
Abstract
Purpose:
This study examined whether demographic factors influence disparities in resources supporting employment (RSE) and employment outcomes among people with disabilities (PWD).
Methods:
The study included 920 working-age, community-dwelling individuals with multiple sclerosis, muscular dystrophy, spinal cord injury, or postpolio syndrome. Zero-inflated multilevel Poisson regression models were used to assess the effects of RSE on employment outcomes (employment status and working hours for pay) and disparities in RSE (awareness and level of availability). The primary reason for not working was analyzed in relation to demographic factors.
Results:
Although greater RSE availability was associated with lower unemployment, PWD with lower education or household income reported reduced access to these resources. Significant three-way interaction effects among education, household income, and RSE on employment were observed. People with disabilities with lower education and household income were more likely to cite health limitations and reliance on disability pensions as reasons for not working.
Conclusion:
Marginalized PWD have reduced access to RSE, which in turn adversely affects employment outcomes, particularly among those with lower education and household income. Promoting equitable employment opportunities requires targeted allocation of RSE that addresses the unique barriers faced by marginalized PWD based on education and income.
The employment rate among working-age people with a disability (PWD) reached its highest level since 2008 at 22.5% in 2023, although it remains approximately a third of that among people without a disability (PWOD) (U.S. Department of Labor, 2024). In addition, compared PWOD, PWD report more unincorporated self-employment, are twice as likely to be employed part-time, and are twice as likely to work part-time involuntarily due to a reduction in hours or because they were unable to find a full-time job (U.S. Department of Labor, 2024). People with disabilities have fewer bachelor’s degrees than PWOD and are less likely to work in management, professional, and related occupations (U.S. Department of Labor, 2024). People with disabilities experience various barriers to employment, which impose considerable individual and family economic burdens (Day & Taylor, 2019; Goodman & Morris, 2020). For example, PWD earn 66 cents for every dollar earned by PWOD, in part because PWD are less likely to work in year-round full-time jobs (Day & Taylor, 2019). This is especially impactful given that a household containing an adult with a disability requires greater financial support, estimated at 128% of the annual cost of living for PWOD (Goodman & Morris, 2020).
While disability-related disparities in employment are a global issue, the United States shows the greatest gap in both employment and poverty rates by disability status among OECD (Organization for Economic Cooperation and Development) countries (see Supplemental Figure A1) (OECD, 2022). The difference in average employment rate in the United States from 2005 to 2019 was close to 50% (25% among PWD vs. 75% among PWOD), while other countries ranged between 25% and 30% (OECD, 2022). The poverty rate of the United States from 2005 to 2019 among PWD was also the highest at 50% compared to 20% among PWOD (OECD, 2022).
In the United States, employment outcomes for PWD are shaped by broader structural and policy environments that govern access to resources supporting employment (RSE). Federal and state-level initiatives—such as the Americans with Disabilities Act, the Workforce Innovation and Opportunity Act, the Ticket to Work Program, Section 503 of the Rehabilitation Act, and Medicaid’s Home and Community-Based Services (HCBS) programs—play critical roles in shaping access to employment supports. Working-age PWD may benefit from RSE, including disability accommodations, job placement and training services, and information on work and volunteer opportunities in the community. Employment decisions among PWD are further constrained by the “benefit cliff,” whereby relatively modest increases in earnings can result in the abrupt loss of income supports or healthcare coverage (Maestas et al., 2013; U.S. Government Accountability Office, 2024). For many working-age PWD, the risk of losing essential benefits creates disincentives to labor force participation.
Access to RSE is shaped by both service characteristics and individuals’ abilities to perceive and engage with services. Availability reflects the presence and structural reach of services, whereas awareness captures individuals’ knowledge of and perceived relevance of those services (Levesque et al., 2013). Even when individuals are nominally aware of RSE, variation and complexity in eligibility criteria across programs may limit functional awareness by obscuring whether services apply to one’s circumstances. Awareness, therefore, functions as a prerequisite for meaningful access, as services cannot be utilized if individuals are unaware of their existence or relevance. Prior research identifies lack of awareness as a significant barrier to accessing HCBS, particularly among individuals with lower income or lower levels of formal education, especially in contexts where services are limited or fragmented (Siconolfi et al., 2023).
Disparities in access to RSE are not evenly distributed across populations. Numerous studies indicate that PWD who are low-income, Black, Indigenous, and People of Color (BIPOC), or have less formal education, tend to use these services less frequently (Kaya et al., 2023). Acceptance of vocational rehabilitation services is also lower among BIPOC individuals compared with non-Hispanic Whites (Yin et al., 2022). Among PWD who do receive such services, those living in disadvantaged neighborhoods are often directed toward less desirable career paths and exhibit lower employment rates (Degeneffe et al., 2023; Fuentes et al., 2023). In addition, a recent scoping review highlighted that BIPOC individuals with disabilities frequently face skepticism from coworkers and employers regarding the legitimacy of their workplace accommodation requests (Fuentes et al., 2023).
Structural intersectionality provides a critical framework for examining employment disparities among PWD. Originating from Black feminist scholarship (Crenshaw, 1989), intersectionality posits that overlapping marginalized identities—such as race, gender, and disability—interact in synergistic ways to produce compounded disadvantages that cannot be understood by examining each identity separately. For example, findings about race (e.g., Black individuals) or gender (e.g., women) cannot be simply generalized to Black women, because intersecting positions generate effects that exceed additive influences. Structural intersectionality extends the individual perspective to the population level, showing how institutions, policies, and labor markets systematically reinforce barriers to employment and support (Homan et al., 2021). Identifying which combinations of identities are most consequential is, therefore, critical for addressing disparities in employment. Intersecting marginalized identities may operate through multiple mechanisms that influence employment outcomes. Employers may demonstrate greater willingness to provide accommodations to individuals with disabilities whom they perceive as highly skilled or indispensable, whereas those viewed as less capable encounter heightened barriers in both hiring and accommodation decisions. Moreover, structural barriers—including unequal access to education, insufficient income to maintain health, and occupational contexts characterized by limited flexibility—further restrict opportunities to obtain high-quality employment supports and training.
Within disability studies, intersectionality has been used to examine how the experience of disability is shaped by social hierarchies and institutional biases. Among PWD, BIPOC women with fewer years of formal education consistently report the lowest annual incomes and are more likely to rely on government financial assistance (60%) compared with individual employment (20%) (Maroto et al., 2019). Older PWD experience higher levels of workplace discrimination (Nangia & Arora, 2021), while Hispanic PWD are more likely to request disability accommodations but less likely to receive them (Hyseni et al., 2024). Women with disabilities also tend to hold jobs with poorer working conditions, contributing to higher stress levels (Brown & Moloney, 2019). However, much of this research has focused on the interaction effects of marginalized identities on outcomes, rather than empirically examining lived experiences of disadvantage or the impact of policy and programmatic interventions. Moreover, most existing studies are cross-sectional, limiting understanding of how interventions—such as RSE—may differentially affect intersectional groups.
People with disabilities with intersecting marginalized identities may, therefore, require greater access to RSE to achieve economic independence. Yet, research examining how intersecting demographic characteristics influence access to RSE or employment outcomes remains limited. Using a structural intersectionality framework, this study examined how key demographics (race/ethnicity, sex, age, education, household income, and rurality) interact to shape disparities in RSE access and employment among working-age PWD. We also aimed to identify which types of RSE most strongly relate to employment disparities and to explore barriers to employment across demographic groups.
