
Abstract
Adult-onset Still’s disease is a systemic autoinflammatory disease the presentation of which can often mimic infection. As a consequence, there is often a delay in diagnosis. Serositis is a recognised but less common clinical feature that can result in complications including cardiac tamponade and constrictive pericarditis. We describe a case of adult-onset Still’s disease without the hallmark rash or significant arthritis, presenting with polyserositis that showed a good response to initial steroid treatment and sustained remission with anakinra. An elevated procalcitonin level was due to active adult-onset Still’s disease, not bacterial infection.
Introduction
Adult-onset Still’s disease (AOSD) is a systemic autoinflammatory disease characterised by daily (quotidian) fever, typical rash and arthritis. Pharyngitis, hepatomegaly, splenomegaly and lymphadenopathy are all recognised features of the condition 1 as are pericarditis and pericardial effusions which can occur in up to 40% of cases. There is typically a striking neutrophilic leukocytosis, hyperferritinaemia and elevated inflammatory markers. We describe a presentation of AOSD in a postmenopausal woman with evidence of serositis in the absence of its hallmark rash.
Case report
A 56-year-old postmenopausal woman presented to a large district general hospital with fever, tachycardia, hypotension and dyspnoea. She had an 18-month history of ‘pyrexia of unknown origin’, with a 2-month history of worsening fevers with night sweats, myalgias, arthralgias, together with 13-kg weight loss.
Repeated investigations had revealed raised inflammatory markers, a normocytic anaemia, neutrophilia and an initial normal ferritin level (164 mg/dL) with normal iron and iron binding capacity. Immunoglobulins, antinuclear antibodies (ANA) and rheumatoid factor (RF) were normal. Serial blood cultures were negative as