
Abstract
Background and aims
Estimate costs for health and social care services in managing older people in the community who fall.
Method and results
Analyses of predominantly national databases using cost of illness methodologies. In Scotland, 294,000 (34%) of people over 65 years and living in the community fall at least once a year. Of these 20%, almost 60,000 people contacted a medical service for assistance. There were almost 30,000 attendances at GP practices, over 36,100 calls to the Scottish Ambulance Service and 46,816 people presenting at A&E, with 16,549 admitted, 30% with a hip fracture. Mortality was high, 7% during the hospital stay, rising to over 12% at 1 year. Over 20% of patients were unable to return to their homes. Associated costs were over £470 million, with 60% incurred by social services, mainly providing long-term care. Cost per person falling was over £1720, rising to over £8600 for those seeking medical assistance. A hip fracture admission cost £39,490, compared with £21,960 for other falls-related admissions.
Conclusions
Transparent, robust cost information demonstrates the substantial burden of falls for health and social care services and should be a driver for implementing evidence-based interventions to reduce falls.
Keywords
Introduction
Falls among older people present a serious and increasing public health challenge. Evidence shows many can be avoided, 1 offering benefits to the person and carer from reduced morbidity and mortality whilst releasing resources and costs that would otherwise be incurred, particularly by health and social services.
Without action, the impact of falls on the NHS and social work will grow substantially with the number of people aged over 65 years forecast to rise by a third by 2025 and those aged over 80 forecast to double in the same period. 2 Moreover, a higher proportion of the population will have multimorbidity (the presence of two or more disorders), 3 have poorer functional status and take polypharmacy, all significant falls risk factors. The cost of doing nothing is thus high in human and financial terms, whilst placing major strains on the services’ ability to co-ordinate care effectively and deliver compassionate and sustainable services.
Despite increasing evidence that interventions reduce the risk of falling in older age,1,4 implementation has been poor.5,6 Policy makers and healthcare professionals have been hampered in allocating scarce resources to falls prevention by the absence of data on cost of falls. Thus, they cannot evaluate if potential programmes provide benefits which outweigh their costs, making funding decisions problematic in the face of competing needs.
A systematic review of peer-reviewed articles reporting falls costs for older people living in the community noted that, in contrast to many areas of healthcare, there is a ‘glaring need’ for such data. 7 Only two studies reported costs in the UK. One was limited to an ambulance service’s costs whilst the other estimated NHS and social care costs at £981 million. Updating that search identified a recent estimate that falls cost the UK NHS over £2.3 billion annually but no supporting information was provided. 8 The burden of falls is thus not well established.
To remedy this, the Scottish Government commissioned research into the burden of falls on its older population living in the community, together with the associated cost implication for its health and social care staff and services. The objective is to quantify the financial burden of serious falls, defined as resulting in injuries that require medical assistance, on health and care services.
Research results will inform decision making on implementing care bundles to reduce falls in the community. This understanding will enable evaluation of alternative programmes and assist implementation by identifying potential resources and costs which should be released by effective preventative interventions.
Methods
A literature search was undertaken on the epidemiology of falls in the UK. Data on the number of people who fall attending general practitioners’ (GP) practices, requiring ambulance service, A&E, hospitalisation and subsequent care home residence were requested from Information Services Division (ISD) 9 and the Scottish Ambulance Service (SAS). Analyses were conducted for Community Health Partnerships (CHP) in Scotland and the results shared with the Falls Lead in each CHP. The Leads were asked to verify these estimates were accurate and consistent with their own records; no inconsistencies were found. Methodologies adopted are consistent with recent guidelines for evaluating falls interventions. 10
This work was supported by Scottish Government who paid Joyce Craig for her input.
Results
Number of people who fall
Population and people who fall in Scotland.

Number of falls-related events Scotland 2010/2011.
