
Abstract
Background
Gentamicin, one of the most commonly used antibiotics in neonates, has potential toxicity. This study was performed to determine the incidence of potential toxicity of gentamicin in term and preterm neonates.
Methods
A one-year retrospective study in neonates admitted to Special Baby Care Units at University Hospital of North Durham and Darlington Memorial Hospitals. We reviewed each admission and looked through the case notes in detail to document information about gentamicin administration, dosage and elevated gentamicin levels in the blood. Pre-third dose gentamicin levels >2 mg/L were classified as elevated.
Results
Overall, 192 babies (83 term and 109 preterm) had documented gentamicin levels. Of these, 43% (84/192) manifested elevated gentamicin levels. Of the babies with elevated gentamicin levels, 67% (56/84) weighed less than 2.5 kg. When a combination of gestation period and weight was considered, 61% (51/84) of preterm infants weighing <2.5 kg had elevated levels whereas only one term infant <2.5 kg exhibited elevated levels.
Conclusion
Preterm neonates and specifically low birth weight neonates tolerate gentamicin poorly. Dosage and/or interval of administration of the medication may need modification in this group to minimise toxicity.
Introduction
Neonatal units across the world use a combination of benzyl penicillin/amoxycillin/ampicillin and gentamicin to treat ‘suspected sepsis’ in neonates.1,2 The usual treatment guideline for suspected sepsis in full-term and preterm neonates >32 weeks’ gestation is benzyl penicillin/amoxycillin/ampicillin (30 mg/kg/dose BD) and gentamicin (5 mg/kg/day). For preterm babies under 32 weeks’ gestation, the guidance followed in administration of gentamicin is same (5 mg/kg/day), but the interval is 36 hourly. This combination is believed to be synergistic and possibly prevents/delays the development of resistance to either of the drugs. Some units consider spontaneous onset of preterm labour as a risk factor for infection in preterm neonates to start prophylactic treatment with this antibiotic cocktail, while other units follow a modified risk factor-based approach to initiate treatment. Nevertheless, it remains a fact that we possibly over treat many neonates – both term and preterm – who are confirmed healthy 48 h after birth by confirmatory tests like blood cultures. While we have information from innumerable numbers of babies across several units who receive antibiotics for ‘safety’ reasons in the 48 h after birth, there are no studies on the long-term implications of this prophylactic treatment on neonates. Acute but reversible derangements of renal functions and auditory/vestibular problems have been reported in babies with elevated gentamicin levels. This study was performed to determine the incidence of potential toxicity of gentamicin in term and preterm neonates, admitted to Special Baby Care Units (SBCU).
Method
We did a retrospective study of all admissions to the SBCU at University Hospital of North Durham and Darlington memorial Hospitals during a one-year period from May 2010 to April 2011. The number of admissions to the units during the study period was taken from the admission register maintained in the unit, excluding readmissions from other units. We reviewed each admission and looked through the case notes in detail for all babies. Gentamicin administration and dosage were checked from the prescription chart maintained in the notes and information regarding levels were obtained from documentation maintained in notes. Gentamicin dosage in babies over 32 weeks was 5 mg/kg once a day, as per recommendations of the Northern Neonatal Pharmacopeia. In babies under 32 weeks, gentamicin dosage used was 5 mg/kg once in 36 h. Gender, birth weight and gestation period were collected for each baby on an excel spread sheet. Gentamicin levels above 2 mg/L before the third dose were taken as the cut off for identifying babies with elevated levels. Data were analysed subsequently using Welch’s T test for univariate analysis of data on birth weight, Student’s T test for analysis of data on gestation and Chi Square test for data on gender. Regression analysis was also done on the combined data.
Results
Patient characteristics.
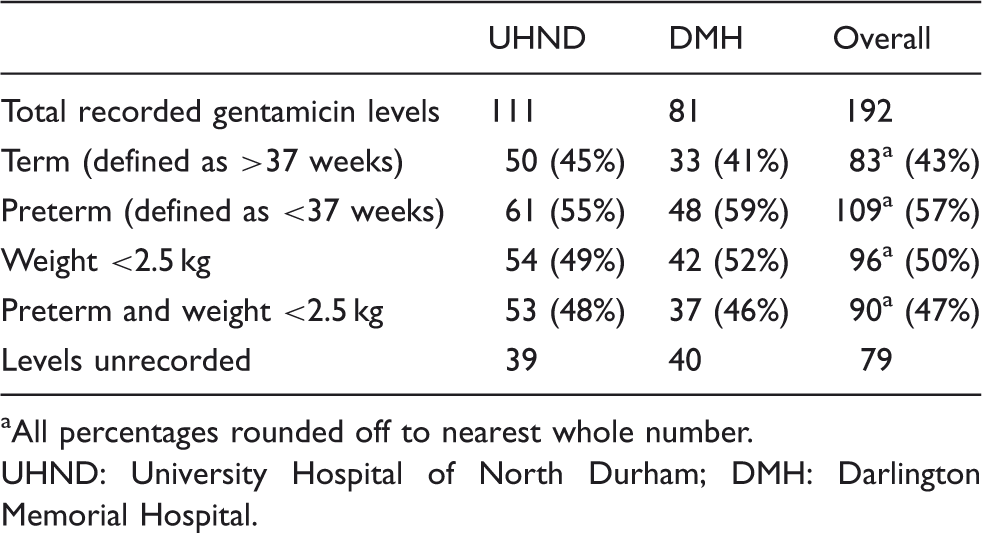
All percentages rounded off to nearest whole number.
