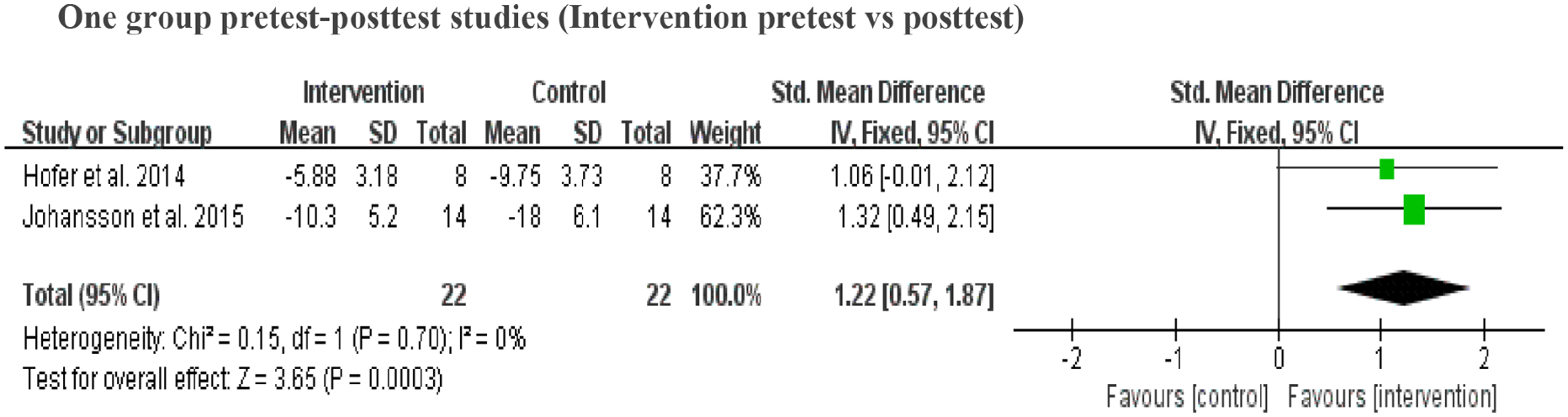
A forest plot showing effects of MABIs on mental fatigue of people with stroke.
Effects of MABIs on Anxiety
The effects of MABIs on anxiety were measured in 2 RCTs (N = 79 participants) and two one-group pretest–posttest design studies (N = 43 participants). A meta-analysis of the two RCTs (Johansson et al., 2012; Majumdar & Morris, 2019) found that the overall effect of MABIs on anxiety was not statistically significant compared to treatment as usual control groups (SMD = 0.07, 95% CI = [−0.37, 0.51]; see Figure 4). Also, a meta-analysis of the two one-group pretest–posttest design studies (Sianturi et al., 2018; Wathugala et al., 2019) found no statistically significant effect of MABIs on anxiety (SMD = 0.85, 95% CI = [−0.48, 2.17]; see Figure 4).
