
Abstract
Objective
This study aimed to evaluate the associations and discriminative performance of TyG-derived composite indices compared to the cholesterol–HDL-C–glucose (CHG) index system for frailty.
Methods
In this cross-sectional study, we examined five consecutive cycles (2009-2018) of the National Health and Nutrition Examination Survey. After excluding participants with incomplete data, 10,311 adults were included. We calculated TyG, CHG, and their adiposity-adjusted composite indices. To assess associations with frailty, we used multivariable logistic regression and applied restricted cubic splines to evaluate potential nonlinearity. Discriminative performance was assessed using receiver operating characteristic curves, with AUC values compared using paired DeLong tests. Incremental discrimination analyses using ΔAUC and net reclassification improvement (NRI) were also performed.
Results
In fully adjusted models, both higher TyG-derived indices and the CHG index system (along with its composite indices) were consistently associated with increased odds of frailty. Among all indices, body-roundness-related composites demonstrated the best discrimination. Specifically, TyG-BRI (AUC 0.706) and CHG-BRI (AUC 0.700) outperformed their individual metabolic markers, TyG (AUC 0.630) and CHG (AUC 0.588), respectively, indicating moderate overall discriminative ability. Incremental discrimination analyses demonstrated that TyG-BRI and CHG-BRI offered enhanced discriminative value compared to their respective base metabolic markers. Sensitivity analyses confirmed the robustness of these findings.
Conclusions
TyG- and CHG-derived composite indices, particularly TyG-BRI and CHG-BRI, were positively associated with frailty. They demonstrated moderate discriminative performance and superior ability compared to individual metabolic markers for identifying prevalent frailty. However, due to the cross-sectional nature of NHANES, these indices should be regarded as adjunctive markers rather than stand-alone frailty screening tools. Prospective studies are required to further assess their potential adjunctive clinical value.

1. Introduction
Frailty is a complex clinical syndrome that encompasses multiple dimensions, marked by a diminished physiological reserve and heightened susceptibility to stressors.1,2 Accumulating evidence indicates a close association between frailty and both age-related functional decline and metabolic dysregulation. The latter encompasses insulin resistance, abnormal glucose and lipid metabolism, chronic low-grade inflammation, oxidative stress, and unfavorable body fat distribution.3,4 These metabolic disturbances can hinder skeletal muscle metabolism, lead to an accelerated decline in muscle mass and function, and increase systemic vulnerability, thereby playing a significant role in the onset of frailty.5–7 There is growing interest in identifying simple, scalable metabolic markers to characterize frailty risk in population-based settings.8–10
Derived from fasting triglyceride and glucose levels, the triglyceride–glucose (TyG) index is a common non-insulin-based surrogate marker for insulin resistance. It has also been linked to frailty across various populations.11,12 However, frailty is not driven solely by insulin resistance or hypertriglyceridemia. Increasing evidence indicates that central and visceral adiposity, body fat redistribution, and altered body composition also play important roles in frailty pathogenesis.13–15 Composite indices that integrate the TyG index with anthropometric or adiposity-related measures—such as TyG-BRI, TyG-ABSI, TyG-WWI, and TyG-CVAI—may more effectively capture the combined metabolic and body composition abnormalities associated with frailty compared to the TyG index alone. 16 Nevertheless, the associations of these TyG-derived composite indices with frailty have not been thoroughly explored.
In addition to the TyG framework, the cholesterol–high-density lipoprotein cholesterol–glucose (CHG) index is a recently proposed composite metabolic indicator that incorporates total cholesterol, HDL-C, and fasting blood glucose. 17 Unlike the TyG index, the CHG index incorporates cholesterol-related data, potentially allowing it to capture a broader spectrum of glucose–lipid metabolic phenotypes. This broader scope is particularly relevant to frailty, given that HDL dysfunction, abnormal cholesterol metabolism, and lipid-related inflammatory or oxidative pathways can all contribute to muscle dysfunction, impaired physiological resilience, and the progression of the condition.4,18–20 Therefore, CHG and its derived indices may offer supplementary or complementary insights beyond TyG-based indices for identifying frailty. However, evidence regarding the associations and discriminatory effectiveness of the CHG index and its derivatives in relation to frailty remains insufficient.
Utilizing data from the National Health and Nutrition Examination Survey (NHANES), we employed multivariable logistic regression, restricted cubic splines (RCS), subgroup analyses, and sensitivity analyses. Furthermore, receiver operating characteristic curves were compared to evaluate the associations and discriminatory capabilities of TyG-derived indices, the CHG index, and CHG-derived indices in relation to frailty. Our aim was to provide scalable metabolic markers for frailty identification and to evaluate their discriminative performance in adults.
