
Abstract
Background
Nutritional rickets is not uncommon in the western world and has been reported widely. Occasionally, children have presented to paediatrics with afebrile seizures secondary to hypocalcaemia due to hypovitaminosis D. However, association of nutritional rickets with electrocardiography changes and prolonged QT interval is not well documented. It is a rare, potentially serious and yet easy-to-treat complication as shown in our case. Our case also highlights the importance of awareness and education of both parents and clinicians regarding this relatively common but easily treatable condition.
Clinical case
We report a case of undiagnosed nutritional rickets presenting as ‘Afebrile’ seizure in a seven-month-old Somali girl. Her initial blood work-up showed low ionised calcium (0.8 mmol/l) on blood gas sampling, confirmed by laboratory result (adjusted 1.49 mmol/l). She had prolonged QTc on electrocardiography which reverted to normal with treatment. She was treated with intravenous as well as oral calcium after which she had no further seizures. We present a unique case of nutritional rickets-associated hypocalcaemia.
Conclusion
This case highlights the resurgence of nutritional rickets in western societies. We need to keep this disease in our list of diagnoses as it is a potentially serious and yet easily treatable disease. We should be more vigilant for screening ethnic minorities as alarmingly high rates of hypovitaminosis D have been found in ethnic minorities living in Great Britain.
What is known and what is new?
Nutritional rickets is a serious disease which is rarely encountered in modern day England. Rickets in relation to skeletal deformities was initially described by Glisson in 17th century England. The education about good sunlight exposure and the fortification of milk with vitamin D resulted in the decline of rickets by the mid-1900s. 1 Although multiple strategies for prevention are currently in place, it remains a global healthcare issue, even in western countries. Recently, there has been an increase in reports of rickets in dark-skinned, exclusively breastfed infants in the United States. 1
Our patient was a seven-month-old girl of Somali origin presented to us with afebrile seizures lasting for 2–3 min. She had two episodes at home followed by two further episodes while at the paediatric emergency department at a tertiary Children’s Hospital. She had a short history of coryzal symptoms and a preceding diarrhoeal illness; nevertheless, she had no fever.
She was born via spontaneous vaginal delivery with no complications. She was the first child of the Somali couple. Her medical history was unremarkable. She was exclusively breastfed and had up-to-date immunisation records. There were no concerns reported about her development. Her mother had not used any vitamins or calcium supplements to date.
Afebrile seizures are not the initial presenting feature of rickets but the disease was uncovered only after a careful history and physical examination along with haematological pointers. The diagnosis was later confirmed by quantitative laboratory testing.
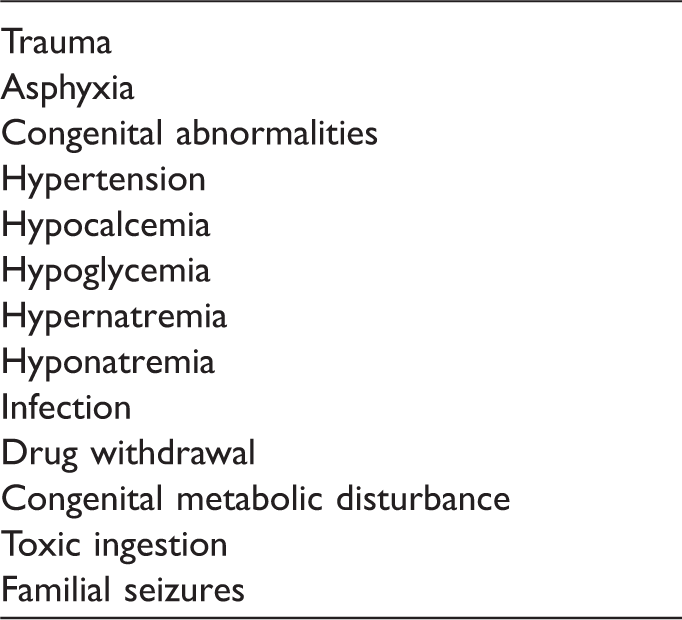
Afebrile seizure has a long differential diagnosis list (Table 1). Hence, as part of screening for ‘Afebrile’ convulsions in absence of trauma, she had full work up including blood investigations, electrocardiography (ECG) and blood gas analysis. Her ECG showed prolonged QTc interval at 490 ms (Figure 1). Her ionised calcium on blood gas sampling was 0.8 mmol/l with adjusted laboratory calcium of 1.49 mmol/l (2.2–2.7). Her alkaline phosphatase (ALP) was elevated at 719 IU/l (70–250 IU/l). Her parathyroid hormone (PTH) was high, measuring 28.1 pmol/l (1.6–6.9). The total 25-hydroxy (OH) vitamin D levels of the patient were <6 nmol/l (normal range >75 nmol/l) indicating ‘severe’ vitamin D deficiency. No consensus on optimal concentrations of serum 25-hydroxyvitamin D exists at present; rather a cut-off of 25–37 nmol/l is typically used to define vitamin D deficiency.
