
Abstract
Menopausal transition (MT) is often described in medical terms or treated as a private matter, but it also characterises women’s working lives. Drawing on Giddens’ structuration theory, this cross-cultural study explores how institutional and cultural structures influence women’s agency and how women’s everyday practices reproduce and, at times, reshape these structures in the workplace during MT. Based on 51 semi-structured interviews with working women in France, Germany and Türkiye, we explore how women negotiate the experience of menopause in the context of the workplace amidst physical, emotional and cultural challenges. The findings reveal similarities between the contexts: in all three countries, women reported that formal support through workplace policies and healthcare was limited, and even when formal workplace structures were in place, cultural taboos often made it difficult to talk openly about menopause. Women described their MT mostly as positive and described that they sought support through informal networks, e.g. talked to trusted colleagues, adapted their work routines and developed personal coping strategies. Nevertheless, there were nuanced national differences in women’s interpretation of MT: French participants often associated it with loss of femininity, Turkish participants with loss of fertility and German participants with declining productivity, indicating the importance of recognising menopause as both a public and professional issue, as this framing can influence how women experience and shape their working lives.
Introduction
Menopause, clinically defined as the permanent cessation of menstruation and reproductive function (World Health Organization, 2024), typically occurs between the ages of 45 and 55 (Schoenaker et al., 2014). However, in women’s lived experience, menopause is not a single event, but a longer process – known as menopausal transition (MT) – that begins with peri-menopause and continues into post-menopause. In this context, we use the term women for persons which at some point in their life experienced a menstrual cycle, as the menopausal transition ends this process. We acknowledge that some women never experience menstruation or menopause. Their experience is not explored in this study. The menopausal transition involves hormonal changes, bodily symptoms and changing identities that unfold over time, usually beginning with irregular menstruation and often accompanied by physical and emotional symptoms (Talaulikar, 2022).
Although there are medically defined phases, the experience of MT is anything but uniform. Harlow et al. (2012, p. 112) write:
The relatively wide age range (42–58 years) for menopause in [. . .] women seems to indicate that the biological process does not necessarily occur at a uniform pace [. . .]. It varies greatly in terms of the number of years in which each phase occurs.
These years often coincide with complex life demands, particularly for women in the so-called ‘sandwich generation’ who are caring for children and ageing parents at the same time (Waite-Jones & Rodriguez, 2025).
This overlapping of menopause and responsibilities creates pressure that can be felt in particular at work. As a response, many women in the United Kingdom (UK) report that they reduced their working hours or gave up employment altogether due to the difficulties associated with MT (Chartered Institute of Personnel and Development, 2023). Nevertheless, most workplaces continue to reflect the normative ideal of the ideal worker, who is assumed to be masculine, productive, emotionally stable and bodily able (Acker, 1990; Jack et al., 2016). Within this model, symptoms of menopause such as hot flushes, insomnia, anxiety and cognitive fog are difficult to express or process (Maki & Jaff, 2022; Steffan & Potočnik, 2023). Cultural expectations about what is considered relevant and allowed in the work environment reinforce this silence.
In contrast to the UK, where in recent years menopause has received significant attention in the public and political debate (Cowell et al., 2024; Hardy et al., 2019b; Throsby, 2026), France, Germany and Türkiye are only beginning to recognise menopause publicly – mainly through growing media interest, emerging health dialogues and early awareness-raising in the workplace. As the three countries are at different stages of framing the MT as a policy issue, we expect that these cultural and national differences will shape menopause experiences differently (Lock, 1994; Obermeyer & Sievert, 2007). The symptoms of menopause may be similar, but how they are understood, mediated and managed varies depending on the degree of sexism, ageism or ableism that women encounter in their environment (Riach & Jack, 2021).
While initial studies have explored how the MT transition is discussed at work (Rowson et al., 2023) and how menopause-related symptoms affect work (Carter et al., 2025), research has insufficiently explored whether and how variations in a country’s cultural and institutional context substantially change the experience of women during this phase.
To address this gap, we study the impact of institutional and cultural constraints in three national contexts, by adopting Giddens’ structuration theory (1984). Giddens (1984, p. 9) posits that agency is ‘not [about] the intentions people have when they do things, but [about] their ability to do those things at all’. Agency is only possible because social structure provides rules and resources to actors (den Hond et al., 2012). Thus, social structures simultaneously constrain and enable action. Wood et al. (2025) have shown how women draw on these structures – sometimes reinforcing norms, sometimes reshaping them – to sustain agency during MT.
Building on this, in this article we explore how structure shapes the agency of women as they navigate their MT in the workplace and how the enactment of their agency reshapes these structures. To address these questions, we draw on 51 qualitative interviews with women from France, Germany and Türkiye – three countries with differing gender norms, welfare systems and labour market expectations (see Table 1). In Germany, part-time work is common among women, as public childcare remains only partially available. Germany has a high percentage of women participating in the workforce (77%) and a decentralised healthcare system which places more responsibility on employers. However, all working adults are obliged to be insured. A recent study showed that many German women consider reducing hours (26%), changing jobs (16.1%) or retiring early (19.4%) due to menopause-related symptoms (MenoSupport Research Project, 2023). This has triggered policy attention, as the subject of menopause had so far been neglected by policymakers. Moreover, workplaces differ widely regarding whether and what kind of support they provide. In October 2024, Germany’s parliament debated a proposal for a national menopause strategy, aiming to reduce stigma and improve medical and occupational health responses (Deutscher Bundestag, 2025). However, follow-up action has been limited.
Similarities and differences between countries.
