
Abstract
Langerhans cell histiocytosis (LCH) is a rare neoplasm of immature dendritic cells, usually seen in children. Solitary gastric LCH in adults is uncommon, with only a limited number of reported cases. Optimal management remains unclear, although both endoscopic resection and conservative observation have been described in selected localized cases. We report the case of a man in his 50s who presented with several months of postprandial epigastric discomfort partially relieved by proton pump inhibitors. Endoscopy revealed a small, superficially elevated, discolored lesion in the gastric body resembling early gastric cancer. Histopathology and immunohistochemistry showing S-100, CD1a and langerin positivity confirmed LCH. BRAF V600E testing was positive. Systemic evaluation, including PET-CT, bone marrow biopsy, colonoscopy, and laboratory tests, showed no evidence of multisystem disease. After multidisciplinary review, ESD was performed to achieve complete histological assessment and local disease control. The patient remained asymptomatic, with no evidence of residual or recurrent disease during approximately 10 months of follow-up. This case highlights that solitary gastric LCH may closely resemble early gastric cancer on endoscopy, making targeted biopsy, immunohistochemistry, and systemic assessment essential for diagnosis. In selected localized lesions, ESD may serve as a minimally invasive diagnostic and therapeutic option, particularly when complete histological assessment is needed. Longer-term surveillance remains necessary.
Keywords
Introduction
Langerhans cell histiocytosis (LCH) is a rare clonal proliferative disorder of Langerhans-type dendritic cells that predominantly affects children, although adult cases are well recognized.1–3 Bone, skin, and lymph nodes are the most commonly affected sites, whereas gastrointestinal (GI) tract involvement is exceptionally rare, occurring in approximately 2–4% of cases, with symptomatic disease being uncommon.4,5 Solitary gastric involvement in adults is uncommon, with only a limited number of cases documented to date, including recent case series and small cohorts.6–22
Clinical manifestations are often asymptomatic or nonspecific, and many lesions are detected incidentally during endoscopic examinations. Endoscopically, these lesions may mimic early gastric cancer, polyps, or other submucosal tumors, which can complicate the diagnostic process. 5 Histopathological examination, combined with immunohistochemical staining for S-100, CD1a, and langerin (CD207), remains essential for definitive diagnosis. 2
There are no standardized management guidelines for solitary gastric LCH in adults. Nevertheless, limited evidence from recent case series and reviews suggests that both local resection, particularly by endoscopic methods, and conservative observation after biopsy have been associated with generally favorable short-term outcomes in selected patients with localized disease.5,22 Here, we report a case of solitary gastric LCH in an adult treated by ESD and provide an updated literature review summarizing its clinical and pathological features. This case highlights the diagnostic pitfall that solitary gastric LCH may resemble early gastric cancer on endoscopy and illustrates that ESD may be considered as a minimally invasive diagnostic and therapeutic option for selected localized gastric lesions.
Patient information
In July 2025, a man in his 50s was admitted to Affiliated Jinhua Hospital, Zhejiang University School of Medicine, because of several months of recurrent epigastric discomfort that worsened after meals and was partially relieved by proton pump inhibitors. He denied nausea, vomiting, gastrointestinal bleeding, diarrhea, or weight loss. There was no history of chronic disease or relevant family history. Physical examination was unremarkable.
