
Abstract
A patient presented having an acute abdomen on a background of a twelve-month history of worsening asthma. Computed tomography showed giant bilateral intrathoracic hernias extending to both thoracic apices. Our case was unusual as the defect was bilateral and left-sided. Surgical repair revealed each hernia sac measuring >20 cm and to contain the entirety of the small bowel and colon (including retroperitoneal bowel). The appendix was discovered adjacent to right superior pulmonary vein. Both sacs were excised and the defects dissected and transfixed in a single stage operation. In the post-operative stage, he developed a 6.3 cm fluid collection anterior to the right atrium and a left-sided pleural effusion. Morgagni hernias can escape detection and be attributed to other diagnoses courtesy of false localising signs on clinical examination and symptoms in the history.
Introduction
Morgagni hernias occur due to congenital herniation of abdominal contents into the thorax. The pathological process is a retrosternal diaphragmatic defect. Giovanni Battista Morgagni first described them in 1769 as a hernia that originated from the sternocostal trigone. They can escape detection due to symptoms being attributed to other common diagnoses (e.g. asthma and constipation). It requires astute clinical suspicion to avert morbidity and mortality.
Clinical summary
A 45-year-old male presented having an acute abdomen on a background of a twelve-month history of worsening asthma. On admission to a local hospital he had a three-week history of colicky abdominal pain but was not obstructed. No hernias were palpable. His medical history included a non-injurious car accident and a bilateral inguinal hernia repair 17 years ago.