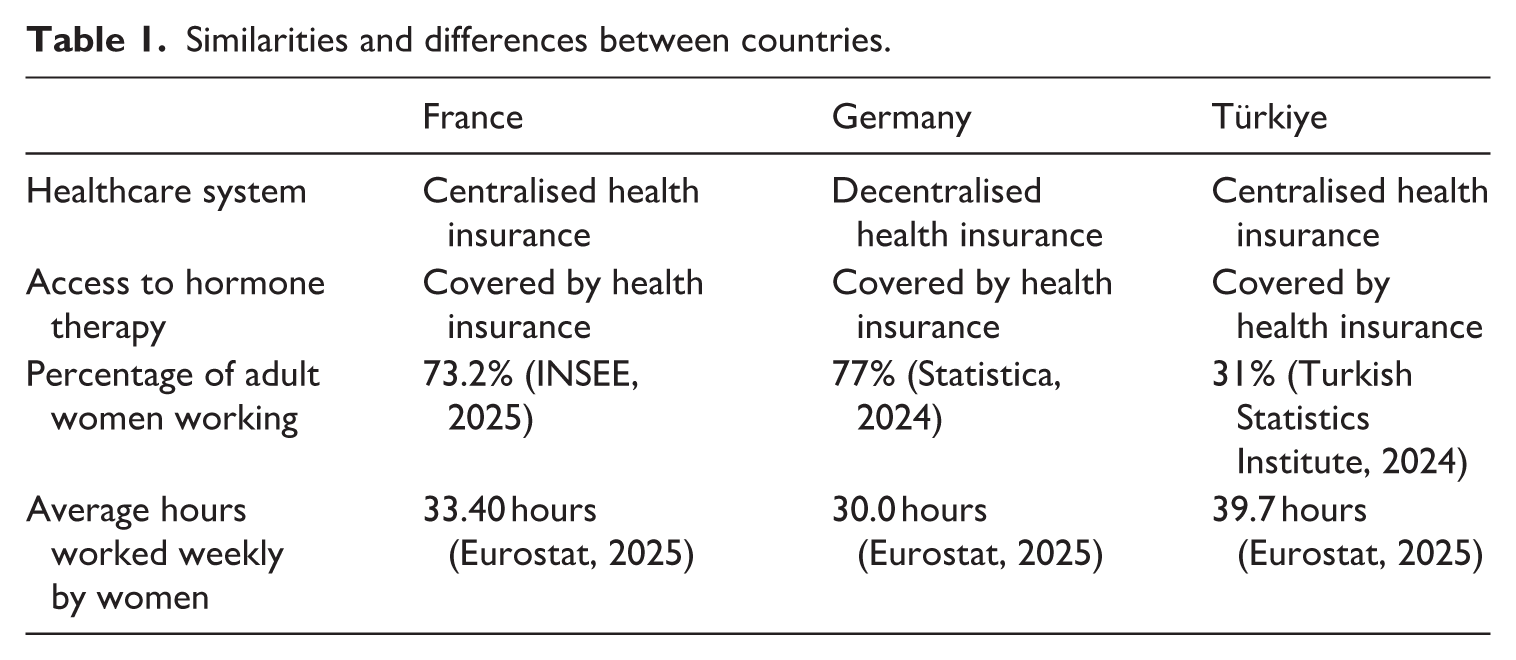
With 73% of women in the workforce, France supports full-time employment through public childcare and a centralised health system; menopause has entered legislative debate but lacks policy follow-up or national study (Ministère de la Santé, 2025). In contrast, Türkiye’s lower female workforce rate (31%) reflects stronger traditional gender norms; menopause is largely absent from public and workplace discourse, with the health system offering only limited self-help guidance with no structural support (Duman et al., 2021; Turkish Ministry of Health, 2023).
Framing menopause as a concurrently private, public and professional experience, and applying Giddens’ structuration theory (1984), our study explores how women interpret and navigate workplace structures – sometimes adapting, sometimes resisting them. Across all three countries, women relied more on informal support, including colleagues, friends and self-developed strategies, than on formal workplace or healthcare systems.
The biomedical model: Defining the clinical body
The biomedical model that dominates medical discourse worldwide defines MT as a series of predictable physiological changes (Rostosky & Travis, 1996), most notably the decline in oestrogen and the cessation of ovarian function. It divides the process into three clinical phases – peri-menopause, menopause and post-menopause (Burger et al., 2008) – to facilitate diagnosis and promote standardised treatments, particularly hormone replacement therapy (Gatenby & Simpson, 2024). Some studies show that women often use biomedical language to describe their experiences (Hyde et al., 2010), such as symptoms, hormones and side effects to describe what they are going through. However, Guillemin (2002) warns against drawing a strict line between official medical discourse and lived experience, as the two are often intertwined.
Nevertheless, the biomedical model has been criticised for portraying middle-aged women as hormonally deficient (Hunter & Rendall, 2007) and for reinforcing what Dillaway (2006, p. 32) calls ‘the equation of women with their reproductive capacities’. This view pathologises a natural life stage and imposes a narrow, universal definition that overlooks diverse experiences (Murtagh & Hepworth, 2003). In contrast, others see menopause as a normal, life-changing transition (Goldstein, 2000), even a meaningful rite of passage that provides space for reflection, autonomy and redefinition (Quental et al., 2023).
A purely medical perspective risks overlooking the social dimensions of menopause, particularly in the workplace, where it is typically treated as a private issue and left out of formal policies and discussions (Verdonk et al., 2022). As a result, symptoms like fatigue or mood swings may be misread as personal issues affecting individual women’s performance (Beck et al., 2018; Laker & Rowson, 2024).
Menopausal transition through the lens of structuration theory
Whether and how a woman’s experience of menopause is perceived and treated depends not only on her own agency (Jack et al., 2019), but crucially also on the cultural and institutional systems that define which experiences count, matter and deserve to be acknowledged and which do not (Williams, 2024). The body going through MT is shaped by both biology and society (Throsby & Roberts, 2024); it is determined by social norms and daily practices within larger structures that define what is acceptable and what support is available.
It is for this reason that Giddens’ structuration theory (1984) seems particularly apt as a lens through which to examine women’s MT experience in the workplace. Structuration theory views all human action as embedded in systems of rules and resources that individuals draw on and reproduce in practice. Giddens (1984, p. 19) writes: ‘One of the main propositions of structuration theory is that the rules and resources drawn upon in the production and reproduction of social action are at the same time the means of reproducing the system (the duality of structure)’. Agency and structure are thus expressed by the fact that people only make decisions that are possible because they have the knowledge and resources to realise them. Knowledge and resources are at the heart of structure, and agency is a free choice among alternatives that are available because of structure. According to Giddens (1984, p. 9), agency ‘refers to events of which an individual is the author, in the sense that the individual could have acted differently at any stage of a particular sequence of behaviour’. Individuals’ action, in this regard, might not only be directed towards shaping everyday practices, but also towards reshaping social structures.
Giddens (1984) goes on to explain that agency involves reflexive monitoring of action, rationalisation and motivation – all of which are shaped by conditions that often remain unrecognised. Applied to MT, women who experience MT in the workplace draw on the knowledge and resources they have acquired, reproducing the structure that enables their agency while exercising agency within the constraints of their structure. In doing so, their everyday practices, such as how they manage symptoms at work or seek support, not only reflect these structures but also contribute to ongoing symptom maintenance and, at times, the incremental reworking of structure by changing how they are collectively perceived and enacted.
This means that women are not simply responding to biological symptoms but are constantly evaluating their actions against the backdrop of social expectations, drawing on both formal knowledge and tacit experience. The routines women adopt, for example, to cope with hot flushes or fatigue, are characterised by what is socially permitted and what is materially supported. Acting against prevailing norms (e.g. modesty norms) requires not only reflexivity but also access to support structures (e.g. colleagues and clients accepting less formal attire, well-aired workplaces). Where there is a lack of individual and structural resources (e.g. social support, physical environment, financial means to make changes), agency is limited – even if a woman knows what could help her.
Agency being limited by resources and knowledge available to women in the MT is particularly evident in the workplace, where amenities such as flexibility or discretion are granted to some and denied to others, reflecting structural inequalities (den Hond et al., 2012). As McPhee (2016) notes, many routines require coordination with others, so a shared understanding of change is crucial. Agency, then, is not just individual autonomy, but an interaction with structures that privilege certain experiences and render others invisible. It is precisely these structures that can reinforce gendered hierarchies (Walby, 1989). Adapting to MT is, therefore, not just a matter of personal resilience (Steffan & Potočnik, 2025) but a negotiation characterised by the recursive relationship between action, knowledge and institutional support.
