
Abstract
Objective
Smoking remains a significant risk factor for prostate, bladder, and kidney cancers. The disease burden and smoking-attributable carcinogenic effects are particularly concentrated in adults aged 40 years and older, making this age group critical for targeted prevention. We aimed to analyze the global, regional, and national disease burden of smoking-attributable prostate, bladder, and kidney cancers exclusively among adults aged 40 years and older from 1990 to 2021, and to provide long-term projections to 2045 for evidence-based tobacco control and cancer prevention strategies.
Methods
This retrospective observational study used data from the Global Burden of Disease Study 2021, we assessed age-standardized mortality rate (ASMR) and disability-adjusted life year rate (ASDR), along with absolute deaths and disability-adjusted life years (DALYs). Trends were evaluated using estimated annual percentage change (EAPC), and future burden was projected using the Nordpred model.
Results
From 1990 to 2021, absolute DALYs and deaths increased globally, while ASDR and ASMR declined. In 2021, DALYs for prostate and kidney cancers peaked at ages 65–69, and for bladder cancer at 70–74. High-SDI regions had the highest ASDR for prostate and kidney cancers, while middle-high-SDI regions led in bladder cancer. ASDR and ASMR decreased for prostate and bladder cancers across most SDI regions, but kidney cancer rates rose in Middle and Low-middle-SDI regions. By 2045, prostate cancer ASDR/ASMR are projected to increase after 2035, while bladder and kidney cancers will continue declining, though absolute burden will rise.
Conclusion
Smoking-attributable urological cancers remain a major public health challenge. Despite declining age-standardized rates, absolute burden is growing, particularly among older adults and in middle/low-SDI regions. Strengthened tobacco control, early screening, and optimized resource allocation are critical to reducing future burden.
Introduction
Tobacco use remains one of the leading global risk factors for disease and death, causing millions of fatalities annually. 1 Smoking is strongly associated with cardiovascular and respiratory diseases, various cancers, and is a significant contributor to many chronic conditions. 2 While the direct link between smoking and lung cancer is extensively studied and widely recognized by the public, the impact of smoking on other cancer types, particularly urological cancers, has not received sufficient attention or widespread dissemination.3,4 The urinary system includes vital organs such as the kidneys, bladder, prostate, and ureters, with prostate, bladder, and kidney cancers being the three most common malignancies in this system. 5 Research has unequivocally established smoking as a major shared risk factor for these three urological cancers, with its effect on bladder cancer risk being particularly prominent, making it one of the most significant preventable causes of the disease.6–8
For prostate cancer, smoking has been linked to higher Gleason scores, advanced tumor stages, and extraprostatic extension.9,10 Although a direct causal relationship is not fully established, evidence suggests smoking plays a role in biochemical recurrence and cancer-specific mortality. 11 Furthermore, smokers with prostate cancer have a higher risk of advanced disease, poorly differentiated cancer, and disease progression compared to non-smokers. 12 For bladder cancer, smoking is one of the most important known risk factors; approximately 50% of bladder cancer patients have a history of smoking, and smokers face a 2 to 3-fold increased risk, which correlates with smoking intensity and duration. 13 The causal relationship is well-defined, with tobacco-derived compounds like aromatic amines being potent carcinogens for the bladder. 14 Regarding kidney cancer, smoking is associated with tumor development, higher tumor grade and stage, and an increased risk of recurrence. 15 Smokers have an increased risk of developing kidney cancer, which increases with the duration and intensity of smoking. 16 Notably, smoking cessation appears to offer protective benefits for patients with prostate and bladder cancer, reducing risks of recurrence and progression.17,18 Additionally, studies indicate that smoking cessation after a kidney cancer diagnosis can significantly improve survival rates and reduce the risk of further deterioration. 19
Given the dynamic changes in global smoking prevalence and cancer burden, analyzing the long-term impact of smoking on prostate, bladder, and kidney cancers among adults aged 40 years and older holds major public health importance. This high-risk group carries the overwhelming majority of smoking-attributable urological cancer risk, making it highly relevant for targeted prevention. Utilizing data from the Global Burden of Disease (GBD) 2021, this study systematically analyzes the global, regional, and national burden of smoking-attributable prostate, bladder, and kidney cancers from 1990 to 2021 among adults aged 40 years and above. We further provide novel long-term projections to 2045, offering forward-looking evidence for tobacco control and cancer prevention planning. We assess temporal trends in disability-adjusted life years (DALYs), deaths, age-standardized mortality rate (ASMR) and age-standardized disability-adjusted life year rate (ASDR), and disparities across regions with different Sociodemographic Index (SDI) levels. The findings aim to support policymakers and clinicians in implementing tailored strategies for adults aged 40 years and older, ultimately reducing the global burden of smoking-attributable urological cancers.
Materials and methods
Data source and data collection
The GBD 2021, led by the Institute for Health Metrics and Evaluation (IHME), is a collaborative international research program designed to systematically quantify, compile, and compare the health impact of diseases, injuries, and risk factors across age groups, sexes, and geographical locations. 20 Since 1990, the GBD study has provided periodic assessments of global disease burden using consistent methodologies. GBD 2021 covers 204 countries and territories, grouped into 21 GBD regions and five SDI regions. The study provides detailed estimates for 371 diseases and injuries and 88 risk factors, including data on incidence, prevalence, mortality, years of life lost (YLL), years lived with disability (YLD), and DALYs. 21
Data for this analysis were obtained from the GBD 2021 database. We extracted the number of deaths, DALYs, mortality rates, and DALY rates attributable to smoking for prostate cancer (ICD-10: C61-C61.9, D07.5, D29.1, D40.0; ICD-9: 185-185.9, 222.2, 236.5), bladder cancer (ICD-10: C67-C67.9, D09.0, D30.3, D41.4-D41.8, D49.4; ICD-9: 188-188.9, 223.3, 233.7, 236.7, 239.4), and kidney cancer (ICD-10: C64-C65.9, D30.0-D30.1, D41.0-D41.1; ICD-9: 189.0-189.1, 189.5-189.6, 223.0-223.1). 22 The study population was restricted to individuals aged 40 years and above, because prostate, bladder, and kidney cancers increase sharply after 40 years of age, with minimal disease burden in those younger than 40 years.23,24 The cumulative carcinogenic effect of smoking also becomes prominent in this age group, supporting 40 years as a rational cutoff that improves the stability of trend analysis and relevance to public health policy. 24 The included population was divided into twelve 5-year age groups (from 40–44 to 95 years and above). ASMR and ASDR were calculated using the GBD standard population age structure to facilitate comparisons unaffected by differences in population age distribution.
