
Abstract


Finn Smith is a 5-year-old boy with autism spectrum disorder (ASD) and food selectivity. Finn’s mother reports that eating is a challenge because Finn eats a very limited variety of foods. Finn does not consume any vegetables or fruits and consumes only one protein. Most of Finn’s diet includes foods that are crunchy, white, salty, or sweet and of a specific brand. For example, Finn will only eat white donuts if they are from Dunkin’ Donuts. Finn’s mother even brings fresh donuts to the school daily so that Finn’s teachers can serve them to him during lunch. Other foods that Finn will occasionally eat include Lay’s potato chips, Idahoan Buttery Homestyle mashed potatoes, string cheese, and Keebler Club crackers. When Finn’s parents or teachers present new or nonpreferred foods (e.g., store-bought donuts instead of Dunkin’ Donuts), Finn screams, turns his head, and aggresses. Finn’s teachers often must end his lunch early when his behavior becomes too intense. A dietician confirms that Finn is missing many nutrients, and Finn’s constipation has worsened. His pediatrician states that Finn is growing well and that most children go through these stages and eventually “grow out of it.”
Given Finn’s very limited diet, his teachers and caregivers should be concerned that he is not getting the proper nutrients he needs to sustain a healthy lifestyle and growth. Most children eat several meals per day, including foods from different food groups, such as fruits, vegetables, dairy products, proteins, and grains. For many children, eating is an enjoyable activity, not only because humans need food to survive but also because it “tastes good” and represents a meaningful social opportunity (e.g., attending birthday parties, eating with friends at school). In fact, most typical children look forward to eating and demonstrate preferences for a wide variety of foods.
It is common, however, to encounter picky eating as children progress through toddler and school-age years (Mascola, Bryson, & Agras, 2010). For example, children may become selective in terms of the foods they request and, like Finn, even begin refusing foods, like vegetables or fruits. Fortunately, for most, selective eating is a transient problem that will resolve without treatment. Ultimately, most kids go on to eat well-rounded diets that include a variety of foods from all major food groups, and they gain weight and grow normally.
There are many cases, like Finn’s, that are severe enough to diagnose a feeding disorder. Feeding is a complex and dynamic behavior, consisting of many steps that involve both nutritive and protective skills (e.g., accepting and chewing the bite, preparing for safe swallowing, retaining food or liquid in the mouth; Milnes & Piazza, 2013). A child’s growth is dependent on consistent intake of sufficient calories and nutrients. Thus, when a child is refusing to eat, there is a risk for a feeding disorder. Ultimately, practitioners diagnose a feeding disorder when the child fails to maintain nutritional status due to insufficient caloric or nutritional intake or both (Milnes & Piazza, 2013).
One approach to determining the severity of a feeding problem is to compare the child’s feeding behavior with typical developmental feeding patterns (Piazza, 2008). For example, it is typical for children between ages 1 and 5 to display food preferences, to engage in minor food refusal with certain types or textures of foods, and to consume varying amounts of calories from day to day. However, it is atypical for children within this age range to display highly pervasive selective eating, unmanageable levels of problem behavior during meals, and poor growth or nutrient deficiencies (Piazza, 2008). These feeding problems are more severe, persistent, and unlikely to resolve without treatment. Some children exhibit total food refusal and eat little to nothing by mouth, resulting in the need for support from supplemental feedings (e.g., gastrostomy tube feedings). Others exhibit severe and persistent selectivity and will eat only foods of a specific brand (e.g., Pizza Hut), type (e.g., starches), texture (e.g., soft foods), color, temperature, or presentation format (e.g., specific plate).