A chest X-ray (Figure 1) conducted six months prior during an original admission for abdominal pain did reveal an abnormal thoracic cavity. During his readmission for colicky abdominal pain inspection of these films concluded a non-abdominal cause for his pain six months previously and a thoracic opinion was then sought. Computed tomography showed massive bilateral intrathoracic hernias (Figure 2) and herniation of abdominal contents through an antero-medial bilateral diaphragmatic defect. Prior to surgical correction he was optimised and received regular clinic reviews due to experiencing exacerbations of abdominal pain. This required an interim admission for analgesia.
(a) CXR (posteroanterior) six months before the operation showing compression of both lung fields and (b) CXR (lateral) six months before the operation showing compression of the left lung field. (a) HRCT (coronal) two months before the operation showing super giant Morgagni herniae, (b) HRCT (sagittal) two months before the operation showing super giant Morgagni herniae, (c) HRCT (axial) at the level of the pulmonary trunk two months before the operation showing super giant Morgagni herniae and (d) HRCT (axial) at the level of the inferior cardiac border two months before the operation showing super giant Morgagni herniae.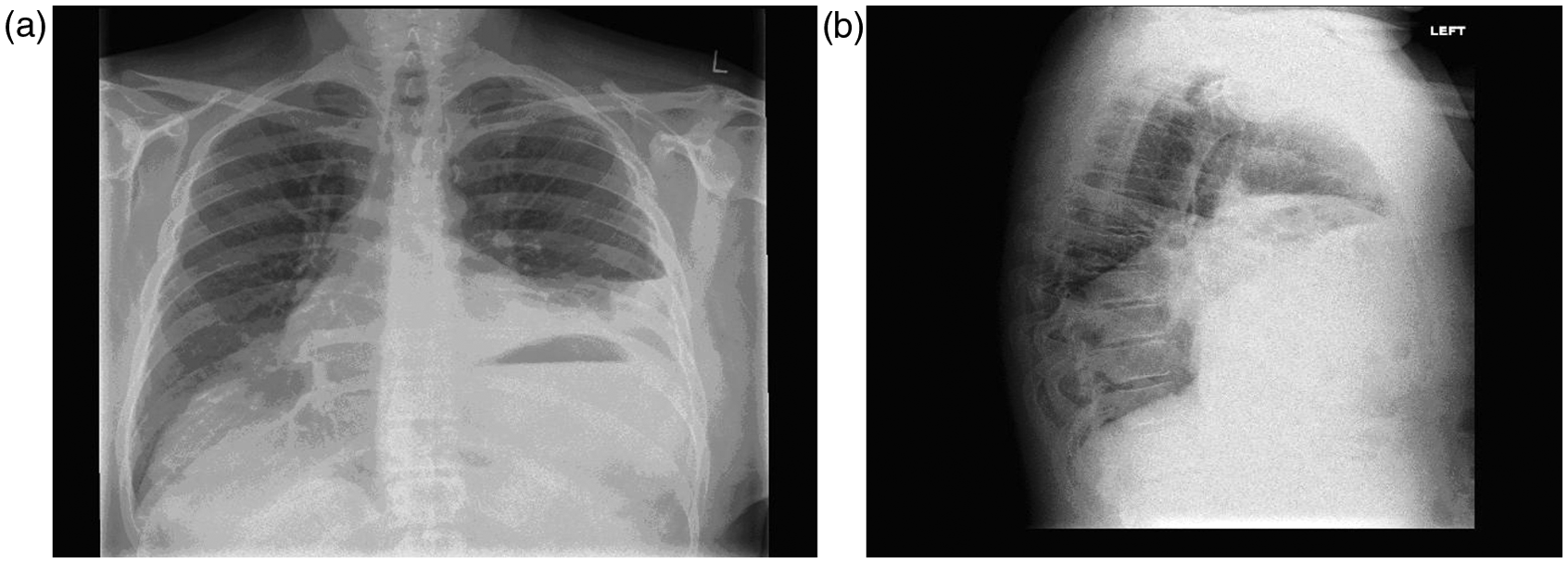
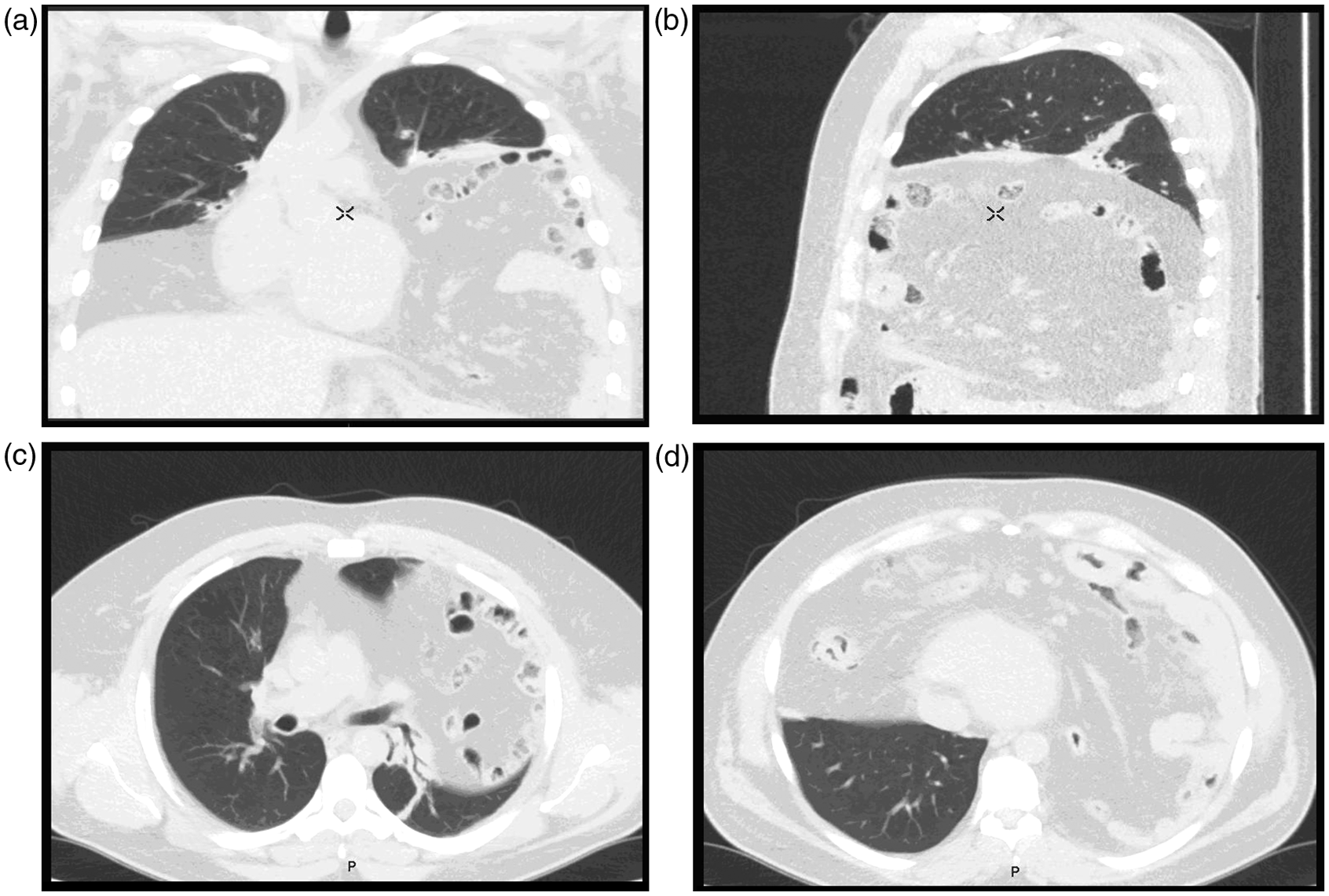
The defects measured 6.7 cm on the left and 6.0 cm on the right. Both included herniated abdominal fat and small bowel and large bowel extending beyond the aortic arch and superior pulmonary vein. Both lungs were compressed into the apices showing marked consolidation and atelectasis. His observations and laboratory results were both remarkably normal. There were no other abdominal and thoracic abnormalities.
