Abstract


Scottish Society of Physicians 60th Annual Meeting
Thursday 1 & Friday 2 November 2018
ABSTRACT BOOK
Venue:
Royal College of Surgeons of Edinburgh
Contents
Oral presentations:
Session 1 – page 3 Session 2 – page 3 Session 3 – page 6 Session 4 – page 6
Index of Poster Presentations – page 9
Scottish Society of Physicians Annual Meeting 1st-2nd November 2018
The 60th annual meeting of the SSP took place in the Royal College of Surgeons of Edinburgh. Around 60 delegates attended from around the country for what was once again an extremely enjoyable event. The lectures were, as always, very informative and covered a very broad range of general medical topics. These included liver transplantation, pleural disease, valvular heart disease, obesity and acute poisoning. The Fitzgerald Peel lecture was given by Professor Marianne Nicholson; she gave an outstanding account of the progress made in the management of lung cancer. The Society will reconvene for its 61st meeting in Fife in 2019.
Thursday 1 November 2018
Oral presentations
Session 1
Chair: Dr John Wilson, President Elect, Scottish Society of Physicians
Liver transplantation in Scotland
Consultant Hepatologist, Royal Infirmary of Edinburgh
The Scottish Liver Transplant Unit was established in 1992, and has now performed over 1600 liver transplants. Outcomes have steadily improved and five-year survival is now around 80%. Indications for transplant are changing slightly. Improved antiviral treatment has led to a reduction in the need for transplants for hepatitis C-related liver failure, but this has been offset by a steady rise in the prevalence of obesity-related liver disease and primary liver cancers.
Unfortunately, demand still exceeds availability of donor organs. This has prompted the use of more marginal donors (e.g. donation after cardiovascular death). Novel machine perfusion techniques are helping to improve outcomes from such organs. The way in which organs are allocated has also recently changed to a national system that takes account of both need and utility, to try to maximize benefit. Finally, the Scottish Government is looking at ways to encourage organ donation. Wales have already moved to a system of presumed consent, and demonstrated improvements in donation rates and public attitudes.
Session 2
Chair: Dr Isla McKenzie, Ninewells Hospital, Dundee
Improving the care of older people admitted to hospital with fractures
Professor of Ortho-Geriatric Medicine, University of Nottingham
Vertebral spinal fractures
The acute vertebral spinal fracture (VFF) is the starting point, for many, of a long-lasting, severely painful and disabling condition. 1 It has also been shown that health-related quality of life is considerably lower compared with controls up to seven years post fracture, and these patients experience increased fear of pain and falling, as well as decreased self-esteem. 2 Pain reduces physical activity leading to muscle hypotrophy, weakness and further acceleration of bone loss.3–5 Long term, this leads to dependency, loss of confidence and social isolation.6,7 Most patients who sustain a VFF will have mild to moderate symptoms, however a significant proportion develop substantial pain and disability and require admission to hospital. 8 Hospitalised patients tend to be more elderly, frail, have co-existing comorbidities 9 and their symptoms are more difficult to manage.
