
Abstract
The purpose of this study was to examine the relationship of the 24 character strengths in Peterson and Seligman’s character strengths model with the 4 value changes in Beatrice Wright’s theory of disability acceptance. Two hundred seventy-four individuals with disabilities completed an online survey. SPSS was used to conduct four regression analyses—one for each of the four subscales of the Multidimensional Acceptance of Loss Scale (MALS). The 24 character strengths, which were measured by the Values in Action Inventory—72 (VIA-72), were entered in one block as predictors of each of the value changes associated with disability acceptance. Collectively, the 24 character strengths significantly predicted each of the 4 value changes in Wright’s theory, as measured by the MALS. Many of the individual character strengths were significantly associated with the value changes. Therefore, character strengths appear to enhance disability acceptance in people living with disabilities. The results provide support for the development of character strengths interventions for people with disabilities.
Individuals who experience chronic illness or disability (CID) face a complex and often challenging process of psychosocial adaptation (Smedema et al., 2022). This adaptation process involves not only adjusting to functional limitations but also integrating the disability into one’s life, identity, self-concept, and body image. As individuals learn to navigate the changes brought on by disability, they must come to terms with a new reality—one that demands shifts in personal values and self-perception. This process is critical, as how individuals accept their disabilities can profoundly impact their psychological well-being, quality of life (QOL), and overall ability to thrive in social, professional, and personal contexts. Psychosocial adaptation to CID is not a linear or uniform experience; rather, it is a deeply personal journey that varies depending on the nature of the disability, the individual’s psychological resources, and the support systems in place. Central to this journey is the concept of acceptance of disability.
Acceptance of Disability
The seminal work of Beatrice Wright (1983) on acceptance of disability centers on how an individual incorporates a disability into their self-concept through underlying changes in their value system. Her model identifies four shifts in values that reflect disability acceptance. The first is Enlargement of the Scope of Values, or one’s ability to recognize areas of life unaffected by the disability and to appreciate values beyond the physical limitations imposed by the condition. This broadening of perspective is essential for people to reclaim a sense of self-worth that is not tied solely to physical function. Next, Subordination of the Physique involves shifting one’s focus from the physical body to other aspects of identity (e.g., personality traits, cognitive abilities, interpersonal relationships). This process helps individuals to de-emphasize physical appearance or ability as the sole determinants of their value, thereby fostering a more holistic sense of self. The third shift is Containment of the Effects of the Disability, which refers to limiting the impact of the disability to the specific areas affected by the physical or functional limitation. By containing these effects, an individual prevents the disability from negatively influencing other areas of their life, such as personal relationships or work, thereby allowing for more positive emotional and psychological outcomes. Finally, within Transformation of Comparative Status Values into Asset Values, one’s unique strengths are emphasized, rather than comparing oneself unfavorably to others. This shift involves reframing the way individuals evaluate themselves, not through comparison with societal standards of “normality,” but by recognizing and valuing intrinsic attributes that contribute to a positive self-concept.
Research shows that disability acceptance is strongly associated with positive psychosocial outcomes in people with disabilities (Li & Moore, 1998). For instance, higher levels of disability acceptance have been linked to enhanced well-being among individuals with epilepsy (Ogawa et al., 2021), spinal cord injury (Smedema et al., 2010), traumatic brain injury (TBI; Yehene et al., 2020), and multiple sclerosis (MS; Wilski et al., 2019). Moreover, disability acceptance has been shown to mediate the relationship between general self-efficacy and QOL in people with traumatic brain injury (Yehene et al., 2020), suggesting that individuals with higher self-efficacy are more likely to accept their disabilities and, in turn, report better overall outcomes. Therefore, disability acceptance serves as both an outcome of psychosocial adaptation and a predictor of improved QOL, making it an important focus of rehabilitation efforts.
It is important to recognize that the process of disability acceptance may differ depending on whether an individual has a congenital disability (present from birth) or an acquired disability (occurring later in life). Individuals with congenital disabilities, such as cerebral palsy or spina bifida, typically develop their self-concept and coping strategies within the context of their disability from an early age, often leading to a more integrated sense of identity that does not require a distinct process of adjustment (Li & Moore, 1998). In contrast, individuals with acquired disabilities, including both sudden-onset disabilities (e.g., spinal cord injury, traumatic brain injury) and progressive conditions (e.g., multiple sclerosis, muscular dystrophy), must navigate a more involved adaptation process where the disability is integrated into the individual’s sense of self (Livneh & Antonak, 2005). These differences suggest that the process of disability acceptance may be more complex for those with acquired disabilities, as they must reconcile their pre-disability identity with their post-disability reality. Thus, while the fundamental principles of Wright’s (1983) model apply across disability types, the specific pathways to acceptance may vary depending on when and how a disability manifests. Recognizing these distinctions is crucial for tailoring interventions that support disability acceptance in ways that align with an individual’s lived experience. One method of improving acceptance of disability that is worthy of consideration by rehabilitation researchers and practitioners is the concept of character strengths.
Character Strengths
Character strengths are positive traits reflected in thoughts, feelings, and behaviors that contribute to optimal functioning and well-being. Linley and Harrington (2006) describe strengths as capacities for action that enable individuals to function optimally and achieve valued life outcomes. Unlike talents, which may be innate, character strengths are considered malleable and can be developed through conscious effort, making them important targets for intervention, particularly among individuals facing significant challenges such as living with a disability.
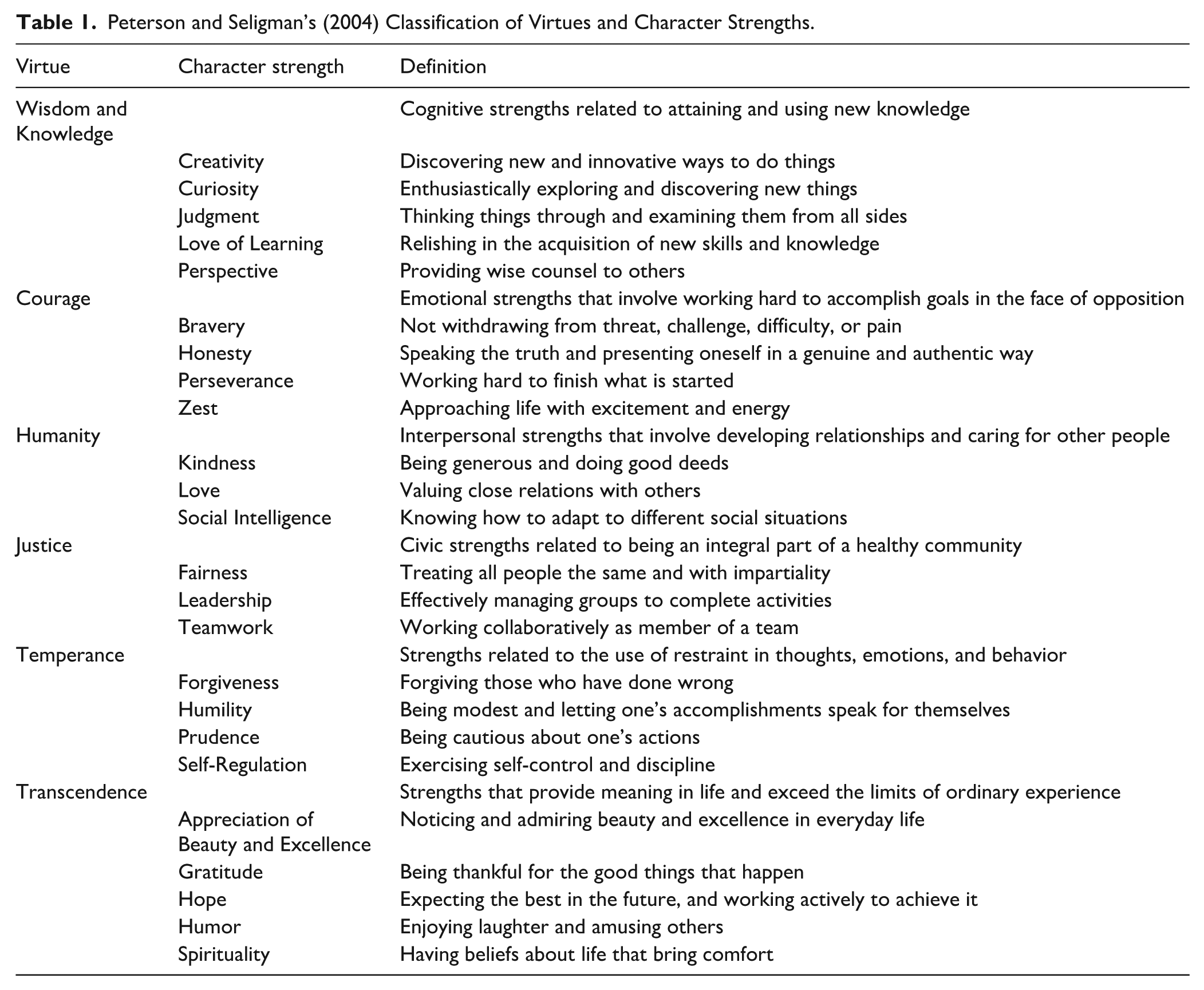
One of the most influential frameworks for understanding character strengths is the Values in Action (VIA) Classification proposed by Peterson and Seligman (2004). This classification system organizes 24 character strengths under six broad virtues that are foundational across cultures and philosophies. The virtues represent overarching qualities, while the 24 character strengths are specific pathways through which individuals can express these virtues in their lives:
Wisdom and knowledge involve cognitive strengths such as creativity, curiosity, and judgment, all of which are related to the acquisition and application of knowledge.
