
Abstract
Studying kinship has involved doing family, displaying family and ‘displaying family’ as a sensitising concept to understand modalities troublesome to display. Fathers at antenatal screening clinics for sickle cell are faced with pressures to produce multiple displays – of family, illness knowledge, the good father and the model citizen – often in the face of racialised identities. Such fathers emphasise the importance of hypervisibility in gendered spaces and hypervigilence, lest pressures to adopt the ‘right’ disposition have adverse consequences for themselves, partners or their children. The displays of fathers, as well as displays they decline, are orientated to repair of social relationships. Where displays are provoked by social relations – resisting racist or gender stereotypes, navigating citizenship uncertainties, negotiating work and family lives – displays become problematic. Family display becomes troubled where the preferred social relationships fathers seek to constitute are ones that are not readily accommodated within extant social relations.
Introduction
The antenatal screening clinic intersects several domains of interest: the politics of health surveillance (Rapp, 2000); the impact of reproductive technologies on selfhood, kinship and family (Strathern, 1996); and how people negotiate gendered identities for parenthood (Henwood and Procotor, 2003; Shirani et al., 2012). Genetic screening is part of health surveillance, and a genetic carrier one of the modernist categories that make up people as matters of concern to the state (Cornford et al., 2013). Historically, most antenatal technology targeted the mother (Rapp, 2000). However, antenatal screening for sickle cell is directed to both sexes (Reed, 2011), disrupting men’s expectations of impending fatherhood (Dheensa et al., 2013).
Sickle cell disorder (SCD) is an inherited chronic illness, with the (mainly) asymptomatic genetic carrier state (sickle cell carriers) identifiable through screening at antenatal clinic. Sickle cell genetic carrier status is associated with partial protection against malaria and thus has an indirect association with populations who inhabited (historically) malarial areas of Africa, Arabia, the Mediterranean and India. While actually undermining ethnicity as an objective variable (Carter and Dyson, 2011) sickle cell is ‘emblematically black’ (Hall, 2003: 6), leading ‘white’ men to assume wrongly it could not affect them (Reed, 2011). Genetic information medicalises kinship networks (Finkler et al., 2003), renders fatherhood fragile (Turney, 2011) and, in the case of sickle cell screening, disturbs preferred definitions of family that discount the father, while emphasising their ethnicity (Dyson et al., 2007).
To date, sociological study of the clinic has not maximised links to theories of kinship. In this article we consider approaches conceptualising family as an ongoing achievement of actors (Morgan, 1996), as a phenomenon (re)constituted by activities of display (Finch, 2007), and ‘family display’ as a sensitising concept, attuning us to practices/identities problematic to display (Gabb, 2011). We consider these concepts in the light of empirical data: interviews with fathers who have experienced sickle cell screening. We suggest fathers necessarily foreground being present and learning the ‘correct’ dispositions of fatherhood. This is used to assess the role of social relationships, and the role of wider social relations that pertain to men from racialised minorities, in provoking displays of family.
Displaying Families
Sociologists have moved away from conceptions of ‘the family’ to assessing moral actors, ‘doing family’, through meaning-generating practices (Morgan, 1996). Family display consists of the means by which people communicate to each other, and to relevant audiences, that something constitutes family (Finch, 2007). In order to be affective the activities need to be understood by the others to whom they are directed as family activities. Professionals at antenatal clinics, for example, represent official audiences to whom people feel obliged to link their own circumstances to wider culture through family display.
Not all family-creation work is display work. Some family work is part of the taken-for-granted part of constituting family life, for example, a biological father reading bed-time stories to his child (Finch, 2007). The example betrays by implication occasions where display becomes imperative: where social ties are not coterminous with biological ones (Jones and Hackett, 2011), where heteronormative assumptions are transgressed (Almack, 2008) or where transnational families are not co-located within the same households (Heath et al., 2011). The concept of display is grounded in reconstituting the family in situations rendered extra-normative by social relations of, say, gender and racism. Thus we may
perpetuate normalising discourses which privilege certain sets of attachments and forms of relationships and erase the value of others which do not have readily available scripts and/or that are already demonised by sets of moral values which determine what displays affectively count. (Gabb, 2011: 57)
Considering the role of fathers in display work suggests that the ‘normalising gaze’ gives legitimacy to certain displays at the expense of others, with display (fathers’ use of heroic narratives when thrust unexpectedly into the role of primary care-giver) linked to notions of hegemonic masculinity (Doucet, 2011). Displays of fatherhood, Doucet argues, become more intense when men are in gendered spaces (plausibly, the antenatal clinic). Indeed, a mother of African descent stated: ‘African men regard the UK as a women’s country’ (Field notes) and antenatal spaces may thus be doubly gendered, making antenatal care a fruitful location to consider the display of fathers-to-be. Owing to expectations of male behaviour, displaying intimacies renders fatherhood ‘risky by default’ (Gabb, 2011: 47). Family display may help in being publicly viewed as a non-threatening male (Henwood and Proctor, 2003). Meanwhile, in the practice of antenatal sickle cell screening in England, ethnicity is foregrounded (Aspinall, 2013). Furthermore, opportunistic screening practices mean (black) men who attend antenatal screening are tested for HIV (Dhairyawan et al., 2012), thereby emphasising state surveillance rather than care. Under such heightened ‘watch’ from services, black fathers may experience public spaces as doubly risky (to develop Gabb, 2011: 47). Given racist stereotypes of black masculinity, somatically ‘highly visible’ (Gabb, 2011: 46) and vulnerable to ‘misrecognition’ (Gabb, 2011: 43), black fatherhood is liable to be even riskier to accomplish.
