
Abstract
Chronic sun-induced dysplastic skin changes (actinic keratoses) are extremely common in fair-skinned people in Scotland. These changes are a major cause of morbidity and may develop into skin cancer. Actinic keratoses are often extensive and pose a therapeutic challenge as field-directed treatment is required for chronic disease management. One such treatment approach is hospital-based photodynamic therapy, which is a well-established treatment in Scotland for actinic keratoses, using a photosensitiser pro-drug and red LED light irradiation. However, photodynamic therapy using daylight as the activating light source is increasingly and effectively used in continental Europe, but had not been explored in Scotland until we initiated this in 2013. We report our experience of daylight photodynamic therapy in 64 patient-treatment courses and demonstrate that this can be an effective, well-tolerated treatment, which is liked by patients. Our most recent data show that most patients (73%) achieved clearance or at least a good response to treatment and had high levels of satisfaction with daylight photodynamic therapy. Daylight exposure measurements indicated that treatment is feasible in Scotland between April to September. Daylight photodynamic therapy is an important advancement in treatment options for Scottish patients with extensive pre-cancerous field changes and provides opportunities for home-based treatment and increased efficiency of photodynamic therapy services.
Introduction
Chronic sun exposure is the main environmental risk factor for non-melanoma skin cancer and pre-malignant dysplastic skin changes, defined as actinic keratoses (AK). These skin changes are extremely common in fair-skinned populations, such as in Scotland, and are a major cause of morbidity and concern with regard to risk of development into invasive skin cancer. Chronic disease management is required given the recurrent nature of AK and treatment needs to be field-directed as there is usually extensive background dysplasia. Hospital-based topical photodynamic therapy (PDT) is one such field-directed treatment, which is well established for superficial non-melanoma skin cancer and pre-cancerous changes of Bowen’s disease and AK.1–3 PDT is particularly advantageous for field change carcinogenesis as larger areas, which include sub-clinical disease, can easily be treated. Conventional PDT involves application of a photosensitiser pro-drug (methyl aminolevulinate or 5-aminolaevulinic acid) and, 3 h later after accumulation of the photosensitiser (protoporphyrin IX (PpIX)) in abnormal cells, red light irradiation with an LED source in a hospital outpatient setting. During irradiation, pain and discomfort are usually experienced with reports of up to 20% of patients finding treatment to be significantly painful, which can limit treatment delivery.4,5 Hospital-based PDT requires the patients to attend hospital for half a day and only limited areas can be treated in one session.
The use of the visible wavelengths of daylight for activation of the photosensitiser, as an alternative to LEDs, was initiated in Copenhagen. With daylight PDT, there is no need to wait for 3 h before light exposure as after initial application and absorption of cream containing pro-drug, daylight exposure over 2 to 2.5 h will constantly activate the low-level build-up of photosensitiser on a continuous basis, rather than the sudden activation of larger amounts of photosensitiser that have built up prior to light activation in the hospital setting after a 3-h incubation period. This also is the likely mechanism for why the pain of daylight PDT is much lower than that of hospital PDT. Indeed, several well-designed studies have been undertaken and have shown that topical daylight PDT is at least as effective and better tolerated, with significantly lower pain scores, than conventional hospital-based PDT for AK.6–8 The use of this more convenient form of PDT has extended in continental Europe and Australia, and there is now a large evidence-base to support the efficacy and tolerability of daylight PDT for AK.8–10
A survey in 2011 highlighted that hospital-based PDT was performed in 10 dermatology centres in Scotland and a common indication for PDT was AK.11 However, the extensive and recurrent nature of AK, requiring frequent attendances for treatment, is limiting for hospital-based services. At the time of this survey, daylight PDT had not been introduced in Scotland.
We wanted to investigate whether daylight PDT could in fact be a feasible, effective and well-tolerated treatment for patients with AK in Scotland, despite the possible challenges of the weather. We report our findings after three years of using daylight PDT.
Methods
We offered daylight PDT to patients with multiple areas of AK and field change carcinogenesis who had been referred to the PDT clinic at the Photobiology Unit in Dundee for consideration of PDT between April 2013 and September 2015. Patients generally had failed or were intolerant of other therapies, such as topical 5-fluorouracil, imiquimod or hospital-based PDT, or had recurrent disease before being considered for daylight PDT. Patients had extensive mild to moderately thick AK and involvement of face, scalp, chest and limbs. Daylight PDT was undertaken each year between 1st April and 30th September.