This retrospective observational study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 25 All procedures performed in this study were in accordance with the 1975 Helsinki Declaration and its 2024 revision.
Statistical analysis
EAPC analysis
To analyze trends in the ASMR and ASDR, we used the EAPC method. The specific formula was: ln(ASR) = α + βX + e, where the natural logarithm of the ASR is denoted by ln(ASR), X represents the calendar year under study, α is the intercept, β is the slope reflecting the temporal trend, and e is the random error in the model. 26 The EAPC was calculated as 100 × [exp(β) - 1], representing the annual percentage change. Trends were analyzed based on the EAPC and its 95% confidence interval (CI). A trend was considered increasing if both the EAPC and the lower limit of its 95% CI were positive, and decreasing if both the EAPC and the upper limit of its 95% CI were negative. If neither condition was met, the trend was considered stable. 27
For EAPC estimates, 95% CIs were derived from linear regression residuals. These CIs were incorporated into trend classification, where the statistical significance of temporal trends was judged according to the overlap between EAPC values and their corresponding 95% CIs.
Nordpred age-period-cohort prediction model
We applied the Nordpred Age-Period-Cohort (APC) model to predict the disease burden trends of three urological cancers from 2022 to 2045. 28 The population was stratified into 12 five-year age groups (40–44 to ≥95 years), and annual data from 1990–2021 were aggregated into 5-year periods for modeling. The model was fitted under the Poisson distribution with a power-5 link function (linkfunc= “power5″). Both startestage and startuseage were set as the youngest age group in this study. The parameter cuttrend= c(0, 0.25, 0.5, 0.75, 0.75) was used to constrain period-cohort drift and stabilize long-term prediction results. Model uncertainty was quantified by calculating 95% CIs via maximum likelihood estimation of APC model parameters. The cuttrend smoothing further reduced extrapolation uncertainty, and all uncertainty intervals were fully reported in the results to ensure analytical reproducibility.
We validated model performance using 1992–2014 data for training and 2015–2021 observed data for verification. Three error metrics (MAE, RMSE, MAPE) were calculated, and all MAPE values were less than 5%, verifying good predictive reliability of the model (Table S1).
Study population and analytical software
Bladder and kidney cancer analyses covered the full population of males and females, while prostate cancer analysis was limited to males based on anatomical characteristics. All statistical analyses were conducted using R software (v 4.3.3), relying on tidyverse (2.0.0), dplyr (1.1.4), reshape (0.8.1) for data processing, and patchwork (1.3.2), nordpred package (1.3), ggsci (4.0.0), maps (3.4.3) for data visualization and geospatial analysis.
Results
Global trends in smoking-attributable prostate, bladder, and kidney cancers among adults aged 40 and older
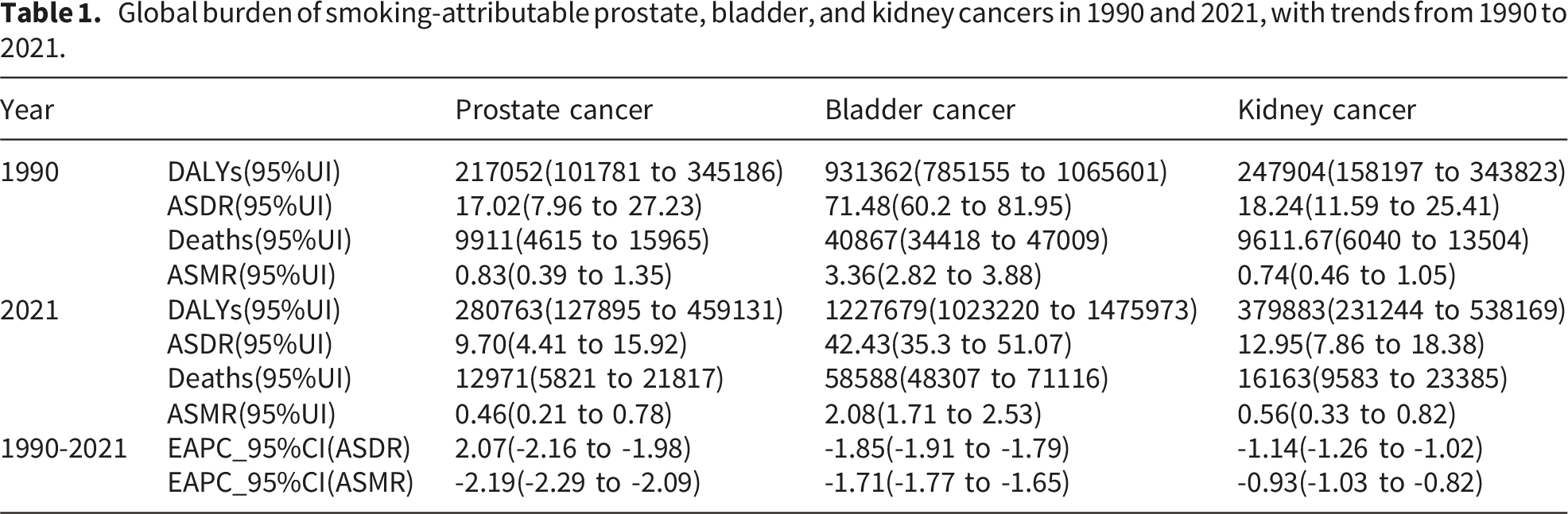
Global burden of smoking-attributable prostate, bladder, and kidney cancers in 1990 and 2021, with trends from 1990 to 2021.