2. Methods
2.1. Cross-sectional study design and data sources and processing
This study employed data from the National Health and Nutrition Examination Survey (NHANES), which encompasses five consecutive cycles from 2009 to 2018. NHANES is conducted by the National Center for Health Statistics (NCHS) and has undergone review and approval by its Institutional Review Board. All participants provided written informed consent prior to their involvement in the study. 21 This study was conducted in accordance with the ethical principles of the Declaration of Helsinki (1975), as revised in 2024. The Ethics Committee of the Affiliated People’s Hospital of Fujian University of Traditional Chinese Medicine waived the requirement for ethical approval, as the NHANES database is publicly accessible and comprises fully de-identified data. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 22
Figure 1 illustrates the participant selection process. Initially, 49,693 individuals from NHANES 2009–2018 were evaluated. After excluding 34,490 participants due to missing TyG index data, 15,203 individuals remained eligible for the study. From this group, we further excluded participants with missing data on key covariates: education (N = 2,694), marital status (N = 5), alcohol use (N = 981), smoking status (N = 6), and poverty–income ratio (PIR) (N = 1,206). These exclusions resulted in a final analysis cohort of 10,311 participants, comprising 2,327 individuals with frailty and 7,984 non-frail individuals. Flowchart of participant selection. TyG index, triglyceride–glucose index; PIR, poverty–income ratio.
2.2. Definition of primary variables
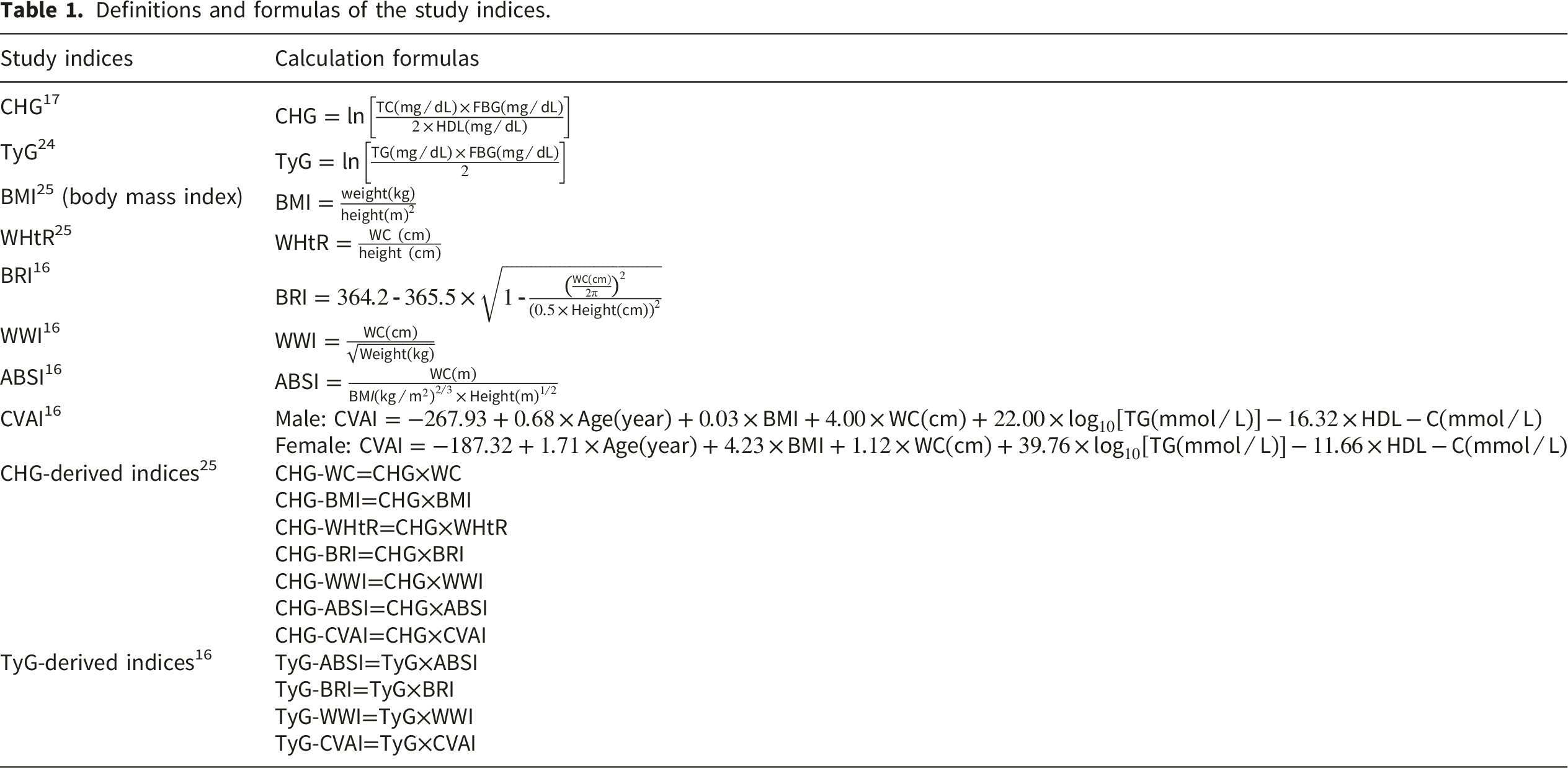
Definitions and formulas of the study indices.
