
Abstract
Objectives
To assess the feasibility of performance enhancement coaching (PEC) for newly appointed Urology registrars (ST3s), specifically: whether the concept appealed, and which areas beyond technical skills acquisition were felt to be most relevant or useful.
Subjects and methods
All delegates on the Urology Bootcamp 2023 were invited to take part in an online survey before and after a 2-hour PEC workshop, collecting: basic demographic data, performance challenges, and the important aspects to include in, and consider with, a coaching programme. The workshop was delivered by a surgeon with a professional coaching qualification, to groups of four delegates at a time over 4 days. Ten pre-defined areas were offered during the session.
Results
On a scale of 1 (poor) to 10 (excellent), the 62 participants’ overall health was reported as a median of 8/10 (physical) and 7/10 (mental). Anxiety during performance was the most common concern (63%) and was accompanied by a tremor in 55%. The next most popular concerns, with 19% of responses each, were: sleep, insufficient operative skill or expertise, and worry about relationships with trainers. The commonest topics discussed were ‘the inner critic’ (100%), ‘autonomic modulation’ (69%), ‘not working, well’ (13%) and ‘optimising study’ (6%). Seventy-seven per cent were unaware of PEC for practising surgeons. All respondents felt that they would benefit from PEC to some extent (80% ≥8/10 where 10/10 was ‘very useful’), ideally at the ST3 level. Sixty-two percent of respondents said there should be a fee for trainees, whereas 38% thought it should be free and paid for by their training authorities.
Conclusion
The concept of PEC is acceptable to ST3 Urology trainees, with particular interest in techniques to mitigate negative self-talk and autonomic modulation techniques. Existing barriers to coaching for the surgical community would need to be addressed in designing an acceptable coaching programme.
Introduction
Surgical performance is complex and demanding, and directly impacts patient outcomes. 1 Team and system factors play a significant role but, at an individual level, performance comprises technical skill, experience, and the physiology, mindset and judgement of the surgeon wielding them. 2 Surgeons must sustain their attention and focus for prolonged periods of time. In addition, they need to be able to self-regulate under stress to optimise their ability to think clearly and physically perform at the highest level. 2 Outside the operating theatre, keeping up with administrative and academic expectations is also required. Alongside these performance and productivity demands, it is important to maintain a good quality of life, health and relationships. 3 This can be challenging, as demonstrated by the high rate of dropout and burnout in surgical training. 3
Coaching is an established tool for supporting personal and professional growth in arenas such as professional sport. 4 Atul Gawande proposed coaching for surgeons in a 2011 New Yorker article, arguing that, like athletes, surgeons rely on intricate bodily motions to do their tasks. 5 The GMC deems coaching ‘essential to supporting and developing good practice’, 6 and surgical coaching has demonstrated encouraging results in improving surgeons’ technical skill and wellbeing. 7 However, the uptake by the surgical community remains low, slow and inconsistent. 8 Unlike elite sports coaching programmes, which consider the whole athlete, including their physiology and psychology, surgical coaching has mainly focused on technical skill acquisition and refinement, in isolation. 7
The aim of this study was to assess the feasibility of surgical performance coaching for newly appointed Urology registrars (ST3s). The objectives were to:
Gauge whether the concept appealed; Assess which areas beyond technical skills acquisition were felt to be most relevant or useful to this group of surgical trainees; Establish how to make coaching most accessible to them.
Subjects and methods
The ethics approval was deemed unnecessary by the St James's University Hospital Research and Ethics Committee because no patients, or patient data, were involved. Written consent was obtained for inclusion in the study.
All delegates on the Urology Boot Camp 2023, an annual in-person five-day course for newly appointed Urology registrars, subsidised by Health Education England (HEE) were invited to take part in an online survey (Google Forms) before and after a two-hour performance coaching workshop. The workshop was delivered by a Surgeon (LC) with a professional coaching qualification (Co-Active Training Institute), accredited by the International Coaching Federation, to groups of four delegates at a time over four days.
The pre-session survey collected demographic data, participants’ current perceptions of their overall physical and mental health (where 1 was ‘poor’ and 10 was ‘excellent’), areas known to affect performance (where 1 ‘was not optimized at all’ and 10 ‘couldn’t be better’, Table 2), and their individual performance challenges, in free text. Where more than one issue was suggested, they were considered separately. Their answers were themed and coded into broad areas using thematic analysis. 9 Participants were asked whether they had an operative tremor and, if so, what affected it; whether they had ever heard of performance coaching for surgeons, and how useful they thought it would be (on a scale where 1 was ‘not at all useful’ to 10 ‘very useful’).
Ten areas understood to support individual performance and productivity outside technical skills acquisition were presented to the participants as potential content for the workshop via an introductory Canva presentation, designed and pre-populated by LC (Table 1).
Presented areas for performance coaching, excluding technical skills acquisition.
