
Abstract
Aims
To assess the incidence of underlying colorectal malignancy in patients admitted as an emergency with a CT diagnosis of acute diverticulitis and determine the need for routine follow up colonoscopy
Methods
A retrospective study was performed on all patients who had been admitted to our surgical unit with CT diagnosed diverticulitis from September 2016 to September 2018 (n = 125).
Results
11 patients (8.8%) required emergency resection with no underlying malignancy found. 76 patients (61%) had a follow up colonoscopy after being discharged. 4 patients were found to have an underlying colorectal malignancy, one of them suspected on CT and another an incidentally detected caecal polyp cancer. Therefore 3/87(3.4%) had an unexpected cancer diagnosis and all those in the diseased segment were within complicated diverticulitis.
Conclusion
Nowadays, multi-slice CT scanners are so good at giving an accurate assessment of colonic pathology. In our study, 96.6% of the patients with a CT diagnosis of acute diverticulitis had no underlying malignancy in the diseased segment with all the cancers within complicated diverticulitis. With such a low yield of underlying malignancy in uncomplicated diverticulitis, we question the need for routine follow up colonoscopy when there is no CT suspicion of malignancy in these patients
Introduction
The incidence of diverticular disease is on the rise across the globe,1–3 and at least 5–25% of patients with diverticulosis have been reported to go on to develop into diverticulitis.4,5 This presents a growing concern as it can potentially add further burden onto our already over-stretched health care systems. With the advances in our current imaging technologies and the easily accessible colonoscopies, more cases of diverticulosis and diverticulitis have been diagnosed.
Recent evidence has shown a high accuracy rate of detecting colorectal pathologies such as malignancy, inflammatory bowel disease, and diverticulitis with our modern Computerised Tomography (CT) scans.6,7 We, therefore, wonder if there is still a need for further routine procedures such as colonoscopy for patients who have an unequivocal CT diagnosis of diverticulitis. Multiple national guidelines have previously recommended routine colonoscopy for all patients who have been diagnosed to have acute diverticulitis8–10 as there were concerns that colonic malignancies could have been missed in the diverticular segment in this group of patients, but is this relatively invasive procedure really necessary?11,12
Our study aims to assess the number of colorectal cancers detected in patients who had an unequivocal CT diagnosis of acute diverticulitis in order to determine if routine colonoscopy is really necessary in this group of patients.
Methods
The study was carried out by collecting all the data retrospectively from our admission database between September 2016 and September 2018, but only patients who were admitted to the acute surgical receiving unit with a CT confirmed diagnosis of left sided acute diverticulitis were included in the study for analysis. Follow up colonoscopy would be defined as any colonoscopy performed within one year after the CT diagnosis of acute diverticulitis however practically speaking those who had a colonoscopy within the preceding year could be argued to have had their bowel adequately assessed via direct visualisation as well.
All the electronic case records, endoscopy reports, pathology results, and radiology reports from this group of patients were reviewed and their accuracies were cross checked from 2015 to 2019. Hinchey’s classification and any surgical or radiological interventions undertaken were also recorded. The radiological diagnosis of diverticulitis was made by the reporting radiology consultant and when possible, correlation with the pathological findings was also made. Any radiological or surgical interventions were also reviewed and cross checked (Figure 1).