Method
This is a secondary analysis of a nationwide longitudinal survey study of >2,000 community-dwelling individuals with a physical disability living in the United States, funded by the National Institute of Disability, Independent Living, and Rehabilitation Research. Inclusion criteria for the original study were age >18, physician-confirmed diagnosis of multiple sclerosis, muscular dystrophy, spinal cord injury or postpolio syndrome, and ability to read and understand English. Eligible participants were recruited through advertisements in organization newsletters and websites, through target diagnosis-specific recruitment via diagnosis advocacy organizations (e.g., the National Multiple Sclerosis Society), and through an existing disability research registry at the University of Washington. The survey was administered in seven waves from 2009 to 2017. In addition, the research team recruited a refresher sample of new participants in 2014, which constituted 20% of participants in that year.
Since the measurement of RSE was included in the survey in 2014, this secondary analysis only includes data from three annual waves, collected from 2014 to 2017. The response rate for each wave of data collection was 81% (Wave 1), 93% one year later (Wave 2), and 90% two years later (Wave 3). A total of 180 participants were lost to follow-up or withdrew during this 3-year window. The research team ensured the completeness of each survey, and any missing data were obtained by contacting the participant and sending email and written reminders if necessary. Participants were paid $25 for each completed survey. All study procedures were approved by the University of Washington’s Human Subjects Division. After excluding participants who were 65 years or older (656 in Wave 1, 650 in Wave 2, and 663 in Wave 3), the final sample size was 920 in Wave 1, 807 in Wave 2, and 733 in Wave 3.
Measures
Resources Supporting Employment
Three questions (Cronbach alpha = .90) from the environmental item bank (Lai et al., 2016) were used to assess the availability of RSE: “Disability accommodation services and supports are available at my work or school” (DA: disability accommodation), “My community offers job placement and training services” (JPT: job placement and training), and “My community offers good information on work and volunteer opportunities and supports” (INFO: information on work and volunteer opportunities). Responses were provided using a 6-point Likert-type scale ranging from “Don’t know—0” to “Always—5.” The total level of resource availability was calculated as the sum of all three responses (range: 0–15).
Employment Status
Participants were asked if they were currently employed outside the home. If they indicated current employment, they were asked to estimate how many hours per week they worked for pay. For analytic purposes, participants who indicated that they were not employed were assigned a 0 for weekly hours.
Demographic Characteristics
Participants were asked to report race/ethnicity, sex, age, education, medical diagnosis, annual household income, and zip code. Since 86% of participants were non-Hispanic White, race/ethnicity was categorized into two groups: non-Hispanic White and BIPOC. Since working hours for pay can affect an increase in household income, we used household income at the baseline for our analysis instead of treating it as a time-varying variable. Household income was divided into three groups based on an income level of $52,000, which is close to the median U.S. household income of $53,657 in 2014 (Denavas-Walt & Proctor, 2015). These were “high household income,” “low household income,” and “refused to disclose.” Participants’ area of residence was categorized as urban or rural based on their zip code.
Physical Function
To assess self-rated physical ability to complete daily activities, we used the PROMIS® (Patient-Reported Outcomes Measurement Information System [PROMIS], n.d.) Physical Function short form (version 1.0). This scale consists of 12 questions on a 5-point Likert-type scale. The raw summed scores are transformed to the T-score metric, with a mean of 50 and a standard deviation (SD) of 10, allowing for comparison with U.S. norms (PROMIS, 2020).
Pain Interference
The PROMIS® pain interference 4-item short form (version 1.1) was used to assess the impact of pain on daily activities at home, work, and social life, using a 5-point Likert-type scale (Amtmann et al., 2010). A T-score (with a mean of 50 and a SD of 10) was computed and compared with the general population. A person with a T-score of 60 for pain interference is interpreted as having 1 SD worse pain interference compared with the U.S. general population.
Main Reasons Not Working
Participants who were not working were asked to indicate their main reason for not working by selecting from nine predefined options or providing an “Other” response. The predefined options included the following: (a) taking care of house or family, (b) attending school, (c) retired, (d) on leave of absence from work, (e) on family or maternity leave, (f) temporarily unable to work for health reasons, (g) have a job or contract but it is off-season, (h) on layoff, and (i) on disability. Option 10 was “Other,” with a free-text description. Free-text responses were reviewed and categorized as follows: persistent health-related limitations (e.g., increased pain or fatigue while working; n = 73), difficulty finding employment (e.g., “no one will hire me” and “lack of skills”; n = 34), and unpaid work (e.g., volunteering; n = 13).
For analytic purposes, responses were regrouped into the following categories: taking care of house or family (n = 104), retired (n = 253), and on disability (n = 1,090). A new category, unable to work for health reasons (n = 127), was created by combining “temporarily unable to work for health reasons” (n = 54) with persistent health-related limitations (n = 73). All remaining responses were grouped as “Other” (n = 86). Within this category, the most frequent reasons included difficulty finding employment (39%), being on layoff (18%), and unpaid work (15%).
Statistical Analysis Plan
Descriptive statistics were used to characterize participants and to examine differences between waves, using the chi-square test, Fisher’s exact test, and one-way analysis of variance (ANOVA). Missing values were observed in pain interference (n = 18), physical function (n = 16), disability accommodation (DA, n = 3), job placement and training (JPT, n = 3), and information on work and volunteer opportunities (INFO, n = 1), which account for 0.7% of observations. To examine disparities in employment, a statistical approach guided by Ward et al. (2019) was applied, examining demographic distribution in (a) RSE (exposure variable), (b) weekly working hours for pay (outcome variable), (c) the effect of RSE on weekly working hours for pay, and (d) the interaction between RSE and demographic characteristics on weekly working hours for pay. Demographic characteristics that showed statistically significant interactions with RSE were further tested to examine whether combinations of demographic characteristics have a more pronounced effect on RSE. For example, we tested three-way interactions involving RSE and two demographic characteristics. The impact of RSE on weekly working hours for pay was evaluated from two temporal perspectives: concurrent effect and lagged effect. While concurrent effect models measured the association between exposures and outcomes at the same wave, lagged effect models examined associations with exposures at Wave 1 and outcomes at Waves 2 and 3. Statistically significant interactions between RSE and exposures were determined using the likelihood ratio test. Marginal plots were included to visually represent statistically significant interaction effects. In this approach, if a group difference in exposure and outcome or a significant effect of exposure on the outcome is observed, the result can be interpreted to suggest that the group difference in exposure contributes to the disparity in employment regardless of the interaction effect (Ward et al., 2019). All differences in each demographic characteristic were examined in the adjusted model because the unadjusted effect of race/ethnicity can be misleading if race/ethnicity is confounded with other demographic characteristics, such as sex, age, education level, living area, household income, and diagnosis.