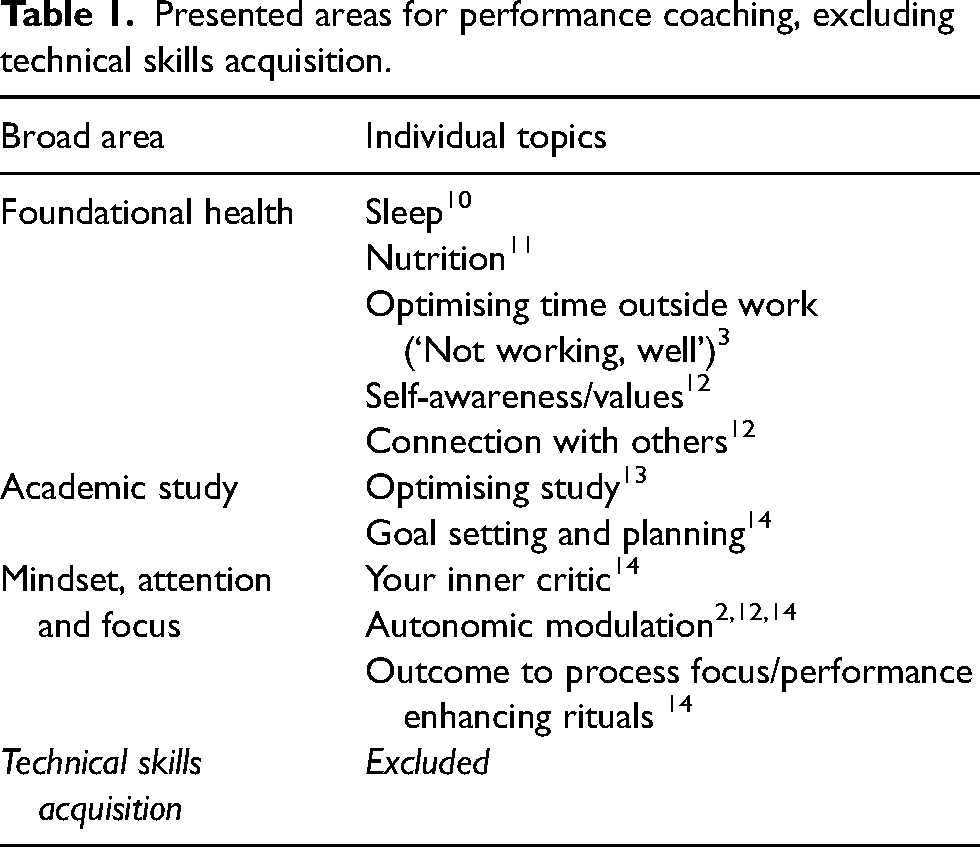
A customised lecture of up to two of these topics chosen by the group of four participants was then constructed, using Canva, lasting 60 min in total and delivered by LC. Further discussion or freestyle coaching was then offered for 30 min.
The survey immediately post-session gathered the perceived importance of the following aspects to include in performance coaching for surgeons: sleep, nutrition, exercise, mindset management, mindfulness training, developing skills around the impact on others, personal growth and development, developing focus, autonomic control, goal setting and motivation, processing emotion and learning to manage rumination. Information about the optimal delivery of performance coaching to surgeons was gathered: in-person vs. remote, one-to-one or in a group, and potential costs. Finally, what the participants liked in the session, how it might be improved or anything that they did not like. At the end of the bootcamp, the utility of all individual sessions/workshops was rated as follows: I found […] session useful, with a scale from 1 (‘strongly disagree’) to 5 (‘strongly agree’).
Medians (and interquartile ranges) or means (and ranges) are reported. All results are given to one decimal place, and cardinal numbers are rounded up or down.
Results
Sixty-four newly appointed registrars to the UK Urology national bootcamp training programme took part in the workshop (100% of bootcamp delegates); 77% were male. 56% were aged 30–34, 36% 25–29 and 8% 35–59 years old. Pre-session surveys were completed by all 64, and 62 gave consent for inclusion in the dataset.
The 62 participants rated their overall physical health at median 8 (IQR 6.3–9) and mental health at median 7 (IQR 6–8) on a scale of 1–10 where 1 is poor and 10 is excellent. 26% (n = 16) of respondents routinely use a health-tracking device to track sleep, movement, etc.