Frailty status was established as the primary outcome of this study. We assessed frailty utilizing a Frailty Index (FI) derived from 49 deficit indicators (Supplementary Table S1), which quantifies the cumulative burden of physiological impairments. These deficit indicators encompass various domains, such as comorbidities, functional limitations, symptoms, self-reported health conditions, and physiological abnormalities. The FI was calculated by dividing the total number of deficits identified by the total number of items with available data.
Consistent with previous NHANES-based studies, a prespecified cut-point of 0.21 was used to define frailty; participants were categorized as frail (FI ≥ 0.21) or non-frail (FI < 0.21).26–28
2.3. Definition of covariates
The covariates included gender, age, race, educational level, marital status, family income-to-poverty ratio (PIR), smoking status, alcohol consumption, diet quality assessed by the Healthy Eating Index–2020 (HEI-2020), physical activity (PA).
HEI-2020, created by the U.S. Department of Agriculture and the National Cancer Institute, serves to evaluate compliance with the 2020–2025 Dietary Guidelines for Americans. The scoring system ranges from 0 to 100, where higher scores signify superior diet quality. 29
Physical activity was measured in weekly metabolic equivalent task minutes (MET-min/week) by analyzing self-reported leisure-time activities conducted over the previous 30 days in the NHANES study and categorized as sedentary (0 MET-min/week), insufficient (<500 MET-min/week), moderate (500–1000 MET-min/week), or high (>1000 MET-min/week). 30
Income levels were stratified using PIR to reflect socioeconomic status: households with a PIR of 1 or less were classified as low-income, those with a PIR between 1 and less than 4 as middle-income, and those with a PIR of 4 or more as high-income. 31
2.4. Statistical methods
Given the complex, multistage sampling design of NHANES, all statistical analyses utilized the appropriate sampling weights. In line with NHANES analytical guidelines, the original two-year cycle weights were adjusted by dividing them by five (1/5) to accurately reflect the entire 10-year analytical period.32,33
Baseline characteristics were presented as means (mean ± SD) for continuous variables and as N (%) for categorical variables. Unpaired Student's t-tests were employed to compare continuous variables between groups, while chi-square tests were utilized for categorical variables. To assess associations between the study indices and frailty, logistic regression models were fitted as appropriate. The TyG index, CHG index, and their derived indices were analyzed both as continuous variables (per 1-SD increase) and as categorical variables (tertiles).
Model 1 was unadjusted. Model 2 was adjusted for gender, age, race, education, marital status, and PIR. Model 3 was adjusted for various factors, including age, gender, race, education, marital status, PIR, alcohol consumption, smoking status, PA, and the HEI-2020. To investigate potential non-linear dose–response relationships, restricted cubic spline (RCS) functions were employed. Specifically, restricted cubic spline regression was utilized to examine non-linear associations, using three knots positioned at the 10th, 50th, and 90th percentiles of each exposure distribution, with the median value serving as the reference point. 34 Multicollinearity among covariates was assessed using VIFs, with VIF <5 considered acceptable.35,36
To reduce potential bias arising from missing data, multiple imputation was performed utilizing the “mice” package in R. This process generated five imputed datasets, of which the first completed dataset was employed for the subsequent analyses, consistent with previous studies.37,38 To assess the stability of our results, we conducted two sensitivity analyses: (1) an analysis utilizing the unweighted dataset; and (2) an analysis employing the unimputed dataset. Finally, the discriminatory performance of the CHG index, TyG index, and their derived indices for identifying prevalent frailty was evaluated using receiver operating characteristic (ROC) curve analysis, and the area under the curve (AUC) was calculated. The optimal cutoff value was identified by maximizing the Youden index. 39 The incremental predictive value beyond the reference model was further quantified through the use of net reclassification improvement (NRI). 40 A two-sided p value < 0.05 was considered statistically significant. All statistical analyses were performed using R software (version 4.4.1).
3. Results
3.1. Baseline characteristics of participants
Baseline characteristics of participants stratified by frailty status.

HEI, Healthy Eating Index; PA, physical activity; PIR, poverty income ratio; TyG, triglyceride-glucose index; CHG index, cholesterol–high-density lipoprotein cholesterol–glucose index; WC, waist circumference; WHtR, waist-to-height ratio; WWI, weight-adjusted waist index; ABSI, a body shape index; BMI, body mass index; BRI, body roundness index; CVAI, Chinese visceral adiposity index; FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides.
Conversely, high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) were lower in frail participants (both P<0.001), and total cholesterol (TC) was similarly reduced, though with a modest difference (P=0.032). Frail participants also exhibited a higher prevalence of female sex, smoking, low income, and a sedentary lifestyle, while alcohol consumption and high physical activity were less prevalent (all P<0.001). Distributions of race, education, and marital status also differed between groups (all P<0.001).
3.2. Associations of TyG- and CHG-derived indices with frailty
Weighted logistic regression analyses of TyG-derived indices in relation to frailty.

Model 1: non-adjusted model.
Model 2: Adjusted for gender, age, race, education, marital, PIR.