Methodology
This study uses a qualitative approach drawing on semi-structured interviews to develop a deeper understanding of how women in France, Germany and Türkiye manage MT in the context of their professional lives and vis-a-vis work structures. Semi-structured interviews were designed to cover various aspects of the MT, e.g. which symptoms women encountered, how they affected work, which coping mechanisms and treatments were explored and which were effective. During the interview, we ensured that participants could add any other aspect they considered relevant. Participants were asked to share their personal menopause-related experiences of health, work and life transitions, with the interviewers paying attention to how the women framed, interpreted and made sense of these experiences. We aimed at understanding how structure shapes the agency of women as they navigate their MT in the workplace and how the enactment of their agency reshapes these structures.
Sample and data collection
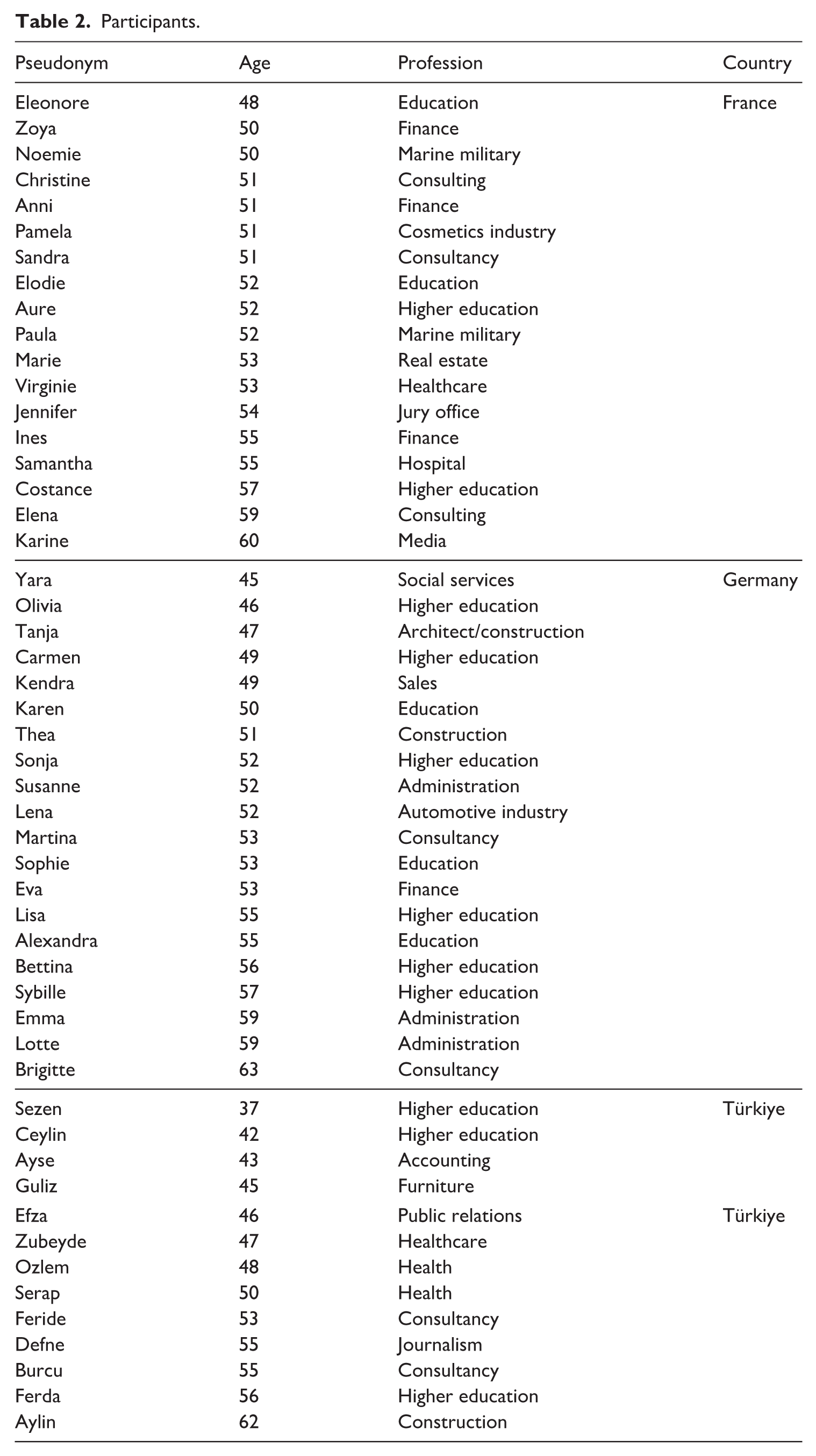
When selecting interviewees, care was taken to ensure that they were diverse in terms of age, occupation, menopause phase and socio-cultural background (see Table 2), aiming for a maximum variation of perspectives including some respondents who experienced their MT early (Mays & Pope, 1995). Recruitment included a wide range of white-collar professions representing different types of employers (e.g. various industries and different sizes of employer organisation), and working conditions (e.g. part-time vs full-time). All participants were experiencing their MT or had experienced it. Furthermore, all participants were highly educated. These sampling criteria take into consideration that education and work environment influence women’s quality of life during MT (Theis et al., 2023), reflecting access to resources. As a result of this sampling strategy, participants’ prior knowledge and experience of menopause varied widely, from women who had extensive health knowledge and were in control of their symptoms to women who were uncertain about MT or only recognised their symptoms after significant professional or personal disruption.
Participants.
In the first phase, we recruited participants via personal networks and employed a snowball system. We asked our personal connections whether they were at any stage of MT and were experiencing any menopause-related symptoms, and whether they would be willing to be interviewed. After the interviews, we asked them whether they would be interested in referring us to another potential participant. In the second phase, we published calls for participation in the alumni newsletters of our research institutions, which reach a large number of women in the relevant education and age group. Once women agreed to be interviewed, we conducted interviews using Microsoft Teams and Zoom video conference tools, which permitted the recording of interviews and facilitated transcription. Each automatically created transcript was carefully checked referring back to the recording shortly after the interviews ended to ensure their accuracy and completeness. After approximately half of the interviews in each country were completed, the researchers began discussing themes in the data and continued conducting further interviews until a consensus on data saturation was reached (Saunders et al., 2018). Recruitment ended when data saturation was reached, i.e. when no new topics were identified during the interviews.
Four experienced researchers conducted 51 online interviews with women in employment between July 2024 and February 2025: 18 in France, 20 in Germany and 13 in Türkiye in French, German, Turkish or English depending on the participants’ preferences. This included some women with double nationalities or migrant experience, although most women have lived most of their lives in the country in which they were interviewed. The interviews were designed to encourage open, reflective dialogue. Aware of the stigma surrounding menopause (Whiley et al., 2023), the researchers approached participants with empathy and encouraged them to speak freely. This included some interviews where interviewers shared personal experiences of MT. Shared experiences helped to build trust, which allowed participants to disclose previously private issues of women’s health. The study received ethics approval from Rennes School of Business (France), followed institutional guidelines, and ensured voluntary, confidential participation with informed consent for audio recording and data use. Across the three contexts, differences in welfare arrangements, labour-market norms and public discussion of how MT is spoken about, supported and managed at work were identified. This comparison brings out both common patterns and context-specific differences, while variations in the depth of national material may reflect both real differences and the visibility of MT in each setting.
