
Abstract
Introduction
Heterotopic ossification is the formation of lamellar bone in periarticular soft tissue that can be seen in paralysed patients or following trauma. It can cause significant burden to already debilitated patients.
Case presentation
A 12-year-old boy with paraplegia due to neuromyelitis optica presented with progressive right knee pain and swelling. There was no history of trauma to the knee. Anteroposterior radiograph of femur at the initial presentation showed a supracondylar femur fracture for which casting was performed. Six weeks later, when casting was removed, swelling along with increased rubor in distal thigh region was noted. Radiography of the right femur revealed an unhealed distal femur fracture along with massive ossification extending from lesser trochanter to fracture line along the soft tissue around the femoral shaft.
Conclusion
This case presented the clinical and imaging findings of a giant heterotopic ossification in the thigh region following an extra-articular fracture.
Introduction
Heterotopic ossification is new bone formation in the soft tissues around periarticular regions. 1 Heterotopic ossification can be seen following trauma-related fractures, blast injuries, burns or following central nervous system injury including traumatic brain injury and spinal cord injury. It is most commonly seen in paralysed patients with reported incidence rates of 20–35% after spinal cord injury. 2 Heterotopic ossification can be a cause of significant burden to already debilitated patients by causing persistent pain, decubitus ulcers, decreased range of motion (ROM) at affected joints and compression neuropathy.3,4 The diagnosis depends on clinical and laboratory evaluation, along with radiographic imaging; however, diagnosis can be difficult as symptoms may precede radiographic findings of soft-tissue bone formation. 3 Herein, we present the case of a severe heterotopic ossification with extensive involvement of the thigh region. This case is notable for the extent of heterotopic ossification.
Case presentation
A 12-year-old male patient with paraplegia due to neuromyelitis optica presented with progressive right knee pain and swelling. No trauma history prior to knee pain was elicited. Anteroposterior radiograph of distal femur and knee joint at the initial presentation revealed a supracondylar femur fracture accompanied by soft-tissue swelling for which casting was performed (Figure 1(a)). Six weeks later, when casting was removed, progression of swelling along with increased rubor in distal thigh region