Model 3: Adjusted for gender, age, race, education, marital status, PIR, alcohol consumption, smoking status, PA, and HEI-2020.
TyG, triglyceride–glucose index; PIR, poverty-to-income ratio; PA, physical activity; HEI-2020, Healthy Eating Index–2020.
In continuous analyses, each 1-SD increase in TyG-derived indices was linked to higher odds of frailty in Model 3 (TyG-ABSI OR 1.44; TyG-BRI OR 1.77; TyG-CVAI OR 1.95; TyG-WWI OR 1.73; all P<0.001) (Table 3). Similarly, the CHG index was independently associated with frailty (OR 1.45, P<0.001), and all CHG-derived composites remained significant (CHG-ABSI OR 1.36; CHG-BRI OR 1.74; CHG-CVAI OR 1.90; CHG-WWI OR 1.62; CHG-BMI OR 1.76; CHG-WC OR 1.76; CHG-WHtR OR 1.79; all P<0.001) (Supplementary Table S3).
Tertile analyses further indicated that the differences in the odds of frailty were predominantly observed in the higher categories. In Model 3, Q3 versus Q1 ORs ranged from 2.03 to 3.61 for the TyG system (TyG-ABSI 2.03, TyG-BRI 3.38, TyG-CVAI 3.61, TyG-WWI 2.87; all P<0.001) (Table 3) and from 1.85 to 3.38 for the CHG system (CHG 2.26, CHG-ABSI 1.85, CHG-BRI 3.17, CHG-CVAI 3.38, CHG-WWI 2.41, CHG-BMI 3.36, CHG-WC 3.25, CHG-WHtR 3.30; all P<0.001) (Supplementary Table S3).
3.3. Restricted cubic spline analyses of TyG- and CHG-derived indices in relation to frailty
To better understand the relationships between TyG-related indices, the CHG index system and its derived indices, and frailty, we performed restricted cubic spline (RCS) analyses (Figure 2). Our findings revealed significant nonlinearity for several indices, including TyG-BRI, TyG-WWI, and TyG-ABSI, as well as for CHG and its variations: CHG-ABSI, CHG-BRI, CHG-BMI, CHG-WC, CHG-WHtR, and CHG-WWI (all P for nonlinearity < 0.001). Conversely, no nonlinearity was detected for TyG-CVAI (P for nonlinearity = 0.105) or CHG-CVAI (P for nonlinearity = 0.287). In our RCS analyses, we established the median value for each exposure as the reference point (OR = 1). The specific reference values identified were 44.86 for TyG-BRI, 95.53 for TyG-WWI, 0.71 for TyG-ABSI, 1174.69 for TyG-CVAI, 5.22 for CHG, 0.43 for CHG-ABSI, 27.28 for CHG-BRI, 148.39 for CHG-BMI, 518.32 for CHG-WC, 3.11 for CHG-WHtR, 58.06 for CHG-WWI, and 710.98 for CHG-CVAI. As the values of these indices exceeded their respective thresholds, the likelihood of frailty increased progressively. Furthermore, the overall associations between these indices and frailty were statistically significant (all P < 0.001). Restricted cubic spline analyses of TyG- and CHG-derived indices in relation to frailty. (A) CHG; (B) CHG-ABSI; (C) CHG-BRI; (D) CHG-WHtR; (E) CHG-CVAI; (F) CHG-WC; (G) CHG-BMI; (H) CHG-WWI; (I) TyG-ABSI; (J) TyG-BRI; (K) TyG-WWI; (L) TyG-CVAI. adjusted for all covariates included in Model 3.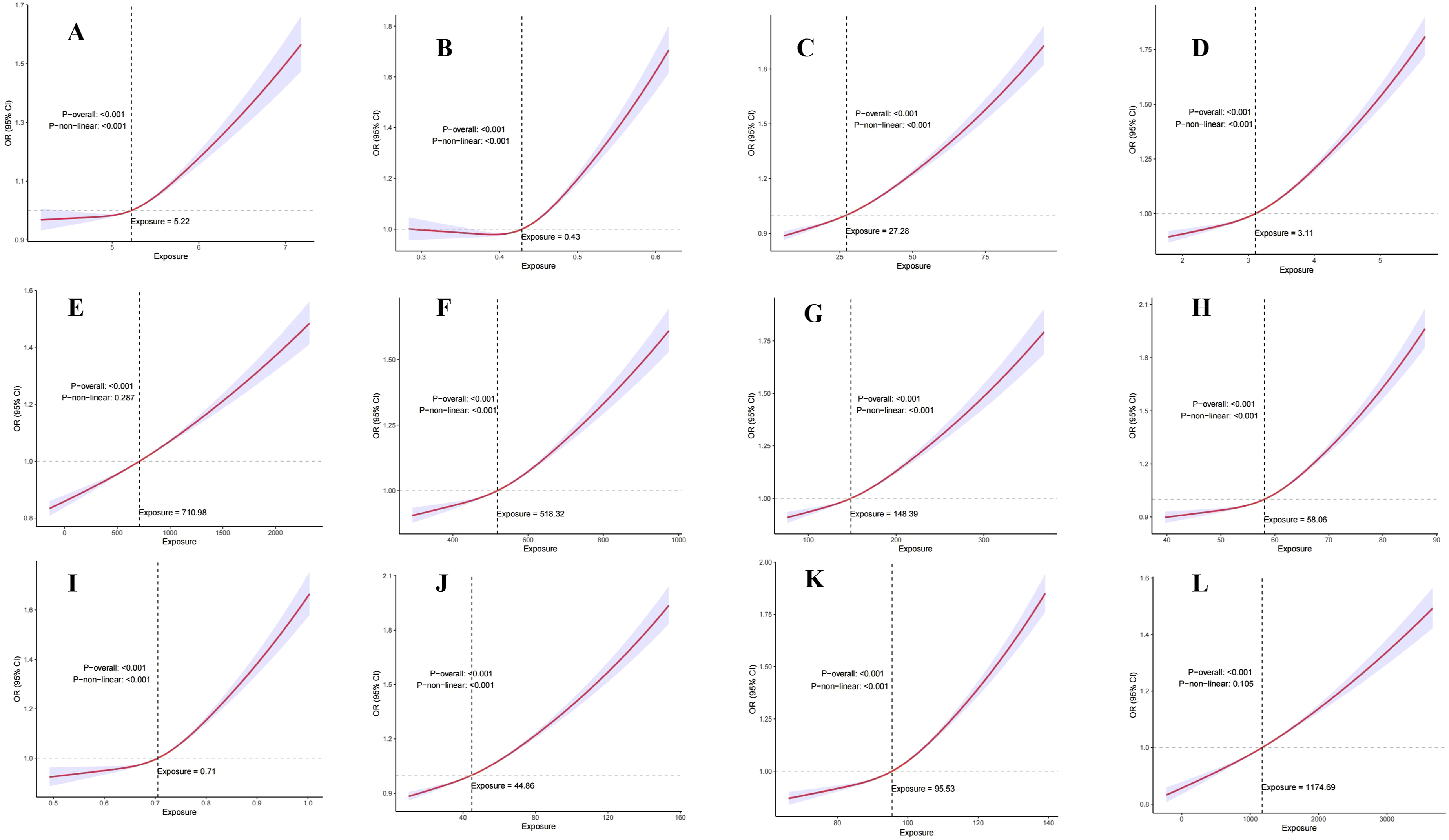