In order to gain insight into the participants’ personal views and experiences with MT in relation to their work, the interview guide was designed as follows. Following initial questions on socio-demographic and work-related information, interviewees were asked how they became aware of the physical or emotional changes they have been experiencing in the context of their MT, what symptoms they experienced, how these affected their work, and what coping strategies they used. Subsequent questions focused on institutional and social support (or lack thereof), medical care, stigma and facilitators and barriers in the professional context.
Data analysis
The interview data were transcribed verbatim and repeatedly checked by critical reading in the initial phase of the analysis. The transcripts of the three countries were each coded independently by at least two researchers who were fluent in the language of the interviews. Where necessary, English translations were used for French, German or Turkish transcripts during the analysis and writing process.
Although conventional categories such as nationality, age and profession offered contextual relevance, they did not explain the nuanced diversity of women’s MT experiences. Participants instead described a dynamic interplay of occupational demands, familial roles, cultural norms, physiological changes and personal perspectives. Certain patterns recurred – for example, whether menopause was seen as decline or transformation often depended on the availability of support and the individual’s perceived agency (Süss et al., 2021). This corroborates current literature that stresses that MT has to be understood as a socially situated process shaped by knowledge, coping strategies and the institutional and cultural environment (Orgad & Rottenberg, 2024). These insights align with our theoretical aim of exploring how individual meaning-making intersects with structural constraints, especially through routinised practices (Giddens, 1984).
Methodologically, the initial familiarisation with the data, as well as the proposed theoretical framework of Giddens’ structuration theory, led the research team to apply the approach of thematic analysis (Braun & Clarke, 2006). Thematic analysis is theoretically open and ‘through its theoretical freedom, [it] provides a flexible and useful research tool, which can potentially provide a rich and detailed, yet complex account of data’ (Braun & Clarke, 2006, p. 78). Thematic analysis lends itself to a variety of research questions and allows capturing the complexity of women’s experiences of MT in the workplace, informed by Giddens’ theoretical framework.
Accordingly, data were analysed in six phases (Braun & Clarke, 2006). The analysis began with familiarisation (phase 1), followed by initial coding (phase 2) and theme identification (phase 3). In phase 4, we refined the inductively generated themes and integrated Giddens’ structuration theory into the analysis. Phase 5 involved defining and naming themes through a more systematic application of this framework, while remaining open to disagreement and adaptation. In phase 6, we finalised the findings through writing, reflection and revision. Next, we present findings that reflect how the MT experiences described by participants are affected by structures at the societal, organisational and individual level.
Findings
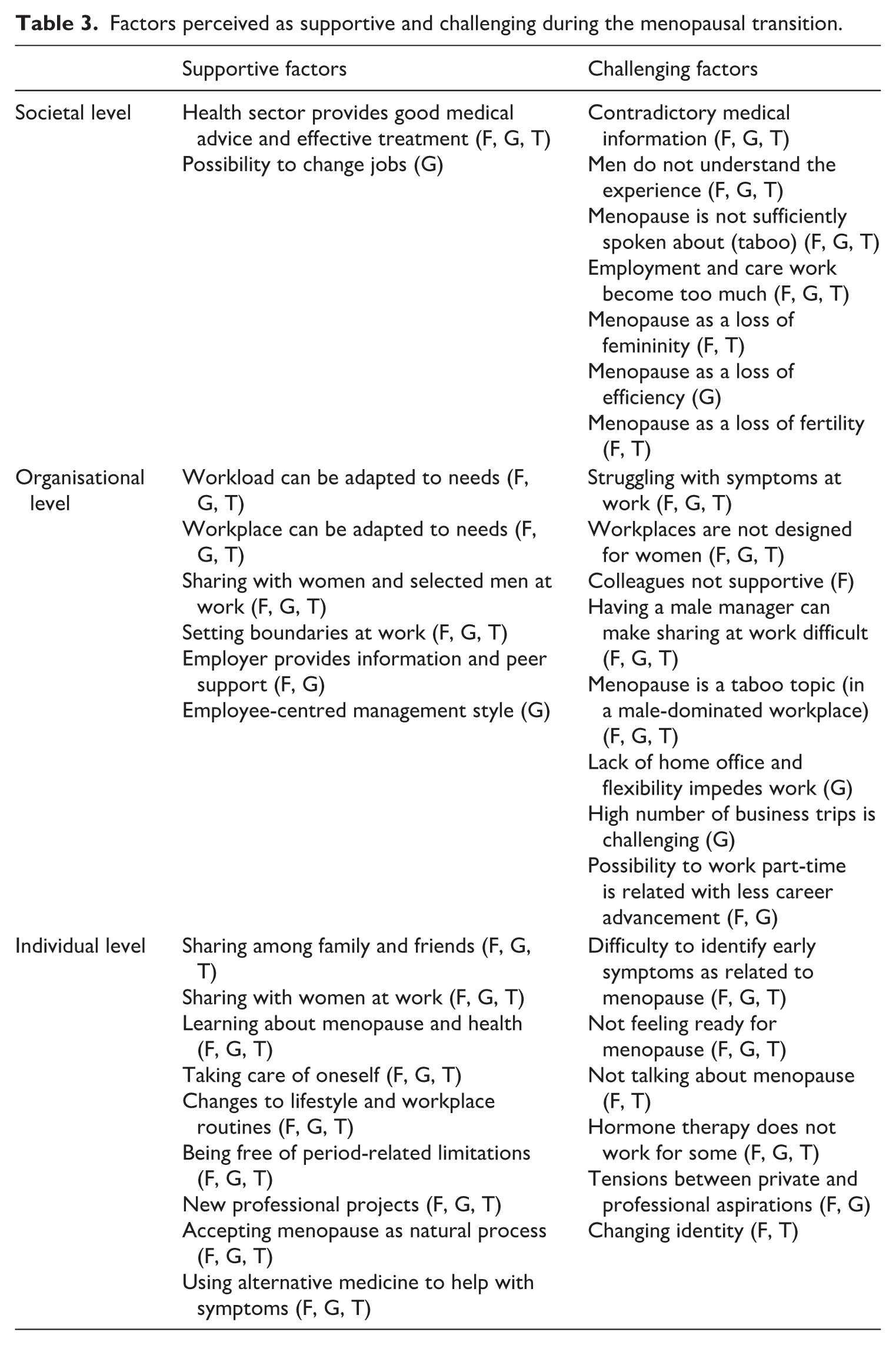
Although the national contexts of France, Germany and Türkiye have their differences (see Table 1) our participants reported remarkably similar experiences when it comes to coping with their MT at the workplace, facing structures enacted at societal, organisational and individual level. Table 3 provides an overview of the factors described as supportive or challenging at these three levels. The table also indicates the countries in which these factors were observed.
Factors perceived as supportive and challenging during the menopausal transition.
Societal level: Medical support, cultural frames, taboo and ignorance
The social structure manifests itself in the institutions that people create, enact and constantly reproduce (Giddens, 1984). In our study, formal healthcare institutions and those that provide health-related information were discussed as sources of support and challenge. In addition, cultural institutions such as the taboo surrounding menopause, nature of information outlets and cultural narratives about menopause shape the environment in which women navigate their MT.