Unfortunately, medical professionals and researchers do not yet have a full understanding of why feeding disorders develop. Research has shown that child feeding problems do not develop due to one specific condition or event but are the result of a combination of medical conditions, anatomical abnormalities, oral-motor skill deficits, and behavioral factors (Rommel, De Meyer, Feenstra, & Veereman-Wouters, 2003; Volkert & Piazza, 2012). Medical conditions that produce pain or discomfort as a byproduct of eating may result in food refusal. For example, if a child is experiencing pain during eating due to reflux or food allergies, the child may start to refuse all foods to avoid experiencing pain. Children with significant oral-motor delays may not have the ability or stamina to consume food safely. Regardless of the etiology, children can learn to avoid eating by engaging in behavior that is then maintained by social consequences. That is, caregiver (i.e., teacher, parent) responses to child refusal behavior such as attention (e.g., coaxing, reprimands) or removal of nonpreferred foods may inadvertently worsen the problem (Piazza, Fisher et al., 2003).
Studies have shown that feeding problems occur in up to 72% of children with ASD and intellectual and developmental disabilities (Schreck et al., 2004). Therefore, many professionals who work with young children with ASD and other developmental disabilities will need to address food selectivity.
Food Selectivity in Children With ASD
Food selectivity is the most commonly reported feeding problem in children with ASD. Schreck et al. (2004) surveyed 472 caregivers of children between 5 and 12 years of age. They found that 72% of those children diagnosed with ASD had feeding difficulties, significantly higher than same-age peers without ASD.
Unfortunately, little is known about the development and maintenance of food selectivity. One of the defining features of ASD is inflexible, restrictive, or repetitive behavior and insistence on sameness (American Psychiatric Association, 2013). Given the prevalence of food selectivity in this population, it could be that rigid feeding behavior is another manifestation of resistance to change (Shuster, Perry, Bebko, & Toplak, 2013). For example, children with ASD often insist on eating the same foods, wearing the same clothing, or going the same route to and from school every day. Given that life can be unpredictable, many features of the environment cannot be arranged or controlled. For children who are typically developing, sudden changes to routines might be frustrating or temporarily disappointing, but most are able to adapt. For children with ASD, even small changes can be aversive and often lead to problem behavior, such as aggression or self-injury.
Children’s resistance-to-change behavior can be quite challenging for teachers, given that it often results in the teacher having to carefully arrange the child’s environment to avoid disruptions or changes to routines. Teachers also might need to carry out unconventional feeding routines, such as having to prepare special meals for the child, arranging for the child to eat in a separate environment from peers to minimize distraction, or training additional staff to assist with specific meal plans. These alternative feeding plans can present time and resource constraints for teachers and could even put others or the child with ASD in danger if disruptions to the routine result in aggression or self-injury (Auslander, Netzer, & Arad, 2003). Behavioral rigidity may also be stigmatizing and impede the ability of children with ASD to socialize with peers, already a difficult task (Rodriguez, Thompson, Schlichenmeyer, & Stocco, 2012).
For children with food selectivity, immediate health risks may not be apparent if the child is growing and gaining weight normally. Finn, for example, suffers from constipation and nutrient deficiencies but otherwise appears healthy and is growing well. Children who display persistent food selectivity are still at risk for many major health problems because their diets often consist mostly of foods that are high in fat or sodium (e.g., potato chips) or low in nutritional content (e.g., donuts). Inadequate dietary intake and malnutrition could lead to further impairments in cognitive, academic, or behavioral functioning; anemia; compromised immune system; or unhealthy weight gain (Cohen, Piazza, & Navathe, 2006; Latif, Heinz, & Cook, 2002). For example, children who consume meals predominantly composed of high-fat foods are at greater risk for developing severe health problems, such as obesity and type 2 diabetes. If the child’s diet is deficient in micronutrients, such as iron, zinc, and vitamin C, because the child refuses to eat meat, fruits, and vegetables (Sullivan et al., 2002), the child may be at risk for an iron deficiency that may impair brain function and cannot be reversed if left untreated.
For children with food selectivity, immediate health risks may not be apparent if the child is growing and gaining weight normally.
Steps in the Assessment of Food Selectivity
Before attempting to treat Finn’s food selectivity, his teachers should use a data-based approach to objectively assess his behavior, develop a plan, evaluate treatment, and continuously track success. An overview of the assessment and treatment process is presented in Figure 1.