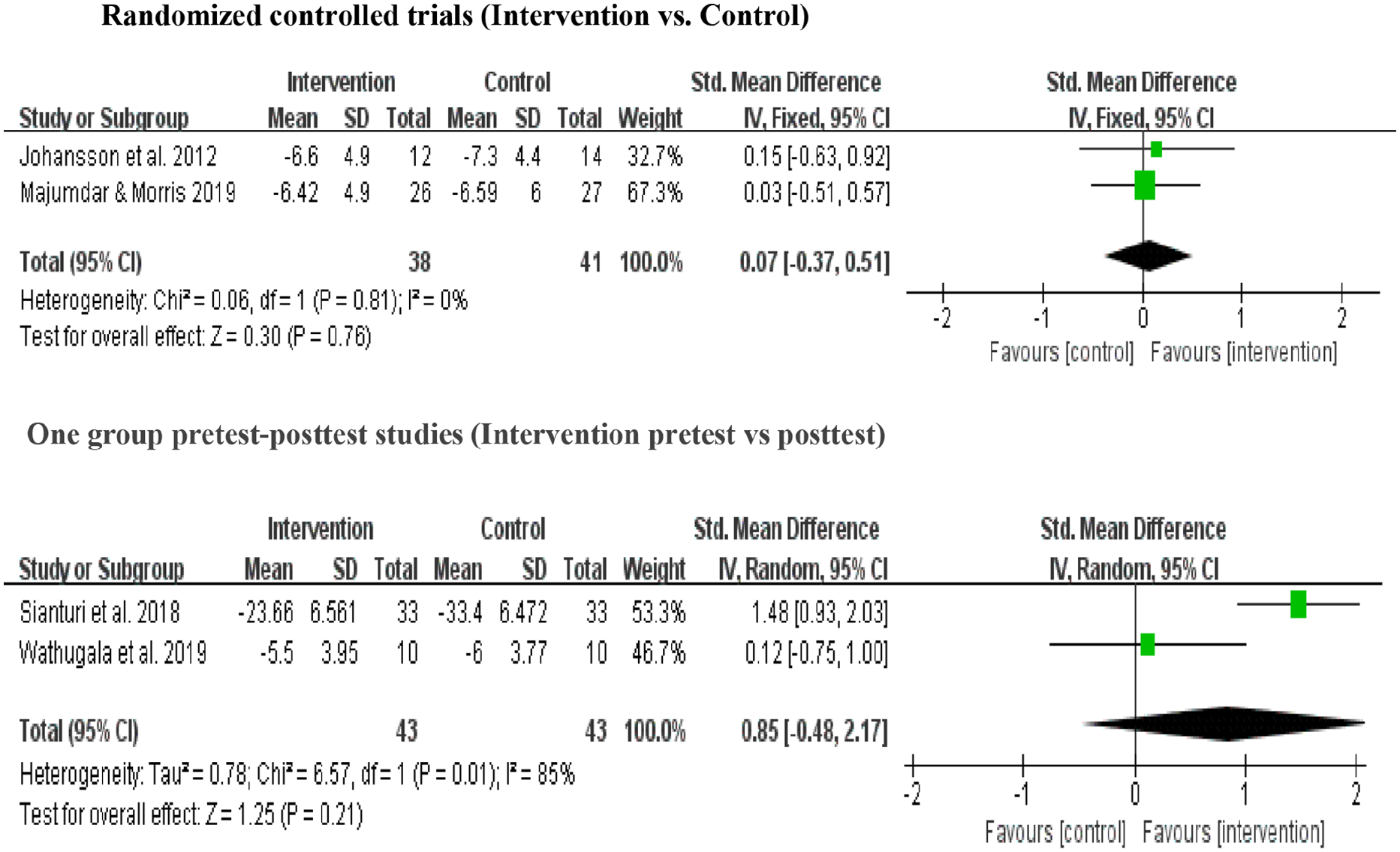
Forest plots showing effects of MABIs on anxiety of people with stroke.
MABIs in the included studies were 8 weekly group-based MBSR sessions (2.5 hrs/session) by Johansson et al. (2012); 4 weekly group-based ACT sessions (2.5 hrs /session) by Majumdar and Morris (2019); ACT administered by specialist nurses in the stroke ward in Sianturi et al. (2018); and adapted MBSR involving 2-week, daily, home-based mindfulness meditation program using prerecorded audio recordings by Wathugala et al. (2019). Anxiety was measured using self-reported questionnaires, including the CPRS (Svanborg & Asberg, 1994) by Johansson et al. (2012), Generalized Anxiety Disorder (GAD)-7 (Spitzer et al., 2006) in Majumdar and Morris (2019), Hamilton Anxiety Rating Scale (HARS; Hamilton, 1959) by Sianturi et al. (2018), and Hospital Anxiety and Depression Scale (HADS)—Anxiety (Zigmond & Snaith, 1983) by Wathugala et al. (2019).