Treatment was undertaken by a PDT technician or nurse, with clinician oversight and assessment of response. An absorbent SPF sunscreen (Actinica®, Galderma UK) was applied to all sites that would be exposed to daylight. This was done in order to prevent ultraviolet radiation-induced sunburn but not reduce visible light transmission, which was required for therapeutic activation of PpIX. Superficial surface preparation of areas of hyperkeratosis was undertaken 10–15 min after sunscreen application, using a disposable ring curette (Stiefel®), without the need for local anaesthetic, and the photosensitising pro-drug was then applied to the area to be treated. All patients were treated with methyl aminolevulinate cream (Metvix®, 16%, Galderma, UK). Six of the eleven patients treated in 2013 also had areas treated with 5-aminolaevulinic acid (Ameluz®, 8%, Biofrontera, Spirit Healthcare) on subsequent visits but as no apparent difference was noted, these data were included in overall analysis. Patients were then advised to expose the treatment sites to 2 h of unshaded continuous daylight, starting within 30 min of the cream being applied. Patients were able to undergo treatment on all days, including cloudy days, with the exception of heavy rain in which case they could either sit in a conservatory or indoors adjacent to a large window for the same time period. If they were outdoors and treatment had to be abandoned because of rain, they were asked to record how long they had been outdoors before this happened. Weather conditions and temperature were recorded on a daily basis in the Photobiology Unit. The BBC 5-day weather forecast was scrutinised in order to plan ahead with respect to the likelihood of treatments being able to be undertaken on specific days of a given week, with short notice rescheduling of treatment if necessary or use of conventional hospital-based PDT as an alternative back-up plan in the event of rain.
During the first year of treatment (2013), telephone follow-up was obtained the following day and the patients were seen at weeks one and four. However, as treatment was so well tolerated, this was not considered necessary in 2014 and 2015. In the latter, two-year patient review took place at 4–12 weeks, being arranged dependent on the severity of AK at presentation and likelihood of need for repeat treatment based on clinical assessment, according to complete, partial or no response. The maximal pain experienced during PDT was assessed by a numerical rating scale of 0 to 10 and patients were also asked to describe treatment site reactions, with erythema (redness) being either mild, moderate or severe and, if able, were asked to take photographs. If residual AK remained at the review appointment (4–12 weeks), a further treatment was undertaken over the spring and summer months, with application of sunscreen and pro-drug cream at the hospital as for the first treatment, with the patient then returning home or spending time in the hospital grounds in order to expose themselves outdoors. At the end of treatment, patients completed a questionnaire in which they were asked to evaluate treatment and how it compared with other treatments that they may have had previously for this condition.
In 2013, daylight illuminance was recorded by staff at the Photobiology Unit, with a luxmeter prior to each treatment. The illuminance was converted to PpIX-weighted spectral irradiance (mWcm−2), which could be integrated over the time of exposure resulting in a PpIX-weighted light dose (Jcm−2). In an effort to improve the accuracy of our daylight dosimetry, we purchased portable data logging light meters (HOBO® Pendant Temperature/Light Data Logger, Onset Computer Corporation, 2009) before commencing daylight PDT in 2014. This offered a more robust approach to recording daylight doses received by patients during their PDT treatments as the devices recorded light levels every 15 s over the total exposure time, while placed next to the patient (2014) or pinned to their clothing (2015).
Results
Sixty-four patient-treatment courses took place between 2013 and 2015 (in 35 males and 13 females; median age 72 (range 52–89) years). Five patients were treated in both 2013 and 2014 and 10 treated in both 2014 and 2015, although only one patient received treatment in each of the three years. The median number of field areas treated on individual patients was 3 (range 1–17), each of up to 20 cm diameter, indicating extensive field change. The median number of treatments received was 3 (range 1–5). At final review at the end of the summer months, all patients showed clearance or clinically important improvement of AK and field change carcinogenesis as reflected by reduction in the number and extent of lesions (Figure 1; Table 1). In those patients treated each year, we noted that sub-clinical dysplastic foci were picked out by treatment and became inflamed and more obvious in the days following treatment (Figure 2). Only two patients (who lived 51 and 142 miles away from the hospital) remained in the hospital grounds for daylight exposure. All other patients returned home for treatment outdoors. Nine patients had at least one of their treatments in a conservatory. The median distance that these patients lived from the hospital was 15.8 (range 1.3–52.8) miles.