Courage includes emotional strengths like bravery, perseverance, and honesty, which allow individuals to pursue goals in the face of adversity.
Humanity encompasses interpersonal strengths such as kindness, love, and social intelligence, all of which enhance relationships and the capacity for compassion.
Justice refers to strengths that support social fairness, such as teamwork, fairness, and leadership, which are essential for building healthy communities.
Temperance involves traits like forgiveness, humility, and self-regulation, which help individuals manage their impulses and avoid excess.
Transcendence includes strengths that foster connections to the broader universe, such as appreciation of beauty, gratitude, and spirituality, providing meaning and purpose in life.
More details about the individual character strengths in the model can be found in Table 1.
Peterson and Seligman’s (2004) Classification of Virtues and Character Strengths.
The VIA Classification system allows individuals to identify and cultivate their own unique strengths, which in turn enhance their capacity for achieving well-being, resilience, and life satisfaction. In a study conducted by N. S. Park et al. (2006), the most commonly endorsed strengths among 83,576 Americans were kindness, fairness, honesty, gratitude, and judgment. Less frequently endorsed strengths included self-regulation, humility, prudence, zest, and spirituality. Research has shown that certain character strengths are more closely associated with life satisfaction and well-being than others. For example, N. S. Park et al. (2004) found that hope, zest, love, gratitude, and curiosity were the strengths most strongly correlated with life satisfaction in the general population.
While research on character strengths in the context of disability is still emerging, studies suggest that strengths can play a significant role in helping individuals with disabilities navigate challenges and maintain well-being. Using an international dataset from the VIA Institute on Character, Umucu et al. (2022) found that the most commonly endorsed character strengths among people with disabilities include love of learning, honesty, appreciation of beauty and excellence, kindness, and fairness. In contrast, less frequently endorsed strengths include self-regulation, perseverance, zest, spirituality, and prudence. In terms of the relationship between strengths and well-being in people with CID, an early study on recovery from illness by Peterson et al. (2006) analyzed data from 2,087 adult volunteers recruited through the VIA website. They found that physical illness was less likely to lead to reductions in life satisfaction among individuals who reported high levels of bravery, kindness, and humor. In the same study, psychological disorder was less likely to lead to reductions in life satisfaction among those reporting the strengths of appreciation of beauty and love of learning. Hanks et al. (2014) conducted a survey study investigating character strengths in individuals with TBI at a midwestern rehabilitation hospital in the United States and found that hope, zest, humor, and perseverance were among the strongest predictors of life satisfaction in this population. Their findings support the contributions that character strengths make to subjective well-being and perceived community integration, supporting the development of interventions that focus on developing strengths in rehabilitation settings. Similarly, Smedema and Bhattarai (2021) distributed online surveys through the National Multiple Sclerosis Society website to explore the role of character strengths among individuals with MS. Their findings demonstrated that strengths significantly influenced QOL, even after controlling for other well-established psychosocial factors such as resilience, social support, and personality traits. These findings highlight both the diversity of character strengths in disability populations and the need for tailored interventions that can build strengths to improve well-being.
Connecting Character Strengths and Acceptance of Disability
The character strengths framework offers a valuable approach for improving disability acceptance and well-being in individuals with disabilities. It complements existing understandings of disability acceptance by focusing on the development and use of personal strengths to cope with the challenges posed by CID. The combination of character strengths and disability acceptance theories provides a holistic view of how individuals can adapt and thrive with a disability.
The importance of character strengths to disability acceptance is further supported by Niemiec (2020), who identified key functions that character strengths serve when navigating life’s opportunities and adversities, such as buffering, reappraisal, and resilience. It builds on the VIA model and suggests practical ways to harness strengths to achieve greater well-being and flourishing, particularly in challenging circumstances such as CID. Understanding these functions within the context of disability provides insight into how character strengths can facilitate the acceptance of disability. Character strengths can be used to reinterpret the experience of disability, helping individuals focus on their potential rather than limitations, which aligns closely with Wright’s (1983) disability acceptance model. Thus, the purpose of this study is to examine the relationship of the 24 character strengths in Peterson and Seligman’s (2004) model with the four value changes in Wright’s (1983) theory of disability acceptance.
Based on prior literature, the hypotheses for the current study are as follows:
Although the character strengths in Peterson and Seligman’s (2004) model consist of 6 overarching virtues, the present study entered all 24 character strengths as a single block in the regression models rather than grouping them by virtue category. This decision was based on prior research suggesting that individual character strengths demonstrate unique predictive relationships with psychosocial outcomes, independent of their virtue classification (Niemiec, 2023). Moreover, empirical support for the six-virtue factor structure remains inconclusive, with studies indicating that certain strengths do not consistently cluster within the theorized virtue domains (e.g., Diez et al., 2022). Given these concerns, structuring the regression models based on individual strengths rather than virtue categories allowed for a more precise examination of their distinct contributions to disability acceptance.