3.4. Subgroup analysis
In subgroup analyses, the associations of the CHG-derived indices and TyG-derived indices with frailty were directionally consistent across strata (all subgroup ORs >1); however, effect sizes varied by participant characteristics (Supplementary Figure 1). Interaction tests indicated that race was the principal effect modifier for both types of indices, with significant race-stratified interactions observed for most indices (P<0.05). Additionally, PA and marital status also exhibited significant effect modification for selected indices (both P<0.05). Beyond race, the CHG index notably showed effect modification by sex and age, while TyG-CVAI exhibited broader effect modification, encompassing sex, smoking, and HEI-2020 (all P<0.05). Overall, while the directions of association remained robust, their magnitudes appeared to be influenced by race, PA, and selected lifestyle and clinical factors.
3.5. Sensitivity analysis
We performed sensitivity analyses to evaluate the robustness of our main findings. Initially, the analyses utilizing the unweighted dataset aligned with the primary survey-weighted models, revealing consistent associations between the TyG, CHG, and their derived indices with frailty (Supplementary Table S4). Second, applying weighted multivariable logistic regression to the unimputed dataset yielded similar estimates, reinforcing the strength of these associations (Supplementary Table S5).
3.6. ROC curve and incremental discrimination analyses
ROC curve analysis was employed to evaluate the discriminative performance of the TyG, CHG, and their composite indices that integrate adiposity in relation to frailty (Figure 3). Overall, composite indices incorporating adiposity-related measures outperformed the single indices in discriminating frailty, and the observed AUC values indicated moderate discriminative ability overall. Among the evaluated metrics, TyG-BRI showed the highest AUC (0.706), followed closely by CHG-BRI (0.700) and TyG-CVAI (0.696); TyG-WWI and CHG-WHtR demonstrated similar performance, with AUCs of 0.692 and 0.691, respectively. In contrast, TyG and CHG yielded lower AUC values of 0.630 and 0.588, respectively. ROC curves comparing the discrimination of the TyG and CHG indices and their derived composites for frailty. ROC, receiver operating characteristic; AUC, area under the curve; TyG, triglyceride–glucose index; CHG, cholesterol–high-density lipoprotein cholesterol–glucose index; BRI, body roundness index; ABSI, a body shape index; WWI, weight-adjusted waist index; CVAI, Chinese visceral adiposity index; BMI, body mass index; WC, waist circumference; WHtR, waist-to-height ratio.
