
Abstract
Introduction
Digital health (DH) is continuously evolving by use of information and communications technology to improve healthcare provision, thereby reshaping systems and clinical practices. Recent studies identified an overwhelming lack of awareness of DH within the profession. This study aimed to analyse student perceptions and knowledge of DH to assess confidence in its use to develop greater DH awareness and literacy.
Methods
Students enrolled in undergraduate medical degrees were invited to take part in an online survey assessing aspects of DH including demography, familiarity, attitudes, level of knowledge and confidence. Anonymised data was collated and subsequently analysed to review DH awareness.
Results
A total of 143 students participated from nine British universities with 28.7% of respondents admitting low levels of familiarity of DH concepts. Students anticipated negative repercussions of DH including reduced data security (42.7%) and deterioration in doctor-patient relationship (30%); while improvements in healthcare access and health-outcomes are expected by 89.5% and 68.5%, respectively. 71.4% of participants believed they had minimal experience of exposure to DH and 76% believed they did not possess the necessary skills to utilise DH. Only 3.5% of students had some exposure to DH teaching during their course.
Conclusion
There is an important requirement to address the lack of knowledge and exposure of students to DH, particularly as the world targets the COVID-19 pandemic. DH is forming the basis of the ‘new normal’ in healthcare, however the full potential of DH cannot be achieved unless there is an increase in its teaching incorporated into medical school curricula.
Background
An inseparable incorporation of technology and health care practice has created a shifting paradigm to maintain the failing and financially unstable healthcare system. This incorporation has brought a positive impact on the health and wellbeing of individuals and communities world-over.1,2 Predicting this change in landscape as early as 1997, the World Health Assembly identified advancing innovation and use of technology in healthcare as one of the essential functions of sustainable health systems. 3
Recognising and emphasising the significance of digital health (DH), The United Nations General Assembly of 2000, in its Millennium Development Declaration, and the 58th World Health Assembly in 2005 both called on their respective member states to cooperate in ensuring the realisation of the potential and promises of DH.4,5 Locally, in the UK, £6.2 billion has been invested by the government, in establishing the National Program for Information Technology within the National Health Service. 6
Defining DH is as complex as its successful implementation. The most widely accepted definition of the term is “the use of information and communications technologies to improve human health, healthcare services, and wellness for individuals and across populations”. 7 DH which includes eHealth, telehealth and mHealth has made a plethora of technologies available. These fall within a broad spectrum ranging from genome sequencing to smartphone-connected electrocardiography devices. 8 The revolutionary discoveries of DH are transforming healthcare services and clinical practice at an unprecedented rate, providing opportunities to enhance quality of health care service provision. It has empowered the public to be more engaged in their health-related needs and wellbeing as well as promoting communication, and a better partnership between physician and patient.1,7,9,10 It promises solutions to many of problems currently existent in healthcare systems and health service provision. As reported in numerous studies, DH is expected to improve efficiency, provide better quality of care, scalability of interventions, increase accessibility to services, reduce costs and enhance accuracy of diagnosis and management.1,9–11
The various components of DH encompass the use of technology to prevent, diagnose, treat and monitor diseases and conditions while supporting, promoting and enhancing management decisions, surveillance, health promotion, awareness, education and research. 12 Despite the potential of improving healthcare systems, opinions and attitudes towards the impact of DH technologies are of uncertainty and doubt. These new tools have raised questions on the potential negative impact on healthcare services, most notably; the physician-patient relationship, ethical considerations, and information security and privacy. One particular study identified a lack of clinician endorsement of DH interventions as an important barrier affecting its successful implementation. 2 This identifies a larger persisting issue of lack of knowledge and attitude towards DH technologies. The existence of these issues and questions among the general population as well as the clinical population, need to be acknowledged and answered in order for optimal implementation of digital health at a large scale.
The COVID-19 pandemic has propelled the world into a DH frenzy, accelerating research and implementation of DH. The high virulence of this microbe has forced medical staff in every country to rethink the practice of medicine, in a manner that minimises patient contact and maximises outcomes. There has been a surge in development of online softwares through which consultations, referrals and management of patients can be guided during this pandemic. 13 The profound and sudden impact of the pandemic revealed that the world was largely unaware of the untapped potential DH holds. The new-found potential revealed the unfamiliarity of the DH concept amongst the medical population, forcing them to adapt to the ‘new normal’. DH has set the premise for this ‘new-normal’ within healthcare as COVID-19 has led to increasing DH use in day to day provisions. This rapid transition to digitizing health may have been smoother through DH training and education, which remains largely non-existent throughout the United Kingdom (UK). 14 In a time where COVID-19 continuously poses a threat to public health, it is vital to optimise the use of DH to continue providing care, particularly remotely.
