
Abstract
Objective
Gout and hyperuricemia (HUA) are common metabolic disorders associated with increased all-cause and cardiovascular disease (CVD) mortality, and gut microbiota-modulating diets may influence prognosis. We aimed to evaluate whether the Dietary Index for Gut Microbiota (DI-GM) is associated with all-cause and CVD mortality among adults with gout or HUA.
Methods
In this prospective cohort study, we analyzed data from 5,325 adults with gout or hyperuricemia enrolled in the 2007–2018 National Health and Nutrition Examination Survey (NHANES). DI-GM scores were calculated using 24-hour dietary recall data, incorporating 14 predefined food components (10 beneficial and 4 harmful to gut microbiota). Mortality status was ascertained through linkage to the National Death Index up to December 31, 2019. Cox proportional hazards models were applied to estimate hazard ratios and 95% confidence intervals, adjusting for demographic, lifestyle, and clinical factors. Sensitivity analyses, interaction tests, and stratified analyses were conducted to assess robustness.
Results
During a median follow-up of 6.5 years (35,625 person-years), 603 deaths occurred, including 197 from CVD. Higher DI-GM scores were associated with significantly lower mortality risk. Participants with DI-GM scores ≥6 had a 33% reduced risk of all-cause mortality and a 45% reduced risk of CVD mortality compared to those with scores ≤ 4. Each one-point increase in DI-GM score was associated with an 8% decrease in all-cause mortality and a 13% decrease in CVD mortality. Results were consistent across all sensitivity analyses.
Conclusions
In individuals with gout or hyperuricemia, higher DI-GM scores were independently associated with reduced all-cause and CVD mortality. These findings suggest that gut microbiota-friendly dietary patterns may provide prognostic value and offer a potential target for dietary interventions in this high-risk population.
Keywords
Introduction
Gout and hyperuricemia (HUA) are common metabolic disorders with a steadily increasing global prevalence. 1 Gout has become a significant public health concern, affecting approximately 50 million individuals worldwide, 2 including nearly 12 million adults in the United States—around 5% of the adult population. 3 Persistent elevation of serum uric acid (SUA) can lead to the deposition of monosodium urate crystals in joints and soft tissues, triggering immune responses and resulting in gouty arthritis. 4
Among the various risk factors for HUA, dietary habits play a central role. Eating shellfish, alcohol, and drinks with sugar in them have all been linked to higher SUA levels and a higher risk of gout. 4 Furthermore, gout frequently coexists with a range of cardiometabolic conditions, including obesity, metabolic syndrome, type 2 diabetes, hypertension, chronic kidney disease, and atherosclerosis. 5 Accumulating evidence suggests that both gout and HUA are independently associated with increased risks of all-cause and cardiovascular disease (CVD) mortality.6,7 Elevated SUA levels have been linked to adverse CVD outcomes such as coronary artery disease, acute myocardial infarction (AMI), and chronic heart failure (CHF), indicating a potential pathophysiological role of uric acid in CVD progression. 8 In the Uric Acid Right for Heart Health (URRAH) study, Virdis et al. analyzed data from 22,714 Italian participants and found an independent association between SUA levels and both all-cause and CVD mortality. 9 Similarly, Kuo et al. reported higher mortality risks in patients with gout, even after adjusting for age, sex, metabolic syndrome, and proteinuria. 10 Other studies estimate that gout patients face an approximately 2.21-fold higher risk of all-cause mortality compared to the general population. 11
Recent research has highlighted gut microbiota as a key contributor to the development and progression of gout and HUA. The gut microbial community is actively involved in purine metabolism and uric acid homeostasis. Dysbiosis—an imbalance in microbial composition—can disrupt these processes by promoting urate overproduction or impairing its excretion, thereby increasing SUA levels and disease risk. 12 Studies have shown that gout patients exhibit significantly reduced microbial diversity and richness, along with distinct shifts in microbial gene functions.13,14 Furthermore, disruptions in amino acid, purine, and lipid metabolism—modulated by both host and microbial factors—may further exacerbate gut microbial imbalance. Factors such as alcohol consumption, gender, age, diet, and smoking can also affect the microbial composition.15–18
Among various environmental factors influencing gut microbiota, dietary intake stands out as a primary and modifiable determinant. To objectively evaluate the dietary impact on gut microbiota, the Dietary Index for Gut Microbiota (DI-GM) was established, integrating multiple dietary components known to modulate microbial ecology. 19
Recent findings have demonstrated a negative correlation between DI-GM scores and hyperuricemia, indicating that diets conducive to microbial health may be associated with reduced SUA levels. 20 Dysbiosis has also been implicated in broader metabolic dysfunctions; microbial imbalance can disrupt amino acid synthesis and lipid metabolism, promoting conditions such as obesity and insulin resistance. 21 Furthermore, DI-GM scores enhance CVD outcomes, with each 1-point rise reducing CVD risk by 4%. 22
Although the impact of DI-GM on metabolic health has garnered growing attention, its association with mortality—particularly among individuals with gout and HUA has not yet been systematically investigated. Therefore, to investigate this previously unexplored relationship, we utilized data from the National Health and Nutrition Examination Survey (NHANES), a large-scale database that provides detailed information on dietary intake, health status, and mortality outcomes. In the present study, DI-GM scores were calculated to quantify gut microbiota-related dietary patterns, and their associations with mortality risks specifically all-cause and cardiovascular mortality—were evaluated among adults diagnosed with gout or HUA. This research may offer new information on the predictive significance of dietary patterns linked to microbiota in people with HUA and gout.