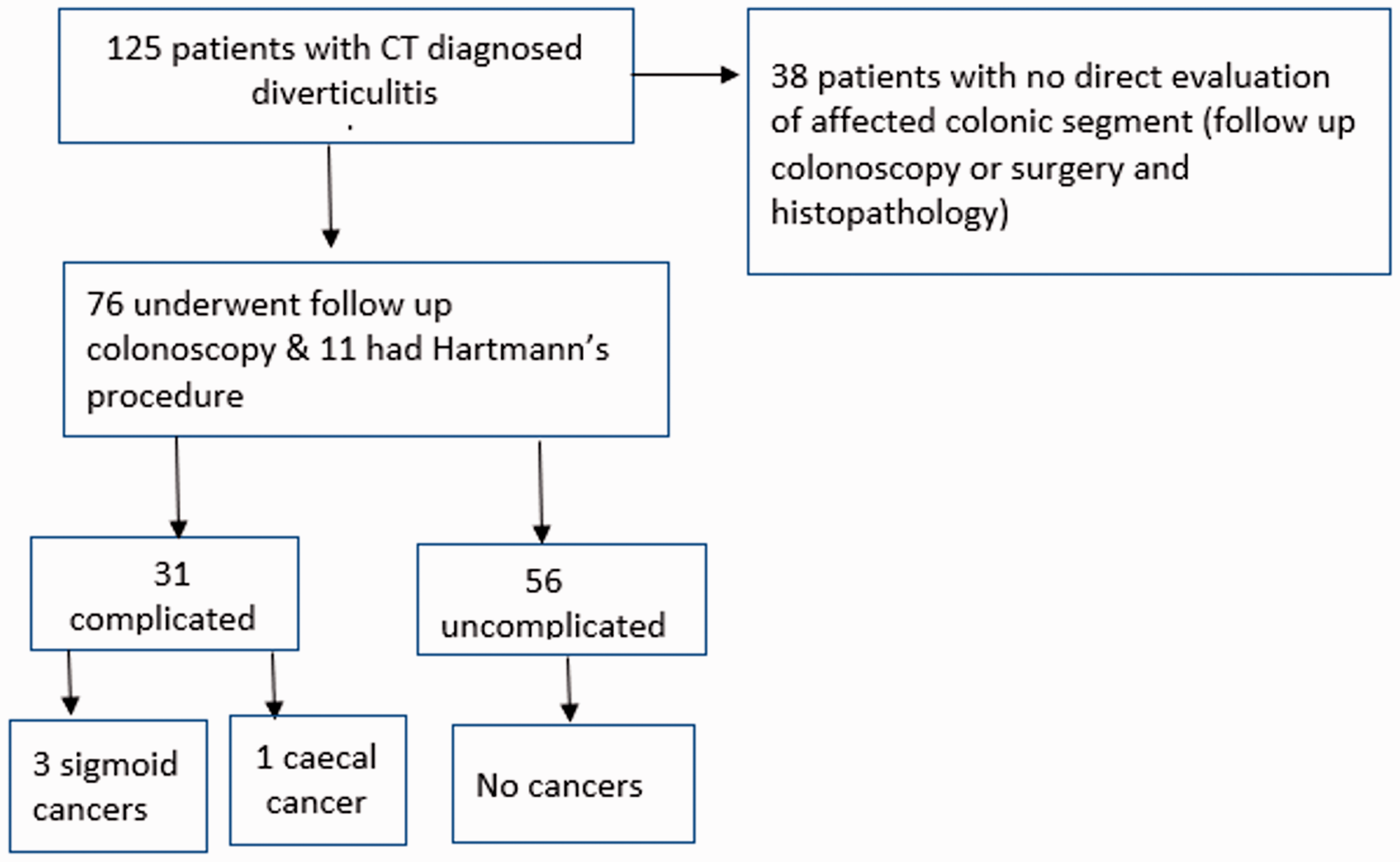
Outline of patients in the study.
The work was registered as a retrospective clinical audit and therefore no specific ethics committee approval was required.
Results
125 patients were identified during this study period, and their electronic records were reviewed. 87 were females and 38 males. Their age ranged from 30 years to 95 years with a mean age of 61 years. Out of all the patients with a CT diagnosis of diverticulitis, 40 (32%) patients had complicated and 85 (68%) uncomplicated diverticulitis. Out of these two groups of patients, 76 (61%) had a follow up colonoscopy after being discharged from the hospital, 11 (9%) had emergency bowel resection, 38 (30%) did not have either a follow up colonoscopy or a surgical resection. 87 patients in total therefore had their bowel adequately assessed via direct visualisation with colonoscopy or histopathological examination.
None of the patients who underwent resection were found to have cancer in their resected specimens. Amongst those 87 patients 4 cancers (4.6%) were detected (Figure 2). However, one of those cancer patients was suspected to have an underlying malignancy in the diverticular segment on CT and the reporting radiologist had recommended direct endoscopic visualisation. Another cancer patient was found to have an incidental polyp cancer in the caecum but no cancer lesion was detected in the diverticular segment. Excluding the caecal cancer patient would reduce the incidence of cancer detected after CT diagnosis of diverticulitis(within the diverticular segment) to 3.5% and excluding the one suspected on CT as well would reduce the rate of unexpected cancers within the diverticular segment further down to 2.3% (Figure 3).