Healthcare system as a source of support and frustration
At a societal level, receiving relevant and helpful advice from doctors and other healthcare providers on how to effectively manage menopause-related symptoms was seen by study participants as crucial to managing MT. Some women described their experiences with the healthcare system as positive, as they have access to appropriate counselling and effective treatment plans that help them use their agency to improve their quality of life. However, for some, their experiences with healthcare services caused them further frustration as treatments prescribed were ineffective or recommendations were confusing. For instance, while Bettina (Germany) shares that starting hormone replacement therapy very early has helped her ‘manage it pretty well before. . . nasty side effects’ occurred. For Martina (Germany), switching doctors worked better:
[T]he [first gynaecologist] looked at my blood values and said everything was okay. . . then it’s been months, when you realize you’re not okay. . . [then]. . . we went to the other gynaecologist, and she prescribed me hormone preparations. And what I’m already noticing is that I’m sleeping better again. (Martina, Germany)
The needs of women going through MT vary, therefore responsive care is crucial. Yet participants often described receiving unclear and/or conflicting advice from health professionals (e.g. hormones do or do not cause cancer), adding confusion to an already challenging time. While healthcare professionals often stress that MT varies, many women in our study expressed a wish for clearer guidance and more consistent treatment, pointing to a gap between medical uncertainty and women’s need for reliable support. Echoing a similar point, Zubeyde (Türkiye) shared how she felt unsupported by some of her doctors with the decision on how to address her menopause-related symptoms:
This woman doctor. . . said, ‘I went through this at your age too. Here’s how it was for me. This is how it is now. So, we’re going to do this.’ Whereas with others – especially male doctors – they just say, ‘These are our options: this, this. . . and that. . . which one makes sense to you? You’ll have to decide.’ (Zubeyde, Türkiye)
Zubeyde points here to another challenge more frequently described by women in Türkiye than France and Germany: her experience that male doctors sometimes find it difficult to understand how women experience MT. This challenge is exacerbated by the taboo nature of menopause even in medical contexts, which makes open discussion more difficult and limits how clearly these experiences are recognised in medical consultations.
Taboos around menopause
In all three countries, women describe menopause as a taboo topic – especially in France and Türkiye, where many participants felt unprepared for it, as they felt they lacked an in-depth understanding. The high visibility of menopause as a public topic and commodity, as described by literature about the UK (Orgad, 2026; Orgad et al., 2026; Throsby, 2026), is not reflected in the interviews of this study. For the women we interviewed in France, Germany and Türkiye, taboos around menopause significantly limit their agency because relevant knowledge is not shared, and consequently support cannot be sought or provided without transgressing a taboo. Still, some participants reported that they do talk informally with trusted colleagues or female friends, particularly in the German sample. Emphasising this cultural silence in France, Ines states that ‘women. . . didn’t dare to talk about it. . . in our culture. . . it is perceived as a limit and an end’. The same sentiment echoed in the experiences of the participants from Türkiye. Ferda (Türkiye) states that ‘menopause. . . is a closed-off topic, really closed. . . still very much a taboo’ and she highlights the following: ‘Even in the family I grew up in, this wasn’t something openly talked about.’ The taboo around menopause is so strong in families that even women who have gone through their own menopause experience do not discuss it with each other. For instance, not being able to learn from their mothers is mentioned by several women as a problem (Ceylin, Türkiye; Elodie, France).
In all three countries, the women described that men are not aware of the importance of the issue for women, that they trivialise or misunderstand the experience, regardless of position – be it as a ‘partner’ (Kendra, Germany), ‘brother’ (Zoya, France), ‘colleague’ (Ayse, Türkiye), ‘manager’ (Ceylin, Türkiye) or ‘doctor’ (Zubeyde, Türkiye). For instance, when Kendra (Germany) decided to sleep in a separate room to manage her insomnia, her husband found it initially difficult to accept the change: ‘I’ve gotten some incomprehension [from the husband] when I’ve moved, but I think he’s come to terms with it.’ Overall, therefore, the widespread taboo around menopause leaves many women unprepared for its challenges and cuts them off from social, emotional and medical support that could ease their MT transition.
These challenges could be eased with better public information on symptoms, treatment options and coping strategies. As noted, the availability of state-provided information on menopause varies across the three countries (see Table 1). Many women struggle to find reliable information on MT. While there have been more public initiatives in France and Germany than Türkiye, all three countries still lack adequate support and accessible resources. This becomes evident in Karine’s (France) statement: ‘To be honest, there isn’t much research out there on menopause – or if there is, it’s definitely not something people. . . share widely.’ Compared with France and Germany, none of the women in Türkiye mentioned access to state-level provided information.
In all three countries, women sought information about menopause in a variety of sources – online (Paula, France), in books (Ozlem, Türkiye) and podcasts (Anni, France). However, these sources differ in quality depending on the expertise of their authors, who ranged from leading researchers to women going through menopause sharing their stories. Thus, the information women find often lacks clarity and consistency, adding to confusion. In the absence of accessible support structures within national structures that provide reliable information on menopause, women continued to depend on their effortful individual research, including self-help literature, which reinforces its own biases in imagining MT (Throsby, 2026). As a result, agency is focused on learning before women can experiment with potential remedies and coping strategies.
While women in all contexts had similar embodied experiences of MT, the cultural framework shaped the way they processed the experience and expressed their feelings of loss in significant ways. In France, menopause was often seen as loss of femininity, while in Türkiye it was associated more closely with fertility. As Marie (France) says:
Menopause is loss of femininity. For some women, menopause can be an identity shock. It’s not just about not having kids anymore – it’s like your femininity takes a hit. You’re no longer seen as sharp. . . desirable, as if menopause makes you fade into the background. (Marie, France)
In the French public discourse, women going through MT are framed as less feminine and attractive and appear to become less visible in society. In Türkiye, Ceylin reflects on how social expectations of fertility are internalised by the women in her community, stating, ‘I felt as if something that made me a woman – not fertility itself, but something connected to it – had been taken away from me. . . my mother-in-law has a saying that came to mind: “You become half a woman.”’ In Türkiye, women in the stages of MT are no longer framed as full participants in social life, as ability to reproduce is lost – which is closely linked to a woman’s identity as a mother that gives them social status in society. German participants also associated that phase of their life with loss, but more in terms of their ability to do the things they want to do: thus a loss of energy. Martina describes her struggles with this loss of productivity as follows:
I used to live in a sprint, and I can’t do that anymore. I just don’t have the strength and energy anymore and I have to switch to marathon mode, which is extremely difficult. . . I need many, many more breaks to regenerate, and it’s just difficult to incorporate. . . (Martina, Germany)
Although the women in France and Türkiye also mention exhaustion, the German participants described the menopause more as a loss of everyday and professional performance, i.e. less as a physical problem than as a decline in productivity. Arguably, the loss of femininity, fertility and productivity each affects agency by shaping women’s perception of achievability and what others think they can achieve. Even if the sense of loss varies in intensity from woman to woman, better medical support by the healthcare system could ease the burden for some. However, everywhere persistent taboos continue to limit open dialogue and recognition of women’s needs, both at home, in medical care and in the workplace, and subtly shape professional dynamics.