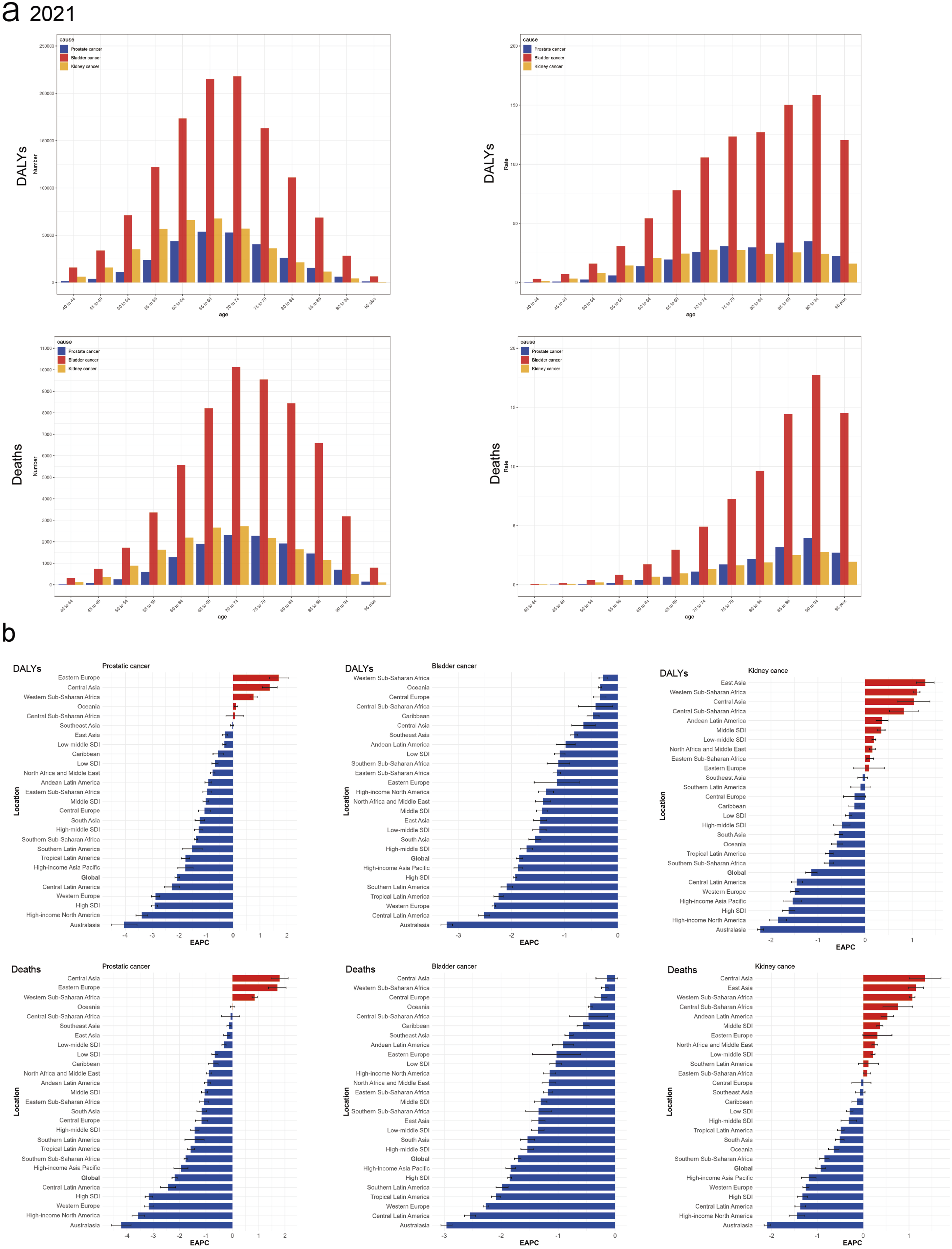
Age distribution and EAPC in the global burden of smoking-attributable prostate, bladder, and kidney cancers (1990-2021). (a) Age distribution of DALYs (upper row) and Deaths (lower row) attributable to smoking-attributable prostate cancer (blue), bladder cancer (red), and kidney cancer (orange) in 2021. (b) EAPC in DALYs (upper row) and Deaths (lower row) attributable to smoking-attributable prostate cancer, bladder cancer, and kidney cancer, from 1990 to 2021, across globe, five SDI regions, and 21 GBD regions. Blue indicates an EAPC < 0 (representing a decreasing trend), and red indicates an EAPC > 0 (representing an increasing trend).
Mortality trends were consistent with ASDR trends: bladder cancer maintained the highest burden in 2021, with the greatest number of deaths and highest ASMR, followed by kidney and prostate cancers (Table 1). From 1990 to 2021, ASMR declined significantly for all three cancers, again with prostate cancer showing the most substantial decrease (Table 1). In terms of age distribution, the 70-74 year age group had the highest number of deaths for all three cancers in 2021, whereas the highest mortality rates were observed in the 90-94 year age group (Figure 1(a)).