1
A 12-lead ECG showing prolonged QTc interval at 490 ms. Differential diagnosis of seizure in an infant.
2

An X-ray of her left wrist showed signs of rickets (Figure 2). She received calcium supplements following a stat dose of intravenous calcium gluconate bolus, and she had no further seizures. She was treated for vitamin D-deficient rickets with high-dose vitamin D and calcium supplements. Her serum calcium levels and QTc interval normalised (Figure 3) prior to discharge.
An X-ray film of the patient’s left wrist showing signs of rickets. A 12-lead ECG showing normalisation of QTc interval.

Discussion
Rickets has been known since the mid-17th century. It was previously thought to be a disease of the developing world but in one Canadian study the overall annual incidence rate was 2.9 cases per 100,000, while the mean age at diagnosis was 1.4 years. 3 The two-third victims had either intermediate or darker skin. 3
Vitamin D plays a pivotal role in calcium metabolism. Apart from oily fish, most naturally occurring food have little vitamin D. It can be obtained in the diet from fortified products and produced in sun-exposed skin. In Great Britain, dietary intake of vitamin D may be low, as vitamin D fortification is mandatory only for margarine, while in contrast in the United States and Canada, milk is also fortified. 4
The lack of vitamin D results in decreased serum calcium by impaired absorption from intestine. In nutritional hypocalcemic rickets, PTH is elevated, which compensates for hypocalcaemia by increasing calcium absorption from the kidneys and indirectly through the gut by activation of vitamin D. In kidneys, as calcium is coupled with phosphate, the increase in renal calcium absorption will lead to increased phosphate excretion. The elevation of PTH will also act to increase bone resorption, leading to elevations in ALP. Severe deficiency not only halts mineralisation of bone tissue but also impairs growth plates resulting in rickets. Other clinical manifestations during childhood include hypocalcaemia seizures, fractures, lower-limb deformities, abnormal dentition and delayed developmental milestones. 3
The enlargement of the costochondral junctions, also known as rachitic rosary, may be physically evident during examination or seen on chest X-ray. The enlargement of the wrists, lateral bowing of the tibia and femur, and parietal and frontal bossing of the skull can also be seen. 2
It should be part of a paediatrician’s role to educate patients and their families about rickets and the associated health risks. If the infant is exclusively breastfed, families should be encouraged to add vitamin supplementation as per current recommendations from the Department of Health, UK, as limited exposure to sunlight due to cloudy British weather as well as dark skin colour can impair the synthesis of vitamin D. This is of extra significance when dealing with ethnic minorities living in Great Britain due to high rates of hypovitaminosis D. 4 Vitamin D supplementation should be a common practice to advocate, as its absence can cause a potentially serious yet easily treatable disease.
The presented case is a unique case of first presentation of nutritional rickets with serious complications. Despite many preventive strategies, the incidence of nutritional rickets in western world is on the rise. Although it is well reported but can be easily missed until complications occur. Our report highlights the potentially life-threatening complication which is easily treatable as well as preventable.
Footnotes
Author contributions
All authors have contributed equally to this manuscript.
Consent
Family consent was obtained for publication.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.