Method
Participants
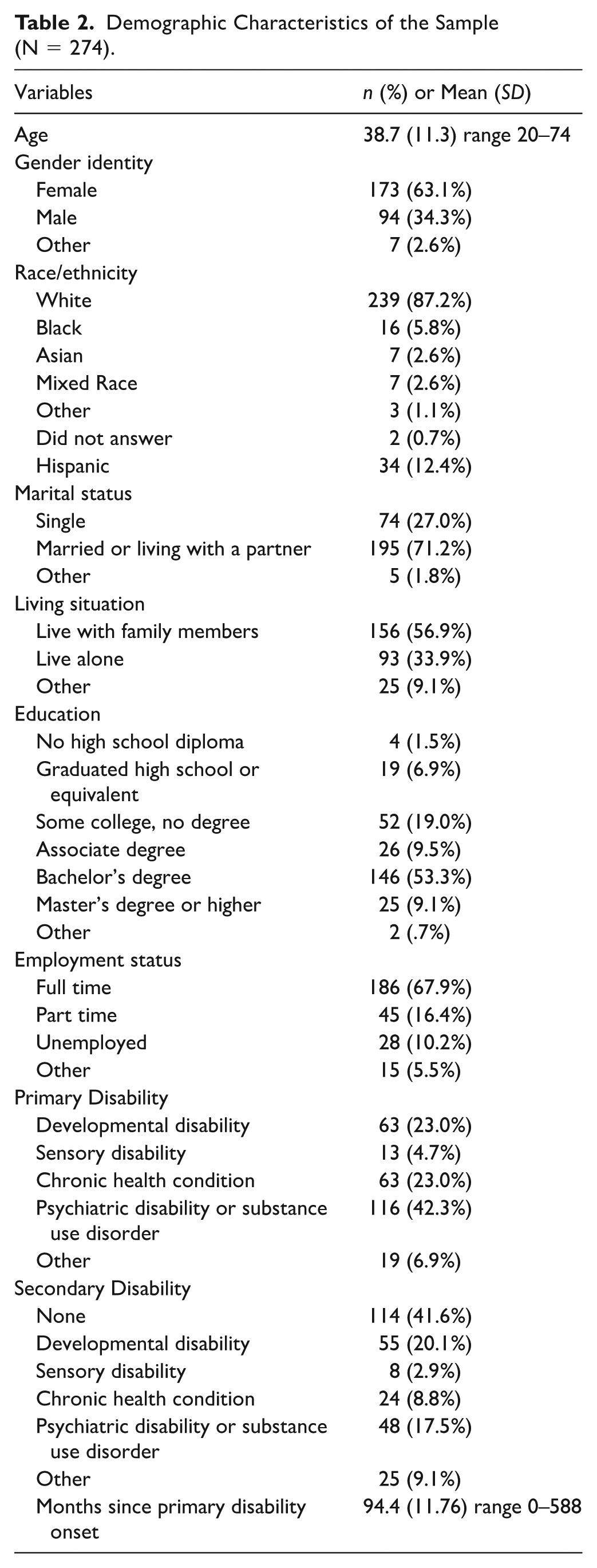
The participants in this study included 274 individuals with self-reported disabilities. The majority of participants identified as female (63.1%), white (87.2%), married (71.2%), living with family members (56.9%), having at least a bachelor’s degree (62.4%), and working full time (67.9%). The mean age for participants was 38.7 years (SD = 11.3, range = 20–74). Regarding primary disability, 63 (23.0%) participants identified living with a developmental disability, 13 (4.7%) identified as having a sensory disability, 63 (23.0%) indicated that they live with a chronic health condition, 116 (42.3%) reported having a psychiatric disability or a substance use disorder, and 19 (6.9%) reported having “other” disability. Participants reported having their primary disabilities for an average of 94.4 months (SD = 11.76, range = 0–588). Full participant demographic information can be found in Table 2.
Demographic Characteristics of the Sample (N = 274).
Measures
Demographic Questionnaire
The demographic questionnaire included questions about the participant’s age, gender identity, race and ethnicity, marital status, educational level, employment status, living situation, primary disability, and secondary disability.
Values in Action Adult Assessment—72-Item Version (VIA-72)
Character strengths were measured by the VIA-72. In this instrument, each of the 24 character strengths in Peterson and Seligman’s (2004) model was measured using three items. A sample item is “I experience deep emotions when I see beautiful things” (Appreciation of Beauty and Excellence). For each item, participants are asked to use a five-point Likert scale (1 = “Not at all like me” to 5 = “Very much like me”) to indicate the degree to which the statement is similar to them. Higher scores on each subscale reflect greater levels of the corresponding character strength. Peterson and Seligman (2004) reported the internal consistencies for each subscale to be in the .75 range. The Cronbach’s alpha coefficients for the VIA-72 subscales in the present study range from .46 (Humility) to .91 (Spirituality). The following subscales had Cronbach’s alpha values below .70: Humility (.46), Love of Learning (.60), Kindness (.64), Leadership (.67), Curiosity (.68), Fairness (.68), and Forgiveness (.69). The three-item structure of each VIA-72 subscale likely contributed to reduced internal consistency. While higher-item versions of the VIA (e.g., VIA-120) may provide improved psychometric performance, the VIA-72 was selected to minimize participant response burden given the length of the full survey. The potential impact of lower reliability on interpretation is addressed in the “Limitations” section. All subscale item means, standard deviations, and alphas are provided in Table 3.
Item Means, Standard Deviations, and Alphas of Character Strengths, and Correlations With Four Value Changes Associated With Acceptance of Disability (N = 274).
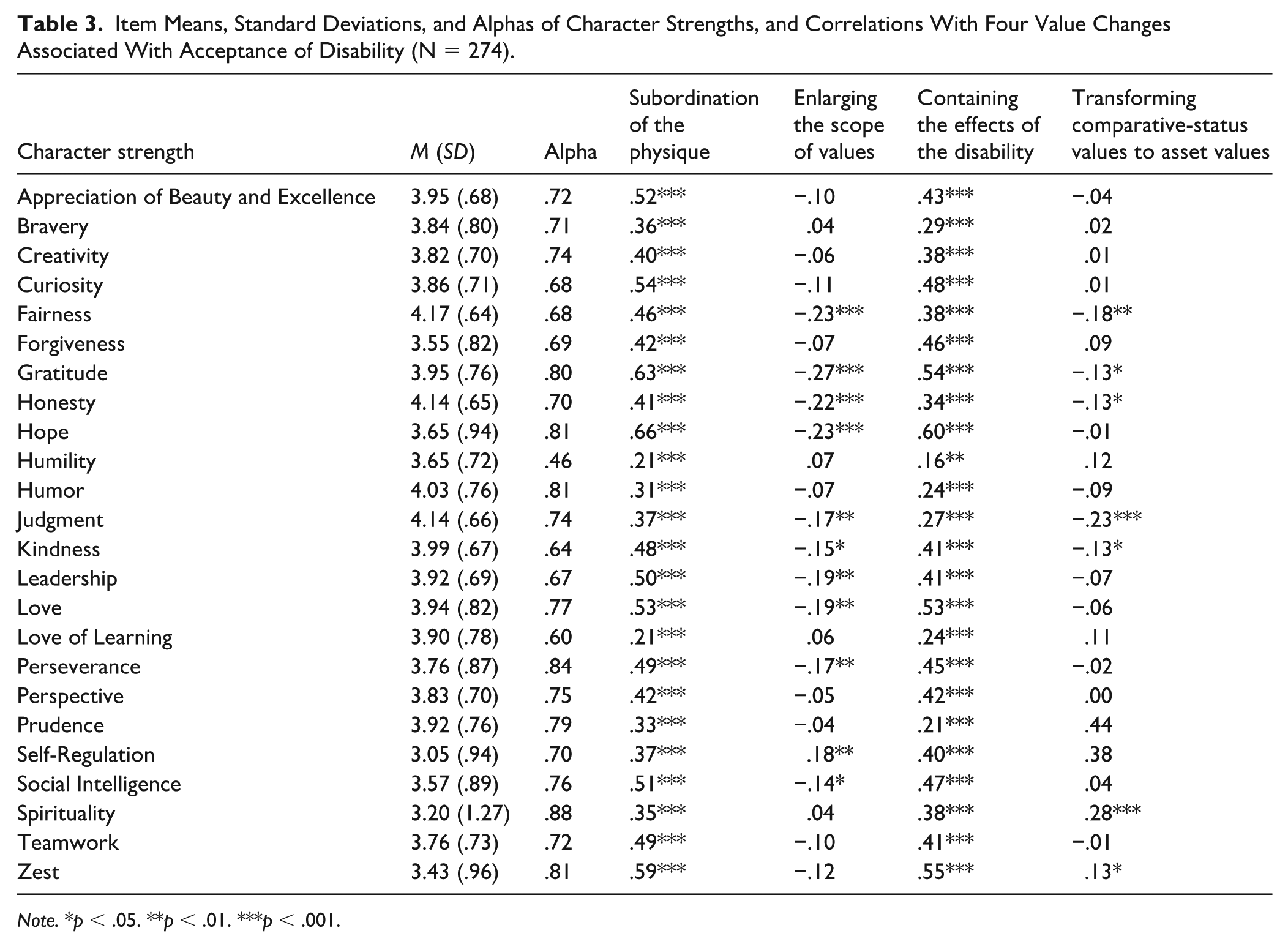
Note. *p < .05. **p < .01. ***p < .001.