Trends in smoking-attributable urological cancers by SDI among adults aged 40 and older
In 2021, the smoking-attributable burden varied considerably across SDI regions: the High SDI region had the highest ASDR for prostate and kidney cancers, while the High-middle SDI region had the highest ASDR for bladder cancer (Table S2, Figure 1(b)). prostate and bladder cancer ASDR declined across all five SDI regions, with the most significant decrease in the High SDI region and the smallest decline in the Low-middle SDI region (Table S2, Figure 1(b)). A key difference emerged for kidney cancer:ASDR increased in the Middle and Low-middle SDI regions (most notably in the Middle SDI region) but declined in the High SDI region (with the most pronounced decrease) (Table S2, Figure 1(b)).
Mortality distribution across SDI regions mirrored ASDR patterns: the High SDI region had the highest number of deaths and ASMR for prostate and kidney cancers, while the High-middle SDI region had the highest for bladder cancer (Table S3). ASMR trends from 1990 to 2021 were consistent with ASDR trends: prostate and bladder cancer ASMR declined across all SDI regions (most notably in the High SDI region), while kidney cancer ASMR increased in the Middle and Low-middle SDI regions (most significantly in the Middle SDI region) (Table S3, Figure 1(b)).
Changes in the burden of smoking-attributable urological cancers across 21 GBD regions among adults aged 40 and older
Substantial shifts occurred in the geographic distribution of the burden of smoking-attributable urological cancers across the 21 GBD regions between 1990 and 2021. In 1990, Western Europe reported the highest number of DALYs for all three cancers: prostate cancer, bladder cancer, and kidney cancer (Table S4). By 2021, Western Europe remained the region with the highest number of DALYs for prostate cancer, whereas East Asia emerged as the region with the highest number of DALYs for both bladder cancer and kidney cancer (Table S5). The regions with the highest ASDR also changed over this period. In 1990, the highest ASDR for prostate and kidney cancers was in High-income North America, while Western Europe had the highest ASDR for bladder cancer (Table S6). By 2021, the Caribbean, Eastern Europe, and Central Europe had the highest ASDRs for prostate cancer, kidney cancer, and bladder cancer, respectively (Table S7, Figure 2(a)). Analysis of trends from 1990 to 2021 across the 21 GBD regions revealed heterogeneous patterns in ASDR. The ASDR for prostate cancer increased in 5 regions, with the most significant increase in Eastern Europe, but decreased in others, most notably in Australasia. The ASDR for bladder cancer decreased across all 21 regions, with the most substantial decline in Australasia. For kidney cancer, ASDR increased in 8 regions, led by East Asia, while decreasing in others, with the sharpest decline in Australasia (Table S2, Figure 1(b)). Global distribution of and socio-demographic associations with smoking-attributable urological cancer burden (1990-2021). (a) ASDR (upper row) and ASMR(lower row) for smoking-attributable prostate cancer, bladder cancer, and kidney cancer across globe, five SDI regions, and 21 GBD regions in 1990 (blue) and 2021 (red), with rates presented per 100,000 population. (b) Association between SDI and ASDR (upper row) and ASMR (lower row) for smoking-attributable prostate cancer, bladder