Actinic keratoses on the scalp (a) before and (b) after daylight PDT. Note clearance of AK. Lentigines and telangiectasiae, which are benign and not dysplastic, remain as expected and do not require any treatment. Erythema and crusting at sites of actinic keratoses on the scalp 24 h after a single daylight PDT treatment. Note: sub-clinical disease becomes more apparent as field changes are treated by daylight PDT.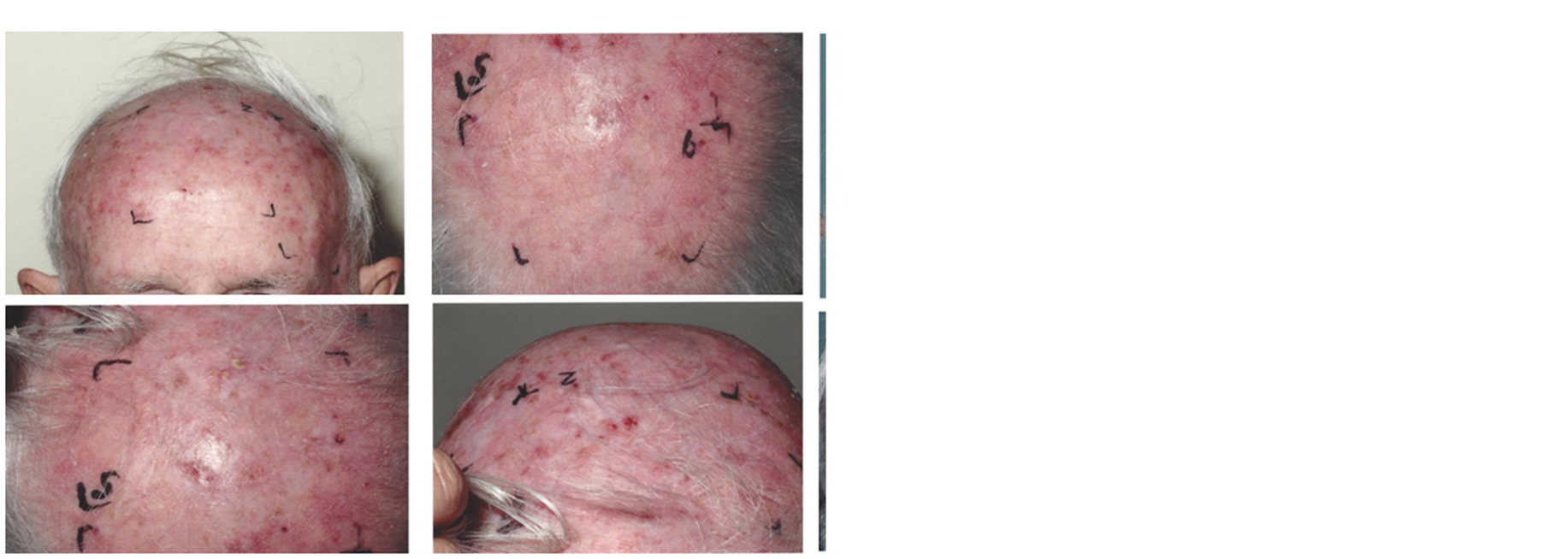

Daylight exposure doses and conditions.