The inevitability of healthcare services’ dependency on digital technologies must be accepted along with the inevitability of future transformations caused by technological advancements. Physicians are likely to keep abreast with this rapidly changing paradigm. Thus, it is vital that current healthcare staff and future physicians (i.e. medical students) are made aware of the importance of DH and the importance of regularly updating knowledge and skills related to it.
With the prediction and reality of digital health redefining and reshaping the medical practices as they are known, it is imperative to ask whether healthcare providers are prepared to digitalise their practice, in addition to providing adequate training for future staff. Thus, the main aims of this study were to assess current perception and knowledge of DH amongst medical students, and to assess their preparedness in contributing towards further developing DH.
Materials and methods
Study design
An observational, multicentre cohort study was conducted by inviting medical students across the UK to respond to an online questionnaire. Participation was optional and data was collected anonymously with questionnaire completion considered as consent to participate. Participants were contacted through administrators at various medical schools. The questionnaires were then subsequently distributed to students.
Settings and participants
All active students enrolled in a General Medical Council recognised medical school in the United Kingdom were eligible to participate. Data collection was performed using an online questionnaire created using the GoogleForms™ platform. Participants from nine medical schools offered to circulate the questionnaire among their students.
Survey content
The survey was developed in cooperation by the authors of this study. Numerous amendments and revisions of the survey were carried out prior to utilisation of the survey. The survey was subsequently distributed amongst nine UK medical schools. It allowed for multiple choice responses and free-text bound within the following domains:
Demography – year of study, gender, interested specialty Familiarity with the concept of digital health. Attitudes towards digital health. Current level of knowledge and skills related to digital health.
The questions were randomly allocated in order to avoid priming, framing or any other potential biasing phenomenon that may occur with theme-based ordering of questions. The questionnaire was circulated via weekly bulletin emails, social media posts and direct emails to students by medical school administrative teams. All medical students, at the time of the survey conduction, of participating universities were invited to take part. Participants were re-contacted two weeks following the initial survey distribution to maximize response rate.
Statistical methods
Data analysis was reported using descriptive statistics. Microsoft Excel™ was used to conduct statistical analysis in this study. Responses were collated and numerical analysis was carried out to identify the current perceptions in relation to DH. Both qualitative and quantitative analysis was carried out on the collected data.
Results
Demographics
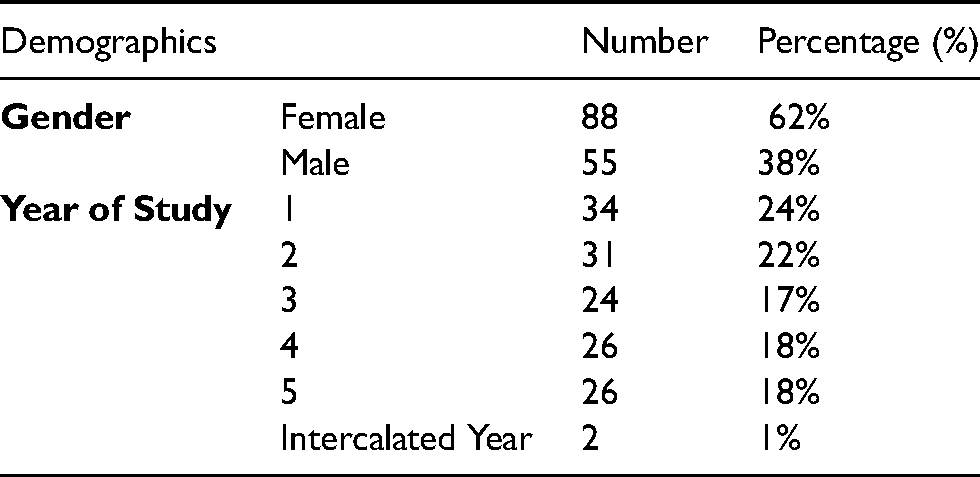
A total of 143 students from nine different medical schools across the UK voluntarily participated in this study. 62% of the respondents were female with the students distributed across all years of medical school. 1% of the respondents were undertaking an intercalated year at the time of surveying as described in Table 1. A response rate could not be calculated as the total number of recipients for the questionnaire invite was unknown as it was distributed amongst entire schools.
Basic demographics of study population.