was noted. On physical examination, there was a 13 cm difference between thigh circumferences (Figure 1(b)). Radiography of the right femur revealed an unhealed distal femur fracture along with massive ossification extending from lesser trochanter to fracture line along the soft tissue around the femoral shaft (Figure 1(c)). Laboratory tests revealed a C-reactive protein level of 0.31 mg/dL (normal < 0.5 mg/dL), an erythrocyte sedimentation rate of 14 mm/h (normal range 2–20 mm/h), 25-OH vitamin D level of 29.2 ng/mL and parathyroid hormone level of 24.6 (normal range: 15.0–68.3 pg/mL).
A 12-year-old male patient with paraplegia presented with progressive right knee pain and swelling. (a) Anteroposterior radiograph of right thigh and knee shows a supracondylar femur fracture extending into epiphysis. (b) Six weeks later, progression of swelling was noted with 13 cm difference between thigh circumferences. (c) Lateral radiography of right thigh revealed massive heterotopic ossification extending from lesser trochanter to distal femur metaphysis.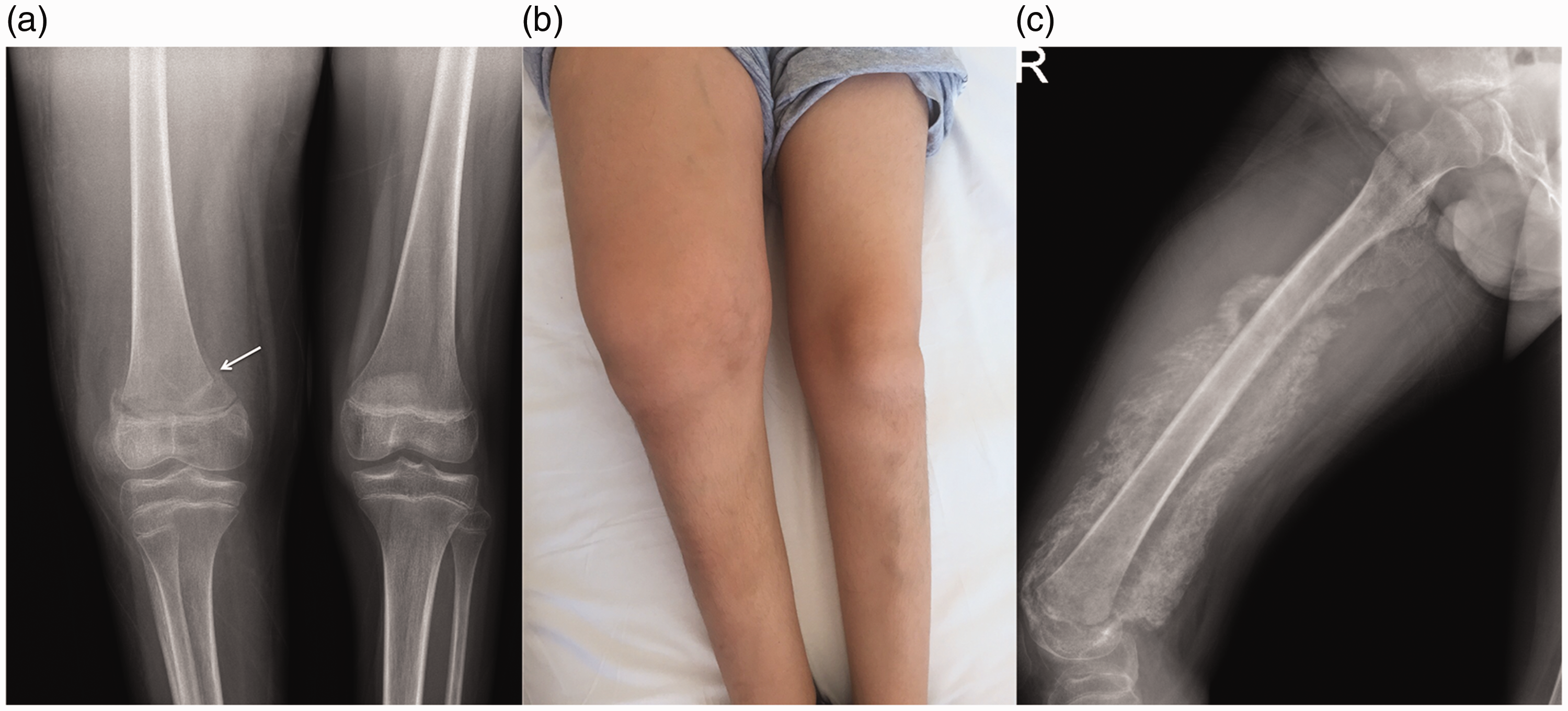
Subsequently, magnetic resonance imaging (MRI) of the right thigh revealed extensive regions corresponding to immature bone formation in the soft tissues along femur diaphysis and a collection between bone cortex and inner margin of heterotopic ossification (Figure 2(a) to (c)). Clinical and imaging findings were consistent with a diagnosis of heterotopic ossification. The patient started receiving ibuprofen and passive ROM exercises for right knee. Follow-up at two years revealed limited ROM in knee joint with 10 degree of contracture in knee flexion and 20 degree contracture in passive knee extension (Figure 3).
(a) Sagittal nonenhanced T2-weighted fast spin-echo short inversion time inversion-recovery (STIR) MRI shows diffuse hyperintense area (arrow) in the soft tissues along femur diaphysis, corresponding to immature bone formation and hyperintense collection (thick arrow) in the inner margin of heterotopic ossification. (b) Coronal nonenhanced fat-suppressed T1-weighted MR image of the right thigh shows a large mass isointense to muscle in the region of the immature heterotopic ossification (arrow). Also slightly hyperintense areas (thick arrow) corresponding to collections on STIR images are noted. (c) Coronal T1-weighted contrast-enhanced MR image of the right thigh shows enhancement of immature heterotopic bone (arrow) and rim enhancement (thick arrow) around the collection. Follow-up radiography at two years: persistence of heterotopic ossification.