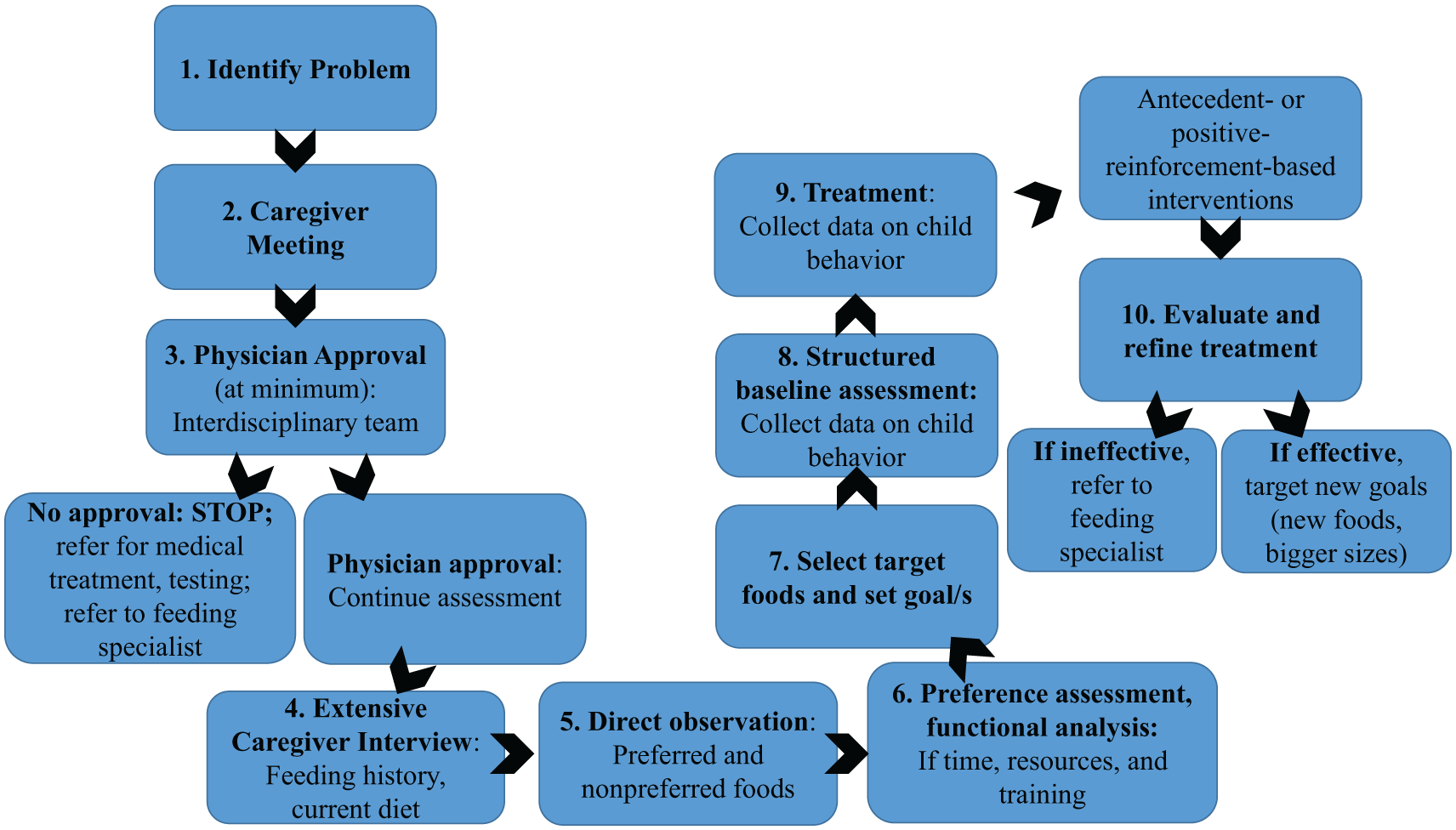
Assessment and Treatment of Food Selectivity
Step 1: Identify the Problem
First, the teacher should define and describe the feeding problem in specific terms, for example, “Finn refuses all novel foods” or “Finn eats only a limited number of junk foods.”