Effects of MABIs on Quality of Life and Mindfulness
A meta-analysis of two RCTs (N = 187 participants) revealed that the overall effect of MABIs on quality of life was not statistically significant compared to control groups (SMD = 0.12, 95% CI = [−0.17, 0.41]; see Figure 5). The included two RCTs tested the effects of MABIs on quality of life compared to either a treatment as usual control group (Majumdar & Morris, 2019) or an attention control group providing stress management education (X. Wang et al., 2020). MABIs in the included studies involved 4 weekly group-based ACT sessions (2.5 hrs/session) by Majumdar and Morris (2019) and 8 weekly group-based MBCT sessions (2 hrs/session) by X. Wang et al. (2020). Quality of life was measured using self-reported questionnaires, including the EQ-5D-5L (Herdman et al., 2011) involving mobility, self-care, usual activities, pain/discomfort, and anxiety/depression by Majumdar and Morris (2019) and the Functional Assessment of Cancer Therapy-brain (FACT-Br; Weitzner et al., 1995) involving physical well-being, social well-being, emotional well-being, functional well-being, and concerns that correspond to patients with brain tumors by X. Wang et al. (2020).
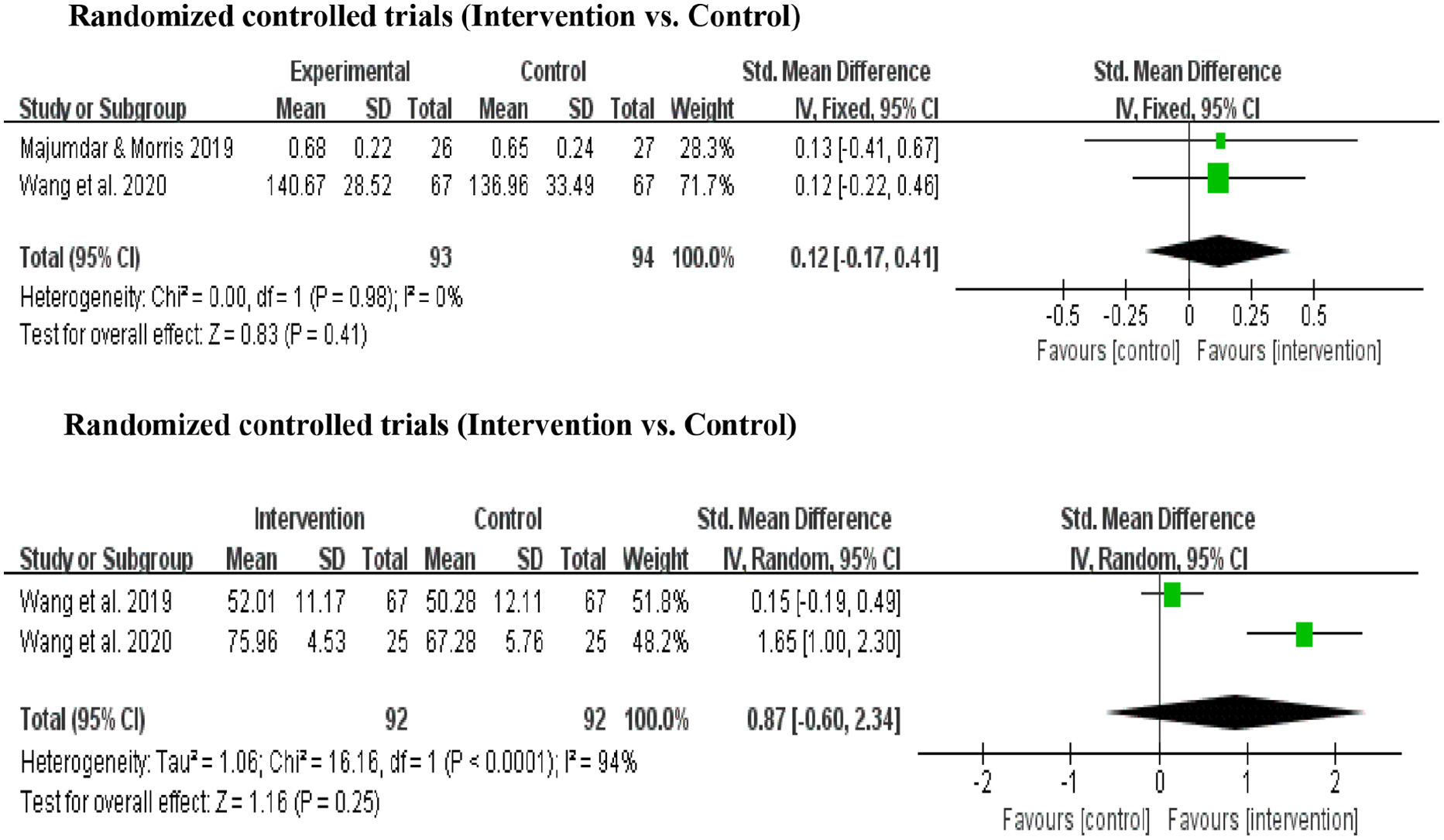
Forest plots showing effects of MABIs on quality of life and mindfulness of people with stroke.