We do not regard sickle cell carriers as bodies principally constituted through performance (cf. Butler, 1993). For instance, sex dichotomism represents a generative ontological reality underlying a tendency to groupings of physical traits – sex – within a spectrum of overlapping, indeterminate and intermediate traits, groupings subsequently culturally endowed with gendered meanings (New, 2005). Thus social performance of gender does not obviate the reality of sex dichotomism. Likewise, genetic recombination generates carriers, non-carriers and those with SCD (but also overlaps and rare complexities, for example, those with carrier genotypes, but SCD phenotypes). Such biological variations form an anterior material substrate to cultural experience, which may or may not be actualised (see Elder-Vass, 2008 on the limits of Latourian notions of performance). As we will argue, sickle cell carriers undertake normative-countering ‘family displays’. However, being a sickle cell carrier entails real, if generally not actualised, ontological changes in the body, and thus cannot be reduced to performance.
Methods
The research aimed to understand fathers’ experiences of sickle cell screening, and received approval from the National Research Ethics Service. The sample was generated with eight sickle cell non-governmental organisations (NGOs), recruiting 24 fathers from nine different cities, with three declining (one African, two white). The NGOs were given recruitment fees and the fathers were paid a fee plus travel expenses for participation. The sampling strategy sought diversity in terms of age, ethnicity and knowledge of carrier status (Table 1). Interviews, of 30–90 minutes, were transcribed in full, and analysed using Atlas-Ti. Using the concept of ‘display’ as a theoretical framework, but focusing on accounts of display as a way of opening up emotions and the invisible, allowed the identification of two main themes: (1) the behaviours the fathers reported during antenatal care; and (2) the ostensible goals of such behaviours.
Characteristics of the sample of fathers.
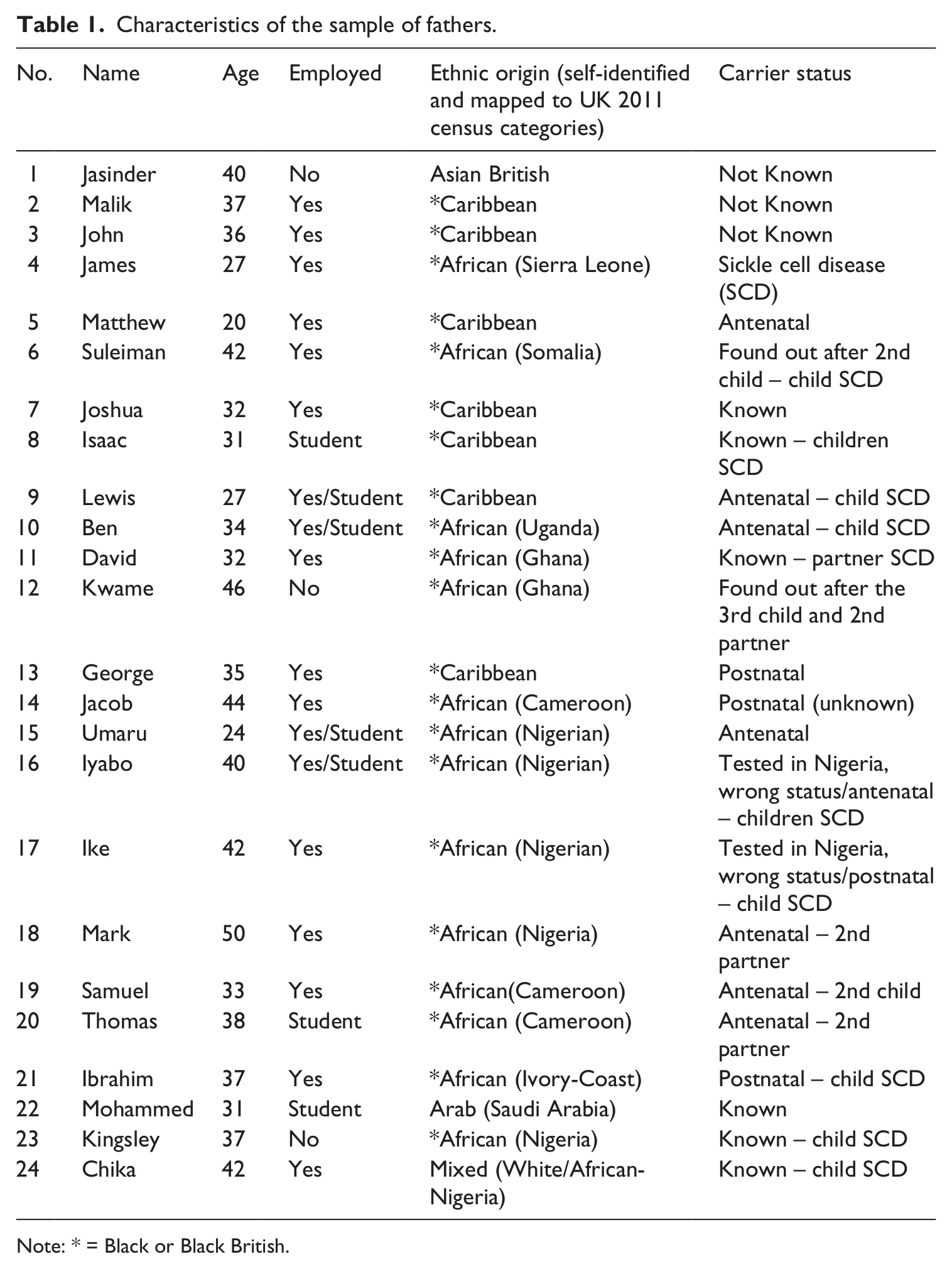
Note: * = Black or Black British.