Multidimensional Acceptance of Loss Scale (MALS)
Acceptance of disability was measured by the MALS (Ferrin et al., 2011). This 42-item scale was developed based on the four value changes in Wright’s (1983) disability acceptance theory, including Subordinating Physique Relative to Other Values (12 positive items, e.g., “I am a person of worth even though I have a disability”), Enlarging the Scope of Values (10 negative items, e.g., “I think a lot about what I have lost because of my disability”), Transforming Comparative-Status Values Into Asset Values (11 negative items, e.g., “Because of my disability, everything about me is subaverage”), and Containing the Effects of the Disability (nine positive items, e.g., “I am satisfied in doing my best and being rewarded for my efforts”). For each item, participants are asked to use a four-point Likert scale (1 = “Strongly disagree” to 4 = “Strongly agree”) to indicate their agreement with the statement. Higher scores on the Subordinating Physique Relative to Other Values and the Containing the Effects of the Disability subscales reflect greater levels of value change and disability acceptance. In contrast, because the Enlarging the Scope of Values and the Transforming Comparative-Status Values into Asset Values subscales consist entirely of negatively worded items, lower scores on these subscales reflect greater levels of value change and disability acceptance. Ferrin et al. (2011) reported the internal consistencies for each subscale to be between .80 and .88. The Cronbach’s alpha coefficients for the MALS subscales in the present study are .89 (Subordinating Physique Relative to Other Values), .93 (Enlarging the Scope of Values), .88 (Transforming Comparative-Status Values Into Asset Values), and .75 (Containing the Effects of the Disability).
Procedures
The current study was approved by the Institutional Review Boards (IRBs) at two midwestern universities in the United States, where the authors were affiliated during the project period. Participants were recruited through Amazon Mechanical Turk (MTurk), a crowdsourcing platform. MTurk has several advantages for conducting rehabilitation research, including access to a large and diverse sample, cost-effectiveness, and a greater percentage of potential participants with disabilities compared to traditional samples (Huang & Smedema, 2023). This recruitment approach allows for efficient access to a geographically dispersed sample and aligns with prior disability research utilizing MTurk.
A Qualtrics pre-screening survey was distributed through the MTurk website to recruit eligible participants. The pre-screening survey included three multiple-choice questions about age, country of residence, and disability type (including the option of “none”). Participants were eligible if they (a) were 18 years or older, (b) were living in the United States or Canada, and (c) self-reported to have one or more disabilities. Each participant received $0.01 through MTurk after completing the pre-screening survey, regardless of their eligibility for the study.
Of the 1,065 participants who submitted the pre-screening survey, 535 (50.2%) met the eligibility criteria. Eligible participants were notified about the formal study through the MTurk website’s messaging system. The formal Qualtrics survey was also distributed through MTurk and made visible to the eligible participants. The survey included an electronic consent form and the study measures. Participants advanced to the study measures only after they agreed to take part by checking the box on the electronic consent form. Each participant received $5.00 through MTurk after completing the formal survey if they passed an attention check question embedded in the middle of the VIA-72, asking them to select “unlike me” to indicate they were reading the items carefully.
Of the 392 (73.7%) eligible participants who submitted the formal study survey, 51 participants were excluded due to incomplete study measures, 12 were excluded due to failing the attention check, and 35 reported not having a disability even after making it through the pre-screening survey. Therefore, the sample size for this study was 294.
Data Screening and Analysis
All data analyses were conducted using SPSS version 29.0. Several diagnostic tests, including examination of missing data, identification of outliers, and examination of normality and multicollinearity of all variables, were conducted prior to data analysis. No measure had higher than 5% of values missing, and mean imputation was used to replace missing values. Twenty multivariate outliers were detected and removed after Mahalanobis distances were examined. This resulted in a final sample of 274 participants. All variables were deemed to be normally distributed after inspection of skewness and kurtosis values. The bivariate correlation matrix of the 24 character strength variables and Variance Inflation Factors (VIF) were examined in order to determine any issues related to multicollinearity. Three correlations exceeded the recommended .70 cutoff (Tabachink & Fidell, 2001): Hope and Gratitude (r = .72), Hope and Zest (r = .79), and Curiosity and Appreciation of Beauty and Excellence (r = .90). VIFs ranged from 1.37 (Love of Learning) to 6.71 (Curiosity). Curiosity (6.71) and Appreciation of Beauty and Excellence (6.10) exceeded the conventional threshold of 5. While these values indicate moderate multicollinearity, all predictors were retained due to the exploratory nature of the study and theoretical interest in examining the full set of strengths concurrently.
Four linear regressions were conducted to test the contribution of the 24 character strengths in the Peterson and Seligman (2004) model to the four value changes in Beatrice Wright’s (1983) acceptance of disability model. An a priori power analysis was conducted using G*Power 3.1.9.7 (Faul et al., 2007), a software tool for power analysis. Using 24 predictor variables, power equal to .80, and an alpha level of .05, the analysis determined that a sample size of 169 would be needed to detect a medium effect size (f 2=.15; Cohen, 1988). The final sample obtained in the present study, 274, was therefore deemed adequate to proceed with the analyses.
Disability-related and demographic variables were not included as control variables in the regression models due to the exploratory nature of the study and the focus on understanding the relationships between character strengths and disability acceptance. While factors such as disability type, duration, and demographic characteristics may influence disability acceptance, prior research suggests that character strengths contribute to well-being and adaptation across diverse populations (e.g., Smedema & Bhattarai, 2021). Given the study’s primary aim of identifying which strengths are most relevant to disability acceptance, controlling for these variables may obscure meaningful relationships. Similarly, because the study was exploratory and intended to identify preliminary patterns, no corrections for multiple comparisons were applied. The risk of Type I error is therefore acknowledged and addressed within the limitations section.
Results
Means, standard deviations, alphas, and correlations among all character strengths and the four value changes are presented in Table 3. Bivariate correlations revealed significant relationships between many character strengths and the four value changes associated with disability acceptance. Notably, Hope, Gratitude, and Self-Regulation showed the strongest positive associations with Subordination of the Physique and Containment of Disability Effects, while Honesty and Judgment were most strongly related to Transforming Comparative Status Values to Asset Values. In terms of descriptive findings, the most highly endorsed character strengths in the sample were Fairness (M = 4.17, SD = .64), Honesty (M = 4.14, SD = .65), and Judgment (M = 4.14, SD = .66), while the least endorsed were Self-Regulation (M = 3.05, SD = .94), Spirituality (M = 3.20, SD = 1.27), and Zest (M = 3.43, SD = .96).