One challenge in the data was a large number of zeroes for the three RSE items (39% of DA, 36% of JPT, and 29% of INFO). These zeroes indicate a response of “I don’t know” regarding the availability of the resource. Similarly, there was a significant number of zeroes (68%) for weekly working hours for pay, reflecting no paid work outside the home. To address excessive zeroes in the data and account for its longitudinal nature, we employed a zero-inflated Poisson mixed model with a random intercept using the glmmTMB (Brooks et al., 2017) package, simultaneously considering binary outcomes (the occurrence of zero) and count outcomes (the level of availability in RSE and the number of working hours for pay). When treating RSE as an independent variable, we modeled it as a continuous measure. A sensitivity analysis excluding respondents who were unaware of RSE (zeros) yielded similar patterns, supporting the robustness of our findings. Odds ratios (ORs) for the zero-inflated component, mean ratio (MR) for the count component, and 95% confidence intervals (CIs) were provided. The significant estimate with wide confidence intervals indicates limited precision and uncertainty of the true effect size (Sim & Reid, 1999). In addition, stratified analyses were conducted for each type of RSE (DA, JPT, and INFO) to investigate their distribution (Models 2–4) and the effect of each resource on weekly working hours for pay (Models 7–9).
The association between demographic characteristics and reasons for not working was examined using a Bayesian multinomial logistic regression with random intercepts to account for repeated measures. Participants were categorized into six groups based on education level (college graduate or higher vs. some college or less) and household income (high, low, or refused to answer). Predictors included race/ethnicity, sex, age, education/household income, and living area. Models were estimated using the brms (Bürkner, 2017) package with weakly informative priors, and results are reported as odds ratios with 95% credible intervals (CrIs). Convergence and model fit were evaluated using R-hat values, effective sample sizes, and posterior predictive checks. All analyses were conducted in R (version 4.4.2).
Results
The majority of participants at Wave 1 were non-Hispanic White (86%) and women (63%), with a mean age of 53.5 years (SD = 9.1). They had completed college or graduate-level education (54%), resided in urban areas (80%), and reported a household income of $52,000 or more (42%; see Table 1). The most common medical diagnosis in the data set was multiple sclerosis (36%), followed by spinal cord injury (32%), muscular dystrophy (23%), and postpolio syndrome (9%). Compared with the U.S. general population (M: 50, SD: 10), participants reported more physical impairment (M = 37.0, SD = 11.1) and greater pain interference (M = 56.2, SD = 10). About 33% of participants were employed, and the mean working hours for pay among employed participants was 33 hr (SD = 14.2). The number of participants unaware of RSE significantly increased in Waves 2 and 3 compared with Wave 1 (p < .001), leading to lower mean scores in subsequent waves. However, among those aware of RSE, the mean score slightly increased in the following waves (p < .001), indicating that although overall awareness declined, individuals with prior awareness may have enhanced their understanding or engagement, contributing to a widening disparity. Participants who dropped out of the study were generally similar to those who remained, with age being the only notable difference, as individuals who turned 65 were excluded from the study.
Demographic Characteristics of Participants (2,460 Observations Across 920 Individuals).
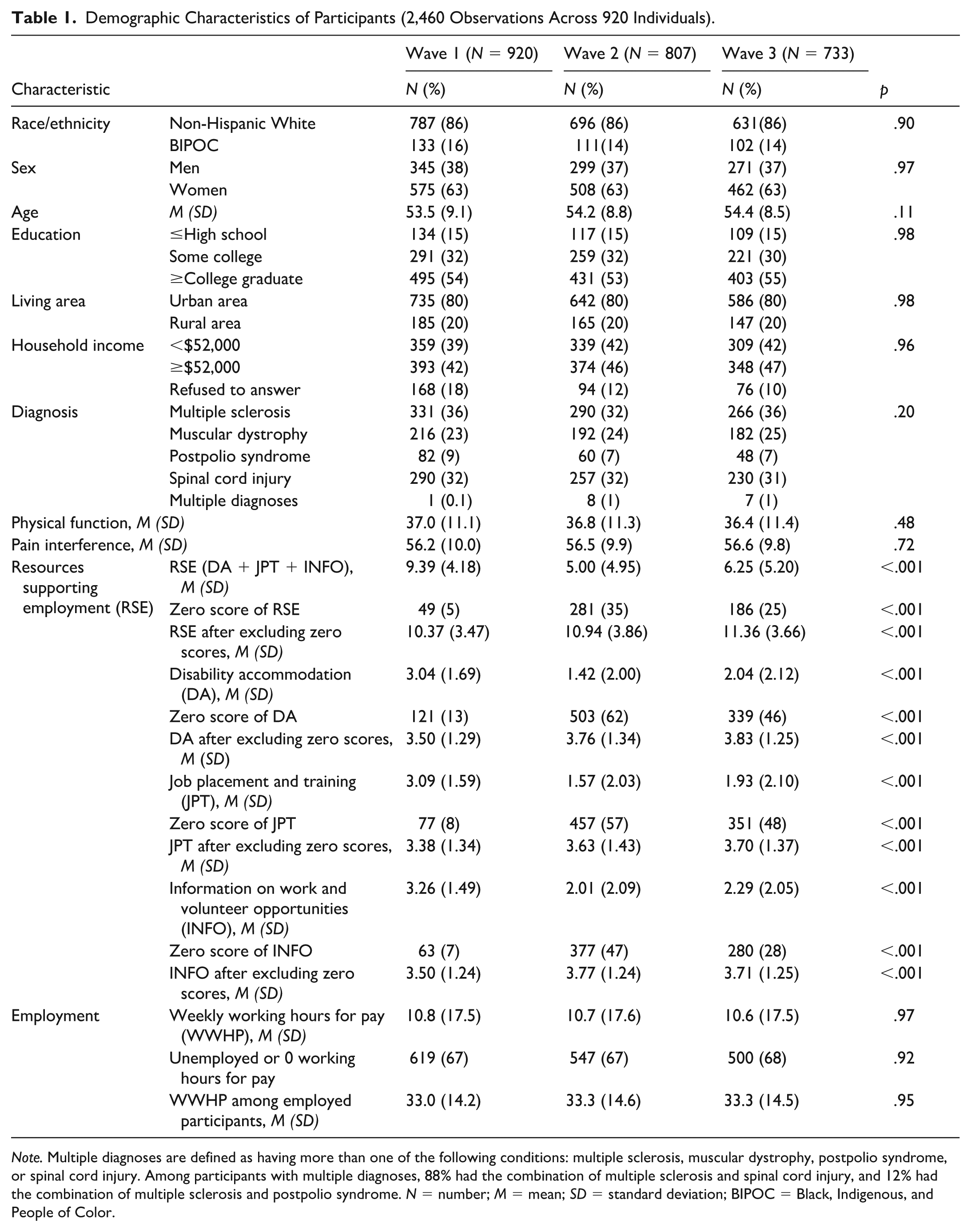
Note. Multiple diagnoses are defined as having more than one of the following conditions: multiple sclerosis, muscular dystrophy, postpolio syndrome, or spinal cord injury. Among participants with multiple diagnoses, 88% had the combination of multiple sclerosis and spinal cord injury, and 12% had the combination of multiple sclerosis and postpolio syndrome. N = number; M = mean; SD = standard deviation; BIPOC = Black, Indigenous, and People of Color.
The Distribution of RSE by Demographic Characteristics
Model 1 in Table 2 displays the level of awareness and availability of RSE by race/ethnicity, sex, age, education, living location, and household income, adjusted for diagnosis type, physical function, pain interference, and data collection wave. Older age, fewer years of formal education, and low household income were associated with lower awareness of RSE. Specifically, being 1 year older was associated with a 4% increase in the odds of unawareness of RSE. In contrast, participants with a high household income and a college degree or higher reported 44% and 60% greater awareness of RSE, respectively, compared with their respective reference groups. Living location did not exhibit significant associations with awareness of RSE.