cancer, and kidney cancer across 204 countries and territories in 2021. Colors represent the magnitude of ASDR or ASMR (per 100,000 population), and the size of dots indicates the population size of each country or territory. The blue curves denote the fitted trends. Colors represent the magnitude of ASDR or ASMR (per 100,000 population), and the size of dots indicates the population size of each country or territory. The blue curves denote loess-fitted nonlinear trends, with shaded areas indicating 95% confidence intervals. Pseudo-coefficients of determination (pseudo-R2) were as follows: Prostate cancer (ASDR=0.18, ASMR=0.17), bladder cancer (ASDR=0.28, ASMR=0.26), kidney cancer (ASDR=0.46, ASMR=0.48), quantifying the explanatory power of SDI for cross-national variations in cancer burden.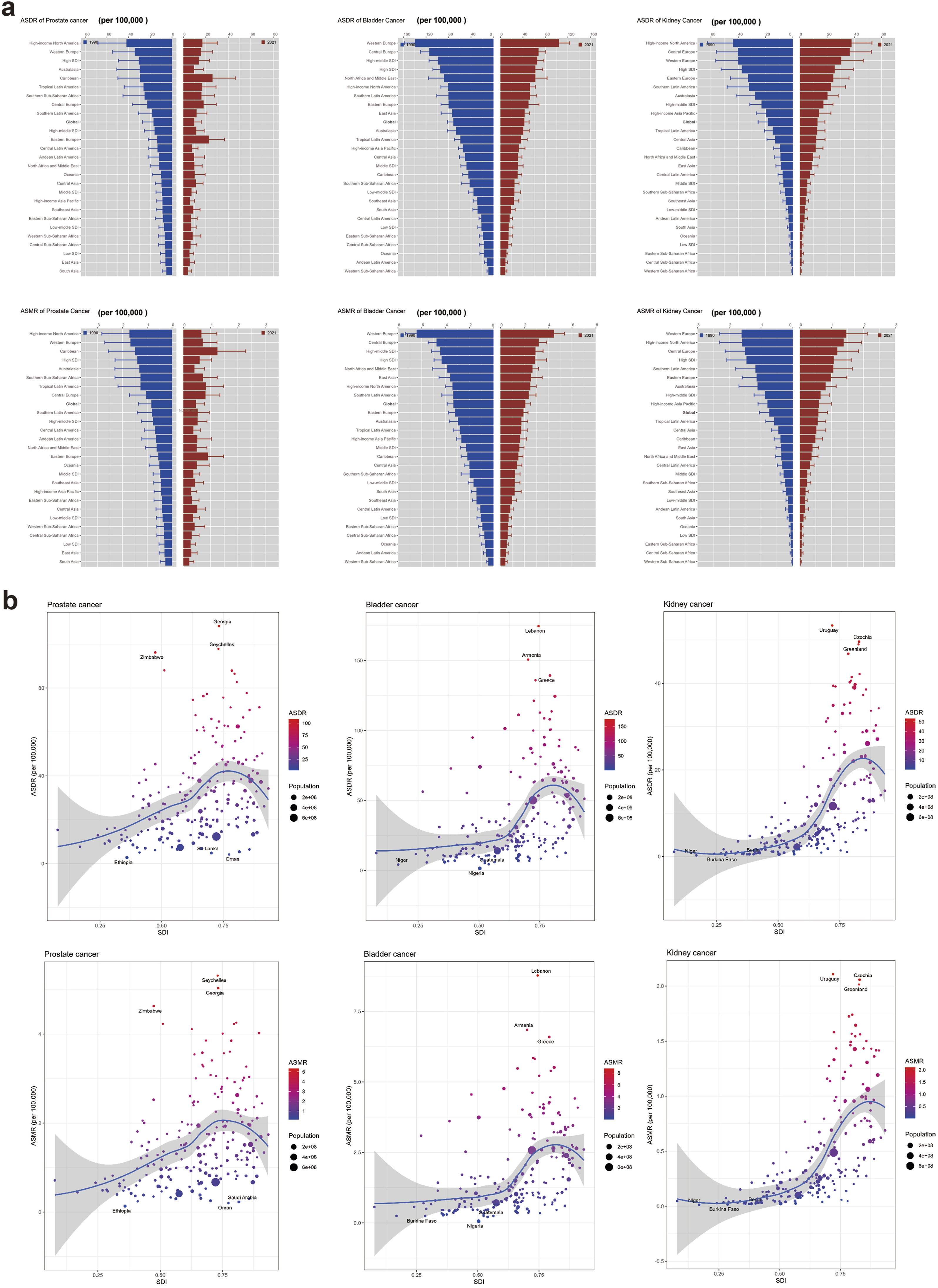
A similar geographic transition was observed for mortality. In 1990, Western Europe had the highest number of deaths from prostate, bladder, and kidney cancers (Table S8). By 2021, Western Europe still had the highest number of deaths from prostate cancer, but East Asia reported the highest number of deaths from bladder and kidney cancers (Table S9). The patterns for ASMR also shifted. In 1990, Western Europe recorded the highest ASMR for both bladder and kidney cancers, and high-income North America for prostate cancer (Table S10). By 2021, the Caribbean region had the highest ASMR for prostate cancer, while Central Europe had the highest ASMR for both bladder and kidney cancers (Table S11). Trends in ASMR from 1990 to 2021 varied by cancer and region. Prostate cancer ASMR increased in 4 regions, most significantly in Central Asia, but decreased in others, with the sharpest decline in Australasia. Bladder cancer ASMR decreased across all regions, most markedly in Australasia. Kidney cancer ASMR increased in 9 regions, led by Central Asia, while decreasing in others, most substantially in Australasia (Table S3, Figure 1(b)).
Patterns of smoking-attributable urological cancers among adults aged 40 and older across 204 countries and territories
Across the 204 countries and territories in 2021, the relationship between SDI and the ASDR/ASMR of smoking-attributable prostate, bladder, and kidney cancers was non-linear. As SDI increased, the ASDR and ASMR showed an initial rise followed by a decline, forming an inverted U-shaped curve (Figure 2(b)). Additionally, there were significant disparities in the ASDR and ASMR of the three cancers among different countries (Figure 3), as well as in the absolute numbers of deaths and DALYs (Figure S1). In 2021, the country with the highest ASDR for prostate cancer was Seychelles and the lowest was Ethiopia, while the highest ASMR was in Seychelles and the lowest was in Ethiopia; for bladder cancer, the highest ASDR was in Lebanon and the lowest was in Nigeria, while the highest ASMR was in Lebanon and the lowest was in Nigeria; for kidney cancer, the highest ASDR was in Uruguay and the lowest was in Niger, while the highest ASMR was in Uruguay and the lowest was in Niger (Table S12, Figure 2(b)). Global geographic distribution of smoking-attributable urological cancer burden, 2021. Global distribution of the ASDR (a) and ASMR (b) for smoking-attributable prostate, bladder, and kidney cancers in 2021 (per 100,000 population). Color gradients indicate rate intervals, highlighting global geographical variations in disease burden.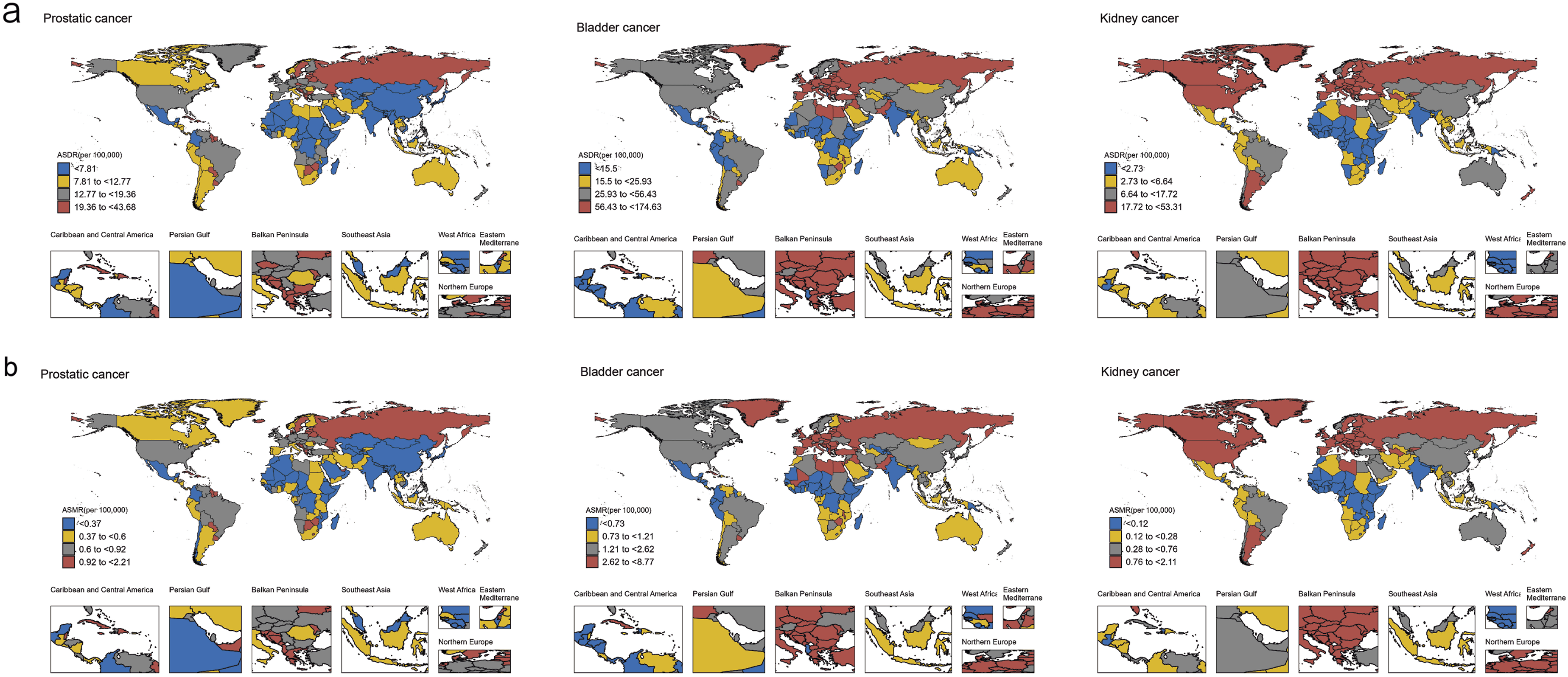