Methodologically, our data rest on accounts (of display and as display) not on direct observations at clinics. In Goffman’s (1959) terms the interviews are at once ‘off stage’ from displays directed to health professionals at clinics, but ‘front stage’ in a research interview. This does not substantively affect our analysis: reflecting both on reported displays in the clinic and displaying for the interviewer tell us something about how the fathers feel they have to embody fathers/sickle cell carriers.
Family relationships can be accomplished without recognisable displays but within the ethnic minority/migrant fathers in our sample, we wondered how any pressures to display ‘the good father/citizen’ to health officials might be negotiated. During the antenatal trajectory, some displays ‘may fall outside the registers of cultural intelligibility’ (Gabb, 2011: 53), and a research interview comprises an opportunity to repair the display of family to officialdom. The fathers aligned the interviewer (white, female and bilingual, so able to build rapport with Francophone African respondents, though all interviews were in English) with the voluntary sector but also, variously, with the medical profession, social services and with having new knowledge to impart. Based on differing social histories of suffering linked to medical services, some fathers were initially wary of research (based on hostility to official institutions or doctors), testing the interviewer out, while others were friendly and gregarious. Yet fathers each had specific things they wished to derive from the interview – to clarify genetic information, ensure improvement in services or to seek moral reassurance. Such accounts are considered as co-ordinating practices, recrafting personhood and seeking to (re)constitute family.
Display Activities in Reporting Care
Those interviewed presented complex orientations to antenatal care depending on age, ethnicity, class and understanding of carrier status, but, in keeping with our theoretical aims, we focus on two in particular. One was the importance of being there: in being present (doing and displaying family) when the mother-to-be was undergoing antenatal care, including sickle cell screening. The other was in adopting the ‘right’ disposition, the correct way of comporting oneself in antenatal spaces. Such spaces were not necessarily congruent with inclusion of men, as George (‘Dad’s just there in the background’) and Isaac (‘Hi Dad, you’re in the corner’) both remarked on. We now consider these two themes – being present and adopting the ‘right’ orientation.
Being There
With expanded conceptions of fatherhood comes the expectation that fathers will be present in child-relevant spaces (Henwood and Proctor, 2003). To extend the notion of hyperparenting (Hoffman, 2010), all the fathers were hypervisible: attending appointments, taking part in antenatal classes, being there for scans. Moreover, as well as expectations to display family through presence, fathers felt they also needed bodily engagement to secure ‘doing family’. Sickle cell screening was not consciously rehearsed as an autonomous choice but was accepted because the ‘good father’ (Henwood and Proctor, 2003) was now embodied in antenatal care. Blood tests for sickle cell were processes accepted as part of the dutiful father role. Women were still gatekeepers to bodily involvement but most fathers recounted an imperative to test: ‘You’re going to have a blood test’ (Malik). You, that is, any reasonable person, is interpellated to take such tests (see Yates and Hiles, 2010).
The moral desirability of being there could be inferred from the manner in which they accounted for attendance. They had to ‘curtail my social life’ (John), ‘take days off work’ (David) or ‘make time’ (Mark) to go to appointments. Fathers who had children with SCD (that is, the condition, not the genetic carrier status) were simultaneously learning that they had to display ‘sickle cell’ correctly to health services. Jacob recounts being asked about sickle cell by the midwife in front of students ‘and I answered the questions and she was happy’. Fathers who were asylum seekers were versed in the particular docility required of them by immigration services, involving displaying good citizenship. This might explain some fathers’ enthusiasm for mandatory testing. Yet, this particular visible bureaucratic docility could also endanger the family if unwarranted (health) services were imposed, and thus presence was also about hypervigilance. Overlapping pressures to display come together in this account of the strains of caring for a child with SCD in severe pain as the father attempted to resolve immigration issues.