UHND: University Hospital of North Durham; DMH: Darlington Memorial Hospital.
Break up of elevated gentamicin levels unit wise.
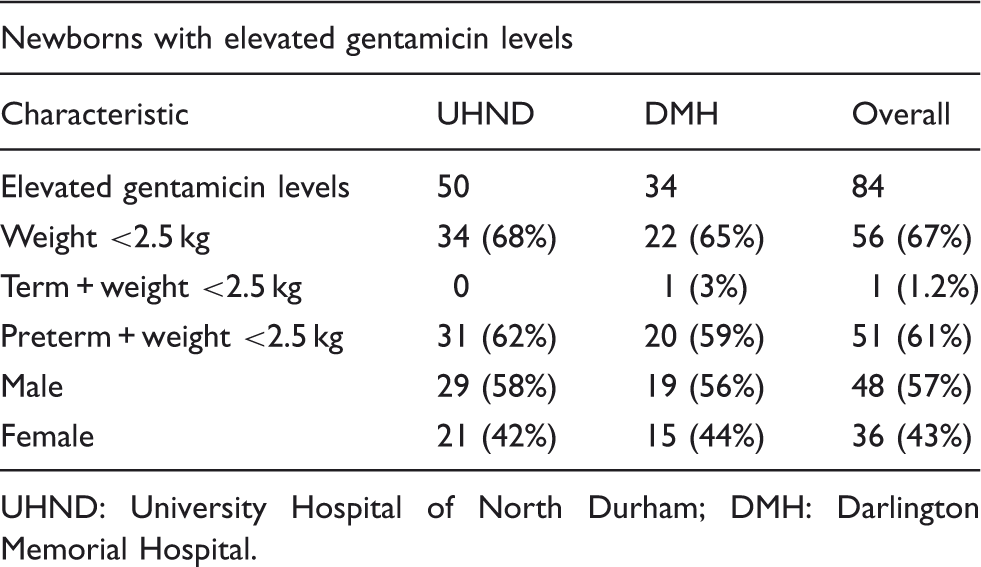
UHND: University Hospital of North Durham; DMH: Darlington Memorial Hospital.
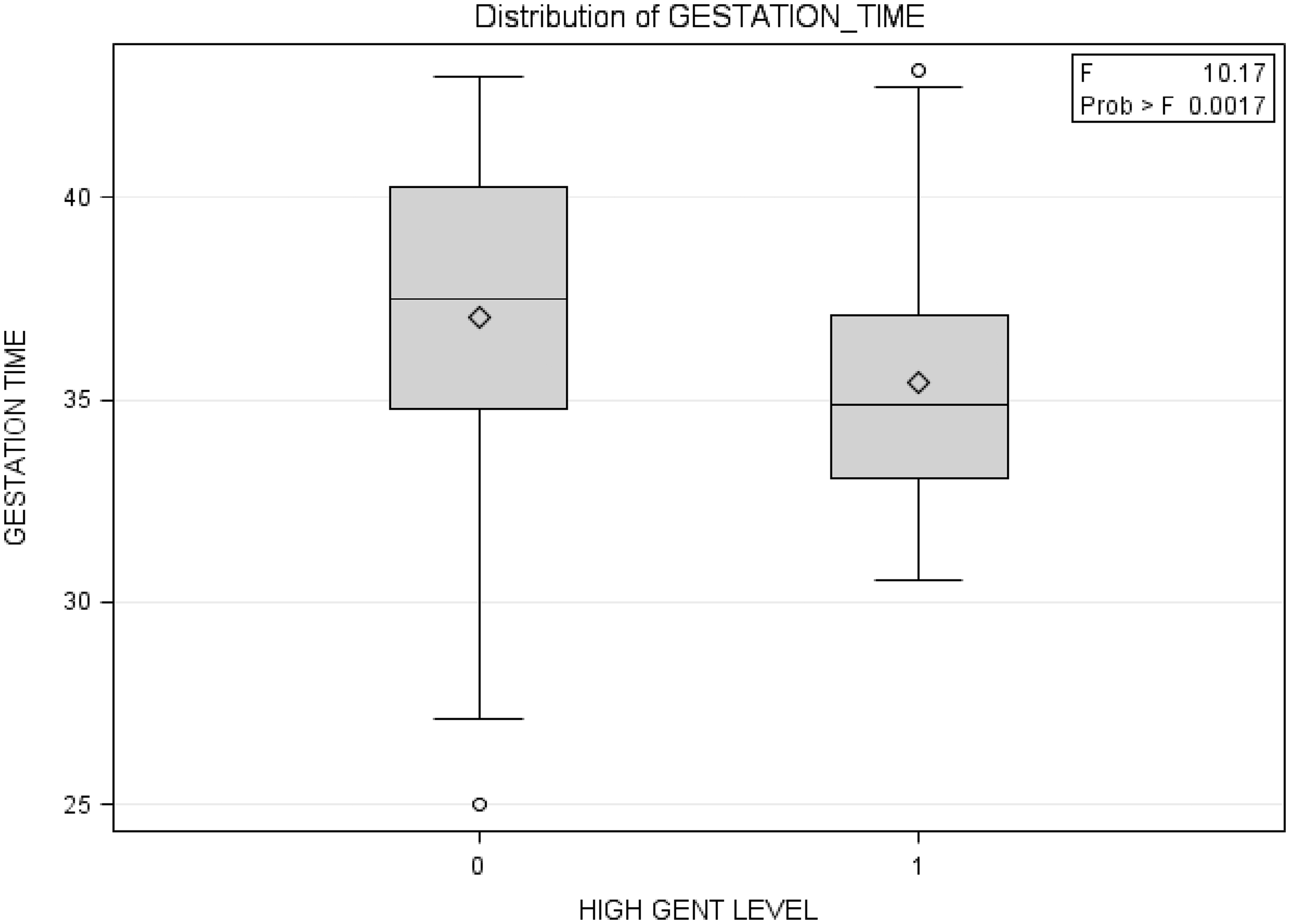
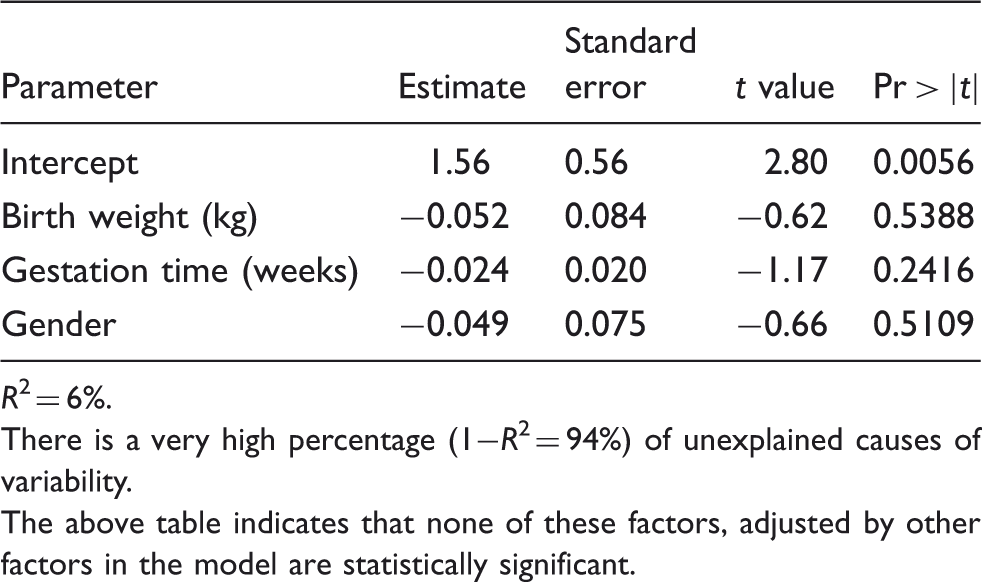
Univariate analysis (using Welch’s T test) confirmed low birth weight as a risk factor for elevated gentamicin levels (p = 0.0007) (Figure 1). Preterm gestation as an independent risk factor for elevated gentamicin levels was also confirmed to be statistically significant with a ‘p value’ of 0.0017 (using Student’s T test) (Figure 2). There was a minimal observed difference in the percentage of elevated levels between boys and girls, but no statistical significance for the difference was noted using Chi Square test (p = 0.74). Regression analysis using all three variables namely birth weight, gestational age and gender showed that none of these factors, adjusted by other factors in the model are statistically significant and that in 94% of cases, the causes of variability remain unexplained (Table 3).