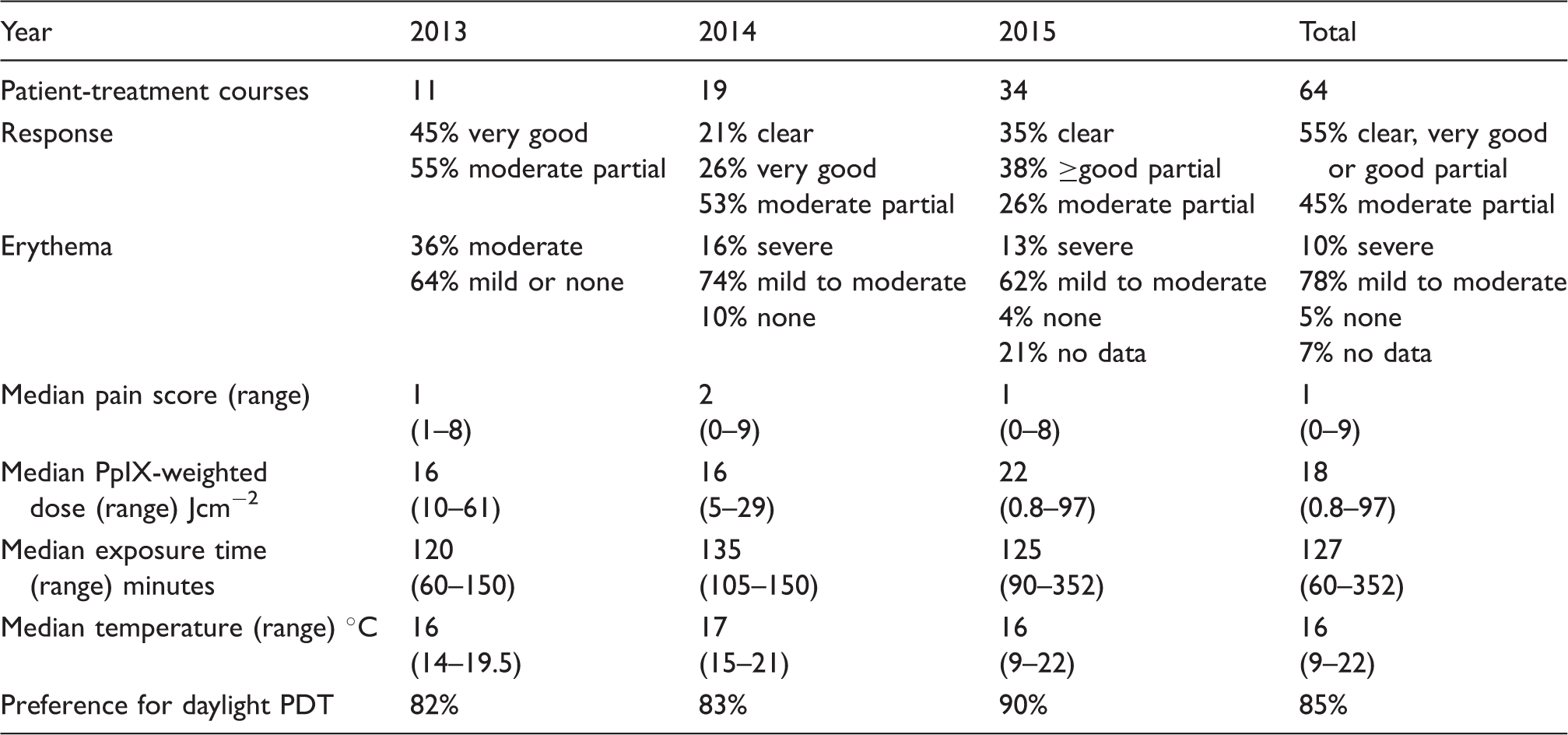
PDT: photodynamic therapy; PpIX: protoporphyrin IX.
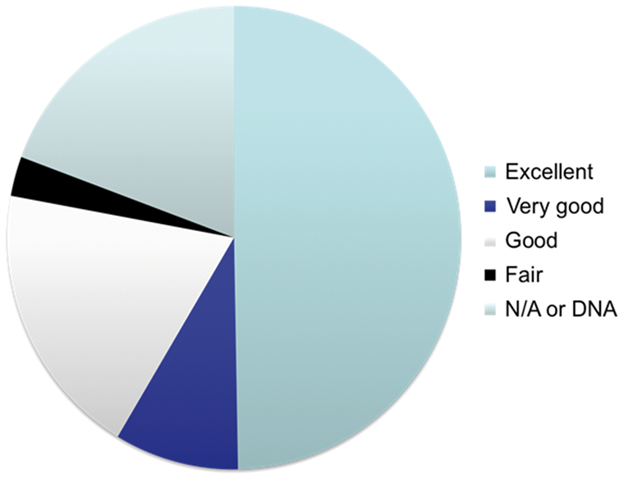
Semi-quantitative assessment of patient satisfaction with daylight PDT in 2015 (n = 34).