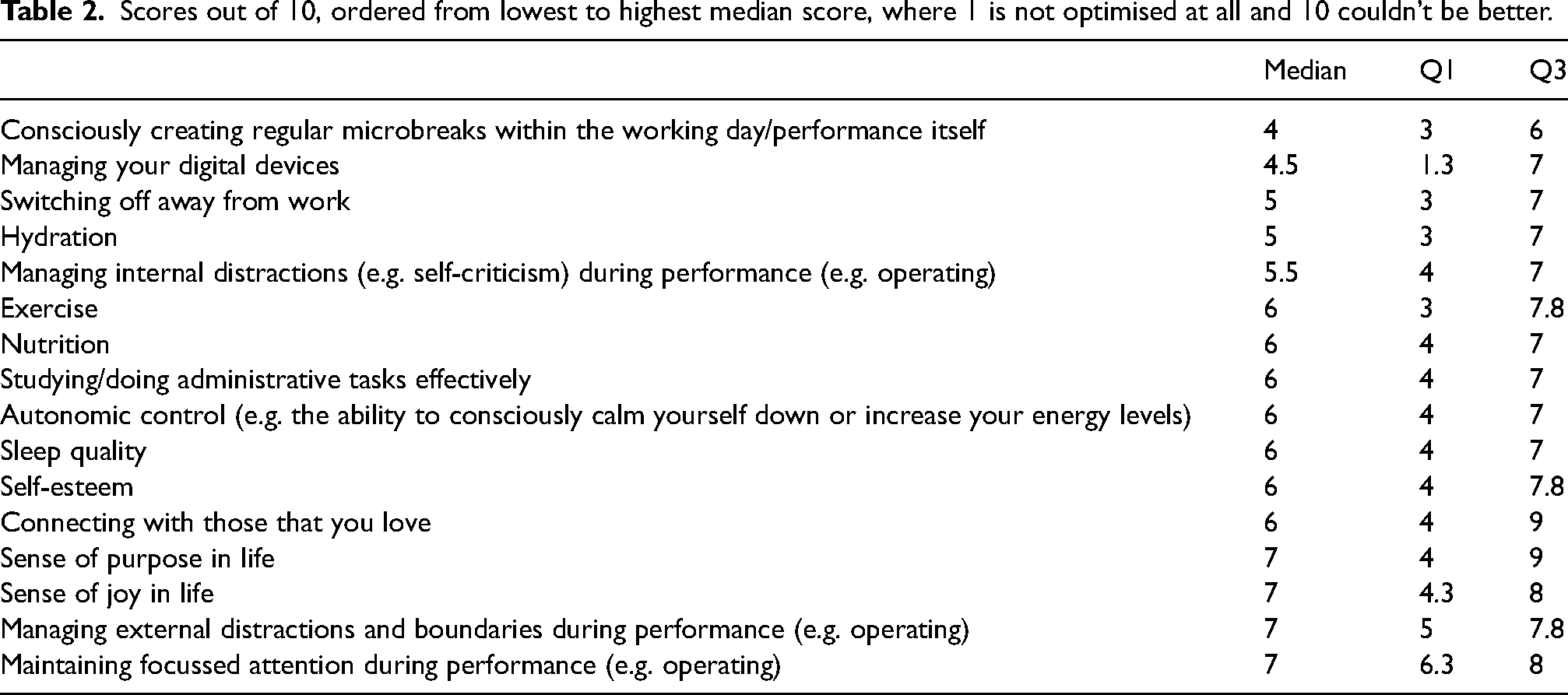
Table 2 outlines the weakest to strongest areas affecting performance, for the participants.
Scores out of 10, ordered from lowest to highest median score, where 1 is not optimised at all and 10 couldn’t be better.
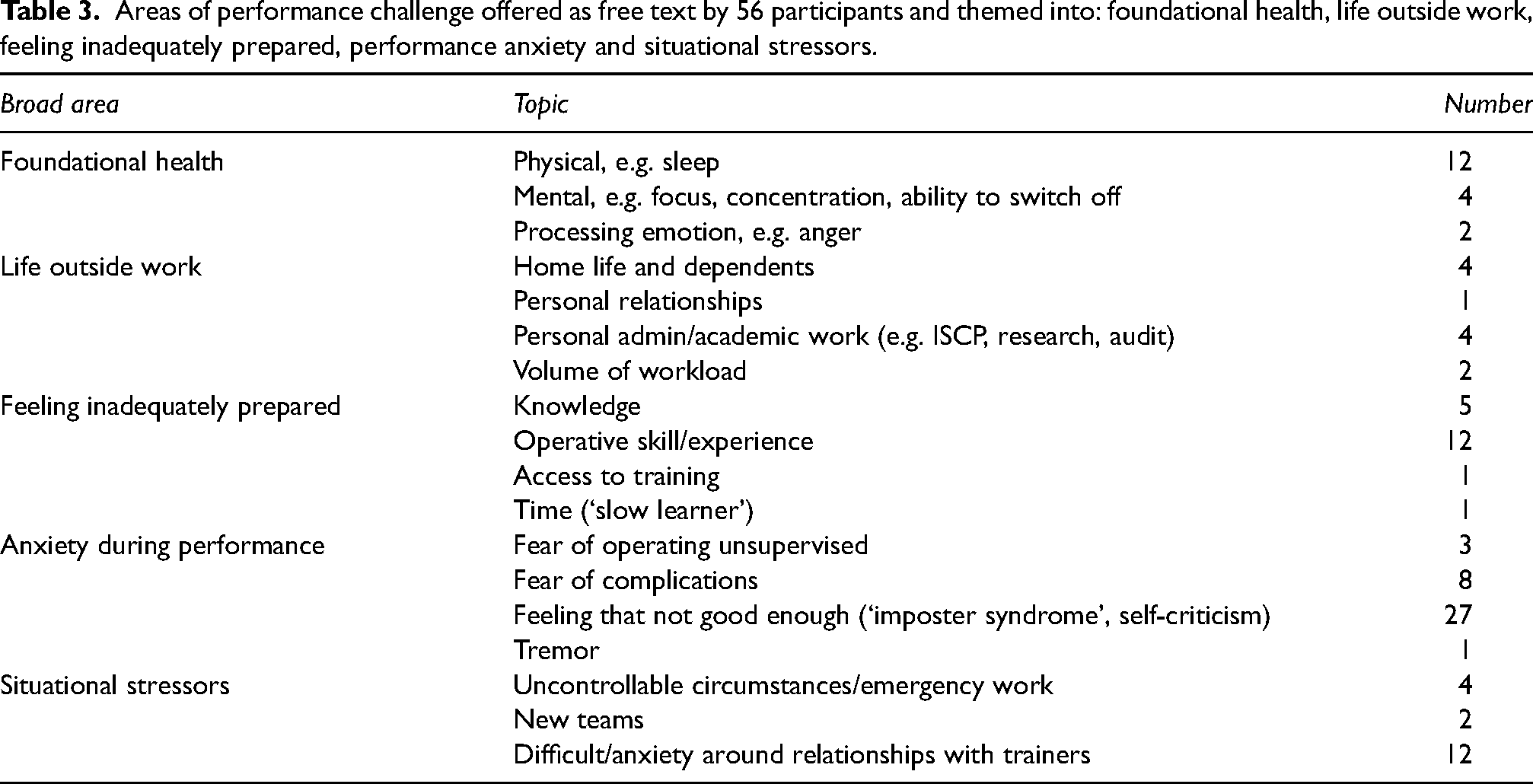
Approximately 90% (n = 56) of respondents offered free text current performance concerns, some giving multiple areas (Table 3). Of these, 63% described anxiety during performance: fear of operating unsupervised, fear of complications, not feeling good enough or a troublesome tremor. Issues around foundational health such as sleep, inadequate operative skill or experience and anxiety around relationships with trainers were the next commonest concerns, at 19% of respondents each.