Methods
Study participants
NHANES is a prospective survey program designed to capture detailed information on the nutritional status and overall health of the non-institutionalized U.S. civilian population, with approximately 5,000 participants evaluated annually. Center for Health Statistics (NCHS) and written informed consent was obtained from all participants prior to their enrollment.
For the present analysis, we drew data from six consecutive cycles of the NHANES, covering the years 2007 to 2018. From an initial pool of 32,016 participants between 20 and 79 years of age, with pregnant individuals excluded, several exclusion criteria were applied to ensure data completeness and analytical validity. Specifically, 113 individuals were excluded due to missing mortality linkage data, and an additional 3,427 participants were removed because their dietary recall information was insufficient for calculating DI-GM scores. The final analytic sample thus comprised participants with complete mortality follow-up and valid dietary data suitable for DI-GM assessment, yielding a pool of 28,476 individuals. Moreover, 22,355 participants were free of gout or HUA and the variables of 796 participants were not incorporated due to their absence.
Gout status was determined through self-reported medical history, specifically based on participants’ affirmative responses to the question: “Has a doctor or other health professional ever told you that you had gout?” HUA was defined according to established sex-specific thresholds for SUA concentrations, with cut-off values set at ≥7.0 mg/dL for men and ≥6.0 mg/dL for women. 23 These criteria allowed for consistent classification of participants into gout and hyperuricemia subgroups for subsequent analysis. Table S1 displayed the values and percentages of variables that were missing. Finally, the present study included 5,325 individuals with gout and HUA and was designed as a prospective cohort, and Figure S1 displayed the eligibility screening flow.
The present study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. The original NHANES protocol was reviewed and approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and all participants provided written informed consent at the time of enrollment. Because the present analysis used only de-identified, publicly available NHANES data, additional ethical review was waived by our institutional review board, and all patient information was de-identified prior to analysis. Participants were drawn from the NHANES multistage, stratified probability sample of the non-institutionalized U.S. civilian population; within each NHANES cycle, eligible adults with gout or hyperuricemia and complete dietary and mortality data were included consecutively, without further selection. The reporting of this observational study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, 24 and the completed STROBE checklist is provided as Supplementary Material.
Assessment of DI-GM
DI-GM was constructed to reflect the extent to which individual dietary patterns support gut microbiota health, based on intake levels of 14 predefined food components, following the methodology originally proposed by Kase et al. 19 and Supplementary Table S11 lists each component and its classification. Among these, 10 items were categorized as favorable for gut microbial diversity and function—specifically, fermented dairy products, chickpeas, soybeans, whole grains, dietary fiber, cranberries, avocados, broccoli, coffee, and green tea. The remaining 4 components—red meat, processed meat, refined grains, and a high-fat diet (defined as ≥40% of total caloric intake derived from fat)—were classified as unfavorable due to their potential to negatively affect gut microbial composition. 19
Scoring was performed in a binary manner based on sex-specific median intake values for each food group. For the favorable components, participants received a score of 1 if their intake exceeded the gender-specific median, and 0 otherwise. Conversely, for the unfavorable components, a score of 1 was assigned if intake fell below the median value, indicating limited consumption of potentially harmful items; a score of 0 was applied when intake met or exceeded the median threshold. The total DI-GM score, ranging from 0 to 14.
Outcome assessment
Mortality outcomes, including all-cause and CVD deaths, were identified through linkage with the National Death Index, 25 with follow-up with follow-up ending on December 31, 2019. With the use of the International Classification of Diseases, Tenth Revision (ICD-10), the NCHS was able to determine the causes of mortality. 26
In this prospective cohort research, mortality due to cardiac conditions or cerebrovascular events were classified as cardiovascular mortality, corresponding to ICD-10 codes I00–I09, I11, I13, I20–I51, and I60–I69. Follow-up time was calculated from the date of the mobile examination center (MEC) visit to either the date of death or the 31st of December 2019, whichever event happened first.
This allowed for precise estimation of person-time at risk and ensured consistent mortality tracking across the study population.