Endoscopic findings
Upper gastrointestinal endoscopy revealed a well-circumscribed, superficially elevated lesion approximately 0.5 cm in diameter on the lesser curvature of the gastric body, with mild erythema and discoloration, mimicking early gastric neoplasia (Figure 1(a)). Under narrow-band imaging (NBI), the lesion showed a more clearly demarcated margin compared with white-light endoscopy, with subtle mucosal discoloration and surface irregularity. No definitive disease-specific NBI pattern was identified. Given its small size, superficial elevation, discoloration, and resemblance to early gastric neoplasia, targeted biopsies were taken for histopathological evaluation (Figure 1(b)). (a): Conventional endoscopy reveals a small, superficially elevated lesion in the gastric body, characterized by mild erythema and discoloration (arrow). (b): Narrow-band imaging (NBI) provides enhanced delineation of the lesion margin and highlights subtle mucosal discoloration and surface irregularity (arrow).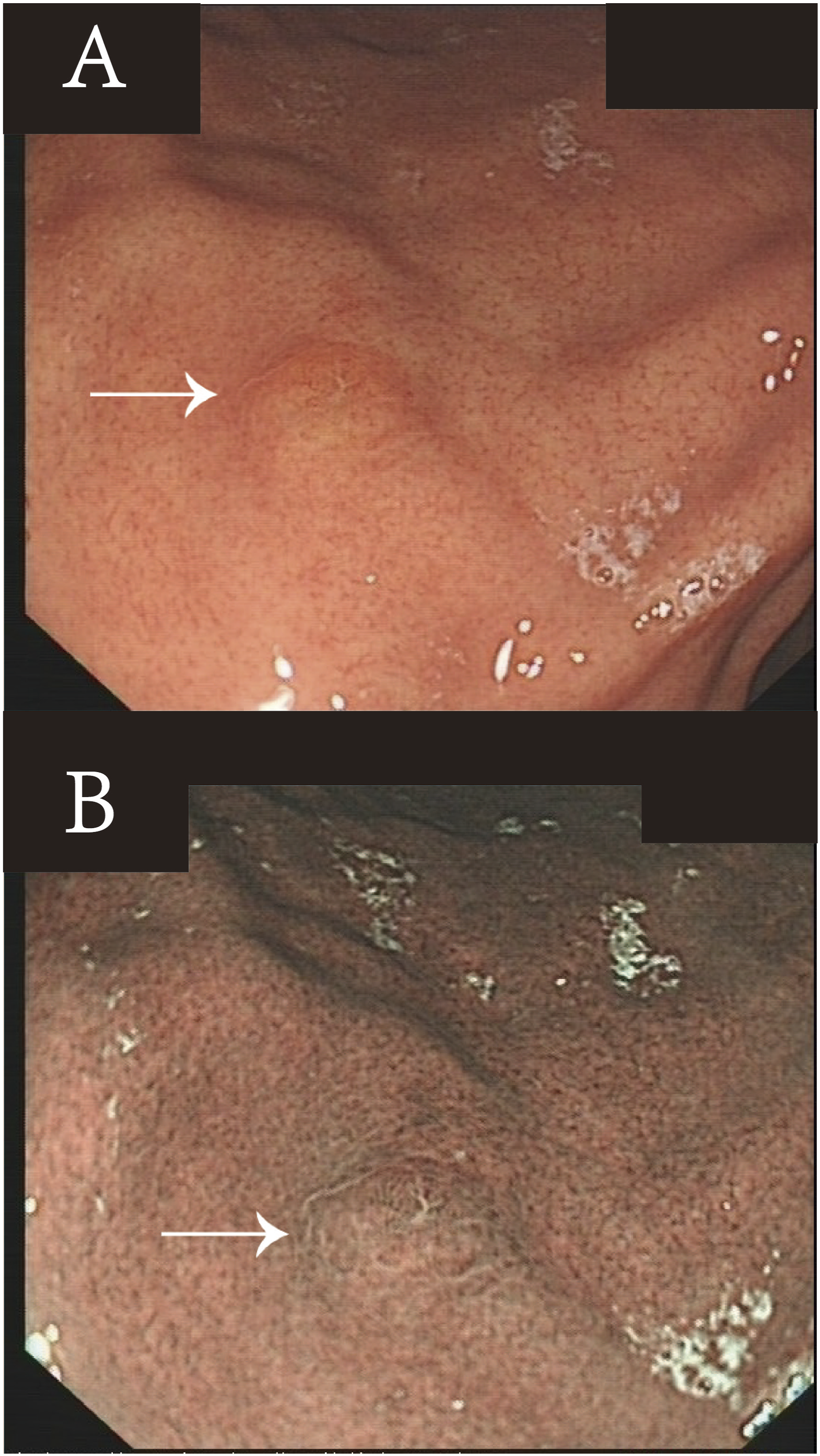