The results of the linear regression analyses performed with the set of character strengths and the four value changes are presented in Tables 3–6. For the value change of Subordination of the Physique (Table 4), the model accounted for 56% of the variance, R2 = .56, F(24, 249) = 13.20, p < .001. Examining the standardized partial coefficients, Gratitude (β = .24, p < .01), Hope (β = .25, p < .01), and Self-Regulation (β = .16, p < .01) all significantly contributed to the variance in Subordination of the Physique. For the value change of Enlarging the Scope of Values (Table 5), the model accounted for 27% of the variance, R2 = .27, F(24, 249) = 3.73, p < .001. Examining the standardized partial coefficients, Bravery (β = .19, p < .01), Gratitude (β = −.21, p < .05), Honesty (β = −.21, p < .01), Hope (β = −.26, p < .05), and Self-Regulation (β = .22, p < .01) all significantly contributed to the variance in Enlarging the Scope of Values. For the value change of Containing the Effects of the Disability (Table 6), the model accounted for 50% of the variance, R2 = .50, F(24, 249) = 10.36, p < .001. Examining the standardized partial coefficients, Love (β = −.20, p < .01), Prudence (β = −.21, p < .01), and Self-Regulation (β = .21, p < .001) all significantly contributed to the variance in Containing the Effects of the Disability. Finally, for the value change of Transforming Comparative-Status Values to Asset Values (Table 7), the model accounted for 34% of the variance, R2 = .34, F(24, 249) = 5.25, p < .001. Examining the standardized partial coefficients, Honesty (β = −.17, p < .05), Judgment (β = −.27, p < .01), Self-Regulation (β = .30, p < .001), and Spirituality (β = .23, p < .01) all significantly contributed to the variance in Transforming Comparative Status Values to Asset Values.
Regression Analysis for Subordination of the Physique (N = 274).
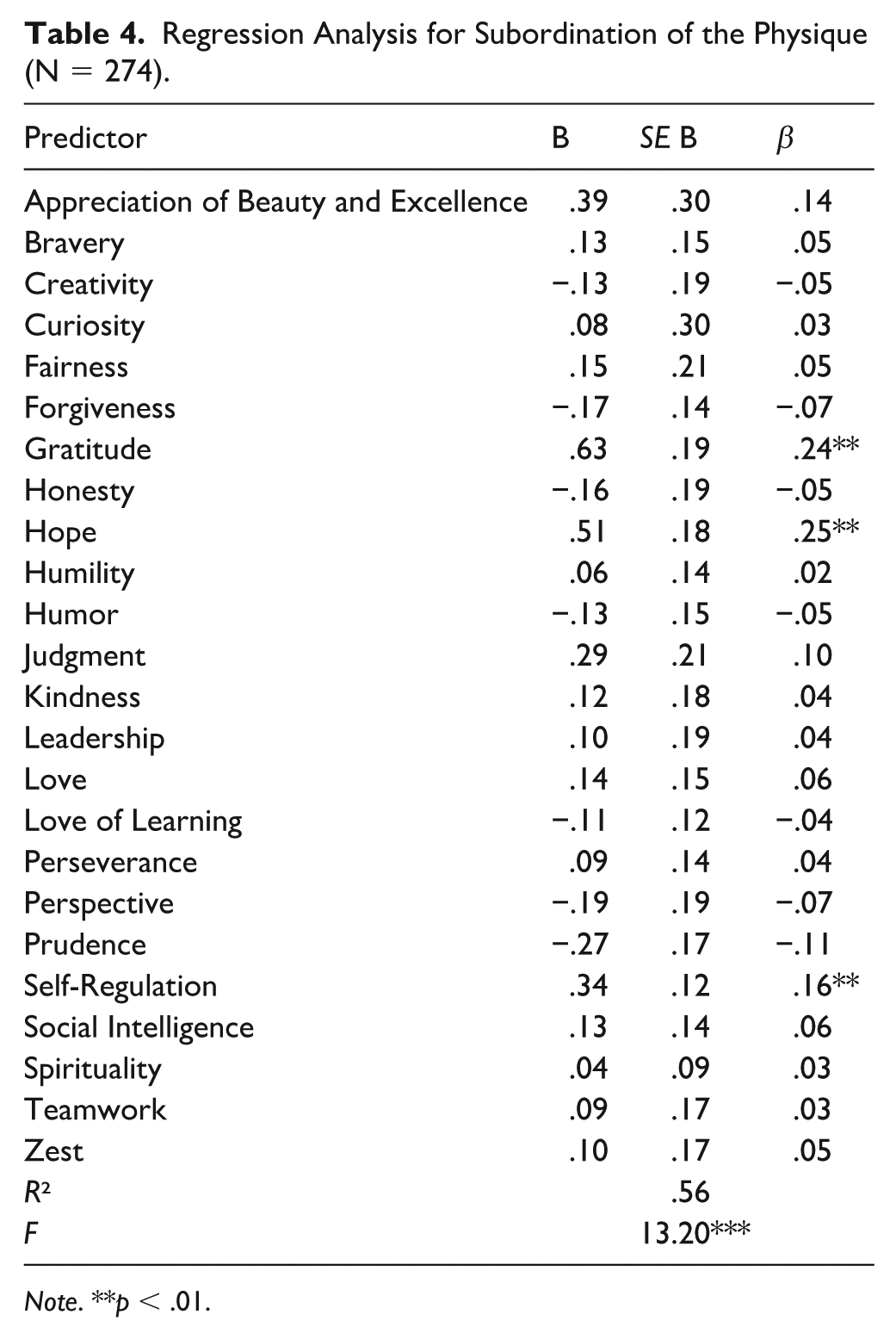
Note. **p < .01.
Regression Analysis for Enlarging the Scope of Values (N = 274).
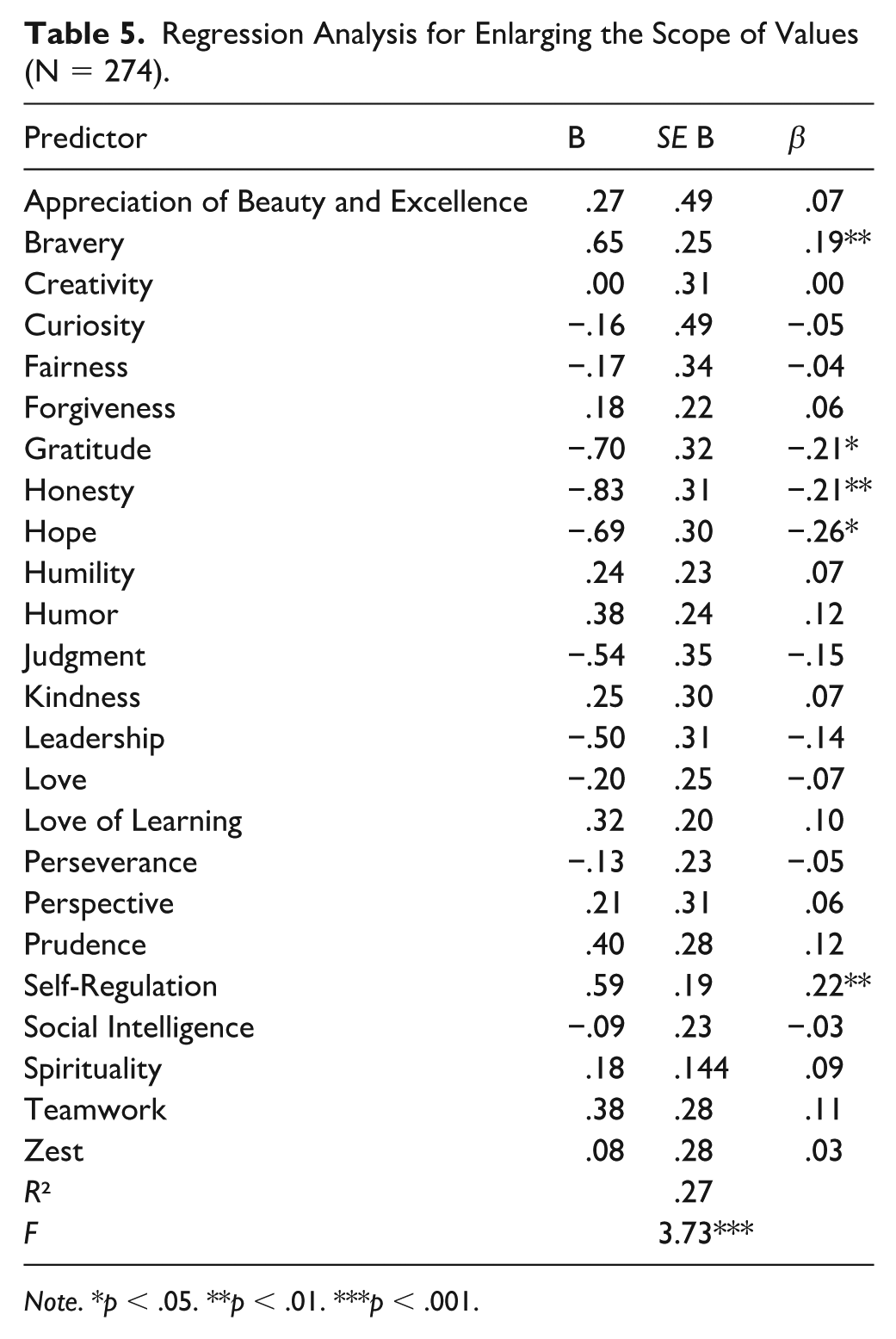
Note. *p < .05. **p < .01. ***p < .001.