Familiarity with digital health
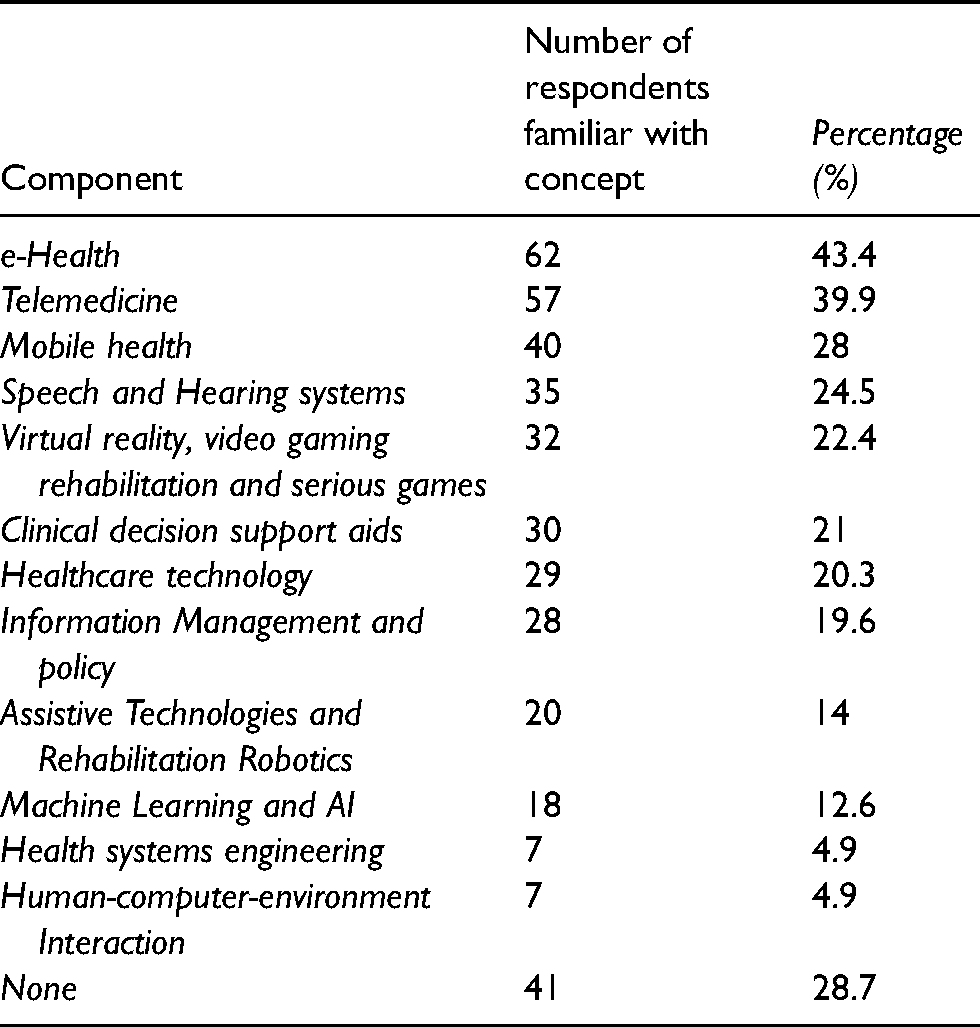
71.3% of respondents were familiar with the concept of DH, with e-Health being the most familiar component amongst 62 (43.4%) respondents, followed by telemedicine with 57 (39.9%) respondents. Health systems engineering and human-computer-environment interaction principles tied for least popular domains with recognition from 7 (4.9%) students. Almost a third of respondents (28.7%) acknowledged they were not familiar with the concept of DH. Further responses to familiarity in DH are detailed in Table 2. Terms were not explicitly pre-defined to limit bias and to allow a better understanding of student understanding of the terms.
Familiarity with digital health.
Medical student attitudes towards digital health
119 (83.3%) respondents believed implementation of DH will impact healthcare service provision in some way, with 46.2% of respondents expecting these to be significant changes. 2 (1.4%) opined that the medical field will remain largely unchanged. Almost 50% of the study population (61) were undecided as to whether doctor-patient relationship would be affected by DH. The remainder were split with 43 (30.1%) believing the relationship would weaken, and 39 (27.3%) believing it would strengthen. Four (2.8%) and 10 (7%) respondents are of the opinion that such relationships would be affected very negatively or very positively, respectively. The general attitude towards the positive impact of DH on patient health outcomes was apparent with only 7 (4.9%) subjects believing DH would contribute negatively towards patient outcomes. 98 (68.5%) respondents expected DH to contribute positively to patient outcomes, with further results detailed in Table 3.