Histopathology and initial diagnosis
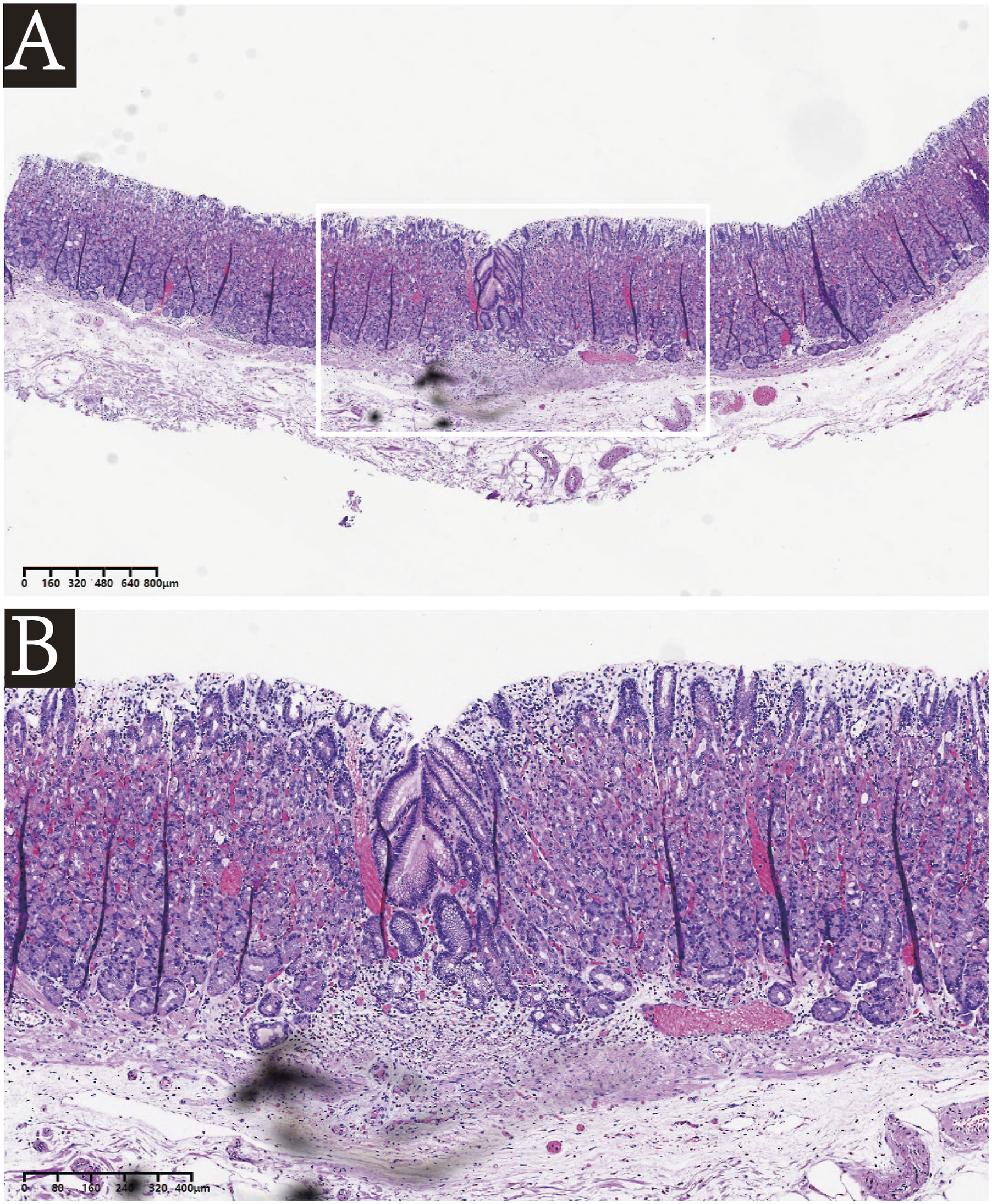
Histological examination of the gastric biopsy revealed diffuse infiltration of medium-sized histiocytic cells arranged in sheets within the lamina propria. The lesional cells exhibited abundant pale cytoplasm and irregularly folded or grooved (“coffee-bean–like”) nuclei, with occasional nuclear indentations. A prominent admixture of eosinophils and scattered lymphocytes was present in the background (Figure 2). Immunohistochemical staining confirmed the diagnosis, showing strong positivity for CD1a, langerin (CD207), and S-100, with a low proliferative index (Ki-67 ∼5%) (Figure 3). BRAF V600E testing was positive (Figure 4). Histopathological findings of gastric biopsy. Immunohistochemical staining of the gastric biopsy specimen. Detection of BRAF V600E mutation in the gastric LCH lesion.