was serology for Hepatitis B, Hepatitis C and human immunodeficiency virus. Transthoracic echocardiogram and chest radiographs had been normal. Multiple empirical courses of antibiotics for possible occult infection had been ineffective.
On admission to hospital, investigations showed white cell count 18.7 (neutrophils 17.0), C Reactive Protein (CRP) 195 mg/L, Erythrocyte sedimentation rate (ESR) 116 mm/h, Haemoglobin (Hb) 93 g/L, alkaline phosphatase 125 IU/L, Alanine aminotransferase (ALT) 16 IU/L, albumin 30 g/L, D-Dimer 2485 ng/mL, International Normalized Ratio (INR) 1.43 and a steep rise in ferritin at 6624 µg/L. The timing of her fever did not show any particular pattern, and a salmon-pink rash, although looked for by inspection of her trunk, neck and extremities, was not observed. Further, multiple cultures of blood and urine were negative.
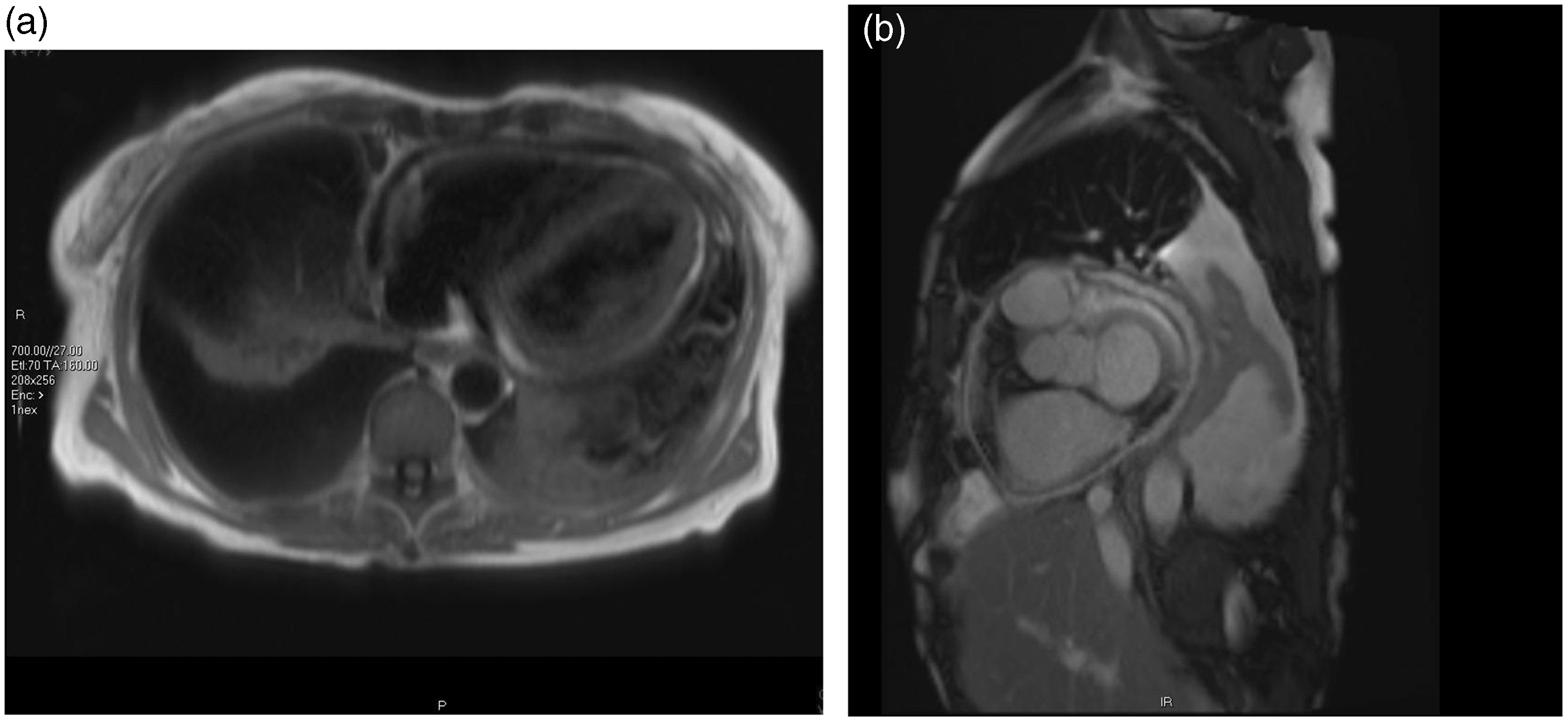