Vertebral augmentation for VFF
Universal standard conservative therapy, for the more painful VFF consists of potent morphine based analgesia, bed rest and back bracing, but are poorly tolerated, particularly in the elderly, leading to additional health problems. 10 Vertebral augmentation is a general term for several techniques used to treat VFF, with the aim of consolidating the fracture and, when possible, achieving height restoration. Percutaneous vertebroplasty (PVP) is a minimally invasive, image-guided procedure that involves injection of radio-opaque bone cement into a partially collapsed vertebral body, in an effort to provide pain relief and stability. The mechanism of pain relief is thought to be a combination of more favourable biomechanics after cement strengthening, chemical toxicity and the exothermic effect of cement polymerisation on nerve endings. 11 Other techniques include percutaneous balloon kyphoplasty (PBK), which attempts to restore vertebral body height by inflating a balloon prior to bone cement injection 12 and percutaneous implant procedures (PIPs), which involve the placement of different types of expandable bone implant systems into the fractured vertebrae.13,14
National institute of Clinical Excellence (NICE) guidance recommends vertebral augmentation for patients who have severe ongoing pain after a recent, unhealed VFF despite treatment for pain, and that the pain has been confirmed at the site of fracture, 15 although the optimum timing remains unclear. The VAPOUR study (Clark et al.) found that PVP offered significant pain reduction (superior to placebo intervention) in patients with acute (less than six weeks) on presenting with a VFF. 16 The recently published Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Guidelines on Percutaneous Vertebral Augmentation recommends that patients should present within four months of the VFF (onset of pain) and have at least three weeks of failure of conservative treatment, although intervention within days of a painful VFF may be considered in patients at high risk for bed rest complications like thrombophlebitis, deep vein thrombosis, pneumonia and pressure ulcer. 17 The recent Cochrane review did not support a role for vertebroplasty for treating acute or subacute osteoporotic vertebral fractures in routine practice, however, the heterogeneity of the studies included in the review must be recognised. 18 The mean age of the patients in the Cochrane review (excluding the studies by Clark et al. and Rousing et al., both of which showed a positive benefit to intervention) was 71.1 years. Interestingly in the studies by Clark et al. 16 and Rousing et al., 19 the mean age of the patients was 80.1 years. Furthermore, of the studies included in the Cochrane review, only the study by Clark et al. 16 included patients presenting as in-patients and the remaining with patients recruited as outpatients, mean symptoms from one week to greater than six months. It is likely that those who may have the most to gain form vertebral augmentation are elderly hospitalised in-patients, who present with greater comorbidity, high VAS scores (>7) and are difficult to manage with non-surgical treatments.
Sacral spinal fractures
Pelvic fragility fractures (PFFs) are another common group of fractures that present to clinical attention. The overall incidence is 30/100,000 per year, 20 rising to 92/100,000 per year in those aged 65 years and older. 21 The highest frequency occurs in women over the age of 85 years (450/100,000 patient years). 22 These fractures are extremely painful and carry significant morbidity and increased mortality. The majority of these patients require admission to hospital for pain symptom control. A recent epidemiological study showed that over the past 12 years, the number of PFF admitted to hospital has increased by 58% and 111% in males and females, respectively. 23 Most of these patients are managed non-surgically, with a 10% 30-day in-patient mortality, 30% at 12 months22,24 and significant medical complications related to immobility.22,25
PFF can be classified into fractures of the anterior pelvic ring (most commonly a pubic rami fracture), fractures of the posterior pelvic ring (most commonly a sacral fracture) or a combination of both. Assessment of the posterior pelvic ring is difficult on a standard X-ray of the pelvis, hence fractures of the posterior ring are frequently missed and are more common than realised. Over half of patients admitted to hospital with a pubic rami fracture will have a concomitant sacral fracture, with a higher, 60–80% incidence, in those aged 75 years and over. Therefore, not only is it important to identify sacral fractures in patients who present with a pubic rami fracture, because of their high prevalence, but also because of their clinical consequences, which are more serious. The mean hospital length of stay for those with an isolated pubic rami fracture is 36.3 ± 30.8 days, but significantly longer (p = 0.034) for patients with a combined pubic rami and sacral fracture, 52.8 ± 37.1 days, with higher complication rates. 25
Sacral augmentation for PFF
The ultimate goal of treatment for PFF is early restoration of mobility and independency. This can only be achieved by efficient pain relief and early out of bed mobilisation. Anatomical fracture reduction and restoration of pelvic symmetry are less important. PFF in older people in the UK tend to be managed non-surgically, consisting of analgesia and mobilisation with weight bearing as tolerated, however optimal pain control and early mobilisation remains challenging. 26 From a biomechanical point of view, the undisplaced anterior ring PFF is more stable than posterior ring PFF. The pubic symphysis contributes to only 15% of intrinsic pelvic stability, whereas the posterior ring provides the majority of the structural support and stabilisation of the pelvic ring. 27 Therefore one approach for treating PFF may be to stabilise the posterior ring fracture surgically, and a more conservative, non-surgical approach for the stable anterior pelvic ring fracture. Surgical options for posterior ring fractures range from minimally invasive procedures, to open procedures with internal fixation.28–30 Minimally invasive keyhole surgery techniques which involve percutaneous cement augmentation (injecting cement into the sacral ala at the side of the fracture) occasionally supplemented by a trans-sacral screw, also inserted using keyhole surgery, are increasingly being performed31–33 and have been shown to reduce pain, reduce the amount of analgesia required post-operatively, increase patient mobility and are safe procedures in older people.34–36
References
FITZGERALD PEEL LECTURE
Lung cancer – past, present and future
Consultant Oncologist, Aberdeen Royal Infirmary
For decades, lung cancer has been known as a serious diagnosis with incidence rates perilously close to mortality figures. Lung cancer is the biggest cancer killer, accounting for more than 20% of cancer deaths, and historically responsible for more deaths than breast, prostate and colon cancers combined. Politically there has been reticence to fund research into lung cancer possibly partly due to Sir Richard Doll’s data linking it to smoking raising the suspicion that this is a ‘self induced’ tumour, and arguably related to the high tax income from cigarette sales. In addition, the average age of patients diagnosed with lung cancer is 70 years, and it is more common in lower class men so the patients have been a silent majority.