Summary of student attitudes.
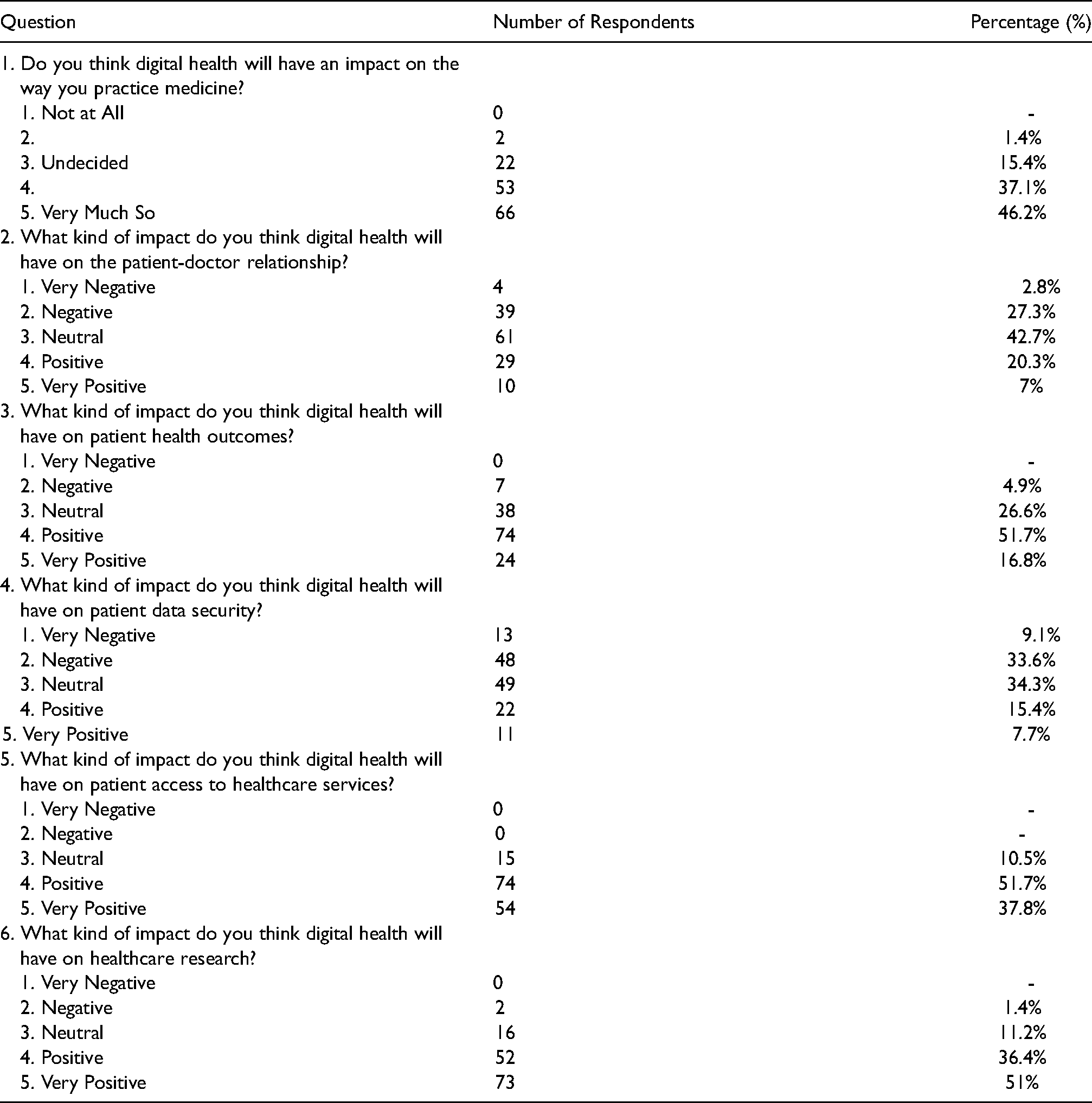
When questioned about data and information security and confidentiality issues, 42.7% of respondents feared for loss of data security with increased vulnerability and higher risk for patient confidentiality breaches. 23.1% believed DH would increase safety of patient information and other data. Nearly all respondents (89.5%) seemed to agree that DH would improve patient access to healthcare with the remaining 15 (10.5%) of the population uncertain about its impact. Similarly, 87.4% of subjects believe healthcare research will benefit greatly from digitalization.