A meta-analysis of two studies with a control group (N = 184 participants), including one RCT and one nonrandomized control group pretest–posttest design study, found no statistically significant effect of MABIs on mindfulness compared to control groups (SMD = 0.87, 95% CI = [−0.60, 2.34]; see Figure 5). The included studies measured the effects of MABIs on mindfulness compared to either a treatment as usual control group (M. Wang et al., 2019) or an attention control group providing stress management education (X. Wang et al., 2020). MABIs in the included studies were 2 weekly mindfulness training sessions (1.5-hr group practice with guided individual daily practice for 20 min) by M. Wang et al. (2019); and 8 weekly group-based MBCT sessions (2 hrs/session) by X. Wang et al. (2020). Mindfulness was measured using the Mindful Attention Awareness Scale (MAAS; Brown & Ryan, 2003) in both studies, which is a self-reported questionnaire assessing mindful attention toward the present moment.
Quality Assessment of the Included Studies
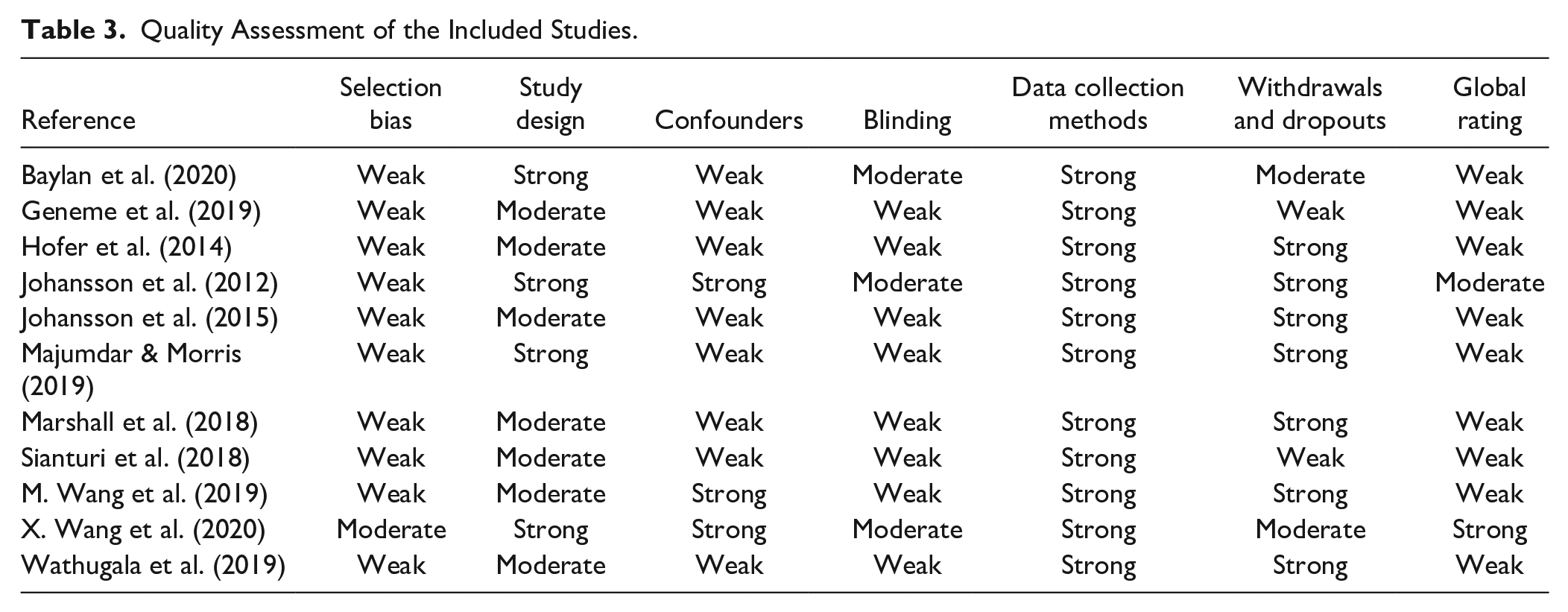
Of the 11 included studies, 9 studies were rated as weak (i.e., two or more weak ratings), 1 as moderate (i.e., 1-weak rating), and 1 as strong (no weak rating in all components) using EPHPP (see Table 3). In particular, the majority of the studies (90.9%; 10 studies out of 11) had a weak rating in the selection bias component (i.e., if participants were self-referred), and there was no study with a strong rating (i.e., if participants were randomly selected from a comprehensive list of individuals in the target population). All the included studies were rated as strong in the data collection methods component as this study included studies using measures with psychometric properties tested or reported.
Quality Assessment of the Included Studies.
Discussion
This systematic review identified 11 studies that assessed the effects of MABIs on outcomes in people with stroke. Meta-analyses found a large effect of MABIs on mental fatigue and a small-to-moderate effect on depressive symptoms. Findings of previous meta-analysis papers for the other populations (e.g., people with fibromyalgia and people with multiple sclerosis) support these findings of this paper to some extent with potential to show more positive outcomes with further research in stroke populations. For example, meta-analyses of MABIs in people with fibromyalgia showed moderate effects of MABIs on depressive symptoms, large effects on quality of life, and