Discussion
We report on the first experience of daylight PDT in Scotland and demonstrate that this is a feasible and effective treatment strategy, with our most recent data (2015) indicating that 73% of patients achieve either disease clearance or at least a good therapeutic response. Treatment was very well tolerated, with minimal adverse effects (median pain score of 1 compared with a median score of 6 for a historic cohort treated with conventional hospital-based PDT12). Patients expressed high levels of satisfaction with treatment, with the majority having a preference for further daylight PDT compared with conventional PDT or other treatments.
Patients with AK and field change carcinogenesis are difficult to treat effectively and efficiently within a PDT clinic set up due to the limitations of field size and treatment numbers required. Thus, daylight PDT, which allows larger areas to be conveniently and comfortably treated in single home-based sessions, is beneficial for chronic disease management in patients with extensive AK and whilst this will not suit all patients, we anticipate that this could facilitate streamlining of dermatology PDT services in Scotland and beyond.
We had initial concerns about the introduction of a service that relied on Scottish weather for effective delivery. However, we closely monitored exposure doses during the treatment periods between April and September. Our median PpIX-weighted dose of 18 Jcm−2 was much higher than the minimum dose of 8 Jcm−2, considered to be required for effective treatment. Published dose data have varied considerably, not only between different centres but even from a single centre. Our median PpIX-weighted dose (18 Jcm−2) was approximately half of the dose recorded in the first published daylight PDT publication from Denmark (43.2 Jcm−2) but was double that of the follow up publication in 2012 (9.6 Jcm−2).6,7 In this and other published daylight PDT studies, there is a large variation in exposure doses. Exposure time will play a role as it is directly proportional to dose, and weather conditions will also be key. However, in our study, at least part of this variation may represent the move from monitoring a small number of patients who were very tightly controlled in 2013 to a larger patient population with more freedom to control their own treatment by 2015. The variation in measured dose may also be explained by the move towards patient-specific dosimetry over the period described. By 2015, data-logging light meters were being attached to the patients’ clothing during their exposure. This enabled an accurate record of the specific light levels patients were being exposed to as they went about their daily activities during treatment. Prior to 2015, the measurement of light was not with the patient during their exposure but was close to them or made at a single point prior to treatment. While these techniques were reliable indicators of patient dose, we believe our current technique provides the most accurate patient exposure data. However, caution should be exercised when using light meters as not all will give a true illuminance value, and calibration against the treatment light source (i.e., the sun) is required.
Our data indicate that even at low-exposure doses, most patients receive adequate daylight to result in effective treatment. This provides us with reassurance that for others centres in Scotland and beyond who are setting up a daylight PDT service, measurement of exposure doses is not required. As long as it is not raining (where the practicalities of cream running off into eyes may be limiting), effective daylight PDT can be achieved by the patient having 2 h of daylight exposure from April until the end of September as long as it is warm enough (>10℃) to stay outdoors, or alternatively spend time in a conservatory. There is a requirement for patients and, if required, their carers/partners to be engaged in the treatment process itself, which will of course not suit all. However, whilst some patients may not be able or wish to comply with the requirements of treatment, as conservatory-based treatment is an option, this may also allow frail, elderly patients who are relatively housebound to receive daylight PDT. We intend to continue to look at ways to increase the convenience and ease of home-based daylight PDT. Indeed, one option is for patients to self-apply sunscreen and photosensitiser pro-drug cream at home before outdoor exposure. This will require patients to be fully aware of what is involved and able to undertake the necessary steps in the procedure. However, this will be of added benefit for many patients.
Thus, in summary, we report on the first experience of daylight PDT in Scotland and show that this is a feasible, convenient, effective and well-tolerated treatment for patients with chronic AK and pre-cancerous skin changes. Daylight PDT provides opportunities for patients to become more involved in their own treatment and to be treated in their home environment, without the need for specialised equipment. We consider that daylight PDT could be effectively used in many dermatology settings in Scotland and has the potential to streamline the efficiency of management of patients with this extremely common pre-cancerous condition.
Footnotes
Acknowledgements
We would like to thank Lynn Fullerton, Susan Yule and the photobiology technicians for their invaluable help in undertaking the daylight PDT treatments and in data assimilation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SI has received honoraria and travel expenses from Galderma and Spirit Healthcare and has been an investigator on studies funded by Galderma and Biofrontera.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to acknowledge the support of the Alf Stewart Scottish PDT Centre, which facilitates all of our PDT clinical and research activities.