Chest X-ray showed a small right-sided pleural effusion that progressed bilaterally over a few days (Figure 1). Pleural fluid analysis showed glucose 5.5 mmol/L, LDH 2905 IU/L, total protein 39 g/L and adenosine deaminase 31 IU/L. A transthoracic echocardiogram and a heart CT scan demonstrated a small pericardial effusion and a global reduction of left ventricular function (ejection fraction = 53%) (Figure 2).
Chest X-ray showing moderate left-sided pleural effusion and a small right-sided effusion. (a, b) MRI myocardial viability scan showing pericardial effusion measuring up to 1 cm in depth lateral to the left ventricular free wall. Thickening of both visceral and parietal pericardium is seen.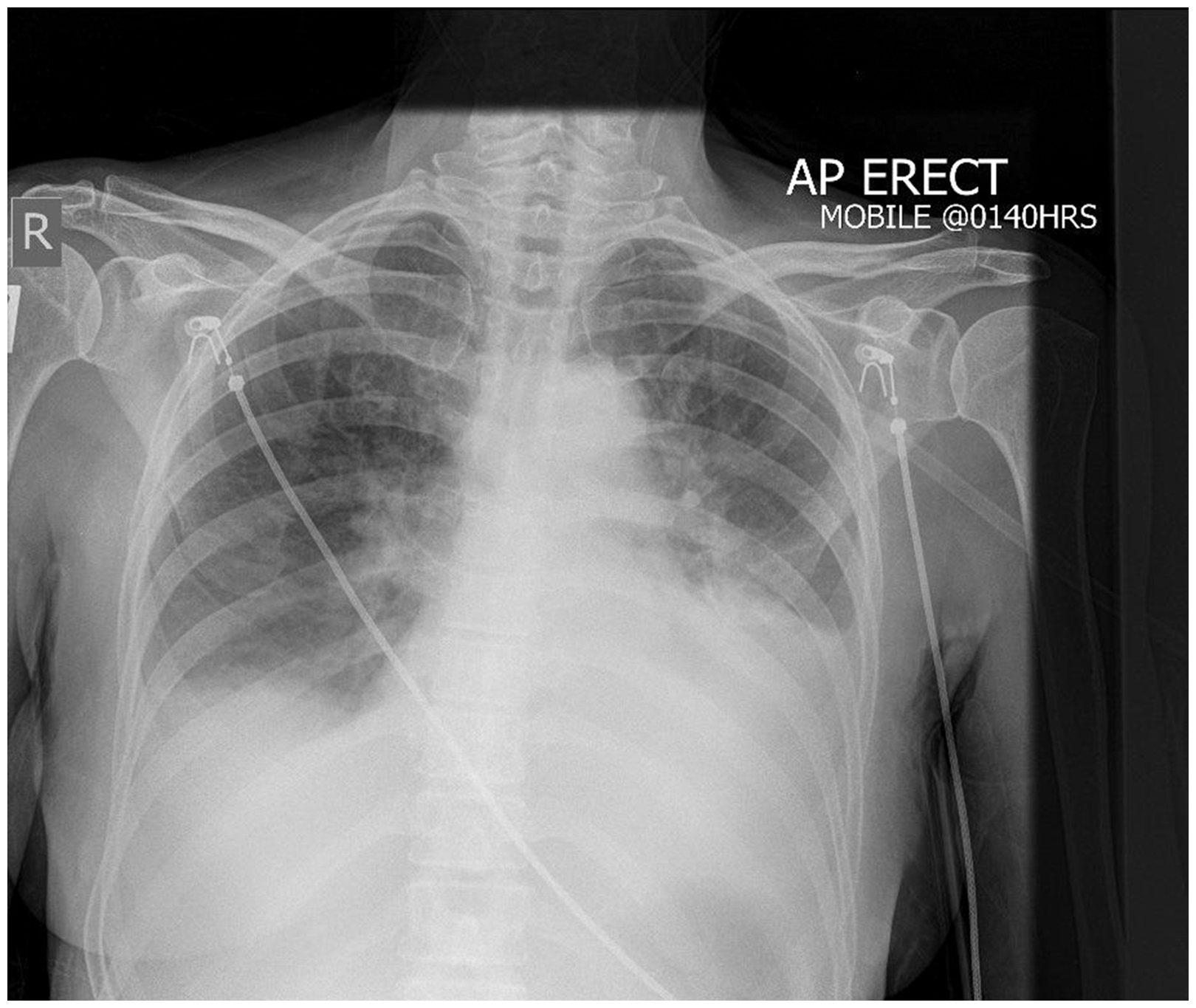
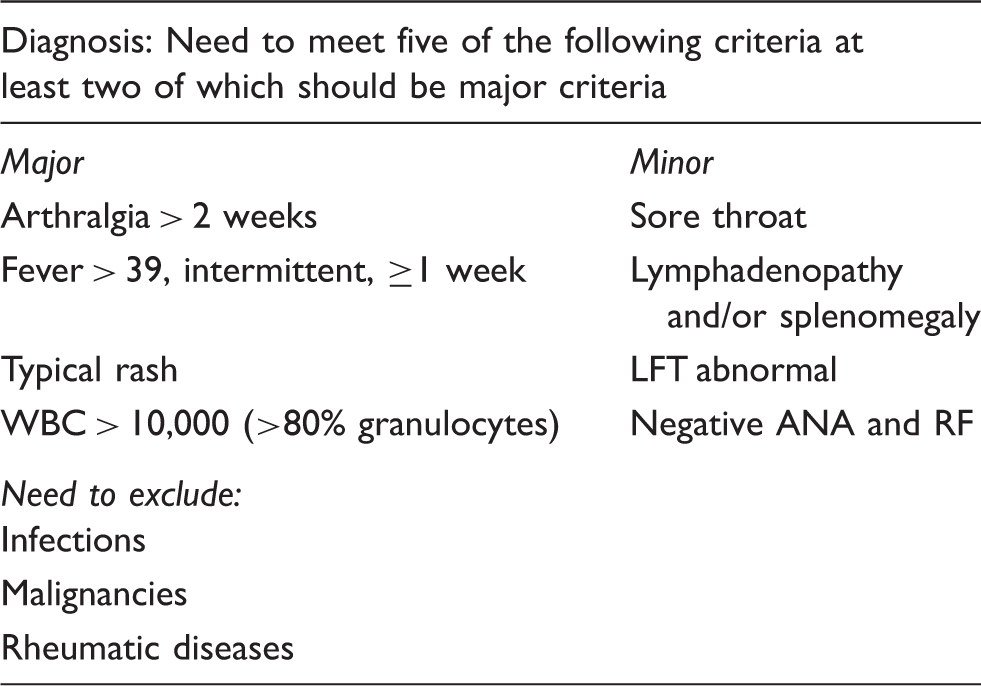
Yamaguchi et al. criteria for AOSD. 6
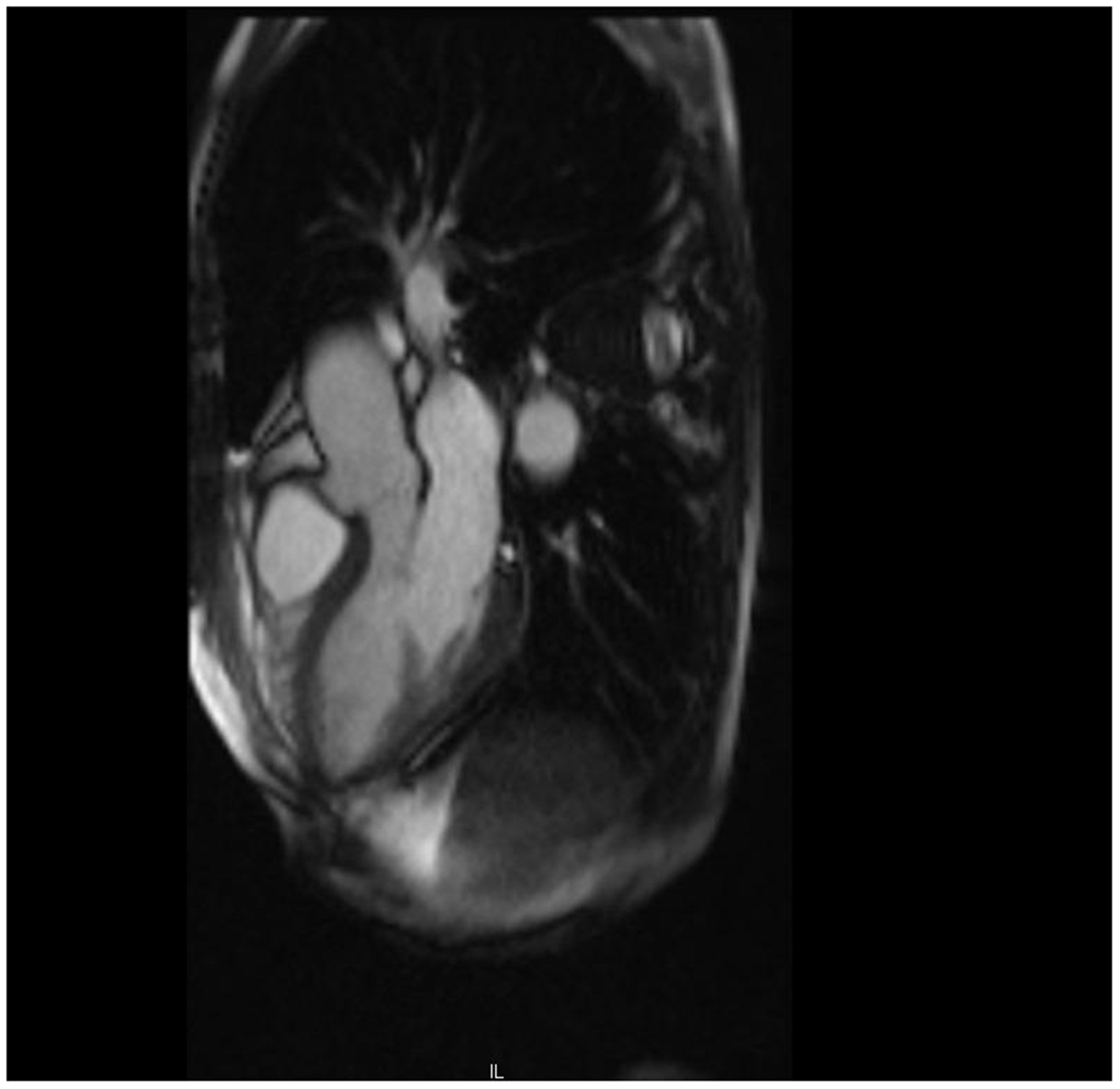
Interval MRI myocardial viability scan (at one month) showing resolution of pericardial effusion with normal looking pericardium.