Areas of performance challenge offered as free text by 56 participants and themed into: foundational health, life outside work, feeling inadequately prepared, performance anxiety and situational stressors.
Some degree of tremor during performance was experienced by 55%, ranging from 2 to 8/10 in severity, where 1 = ‘I don’t have a tremor’ and 10 = ‘interferes with my ability to operate’.
The majority (77%) were relatively mild (≤3/10). Anxiety due to being observed was the most common cause for tremors (40%, n = 25), then caffeine (32%, n = 20), anxiety due to the perceived importance of the procedure (31%, n = 19), physical tension/ergonomics (26%, n = 16), lack of sleep (21%, n = 13), physical exertion (15%, n = 9), diet/blood sugar (6%, n = 4) and drinking alcohol the night before (5%, n = 3). One person routinely used beta-blockers to manage their tremor pre-emptively.
The lecture areas chosen during the sessions after presenting the options in Table 1 and discussion within themselves as a group of four were: ‘the inner critic’ in 100%, ‘autonomic modulation’ in 69%, ‘not working, well’ in 13% and ‘optimising study’ in 6%.
Of the 62 respondents, 77% (n = 48) had never heard of performance enhancement coaching for practising surgeons, 16% (n = 10) had, and the rest were unsure. Before the session started, all respondents felt that performance coaching would be useful to them to some degree, 80% ≥8/10 where 10/10 was ‘very useful’ (Figure 1).
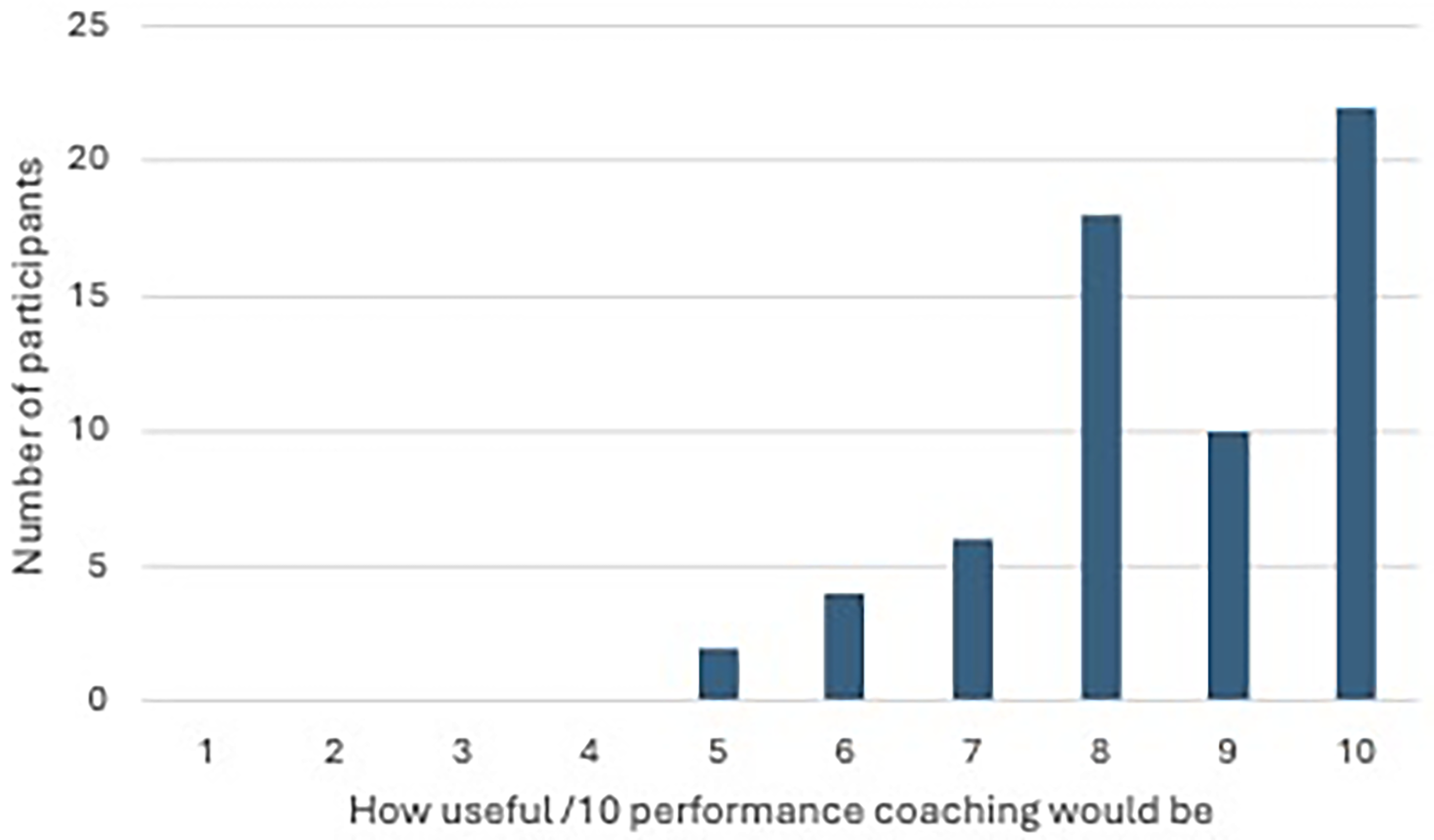
How useful trainees felt that performance coaching would be, where 1/10 was not useful at all and 10/10 was very useful.
With regard to the timing of the session, 86% felt that the most useful time to provide coaching was at ST3, but other suggested opportunities were at ST5, peri-exam and as a new consultant. In providing performance coaching, 47% preferred one-to-one, 41% small group and 6% a blend of both. 27% felt that it should be face-to-face rather than remote.
Within a performance coaching programme, the topics that individuals felt most important to focus on are represented, in Box 1.
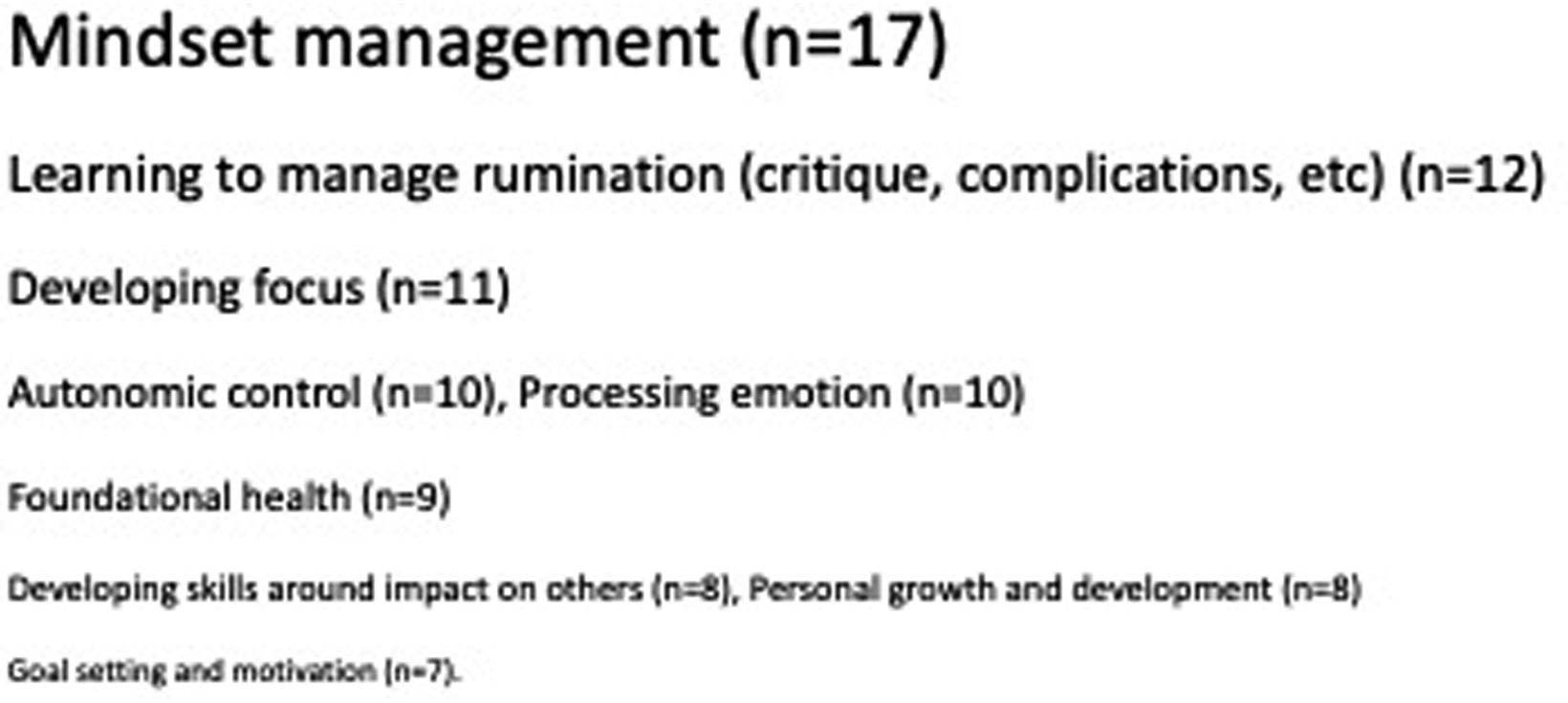
The topics considered most important to cover in a performance coaching programme. The number of participants voting for the topic being the most important is represented by the relative font size in the figure. Individuals were able to select more than one option for the top position.