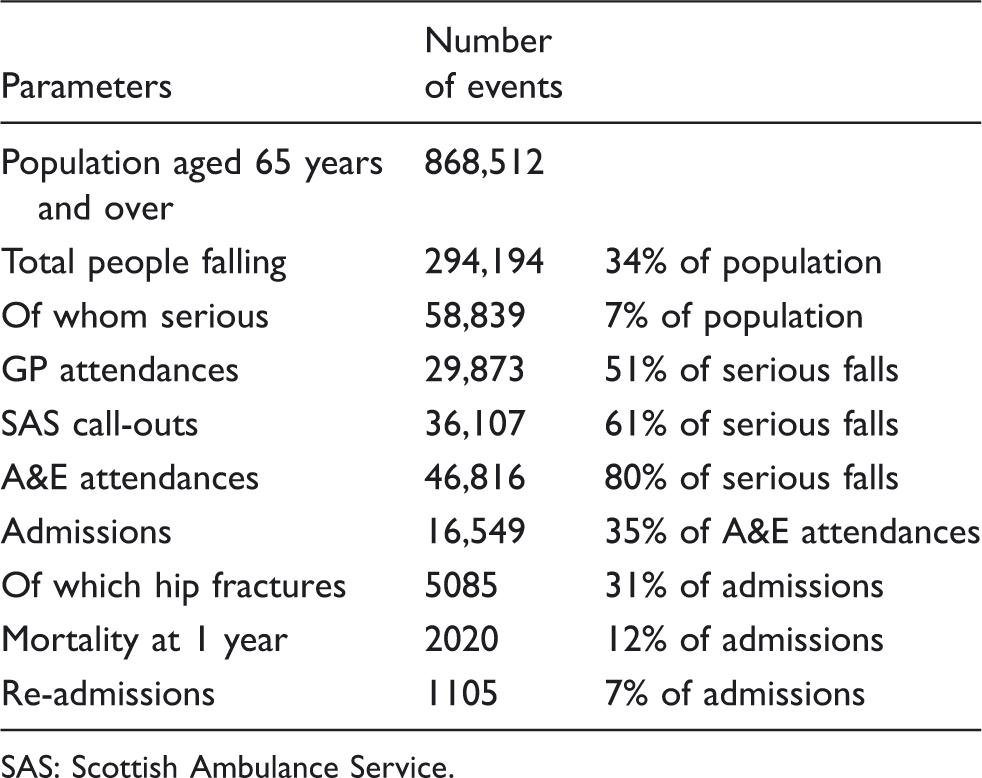
SAS: Scottish Ambulance Service.
ISD estimated that in 2011, the number of people aged over 65 years living in the community and attending their GP for a fall-related incident was 23,480, (95% confidence intervals (CI) of 18,500–28,440). The mean GP contacts per faller were 1.27, giving a total number of GP attendances as 29,873. One quarter of attendees were aged between 65 and 80 years, with three quarters over 80 years.
Annualising data from SAS for the first half of 2011 suggested in that year falls-related incidents attended for older people living in the community were 36,107, with 28,090 (78%) conveyed to hospital.
No national data were available on the number of A&E attendees resulting from a fall. The estimated number was 46,816, assuming 40% arrive other than by ambulance. This was based on data from two NHS areas and was consistent with preliminary data from a pilot A&E IT project.
Admissions and length of stay
ISD data showed 35% of presenters at A&E after a fall were admitted; 16,549 people of whom over 30% (5085) had a hip fracture. About 7% were re-admitted within 1 year with a fall or hip fracture as the primary diagnosis.
The length of hospital stay showed considerable variation across mainland NHS boards. Mean stay for a hip fracture or a falls event were 29 days (range 21–37 days) and 19 days (range 14–24 days) respectively. Re-admissions were assumed to have the same length of stay as initial admissions.
Mortality and discharge by place of residence
Overall mortality was 7% (1081 patients) and 12% (2020) in hospital and at 1 year post-discharge respectively. Scottish Hip Fracture Audit 2008 provided discharge destination following acute care. 12 At 120 days post-admission for a hip fracture, 64% of people resided at home with the balance in some form of rehabilitation or long-term care home setting or still an inpatient.
Post-discharge
At discharge, all patients were assumed to have a shared assessment by a social care worker and community therapist taking 1 h at a cost of £84. For those going directly home, a package comprising a GP visit (£36) and 8 weeks of ‘low cost’ care including home care and healthcare at a unit cost of £207 per week was assumed, giving a total cost, including assessment, of £1776.
Using data from the annual census of care homes conducted by ISD, 13 for those discharged into a care setting but able to return home by 120 days, a care package comprising 60 days of residential care at a cost of £780 per week plus the same package of care provided to those discharged directly home was assumed at a total cost of £8406.
Costs for those remaining in residential care were estimated at £2810 per month Applying a mean length of stay 27.3 months, also obtained from census data, gave an estimated out-turn cost per resident of £76,630. This was discounted at 3.5% per annum in accordance with central guidance 14 to give an equivalent cost in 2012 of £65,942.
Estimated cost of falls
Estimated cost of falls and fractures in Scotland 2010/2011.