The Level of RSE, DA, JPT, and INFO by the Demographic Characteristics Among People With Disabilities.
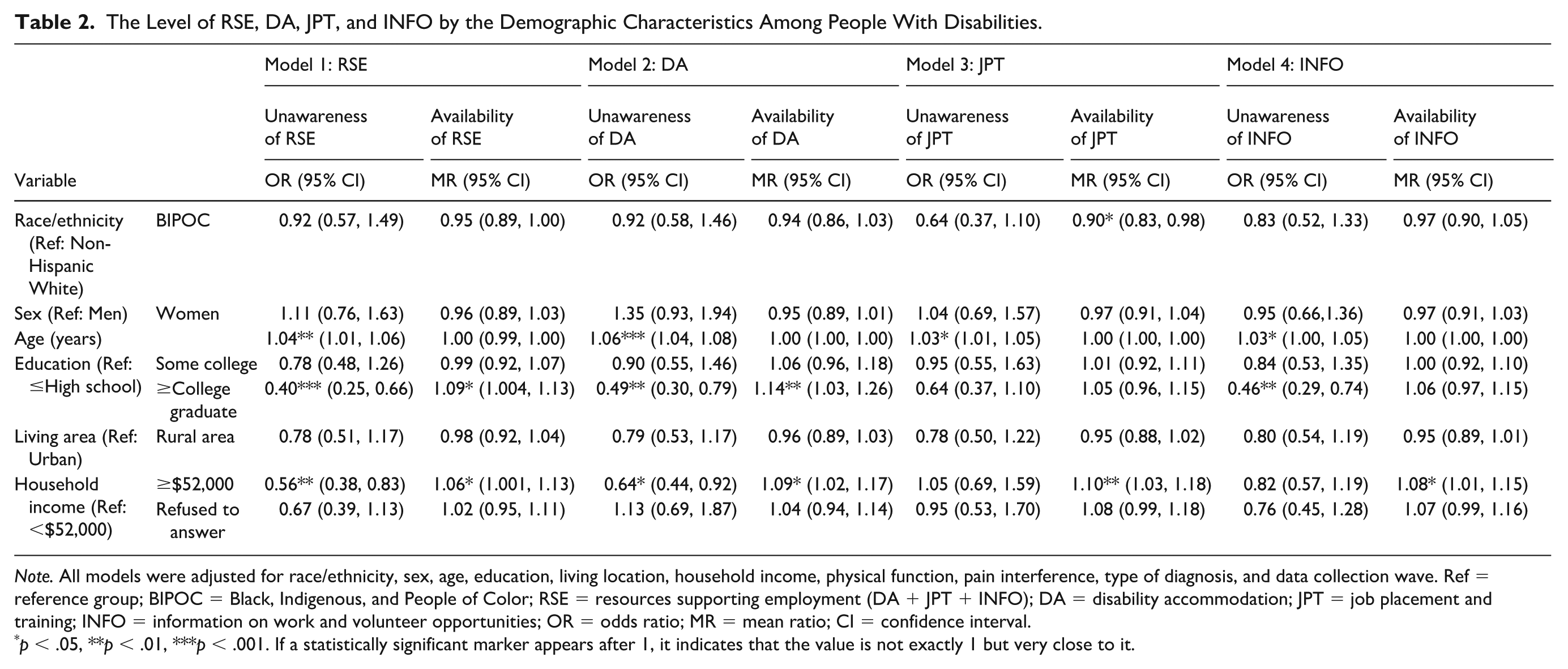
Note. All models were adjusted for race/ethnicity, sex, age, education, living location, household income, physical function, pain interference, type of diagnosis, and data collection wave. Ref = reference group; BIPOC = Black, Indigenous, and People of Color; RSE = resources supporting employment (DA + JPT + INFO); DA = disability accommodation; JPT = job placement and training; INFO = information on work and volunteer opportunities; OR = odds ratio; MR = mean ratio; CI = confidence interval.
p < .05, **p < .01, ***p < .001. If a statistically significant marker appears after 1, it indicates that the value is not exactly 1 but very close to it.
In terms of RSE availability, PWD with a college degree or higher reported 9% greater RSE availability (MR = 1.09, 95% CI = [1.004, 1.13]) compared to those with a high school education or less. Participants with high household income, compared to those with low household income, reported greater RSE availability (MR = 1.06, 95% CI = [1.001, 1.13]). However, race/ethnicity, sex, age, and living area were not significantly associated with perceived RSE availability.
Models 2–4 in Table 2 depict levels of DA, JPT, and INFO by demographic characteristics. Disability accommodation followed a pattern similar to RSE in Model 1. Older age was associated with greater unawareness of JPT and INFO. Black, Indigenous, and People of Color participants had lower JPT availability than non-Hispanic White participants. Education was associated only with unawareness of INFO, whereas household income was linked to availability—but not unawareness—of JPT and INFO.
The Distribution of Employment by Demographic Characteristics
After adjusting for physical function, pain interference, disability diagnosis, and data collection wave, a number of demographic characteristics were associated with unemployment and hours worked for pay (see Model 5 in Table 3). Women reported fewer weekly paid working hours than men (MR = 0.83, 95% CI = [0.72, 0.96]). Older age was linked to higher unemployment odds (OR = 1.40, 95% CI = [1.24, 1.58]) and slightly fewer paid working hours (MR = 0.99, 95% CI = [0.98, 0.99]). People with disabilities with some college education or a college degree or higher had lower odds of unemployment (OR = 0.09, 95% CI = [0.01, 0.97]) and (OR = 0.004, 95% CI = [0.00, 0.04]), respectively, compared with those with a high school education or less.
The Association Between Weekly Working Hours for Pay and Demographic Characteristics Among People With Disabilities.