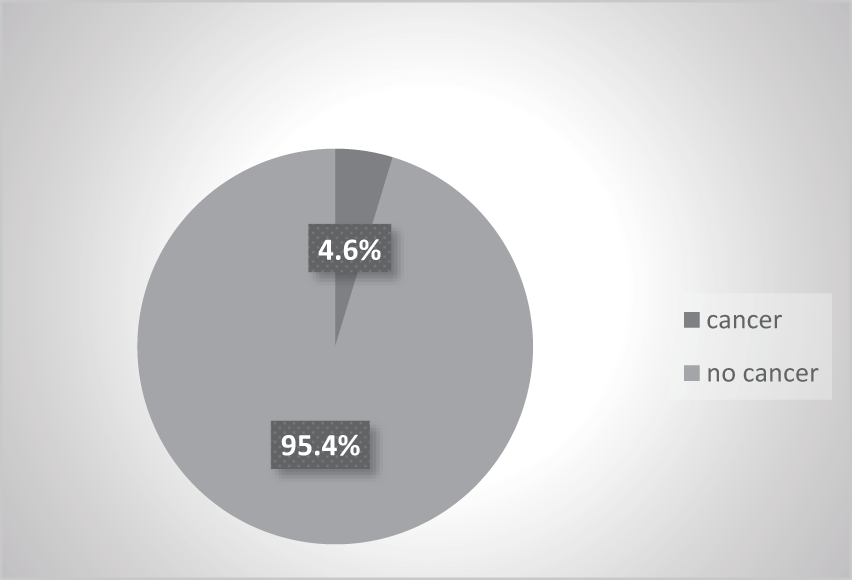
Overall colorectal cancer detection rate in diverticulitis patients.
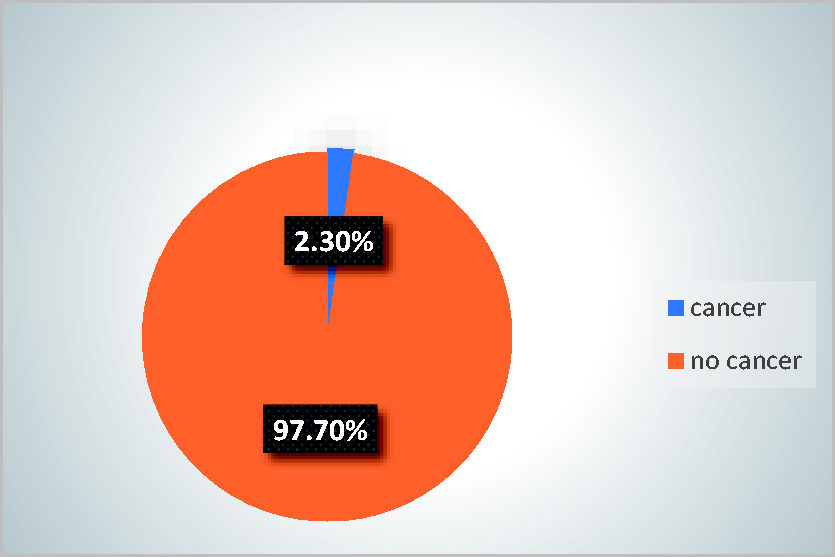
Unexpected cancers detected in the diverticular segment.
There were 38 patients in total out of the whole cohort who did not have follow up colonoscopy or bowel resection. Seven of them was due to the fact that they have had a colonoscopy within 1 year prior to their CT diagnosis of acute diverticulitis but the rest of the 31 patients were either lost to follow up, or thought to be too young for suspecting any underlying malignant disease, or deemed to be unfit for further investigations by the attending surgical teams. None of these patients were reported to have a bowel cancer to date.
Complicated diverticulitis was diagnosed in 40 patients. Complicated diverticulitis was defined as any grade higher than Grade1a in the modified Hinchey classification. All the cancers were detected only in those who had complicated diverticulitis and the prevalence of colorectal cancer within this group of patients in our study was provisionally calculated as 3/40 (7.5%). As previously mentioned 11 of the patients with complicated diverticulitis had the diverticular segment resected with no cancers detected and of the remaining 29 patients 2 patients were deemed unfit for further investigation due to age/comorbidity and one did not attend their colonoscopy appointment, one was visiting from abroad and was advised to have further follow up in their home country. 2 other patients had a CT colonography as an alternative to colonoscopy and 3 have already had a clear colonoscopy within the preceding 12 months . The remaining 20 patients did get a follow up colonoscopy. Taking into account only the patients that had a colonoscopy after the acute admission or a bowel resection/histology the prevalence of cancer within the complicated diverticulitis group would be 9.7% (3/31) as demonstrated in Figure 4. Comparing this to zero cancers in the uncomplicated diverticulitis group who had their bowel adequately assessed (56 patients) using the Fischer exact test would give a p value of 0.0424 demonstrating a statistically significant difference between both groups (with significance level cut off set at p < 0.05)
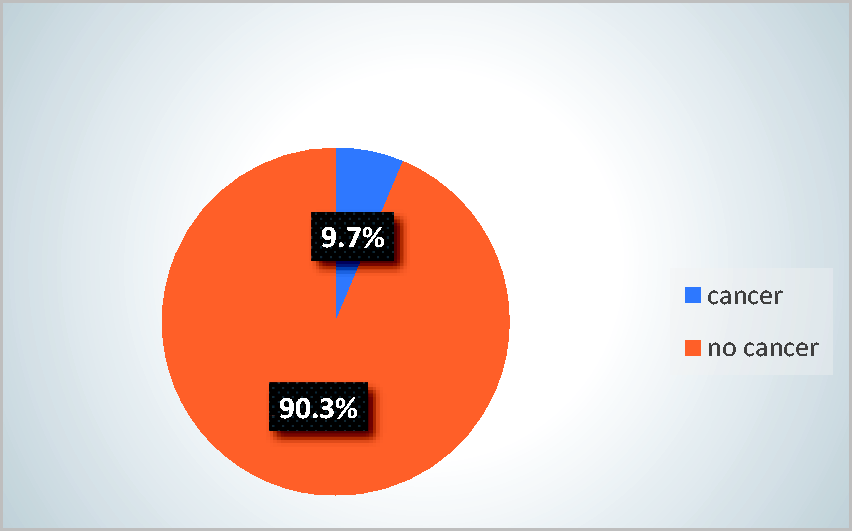
Cancers detected within complicated diverticulitis.