I was an asylum seeker, so everything was coming into my head. The pressure of the family. The pressure of I have report to Home Office with a sick child. Taking him to the hospital […], bringing him to the Home Office to come and report, and one day he have a crisis right there in the Home Office and I was trying to say that he’s having a crisis. […] the people over here does not know about the illness at all. At all. So, I was actually just talking until someone could understand me, until the kid passed out and they called the ambulance. […] To have people in front of you most of the time about security and you don’t get close to official that are probably right above. They cannot come down because they’re scared, you’re lowly, nobody speaks probably to an asylum seeker and open up to understand what the person is trying to explain. So, we were just waiting and holding on to fate, just hoping that someone will call for an ambulance and I can try to explain to them […] the ambulance has come, they took him away and I still had to report for whole family. And my wife was penalised because she did not report that time. They fine her £3000. (Samuel)
The ultimate in accounting for absence were occasions where the father was able to invoke care work for other children or his wife. Iyabo reported that his efforts to attend postnatal care were thwarted by having to care for his other child with SCD and to attend hospital appointments with him.
James, who had SCD, and David, Mohammed and Chika (married to women with SCD) noted how their ‘displays’ confounded expectations that screening concerned only genetic carriers. Chika explained how being interpellated to antenatal decision making overlaid his caring responsibilities (for both his wife with SCD and children with SCD), which subsequently affected his personal relationship with his partner and ability to perform caring work. Malik ‘wasn’t condemned out of the room’, implying there are fathers who might be excluded were their displays deemed illegitimate. The implication is that the extended embodied presence of fathers is not part of taken-for-granted family work. The right to be present is a moral issue, and has to be earned by adopting the ‘right’ disposition.
Do the Right Thing
Men’s involvement in decision making around pregnancy could be conceived as a form of control over women (Rapp, 2000). However, the importance of disaggregating both men and women, as well as questioning assumptions of their oppositional interests (Annandale and Clark, 1996) and of examining ethnicity as well as gender (Reed, 2011) means that male involvement in prenatal decision making cannot be dismissed as a new articulation of hegemonic masculinity. For example, some fathers related that they had to deal with managed information, information that was relayed and controlled by their partners or health professionals.
Moreover, men might be viewed as gaining their access to gendered spaces surrounding pregnancy at the expense of co-option to health surveillance. This leads us to the second theme, that of adopting the ‘right’ disposition. Thus fathers were supposed to monitor the mothers in taking supplements (Suleiman), in their diet (David) or undertake emotional work: helping them to absorb distressing news (Ibrahim), to overcome the mother’s resistance to aspects of care (Samuel) or to ‘play Mr Nice Guy so as not to stress her out’ (Lewis). The accounts of the fathers suggested they are to be docile bodies in the antenatal clinic, teachable, but also passive, subservient and obedient. Jasinder recounted how bodily and emotional displays of support were taught by professionals: ‘And then the midwife had to kind of say, you know, [laughs], “Do you want to hold your wife’s hand?”’
There were rules of the game fathers felt they needed to learn, and not only with respect to the antenatal world. Jacob, to whom the key difference between carrier and condition had not been adequately explained, struggled to understand what he needed to learn and what he needed to teach his child. His display was not just about care, but much broader to how, as a sickle cell carrier, he should comport himself in a moral fashion in life.
On the one hand fathers viewed themselves as needing to exhibit obedient docility in order that they and their partner emerged ‘unscathed’ from the encounter with health services (Jasinder), while Joshua and Kwame submitted to the same tests more than once. On the other hand, fathers needed to ensure that they could raise questions, including about screening, and protect themselves and their families when needed. Having test results was perceived as empowering by some fathers (Mark, Mohammed), even if they waited until after the child was born (George, Jacob). For other fathers who tested positive, this meant more uncertainties, acceding to perceived indignities, and accepting invitations of prenatal diagnosis (PND) and choice of termination. Situated strategies that resisted such positioning were rendered, in effect, dys-plays: joking to be noticed (James) risked confirming their marginalisation as appropriate. Asserting their view (Ben) risked displaying lay ignorance (if aligned with the mother) or male interference (if the mother aligned with health professionals). Lewis was angered by several aspects of his antenatal experiences. When told he has to have a blood test for sickle cell he ‘feels obligated to do it, cos it’s my child’ but is frustrated when, having been tested early in pregnancy, it is only in the last month of pregnancy that the child’s SCD is confirmed ‘so I’m thinking it’s pointless you even telling me this now cos you could have done that from before’.
However, raging because of bad experiences risked confirming to professionals his unsuitability for antenatal spaces:
They were treating us kind of separate. Cos when I said something, they’re telling her something else. ‘Oh it would be better for you da-da-da-da-da-da-da-da-da.’ It’s like they’re telling her ‘Oh, he’s not in the position you’re in right now, he’s just here for you basically.’ So it’s only when I got angry at one point I walked out of the room for five minutes. I came back and she’s getting an injection in her back. I’m thinking like we said we weren’t going to do this and as soon as that they convinced her to do it.