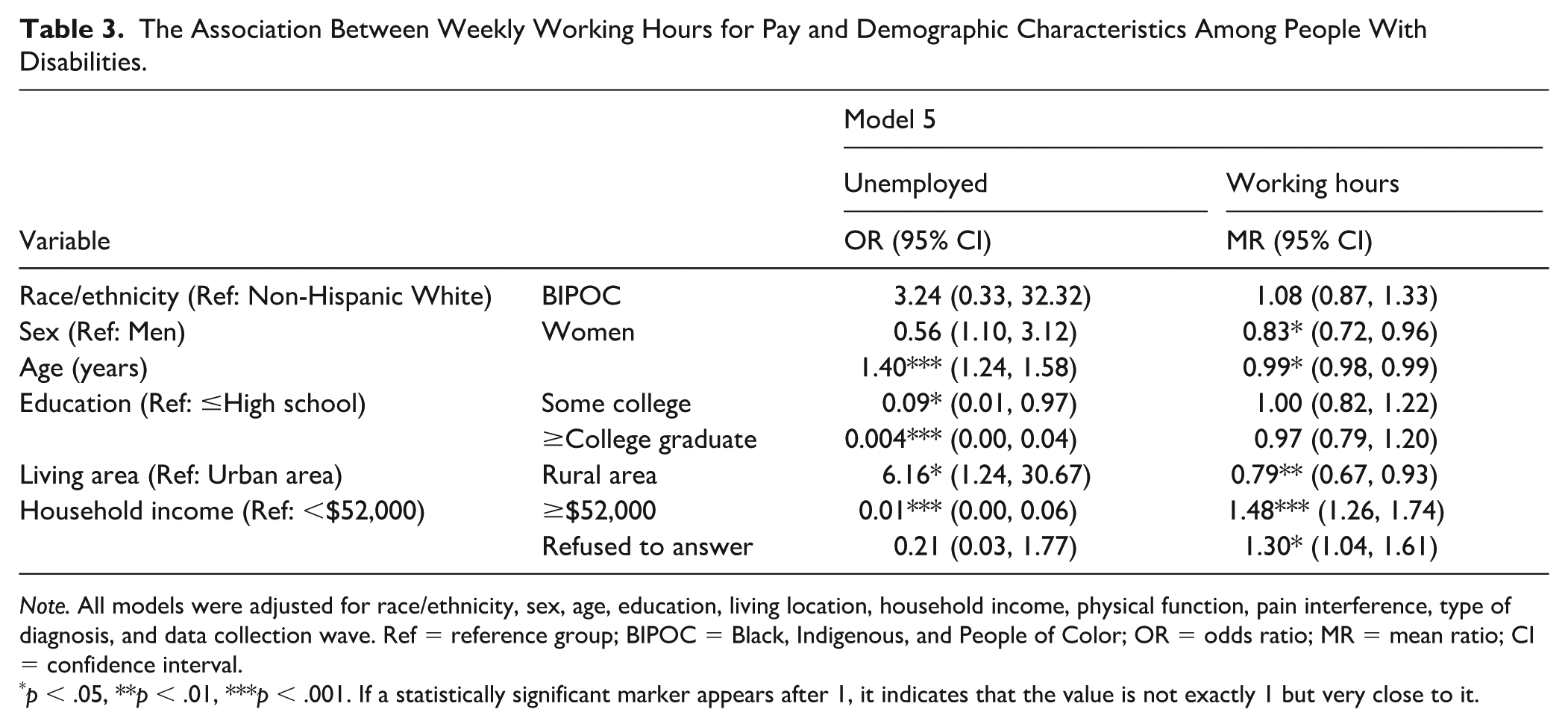
Note. All models were adjusted for race/ethnicity, sex, age, education, living location, household income, physical function, pain interference, type of diagnosis, and data collection wave. Ref = reference group; BIPOC = Black, Indigenous, and People of Color; OR = odds ratio; MR = mean ratio; CI = confidence interval.
p < .05, **p < .01, ***p < .001. If a statistically significant marker appears after 1, it indicates that the value is not exactly 1 but very close to it.
Low household income or rural residence was linked to higher unemployment and fewer working hours compared with their respective reference groups.
The Impact of RSE on Employment
Table 4 indicates the concurrent and lagged effects of RSE on employment. In concurrent model, the availability of RSE, measured as a total score, was associated with lower levels of unemployment (OR = 0.88, 95% CI = [0.81, 0.94]), but not working hours (MR = 1.00, 95% CI = [0.99, 1.01]), after adjusting for physical function, pain interference, a type of diagnosis, and data collection waves (see Model 6A in Table 4). Models 7–9 display effects for DA, JPT, and INFO, respectively. Analyzing the three types of RSE individually, only DA significantly influenced employment, associated with lower unemployment (OR = 0.61, 95% CI = [0.51, 0.73]) but not working hours (MR = 1.00, 95% CI = [0.99, 1.01]). Remarkably, the lagged effect model revealed more pronounced results. Resources supporting employment (OR = 0.61, 95% CI = [0.46, 0.81]), DA (OR = 0.20, 95% CI = [0.09, 0.44]), and INFO (OR = 0.38, 95% CI = [0.16, 0.91]) were associated with lower unemployment levels, and higher DA scores were associated with longer working hours for pay (MR = 1.10, 95% CI = [1.05, 1.16]).
Effects of RSE, DA, JPT, and INFO on Weekly Working Hours for Pay Among People With Disabilities.
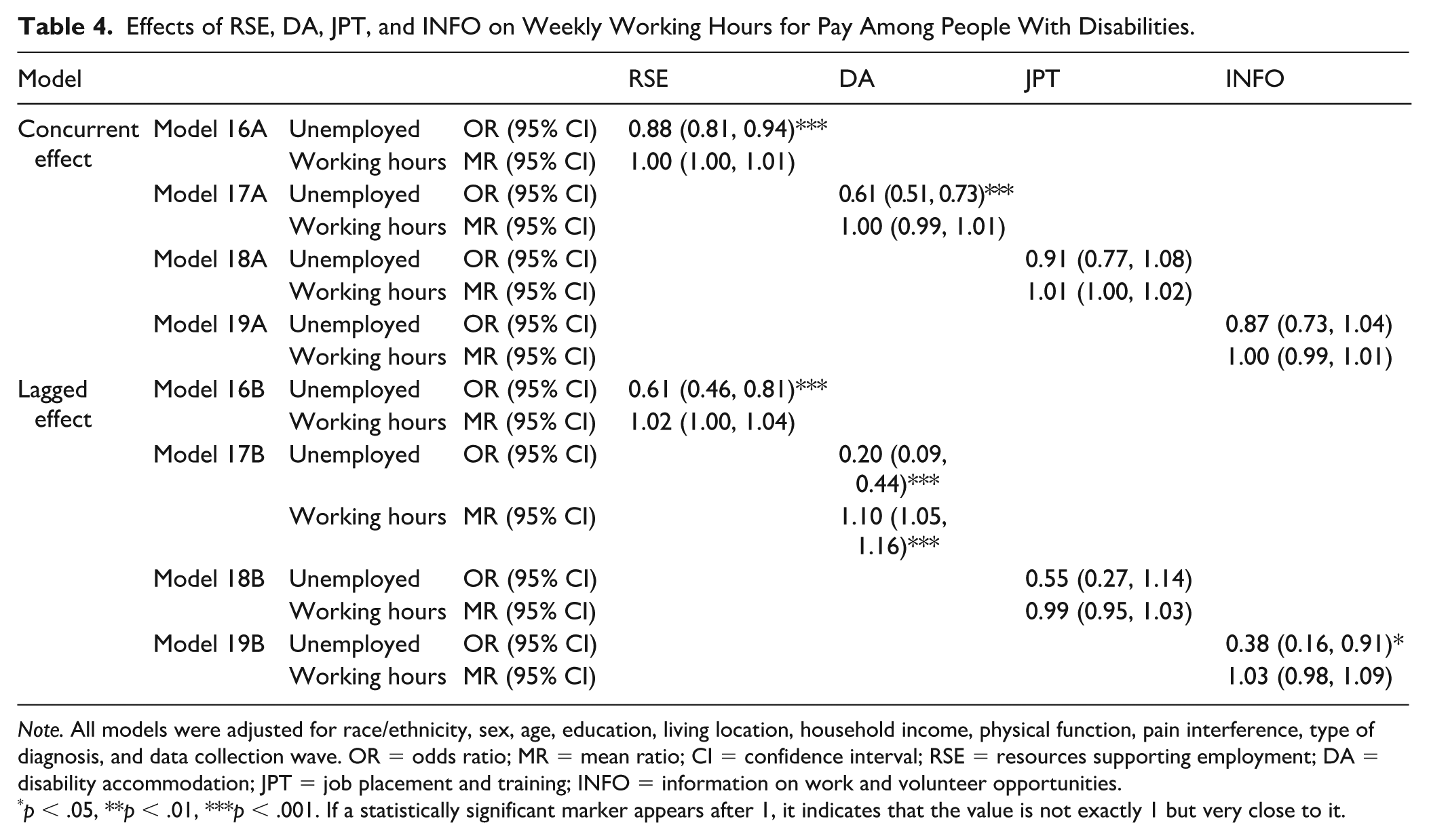
Note. All models were adjusted for race/ethnicity, sex, age, education, living location, household income, physical function, pain interference, type of diagnosis, and data collection wave. OR = odds ratio; MR = mean ratio; CI = confidence interval; RSE = resources supporting employment; DA = disability accommodation; JPT = job placement and training; INFO = information on work and volunteer opportunities.
p < .05, **p < .01, ***p < .001. If a statistically significant marker appears after 1, it indicates that the value is not exactly 1 but very close to it.