Twenty-four participants shared a view on the cost of performance coaching; 62% (n = 15) thought that there should be a cost to trainees, while 38% (n = 9) felt that it should be free to trainees and paid for by their training bodies (the Deanery or HEE). Amounts charged for performance training varied from <£100 (n = 3), to £100-£200 (n = 4), to £500-£1000 (n = 2) or ‘a lot’, ‘as much as it needs’, ‘affordable’, ‘It's invaluable’, ‘nothing should be free for trainees’, ‘it's difficult to put a number, but can impact relationship with coach if expensive’.
In the post-bootcamp feedback, the performance enhancement session was given an average score of 4.7/5 (range 2–5).
Discussion
Surgeons are performance professionals. Like high-level sportspeople and professional musicians, they must consistently technically and cognitively perform, despite significant stressors. 2 Their ability to do this plays a critical role in patient outcomes.1–3 Multiple factors interweave around human performance, with individual, team, system and institutional strands. 2 Focusing on the individual components is only a piece of the pie 15 but, unlike others, is directly within the individual's control.
A key individual component of performance is the ability to manage stress. Experiencing excessive or chronic stress has physical, cognitive and emotional effects known to be detrimental to attention, decision-making, knowledge recall, communication, technical ability, to affect patient care and to potentially lead to burnout.2,3,15,16 Burnout, which increases the risk of surgical errors by two and a half times, affects 40% of surgeons, who are at particular risk earlier on in surgical training. 17 Junior surgeons are less adept than senior surgeons at recognising the signs of stress and dysregulation and calming themselves down in acute settings. 2 Surgeons usually develop the ability to handle stress through trial and error, with consequently inconsistent and, sometimes, dysfunctional results.2,14,18
Confusingly, many surgeons enjoy stress and predictable, moderate and short-lived physiological arousal provides the optimum conditions for performance and flow.2,15 The recognition and skilful management of autonomic states is taught in aviation, the military and professional sport, and includes self-awareness around individual cognitive, emotional and physical signs of stress, techniques to modify these responses to maintain technical and cognitive skills during times of tension, and actively increasing stress tolerance thresholds.2,18 This allows the interruption of stress so that it does not become chronic, the skill set to conserve energy through remaining in less aroused states when higher energy, stressed states are not required or impair function and the ability to harness acute stress to support performance. 18 Coaching and training in psychological and physiological stress modulation, and foundational health parameters affecting stress resilience, such as sleep 10 can, therefore, be considered a spectrum connecting resilience to performance enhancement (Figure 2).

Resilience and performance coaching can be considered two ends of the same spectrum.
While performance coaching is well established elsewhere, 4 only 16% of participants had heard of performance coaching for surgeons. Surgical performance coaching programmes do exist however and have been associated with improved technical surgical performance, high learner satisfaction, positive subjective changes to teamwork and communication skills, situational awareness and wellbeing.7,19 Despite this, cultural barriers prevail, and uptake is low, slow and inconsistent: 15 ‘Most of us wouldn’t think of it, or might think it's a bit of a “namby pamby” thing to do’. 20 Coaching can conflict with surgeons’ identity as a competent professional, and there is concern that they may appear vulnerable or incompetent. 8 ‘You’re a trained surgeon. You should know by that point what to do’. 20 Further barriers to coaching uptake may be practical (such as working around a surgical rota), financial or related to a lack of perceived utility.7,8 Further, programmes that do exist focus on technical skills acquisition (goal setting, intra-operative observation, debrief and deliberate practice), as opposed to physiological and psychological techniques around stress management and foundational health,7,19 despite recommendations to the contrary. 7 So what is coaching, and does it have a role for surgeons?
Coaching optimises individual personal and professional potential through increased self-awareness, self-management and self-efficacy. It differs from counselling, which is reparative in nature, and is also technically differentiated from training, which is usually highly structured, and seeks specific outcomes designed to increase individual knowledge and skills to a given standard; mentoring, which is a longer-term relationship with someone experienced in the same field; and consulting, which involves telling clients what to do to solve their problems. 21 In surgical training, most informal firm-based tuition tends towards the directive end, particularly early on in training or when learning a new procedure (Figure 3).