Open surgical repair through a left-sided approach revealed each hernia sac to measure >20 cm and to contain the entirety of the small bowel and colon (including retroperitoneal bowel). The appendix was discovered adjacent to the right superior pulmonary vein. But both sacs were excised and the defects dissected and transfixed in a single-stage operation: the right being sutured around the costal cartilage and the left repaired using a Marlex mesh. Sputum cultured pseudomonas requiring a sustained course of IV antibiotics.
In the post-operative period, he developed a 6.3 cm fluid collection anterior to the right atrium and a left-sided pleural effusion. Insertion of a chest drain ameliorated the effusion and he was discharged home.
Discussion
Morgagni hernias are a rare form of congenital diaphragmatic hernia. It represents 2% of the 2/10,000 incidence of congenital diaphragmatic herniae. 1 The defect occurs through the foramen of Morgagni–Larrey. The weakness is caused by defective fusion of the septum transversum around the costal edge of the diaphragm. 2 The hernia is usually right-sided as it is hypothesised that additional attachment of pericardial ligaments reinforces the left side of the diaphragm. Our case was unusual as the defect was bilateral and left-sided. It highlights the confusing picture of lobe compression masquerading as respiratory symptoms in someone assumed to be asthmatic.
Our case highlights a diagnostic dilemma of a longstanding history of asthma being complicating diagnosis. Shackleford and Hunt 4 highlight this difficulty in a historic case resulting in a patient being misdiagnosed as having asthma. Other cases report the correct diagnosis being delayed by the patient presenting with predominantly respiratory symptoms and signs (e.g. pneumonia). 4 Retrospective studies clarify the observation that the most common symptoms at presentation are respiratory ones and the need for heightened clinical awareness to reduce diagnostic delay.5,6 Horton et al. 3 showed in a large retrospective analysis of 300 cases that 72% of Morgagni hernias are symptomatic.
Risk factors include a predisposition to increased intra-abdominal pressure.5,7,8 Our patient was obese and worked as a manual labourer having previously undergone two inguinal hernia repairs occurring and sustained abdominal trauma in a road traffic accident.
Increasing evidence supports a less invasive approach (e.g. laparoscopic) in small unilateral hernia. But defect size and bilateral nature in our case necessitated an open reduction and repair. 5 Less invasive approaches minimise risks but the complications can include fatal pneumopericardium. 9 Given that both hernia sacs were extremely large and both lungs had endured chronic compression the probability of complication was high further necessitating open repair.
Conclusion
Morgagni hernias can escape detection due to symptoms ascribed to other diagnoses. Our patient endured a twelve-month history of worsening asthma. It requires astute clinical suspicion to avert potential unnecessary morbidity and mortality and in some cases still requires open as opposed to laparoscopic surgical repair.
Footnotes
Acknowledgements
The authors wish to thank NHS Lothian and the Department of Cardiothoracic Surgery at the Royal Infirmary of Edinburgh and the Department of Medicine at the Victoria Hospital in Kirkaldy for their support.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.