Diagnostic assessment
Following the principles of adult LCH consensus recommendations, 3 a systematic assessment was performed to exclude multisystem involvement. Clinical history and physical examination specifically assessed for skin lesions, bone pain, respiratory symptoms, neurological or endocrine symptoms suggestive of pituitary involvement, and other systemic manifestations. Laboratory tests—including complete blood count, biochemistry, electrolytes, coagulation profile, CRP, ESR, LDH, and tumor markers—were all within normal limits. Contrast-enhanced computed tomography (CECT) of the abdomen and positron emission tomography-computed tomography (PET-CT) revealed no evidence of extra-gastric disease, lymphadenopathy, bone involvement, pulmonary lesions, or other metabolically active lesions. Bone marrow aspiration/biopsy and colonoscopy were negative for systemic involvement, supporting the diagnosis of solitary gastric LCH.
Therapeutic intervention
After confirming the solitary nature of the gastric lesion, the case was discussed by a multidisciplinary team (MDT) including gastroenterology, hematology, gastrointestinal surgery, and pathology. The MDT considered both conservative observation and endoscopic resection. Observation was considered given the small size of the lesion and the absence of systemic involvement. However, endoscopic resection was favored because the patient had persistent mild epigastric symptoms and the lesion closely resembled early gastric neoplasia on endoscopy. Although EMR could be considered for a small superficial lesion, ESD was selected to allow controlled en bloc resection, more accurate assessment of horizontal and vertical margins, and complete histological evaluation, given the concern for early gastric neoplasia. In this context, ESD was considered a minimally invasive diagnostic and therapeutic option that could provide complete histological assessment and local disease control. Systemic therapy was not considered necessary because PET-CT, bone marrow biopsy, colonoscopy, and laboratory evaluation showed no evidence of multisystem involvement. After discussion of the potential benefits and risks, and taking the patient’s preference into account, ESD was performed. The lesion was completely resected with negative margins, and the procedure was uneventful (Figures 5 and 6). Successful complete removal of the gastric lesion by endoscopic submucosal dissection (ESD). Histopathological examination after ESD shows complete removal of the lesion with negative horizontal and vertical margins, and no residual disease.