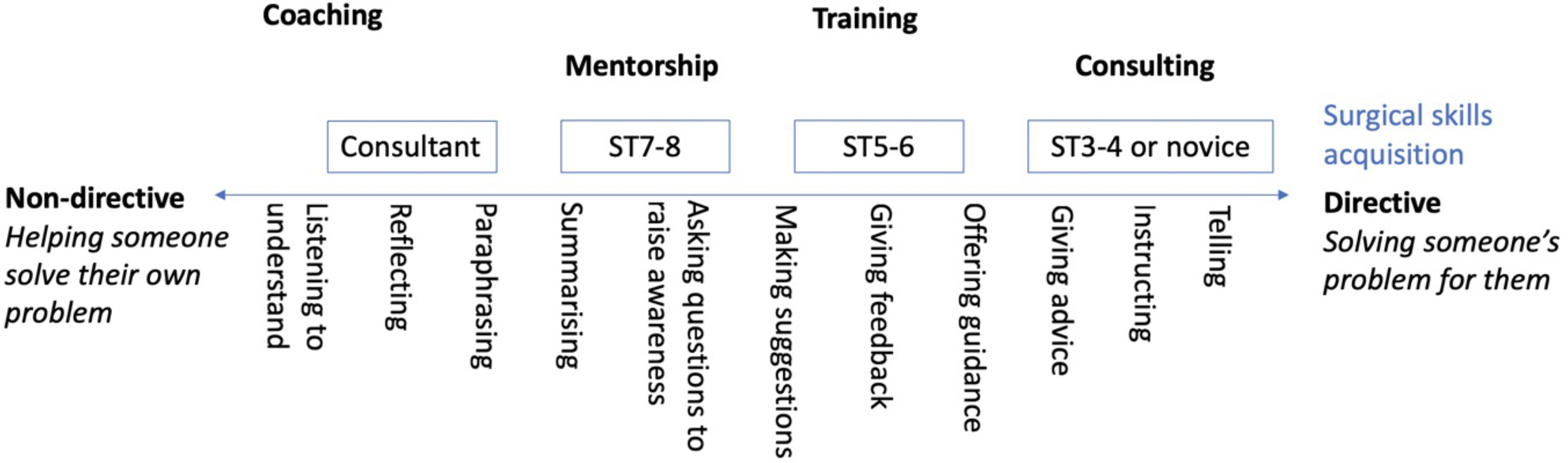
The various types of support overlaid on Downey's spectrum of non-directive to directive coaching. 22 Non-directive or autonomy style coaching, where clients’ perspectives and feelings are considered, and they are given information to make their own decisions tends to cultivate more self-awareness, greater intrinsic motivation and greater performance compared to controlling or directive styles. 21
Surgeons in the initial stages of their training are less adept at self-regulating in high-stress situations and are more likely to experience burnout.14,17,18 We therefore focused on surgical registrars within a month of appointment to assess for the acceptability of coaching as, logically, this would be a good time to head off the problem. But is there a need for coaching in first-year urology registrars and, if so, what are their issues? Overall, their scores for mental and physical health were good (median 7 and 8/10), and only 26% used health-tracking devices. This is lower than the 82% of self-defined athletic people in the UK 23 which may indicate a low engagement with health practices, a lack of engagement with tracking as a technique, or the impracticality of body-worn (ring or wrist based) trackers for surgeons due to clinical restraints on wrist or finger-worn jewellery.
Non-optimised aspects for this group of trainees around performance were: creating microbreaks within the working day, which may relate to losing doctors’ messes in many hospitals, or simply the busyness of their rotas; hydration, a common issue for doctors, 24 potentially secondary to a lack of availability of water sources and cups, or difficulty in drinking when very busy or scrubbed; managing internal distractions (e.g. self-criticism) during performance, a known source of distraction and performance issues, 18 and managing digital devices and switching off away from work. Communicating via messaging platforms on personal phones may be relevant here, rather than the use of pagers or bleeps that could be left at work.
It was encouraging that having a sense of purpose and joy in life was rated relatively highly. Both are protective factors in resilience and a finding that we would traditionally expect with a ‘profession’ like medicine, but this finding contrasts with recent literature around junior doctors’ experiences at work. 3 Also relatively highly optimised were managing external distractions and boundaries and maintaining focused attention during performance, again surprising (in hospitals, doctors are interrupted on average every 11 min 25 ) but encouraging, since distractions increase cognitive load and have been associated with impaired procedural skills. 26 Distractions have also been reported as an issue in the operating theatre, 27 but seem to be less problematic for this cohort. This may be because most operating at this training stage is elective so not interrupted by bleeps, or that in this specialty most referral bleeps go through another team member first. Exercise, nutrition, studying/administrative work, autonomic control, sleep, self-esteem and connection with loved ones all scored a median 6/10 with a large IQR, suggesting a range of experiences.