So far so bad, but thanks to improved understanding of its molecular biology, we are now in a new era of better therapies for the 85% of patients who present with incurable lung cancer. Equally importantly, new data on the effectiveness of screening in high risk patients mean that if we can win the political argument to introduce lung cancer screening, we should be able to diagnose people at an earlier and potentially curable tumour stage.
In the 2018 Fitzgerald Peel lecture, I hope to re-enthuse the audience at the Scottish Society of Physicians and to convince them that we are making significant progress in diagnosis and treatment of lung cancer.
Friday 2 November 2018
Session 3
Chair: Professor Sandra MacRury, Consultant Physician, Raigmore Hospital, Inverness
How can we get people to lose weight – lifestyle, drugs or surgery?
Senior Lecturer, University of Glasgow
This talk will cover the evidence base for obesity treatments, new and emerging, and how they are delivered as part of the weight management pathway. The effectiveness of weight loss for a variety of obesity-related conditions will also be covered. Most importantly, this talk will cover how you can help your patients by using the right language when discussing weight with them.
Modern approaches to management of pleural disease
Consultant Respiratory Physician, Queen Elizabeth Hospital, Glasgow
Pleural Medicine covers a diverse range of clinical entities, including malignancy, infection, trauma and a few rare but important genetic conditions. The management of these must be combined with safe and effective interventional approaches in almost all patients. The last 15 years have seen considerable development of the diagnostic techniques available in pleural disease and rigorous testing of new therapies in large multicentre clinical trials. This presentation will summarise the current state-of-the art, focusing on the major disease areas; pleural malignancy, including Mesothelioma, pleural infection and pneumothorax.
Fitzgerald Peel Prize Winner
Session 4
Chair: Professor Jesse Dawson
Professor of Stroke Medicine, University of Glasgow (presenting author underlined)
Research Into the Effect of Sodium-Glucose Linked Transporter Inhibition in Left Ventricular Remodelling in Patients with Heart Failure and Diabetes Mellitus (REFORM Trial)
1Specialty Registrar in Cardiology, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
2Specialty Registrar and Clinical Lecturer in Cardiology, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
3Foundation Year Doctor, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
4Medical Student, Division of Population Health and Genomics, School of Medicine, University of Dundee, UK
5Professor of Biostatistics, Division of Population Health and Genomics, School of Medicine, University of Dundee, Dundee, UK
6Research Fellow, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
7Consultant Cardiologist and Senior Lecturer, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
8Medical Physicist, Department of Medical Physics, NHS Tayside, Dundee, UK
9Professor of Diabetic Medicine, Division of Population Health and Genomics, School of Medicine, University of Dundee, UK
10Professor of Radiology, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
11Professor of Cardiology, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
12Professor of Cardiology, Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee, UK
References
Improve diagnostic accuracy following routine C-peptide testing in individuals with a clinician diagnosis of Type 1 diabetes
Current post for presenter: ST6 in Endocrinology & Diabetes All authors: Western General Hospital, Edinburgh
84 patients (15.5%) had C-peptide ≥ 200 pmol/L and their initial diagnosis of T1D was re-visited. 11 of these patients (13.0%) had C-peptide > 900 pmol/L with negative autoantibodies and their diagnosis was revised to T2D. Median age of diagnosis was 49 years of age with 9 years median duration of insulin therapy. Three of these patients were Caucasian and had presented with ketoacidosis at diagnosis. So far 4 patients have switched from insulin to alternate anti-diabetic therapy and 6 other patients are in the process of insulin withdrawal.