small effects of anxiety and mindfulness (Haugmark et al., 2019). Recent meta-analyses found moderate to large effects of MABIs on improving quality of life and decreasing symptoms of depression, anxiety, stress, and fatigue among people with multiple sclerosis (Han, 2021a, 2021b). Depressive symptoms and mental fatigue are common in stroke survivors, which could contribute to lower levels of quality of life, overall mental health, and activity participation (Kim et al., 2018; Naess et al., 2012; Tse et al., 2019). Studies suggest mindfulness meditation training to be helpful in decreasing depressive symptoms, improving attention, and coping with stressful situations better that could save mental energy, explaining why depressive symptoms and mental fatigue could be reduced with MABIs (Haugmark et al., 2019; Johansson et al., 2012; Kilpatrick et al., 2011). No statistically significant effect of MABIs on anxiety, quality of life, and mindfulness was found in this meta-analysis for stroke survivors. Relatively fewer studies with smaller sample sizes were included in these meta-analyses, indicating more studies are needed to assess effects of MABIs on stroke survivors. When considering MABIs as a newly emerging evidence-based practice and found treatment effects in other populations, such findings are promising.
Effects of MABIs on outcomes in stroke survivors might increase if the studies were designed to target specific outcomes. The included studies for the meta-analysis in depressive symptoms (Johansson et al., 2012; Majumdar & Morris, 2019; X. Wang et al., 2020) did not directly target stroke survivors with depressive symptoms. Participants in these included studies had mild depressive symptoms on average. Effects of MABIs on depressive symptoms might increase if the interventions were designed for people with moderate to severe depressive symptoms and the studies recruited such participants. The included studies for the meta-analysis in mental fatigue directly targeted stroke survivors who had been suffering from pathological mental fatigue for at least 1 year before study participation, showing significant large pretest–posttest changes (SMD = 1.32, 95% CI = [0.49, 2.15]; see Figure 3). Such findings indicate that meta-analyses of the included studies in the other outcomes (i.e., anxiety, quality of life, and mindfulness) might show statistically significant effects of MABIs if the studies were designed for stroke survivors who had specific challenges in those outcomes.