Incremental discrimination analyses (Supplementary Table S6), including DeLong tests, ΔAUC, and NRI, further supported these differences. Using TyG as the reference, all TyG-derived composites yielded higher AUCs than TyG (all P ≤ 0.05), with the largest gains observed for TyG-BRI (ΔAUC = 0.075, NRI = 0.469), TyG-CVAI (ΔAUC = 0.066, NRI = 0.427), and TyG-WWI (ΔAUC = 0.061, NRI = 0.594). Most CHG-derived composites also outperformed TyG (all P < 0.001), while CHG and CHG-ABSI performed worse than TyG (ΔAUC = -0.042 and -0.016, respectively; P < 0.001 and P = 0.005, respectively). Using CHG as the reference, all TyG- and CHG-derived composites showed higher AUCs than CHG (all P < 0.001), with the largest gains observed for TyG-BRI (ΔAUC = 0.117, NRI = 0.578), CHG-BRI (ΔAUC = 0.111, NRI = 0.571), CHG-WHtR (ΔAUC = 0.103, NRI = 0.593), and CHG-WWI (ΔAUC = 0.082, NRI = 0.579). These findings indicate that composite indices integrating adiposity-related information provided additional discriminative value over the corresponding base metabolic markers.
Optimal cut-offs were determined by maximizing the Youden index (Supplementary Table S7). The optimal cut-off for TyG-BRI was 50.20 (Se = 0.642; Sp = 0.678; Youden = 0.319), and that for CHG-BRI was 30.89 (Se = 0.625; Sp = 0.682; Youden = 0.307).
4. Discussion
This study identified strong independent associations between TyG- and CHG-derived composite indices and increased odds of frailty in a nationally representative sample of U.S. adults. Fully adjusted logistic regression models confirmed consistent positive associations in both continuous and tertile-based analyses. Restricted cubic spline analyses demonstrated nonlinear relationships for most indices. ROC comparisons indicated that composite indices incorporating body fat distribution (e.g., TyG-BRI and CHG-BRI) generally outperformed their corresponding base metabolic indices and other derived composites. Incremental discrimination analyses further supported this pattern, revealing that TyG-BRI and CHG-BRI provided greater discriminative value than their base markers. However, AUC values remained around 0.70, reflecting moderate discriminative ability. Therefore, these indices are best considered adjunctive markers, not stand-alone frailty screening tools. Together, these findings suggest that an integrated phenotype of metabolic dysregulation combined with adverse adiposity configuration may enhance the discrimination of frailty status.
Prior studies have consistently suggested that novel anthropometric indices reflecting central and visceral fat burden are stably associated with frailty. An analysis based on NHANES 2007–2018 showed that WWI was significantly and positively associated with frailty and remained independently associated after multivariable adjustment, suggesting that an abnormal accumulation of waist circumference in relation to body weight may more effectively identify body composition phenotypes related to frailty. 13 Similarly, another NHANES study indicated that a higher BRI was linked to an increased prevalence of frailty in older adults, supporting the value of indices that more closely reflect abdominal fat morphology for characterizing gradients of frailty. 14 Concerning measures related to visceral adiposity, a cross-sectional study conducted in rural northwestern China evaluated frailty utilizing the frail scale and found a positive association between CVAI and frailty; this association remained a stable linear positive trend in multivariable logistic regression and RCS analyses. ROC analyses further suggested that CVAI, WHtR, and BRI have discriminatory ability for frailty with some indices showing AUCs superior to traditional waist circumference or BMI, providing direct population-based evidence for the potential utility of CVAI in characterizing frailty. 15
Recent studies have highlighted that integrating metabolic signals with anthropometric data can enhance our understanding of the relationship between fat distribution or body shape and frailty. Using NHANES data, Yin et al. 11 found that higher TyG and its composite indices (TyG-WC, TyG-WHtR, and TyG-BMI) were associated with increased frailty prevalence, and that composite indices often outperformed TyG alone, indicating that the combination of IR-related metabolic burden and central obesity information better captures frailty status. Furthermore, Fu et al. 41 conducted a nationwide prospective cohort study involving individuals with CKM syndrome. Their findings revealed that the TyG-BRI index was significantly linked to the trajectories and progression of frailty. This suggests that TyG-BRI is not only indicative of an individual’s current frailty status but also correlates with longer-term pathways of functional decline. This provides longitudinal evidence supporting a temporal relationship between metabolic-adiposity composite phenotypes and frailty.