17 patients (20.2%) had C-peptide ranging from 600-900 pmol/L. Of these, 5 patients had at least one autoantibody positive in high titre. 1 patient had an isolated anti-GAD antibody titre of 12.5 U/ml and a high T1D genetic risk score (93rd centile); this patient stopped insulin after 6 years and is now on oral anti-diabetic therapy. These 6 patients were all considered to have T1D; their median [range] duration of diabetes was 6 [4-13] years. 11 had negative autoantibodies, of whom 7 were considered to have T2D. 1 patient had confirmed HNF1α monogenic diabetes and has now discontinued insulin after 10 years. 3 patients are undergoing further investigation;
56 patients (66.6%) had C-peptide 200-600 pmol/L. 21 of these patients had positive autoantibodies, consistent with T1DM; 1 patient in this group had antibodies in low titre and was also identified to have a pathogenic HNF4α gene mutation. 21 had negative autoantibodies and are undergoing further investigation; thus far, one patient has confirmed mitochondrial diabetes, and another has a pathogenic HNF4α gene mutation. 14 are awaiting confirmation of antibody status.
References
Should we be using the shock index to assess patients presenting with upper GI bleeding?
Clinical Research Fellow 1Glasgow Royal Infirmary
2Odense University Hospital
3Yale University
4Royal Cornwall Hospital
5Singapore General Hospital
6Dunedin Public Hospital Emial:
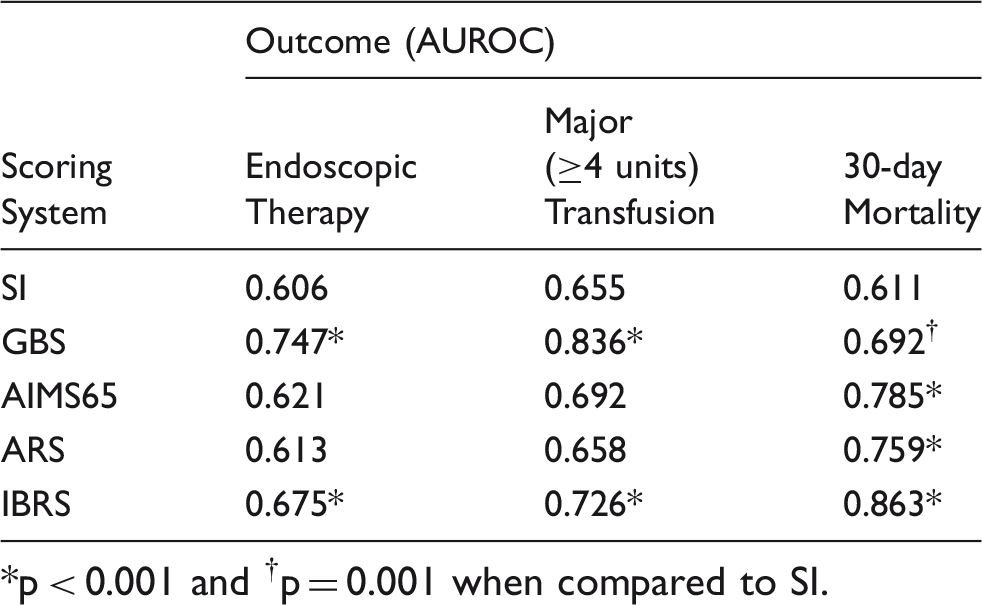
*p < 0.001 and †p = 0.001 when compared to SI.