Advantages and disadvantages of digital health
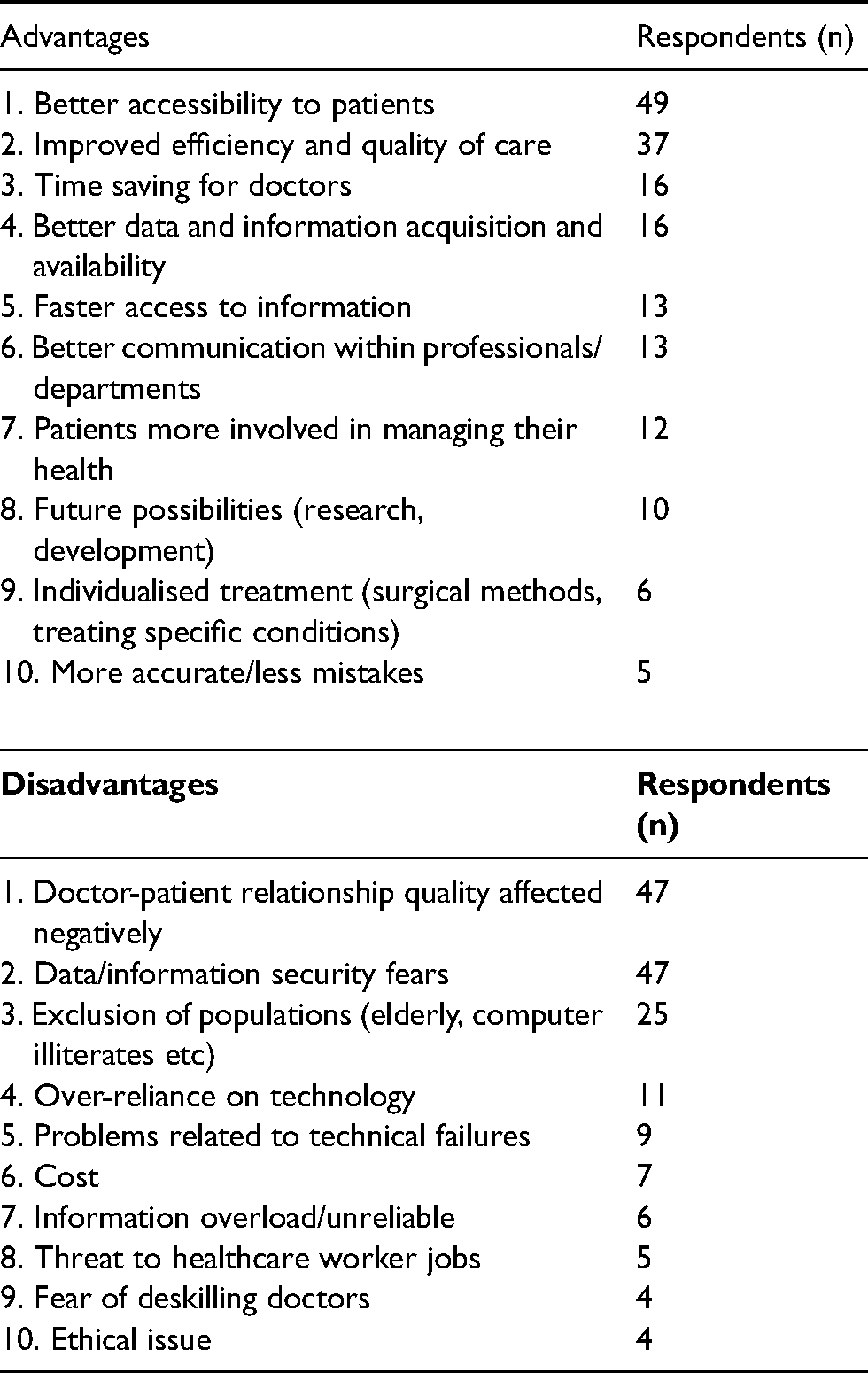
Respondents were provided a free-text area to express their opinion in regard to the advantages and disadvantages of DH. Common and recurring themes were isolated amongst the responses and were categorised into various domains as represented in Table 4. The most common advantage expressed among participants was that of improving accessibility of healthcare to patients. A negative effect on doctor-patient relationship was noted as the most frequently addressed disadvantage of DH.
Advantages and disadvantages of digital health.