Follow-up and outcomes
The patient was discharged without complications. A subsequent follow-up extended the overall follow-up duration to approximately 10 months after ESD. The patient remained asymptomatic, with no evidence of residual or recurrent disease during follow-up (Figure 7). Given the lack of standardized surveillance guidelines for solitary gastric LCH, continued individualized follow-up was planned, including periodic clinical assessment, repeat endoscopy to assess the post-ESD scar and detect local recurrence, and routine laboratory tests. Additional CT or PET-CT would be considered if symptoms, abnormal laboratory findings, or endoscopic findings suggested recurrence or multisystem involvement. Surveillance endoscopy at 10-month follow-up showing only a scar at the resection site.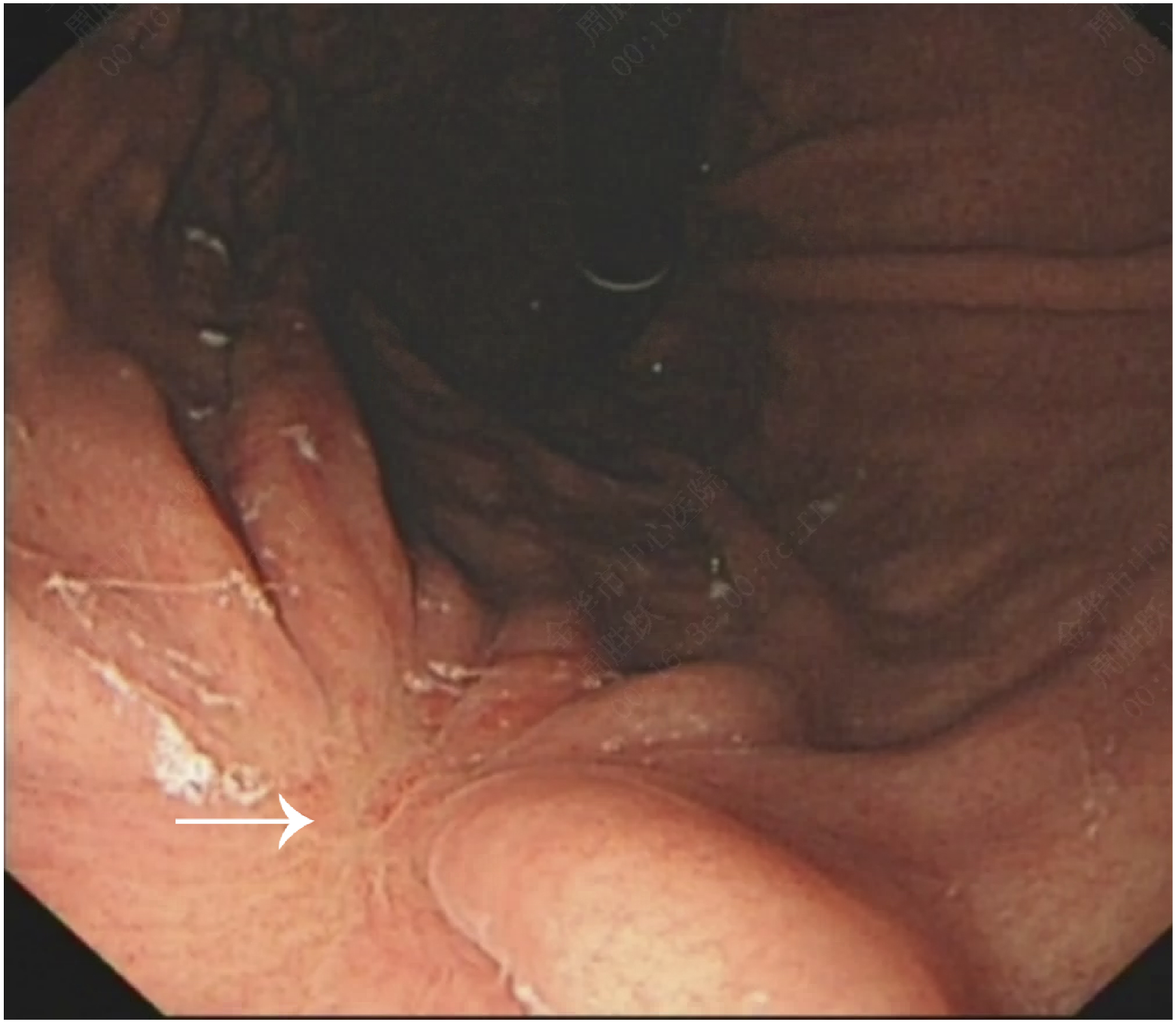
Literature search strategy and selection criteria
Clinicopathological features and outcomes of adult solitary gastric langerhans cell histiocytosis.