Gentamicin levels in relation to birth weight. Gentamicin levels in relation to gestational age. Regression analysis using birth weight, gestational age and gender for elevated gentamicin levels. R2 = 6%. There is a very high percentage (1−R2 = 94%) of unexplained causes of variability. The above table indicates that none of these factors, adjusted by other factors in the model are statistically significant.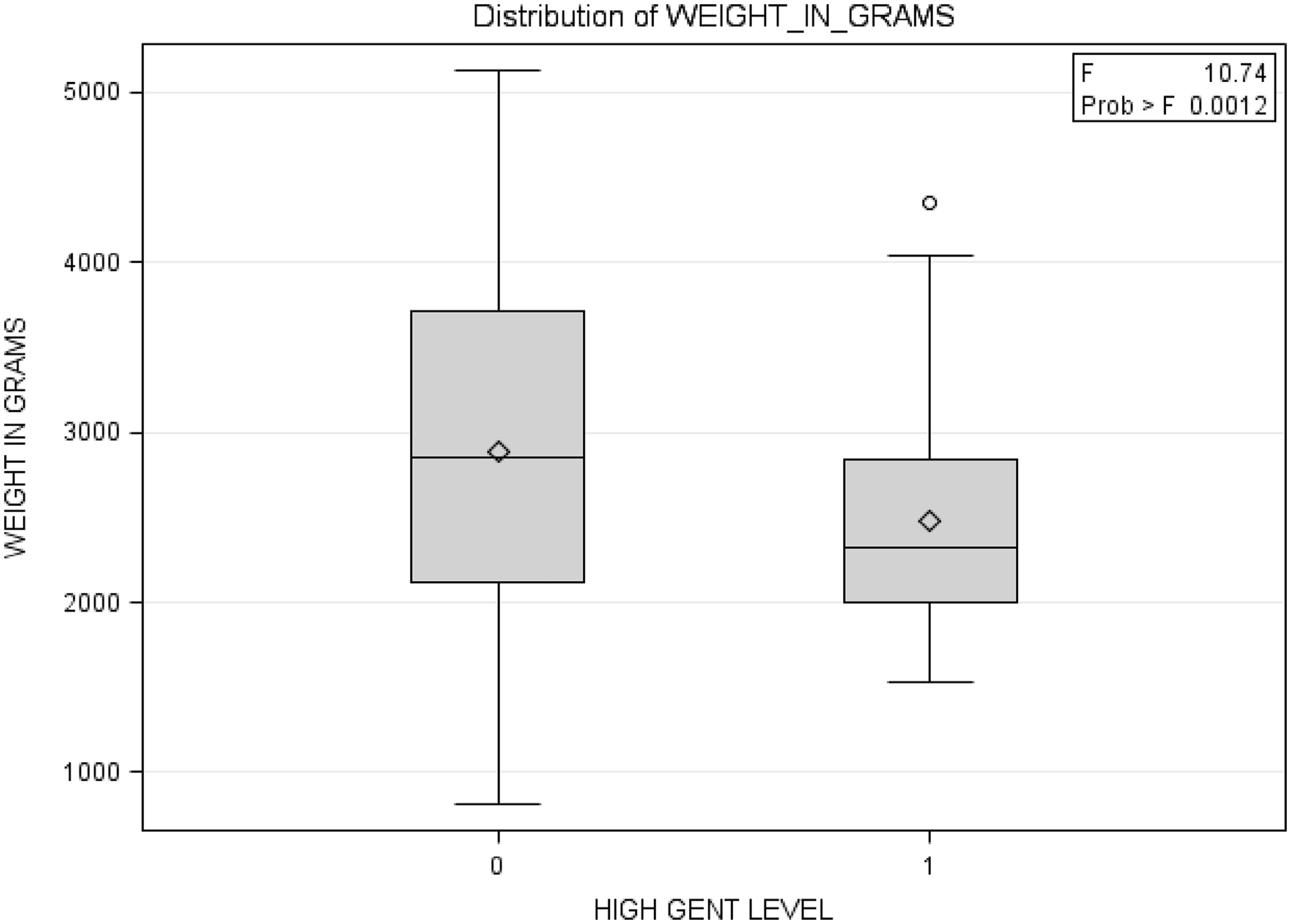
Discussion
This retrospective study in two hospitals in the United Kingdom suggests that preterm babies and babies of low birth weight tolerate gentamicin poorly and the dosage needs modification in them. This study gains more significance in the light of the current National Patient Safety Agency (NPSA) alert and national audit of gentamicin administration in term and preterm neonates.