Knowledge, skills and contributions
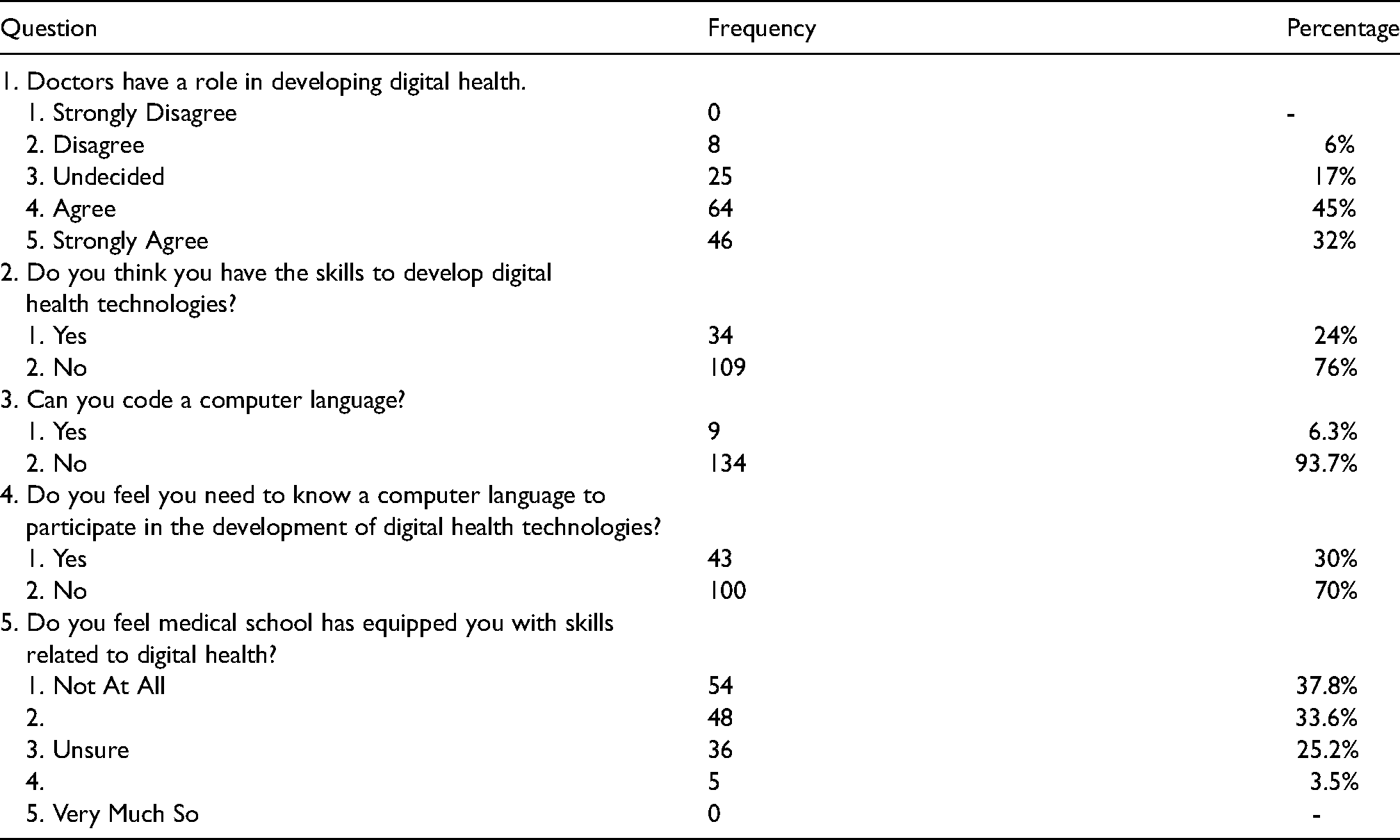
Participants were also queried about student satisfaction with the volume of teaching, training and exposure to DH provided by medical schools. Overall, the majority of respondents were lacking in knowledge and skills relating to DH. Only 3.5% of the respondents agreed to having some exposure to DH teaching. 71.4% reported they had very little to no experience at all within the domain of DH. Despite a lack of knowledge in using DH, 77% of respondents believed that doctors have a significant role in developing DH technology, as represented in Table 5.
Summary of student knowledge and skills.
Discussion
The promises, potentials and possibilities arising from development of DH technologies are innumerable and largely unexplored. Despite these promises and positive evidence from numerous reports of small and medium-scale implementations, DH as an entity is struggling to be integrated and considered routine practice within the health care service. 2 To reach the full potential of growth and development, emphasis should be placed not only on technological and infrastructural advancements but also on DH education. DH knowledge and skills among physicians and medical students alike is imperative to implementing and further exploring DH. This study aimed to ascertain the attitudes towards DH while assessing the level of knowledge and skills related to digital health among medical students along with their confidence levels in contributing towards sustaining and developing the field.