Discussion
A routine follow up colonoscopy after a successful treatment for diverticulitis was previously recommended by a number of surgical and gastroenterological societies.8–10 It was thought that a malignant process in the diverticular segment could have been the cause of some or if not all of the presenting symptoms. Obviously if a follow up colonoscopy is not advocated, then there is a worry that a significant number of cancers could have been missed. In our study, we have shown that 3.4% of patients who either had a follow up colonoscopy or surgical resection after a CT diagnosis of acute diverticulitis were found to have a cancer in their diverticular segment. The true percentage for this group of patients could have been lower if we have included those 38 patients who did not have a follow up colonoscopy or surgical resection. Certainly when we conducted our study, none of these patients had been reported to have a colorectal cancer, but we do realise that our data were incomplete for this group of patients as some of them had been lost to follow up. However including the 7 patients that had a colonoscopy within the preceding year and excluding the patient with the suspected cancer on CT would further reduce the pickup rate of unexpected cancer down to 2.1%.
We also need to remind ourselves that colonoscopy is an invasive procedure which is not without its own risk of some serious complications. With the introduction of the national bowel screening and urgent cancer suspected symptomatic investigation pathway, the demand on colonoscopy is on the rise across all health boards in the UK. Hence, we need to reconsider whether there is still a strong indication for a routine follow up colonoscopy after CT diagnosis of uncomplicated diverticulitis. With only 3.4% chance, at the most, of an underlying cancer in the diverticular segment and almost exclusively within complicated diverticulitis, one could argue that this percentage is probably low enough to avoid a routine colonoscopy in uncomplicated diverticulitis. Some surgical and gastroenterological societies have in fact already issued guidelines to negate the need for follow up colonoscopy after the diagnosis of acute diverticulitis.11,12
In our dataset, all the cancers were only found in the complicated diverticular disease group, which is defined as Hinchey’s Ib or above. Accordingly, we believe that it would be safe to advocate no routine follow up colonoscopy for the uncomplicated group of patients and this is also in keeping with the recent evidence published in a meta-analysis looking at the prevalence of colorectal cancer in the complicated diverticulitis versus the uncomplicated diverticulitis groups. 13 This study demonstrated an overall prevalence of cancer of as low as 2% within diverticulitis in general but the prevalence was even lower (0.5%) in the uncomplicated group. 13 The low prevalence in the uncomplicated group was also found to be comparable to that in the asymptomatic bowel screening population (0.4-1%) as published in other studies.14–20 However, on the contrary, the prevalence in the meta-analysis was found to be much higher in the complicated group (8.3%). This significant difference between the two diverticular groups also correlates with the findings in our study. Accordingly we would suggest that limiting follow up colonoscopy to that high risk group would result in better use of resources with a negligible risk of missing any underlying sinister pathology in the uncomplicated diverticulitis group. Certainly if any of these patients were to develop any red flag symptoms of possible underlying bowel cancer or test positive in bowel screening then a colonoscopy would definitely be indicated to investigate this further.
In summary, there seems to be little benefit in subjecting patients with an unequivocal CT diagnosis of uncomplicated diverticulitis to routine follow up colonoscopy. However, for patients who have a CT diagnosis of complicated diverticular disease or suspicious features of underlying malignancy, follow up colonoscopy would still be quite justified and definitely recommended.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.