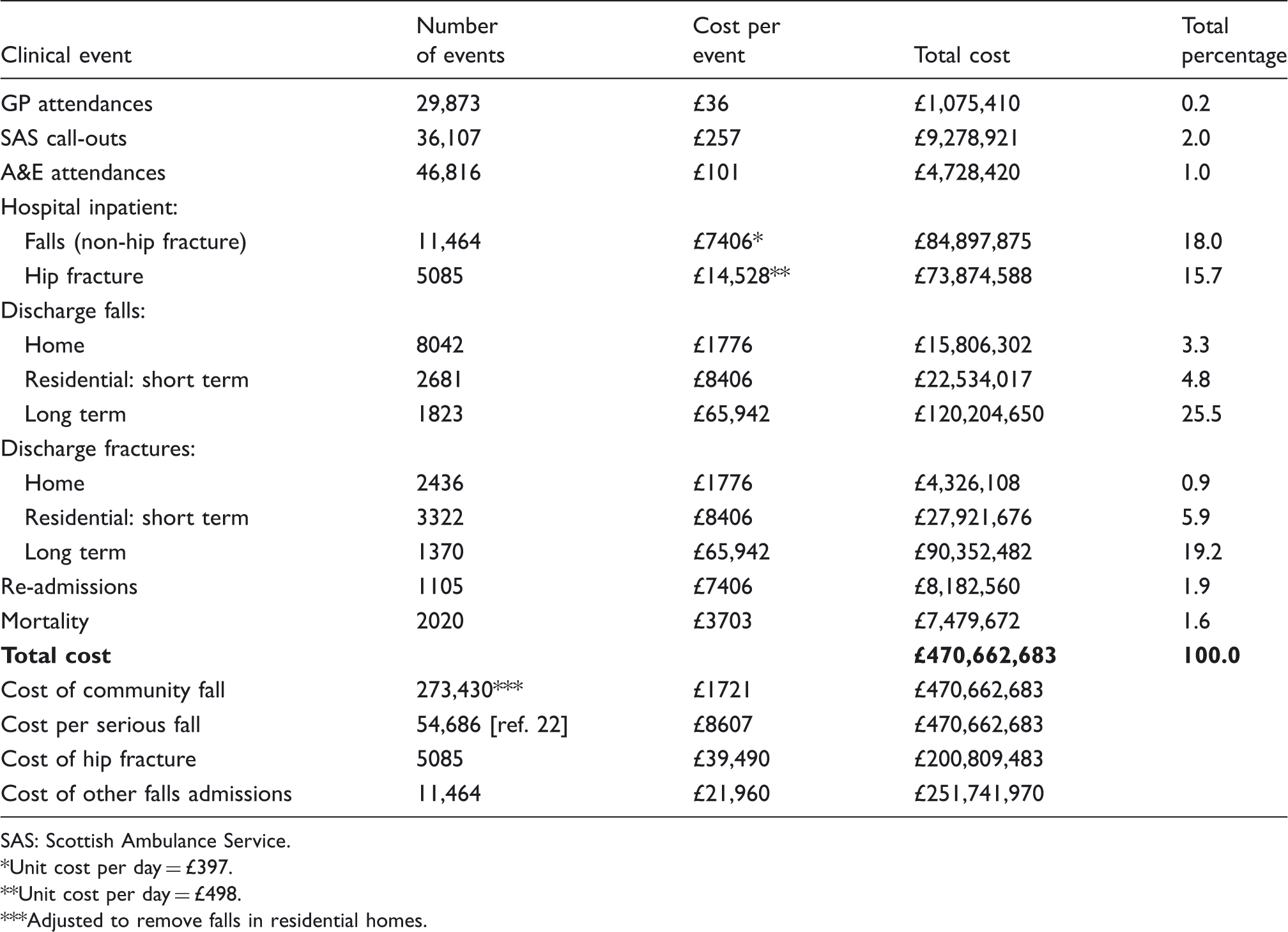
SAS: Scottish Ambulance Service.
Unit cost per day = £397.
Unit cost per day = £498.
Adjusted to remove falls in residential homes.
Dividing total cost by the number of falls in the community (273,430) gave an estimated cost per fall of almost £700 to the NHS rising to £1721 including social care costs. The estimated cost to manage the 20% of these which are serious, requiring medical attention was £3466, increasing to £8607 including social care costs. Cost of a hospital admission for a hip fracture, from calling an ambulance to costs arising after discharge, including any subsequent re-admissions, was estimated at £39,490, with each other falls-related admission estimated to cost £21,960.
Discussion
Evidence from Scottish national datasets has identified the burden of falls on health and social care services as being approximately 85,000 episodes each year resulting from attendances at GP practices, calls to SAS or people presenting directly at A&E. This leads to 16,549 hospital inpatient admissions annually in Scotland. Of these, 7% died before discharge and over 20% were unable to return home. Associated costs were estimated at over £470 million, with 60% falling on social services.