Insight obtained from analysis of data collected from 143 students across nine medical schools in the UK was provided in this report. Although e-health and telemedicine were identified as the two most popular components of DH, nearly 30% of the study population acknowledged they were not familiar with the concept of DH. This finding is vital considering the importance that components of DH play in current patient care and also demonstrates the lack of education and awareness related to DH in medical schools.
Echoing literature findings, a large proportion of participants believed and expected DH to exert a positive impact on medical practice. Improved interpersonal and interdepartmental communication, increased involvement of patients in their care primarily allowing for individualised treatment plans are some of the potential enhancements, according to participant responses. Eysenbach 15 has reflected this finding by providing a summary of potential promises of efficiency, improved quality of care, improved doctor-patient relationship and e-health related positive outcomes.
This study is similar in nature to a previous study conducted by Machleid et al.; 17 however, focuses on perceptions and teaching within the United Kingdom as opposed to Europe. Approaching single countries individually may provide baseline information on perceptions of DH, which could subsequently contribute to larger scale studies with more pronounced recommendations based on the findings. The overall findings of this study replicate those found in the earlier study by Machleid et al. where there was a widely reduced perception of DH, as well as a lack of DH teaching in medical school curricula.
Patient-Doctor relationship
30% of participants believed that DH would have a negative impact on the patient-doctor relationship. This reflects findings of certain previous studies which highlighted the belief that the impact of DH will downgrade the quality of patient-doctor relationships as technology grows to take over the role of the physician. Many believe digital interventions will damage the therapeutic and social nature of the relationship by transforming the interaction into one that is impersonal. 11 However, recent literature suggests that this negative belief is merely a misconception. Baird and Nowak 16 challenged this negative understanding by highlighting the findings of several studies which generally report improvements and increased efficiency in patient-doctor communication. This was primarily following the introduction of digital platforms in clinical practice. 68.5% of respondents in this study believed DH would have a positive impact on medical practice. These studies provide us reassurance that with planned, appropriate and well-executed integration, DH may improve patient-doctor communication along with a myriad of other benefits such as improved compliance rates.2,18 These studies also serve as evidence to medical professionals who are sceptical of implementing DH, that multiple beneficial effects in practice exist
Patient health outcomes
68% of the study population believed that health outcomes would improve through increasing DH practices. Furthermore, they believed that DH enhances efficiency and quality of care as well as minimizing human factor errors which would improve the standards and safety of healthcare provision. A recent systematic review demonstrated that patients often reported shortcomings in their care and hoped DH would minimize mistakes. 11 This supports the findings from this study that medical professionals and patients alike believe that DH has potential to improve health outcomes.
Patient data security
A significantly large proportion of participants (43%) expressed concerns regarding the negative effects DH may have on data security. These are rational concerns that are consistent with current fears within society in large. O’Connor et al. 11 concluded that information security fears are one of the major factors for the low level uptake of DH, particularly among patients. A further study reported a 125% increase in healthcare data breaches over a 5 year period, with the strongest motivator for criminal cyberattacks being the value of information. 19 Healthcare information has the highest cost per capita for a stolen record as compared to any other industry. As a result, the primary cause of data breaches within healthcare are criminally motivated. Recently, this has led to increasing cases of medical identity theft. This remains a significant threat to the prosperity and development of DH, and must be addressed appropriately in order to increase its uptake.
Patient access to healthcare services
No participants within this study believed that DH would negatively impact access to healthcare services. However, concerns were raised about the possibility of “exclusion” of certain patient groups due to numerous reasons, including inadequate finances and computer literacy. There is an increasing requirement to focus on these problems within healthcare provision such as poor access, uncoordinated care and increasingly costly healthcare. 11 This would lead to a wider range of access to DH allowing greater access to healthcare.
Healthcare research
A significant majority (87%) of participants believe digitizing healthcare will have a positive impact on research activities. This is mainly due to centralizing information, offering reduced manual workload, increasing data points in an increased number of patients as well as improving quality and efficiency of electronic records. 9 These factors allow for research to be conducted in a more efficient, controlled and accurate manner.
Knowledge and skills related questions
This study identified low levels of both knowledge and skills regarding use of DH amongst the study population. Less than a quarter of the respondents believed they had adequate knowledge to contribute towards digital health development despite 77% of respondents believing doctors have an important role in developing DH. This finding, when analysed alongside the finding of reduced familiarity with the concept of DH shows a major lack of knowledge and awareness among medical students highlighting a gap in the medical school curriculum.