Step 2: Host Caregiver Meeting
In Finn’s case, the teacher should set up a meeting with Finn’s parents to discuss feeding problems at school. If the teacher and parents agree that food selectivity is a significant problem, they should begin the assessment process.
Step 3: Engage Interdisciplinary Approach and Seek Physician Approval
Given the complexity of food selectivity in Finn and many children with ASD, teachers should begin the assessment with an interdisciplinary approach (i.e., gathering input from other professionals), if possible. It is important to consult with various medical and behavioral specialists, given that the health risks associated with food selectivity may not be immediately apparent. Consider Finn’s case, in which his mother required a dietician’s report to understand the impact of his selectivity. Thus, recommendations from an interdisciplinary team are very important.
Potential members of an interdisciplinary team include (a) a physician, to rule out physical or medical contributors to the feeding problem; (b) a dietitian, to evaluate the child’s caloric and nutritional needs and monitor growth; (c) a speech or occupational therapist, to evaluate oral-motor status and safety; and (d) a behavior analyst, to assess the environmental variables affecting child behavior. If teachers are unable to seek advice and recommendations from all members of this interdisciplinary team, at a minimum, they should obtain approval from the child’s physician (e.g., pediatrician) before initiating treatment.
The child’s caregivers should make an appointment with the child’s pediatrician to determine readiness for feeding treatment first. If the physician has concerns, he or she can complete or refer the child for additional medical procedures or consultations. Once testing is complete, the physician can recommend that the teacher (a) proceed with feeding treatment, (b) stop treatment until the child is able to get medical attention, or (c) refer the child to a more intensive feeding program that is able to closely monitor medical, oral-motor, behavioral, nutrition, and growth concerns. Conditions that warrant medical attention include, but are not limited to, children suffering from gastroesophageal reflux disease, children without enteral feedings (tube feedings) who are failing to thrive, children displaying risks for choking or aspiration with or without oral-motor skill deficits, or children with possible or confirmed food allergies. If the child’s caregivers and physician agree there is a need for more intensive treatment, they should reach out to a feeding program. There are only a few programs in the country that specialize in the treatment of pediatric feeding disorders, which include the University of Nebraska Medical Center’s Munroe-Meyer Institute; the Kennedy Krieger Institute at John’s Hopkins Hospital in Baltimore, Maryland; and the Emory University’s Marcus Institute in Atlanta, Georgia.
Step 4: Conduct Extensive Caregiver Interview
After receiving clearance from a physician, the next step in the process is to conduct a more extensive caregiver interview to obtain detailed information about the child’s feeding history and diet. To do this, ask caregivers to record all foods and liquids the child consumes orally over the course of 3 to 5 days. Ask caregivers to be as specific as possible regarding food brands or additives (e.g., butter; see Figure 2 for sample food record). This information helps identify nutritional deficits in the child’s diet (e.g., no protein). Teachers also might use the food record to determine whether the child is following a meal schedule, given that many children with food selectivity “graze” on snacks all day instead of following schedules. See Figure 3 for sample questions.