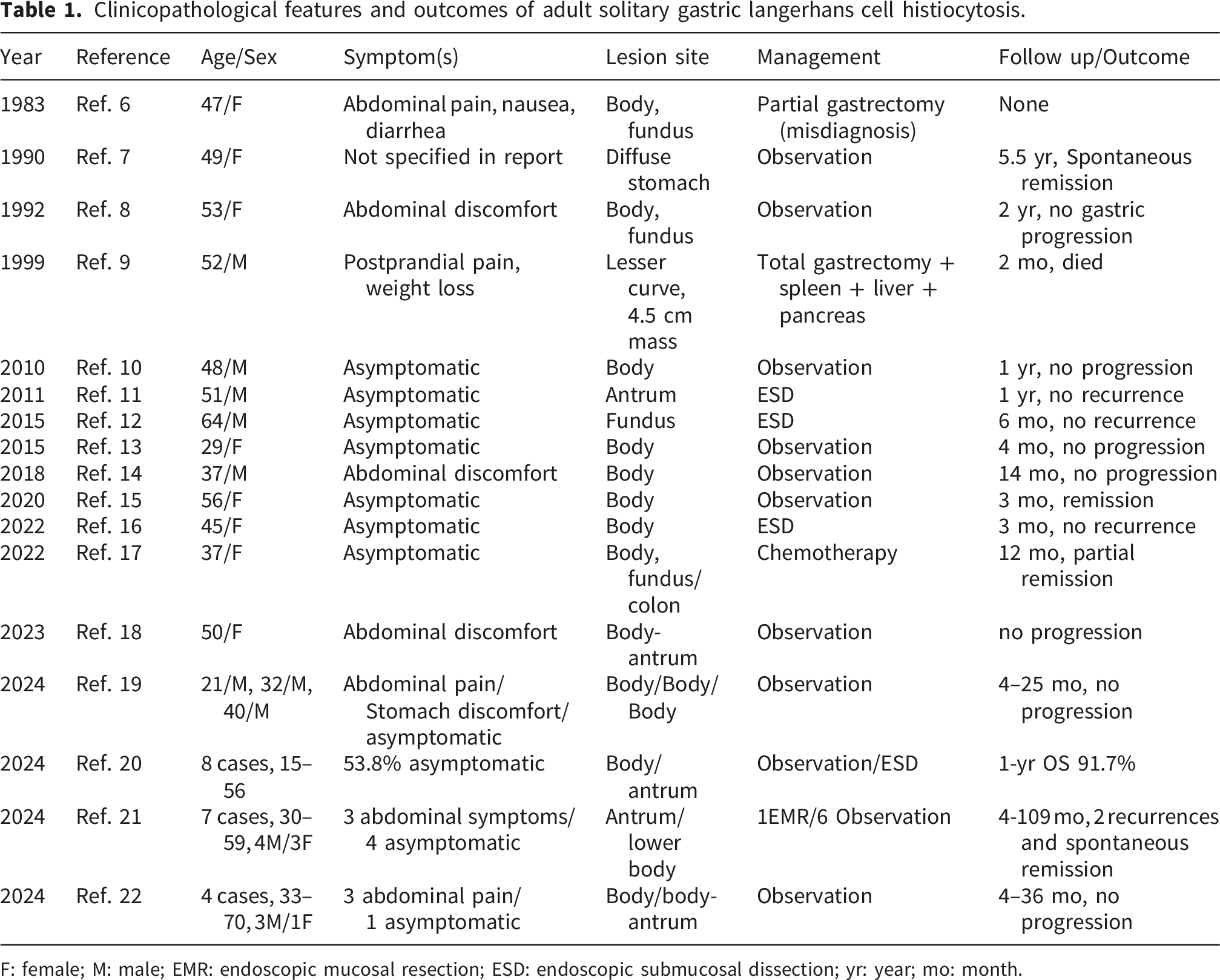
F: female; M: male; EMR: endoscopic mucosal resection; ESD: endoscopic submucosal dissection; yr: year; mo: month.
Discussion
LCH is now recognized as a clonal disorder of dendritic cell lineage with heterogeneous clinical behavior depending on age, organ involvement, and disease extent.1–3 Gastrointestinal (GI) involvement is uncommon, accounting for approximately 2–4% of LCH cases,4,5 and adult solitary gastric LCH has been described mainly in case reports and small case series. From a biological perspective, activating alterations in the mitogen-activated protein kinase (MAPK) pathway, most commonly BRAF V600E and less frequently MAP2K1 or other pathway alterations, play a central role in LCH pathogenesis. The clinical significance of these alterations in solitary gastric LCH, including their relationship with recurrence risk and management, remains insufficiently defined. Based on our literature search, the clinicopathological features, treatment strategies, and outcomes of eligible adult cases are summarized in Table 1.