According to Lewis the professionals perform a caesarean, both medically and in a discursive sociological sense. He says:
They wanted to caesarean her from the beginning but I told them no, if you caesarean her she will be limited to the number of children she can have, understand? […] They didn’t give us a lot of choice there and then. So they’re like, you have to do that. And I’m like, ‘No, we don’t have to do this we can wait.’ They’re like ‘If you wait any longer the baby’s going to die or suffocate.’ […] I thought they used us as a guinea pig […] that night there were a lot of pregnant women on the ward. So I’m guessing they just wanted the quickest way for them to get all the kids out in any one go.
Beyond anger, the only possibility was to engage broader contextual resources: moving antenatal care to another hospital (Matthew, Kwame), making an official complaint about discrimination (Ben) or having recourse to the law. Chika, taking legal action against the hospital after being denied IVF (and hence access to pre-implantation genetic diagnosis, a means of having further children without having another child with SCD) feels racism is subtle (‘people that are more educated might have their views but are good at masking’), and that the consultant who wrote the letter that led to their IVF offer being withdrawn was protected (‘[hospitals] have a legal department, they look after staff. “Oh, [consultant] didn’t mean it that way”’).
Furthermore, being docile (teachable) required fathers to be contingently proactive: reading up or researching the internet for information. They felt obliged to demonstrate that they are not passive in expecting health workers to provide them, unsolicited, with information.
Moreover, fathers had often not received the information they felt they needed, a situation betrayed by the majority, especially those who had children with SCD, who still sought genetic information, including from the interviewer.
However, adopting the ‘right’ disposition also came with a cost. Isaac, Samuel and Chika mentioned religious faith that sustained themselves and their families when dealing with the difficult decision making that SCD diagnosis brings. Ibrahim believed in God as a practical way of dealing with the uncertainty generated by the stress of hypothetical-abstract genetics, though expressing faith publicly risked provoking unwarranted assumptions of fatalism (Atkin et al., 2008). Umaru’s wife was circumcised (before they met) and he accepted moral surveillance as an obligation to ‘accept the culture here’, a culture that ‘monitors her to make sure she doesn’t do the same for the child’. In a context where, in his home country, only female relatives accompany pregnant women for support, Ben stated: ‘When you come here, you find that fathers do get more involved. So I adopted the culture.’ Thomas contrasted the way health workers bypass another father, with the personal phone calls he received, relating this to his docility in accepting PND for his own wife’s pregnancy ‘but because me, I decided to co-operate, it was different’, an acceptance he later regretted.
Finally, there are occasions when the attempt to display the right tendencies – to exercise choice, display the fruits of knowledge searches and to be attentive to details of health information imparted – are thwarted. It is here that the social relations underpinning display come to the fore.
Reasons for Display Activities
By recalling the classic idea connecting personal troubles to public issues (Mills, 1959) the researchers inferred two types of reasons for fathers’ displays. The first concerns interactions at the level of situated activity (Layder, 1990), characterised by observable or actual social relationships, encounters to which people bring their own biographies. The second type concerns contextual resources of class and racism, and institutional systems of health, education and the law. These contextual resources and institutional arrangements are at a level beyond individual consciousness, are relatively opaque to the individual social actor and are encapsulated by the concept social relations (Layder, 1990).
Reasons for Displaying: Relationships
Displaying family becomes important when the activities concerned cannot be taken for granted as part of everyday family life (Finch, 2007). There are reasons arising from social relationships, for example reconstituted partnerships or transnational kinship networks, why display may be necessary. For Jasinder, the basis for display was that, while the mother had several children with previous partners, the baby was his one-and-only possibility for fatherhood. Moreover, display may be required to be of different intensities at different points of time. Display comprises interaction, being witnessed by other audiences, or connecting a person’s particular narrative to broader societal tropes (Finch, 2007), but it may also consist of bodily actions, and these may constitute a display of couples to interviewers that their family ‘works’ (Doucet, 2011). Jasinder’s transcript reads: ‘Wife is sitting next to him on the sofa breastfeeding the baby and he wants to include her in the conversation. […] Father seems very protective of mom and baby.’ The need for display, it would seem, arises in circumstances where a normative expectation of family is subverted. Display thus becomes more necessary if the family is reconstituted, or if the normative family form is not in one’s own life history. Isaac says:
I’m half a single parent, I’m half an only child. I’m an only child from my mum but I’ve got three half-brothers from my dad. So yeah, I think there is that understanding what it’s like to be in a single parent family, I wanted to make a family, feel like a family.