Regression Analysis for Containing the Effects of the Disability (N = 274).
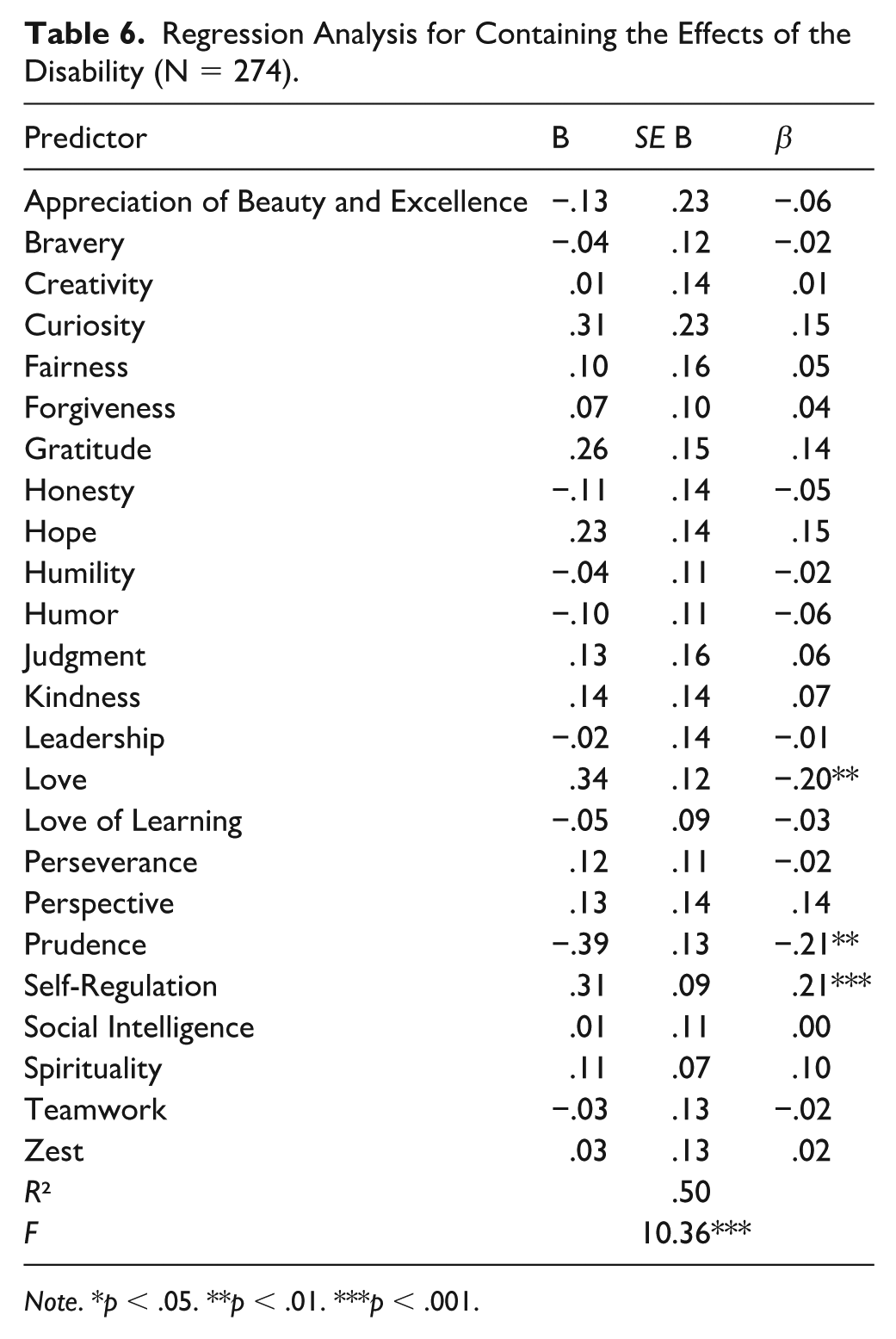
Note. *p < .05. **p < .01. ***p < .001.
Regression Analysis for Transforming Comparative-Status Values to Asset Values (N = 274).
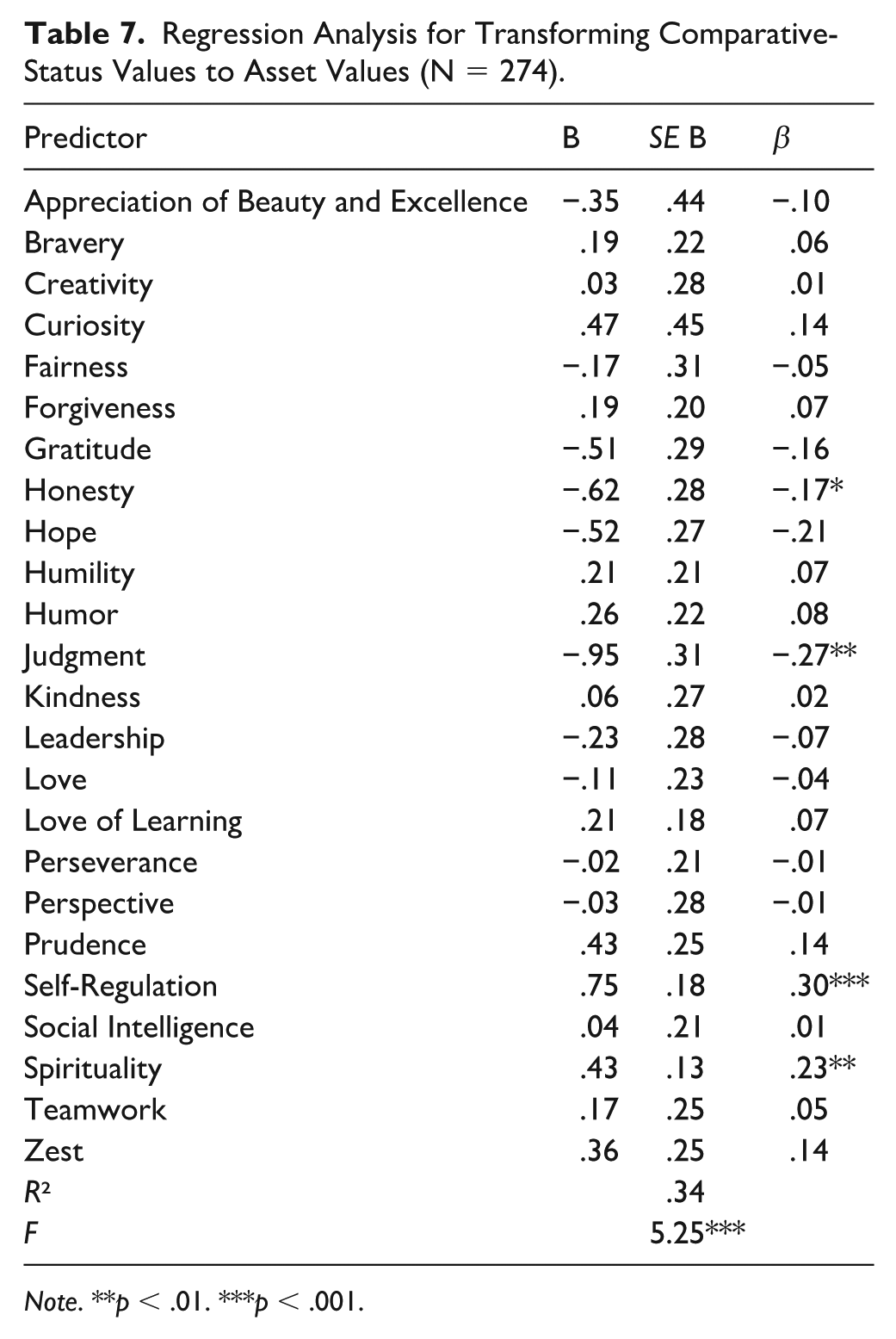
Note. **p < .01. ***p < .001.