The main limitations of this study include the use of only national datasets. These include data which are quality assured for consistency of definitions, coding, accuracy and comparability across sources. 17 Consequently, no activity or costs were provided for non-quality assured data including attendances at outpatient services, fracture liaison clinics, osteoporosis services, medications, long-term social care support in the community, provision of aids and adaptations, and of community alarms and other telecare devices. Furthermore, data quality relies on consistent use of coding across health boards. Historically, falls have been under-recorded. We also acknowledge that indirect costs incurred by patients, families, unpaid carers and wider societal costs including loss in productivity from absenteeism go unaccounted for. Hence, the costs in this analysis are judged conservative estimates. Nevertheless, these costs, whilst specific to Scotland, are anticipated to generalise to other parts of the UK. For example, the cost per fall, calculated by dividing the independently derived estimated cost of £2.3 billion 8 in the UK, by the estimated number of falls, was £667; a difference of under 5% from the £693 estimated from this work.
The high cost of falls, in particular of hip fractures, at £39,490 per event, supports the evaluation of effective interventions to reduce the risk of fracture at either the individual or population level. The evidence base for falls risk reduction is expanding with the most recent Cochrane review in 2009 systematically reviewing 111 trials with 55,303 participants in a community setting. 1 This concluded ‘assessment and individualised multifactorial intervention programmes appear effective in reducing the rate of falls in studies from different healthcare systems’. However, only eight studies provided a comprehensive economic evaluation leading the authors to further comment: ‘there was some, although limited, evidence that falls prevention strategies can be cost saving during the trial period, and may also be cost-effective over the participants remaining lifetime’.
The evidence base for single interventions, in particular exercise,18,19 is widely published. In 2008, Sherrington et al.’s 4 meta-analysis confirmed that ‘the pooled estimate of the effect of exercise was that it reduced the rate of falling by 17% (44 trials with 9603 participants, rate ratio (RR) = 0.83, 95% confidence interval (CI) = 0.75–0.91, P < 0.001’. The greatest benefit arose from programmes providing over 50 h of individualised targeted gait and balance exercises. Originating from New Zealand, the Otago Exercise Programme adheres to these recommendations and has demonstrated in meta-analysis significantly reduced fall rates (incidence RR = 0.68, 95% CI = 0.56–0.79). 20 It is one of the few exercise interventions to prove its cost effectiveness in adults over 80 years old, alongside two other interventions; an individually customised multifactorial programme in those with four or more of the eight targeted fall risk factors and a home safety programme in those who had previously fallen. 21 However, earlier papers by the New Zealand group in 2001 did not demonstrate net savings in healthcare costs despite showing a clear reduction in falls with the home-based exercise programme. 22 More recently in Australia, the most cost-effective intervention at a population level was analysed to be Tai Chi. 23 Despite the relative paucity of cost-benefit evidence, some authors have argued that given falls are the largest single risk factor for hip fracture, 24 interventions to reduce these should be prioritised for evaluation.
Of course, prevention of hip and other fractures should also include assessment and management of osteoporosis. Oral bisphosphonates remain the mainstay of treatment and have been shown to be cost effective for all women, regardless of quartile of life expectancy or age. 25 Further research is ongoing regarding newer medicines including zoledronate and denosumab.
Less easy to quantify is the impact of falls on physical and psychological functioning including the impact of early admission to long-term care facilities upon quality of life. People who fall and remain in the community also have a high incidence of post-fall syndrome; symptoms include loss of self-confidence, mobility and balance issues with the resulting social isolation associated with loneliness, depression, increased dependency and a poorer quality of life. These factors can affect quality of life more profoundly than the initial fall, with repercussions on the lives of family and friends. 26
Further work is required to assess the economic implications of investing in national falls programmes and care bundle in an attempt to reduce the heavy financial burden of falls to health and social care, balanced against the current evidence of their clinical and economic effectiveness. This study should provide new and important data to enable policy makers and planners to decide where best to allocate resources. In addition, clinicians and researchers should find the data useful when evaluating falls interventions.
Footnotes
Declaration of conflicting interests
None declared.
Funding
Funding was provided by the Scottish Government to JC to lead the analysis. The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report or the decision to submit for publication. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Ethical approval
No ethical approvals were required.
Contributorship
AM and SM developed the initial concept of the work, approved the project design and collaborated with project delivery. JC provided the draft project design, requested data from various sources and undertook the data analysis. SC provided the data on NHS events and associated costs, whilst LS provided data on social care events and associated costs. LB provided the substantive draft and critically appraised the analysis. All commented on versions of the draft report and approved the version to be published.