Among the cases included in Table 1, the median age at diagnosis was approximately 47 years (range: 22–70), with a slight male predominance. The majority of patients are either asymptomatic or experience only mild, non-specific gastrointestinal symptoms such as epigastric discomfort or dyspepsia; in many cases, the lesion is discovered incidentally during routine endoscopic screening. Endoscopically, these lesions are typically small (<1 cm), superficially elevated or polypoid, sometimes displaying mucosal discoloration or erosion, and frequently mimic early gastric cancer, hyperplastic polyps, or submucosal tumors. The endoscopic differential diagnosis also includes gastric adenoma, inflammatory polyps, gastric xanthoma, neuroendocrine tumor, mucosa-associated lymphoid tissue lymphoma, and other small subepithelial lesions. Because these entities may share similar nonspecific features, such as slight elevation, discoloration, erosion, or surface irregularity, endoscopic appearance alone is insufficient for diagnosis. Image-enhanced endoscopy, including narrow-band imaging (NBI), may help delineate lesion margins and identify suspicious mucosal changes. In our case, NBI provided clearer visualization of the lesion margin and highlighted subtle mucosal discoloration and surface abnormality, which contributed to the initial impression of early gastric neoplasia. However, no disease-specific NBI pattern for gastric LCH has been established, and NBI findings alone cannot reliably distinguish LCH from early gastric cancer or other small gastric mucosal lesions. Therefore, targeted biopsy remains essential.
Histopathologically, LCH is characterized by sheets or nests of medium-sized histiocytic cells displaying irregular, grooved (‘coffee-bean’) nuclei, pale cytoplasm, and prominent eosinophilic infiltration. Immunohistochemistry plays a critical role in diagnosis, with tumor cells showing strong positivity for S-100, CD1a, and langerin (CD207), and negativity for cytokeratin 6. 23 The histopathological differential diagnosis includes poorly differentiated carcinoma, inflammatory fibroid polyp, granulomatous or xanthogranulomatous inflammation, reactive Langerhans cell proliferation, other histiocytic disorders, and Langerhans cell sarcoma. Epithelial malignancies are usually cytokeratin-positive and lack CD1a/langerin expression, whereas most non-Langerhans histiocytic or granulomatous lesions are negative for CD1a and langerin. Reactive Langerhans cell proliferation may show scattered Langerhans cells, but typically lacks a dense sheet-like infiltrate and mass-forming pattern. Langerhans cell sarcoma may share CD1a and langerin positivity but is distinguished by overt cytologic atypia, increased mitotic activity, necrosis, and a higher Ki-67 index. In our case, BRAF V600E testing was positive, supporting the clonal/neoplastic nature of the lesion; however, it did not alter management because systemic involvement had been excluded and complete local resection was achieved.
Recent literature, including the present summary (Table 1), indicates that treatment strategies for solitary gastric LCH in adults generally include endoscopic resection (EMR/ESD) and conservative observation after diagnostic biopsy. Some reported cases underwent endoscopic resection, typically for symptomatic, endoscopically suspicious, or technically accessible lesions.12,16,19 Another group of cases, mainly small, incidental, and asymptomatic lesions, were managed with biopsy followed by close endoscopic surveillance, with no progression or recurrence reported in the majority of published cases.13,15,21 Surgical intervention or systemic therapy has generally been reserved for rare patients with multifocal, bulky, or multisystem disease.9,17 A formal comparison between ESD and conservative management is difficult because the available evidence is limited to case reports and small case series with heterogeneous indications and follow-up durations. ESD/EMR may offer complete histological assessment and local disease control, whereas observation avoids procedural risks but requires close surveillance. Current evidence is insufficient to establish the superiority of either strategy. Therefore, the optimal management of adult solitary gastric LCH should be individualized, taking into account lesion characteristics, symptoms, endoscopic suspicion, technical feasibility, comorbidities, patient preference and the results of systemic evaluation. 3 An MDT discussion helped integrate endoscopic suspicion, pathological diagnosis, molecular findings, and staging results.