Discussion
Heterotopic ossification is most commonly seen in paralysed patients, occurring below the level of neurologic impairment with usual involvement of the para-articular region. The hip joint is the most common affected region. 2 Complications of heterotopic ossification can be a cause of significant morbidity with subsequent loss of the patient's independence. These include decubitus ulcers, restricted joint motion and ankylosis of joints. 2 Diagnosis can be challenging, as symptoms often precede radiologic evidence of ectopic bone formation. The differential diagnosis of a soft-tissue swelling in a paralysed patient includes deep venous thrombosis, cellulitis, abscess, haematoma and osteomyelitis.
There are different phases of heterotopic ossification with a progression from amorphous calcification to immature and mature ossification. 5 Plain X-rays and computed tomography (CT) are the standard imaging modalities to demonstrate calcification in soft-tissue planes with CT more accurately defining the different stages of ossification than do plain X-rays. 5 MR imaging is a commonly performed study in paralysed patients to evaluate soft-tissue infections related to decubitus ulcers. Thus, MRI may be the initial imaging study performed and findings on MRI are important for a differential diagnosis. However, MR findings depend on the level of heterotopic ossification maturity and can be a source of confusion, especially at the amorphous calcification and immature ossification stages. 5 On T1-weighted images, immature ossification areas have low to similar signal intensity relative to muscle on T1-weighted images and high signal intensity on T2-weighted images. With progressive maturation of heterotopic ossification, there is a steady decrease in hyperintensity on T2-weighted images and increased signal intensity on T1-weighted image similar to bone-equivalent signal intensity. 2
Management options vary depending on the stage of ossification. In orthopaedic trauma patients, two commonly used options in heterotopic ossification prophylaxis include non-steroidal anti-inflammatory drugs (NSAIDs) and single-dose radiation therapy. 1 The early (two to six weeks) period is the inflammatory phase where NSAIDs intervene by inhibiting inflammatory prostaglandins that are important pathways in heterotopic bone induction. 1 The role of physiotherapy in patient management is a controversial topic. 6 Proponents of physiotherapy state that passive ROM exercise is helpful in preserving joint ROM and in preventing ankylosis. 7 Other studies indicated aggressive passive ROM exercise may cause spasticity and ankylosis by microtrauma and local haemorrhage. 8
Other medical therapy options include bisphosphonates and warfarin. 9 Bisphosphonates inhibit calcium precipitation and osteoid mineralisation. In the study by Spielman et al., bisphosphonates were effective as a prophylactic regimen. 10 In other studies, bisphosphonates failed to halt the progression of heterotopic ossification after mature bone formation has taken place.9,11 There is low level evidence for warfarin to reduce the development of heterotopic ossification following spinal cord injury. 12 Bone-morphogenic protein antagonists may be a potential option for heterotopic ossification management by downregulating the osteogenic differentiation. 13
Although surgical resection is an option, it is usually reserved for patients with significant joint ROM limitation, ankylosis, nerve entrapment or decubitus ulcers. 14 Surgery is usually performed in combination with pharmacological treatment; however, re-ankylosis may still complicate heterotopic ossification resection. 9 In the study by Moore et al. which included 17 brain injury patients, surgical resection of heterotopic ossification with bisphosphonate therapy had a recurrence rate of 15%. 15 Kolessar et al. reported a recurrence rate of 23.8%. 16
Diagnosis of heterotopic ossification can be challenging, as symptoms often precede radiologic evidence of ectopic bone formation. In this case, we presented the clinical and imaging findings of an atypical heterotopic ossification extensively involving the thigh region following an extra-articular fracture.
Footnotes
Patient consent
The patient gave informed written consent and waived his rights for the publication of images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.