In the case of some fathers geographic separation through circumstances of employment or migration (Thomas had left behind a wife and child in Africa because of ‘immigration reasons’) may produce an impetus to display family. Moreover, if the pregnancy is unplanned, if the partners are unmarried or not living together in a stable relationship, or indeed if the father–mother–child triad is contested as constituting family, then display may be required. For example, John, involved in contested child custody, compared himself to younger men, who, unlike him, would not be competent fathers:
they’re not really hands on, knowing what’s what. I’ve done everything with my son. Like when he’s got a cold, suck all the snot out of his mouth […] so he can breathe properly, and people are like: ‘Ugh, how can you do that?’ ‘That’s my son.’ ‘Who told you how to do that?’ ‘Nobody, it’s just natural instinct’. My Dad done it when I was younger.
Willing to be very hands-on, and dealing with bodily fluids in a manner some would find distasteful, he regarded his actions as a display of embodied fatherhood, a ‘heroic narrative’ (Doucet, 2011: 85). The relationship of the men with their own father, whether as a role model (Malik), or not being part of the person’s life at all (Lewis), may also be drawn upon in accounting for impending fatherhood and how services support or confound those displays. Thus, several fathers argued that information about genetic status came too late for them to make real choices about what kind of fatherhood they wanted. Displaying genetic responsibility as a father can also be achieved by projecting into the future: Mohammed referred to a discussion with his extended family, orientated to his son being knowledgeable about sickle cell carriers in the future, stating ‘I want you to be better than your father’. Jacob believed an understanding of sickle cell would repair notions of genetic blame in his African extended family where many people died unexpectedly without adequate medical care.
There are also situations where fathers-to-be may come to be regarded by professionals as especially accountable with regard to sickle cell. Some fathers had a prior connection, such as their own father working for a sickle cell charity (Matthew), a mother who spoke publicly on sickle cell (Joshua) or having relatives who died of SCD (Umaru, Ike, Thomas, Mohammed). Fathers varied in whether they had been tested, whether they understood the difference between a carrier and SCD or where, for them, genetic responsibility lay, but in every case asking interview questions about antenatal care, (‘were you tested?’), topicalises fathers’ behaviour as potentially problematic. Some fathers were struggling with conceptualising genetics, but others were felt to be obfuscating knowledge because of what it might display about them or their families, especially if they were educated about sickle cell, had SCD or chose to be with a partner who had SCD. In the case of those from Africa, prior experience of SCD is sometimes in a context of relative poverty with relatively inaccessible/unaffordable health care, with SCD stigmatised because of its association with early death or the supernatural (Nwezi, 2001). This imparts a very limited experiential knowledge of sickle cell: of knowing people with SCD who are skinny, regularly sick or in pain (Iyabo, Mark, Ben), and often dying in childhood (Samuel).This intensified this sense of being held accountable. Often the stigma of sickle cell and role of myths meant information was concentrated more on prevention before rather than within relationships. This was mitigated by the strong cultural imperative for children, primacy of relationships and love both for mother or father, faulty negative carrier tests given in Nigeria, belief in improving health care and prospects for living with sickle cell, religious faith, as well as economic and social pressures to have children when a migrant in a new country.
Reasons for Displaying: Social Relations
Sickle cell screening is implicated in wider socio-cultural contexts (Carter and Dyson, 2011) and thus there are also broader societal and institutional framings that appear to underlie reports of displays in antenatal clinics. John and Matthew accepted testing because SCD, being racialised, was accepted as ‘natural’ for African-Caribbeans. Six of the 24 fathers were migrants. Their various statuses, as skilled workers, students or asylum seekers, meant differing expectations of involvement. Samuel was unfamiliar with even the concept of antenatal care, so although social support was there, it was displayed in other ways, such as ensuring the breadwinner role. Likewise, when Jacob could not go to all the antenatal appointments he bought a car for his wife. This is contrasted with a younger transnational African generation who expected to be involved in services but found their displays resisted:
I made an assumption that, OK, a lot of fathers, especially in certain areas and from ethnic minorities; they’re not really that supportive, so perhaps they had that perception. But I thought it was unfair, cos I wasn’t one of them. (James)
However, he qualifies those displays by noting that even if you are a modern father, your own involvement in screening could be inhibited by the socio-cultural ascriptions given to sickle cell by the extended family. It is this tightrope of different required displays that they must negotiate. Some fathers have not only to learn the alien concept of antenatal care, but also that adopting the correct disposition to such care is part of the public display of family pertinent to securing leave to remain in the country: ‘I mean this is another country so we came abroad, came down here, we must follow, I mean the rules. If GP say you are immigrant here, come so many years ago’ (Suleiman). This is particularly the case if the father has work commitments abroad (Matthew), as these compromise his opportunities to demonstrate commitment through participation in screening and by engaging in traditionally non-male spaces. Being an immigrant also means having to adopt UK culture. This may be a deliberate flight from one’s own culture as in the case of one father who ‘says it is best not to have too close contact with people in the [African country] community because of the political situation’. Accommodating to racism in UK society was exemplified by another father who reported adopting a regional accent and using skin-lightening creams.