It is also noteworthy that a small subset of patients in the literature had synchronous gastrointestinal malignancies, including colorectal or gastric adenocarcinoma, at the time of LCH diagnosis.18,24 This highlights the need to exclude concomitant neoplasms, particularly when endoscopic findings are nonspecific. Because standardized surveillance protocols for solitary gastric LCH have not been established, follow-up should be individualized according to disease extent, treatment modality, molecular findings, and clinical course. For patients undergoing ESD, periodic clinical assessment and repeat endoscopy to evaluate the resection site may be reasonable, whereas additional imaging should be considered only when symptoms, abnormal laboratory findings, or endoscopic abnormalities suggest recurrence or multisystem involvement. Although BRAF V600E positivity does not by itself mandate systemic or targeted therapy in localized disease, it may provide useful molecular information if progression or recurrence occurs. 25
Our case illustrates localized gastric LCH presenting as a small, well-circumscribed lesion with classic histological, immunophenotypic, and BRAF V600E-positive findings, without evidence of systemic involvement. Complete ESD resection was followed by uneventful recovery and no evidence of recurrence during approximately 10 months of follow-up, although longer-term surveillance remains necessary.
This report has several limitations. First, it describes a single case, and therefore the findings cannot be generalized to all patients with solitary gastric LCH. Second, the follow-up duration has been extended to approximately 10 months, but it remains relatively short, and longer-term surveillance is required to assess sustained disease control. Third, our literature review was intended to provide an updated narrative summary rather than a formal systematic review or meta-analysis; therefore, selection bias and publication bias cannot be excluded. Future multicenter studies with longer-term follow-up are warranted to clarify the natural history, optimize surveillance strategies, and determine the clinical significance of molecular alterations such as BRAF mutations.
Conclusion
In summary, solitary gastric LCH in adults is uncommon and may mimic early gastric cancer on endoscopy. Accurate diagnosis requires integration of endoscopic, pathological, immunophenotypic, and, where available, molecular findings, with systematic exclusion of multisystem involvement. In this selected case, ESD provided complete histological assessment and local disease control; however, its role in solitary gastric LCH requires further validation through longer follow-up and additional cases. Our case, together with the current literature, highlights the importance of multidisciplinary evaluation, systematic assessment, individualized management, and continued follow-up.
Supplemental material
Supplemental material - Solitary gastric langerhans cell histiocytosis treated by endoscopic submucosal dissection: A case report and literature review
Supplemental material for Solitary gastric langerhans cell histiocytosis treated by endoscopic submucosal dissection: A case report and literature review by Shengyue Zhou, Chunxiao Hu, Xiaohua Ye, Jin Ding, Hongjun Hua, and Yilan Ma in Science Progress.
Footnotes
Acknowledgements
We thank the patient for his cooperation and consent to publish this report.
Ethical considerations
As a retrospective case report with anonymized patient data, this report is exempt from formal ethics review.
Consent to participate
Written informed consent was obtained from the patient for all procedures performed during the treatment course and publication of medical details and images.
Author contributions
Xiaohua Ye and Hongjun Hua performed the endoscopic procedure. Shengyue Zhou and Yilan Ma contributed to drafting and critical revision of the manuscript, and independently reviewed the final manuscript. Chunxiao Hu and Jin Ding contributed to the collection of the data and supervision of the manuscript. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are included in the manuscript. Additional anonymized data are available from the corresponding author upon reasonable request.
Patient perspective
The patient was informed about the diagnosis, treatment options, and follow-up plan. He agreed with the decision to undergo endoscopic treatment and continued surveillance.
CARE checklist statement
The reporting of this study conforms to CARE guidelines. 26
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.