Interaction Between RSE and Demographic Characteristics on Employment
No significant interaction was found between individual demographic characteristics and RSE on employment or weekly paid working hours in the concurrent model. However, in the lagged effect model, significant interactions emerged between RSE and education, as well as RSE and high household income (see Supplemental Figure A2). As shown in the figure, increases in RSE were associated with larger gains in employment among PWD with higher levels of education or higher household income, compared to those with lower education or income. In other words, the positive effect of RSE on employment was stronger for PWD who had more educational and economic resources. Similar patterns were observed for DA and INFO.
Figure 1 summarizes how education, household income, and RSE jointly relate to employment (color version available in Supplemental Figure A3). Among PWD with a college degree or higher, the likelihood of employment increased as RSE increased, with substantially larger gains among those with higher household income (see Figure 1A). For example, individuals with higher income showed sharp increases in employment at higher RSE levels, while those with lower income experienced much smaller changes. Among individuals with some college education, employment gains were more modest and were primarily observed among those with higher household income. Across all RSE levels, employment remained very low among individuals with a high school education or less, as well as among those with only some college and lower or unreported household income. Comparable patterns were observed for DA and INFO (see Figure 1B and C).
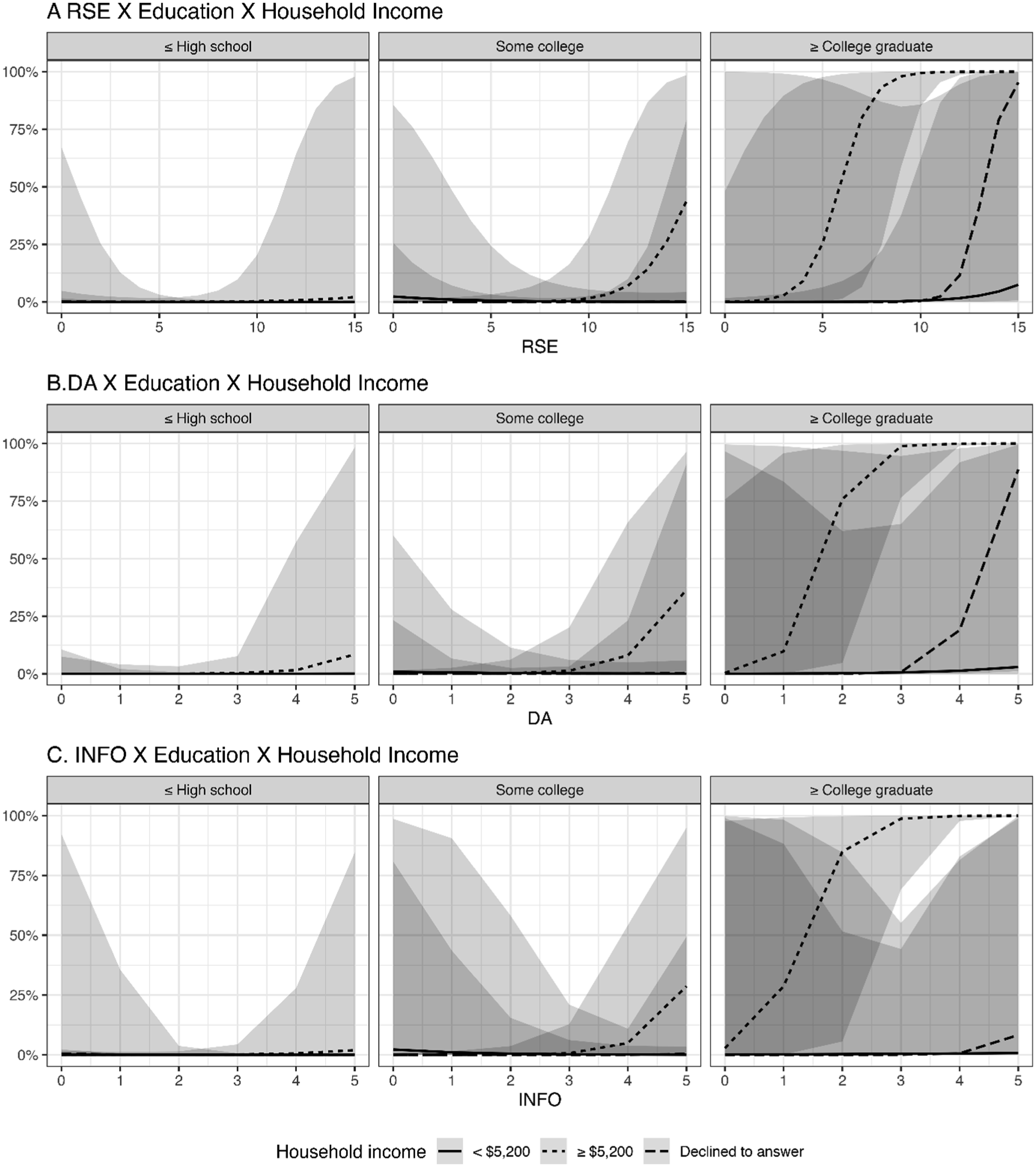
Predicted probability of employment after 1 or 2 years.
Main Reason for Not Working by Demographic Characteristics
Table 5 presents the associations between demographic characteristics and the primary reasons for not working among participants with disabilities. Black, Indigenous, and People of Color participants were significantly more likely to report being unable to work due to health reasons (OR = 5.79, 95% CrI = [1.48, 26.36]). Women more frequently cited caregiving responsibilities as their reason for not working. Increasing age was associated with higher odds of being retired (OR = 1.63, 95% CrI = [1.43, 1.88]) or receiving a disability pension (OR = 1.11, 95% CrI = [1.05, 1.19]). Compared with participants with a college degree or higher and high household income, those with similar education but low household income had greater odds of reporting health-related work limitations (OR = 9.36, 95% CrI = [1.37, 67.27]) and receiving a disability pension (OR = 10.66, 95% CrI = [2.18, 53.38]) rather than caregiving responsibilities. Participants with lower education and income (some college or less and household income less than $52,000) showed the strongest associations of all groups, being substantially more likely to report not working due to health limitations (OR = 43.23, 95% CrI = [8.38, 276.67]) or receiving a disability pension (OR = 21.58, 95% CrI = [5.10, 102.82]).
Associations Between Demographic Characteristics and Reported Main Reasons for Not Working.