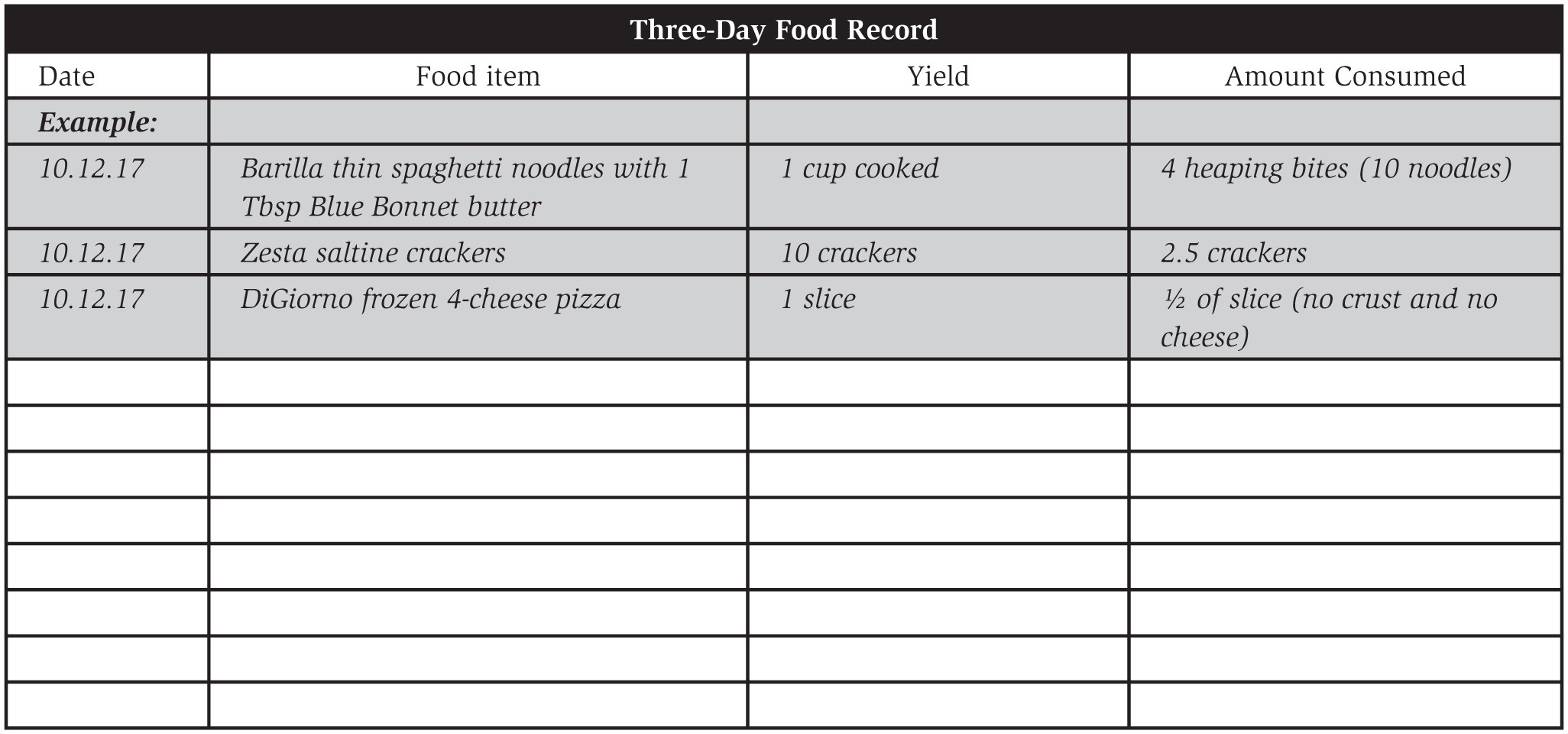
Sample Food Record
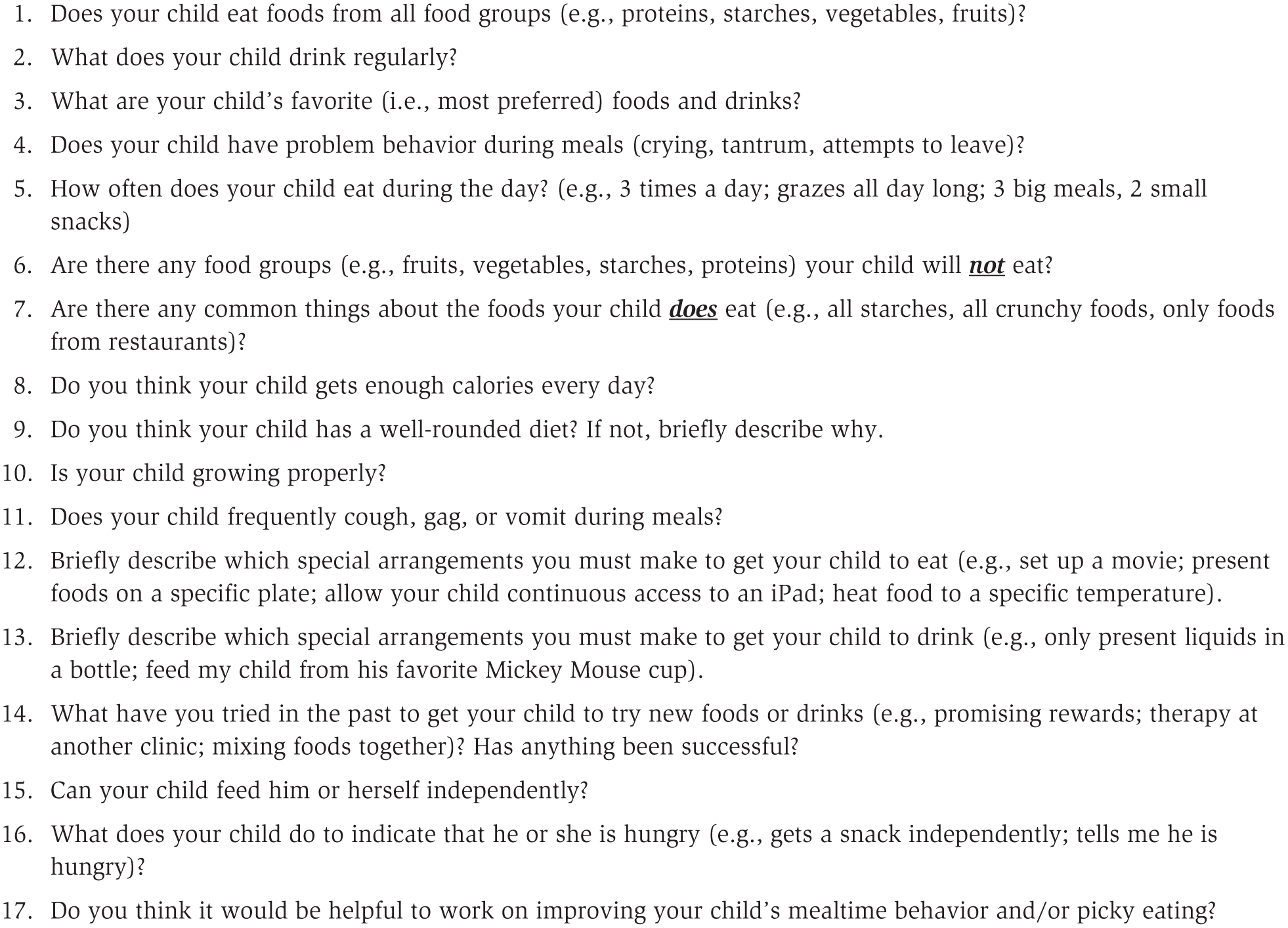
Caregiver Interview Questions
Step 5: Conduct Direct Observation
Next, the teacher can directly observe the child’s mealtime behavior to determine how caregivers respond to challenging behavior. If possible, schedule a time for the caregivers to conduct two small meals with the child: one that includes foods the child consistently eats and one that includes foods the child consistently rejects. In Finn’s case, we might ask his caregivers to present white donuts from Dunkin’ Donuts during the first meal and bites of strawberries during the second meal. These meals provide a snapshot of how the child and caregiver respond and interact during meals, provide helpful insight into what might be reinforcing child behavior (e.g., early meal termination), and show whether the child has any skill deficits (e.g., failure to chew food before swallowing).
Step 6: Conduct Preference Assessment and Functional Analysis
If there is time, conduct additional assessments, such as a paired-item preference assessment (refer to Fisher et al., 1992, for procedural recommendations), to determine which foods the child prefers. For Finn, the teacher could determine which foods he prefers most (e.g., donuts or Lay’s potato chips) relative to other similar items (e.g., Lay’s cheddar potato chips). The teacher could use this information and present highly preferred foods as positive reinforcement during treatment (e.g., “If you take one bite of carrot, you can have a bite of donut”). When possible, conduct a functional analysis of inappropriate mealtime behavior (Piazza et al., 2003). To conduct a functional analysis, use procedures similar to Iwata, Dorsey, Slifer, Bauman, and Richman (1982/1994) with modifications that are relevant to a feeding context (e.g., removal of the spoon during an escape condition; Piazza, Fisher et al., 2003). If teachers do not have the resources, training, or time to conduct a traditional functional analysis, we recommend contacting a behavior analyst with experience in feeding disorders or foregoing this assessment, relying instead on caregiver interview and direct observation of child behavior.