Covariates
Information about lifestyle, socioeconomic status, and demographics were gathered by skilled interviewers, conducting one-on-one interviews with the help of computers. There were other categories used to classify racial and ethnic groups, including white, non-Hispanic black, Mexican American, and others. Body mass index (BMI) was computed as the ratio of body weight in kilograms to the square of height in meters (kg/m2). This index is commonly employed in epidemiological studies as a standardized metric to assess general body fat distribution and categorize individuals’ adiposity levels. Obesity was defined as a body mass index (BMI) of 30 kg/m2 or higher. Marital status was characterized as married, single (widowed, divorced, separated, never married), and living with partner. Self-reported education was divided into under high school, high school, and above high school. Income level was evaluated based on the poverty-income ratio (PIR), defined as household (or personal) income divided by the poverty threshold specific to the survey year. When people were polled, “current smoking” meant smoking cigarettes. The term “current drinking” was used to describe people who had consumed any alcoholic beverage within the previous twelve months.
To quantify the amount of physical activity, metabolic equivalent (MET)-minutes, which represents the ratio between one’s metabolic rate while physically active and at rest, were calculated. Individual physical activity was categorized as insufficient (<600 MET-minute/week) and sufficient (≥600 MET-minute/week). Using mercury sphygmomanometers, examiners took blood pressure readings. The following conditions were considered hypertension: systolic blood pressure of 140 mm Hg or higher, diastolic blood pressure of 90 mm Hg or higher, hypertension diagnosed by a physician, or the use of hypertension medication as directed. Diabetes was defined based on multiple criteria, including a fasting plasma glucose (FPG) concentration of at least 126 mg/dL, a glycated hemoglobin A1c value equal to or exceeding 6.5%, a self-reported physician diagnosis of diabetes, or the use of insulin or oral hypoglycemic agents. Participants meeting any of these conditions were classified as having diabetes. Participants who fulfilled any of the aforementioned criteria were classified as having diabetes.
Statistical methods
Analyses were conducted using sampling weights and sample design factors, taking into consideration the intricate, several stages, and probability sampling used in the NHANES design. Categorical variables were summarized using unweighted frequencies along with weighted percentages to account for the complex sampling design of NHANES. Continuous variables were expressed as weighted means accompanied by their corresponding standard errors (SEs). We used logistic regression for categorical variables and linear regression for continuous ones to compare the demographic features of the DI-GM groups. We generated and compared weighted mean and 95% CIs of DI-GM based on demographic characteristics to linear regressions.
For the purpose of determining whether or not there were variations in survival probability across DI-GM groups, Kaplan–Meier (K-M) curves were generated and compared using the log-rank test. Subsequently, the relationship between DI-GM and mortality risk was explored using Cox proportional hazards regression models. Adjustments for relevant covariates were incorporated to control for confounding factors, thereby enhancing the robustness of the findings. The validity of the proportional hazards’ assumption was assessed using Schoenfeld residuals, which revealed no evidence of violation, thereby supporting the use of Cox regression models in the analysis. In the baseline adjustment model (Model 1), we controlled for essential demographic factors, including sex (male or female), age category (<50 or ≥50 years), and race/ethnicity (non-Hispanic White vs. all other racial/ethnic groups). To further account for potential confounding influences related to socioeconomic status, behavioral factors, and chronic conditions, a second multivariable model (Model 2) was constructed. This extended model included additional covariates such as obesity (classified as yes or no), marital status (married vs. others), and the family poverty-income ratio (PIR), dichotomized as <3.5 versus ≥3.5. Educational attainment was also considered, categorized as above high school versus high school and below. Furthermore, lifestyle variables, including current smoking and current alcohol consumption (each coded as yes or no), as well as physical activity level, defined using the threshold of 600 MET-minutes per week—were incorporated. Lastly, clinical diagnoses of hypertension and diabetes (both coded as yes or no) were adjusted to minimize residual confounding.
Linear trend was assessed by introducing medians of DI-GM groups as continuous variables into the model. Multivariable-adjusted hazard ratios (HRs) with 95% CIs for mortality associated with per score increment in DI-GM were additionally calculated. To explore potential heterogeneity in the association between DI-GM scores and mortality outcomes, a series of stratified analyses and interaction tests were conducted across multiple subgroups defined by demographic, socioeconomic, lifestyle, and clinical characteristics. These stratification variables included age sex, race/ethnic background, body weight status, marital status, educational attainment, and household economic status, as indicated by the PIR. Additional factors considered in the stratification included current smoking status, alcohol consumption, levels of physical activity, as well as whether participants had hypertension or diabetes. To formally assess effect modification, multiplicative interaction terms were introduced into the multivariable Cox proportional hazards models. These interaction terms were created by multiplying DI-GM (as a continuous variable) with each stratification variable, also treated continuously or dichotomously as appropriate. The statistical significance of these interactions was then evaluated to determine whether the association between DI-GM and mortality risk differed across strata. Given the number of subgroup comparisons, the false discovery rate (FDR) method was applied to control for potential type I errors. An FDR-adjusted p-value <0.05 was considered indicative of a statistically significant interaction.