Organisational level: Breaking workplace silences and facilitating informal support
The idea that structures guide actions but are concurrently shaped through practice (Giddens, 1984) provides a useful lens for understanding how organisational systems evolve over time (Vaara & Whittington, 2012). Organisational arrangements appear to influence how participants experience MT in the workplace. Participants in France, Germany and Türkiye described similar challenges related to symptoms and noted that flexible working arrangements – where available – could mitigate some difficulties. However, such provisions were not consistently accessible and were rarely designed with MT in mind. In contexts where formal support was limited, many women described developing informal strategies, such as peer support and boundary-setting, to more effectively manage their professional environments, restoring some of the agency affected by menopause-related symptoms.
Formal structural support at the workplace
Some women reported adapting their work arrangements, such as remote work, flexible scheduling or shifting meetings. For instance, Sezen (Türkiye), who works in academia, explains: ‘in situations like this, [academia’s] flexibility really works in my favour. . . I manage my own classes, so I can take breaks whenever I need to’. This ability to change one’s own schedule allows one to manage fatigue and stress and to address physical needs in a timely manner. Similarly, Susanne (Germany) shares, ‘Yes, I’m very free in that respect. I can organise my time myself. . . I just take breaks or lie down from time to time’, illustrating the benefits of autonomy in managing the impact of MT on work. Furthermore, part-time working contracts are found in Germany (Sonja) and France (Elena), a choice that usually entails reduced professional advancement, but helps women with MT. Still, German participants also report suffering from work arrangements that cannot be adjusted to their changing needs, e.g. when self-employed work requires lot of business trips or when flexibility of working hours or home office is not given (Martina, Alexandra, Germany). Some, like Sonja (Germany) even consider early retirement as a solution.
Some workplaces organise seminars and workshops to raise awareness of menopause. For instance, in Germany and France, some employers formally provide information about menopause and encourage peer support battling the taboo. Sonja (Germany) mentions an initiative she started ‘on the topic of menopause for women’, while Aure (France) reports the availability of ‘“gender equality working groups” offering some support’. However, such workplace support was reported mostly in the French and German sample, while in Türkiye only one participant (Zubeyde, Türkiye), who works in an international company, reported that such support is available to her.
Although some women benefit from the visibility of MT and the availability of formal support structures in their workplaces, not all women feel comfortable to discuss the subject of menopause, especially in male-dominated workplace settings, as they fear being stigmatised, as stated by Marie (France): ‘I don’t want to be perceived as ageing or less capable. That’s why I handle it in silence and find solutions to stay effective, like taking a short nap in my car during lunch break when I’m too tired.’ Thus, although women can benefit from available support, they may decide against using it because of prevalent taboos that are reinforced by a fear that co-workers and employers might use menopause as an excuse for discriminating against their ageing female colleagues. In this context, even if the intention is to increase visibility, broader social norms may hinder meaningful change.
Workplace silence
Social structures in all three countries appeared to enforce barriers between work and private life. Physical health was mostly framed as belonging to the private sphere, as people who are not well enough to work can take sick leave. Hence, for some women, the combination of MT being framed as private and taboo often results in workplace silence, as Ines (France) observes: ‘No one talks about menopause at work – it’s like there’s just no room for it. Most of the time, managers and co-workers just brush it off as a “personal thing” instead of actually trying to understand or support you.’
Women who described their workplace as male-dominated tended to struggle with this the most: Tanja (Germany), an architect who defines her workplace as ‘somewhat male-dominated’, expressed the following: ‘I do talk about things like that privately with colleagues. But only during the breaks. I don’t actively spread the word about it in the office with everyone.’ The resulting isolation can lead to feelings of invisibility, as Pamela (France) shared, ‘Since no one really brings it up, you end up feeling really alone and invisible.’ Limited public awareness, male ignorance, the absence of open dialogue and a lack of formal workplace support appear to reinforce the social taboo around menopause, which may negatively affect women’s agency, wellbeing and career progression during this stage of life.
Informal support structures and breaking the menopause taboo at the workplace
The lack of formal support plus workplace silence, especially in male-oriented industries, appears to have strengthened informal, supportive interactions among (mostly women) colleagues. Many women share their experiences privately with their colleagues, as expressed by Ceylin (Türkiye): ‘I talked about this with all women colleagues I have close relationships with, but not with my male manager.’ This means that within a general taboo on a societal level and in many workplaces, women in our study engage in an informal exchange about MT experiences with female colleagues. This shows how these women act as (change) agents within their formal structures, because they are willing to break the taboo around MT in their workplace. Whether consciously or unconsciously, they help to reshape the structural environment in which MT is experienced. Some participants even spoke to (mostly female) supervisors, fostering safer, more empathetic workspaces. The informal exchanges also enabled mutual support, such as opening windows during hot flushes (Defne, Türkiye) or taking breaks when tired. Some of these informal efforts end up becoming formal. For example, Lotte (Germany), working in a managerial position, explains how her personal experience informs her employee-centred management style:
In my role as a manager, I sometimes deal with my colleagues and employees who may also be in this situation. . . I encourage them to say: ‘Give me a signal. However, if the meeting is too long for you, if you need a break, whatever.’ I think it is very important for women to get this signal. (Lotte, Germany)
Having said that, it is important to acknowledge that while supportive, such informal, yet secret support still reinforces the continued perception of menopause as a taboo subject in the workplace.
Career progression
The ability to use formal structural support, e.g. using flexible working hours or part-time contracts, coupled with the stigma surrounding menopause while allowing women to continue working without compromising their quality of life, usually comes at a price. For example, as Karine (France) points out: ‘Working at 4/5th was a bit better, but the norm was still that you had to be like a man or accept not having a career.’ However, many participants do not want to accept trade-offs regarding pay and career advancement that come with reducing working hours or physical transformation. For example, Ozlem (Türkiye) explains her reaction to her symptoms:
I really didn’t let it stop me when it wasn’t an actual obstacle. Instead of pausing, I also started a mentorship training. Yes, it was a bit exhausting, my nerves were all over the place. . . But I managed to cope and kept going. (Ozlem, Türkiye)
Some women turn to less visible strategies to preserve their wellbeing. For instance, Samantha (France) explains, ‘Menopause has forced me to ease up a bit – though of course, I’m saying this as someone who has flexible working hours.’ Many women mention taking breaks more consciously (Olivia, Germany) or setting boundaries regarding what should be expected of them (Paula, France). Overall, social structures clearly shape workplace culture, yet formal support for MT remains rare. Part-time work is more common in Germany and France, often limiting career advancement but offering some relief of MT. In Türkiye, formal organisational support is almost absent. Still, across all three countries, women were more likely to create informal ways to cope with MT at work than relying on formal structures.
Individual level: Seeking support, coping and embracing
The societal and organisational level structures have a direct impact on individual routines, what Giddens (1984, p. 90) refers to as practical consciousness, i.e. ‘knowing the rules and the tactics whereby daily social life is constituted and reconstituted across time and space’. Within such structures, women have to find new ways to either keep doing what they already do, or they need to change what they do altogether. For some women this means changing how they work and even what kind of work they do. As previously discussed, in France, Germany and Türkiye, where formal social and organisational structures embedding MT experiences are limited, women take reflexive measures to help themselves, to reinforce agency to understand and manage their menopause symptoms and protect their professional role in their workplaces. In doing so, they appear to give new meaning to this phase of their lives. Interestingly, the women in all three countries described similar adaptive, action-oriented strategies within institutional structures, including the workplace.