Discussion
The inflammatory mechanisms involved in AOSD can smoulder over months or years before the diagnosis becomes clear. The disease affects all age groups, but 75% of patients have onset at a younger age (16–35 years). 2
Characteristically, an elevated white cell count with predominant neutrophilia, raised ESR and CRP, anaemia and increased liver enzymes have been described. Serum ferritin above 4000 ng/mL is often seen 3 and since 2002 has been recognised as a major diagnostic criterion. 4 The other diagnostic parameters can be non-specific, with up to 49% patients not having the typical evanescent flat salmon-pink rash, 5 as in our patient. AOSD remains a diagnosis of exclusion, 6 and often follows a relapsing–remitting course, 7 therefore making diagnosis difficult. Our case illustrates that an increase in procalcitonin can be seen in AOSD and is not solely a marker for bacterial infection, as has previously been reported. 8
Interleukin-1 (IL-1) has been shown to provide a stimulus for procalcitonin which in turn acts as a mediator of cytokines. The half-life of procalcitonin is 24 h 8 and hence a lack of response to antibiotics for presumed bacterial infections should warrant consideration of an inflammatory process such as AOSD.
Hb, Plts, ESR, CRP and ferritin before initial IV methylprednisolone infusion, 1 week post infusions on oral prednisolone 40 mg.
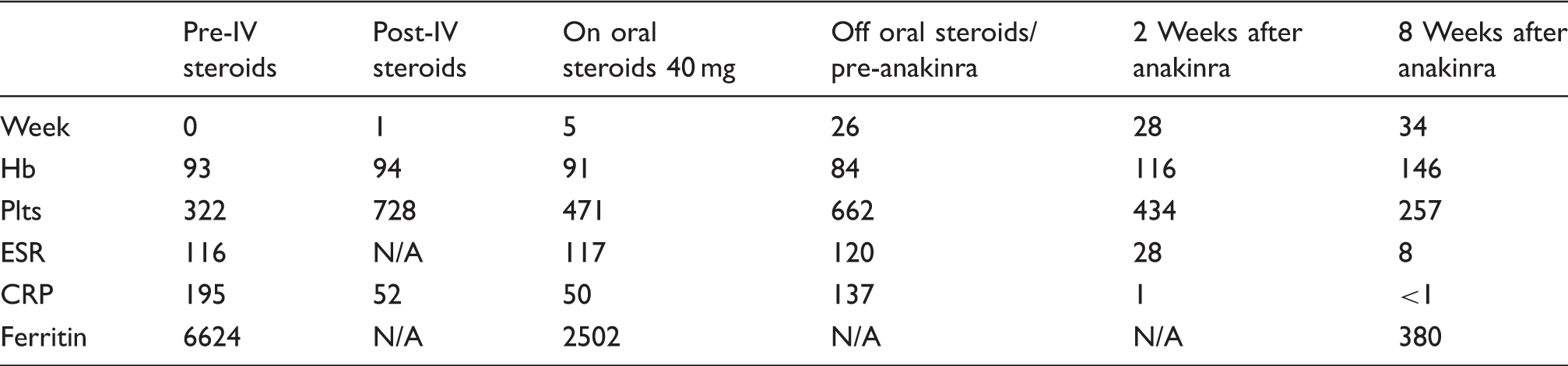
N/A: not available.
Prednisolone was tailed off by week 10 because of steroid mania.
Hb (g/L – normal range 120–150).
Platelets (Plts) (109 – normal range 150–410).
ESR (mm/h – normal range 1–19).
CRP (mg/L – normal range<9).
Ferritin (µg/L – normal range 15–400).
Steroids are often the initial treatment of choice, having a response rate of 76–95% with many patients requiring maintenance doses of prednisone. 5 AOSD refractory to oral prednisone has been shown to respond well to intravenous pulse therapy with methylprednisolone. 9 Intravenous immunoglobulins, tumour necrosis factor-alpha antagonists, methotrexate, and therapies targeting interleukins (IL-1 and IL-6) have also been used for resistant cases.10–12 In our case, the need to stop steroid treatment meant other treatment options had to be considered. The good response to anakinra, after prior withdrawal of steroids, supports the role for IL-1 in aetio-pathogenesis of the disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.