Consistent with the above studies, we observed a strong association between TyG-BRI and frailty in a U.S. adult sample, without restrictions based on baseline disease spectrum, suggesting that the association of TyG-BRI with frailty is not confined to specific subgroups and may have broader population applicability. Meanwhile, derived indices that combine the TyG index with body shape and fat distribution measures (TyG-WWI, TyG-CVAI, and TyG-ABSI) continued to demonstrate a significant association with frailty after full adjustment, exhibiting overall effect sizes that were stronger than those of the TyG index alone. These findings indicate that frailty may not be solely attributed to elevated glucose or triglycerides levels; rather, it appears to be more closely associated with central and visceral fat accumulation, as well as body composition remodeling in the context of metabolic dysfunction.42,43
We also integrated CHG and its derived composite indices into frailty research and systematically compared them with the TyG framework. We noted consistently stable positive correlations between CHG-related indices and frailty. This indicates that including HDL-C and cholesterol in our analyses may more effectively capture the lipoprotein-related metabolic abnormalities that are pertinent to frailty. This is particularly significant because HDL dysfunction and abnormal cholesterol homeostasis are associated with compromised anti-inflammatory, antioxidant, endothelial-protective, and lipid-transport functions. These impairments can lead to vascular dysfunction, muscle impairment and a decrease in physiological resilience.18,19,44,45 Notably, ROC results indicated that CHG alone had limited discriminative ability, whereas derived indices integrating CHG with adiposity configuration, particularly CHG-BRI, performed substantially better. This suggests that for frailty, information from a single metabolic axis is insufficient, while the combination of metabolic burden and adverse body-fat distribution may better reflect the multisystem phenotype underlying frailty.1–3
RCS analyses indicated significant nonlinearity between frailty and most TyG/CHG indices and their derivatives. This pattern implies that the association between metabolic burden and frailty may not remain consistent across the entire exposure range. At lower exposure levels, metabolic compensation may help preserve physiological stability; however, at higher exposure levels, the cumulative effects of glucose–lipid dysregulation, inflammation, oxidative stress, and adverse adiposity may be intensified, leading to a more pronounced increase in the odds of frailty.3,4,46 In contrast, tests for nonlinearity yielded insignificant results for TyG-CVAI and CHG-CVAI, suggesting that their relationships with frailty were more aligned with a linear gradient within the observed exposure range.
Subgroup analyses revealed mostly consistent associations; however, race emerged as the primary effect modifier. Additionally, certain indices demonstrated interactions across strata such as physical activity and marital status. This trend may indicate variations among populations in factors such as body fat distribution, muscle mass, insulin sensitivity, lipoprotein profiles, lifestyle choices, and social context.47–50 In other words, identical values of a metabolic-body-shape composite index may correspond to varying levels of visceral fat burden or muscle mass across different populations, contributing to heterogeneity in effect size. Based on these results, future studies should implement stratified calibration and validate population-specific thresholds in external cohorts or multicenter datasets.
Existing evidence suggests that insulin resistance (IR) and dysregulated glucose–lipid metabolism are associated with chronic low-grade inflammation and oxidative stress through metabolic stress, while also being linked to impaired skeletal muscle energy utilization and protein metabolic homeostasis, and potentially contributing to declines in muscle mass and functional reserve and increasing susceptibility to frailty.12,51–54 In this context, composite indices capturing both glycemic and lipid metabolic burden may represent a feasible approach for identifying prevalent frailty. Given that both TyG and CHG are constructed from glucose- and lipid-related parameters, their association with frailty may reflect glucose dysregulation, lipid metabolic abnormalities, and IR-related metabolic stress, which may be further amplified through coupled pathways such as inflammation and oxidative stress and be linked to functional decline at the tissue and organ level.3,51,55,56
From a pathophysiological perspective, frailty is a composite state defined by diminished multisystem physiological reserve and increased vulnerability to stressors. Its progression is intricately linked to chronic low-grade inflammation, oxidative stress, mitochondrial dysfunction, metabolic reprogramming, and reductions in skeletal muscle mass and function.1–3 The Frailty Index serves as a measure of the accumulation of deficits across various physiological systems, making it relevant to consider metabolic indices like TyG. Specifically, the glucose–lipid metabolic burden indicated by TyG could negatively impact skeletal muscle metabolism. This impairment may occur through pathways associated with inflammation and oxidative stress, ultimately leading to a decline in muscle function and physiological reserve.3,4 When central and visceral adiposity are present, factors such as adipose–skeletal muscle crosstalk, adipokine imbalance, local inflammation, ectopic fat deposition, and intramuscular fat infiltration can exacerbate insulin sensitivity and muscle quality. This interaction generates a vicious cycle where metabolic abnormalities and declines in muscle function mutually reinforce each other.42,57–59
In comparison to the TyG index, the CHG index integrates cholesterol and HDL-C into its framework, potentially providing a more comprehensive assessment of the coupled dysregulation of hyperglycemia and abnormal lipoprotein profiles. Furthermore, HDL dysfunction associated with metabolic syndrome or chronic inflammation—characterized by diminished anti-inflammatory, antioxidant, and endothelial-protective effects—closely correlates with the inflammation-oxidative stress environment implicated in frailty. 44 Therefore, the stable associations between CHG (and its derived composite indices) and frailty may indicate that when glucose abnormalities coexist with an abnormal lipoprotein profile, vulnerabilities in inflammation, vascular function, and muscle metabolism are more readily and persistently amplified.3,4,44 In our study, these associations indicate that the coexistence of glucose abnormalities and lipoprotein profile abnormalities leads to an enhanced and sustained vulnerability in inflammation, vascular function, and muscle metabolism, thereby being associated with higher prevalence of frailty.3,43,45,60 The superior performance of composite indices that incorporate fat distribution information (e.g., TyG-BRI and CHG-BRI) in ROC comparisons offers methodological support for the conclusion that combined information on metabolic abnormality × adiposity configuration is more valuable for frailty identification.