To assess the robustness of our findings, we conducted five distinct sensitivity analyses. As a first step, participants with extreme DI-GM values—defined as those falling below the 1st percentile or above the 99th percentile—were excluded. This approach was used to determine whether the observed associations were disproportionately influenced by outliers or extreme dietary patterns. Second, we further adjusted for energy intake and dietary quality, which was evaluated with Healthy Eating Index (HEI)-2015 score, in multivariable models. Third, we disregarded the fatalities that occurred within the initial year of the follow-up period. Fourth, using the random forest technique and fully conditional specification (FCS) to multiple imputations (MI) to fill in missing covariates. Finally, based on the measured covariates, we determined the E-values to evaluate the possibility of residual confounding. An E-value is the lowest possible HR scale association between an unmeasured confounder and both the exposure and the outcome that would completely explain away the observed exposure-outcome association. All statistical analyses were conducted by R software (version 4.1.3; R Foundation for Statistical Computing, Vienna, Austria). A two-tailed P-value of less than 0.05 was considered indicative of statistical significance.
Results
Population characteristics
Baseline characteristics of the selected participants.
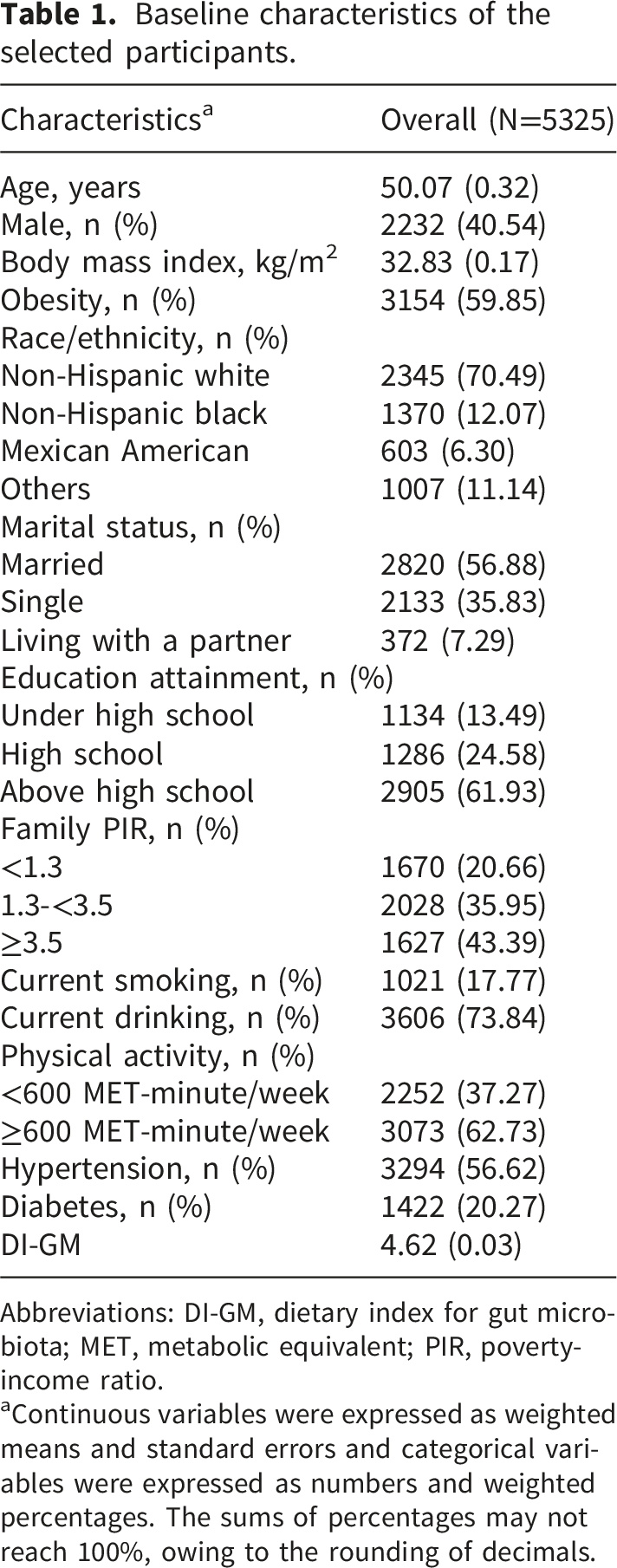
Abbreviations: DI-GM, dietary index for gut microbiota; MET, metabolic equivalent; PIR, poverty-income ratio.
aContinuous variables were expressed as weighted means and standard errors and categorical variables were expressed as numbers and weighted percentages. The sums of percentages may not reach 100%, owing to the rounding of decimals.