The EAPC in ASDR and ASMR from 1990 to 2021 also varied markedly across nations. For prostate cancer, Georgia recorded the most significant increase in ASDR, whereas Canada experienced the steepest decline; the corresponding most extreme increases and decreases in ASMR were observed in Georgia and Australia, respectively. For bladder cancer, the most notable increase in ASDR was in Cabo Verde and the most substantial decrease was in Norway; similarly, for ASMR, the largest increase was in Cabo Verde and the largest decrease was in Norway. For kidney cancer, Mongolia saw the most dramatic rise in ASDR, in contrast to the sharpest decline observed in Sri Lanka; the pattern for ASMR was consistent, with Mongolia and Sri Lanka showing the greatest increase and decrease, respectively (Table S13, Figure S2).
Projections of smoking-attributable urological cancer burden through 2045 based on the nordpred model
To better understand the future global trends of smoking-attributable prostate, bladder, and kidney cancers, we projected the ASDR, ASMR, DALYs, and deaths from 2022 to 2045 using the Nordpred model (Figure 4). Projections indicated that the absolute DALYs and death numbers for prostate cancer will continue to rise throughout the projection period, while its ASDR and ASMR present a trend of initial decline followed by a rebound with an inflection point around 2035, and the standardized rates in 2045 are still projected to be lower than the 2021 baseline. For both bladder and kidney cancers, DALYs and death counts are expected to drop slightly in 2022 relative to 2021 and then increase continuously up to 2045; conversely, the ASDR and ASMR of bladder cancer will maintain a steady downward trend during 2022–2045, and kidney cancer will also show consistent declines in age-standardized rates over the same period (Table S14, S15). Global burden trends (1990–2021) and projections (2021–2045) for smoking-attributable prostate (purple), bladder (green), and kidney (yellow) cancers. (a) DALYs. (b) ASDR. (c) Deaths. (d) ASMR. (Solid lines: observed; Dashed lines: predicted). The vertical dashed line marks the year 2021. Rates are per 100,000 population.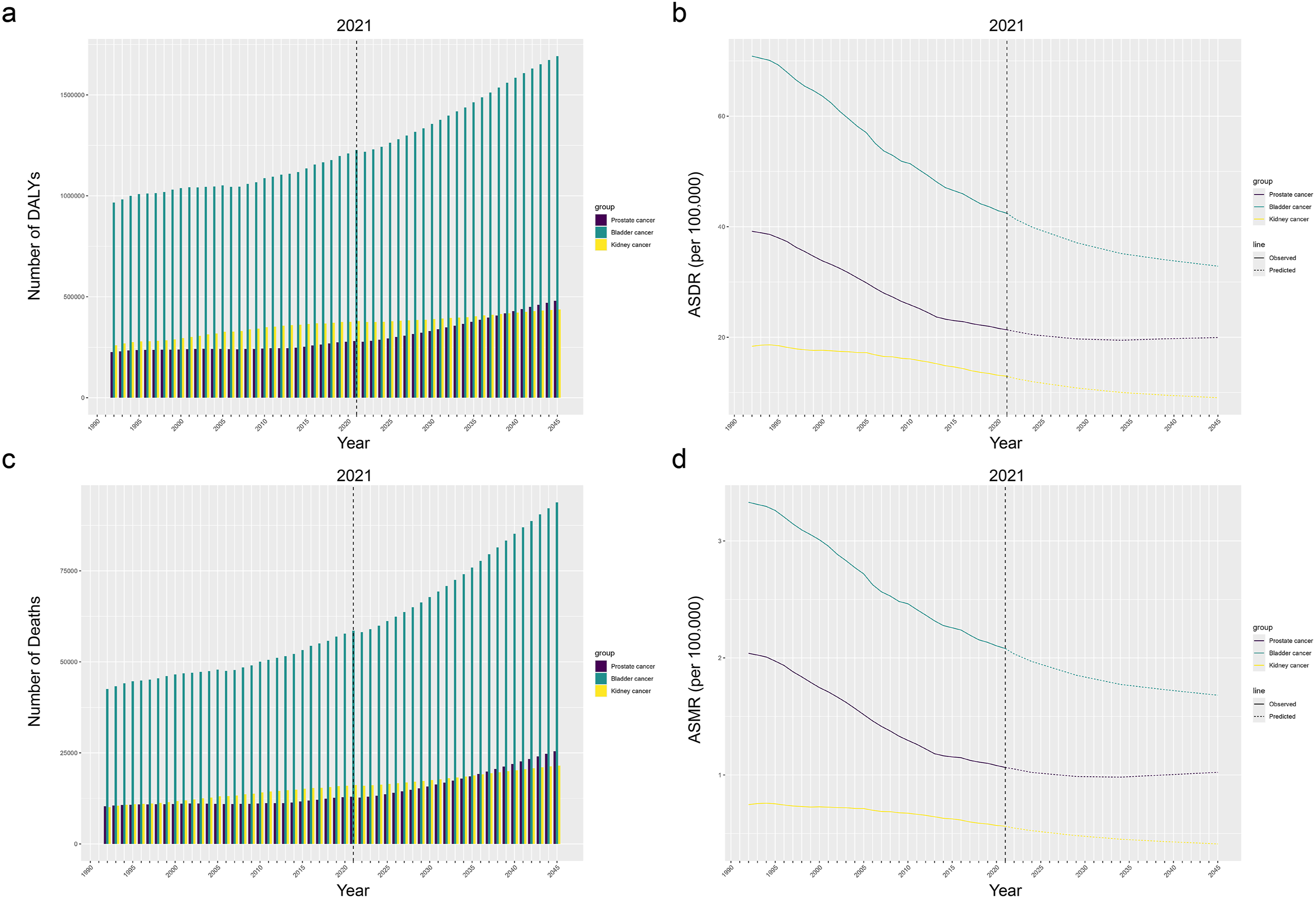
Discussion
Prostate, bladder, and kidney cancers are common urological malignancies posing a major threat to global health. Prostate cancer is the second most frequent cancer in men, while kidney cancer ranks third in incidence among urological malignancies but has the highest mortality rate of the three.29,30 Bladder cancer significantly impacts patients and healthcare systems due to its high recurrence rate and costly treatments. 31 Smoking has a profound and severe impact on urological cancers. According to the World Health Organization, tobacco use kills over 8 million people annually worldwide, including about 1.3 million non-smokers exposed to second-hand smoke.32,33 Smoking not only increases lung cancer risk but is also closely linked to the incidence of several urological cancers. 34 It is a significant risk factor for prostate cancer; tobacco smoke contains at least 69 carcinogens which can increase prostate cancer risk.35–37 Approximately 50% of bladder cancer cases are attributed to smoking, likely due to carcinogen-induced DNA damage.38,39 Smoking is also associated with increased cancer-specific mortality and higher risk of tumor recurrence. 