Controversy exists about the optimal dose and interval of gentamicin administration for neonates. The Northern Neonatal Pharmacopeia (United Kingdom) recommends a dose of 5 mg/kg once in 24 h for neonates over 32 weeks, and the same dose once in 36 h in neonates <32 weeks.
3
British National Formulary (BNF) for children (2011) advocates the use of 4–5 mg/kg every 36 h in neonates <32 weeks and 4–5 mg/kg every 24 h in neonates ≥32 weeks in the extended interval dosing schedule.
4
Following multiple daily dosing for gentamicin, BNF recommends 2.5 mg/kg every 24 h in neonates <29 weeks, 2.5 mg/kg every 18 h in neonates 29–35 weeks and 2.5 mg/kg every 12 h in neonates >35 weeks. A Cochrane review on this topic in 2006
5
looked at 11 RCTs involving 574 patients and summarised the findings as follows: There is insufficient evidence from the currently available RCTs to conclude whether ‘once a day' or ‘multiple doses a day' regimen of gentamicin is superior in treating proven neonatal sepsis. However, data suggests that pharmacokinetic properties of ‘once a day' gentamicin regimen are superior to ‘multiple doses a day' regimen in that it achieves higher peak levels while avoiding toxic trough levels. There is no change in nephrotoxicity or auditory toxicity. Based on this assessment of pharmacokinetics, ‘once a day regimen' may be superior in treating neonatal sepsis in neonates greater than 32 weeks gestation.
There is uniform agreement that trough gentamicin levels need to be monitored to determine the possibility of toxicity, but the actual cut off values indicative of toxicity are a subject of debate. BNF (2011) observes that levels >1 mg/L are indicative of toxicity, while the general consensus from several other studies suggests that a level >2 mg/L correlates better with toxicity. Gentamicin is known to cause reversible dose-related nephrotoxicity, but its long-term effects on auditory and vestibular systems are reportedly irreversible. There are limited numbers of studies that have looked at the longer term impact of elevated gentamicin levels. Two studies6,7 that looked into ototoxicity over a longer timescale (four years) concluded there was no hearing loss that could be attributed to the use of aminoglycosides. One study emphasised the importance of long-term follow-up of hearing, as there is a high incidence of transient auditory abnormalities. Due to reported bacterial adaptations, it is widely believed that peak levels unfortunately do not correlate well with therapeutic efficacy and most units do not monitor this routinely.
A recently published pharmacokinetic study for once daily gentamicin supported extending the dosage interval in all neonates to 36–48 h. 8 Four mg/kg may be an alternative lower dose. The latest National Institute for Clinical Excellence (NICE) guideline 9 for antibiotic treatment of early onset neonatal infection suggests gentamicin dose of 5 mg/kg at 36 h intervals. Serious ototoxicity is normally only seen in babies who receive two aminoglycosides, a loop diuretic and aminoglycoside or 7 to 10 days of aminoglycoside. The NHS National Newborn Hearing Screening Program (NHSP) 10 recommends, ‘Immediate referral to Audiology by Paediatrician (whatever the levels) if child is suspected or known to have the A1555G mitochondrial mutation; otherwise and if high levels, referral to Audiology for behavioural assessment at eight months, or sooner if Paediatrician feels desirable.’
Limitations
The study is limited due to the relatively smaller number of patients, as well as due to absence of information on long-term outcomes in neonates from the elevated gentamicin levels. The significant drop out rates of children on follow up at eight months and the high number of cases where the levels were not documented also limits the validity of this study. The long-term effects of elevated gentamicin levels on hearing would need studying at a later stage and is not covered in this paper.
Conclusion
Gentamicin, used synergistically with Benzyl Penicillin, seems to be the best and safest option in treating neonates with suspected or proven sepsis. Gentamicin dose of 4 mg/kg once in 24 h in 32 weeks and beyond, or a dose of 5 mg/kg once in 36 h in neonates >32 weeks’ gestation seems to be associated with minimum risk of toxicity. More detailed studies on a larger section of preterm and low birth weight neonates with long-term follow up on their auditory and renal functions are needed to confirm reproducibility of these findings and their impact on safety profile of gentamicin.
Footnotes
Acknowledgements
We acknowledge the support of Duke-NUS/SingHealth Academic Medicine Research Institute, Taara Madhavan (Associate, Duke-NUS Graduate Medical School) in editing this article and Gita Krishnaswamy (Associate, Duke-NUS Graduate Medical School) for providing statistical support.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.