The commonest issue affecting performance in 63% was anxiety due to not feeling good enough, the fear of operating unsupervised, the fear of complications or a problematic tremor. This is lower than a comparatively reported rate of performance anxiety of 87%, 16 which may be because performance anxiety can affect individuals differently at a trait level, 18 or that the triggers and circumstances differ between these trainees and the cited survey respondents, who were more senior surgeons within a different specialty (Plastic surgery). There was a performance tremor rate of 55%, predominantly mild, and most commonly associated with anxiety due to being watched (40%), and the perceived importance of the procedure (31%), followed by more functional concerns like caffeine or physical tension, which fits with the literature. 28 The next commonest performance concerns, each affecting 19% of participants, were feeling inadequately skilful or experienced operatively, concerns around relationships with trainers, and issues with sleep. Sleep is a known factor affecting performance; 10 indeed fatigue has been compared with inebriation in its effect on judgement and performance in driving. 29
Eighty per cent of this group of surgical registrars felt that performance coaching would be useful to them >8/10 where 10 was ‘very useful’. They also enjoyed the experience, rating the session at an average 4.7/5. One participant rated the session at 2/5, which is important to note: not everyone loves coaching, and who the coach is should always be a choice, to have optimum impact. 30 Overwhelmingly the most popular topic that was chosen was managing ‘the inner critic’. Task-irrelevant thoughts and concerns about failure are known to create distraction and are associated with prefrontal cortical deactivation and performance decline. 18 Second was ‘autonomic modulation’ (69%), ‘not working, well’ (13%) and ‘optimising study’ (6%). It is likely that, at different stages of surgical training, this may differ. For instance, nearer the exam, ‘optimising study’ may be more popular; when trainees have families, ‘not working, well’ may be more pertinent. However, for this group, in designing a surgical performance coaching course at ST3 stage, the aspects participants felt most important to consider were psychological: mindset management, learning to manage rumination, developing focus, processing emotion, developing skills around impact on others, personal growth and development, goal setting and motivation, followed by physiological: autonomic control and foundational health.
Barriers to coaching are various, including cultural, around vulnerability or being seen to ask for help. Because it has been primarily technical skill acquisition based, surgical coaching has traditionally been delivered by a senior or respected peer in the specialty, which creates issues around delivery (coaching has been described as yet another burden to add to busy consultants’ demands 7 ), and also the vulnerability of coachees. 7 While surgically trained, LC is not a urologist, and it was interesting that this was deemed acceptable in the context of delivering non-task-specific coaching or training. This may not only increase the range of trained coaches available, but also the objectivity and associated psychological safety for coachees in appearing vulnerable, with less perceived knock on in terms of reputation within their specialty. It may well, however, matter that she is a surgeon; credibility is known to be an important issue in uptake with coaching. 4 A reframe from resilience training to performance enhancement (Figure 2), getting buy in from leaders in the field, and demonstrating value through improvement in subjective and potentially objective markers may all help here. Separating out specialty-specific skill acquisition from performance coaching more broadly may also facilitate cross-pollination between surgical subspecialties, grades of training and even professional groups, and boost efficiency in delivery across multiple groups, increasing access, both practicality and compatibility with rotas, and affordability.
Further studies are required to assess qualitative and quantitative differences in surgeons’ mindsets, foundational health and performance.7,18 There is also potential to identify the individuals in most need of support due to demographic, trait or situational factors to mitigate early burnout,17,18 or identify and nurture potential for elite surgical performance. The key career stages to deliver coaching, and the relevant aspects to those cohorts need further work, as does the assessment of personal investment of time and money to maximise any understood value in accountability and commitment, as well as enabling access, and establishing the optimum mode of delivery. There was a mixed preference for group vs. face-to face and in-person vs. remote coaching, emphasising the importance of flexibility in accommodating all-comers, concerns and choices. 7 It also opens up the option for hybrid training to keep prices down and to facilitate fitting coaching into surgical rotas. Lack of protected time and scheduling challenges have been reported as implementation barriers previously, which was solved here by it being a week's protected course. 7 Finally, in establishing the minimum professional standards for training for surgical coaching, and ways to monitor the quality of coaching delivery. 4
This study was limited in the generalisability of results by the grade and specialty of the trainees. Trainees of different grades may have different issues, due to stages of training, life outside work and generational norms. Also, we know that there are specialty differences in performance demands as suggested from previous work on burnout. 3 The design and delivery of the coaching was by an individual coach (LC) and therefore may not be reproducible by others. A further area to note is that the individual is part of the whole; concerns have been voiced that providing individual coaching and training around resilience and performance will exacerbate the blame of individuals and excuse the systems and institutions within which they work. 15
Coaching represents a useful tool in continuing professional and personal development for surgeons and may improve patient care. Performance coaching is a broad church and can offer considerably more than simply surgical skills acquisition. The area of performance coaching outside specific surgical skill acquisition is shared by performance professionals across sports, music, the executive world and more, and there are evidence-based techniques which support resilience but also elite performance, if found to be acceptable culturally and feasible practically. We have identified a need for, and interest in, coaching, on mindset management in particular, for first-year Urology trainees. It may be that other aspects become relevant at other stages of surgical training. Using coaches who aren’t practising surgeons for these transferrable aspects of performance could alleviate some of the burden on practising consultants, enabling both delivery and objective professional input. Reframing performance coaching as performance enhancement rather than remedial coaching could be a cultural incentive. It is time not just to clamber up to the baseline, but to exceed it, and to move through surgical coaching to coaching for surgeons.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MR has worked as a consultant/proctor for Teleflex, Procept, Olympus and Intuitive Surgical. Equipment sponsorship and part funding for the boot camp were provided by: NHS England, Karl Storz, Cook Medical, Coloplast, Ethicon, Dantec, OKB Medical (Surgical Science, previously Simbionix), MediPlus, Teleflex, and European Pharma. The authors have no further conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.