Despite the recent growth of DH, medical schools have not yet integrated DH related teaching into their curricula. A lack of knowledge translates to reduced participation in activities related to usage promotion. Failure of education could also lead to misconceptions about DH subsequently leading to negative attitudes. These concerns were highlighted by the subjects of this study, and have been reiterated previously where students identified a lack of DH teaching as the main obstacle for its uptake. 20 This may be minimised by short DH teaching in the form of lectures, workshops and, if practical, direct student exposure to available DH facilities and resources allowing the students to gain first-hand experience.
COVID-19
The development of DH strategies has become increasingly warranted particularly since the outbreak of the COVID-19 pandemic, where there has been a move towards further digitizing healthcare. This study reveals that prior to this global pandemic, knowledge regarding digital health was very limited amongst medical students. Similarly, knowledge amongst current medical professionals is likely to be low as medical school teaching remains minimal, thus contributing to a slow response from the medical aspect in dealing with this pandemic. An increased knowledge of digital health would potentially have led to a faster response in dealing with the crisis, by means of outgrowing traditional methods of medical practice. One such example is a better engagement with DH would have allowed a faster response for teleconsultations thereby reducing the lapse in regular healthcare provisions in the initial phase of the coronavirus crisis.
As the coronavirus situation is currently ongoing with its threat lingering for the foreseeable future, it is important to incorporate innovative education subjects such as DH into the medical curriculum as these become an inherent part of the medical system, particularly in response to the ‘new normal’ that coronavirus has set. DH can contribute significantly to restructuring healthcare in terms of social distancing by reducing face-to-face meetings, however consecutively providing access to healthcare. This is particularly vital in order to curb the infections throughout the world and decrease further outbreaks. It is likely that in future, the virus is anticipated to become localised to hospitals, as these remain congested areas with high human traffic. This is just one example of the numerous ways in which DH can be utilised in relation to the pandemic. The impact of coronavirus on DH has been profound and acceleratory, leading to a rapid uptake across all specialties. The impact is likely to continue projecting on an upward slope, revolutionising the manner in which multiple specialties operate, from general practice, to surgery to medicine, in order to optimise healthcare provisions.
Limitations
Online survey-based methodologies have many limitations. One of the major limitations to this study was the inability to effectively control the recipients of this survey. This survey was primarily distributed through contacting medical school administrative staff, who subsequently circulated the survey via email and/or social media. Due to this, it was not possible to effectively know how many people were offered participation in this study.
Furthermore, 24% of participants in this study were in Year 1 of their medical education and contributes the largest percentage from the various year groups. This is significant as these participants may not yet have gained enough exposure to their medical curricula to have an adequate understanding of digital health and may not accurately represent the digital health literacy in the surveyed medical schools. The lack of awareness of this subject amongst this subgroup may represent either an overall lack of awareness and teaching of digital health, or it may represent the relative inexperience of the Year 1 medical students participating in this study, as they may not yet have gained exposure to the medical schools’ digital health teaching.
In this study, the terms used were not predefined. The rationale for this was to avoid anchoring bias, wherein a participant would likely ‘anchor’ themselves to the given piece of information and answer subsequent questions based on this information. On the contrary, excluding definitions for terms may also be seen as a limiting factor as participants may not actually understand what the terms mean on an individual basis. However, the lack of understanding of the terms remains an important aspect of this study.
This study was limited by the responses gained, particularly as there are 34 medical schools in the United Kingdom, however, responses were obtained from just 9 of these. This study could be largely improved by targeting each of the medical schools, with a more nuanced focus on how teaching for DH varies between the medical schools, and subsequently, how this affects medical students’ understanding of it. It would be worthwhile to increase the scale and scope of this study to have a larger and more detailed understanding of exactly how deficient UK medical schools are in DH education and how this deficiency can be improved.
Conclusion
The causes for reduced uptake of DH, includes the lack of computer literacy, unawareness of the existence and uses of DH, lack of advice and recommendation from a trusted and knowledgeable source and a lack of clinical endorsement of DH devices. It may also be argued that the lack of clinical recommendation and lack of advice and encouragement of DH resource use can be due to a reduced level of knowledge and awareness of the uses and potential benefits of DH resources among physicians. Hence, it can be assumed the impact of the above-mentioned barriers can be minimised by educating the medical students, subsequently leading to a more appropriate and hopefully increased use of available digital health resources. Furthermore, the implementation of DH does not strike off all traditional methods of practicing medicine, and these approaches continue to remain available as necessary for both physicians and patients alike. Education and incorporation of DH teaching in medical school curricula would benefit the future of DH improving healthcare provisions across multiple domains.