Against this backdrop of existing evidence, the incremental value of our study lies in three main aspects. Initially, we conducted a comprehensive evaluation of the associations between the TyG and several derived composite indices (TyG ABSI, TyG-BRI, TyG-CVAI, and TyG-WWI) within a unified analytical framework. Furthermore, we introduced the CHG index and its associated composite indices (CHG-ABSI, CHG-BRI, CHG-CVAI, CHG-WWI, CHG-BMI, CHG-WC, and CHG-WHtR) into frailty research for the first time, facilitating a parallel comparison with the TyG system. This design addresses the limitations of previous research, which frequently focused on a single metabolic or anthropometric measure. It offers the first systematic epidemiological evidence regarding the association and discriminative performance of CHG-derived indices with frailty. Second, by combining multivariable regression, RCS, and ROC analyses, we characterized these indices’ association strength, nonlinear patterns, and discriminative ability. This supported the added value of composite indices, which integrate body-fat distribution information, for identifying frailty. Third, our sensitivity analyses (both unweighted and weighted, without imputation) were consistent with the primary findings. This reduced the likelihood that results were influenced by sampling-weight handling or missing-data strategies, thereby enhancing the robustness of our conclusions.
This study has several limitations. First, as a cross-sectional analysis, it cannot establish temporal ordering or causality. Elevated metabolic indices may be associated with frailty; however, frailty may also inversely impact glucose and lipid metabolism due to decreased physical activity, dietary modifications, and changes in body composition, suggesting the potential for reverse causation. Prospective cohort studies are necessary to elucidate temporal relationships and evaluate the potential predictive utility of these indices for the onset of frailty. Second, while multiple covariates were incorporated, there remains a possibility of residual confounding due to factors such as inflammatory biomarkers, direct measures of sarcopenia, and medication adherence, which could skew effect-size estimates. Third, the majority of indices relied on single-time point measurements, potentially failing to capture long-term cumulative exposure; since frailty is a dynamic condition, future research employing trajectory models or repeated measurements may provide a more accurate depiction of the relationships between prolonged metabolic–body-shape burden and frailty outcomes. Fourth, race interactions suggest that calibration tailored to specific populations may be necessary; therefore, conducting external validation in diverse countries and ethnic groups is essential for improving generalizability. Furthermore, the study population’s relatively young mean age warrants caution when generalizing these findings to older or geriatric populations, whose frailty burden, body-composition characteristics, and metabolic profiles may differ.
Fifth, while several composite indices demonstrated superior performance compared to their respective single markers, the AUC values observed were approximately 0.7. This suggests that their discriminative ability is moderate at best. Consequently, these indices ought to be viewed as supplementary markers rather than as independent tools for screening frailty. Sixth, many composite indices were formulated using overlapping mathematical components, potentially resulting in residual structural collinearity even though all revised VIF values are below 5. Therefore, caution should be exercised when comparing effect estimates across different indices.
5. Conclusion
In conclusion, composite indices derived from TyG and CHG, especially those based on body roundness, such as TyG-BRI and CHG-BRI, demonstrated a positive association with frailty among U.S. adults. These findings indicate that indices that incorporate metabolic dysregulation and adverse fat distribution may serve as valuable adjuncts in identifying the prevalence of frailty. However, due to the cross-sectional nature of this study, causal inferences cannot be established. Future prospective studies are necessary to elucidate their temporal relationship with frailty and to assess their potential clinical utility.
Supplemental material
Supplemental material - Comparative discriminative performance of triglyceride–glucose derived composite indices and cholesterol–high-density lipoprotein cholesterol–glucose derived composite indices for identifying frailty: A cross-sectional study
Supplemental material for Comparative discriminative performance of triglyceride–glucose derived composite indices and cholesterol–high-density lipoprotein cholesterol–glucose derived composite indices for identifying frailty: A cross-sectional study by Zhe Zhang, Xiao Lei, Xuejuan Lin, Changchun Xie, Dong Cai, Shushen Weng, Lingling Zhao, Mengting Chen, Xiaofen Hou and Kejun Su in Science Progress.
Footnotes
Ethical considerations
Authors contributions
Conceptualization: Zhe Zhang; Methodology and Statistical analysis: Zhe Zhang, Changchun Xie, Dong Cai, Lingling Zhao, Shushen Weng; Data visualization: Zhe Zhang, Dong Cai, Lingling Zhao, Shushen Weng, Mengting Chen; Original draft preparation: Zhe Zhang, Mengting Chen; Draft review and editing: Zhe Zhang, Xiao Lei, Changchun Xie, Dong Cai, Shushen Weng, Lingling Zhao, Mengting Chen, Xiaofen Hou, Kejun Su, and Xuejuan Lin. All authors have reviewed and consented to the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
All authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.