The included studies of this review were similar to those of previous reviews for other populations in terms of type of MABIs. Two previous reviews involved MBSR more than the other types of MABIs (e.g., four studies involving MBSR out of nine included studies by Haugmark et al., 2019 and six studies involving MBSR out of 12 included studies by Collins & Kishita, 2019). Similar to the included studies of this review, duration of interventions varied and adapted versions of MABIs often were used in the included studies of previous reviews for other populations (Collins & Kishita, 2019).
All of the 11 included studies except for one study involved MABIs only. A mindfulness-enhanced program was used by combining MBCT with psychoeducation and neuropsychological interventions to increase awareness of fatigue and its triggers and equip the individual with self-help strategies to manage fatigue by Hofer et al. (2014). Further studies are needed to examine differences in treatment effects among MABIs only and multicomponent interventions including MABIs in different outcomes for stroke survivors. Subgroup analyses, then, can be conducted to see if MABIs alone can show the same treatment effects compared to multicomponent interventions including MABIs. Also, this study was not able to conduct subgroup analyses to see whether effects of MABIs differ according to treatment features (e.g., types and duration of MABIs) due to the limited number of studies under each outcome. A future meta-analysis with such subgroup analyses can be conducted as more studies using MABIs for stroke survivors are conducted.
Limitations
Limitations of this review should be considered when interpreting the findings. This study did not exclude the studies based on treatment fidelity, so some of the included studies might not guarantee if the treatment was conducted consistently and reliably. Meta-analyses were conducted using the immediate posttest data or primary end-point data only as the majority of the included studies were not designed to measure if treatment effects were maintained over time. One author searched the literature, lacking the use of two independent reviewers in the search process. A recent methodological systematic review found that single screening for study selection in systematic reviews conducted by experienced reviewers had no impact on the findings of the meta-analyses (Waffenschmidt et al., 2019). The author of this article, who conducted the search, had extensive experiences in comprehensive literature searches for systematic reviews and meta-analysis and expertise in MABIs, including meta-analyses regarding effects of MABIs on people with multiple sclerosis (Han, 2021a, 2021b). Three electronic databases (i.e., PubMed, CINAHL, and PsycINFO) were used to search the literature, possibly missing some articles if these articles were published in the other databases only (e.g., EMBASE and Cochrane Central Register of Controlled Trials). Only published studies in peer-reviewed journals written in English were searched and included in this review, leading to publication bias. All of the 11 included studies were not used for meta-analysis due to the limited number of studies to run meta-analyses on a specific outcome (e.g., perceived stress assessed only by Geneme et al., 2019). Two studies are suggested to be a sufficient number to perform a meta-analysis (Higgins & Green, 2011). However, involving more studies with the increased sample size will increase the power to detect a treatment effect, indicating the need of more studies measuring effects of MABIs on stroke survivors.
Clinical Implications
Although this meta-analysis study showed promising results, there is insufficient evidence to determine whether or not practitioners should be routinely providing MABIs to stroke survivors due to the lack of studies. It is recommended that MABIs be provided selectively based on professional judgment and client preferences. For example, practitioners may consider providing their clients after stroke with 8 weekly group-based MBCT sessions (X. Wang et al., 2020) to help their clients reduce depressive symptoms and improve mindfulness. Also, practitioners may consider embedding practice of simple mindfulness meditation (e.g., body scan meditations, seated mindfulness meditation practices, mindful eating, and breathing meditations) within their therapy sessions because such mindfulness meditation can be practiced within 3 to 5 min and embedded easily into daily lives of stroke survivors.
Conclusions
This was the first systematic review incorporating meta-analysis to measure the effects of MABIs on stroke survivors. Meta-analyses found a large effect of MABIs on mental fatigue and a small-to-moderate effect on depressive symptoms. Of the 11 included studies, the quality of nine studies were rated as weak. Relatively fewer studies with smaller sample sizes were included in these meta-analyses, indicating more studies are needed to assess the effects of MABIs on stroke survivors. Future studies may consider designing interventions for specific outcomes (e.g., MABIs for stroke survivors with anxiety). Future high-quality studies with follow-up evaluations are needed to measure treatment effects of MABIs on varied outcomes among stroke survivors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.