For predicting need for endoscopic therapy or major transfusion, SI had lower accuracy than GBS and IBRS, but similar to AIMS65 and ARS. In contrast to SI ≥ 1, GBS ≥ 7 correctly identified the majority of patients needing endoscopic therapy (80% vs 21%; p < 0.001). For predicting 30-day mortality, SI had lower AUROC than all other scores. GBS ≤ 1 was superior to SI < 0.7 at predicting low-risk of death (mortality rate 0.35% vs 5.2%; p < 0.001). Patients with S ≥ I1 had lower mortality than those with IBRS ≥ 8 (15.3% vs 34.1%; p < 0.001) and IBRS correctly identified a greater proportion of those who died as being high risk (49% vs 28%; p < 0.001). Adding SI to the IBRS did not improve its predictive accuracy (AUROC 0.864 vs 0.863)
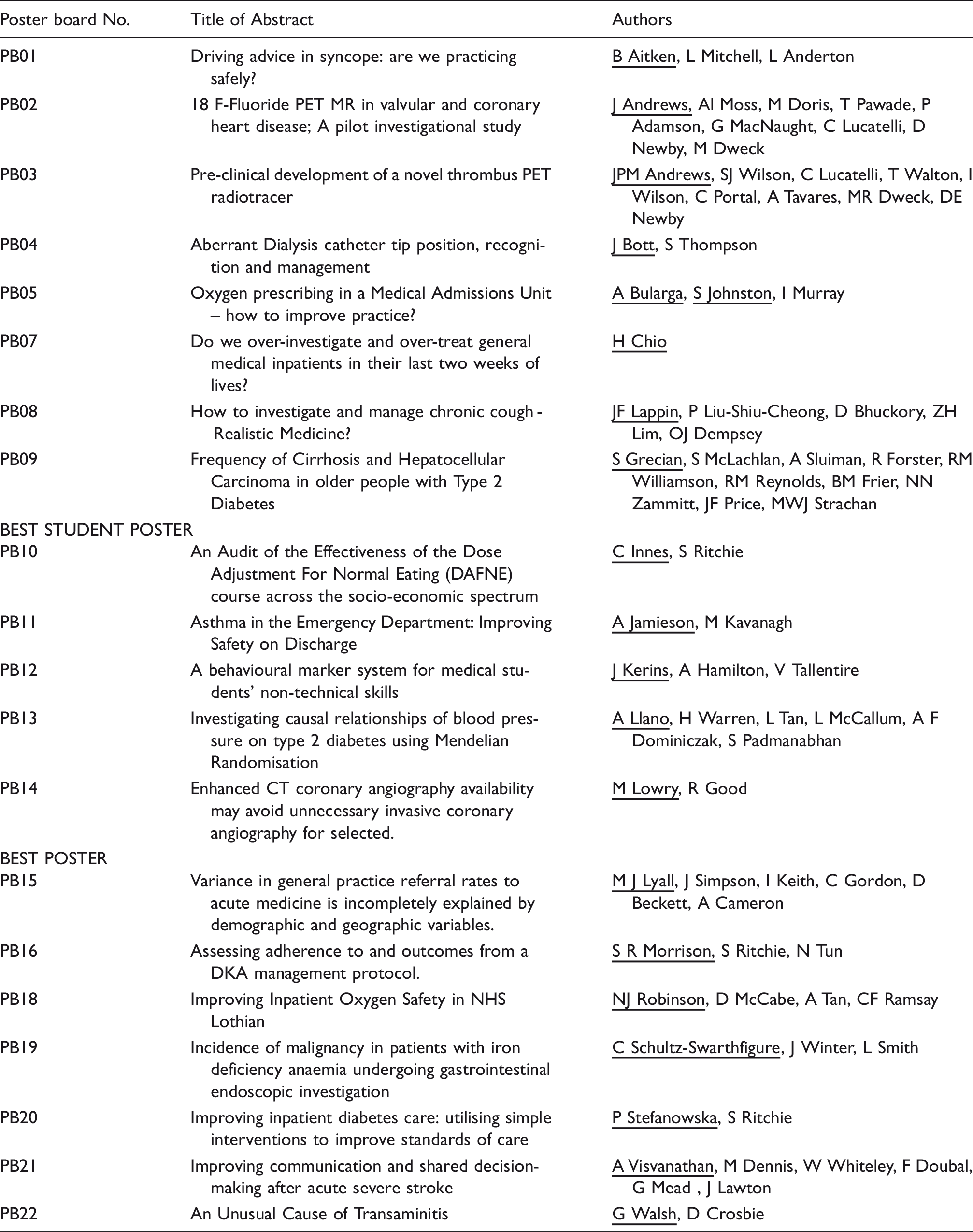
Index of poster presentations