Resisting racism may also mean countering stereotypes of African or Muslim men, stereotypes pertaining to illness (HIV/AIDS) (Matthew, David), religion (Ibrahim) and ‘curses’ (Ben); foregrounding instead their educational or socio-economic positioning with regard to uptake of modern biomedicine, distancing themselves from the concept of reincarnation (Umaru) or from the men who in Africa do not accompany women to hospital (Ike). The countering of stereotypes is sophisticated and shows how and why obfuscation can happen. For example, Ike explained how socio-cultural beliefs and biomedicine are used interchangeably by people. Chika noted how, despite education, some African people may still reject people with SCD because of the wider supernatural beliefs and stigma. Similarly, Kingsley noted how family display is linked to family reputation and how sickle cell can upset that display intergenerationally. Mohammed specifically invited us to speak to his wife, which, in the context of describing segregation in his home country, is a display that differentiates him from caricatures of Muslim husbands as speaking over and above their wives.
For British fathers, of African, Caribbean or mixed descent, their racialisation by others and the wider racisms they face stand as special pressures to display, including family display. The stigmatising of SCD as a black disease means black people ‘will find it distasteful or not get interested’ (David). The disease is especially disheartening in the context of being a black man in a relationship with his first partner, confirming that genetic knowledge is apprehended in particular social contexts, in this case of an experience of racism, which, it is implied, means that black people may be overwhelmed by further bad news: ‘If (African-Caribbean people) are told, you’ve got this disease, that is demoralising. So again, it’s trying to inform people without hurting their pride or hurting their feelings, or making them feel inadequate’ (George). Black people are said not to be valued (David) and fathers may be disrespected in terms of class, ethnicity and gender simultaneously: ‘I’m not rich. I’m a minority, innit. I’m not a priority, so why are they really going to care? […] it’s like, you’re a man, what do you know basically? That’s how they put it. You don’t know nothing’ (Lewis). Because minority ethnic communities are not rich, and because SCD is ethnicised, it is consequently ‘not much in the public eye’ (George). The fathers felt there are stereotypes of the black father and his alleged lack of commitment to the care of children, and that they had to resist stereotypes more generally:
They were [stereotyping me] but I’m not sure what stereotype. Is it the young black male who’s irresponsible, or is it the ‘Ah, he’s just the baby father’. I’m not sure what stereotype but all I know is it wasn’t very nice, because I’m the type of person, I’ve always been determined to do the right thing. And based on that, if I’m here and I’m making an effort, the least you can do is just, treat me normally. Talk to me. There’s two of us. I mean imagine my partner’s here. All the information’s being thrown at her. She’ll pass the leaflets to me. They’ll answer very briefly and then continue talking to her. And that just makes me think, ah [whispering], maybe I just need to shut up. (James)
One father emphasises his upbringing in a deprived urban neighbourhood and his decision to distance himself socially from that milieu:
I had crack heads walking outside my house 24/7. I had undercover police standing outside my house pretending they were crack heads cos they was monitoring my property where I was brought up. […] If you choose not to go to school because you’re watching people outside your house selling drugs, that’s still your choice. (Isaac)
Ultimately, the pressures deriving from broader social relations, such as poverty and resisting racism, to display family commitment when accounting for their experiences in the process of sickle cell screening, ended in a series of double-binds for the fathers. As Isaac said, black people feel ‘trapped, located and processed’, and antenatal care is a site affording ample opportunities for health staff to consider fathers, note their presence, absence or demeanour, and morally process them. One strategy would be to avoid such situations, and yet fathers’ presence is required in order to display family commitment counter to gender and/or ethnic stereotypes.
As we have seen, the processes of antenatal care may thwart attempts by fathers to display family commitment through exercising informed choice, displaying knowledge and critically interrogating care. In an already gendered space, the politics of biosurveillance is such that fathers only became important to the health professionals for HIV testing or after the mother is identified as a sickle cell carrier, by which time she was already well advanced in pregnancy. Fathers were overwhelmingly in favour of ‘testing’ but this support hides different substantive rationalities. First, testing might be approved but only in the sense of caring for the baby (Ibrahim). Second, testing had qualified approval, but only if pre-conceptual (Mohammed was in favour of pre-relationship testing but not in curtailing choice in partnerships or reproductive choices thereafter), or sufficiently early in pregnancy (Lewis, Suleiman). Third, only where relationships were contested, and the man felt tricked into fatherhood, did a father express support for testing orientated to termination of pregnancy (Kingsley). Having a child with SCD did not mean an opposition to testing and to this end Iyabo and Mark emphasised that their pre-conceptual test results (outside the UK) had proven to be incorrect.
The culmination of these double-binds came when test results showed the father (as well as the mother) to be a sickle cell carrier. The wider social relations in which the fathers found themselves – some belonged to racialised minority groups, some were migrants, others were in low income settings – rendered them in socially precarious positions. They needed to display family to antenatal staff. They underwent a sickle cell test and were then guided to prenatal diagnosis. They wanted the best care for the baby, and clinic health information leaflets referred to ‘tests for the baby’s health’. But newborn screening (early identification and treatment) is for the baby’s health and, as Joshua, who declined PND, pointed out, one can wait and test the baby when born if it is the baby’s health one wishes to aid. The only manner to portray termination as ‘for the baby’s health’ was if professionals emphasised that parents should not wish suffering upon their unborn child.