Informal support: Sharing of knowledge and resources outside work
In addition to sharing their experiences privately with colleagues, when support from society in general, including family, is lacking, many women turn to their close like-minded friends to discuss their experiences and create informal support networks. For example, for Jennifer (France) it is important to ‘talk about it openly [with] those who are going through the same thing or have already been through it’. For Ayse (Türkiye) sharing makes her feel ‘better’ because, as she expresses ‘then I don’t feel like I’m going through this in isolation’. Women also discuss coping strategies and treatment options in such conversations, as Sonja (Germany) explains, ‘We. . . exchange ideas. So, what helped you, what helped you?’ Without seeking medical treatment or in addition to it, sharing their unique experiences of MT with others helps women in dealing with their symptoms or emotions like feeling loneliness when going through this transition.
Coping strategies
We observed that women express their agency by creating and employing coping strategies. As Giddens (1984, p. 60) writes, such changes reflect both ‘the personality of the agent’ and ‘the institutions of society, which are such only through their continued reproduction’. Some women managed symptoms (e.g. hot flushes, fatigue) by changing their attitude or through practices such as yoga and meditation (Christine, France; Defne, Türkiye), while others, such as Ceylin (Türkiye), favour cardio exercise to relieve physical and emotional stress. At the structural level, such coping strategies are necessary because of the lack of formal support and the societal message that menopause is a private problem. Thus, women are implied to be individually responsible to re-establish ‘balance’ and to engage in self-care in order to manage MT (Steffan et al., 2026). On the advice of friends and relatives, some women turn to alternative medicine such as homeopathy (Ines, France), often to avoid hormone therapy (Lisa, Germany; Ferda, Türkiye). In relation to the workplace, women report that they take measures to deal with hot flushes, for example by setting up a desk fan (Lena, Germany) or wearing several layers of clothing that can be easily removed (Carmen, Olivia, Germany) or taking extra clothes to work in case a change was needed due to hot flushes (Sezen, Türkiye). To cope with cognitive fog, Susanne (Germany) is one of several women who report taking more notes than before MT: ‘And that’s why I now really work with writing things down, with lists. I really have to write everything down in detail, otherwise I’ll forget it.’ Some women adjusted their expectations of work (Alexandra, Susanne, Germany; Ceylin, Türkiye), changed jobs (Elodie, France) or set new boundaries – e.g. refused to travel, took breaks or limited demanding interactions (Sybille, Germany). By using these strategies, women made their MT easier and used the support and resources available to them while remaining within the limits of the system. That said, while by making these adjustments and employing these agentic strategies they help themselves as well as other women in MT, these coping strategies concurrently hide menopause in the workplace, instead of allowing space for open discussion.
Finding a new path in life
Whether in a supportive or restrictive context, many women described menopause not as a constraint but as a change that puts their agency front and centre. By re-evaluating their lives, they found new roles and opportunities within existing social structures that empower them (Steffan et al., 2026). Many see this process as an opportunity. For instance, Virginie (France) talks about her ‘passions’ and that she now ‘has time to focus’: ‘I took up painting again, wrote a book, and even started my own entrepreneurial project. It’s a time of intense creativity.’ For many, the MT is a time to redefine themselves, for instance due to ‘being liberated from motherhood’ (Zoya, France), and some feel like they are ‘no longer the same person’ (Karine, France).
However, while transformation is mostly framed as having positive outcomes, it is also important to state that this transformation is not always easy. Christine (France) expresses a sense of loss, stating, ‘There’s a kind of mourning for the person you were before. The verdict is quite brutal. . . it’s a rather violent verdict.’ Guliz (Türkiye) shares her feelings openly when she says: ‘There’s a part of my mind that says you need to accept this natural process. But on the other hand, there’s also a part that feels fear, anxiety, the unknown.’
The findings suggest that women in France, Germany and Türkiye create new routines at the individual level to support their MT transition, which are embedded in the social and organisational structures of their societies and characterised by mutual exchange and support. Although the transition process is usually anything but easy, for many women it leads to a new path in their lives that allows them to discover new aspects of themselves and enrich their lives during this phase. Next we discuss how the cultural framing of the menopause in the three countries affects women’s experiences.
Cultural nuances in the interpretation of similar experiences
Giddens (1984) compares social structure with the wall of a room, having fixed boundaries that impose constraints, but within which the individual can move freely, i.e. using her agency. Giddens’ (1984) concept of structure refers not only to formal institutions and norms but also to informal ones embedded in one’s cultural norms and values. Our analysis shows that despite cultural difference, the space in which women negotiate and adapt their work habits during their MT transition looks quite similar for participants in France, Germany and Türkiye. Previous comparative research has challenged the assumption that MT is experienced in the same way across cultures (Lock, 1994; Obermeyer & Sievert, 2007), showing that the country in which a woman lives has a greater influence on her MT experience than the culture in which she grew up (e.g. Hinrichsen et al., 2014) and that social structures like social class differences have a direct impact on women’s menopause-related symptoms (e.g. Delanoë et al., 2012).
In our study, we observe only nuanced national differences in the way women in white-collar jobs interpreted their MT experience: in France, as loss of femininity, in Türkiye, in terms of fertility, and in Germany as focused on performance, while the descriptions of symptoms and supportive and challenging structures were remarkably similar. These differences in the framing of MT suggest that social and cultural norms, like the social value of motherhood in Türkiye (Duman et al., 2021) or the importance of having a heteronormatively feminine appearance in France (Grout, 2024), have a primary impact on how menopause is interpreted by women, as echoed by our participants. In contrast, in Germany, with 77% of women engaged in the workforce currently (Statistica, 2024), it comes as no surprise that MT is framed as a potential threat to their professional performance. However, not only were German women concerned about being perceived as less capable, but French and Turkish women also occasionally expressed these concerns, leading many of them to remain silent about the issue in the workplace.
While our study concludes that these nuanced cultural differences contribute to how women interpret MT (Riach & Jack, 2021) and use their agency accordingly, especially in the beginning, overall they do not have a significant impact on the experience of study participants. This might be the case because we focused on women in white-collar jobs, who usually have more knowledge and resources to support their agency. The cultural framing of menopause and observed differences in symptom patterns related to MT do not appear to translate into differences in the way women cope with their MT at work. While menopause presents itself differently in France, Germany and Türkiye cultures, the general silence about it, particularly in the workplace and healthcare system, is consistent. Some individuals and organisations try to address the challenges faced during MT by proving support. In the next section, we discuss what resources are available to women in the three countries.
Formal and informal support structures
Our study contributes to research on the design of a supportive workplace for women in MT (Rees et al., 2021). We observe that women develop strategies that help them adapt their work environment and practices in ways that potentially reduce the impact of menopause-related symptoms on their work performance (Beck et al., 2019). For some women, this means actively negotiating their tasks in their professional environments (e.g. refraining from business trips, taking breaks), while others try to make their changes discreetly. Structures specifically designed to support women during their MT transition are still rare, although there is international guidance for employers (Rees et al., 2021) and research shows that they improve employee wellbeing (Dennis & Hobson, 2023). However, supportive workplace adjustments, for instance, provided for flexible work time and home office working, and adjustable room temperature. Thus, there are structures at these workplaces that support women to navigate their MT by providing them with resources that allow adjustment of work routines and the working environment to changing needs even without explaining the reasons why they need these changes.