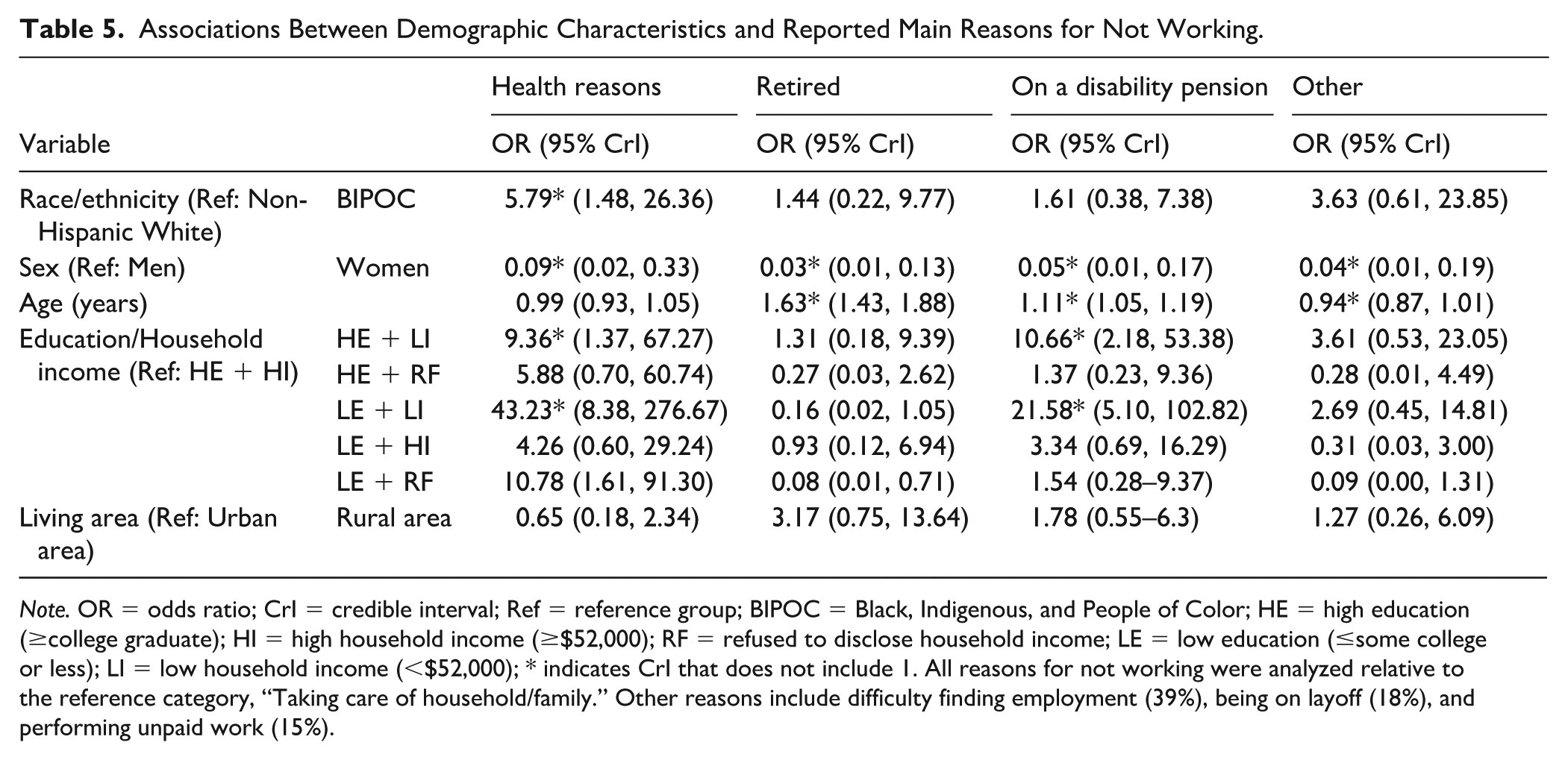
Note. OR = odds ratio; CrI = credible interval; Ref = reference group; BIPOC = Black, Indigenous, and People of Color; HE = high education (≥college graduate); HI = high household income (≥$52,000); RF = refused to disclose household income; LE = low education (≤some college or less); LI = low household income (<$52,000); * indicates CrI that does not include 1. All reasons for not working were analyzed relative to the reference category, “Taking care of household/family.” Other reasons include difficulty finding employment (39%), being on layoff (18%), and performing unpaid work (15%).
Discussion
This study examined longitudinal disparities in employment among PWD, focusing on the role of RSE as well as demographic characteristics and their intersections. Interpreting these findings requires recalling the distinction between RSE availability, defined as the presence and structural reach of services, and RSE awareness, which captures individuals’ knowledge of and perceived relevance of those services (Levesque et al., 2013). Findings highlight significant differences in employment outcomes by education, household income, and RSE.
Intersection of Education, Household Income, and RSE in Shaping Employment Outcomes
Overall, the findings of the three-way interaction indicate that the impact of RSE on employment was particularly pronounced at the intersection of education and household income, suggesting that the benefits of RSE are conditioned by these intersecting socioeconomic factors. This pattern highlights that PWD with higher educational attainment and greater financial resources are better positioned to access and leverage available services, resulting in more favorable employment outcomes. After accounting for physical health, greater RSE availability was associated with higher employment rates—but not with hours worked. People with disabilities with lower educational attainment or lower income reported reduced awareness and availability of RSE, which contributed to varied employment outcomes. Those with a bachelor’s degree or higher and high income had the highest likelihood of being employed 1 to 2 years later. Disability accommodation followed a similar pattern, while INFO effects were weaker.
These results align with prior studies showing that PWD with higher education are more likely to receive vocational rehabilitation counseling (Kaya et al., 2023), perceive the necessity of workplace accommodations (Gignac et al., 2015), utilize accommodations (Zwerling et al., 2003), and be employed (Borg et al., 2021; Degeneffe et al., 2023). In contrast, low-income PWD are less likely to complete vocational rehabilitation programs, more likely to experience unemployment, and more likely to rely on basic income support (Borg et al., 2021; Kaya et al., 2023; Reims & Tophoven, 2021). Limited community resources and concerns about losing government benefits may reduce motivation to seek employment (Ottomanelli et al., 2020).
Reasons for not working also reflected intersecting disadvantages. Compared with high-education/high-income PWD, those with high education but low income and those with both low education and low income were more likely to report health limitations or receipt of disability pensions as barriers. The low-education/low-income group showed the strongest associations. These patterns are consistent with findings from Norway, where individuals with lower education experience shorter work durations and more years lost to illness or disability (Nagarajan & Sixsmith, 2023).
These findings suggest that lower education and income may create structural barriers to employment. Jobs available to individuals with lower education are often physically demanding and require greater health capacity. They typically provide fewer accommodations and limited health insurance, and wages or benefits may be similar to those offered by disability pensions, creating a potential benefit cliff—a situation where earning more income could lead to losing eligibility for existing benefits—reducing financial incentives to work (Hyseni et al., 2024; Schudde & Bernell, 2019; U.S. Government Accountability Office, 2024). Together, these structural barriers likely contribute to lower RSE awareness and reduced employment among PWD with lower education and income.
Taken together, these findings can be interpreted through an intersectionality lens, highlighting how multiple axes of social inequality—disability, class, and educational opportunity—intersect to shape employment outcomes. People with disabilities situated at more privileged intersections (e.g., higher income and education) benefit from cumulative social advantages that facilitate access to RSE and competitive employment. Conversely, PWD at the intersections of low education and economic disadvantage face compounded structural barriers, including limited access to information, fewer opportunities for training, and greater exposure to bias in hiring and accommodation processes. These interlocking disadvantages illustrate how ableism and class inequality operate simultaneously, constraining employment opportunities for low-income, low-educated PWD.