Connection within DI-GM and mortality risk in gout and HUA
Over a total follow-up duration of 35,625 person-years (median: 6.5 years), a total of 603 deaths were documented, of which 197 were attributable to CVD. K-M survival curves revealed significant disparities in both all-cause and CVD mortality across different DI-GM score categories, as evidenced by the log-rank test (P < 0.05) (Figure 1). As shown in Table 2, in the crude model, individuals in the extreme DI-GM category exhibited a lower risk of all-cause mortality (HR: 0.72, 95% confidence interval (CI): 0.59–0.88) and a lower risk of CVD mortality (HR: 0.59, 95% CI: 0.40–0.85) compared to those in the lowest DI-GM group. After adjustment for all potential covariates, a DI-GM score of ≥6 remained significantly related with reduced mortality risks. Specifically, these individuals experienced a 33% lower in all-cause mortality risk (HR: 0.67, 95% CI: 0.55–0.83) and a 45% lower in CVD mortality risk (HR: 0.55, 95% CI: 0.38–0.80), in comparison with those whose DI-GM score was ≤4 (Table 2). Moreover, when DI-GM score was analyzed as a continuous variable, each 1-point increment corresponded to an 8% decrease in the risk of all-cause death (HR: 0.92, 95% CI: 0.88–0.97) and a 13% decrease in CVD mortality (HR: 0.87, 95% CI: 0.80–0.95) (Table 2). To assess the robustness of the associations observed between DI-GM scores and mortality outcomes, additional subgroup analyses were conducted, including both stratified and interaction models. However, no statistically significant effect modification was detected, as all FDR exceeded the 0.05 threshold (Table S4–S5), suggesting the associations remained robust across strata. Kaplan-Meier survival curves for mortality, stratified by levels of DI-GM, in gout and hyperuricemia. (A) all-cause mortality; (B) CVD mortality. Abbreviations: CVD, cardiovascular disease; DI-GM, dietary index for gut microbiota. Multivariable Cox regression analysis of the associations between DI-GM and mortality in gout and hyperuricemia. Abbreviations: CVD, cardiovascular disease; DI-GM, dietary index for gut microbiota. aModel 1 was adjusted for age (<50, ≥50 years), sex (male, female), and race/ethnicity (non-Hispanic white, others). bModel 2 was further adjusted for obesity (yes, no), marital status (married, others), family poverty-income ratio (<3.5, ≥3.5), education attainment (above high school, high school and below), current smoking (yes, no), current drinking (yes, no), physical activity (<600 MET-minute/week, ≥600 MET-minute/week), hypertension (yes, no), and diabetes (yes, no).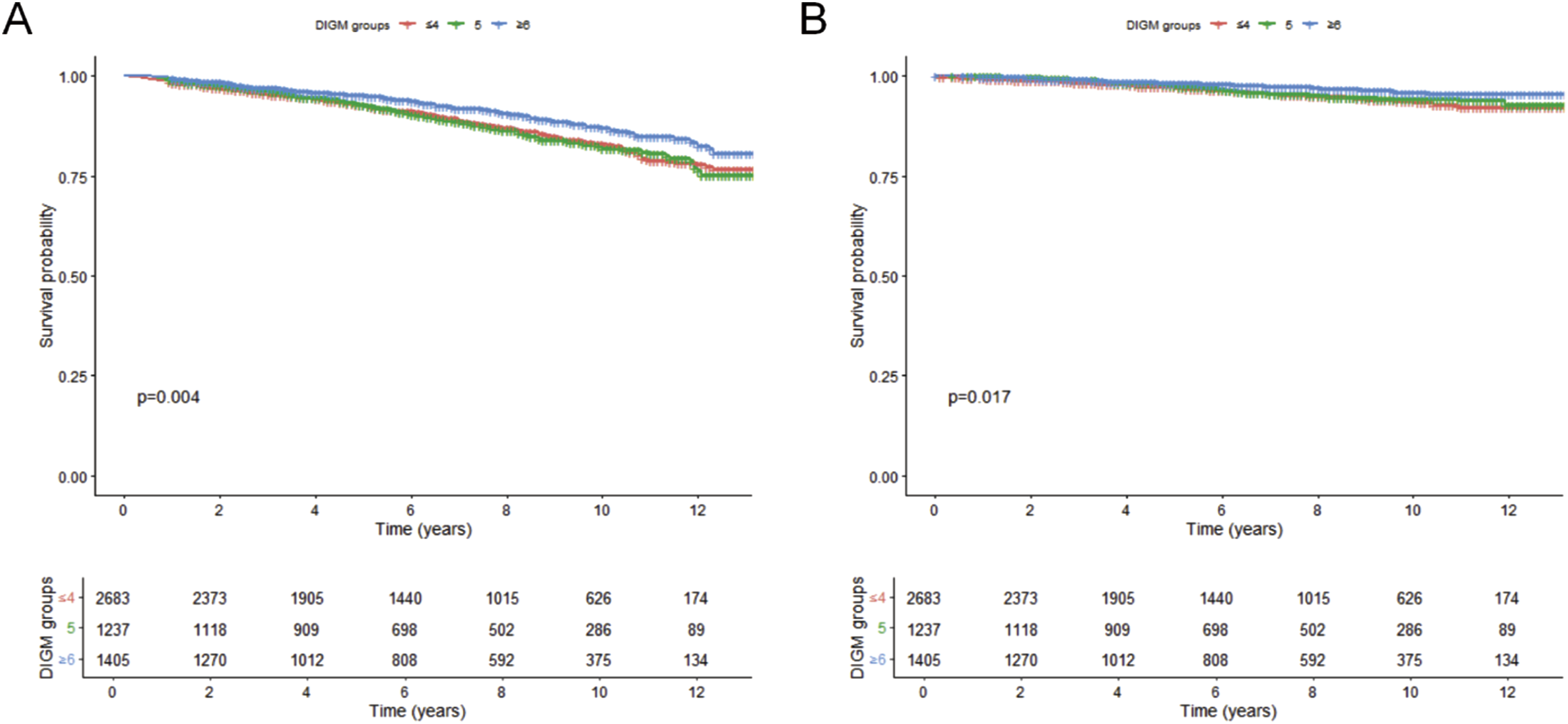

Sensitivity analyses
To further assess the stability and reliability of the main findings, a series of five sensitivity analyses were conducted, the results of which are summarized in Tables S6 to S10. The inverse connections remained consistent in sensitivity analyses that excluded outliers of DI-GM, with HRs (95% CIs) for all-cause and CVD mortality comparing extreme DI-GM groups reported as 0.67 (0.54-0.83) and 0.55 (0.38-0.80), respectively (Table S6). After further adjusting energy intake and dietary quality, inverse connections were perpetually observed, with HRs (95% CIs) for all-cause and CVD mortality associated with each score increase in DI-GM being 0.94 (0.89-0.99) and 0.89 (0.81-0.98), respectively (Table S7). Furthermore, as shown in Table S8, to minimize the potential impact of reverse causality, early deaths occurring within the first year of follow-up were excluded in a sensitivity analysis. Even after this exclusion, individuals with DI-GM scores ≥6 demonstrated a 28% lower risk of all-cause mortality (HR: 0.72, 95% CI: 