Discussion
Results of this study examined the relationship of character strengths and disability acceptance in persons with disabilities. The highest-rated character strengths, Fairness, Honesty, and Judgment, align with prior research indicating that these strengths are commonly endorsed across populations (N. S. Park et al., 2006). In contrast, Spirituality, Self-Regulation, and Zest were the least endorsed, consistent with findings that these strengths tend to be less universally expressed among people with disabilities (Umucu et al., 2022). These patterns suggest that people with disabilities may prioritize strengths related to justice and moral reasoning as adaptive responses to challenges. Future studies should explore whether these trends differ by disability type or other demographic factors to better understand the role of character strengths in disability acceptance.
As a group, the character strengths in Peterson and Seligman’s (2004) model contributed significantly to all four value changes in Wright’s (1983) theory of disability acceptance. While this is the first study to investigate the contribution that character strengths have on disability acceptance, character strengths have previously been found to be positively associated with QOL in people with disabilities (Hanks et al., 2014; Peterson et al., 2006; Smedema & Bhattarai, 2021) and QOL has been found to be positively associated with disability acceptance (Li & Moore, 1998; Ogawa et al., 2021; Smedema et al., 2010; Wilski et al., 2019; Yehene et al., 2020). Thus, it can be inferred that the present results are consistent with prior research findings.
When examining the relationships among character strengths, taken together, and the individual value changes, the strengths had the strongest association with Subordination of the Physique, followed by Containment of Disability Effects. While still significant, Enlarging the Scope of Values and Transforming Comparative Status Values to Asset Values had weaker relationships with the character strengths. Model-level R² values indicated that character strengths explained between 27% (Enlarging the Scope of Values) and 56% (Subordination of the Physique) of the variance across the disability acceptance domains, reflecting moderate to strong explanatory power. Individual strengths demonstrating the strongest unique effects included Hope, Gratitude, Honesty, Judgment, and Self-Regulation, suggesting that strengthening these qualities may be particularly beneficial in clinical interventions aimed at enhancing acceptance.
To better understand these findings, it is helpful to look at the individual contributions of the strengths to the values. With respect to Subordination of the Physique, the strengths with significant associations were Gratitude, Hope, and Self-Regulation. This suggests that people with higher amounts of these strengths may be more successful in shifting their focus away from their physical bodies to appreciate other aspects of their identities. For example, individuals who are grateful for what they have may be more able to appreciate non-physical aspects of their lives. Similarly, individuals with a strong sense of hope, defined as the motivation and ability to identify pathways toward achieving goals (Snyder et al., 1991), may be more inclined to focus on intellectual or social goals rather than physical functioning. On the other hand, self-regulation, or the ability to manage one’s behavior and emotions, can provide the discipline and control needed to divert attention away from the physique to other meaningful areas of life.
Love, Prudence, and Self-Regulation were individually significantly associated with Containment of Disability Effects. Interestingly, people who scored higher in self-regulation but lower in love and prudence seemed better able to prevent their disability from spilling over into other areas of life, suggesting that strong self-regulation may help individuals maintain control over the impact of their disability. In contrast, lower levels of love (emotional connections to others) and prudence (characterized by careful, risk-averse decision-making) might actually contribute to a more compartmentalized approach, allowing the disability to be managed without influencing other life domains. Therefore, individuals with lower levels of love may be more independent and self-reliant, therefore being better able to contain the effect of the disability, while people demonstrating greater prudence may be less likely to engage in other life domains that would bring risk, therefore preventing the disability from affecting other areas of life.
Bravery, Gratitude, Honesty, Hope, and Self-Regulation were individually significantly associated with Enlarging the Scope of Values. Keeping in mind that higher scores on this scale are associated with lower levels of acceptance, these results show that individuals higher in gratitude, honesty and hope, and lower in bravery and self-regulation may be more successfully able to appreciate values other than those affected by the disability. As mentioned, gratitude allows people to find value in what they have, fostering appreciation for non-disability-related aspects of life. Honesty, in this context, could relate to an open acknowledgment of one’s limitations while still finding meaning and value in other areas. Hope, as described above, may push individuals to pursue goals and interests that go beyond their disability, enabling them to value things like relationships, creativity, or intellectual pursuits more easily. While bravery and self-regulation can be incredibly beneficial, individuals high in these traits might take a more rigid approach to overcoming challenges, focusing narrowly on controlling or facing disability-related difficulties. This focus might prevent them from stepping back and considering a wider array of life experiences. On the other hand, those lower in bravery and self-regulation may not feel as compelled to take a direct, disciplined approach and instead allow themselves to explore broader values without the same level of self-imposed pressure.
Finally, Honesty, Judgment, Self-Regulation, and Spirituality were all significantly associated with Transforming Comparative Status Values to Asset Values. This scale is also negatively scored; therefore, people with higher levels of honesty and judgment and lower levels of self-regulation and spirituality may be more successful in shifting the way they evaluate themselves in comparison to others. Honesty may encourage a realistic and transparent self-evaluation, helping individuals acknowledge both their limitations and strengths without focusing excessively on comparisons with others. Similarly, judgment, or the ability to think critically and make balanced decisions, may help individuals assess themselves in a fair and measured way, recognizing their own unique qualities as assets rather than focusing on how they rank relative to others. On the other hand, self-regulation and spirituality may play a different role. High self-regulation could lead to a more controlled, perfectionistic approach, where individuals are more focused on self-improvement and comparison to external standards, making it harder to shift away from comparative values. Spirituality, which often emphasizes connection with something greater than oneself, might encourage a more abstract or externalized perspective, potentially reducing focus on personal assets and leading individuals to compare their spiritual journey or moral standing with others.
Some regression findings diverged from the bivariate correlations, suggesting potential suppression effects or multivariate interactions. For example, Bravery significantly predicted Enlarging the Scope of Values in the regression model but did not show a significant bivariate correlation. This may indicate that, when considered alongside other strengths, Bravery contributes to shifting values beyond disability-related concerns. Similarly, the regression coefficient for Love reversed direction compared to its bivariate correlation with Containing the Effects of the Disability. This suggests that Love may interact with other strengths in complex ways and act as a suppressor variable. Future research should explore these relationships using mediation or moderation analyses to clarify the underlying mechanisms driving these effects.
Implications for Clinical Practice
The results of this study highlight the importance of implementing a positive approach to rehabilitation services, as various character strengths predict the different domains of disability acceptance. This is consistent with one of the most important philosophies of rehabilitation counseling that focuses on strengths. Focusing on clients’ inherent strengths can shift the therapeutic narrative from one of limitations to one of possibility, and to use character strengths to frame disability in terms of identity and growth rather than deficit. This strengths-based perspective enhances motivation for goal setting and builds resilience in the face of adversity (Niemiec, 2020), while helping clients to internalize a more empowered and accepting self-concept (Shogren et al., 2018).