Three Types of RSE
Stratified analyses highlight DA as a critical factor influencing employment outcomes. Disability accommodation significantly affected both employment and working hours 1 to 2 years later, whereas INFO (information on work and volunteer opportunities) exhibited a lagged effect on employment only. Although previous research emphasizes the role of JPT and INFO in supporting employment (Dutta et al., 2008), DA appeared to eclipse these effects in this data set. Disparities in DA and INFO were observed across intersections of education and household income: awareness of INFO varied by education, whereas its availability varied by income, while both the awareness and availability of DA varied by education and income.
Common accommodations included flexible schedules and transportation, more frequently reported among individuals with higher education (Anand & Sevak, 2017). During COVID-19, PWD receiving accommodations were more likely to have higher education and income (Job Accommodation Network, 2020), partly due to occupational differences—telework was more accessible in white-collar roles (Kruse et al., 2022). Physical job demands also shaped employment trajectories; white-collar workers with spinal cord injuries often returned to previous positions, whereas manual workers shifted to less demanding roles (Borg et al., 2021). Definitions of “reasonable accommodations” vary by occupation; in one U.S. case, a cashier with osteoporosis was denied a request to sit due to perceived productivity concerns (Hoffman, 2023).
Age and RSE Awareness
Although RSE availability did not differ by age, older PWD were more likely to be unaware of RSE. They also had lower employment rates and worked fewer hours. Common reasons for not working included retirement and disability pensions, reflecting reduced attachment to the labor force and lower engagement with employment resources. A longitudinal study found that work loss among older adults increasingly stemmed from health-related issues such as long-term sickness leave and transitions to disability pensions (Merkus et al., 2024). Age-related discrimination during job transitions and hiring (Leinonen et al., 2019; Nangia & Arora, 2021) may intensify these challenges.
Race/Ethnicity, Sex, and Living Location
Resources supporting employment awareness and availability were not associated with race/ethnicity, sex, or living location. Our findings comparing BIPOC PWD to non-Hispanic Whites should be interpreted with caution, given the relatively small proportion of BIPOC participants in the sample (14%–16%), which may have limited statistical power and precision. Within this context, our findings indicate that BIPOC PWD reported significantly lower JPT availability, and their employment rates were lower than those of non-Hispanic Whites, although this difference was not statistically significant. These patterns are consistent with previous studies indicating that BIPOC experience higher employment instability (Lu et al., 2023), higher rates of unemployment after age 50 regardless of education (Moen et al., 2022), and a lower likelihood of receiving interview callbacks (Quillian et al., 2017). In addition, BIPOC PWD more frequently cited health limitations rather than caregiving responsibilities as reasons for not working compared with non-Hispanic Whites; however, replication with larger samples is needed to confirm the stability of these findings.
Women with disabilities worked fewer hours than men, likely due to caregiving responsibilities. Gender differences in working hours emerge in early adulthood and widen over the life course (Merkus et al., 2024), as women continue to shoulder the majority of care work (Chandola & Rouxel, 2021; Moen et al., 2022). Similar gendered patterns were observed among individuals with spinal cord injuries (Borg et al., 2021). Employment outcomes were also poorer in regions with lower overall employment rates (Leinonen et al., 2019), although these regional differences were not associated with RSE availability or reasons for not working.
Strengths and Limitations
Strengths include a high response rate (81%–93%) and longitudinal assessment of RSE-related employment disparities among PWD. Examining reasons for not working by demographic characteristics while accounting for repeated measures provides nuanced insight into barriers faced by marginalized groups. Limitations include the convenience sampling method and the small proportion of BIPOC participants (14%–16%), which significantly limit generalizability and may affect the validity of conclusions regarding racial and ethnic disparities. The small BIPOC sample may have reduced statistical power to detect differences, potentially underestimating the magnitude of racial and ethnic effects. Consequently, while observed associations suggest disparities, these findings should be interpreted cautiously and may not fully reflect the experiences of BIPOC PWD in the broader population. In addition, medical diagnoses vary by sex and race/ethnicity; for example, multiple sclerosis is more prevalent among women and White individuals (National Multiple Sclerosis Society, n.d.), Duchenne muscular dystrophy among White men (Salzberg et al., 2018), and postpolio syndrome among women (Oluwasanmi et al., 2019). Because this study focused on specific disability groups, the findings may not be fully generalizable to other disability populations or regional contexts; however, the observed patterns—particularly those related to caregiving, health-related barriers, and labor market conditions—likely reflect broader structural constraints affecting employment among many PWD. Finally, employment measures may not fully capture job quality, such as low-wage, temporary, or unincorporated self-employment versus full-time positions, which may further influence the interpretation of employment outcomes across demographic groups.
Conclusion
This study shows that people with physical disabilities at the intersection of low education and low income face compounded barriers to employment rooted in structural disadvantage. From these data, it appears that health limitations, low-wage labor markets, and constrained access to RSE may conjointly limit participation in competitive employment. These patterns reflect not individual deficits but institutional conditions, including the persistence of an “ideal worker” norm in job design that assumes minimal health, functional, or caregiving responsibilities, systematically disadvantaging marginalized workers (Foster & Wass, 2013).
Best practices for rehabilitation counselors include the incorporation of vocational assessments that consider education and economic precarity, while also evaluating job quality to support sustainable employment. Providing long-term, sustainable career pathways enables low-income, low-educated PWD to acquire new skills, build career progression, and transition into more stable employment without sacrificing current earnings. At the systems level, vocational rehabilitation agencies can continue efforts to expand outreach in disadvantaged communities and to partner with employers to increase inclusive opportunities. Employers can further promote equity by embedding universal design and accommodations into standard workplace practices rather than treating them as exceptional. At the larger policy level, there remains a need for programs prioritizing low-income, low-educated PWD, incentivizing inclusive hiring, and addressing the “benefit cliff,” to allow PWD to pursue higher earnings or flexible work without losing access to health care. Together, these coordinated actions across counselors, agencies, employers, and policymakers can promote equitable, sustainable employment opportunities for marginalized PWD.
Future research should explore access to RSE, examine racial and ethnic differences with greater statistical power, and conduct qualitative studies to clarify the mechanisms underlying RSE awareness, ultimately illuminating how structural systems, rather than individual limitations, reproduce employment disparities among PWD.
Supplemental Material
sj-docx-1-rcb-10.1177_00343552261453377 – Supplemental material for Intersecting Marginalized Identities Among People With Disabilities: Impact on Access to Employment Support Resources and Employment Outcomes
Supplemental material, sj-docx-1-rcb-10.1177_00343552261453377 for Intersecting Marginalized Identities Among People With Disabilities: Impact on Access to Employment Support Resources and Employment Outcomes by Suyoung Kwon and Ivan R. Molton in Rehabilitation Counseling Bulletin
Footnotes
Acknowledgements
The authors would like to express our appreciation for the assistance of Dr. Andrew Humbert in statistical support and the efforts of Rana Salem in data management, both from the Department of Rehabilitation Medicine at the University of Washington. They are also thankful to the participants who generously volunteered their time and contributed their valuable data for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this report were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number H133B130018, 90ARPO0003). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this report do not necessarily represent the policy of NIDILRR, ACL, or HHS, and you should not assume endorsement by the Federal Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.