0.58–0.90) and a 38% lower risk of CVD mortality (HR: 0.62, 95% CI: 0.42–0.92) compared with those scoring ≤4. In addition, the application of MI for handling missing covariates did not materially alter the observed associations, as shown in Table S9, further supporting the robustness of the findings (Table S9). The E-values for all-cause mortality was 2.35, while that for CVD mortality reached 3.04 (Table S10). These E-values suggest that to completely account for the observed inverse associations between DI-GM scores and mortality outcomes, an unmeasured confounder would need to be independently associated with both the exposure (i.e., DI-GM score) and the outcomes (all-cause and CVD mortality) by risk ratios of at least 2.35 and 3.04, respectively.
Discussion
This study examined the association between the DI-GM and both all-cause and CVD mortality among individuals diagnosed with gout and HUA. Higher DI-GM scores were found to be significantly and inversely associated with the risks of all-cause and CVD-related mortality. These associations persisted after multivariable adjustment for potential confounders.
In this cohort of 35,625 participants followed overtime, those with higher DI-GM scores were found to have a significantly lower risk of both all-cause and CVD mortality when compared to individuals with lower scores. After controlling for key covariates, including sex, age, race, obesity status, and smoking behavior, a one-point increment in DI-GM score was significantly associated with an 8% reduction in the risk of all-cause mortality and a 13% reduction in CVD mortality. These adjusted associations highlight the potential protective role of adherence to a DI-GM–aligned dietary pattern in improving both overall survival and cardiovascular health. Moreover, when comparing extreme DI-GM categories, individuals with scores of 6 or higher experienced a markedly lower risk of death: specifically, a 33% decrease in all-cause mortality and a 45% reduction in CVD mortality, relative to those with DI-GM scores of 4 or below. These findings align with previous studies confirm the association between dietary quality and risks of CVD and mortality.27,28 For instance, Micha et al. 27 demonstrated through multinational data analysis that high-quality dietary patterns significantly reduce all-cause and CVD mortality, consistent with our observations. Wang et al. 28 further emphasized the role of improved dietary patterns in modulating chronic disease outcomes, reporting that greater adherence to plant-based diets—particularly those emphasizing healthful plant foods—is associated with substantially lower risks of major chronic diseases including type 2 diabetes (T2D), CVD, malignancies, and premature mortality.
Beyond individual nutrient effects, our findings can be interpreted within a broader systems-level framework in which oxidative stress and chronic low-grade inflammation act as interconnected hubs driving cardiometabolic chronicity. 29 Within this framework, dietary patterns favorable to gut microbial diversity—as captured by the DI-GM—may attenuate systemic inflammation and oxidative burden through multiple convergent pathways, including enhanced short-chain fatty acid production, improved intestinal barrier integrity, and reduced circulating endotoxin and pro-inflammatory cytokine levels. Viewed in this light, the DI-GM may serve as a marker of long-term systemic resilience in patients with gout and HUA, in whom hyperuricemia itself amplifies oxidative and inflammatory signaling. This conceptual perspective is consistent with the observed graded inverse association between DI-GM and both all-cause and CVD mortality in our cohort.