Rehabilitation counseling considers character strengths as malleable factors. Thus, practitioners can provide assessment, encouragement, support, and intervention to individuals with disabilities in order to enhance well-being outcomes. Specifically, practitioners can utilize character strengths assessment tools (e.g., the VIA Inventory) to identify the unique character strengths that a client possesses. Assessment can help uncover the inherent strengths of clients. Any less-developed strengths can, thus, be targets of interventions. Relatedly, given that disability acceptance is a multi-faceted concept, certain character strengths are likely to play a more important role than others in contributing to the different disability acceptance domains. Therefore, the specificity of certain character strengths can be developed through different strategies and/or evidence-based interventions. For example, the use of gratitude journaling and writing gratitude letters can be used to increase positive affect and well-being (Davis et al., 2016). Counseling using the cognitive behavior therapeutic approach can be used to help clients to reappraise and reframe their adversities into different meanings (Folkman & Moskowitz, 2000).
The six functions of character strengths described by Niemiec (2020) may provide a practical way to organize and conceptualize rehabilitation services for individuals with disabilities around character strengths and acceptance of disability. Priming, where individuals become aware of and utilize their strengths, allows individuals to focus on their positive traits, rather than the limitations imposed by their condition. For example, a person with a disability may consciously activate their strengths of perseverance or creativity to find new ways of accomplishing tasks, thereby increasing self-efficacy and fostering a sense of control over their circumstances. Mindfulness, where strengths synergize with present-moment awareness to enhance well-being, can foster greater self-compassion, reduce feelings of frustration or hopelessness, and increase awareness of opportunities for positive action despite physical or psychological challenges. Appreciation, where character strengths help individuals value what has occurred in life, can involve recognizing one’s resilience, capacity for growth, or the small successes achieved in daily life, even in the face of adversity. Appreciation encourages individuals to shift their attention away from what they have lost due to their disability and instead focus on the unique strengths and opportunities that remain. Buffering, where strengths help prevent problems from overwhelming the individual, can be important in managing the emotional and psychological effects of living with a chronic condition. Individuals who actively engage their strengths are better equipped to cope with the stressors associated with disability. Reappraisal, where strengths assist in reinterpreting life challenges more positively, can be a powerful tool for transforming the experience of disability into an opportunity for personal growth and self-acceptance. This allows individuals to see their disability not as an insurmountable barrier, but as an aspect of life that can coexist with strength, purpose, and well-being. Resilience, where character strengths aid in recovering from setbacks and bouncing back from adversity, is a key factor in maintaining a positive outlook and pursuing a fulfilling life, even in the face of physical or psychological limitations. Resilience, bolstered by character strengths, allows individuals to adapt to their circumstances, find meaning in their experiences, and continue pursuing their goals with determination and optimism.
Given these findings, rehabilitation counselors may benefit from prioritizing strengths that demonstrated the strongest and most consistent relationships with disability acceptance, particularly Hope, Gratitude, Honesty, Judgment, and Self-Regulation. Targeted strengths development may support clients in reframing identity, broadening areas of value beyond physical functioning, and reducing comparisons to others. Intervention research evaluating structured strengths-based programs is an important next step.
Limitations and Future Research Directions
The present study has several limitations. First, the study utilized a cross-sectional design, which limits its ability to infer causality or the direction of the relationship between character strengths and disability acceptance. It is unclear whether certain character strengths promote disability acceptance, or whether individuals with higher levels of acceptance are more likely to develop or utilize certain strengths, or whether the relationship is reciprocal. Therefore, longitudinal studies can provide further evidence in exploring the directionality of character strengths and disability acceptance. As described above, the development of character strengths can be a practical intrinsic coping mechanism in promoting disability acceptance. These strategies can be evaluated in terms of how the development of character strengths can have positive outcomes over time.
Second, the eligibility for this study was determined based on participants’ self-reported disability status, which is difficult to verify. For example, 35 individuals reported having a disability in the pre-screening survey in order to qualify, but further indicated that they did not have a disability in the full survey. Future research could address this limitation by partnering with disability organizations or healthcare providers, where disability status can be confirmed through medical records or other forms of verification.
Third, the majority of participants in this study were female, White, and employed. In addition, many participants reported psychiatric disorders or substance use disorders as their primary disability. This limits the study’s ability to generalize its findings to a more diverse population. Although most studies have not found gender or racial differences in disability acceptance (Groomes et al., 2011; Li & Moore, 1998; Martis et al., 2024), our sample may not fully capture the perspectives of those from racially and ethnically diverse backgrounds. Thus, caution should be taken when generalizing these results across different cultural or demographic groups. On the other hand, employment status has been shown to affect disability acceptance. In a sample of individuals with physical disabilities in South Korea, those with low income or poor health status had the lowest level of disability acceptance (E. Y. Park & Kim, 2021).
Also, though there has been limited investigation into the relationship between disability types and disability acceptance, research suggests that people with acquired disabilities and multiple disabilities have lower levels of disability acceptance (Li & Moore, 1998). Similarly, while this study has a large sample size, it is plausible that different disabilities may be unique in their disability acceptance and character strengths experiences. Though our sample has several disability groups, all but one had a relatively low percentage composition, thus it did not allow the testing of character strengths in different disability groups. The refinement of character strengths in relation to disability groups and/or disability acceptance can be further studied. This can be done by using advanced statistical techniques such as latent profile analysis to understand the unique profiling of character strengths and their relationships to other variables.
Fourth, character strengths explained low variances in some of the regression models, particularly Enlarging the Scope of Values and Transforming Comparative-Status Values to Asset Values. This suggests that important factors associated with disability acceptance may have been overlooked. The models may not fully capture the complexity of the disability acceptance process, and additional variables, such as understanding of the disability, family support, depression, and self-efficacy (e.g., Chai et al., 2016), may be critical to understanding the construct more comprehensively. Future studies should consider incorporating additional variables to improve the explanatory power of the models.
Fifth, measurement quality may have affected the results. Several VIA-72 subscales demonstrated Cronbach’s alpha values below .70, which may have reduced the precision of estimates and contributed to suppression patterns within the regression models. Future research should consider using longer multi-item character strength measures such as the VIA-120, or alternative analytic approaches (e.g., latent variable modeling), to improve measurement precision and clarify the structure of strengths in disability populations.
Finally, multicollinearity could inflate standard errors, making it difficult to determine the unique contributions of individual character strengths. Examination of the correlation matrix identified some high correlations (e.g., Hope and Gratitude, r = .72; Hope and Zest, r = .79; and Curiosity and Appreciation of Beauty and Excellence; r = .90). Relatedly, the discrepancies between bivariate correlations and regression results suggest potential suppression effects or multivariate interactions among character strength variables, which may limit the interpretability of individual regression coefficients. For example, Love demonstrated a positive correlation with Containing the Effects of the Disability, yet its regression coefficient was negative, indicating potential suppression. Similarly, the lack of a significant bivariate correlation between Bravery and Enlarging the Scope of Values contrasted with its independent contribution within the regression model. These patterns may reflect multivariate interactions among strengths or context-specific functioning that warrant further investigation. While all strengths were retained in the analyses due to the exploratory nature of the study, future research should more formally assess multicollinearity and apply additional analysis (e.g., mediation or moderation) to clarify the mechanisms underlying these findings.
Finally, the number of regression models and predictors included in the analyses raises the possibility of inflated Type I error. Given the exploratory nature of the study and the desire to retain the full character strengths set for initial investigation, no Type I error correction procedures were implemented. Therefore, statistically significant results should be interpreted with caution until validated in future studies employing confirmatory models or error control techniques.
Conclusion
Our findings provided preliminary support for the role of character strengths in disability acceptance. Character strengths seemed to improve disability acceptance in people with disabilities, with the strongest association with Subordination of the Physique and Containment of Disability Effects. Findings also provided some implications such as the integration of character strengths assessment and intervention into clinical practice.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.