As I say, they say, if the baby, I mean has the sickle cell, it’s better for me to abort because I mean/
To abort, because to prevent the pain and be good.
The father referred to ‘being good’, as if acceding to PND was morally good behaviour for a father identified as a sickle cell carrier. But PND was not to care for the baby. It was to open the option of termination of pregnancy that few fathers wanted (including one who agreed to a termination). Thus in displaying family in the face of structured social relations, some fathers are in a double-bind: resist sickle cell testing, implying a lack of genetic responsibility or accept testing and face an even more troubled process of resistance to PND.
Conclusion
In this article we considered the case of fathers at sickle cell screening clinics. The alleged lack of fathers’ commitment to such testing has been regarded as a policy problem. However, we did not find such a lack of engagement. On the contrary, as Reed (2011) has suggested, fathers recounting experiences of sickle cell screening were engaged counter to stereotypes. Furthermore, they were cognisant of other ways they are caricatured as lacking family commitment, and this underscored their need for family display.
Fathers reported two main types of display: being there, being hypervisible or else demonstrating the obstacles impeding this commitment; and doing the right thing, efforts to display the ‘correct’ disposition to sickle cell testing. This disposition was to be docile: whether this was to be teachable (learning when to be passive for instruction and when to be responsible in actively seeking knowledge), or in the more restricted sense of being obedient to health advice.
Finch (2007: 76) herself distinguished ‘family displays’ from performance/performativity in three ways: (1) as being orientated to social interaction rather than identity (our fathers seemed more concerned with practical consequences – ensuring care for the mother, avoiding deportation, avoiding unwanted termination of pregnancy, rather than identity construction); (2) as consisting of people simultaneously combining the parts of actor and audience (Jasinder, above, is both an audience for the midwife and her students and an actor for embodied fatherhood to the researcher); and (3) as including conveyance of social meaning that does not entail face-to-face interaction (for example, George and Thomas dutifully carried sickle cell cards stating their test results but with an unknowing sense of responsibility, unsure to what purpose).
Finch (2007) further argued that family display may be of different intensities at different points of time. We also considered the reasons behind the family displays of fathers. One set of reasons seemed to be at the level of biographies: whether the family was reconstituted, whether the mother and father were together, whether or not the baby was planned. Those whose relationships were transnational also had to display as if to overcome the lack of commitment implied by geographical separation. Those with intimate personal connections with SCD had to display to mitigate their imputed culpability for not being active in sickle cell testing. But a second set of reasons related to the wider social contexts: migrant fathers in particular had to display a rejection of presumed African culture or Muslim religion in favour of learning the culture of UK antenatal care, but all minority ethnic fathers were constrained to display counter to racist stereotypes.
Developing Layder (1990) we propose that display work becomes especially acute where the preferred social relationships fathers seek to constitute are ones not readily accommodated within extant social relations. It is presumably at the level of social relationships in situated activity that people ‘do family’ (Morgan, 1996). But ‘the family’ as self-evident has been undermined from a structuralist as well as an interactionist perspective, being conceived as a resultant, a network of relationships that arises from the specific character of the social relations between the state and people (Donzelot, 1979). Thus attempts to display family are constrained by social structures: of racism, of immigration law and of social contexts of deprivation. Displaying family was necessary to overcome racist stereotypes of absent fathers, but structurally more difficult to achieve when employment was insecure, when racism pathologised variation from normative family, when migration created transnational families, when citizenship uncertainties were juxtaposed with pregnancy uncertainties.
In conclusion, there are several ways notions of family display may be extended. First, not all display work can be captured by the sense of family display, even in antenatal settings. The fathers in this study displayed in densely layered ways: displays relating to how to be an employee, how to comport oneself in seeking asylum, how to display a child’s SCD illness to ensure treatment; how to foreground, interrogate or obfuscate knowledge of sickle cell carrier status, as well as how to display fatherhood. Second, in half the interviews, the interviewer’s notes indicate that something has been troubling to the interviewer, but that this has not been reflected in either family displays or other displays. It is conceivable that there is a realm of interest, equivalent to Bhaskar’s (1979) domain of the real, comprising matters of concern that are not actualised as displays because mechanisms fail to trigger in particular contexts or because there are counter-acting forces that disable the mechanisms pertinent to the display. These generated too scarce data to analyse here but we note this for future consideration. Finally, the concept of family display has tended to foreground social relationships, betraying the roots of the concept in interactionist views of family. While this has many advantages in analysing social relationships, it fails to account fully for the social relations of contextual resources and institutional arrangements, which also elicit display work.
Footnotes
Acknowledgements
The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. We would like to thank the research participants, the sickle cell organisations and the two reviewers.
Funding
This article presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme [Grant Reference Number PB-PG-0610-22196].