Higher DI-GM scores indicate greater consumption of beneficial dietary components—such as whole grains, cranberries, green tea, and fermented dairy, among others—in patients with HUA and gout. These components may reduce risks of all-cause and CVD mortality through mechanisms including metabolic improvement, antioxidant effects, and anti-inflammatory actions.
Whole grains serve as a rich source of dietary fiber, essential vitamins, bioavailable minerals, and a wide array of phytochemicals, conferring benefits through improved insulin sensitivity, reduced blood lipid levels, and positive impacts on cardiovascular health. In patients with gout and HUA, dietary fiber mitigates metabolic disease risks by slowing intestinal absorption of glucose and fats, enhancing insulin sensitivity, and reducing glycemic fluctuations. Furthermore, Nirmala et al. reported that phytochemicals in whole grains—including phenolic acids and alkylresorcinols—enhance cellular antioxidant defense systems by suppressing NADPH oxidase activity and decreasing superoxide production. Animal studies confirm these compounds mitigate oxidative stress markers (e.g., MDA, 8-OHdG) through Nrf2 pathway activation, demonstrating particular efficacy in models of metabolic disorders. 30 Dietary fiber in whole grains (e.g., β-glucans) may indirectly mitigate uric acid-induced endothelial dysfunction through the modulation of gut microbiota and the reduction of systemic inflammation markers such as TNF-α and IL-6 (30). Simultaneously, the synergistic action of soluble and insoluble fibers delays purine absorption and decreases substrates for uric acid production. Their findings indicate that whole grain consumption is associated with a 23% lower HUA risk and an 18% reduction in CVD risk. 30 Consequently, patients with higher DI-GM scores—characterized by greater whole grain intake—may experience reduced mortality risks through improved metabolic profiles and enhanced antioxidant capacity.
Cranberries are rich in anthocyanins, flavonoids, and vitamin C, which exhibit potent antioxidant and anti-inflammatory properties. These bioactive compounds reduce oxidative stress, ameliorate vascular endothelial function, and attenuate inflammatory responses.31–33 During acute gout flares—characterized by severe joint inflammation—the natural anti-inflammatory constituents in cranberries may help mitigate these pathological inflammatory processes. 34 Furthermore, the flavonoids in cranberries exert noteworthy effects on uric acid metabolism. By inhibiting xanthine oxidase activity and thereby suppressing uric acid formation, these bioactive compounds contribute to the regulation of SUA concentrations and play a crucial role in reducing both the frequency and intensity of gout flare-ups. 34 In patients with higher DI-GM scores, cranberry consumption may constitute a significant contributor to improved CVD outcomes and reduced mortality.
Multiple studies have confirmed that green tea consumption reduces all-cause mortality and CVD risk in adults,35,36 aligning with our findings. Multiple biological pathways have been proposed to explain the inverse relationship between tea consumption and CVD risk. Among these, one prominent mechanism involves theaflavins found in green tea, which have been shown to lower both systolic and diastolic blood pressure. 37 These compounds enhance endothelial-dependent vasodilation (i.e., NO-dependent vasodilation) in healthy individuals and under various pathological conditions. Their capacity to activate endothelial nitric oxide synthase appears to mediate improved flow-mediated dilation and blood pressure reduction. Green tea is also rich in flavonoids. The polyphenolic flavonoids in tea possess antioxidant properties that inhibit low-density lipoprotein (LDL) oxidation both in vitro and in vivo. 38 Furthermore, increased tea consumption elevates concentrations of autoantibodies against oxidized LDL in atherosclerosis patients.39,40 Consequently, higher DI-GM scores—reflecting greater green tea intake—may represent one contributing factor to reduced mortality among patients with HUA and gout.
With respect to harmful dietary factors, the high intake of red and processed meats has been consistently linked to elevated risks of CVD and T2D.41,42 These protein sources contain high levels of saturated fats, which promote oxidative stress and inflammatory responses while elevating blood lipid levels—thereby exacerbating atherosclerosis and amplifying CVD risk. 42 Systematic reviews and meta-analyses of observational studies reveal that higher red meat intake correlates with elevated HUA and gout risks compared to lower consumption. Processed meat exhibits comparable positive associations with both conditions, supporting the pathogenic role of purine-rich animal proteins in uric acid elevation and gout development.43,44 High-fat diet, particularly those rich in trans fats and saturated fats, increase the metabolic burden in patients with gout and HUA. Research indicates that excessive saturated fat intake not only induces dyslipidemia but may also promote uric acid deposition, thereby exacerbating HUA and gout symptoms. Chronic consumption of high-fat diets, especially fried and grilled foods, stimulates production of proinflammatory cytokines and elevates systemic inflammation. Such an inflammatory environment facilitates uric acid crystallization, ultimately precipitating gout development and acute flares. The research presented here found that patients with lower DI-GM scores tended to have higher intakes of red meat, processed meat, and a high-fat diet, which was associated with elevated mortality risks. A higher intake of red meat, processed meats, and diets rich in high fat has been implicated as a potential driver of increased risks for both all-cause and CVD mortality.