40 Smokers face an elevated risk of kidney cancer and higher likelihood of disease recurrence. 19 Given the established links between smoking and these cancers, enhancing public awareness is crucial for promoting prevention, encouraging tobacco cessation, and ultimately reducing their incidence. Education and advocacy are key to alerting people to the dangers of smoking and fostering healthier lifestyle choices, which is vital for alleviating the global burden of these cancers. This study provides a focused, high-risk population-based analysis restricted to adults aged 40 years and older and offers novel 2045 projections, which represent unique strengths compared with general population-based burden studies.
This study provides epidemiological insights into the global, regional, and national burden of prostate, bladder, and kidney cancers attributable to smoking from 1990 to 2021 using the latest GBD 2021 data. We assessed trends over 30 years using EAPC analysis and employed the Nordpred model for future projections. From 1990 to 2021, although the global ASDR and ASMR for these smoking-attributable cancers showed a declining trend, the absolute number of DALYs and deaths continued to rise. This suggests progress in reducing mortality rates, but an increasing overall disease burden, potentially linked to global population growth, economic development, aging, and persistent smoking behavior. The most significant decline in EAPC values for ASDR and ASMR was observed for prostate cancer, possibly due to more effective prevention, early diagnosis (e.g., PSA screening, improved biopsy techniques), and treatment strategies (e.g., advances in surgery, radiotherapy, hormonal therapy, drugs, and active surveillance). Shifts in the age groups with the highest DALYs and deaths for these cancers may relate to medical advancements enabling earlier detection and treatment, as well as changes in cancer progression.
Analysis across five SDI regions revealed significant disparities. High and High-middle SDI regions bore the heaviest burden in 2021 but also showed the largest decreases over 30 years. This could be explained by better implementation of routine early cancer screening and tobacco control policies in High SDI regions, which are established interventions for reducing smoking-attributable cancer mortality. Enhancements in healthcare quality, including novel therapies like targeted treatments and immunotherapy,41,42 along with standardized diagnostic and treatment processes, have contributed to improved outcomes. Furthermore, these regions have implemented effective tobacco control measures such as increased taxation, smoke-free public place laws, and health education.43,44 Notably, Middle and Low-middle SDI regions even experienced an increasing burden for kidney cancer, highlighting global inequities in cancer control. Tobacco use remains prevalent in lower-SDI regions; WHO reports indicate slower declines in tobacco use prevalence in these areas, with absolute user numbers still increasing in some regions due to population growth and aging, potentially raising the overall burden of tobacco-related diseases. 45 Targeted interventions—such as strengthened smoking cessation campaigns, enhanced early screening, and improved healthcare access—are crucial for reducing the global cancer burden, particularly in lower-SDI regions.