Yet, existing adjustments are not available to all (den Hond et al., 2012). While organisational adjustments are often presented as supportive, our findings indicate that not all women feel supported enough to take advantage of such adjustments, as they fear discrimination and as a result continue to keep menopause hidden in the workplace (Steffan & Potočnik, 2023). Thus, women continue to manage the impact of MT on their work experience themselves – even when support is offered. In many cases, support is the result of individual negotiation rather than being built into routines and shared responsibilities. Consequently, even when workplace structures are supportive, many women organise support and resources informally, for example by talking to colleagues during breaks about how tiredness, brain fog and hot flushes are making work difficult, and sometimes colleagues agree to help, hence creating informal structures. This preference to seek informal support is closely linked to the cultural expectation in the workplace that body-related, physical issues such as illness and menopause are not a workplace issue (Verdonk et al., 2022). Formal workplace adjustment is only sought when the situation is particularly difficult, for instance when challenging health issues are involved. Workplace silence on menopause, therefore, creates barriers to seeking formal support in the workplace, even if supports exist, which goes some way to explaining the high importance of informal support networks (Collins et al., 2024).
We observe a similar preference for informal structures when women seek help from the healthcare sector for menopause-related symptoms. We find that the quality of care women receive in the healthcare sector for symptoms varies widely, resulting in many women having to consult several doctors before gaining adequate help. Many women turn to alternative forms of treatment during MT, for which there is less scientific evidence (Djapardy & Panay, 2022) in addition to or as a substitute for medically prescribed treatments.
Overall, designated formal support structures exist, although they are still rare. Social change remains slow because of a strong taboo around menopause (Hardy et al., 2019a), and women are reluctant to engage with formal institutions such as their employers and doctors. Thus, instead of relying on support structures they seek informal and private solutions to the challenge they face. The existence of a structure does not lead to direct ability for its use (den Hond et al., 2012). Our research provides an in-depth understanding of how institutional structures surrounding MT coexist and co-produce each other, influencing how MT is experienced and managed (Williams, 2024). When existing structures are not satisfactory, women collectively produce informal structures to help them manage MT. We now turn to inequality of access to support.
Unequal access to supportive formal structures
Our study suggests that access to support during MT, whether in the workplace or from healthcare providers, remains unequal. In all three countries, participants described moments when they received timely help and situations where support was limited or absent. Some women, even with severe symptoms, were able to maintain a sense of job satisfaction when workplace conditions were flexible or when treatment was effective. Others, faced with inadequate care and little room for adjustment, reported feeling overwhelmed or drained. In these cases, changing jobs, reducing working hours or considering early retirement were among the ways they coped with their situation. These experiences mirror patterns observed in the UK, where research has found that a significant number of women adjust their working lives in response to the menopause, and some consider and take early retirement (Griffiths et al., 2013).
Workplaces may play a role in alleviating some of this pressure. Recent developments in France – for example, the proposed reforms to improve medical support for MT (Ministère de la Santé, 2025) – suggest that menopause is beginning to receive more political attention. But while healthcare is more accessible, menopause continues to receive little attention in formal workplace policies. In Germany, the importance of part-time employment and recent parliamentary debates have opened up some space for public discussion (MenoSupport Research Project, 2023), although concrete measures remain limited. In Türkiye, where female labour force participation is lower and traditional gender roles persist, there is even less institutional visibility. These differences determine the conditions under which support is available, how women adapt their working lives and shape the structures within, through the use of their agency. The need to self-manage this transition seems to be a common thread that emphasises menopause as a particular and shared experience.
Where formal structures fail, women often turn to informal practices – quiet adjustments, private conversations, small acts of boundary-setting that help them cope with everyday working life (Steffan & Potočnik, 2025). These do not replace structural support, and do not solve all challenges, but they do show how women find ways to protect their wellbeing and maintain a sense of control within social structures. In doing so, they also contribute – albeit subtly – to changes in workplace culture (Gill & Orgad, 2018). These everyday negotiations draw attention to the need for action that goes beyond policy and looks more deeply at the ways in which menopause is lived and managed in different settings (Atkinson et al., 2021). Reimagining MT at work requires predictable workplace adjustments and more reliable healthcare pathways, rather than leaving women to manage uncertainty on their own.
From this perspective, coping with menopause in the workplace is more than individual coping; it reflects a relational process characterised by broader social, cultural and institutional dynamics while simultaneously contributing to their reproduction and, at times, gradual change. Understanding agency as something that unfolds within these conditions rather than in opposition to them can provide a more grounded perspective. Giddens’ structuration theory (1984) provides a useful lens for thinking about these patterns, yet it does not fully explain how gendered power operates within institutions. Our study shows that an enduring patriarchy operates as a system embedded in organisational life (Walby, 1989) and reinforces McRobbie’s (2009) observation of the limitations of a gender-neutral framework in capturing how bodies and emotions are positioned within structures of productivity and visibility.
Adjustments made at the level of workplace processes can provide support, particularly when interpersonal relations are strained, for instance, in situations involving unsympathetic or inexperienced managers. Responses to MT challenges are neither fixed nor fully autonomous; rather, they develop within shifting conditions of recognition and support. Framing menopause as a meaningful life-course event (Quental et al., 2023) could help workplaces view it not as a disruption but as part of a broader continuum in which women remain active and productive. Making workplace arrangements that consider the experience of women going through menopause may encourage societal recognition of how care, adaptation and agency unfold in everyday interactions within institutional settings.
Conclusion
In this article, we explored how social structures influence women’s agency as they navigate their MT in the workplace and how the enactment of agency responds to and reshapes these structures. Our study shows that menopausal women’s agency is influenced by social structures in three ways. First, cultural interpretations of menopause shape how women understand how MT affects them. Second, the strong taboo around MT (Hardy et al., 2019a) leads women to primarily enact their agency in order to build up informal structures to find support during MT, rather than relying on the (limited) formal support structures that do exist. In so doing, they reshape and expand existing support structures. Third, because access to effective formal support structures in the workplace and in society are unevenly distributed, some women find it impossible to manage their MT in their workplace despite using coping strategies. The agency in such cases is mostly used to make individual life-changing decisions like changing jobs, reducing working hours or considering early retirement. However, many women still find ways to make changes during MT that lead to their overall life quality improving. To what extent women were able to instrumentalise their agency to change structure is difficult to capture in their narratives: how their exchanges and actions contribute to changing perceptions and attitudes and might precede more visible changes to procedure, resource location and other aspects of structure. Some women did describe recent improvements in the support offered at their workplace, e.g. meetings addressing MT. This suggest that the agency of women like our participants has contributed to changing some aspects of the structure they are confronted with.
Footnotes
Acknowledgements
The authors would like to thank all interview participants who generously shared their experiences and perspectives for this study. We also thank the editors and anonymous reviewers for improving our work with their supportive feedback.
Ethical considerations
This study received ethics approval from Rennes School of Business and was conducted in accordance with institutional ethical guidelines.
Consent for Publication
All participants provided informed consent prior to participation for research purposes.
Funding
The authors received no financial support for the research, authorship,and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Due to the sensitive nature of the qualitative interview data and the need to protect participant confidentiality, the data supporting the findings of this study are available from the corresponding author upon reasonable request and subject to ethical approval.