Dietary diversity serves as a crucial metric for assessing dietary quality. Studies have established that individuals with higher dietary diversity typically exhibit reduced risks of chronic diseases and extended longevity. 45 For patients with HUA and gout, diets characterized by greater dietary diversity provide comprehensive nutritional support, improve uric acid metabolism, and reduce urate deposition—thereby lowering risks of all-cause mortality and CVD mortality. The Mediterranean diet pattern has been extensively validated for conferring significant cardiovascular protection. This dietary approach emphasizes abundant consumption of vegetables, fruits, whole grains, fish, and olive oil while restricting red meat, processed meat, and high-fat diets. 46 Research demonstrates its effectiveness in reducing chronic disease incidence, including CVD and diabetes and significantly lowering mortality. 46 Patients with higher DI-GM scores exhibit dietary structures closely aligned with the Mediterranean pattern, which likely constitutes a key determinant of their reduced mortality. Thus, optimizing dietary quality through increased intake of anti-inflammatory and antioxidant components effectively mitigates mortality risk among gout and HUA patients.
This research presents multiple limitations. First, the cohort comprised exclusively U.S. patients with HUA and gout derived from the NHANES database; thus, findings may not generalize to other racial/ethnic groups, age strata, or clinical populations. Second, gout diagnosis relied solely on a single self-reported question (“Has a doctor ever told you that you have gout?”), without verification through medical records or against ACR/EULAR classification criteria, potentially introducing self-report and misclassification bias; we have therefore consistently described the population as having self-reported physician-diagnosed gout rather than clinically confirmed gout. Third, dietary intake was assessed using two 24-hour recalls, which may not fully capture habitual long-term dietary patterns and is subject to recall bias. Fourth, as the primary endpoints were all-cause and CVD mortality, extrapolation to cause-specific mortality outcomes may be unreliable. Fifth, although we adjusted for most potential confounders, residual confounding from unmeasured factors such as medication use (e.g., urate-lowering therapy), disease duration, and detailed comorbidities may exist due to unmeasured latent variables. As an observational study, our findings can suggest associations but cannot establish causality.
Conclusions
In this nationally representative prospective cohort of U.S. adults with gout or hyperuricemia, higher DI-GM scores were associated with lower all-cause and cardiovascular mortality, with consistent inverse trends across multivariable, sensitivity, and stratified analyses. As an observational study, these results may suggest that dietary patterns favorable to gut microbial diversity could have prognostic value in this high-risk population, but they cannot establish causality. The findings may support the further investigation of gut microbiota-friendly dietary strategies as a complement to conventional management of gout and hyperuricemia. Future prospective and interventional studies are warranted to confirm these associations and to clarify the underlying mechanisms.
Supplemental material
Supplemental material - Association between dietary index for gut microbiota and all-cause and cardiovascular disease mortality in patients with gout and hyperuricemia: A prospective cohort study
Supplemental material for Association between dietary index for gut microbiota and all-cause and cardiovascular disease mortality in patients with gout and hyperuricemia: A prospective cohort study by Zhengtian li, Lin Wang, Jinmin Zhao in Science Progress
Footnotes
Acknowledgements
We appreciate the cooperative work of the NHANES study collaborators.
Ethical considerations
The NHANES is collaboratively administered by the Centers for Disease Control and Prevention (CDC) and the NCHS. Approval for the NHANES research protocol was granted by the NCHS Research Ethics Review Board after a review.
Consent to participate
All individuals taking part in the NHANES study have signed informed written consent forms.
Author contributions
Lin Wang and Zhengtian Li contributed equally to this work and share first authorship. Lin Wang contributed to the original study design, data acquisition, statistical analysis, and drafting of the initial manuscript. During the revision stage, Zhengtian Li made substantial additional contributions and took primary responsibility for the revised submission, including responding to the editor and reviewers’ comments, revising the Methods, Results, Discussion, Limitations, and Conclusions sections, integrating additional literature and methodological references, preparing the STROBE checklist and supplementary DI-GM component table, and drafting the response-to-reviewers letter. Jinmin Zhao, as the corresponding author, provided overall supervision and research guidance, secured funding, and critically revised the manuscript. All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Guangxi Science and Technology Base and Talent Special Project (Grant No. GuikeAD19254003) provided funding for this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to institutional policies, the dataset analyzed in this study is not publicly available; however, access may be granted by the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.