Examining 21 GBD regions showed significant variations in the DALYs and mortality of smoking-attributable cancers. The highest burden shifted from Western Europe and High-income North America to East Asia (in terms of DALYs for bladder and kidney cancers) and multiple Central and Eastern European regions (in terms of ASDR/ASMR). This period was characterized by universally declining bladder cancer rates, contrasting with rising prostate and kidney cancer rates in specific regions such as Eastern Europe and Central Asia. These divergent trends underscore the differential effectiveness of global tobacco control and highlight the urgent need for targeted prevention and early detection strategies in high-risk regions.
Analysis at the national level revealed that while high-income countries have made significant progress, middle- and low-income countries face growing cancer burdens. According to the WHO, about 80% of the world’s 1.1 billion adult smokers live in low- and middle-income countries, with approximately 226 million living in poverty. 46 Additionally, 44 countries lack implementation of any WHO MPOWER tobacco control measure, and 53 countries do not have completely smoke-free healthcare facilities. Future policy efforts should focus on strengthening tobacco control in middle-income countries, promoting effective early screening and health interventions, and improving healthcare resources and services in low-income regions to reduce the global burden of smoking-attributable cancers.
Finally, our projections for 2022–2045 suggest divergent future trends across the three smoking-attributable urological cancers. The ASDR and ASMR of prostate cancer may gradually decline before rebounding after 2035, a pattern partly driven by population ageing and shifts in screening practices. Since prostate cancer is affected by multiple non-lifestyle and metabolic risk factors independent of smoking, the long-term benefits of tobacco control may be gradually offset by other population-level drivers. 47 In contrast, bladder cancer is projected to maintain a steady downward trend without a clear inflection point. This likely reflects its stronger epidemiological association with smoking, making its burden more responsive to tobacco control interventions, while the lack of population-wide screening minimizes artificial changes in recorded incidence. 48 For kidney cancer, with a weaker smoking-attributable association, age-standardized rates are expected to decline slowly and steadily; stable metabolic risk profiles and limited routine screening may also contribute to this smooth long-term trajectory. 49 Notably, despite heterogeneous trends in age-standardized rates, the absolute numbers of deaths and DALYs for all three cancers are projected to rise continuously, mainly due to global population growth and ageing.
Based on these projected divergent trends, targeted prevention strategies can be tailored to regions with different SDI levels. For High and High-middle SDI regions facing potential prostate cancer burden rebound, rational screening planning and standardized tobacco control are essential to address the combined impacts of population ageing and lifestyle-related risks. Middle SDI regions should sustain tobacco control efforts to maintain declining bladder and kidney cancer burdens. For Low-middle and Low SDI regions with growing absolute disease burden, priority should be placed on health promotion and community-level interventions to curb future case growth.
This study has several prominent strengths. First, this analysis was based on standardized GBD data covering population-based epidemiological records across 204 countries and territories, ensuring good comparability and generalizability. Second, we performed multi-dimensional assessments stratified by global regions, individual countries, and SDI levels, clarifying hierarchical disparities in smoking-attributable urological cancer burden. Third, we jointly compared three major smoking-attributable urological cancers, identifying their distinct epidemiological features and heterogeneous long-term trends. Fourth, we used the EAPC model to quantify 31-year temporal trends and the Nordpred model to project burden trajectories to 2045, providing evidence for differentiated tobacco control and cancer prevention strategies.
This study also has limitations. Data were derived from GBD 2021 modeled estimates instead of direct surveillance data, whose accuracy is constrained by incomplete vital registration, cancer registry, and survey data, especially in low-income and low-SDI regions with underdeveloped health information systems. GBD 2021 applies the Bayesian hierarchical DisMod-MR model to impute missing data, yet under-reporting and under-diagnosis may introduce estimation bias in resource-limited areas. Moreover, model-driven extrapolation and smoothing may mask local epidemiological heterogeneity, increasing uncertainty in data-sparse regions. Thus, our findings should be interpreted cautiously, highlighting the need for improved global health data infrastructure. In addition, 2045 burden projections are scenario-based simulations rather than fixed predictions; future tobacco policies, smoking prevalence, medical advances, and demographic changes may alter real-world trends.
Conclusion
In conclusion, from 1990 to 2021, the global burden of smoking-attributable prostate, bladder, and kidney cancers in adults aged 40 years and older has changed dynamically. Substantial differences exist between age groups, SDI regions, 21GBD regions, and 204 countries and territories. Targeted public health interventions are needed, integrating intensified tobacco control and cancer screening into healthcare for middle-aged and older adults, with a focus on low-SDI regions.
Supplemental material
Supplemental material - A retrospective observational analysis of the global burden of smoking-attributable prostate, bladder, and kidney cancers among adults aged 40 years and older: Based on the global burden of disease study 2021 with projections to 2045
Supplemental material for A retrospective observational analysis of the global burden of smoking-attributable prostate, bladder, and kidney cancers among adults aged 40 years and older: Based on the global burden of disease study 2021 with projections to 2045 by Naiwen Chen, Jinming Cai, Jinpeng Feng, Yi He, and Dongliang Xu in Science Progress.
Footnotes
Acknowledgements
The authors would like to thank the IHME for providing the publicly available GBD 2021 dataset.
Author contributions
NC, JC and JF conceived and designed the study. NC performed data extraction and statistical analysis. NC and JF drafted the manuscript. YH and DX supervised the whole work, revised the manuscript critically. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82174122 to Dongliang Xu), the Health Discipline Leader Program of Shanghai Health Commission (2022XD011 to Dongliang Xu), and Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine - Project Challenge Initiative (SGYYJBGS-002 to Dongliang Xu), and the Jiaxing Key Laboratory of Precision Diagnosis and Treatment of Urologic Tumors (2020-mnzdsys to Yi He).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.