Step 7: Select Target Foods and Set Goals
Next, select target foods and set goals with the caregivers. Ask which foods the child currently does not eat but that the caregivers would like the child to eat. Finn’s parents, for example, might select strawberry, carrot, and ham because Finn currently has no fruits or vegetables in his diet and only one protein. We recommend beginning with a small number of target foods (e.g., one to three). Once the child is successful with a fewer number of foods, implement the same treatment with new foods. It is essential for a physician to approve that the child is not at risk of choking before selecting target foods. If the child is not at risk, teachers should still use small pieces of table-textured foods (e.g., 1/4 by 1/4 by 1/4-inch; pea-sized) or pureed foods to minimize risk of choking during meals.
Set goals with the child’s caregivers that are objective, measurable, and reasonable to achieve. For example, a goal for Finn could be to increase acceptance of bites of carrots to 80% of opportunities across 3 consecutive days. Once the child is successful, teachers may continue to advance and set additional goals. For example, once Finn is consistently accepting, chewing, and swallowing bites of carrot, the teacher can add goals to expand variety and include other food groups or increase volume (e.g., three bites; five bites).
Step 8: Conduct Structured Baseline Assessment
Once goals are established, teachers can conduct a structured baseline assessment of the child’s feeding behavior with the target food or foods selected for treatment. During the structured baseline assessment, the feeder should conduct sessions that consist of a predetermined amount of the target food (e.g., five bites of carrot) according to a fixed-time presentation schedule (e.g., present one bite of carrot to the child every 30 seconds). The feeder should conduct a minimum of three five-bite baseline sessions with each target food separately before starting treatment. Establishing a baseline helps to show whether the treatment is effective. If the child does not accept any bites in baseline but accepts all of the bites during treatment, you now have preliminary evidence that the treatment is working.
Throughout the baseline assessment and treatment, it is essential to collect data on child behavior. First, we recommend purchasing a small food scale or other measuring equipment (e.g., measuring cups, plastic syringe) to calculate amounts of food or liquid. Calculate total amount consumed by carefully weighing or measuring the amount of food presented at the beginning (preweight) and at the end of the meals (postweight). Carefully measure any food that spilled during the meal (onto the floor, child’s lap) and subtract the postweight plus any spill from the preweight to calculate total amount consumed.
Throughout the baseline assessment and treatment, it is essential to collect data on child behavior.
If you do not possess accurate food-measuring equipment, you also can calculate the total number of accepted and swallowed bites during the meal. Acceptance is any instance in which a bite of food (at least the size of a pea or larger) passes the plane of the lips into the child’s mouth within 8 seconds of the bite being presented to the child. For example, the feeder would place one bite of carrot on a spoon inside a bowl in front of the child, along with a verbal prompt for the child to “take a bite.” Acceptance occurs if the child deposits the bite inside his or her mouth within 8 seconds of presentation of the bite. In addition to acceptance, measure mouth clean to determine whether the child swallowed the bite. Mouth clean is when no food larger than a pea remains inside the child’s mouth approximately 30 seconds after the bite entered the mouth, in the absence of expulsion (i.e., spitting food). That is, 30 seconds after the bite entered the child’s mouth, the feeder would say, “Show me ahhh” while modeling an open mouth. To be more accurate, measure mouth cleans instead of swallows. For every bite acceptance, there is only one opportunity to record a mouth clean. Record the total instances in which the child had both acceptance and mouth clean during the meal to get the number of “successful” bites (see Table 1).
Data Collection: Identify “Successful” Bites Based on Whether the Child Accepted the Bite, Displayed Mouth Clean, and Refrained From Engaging in Problem Behavior
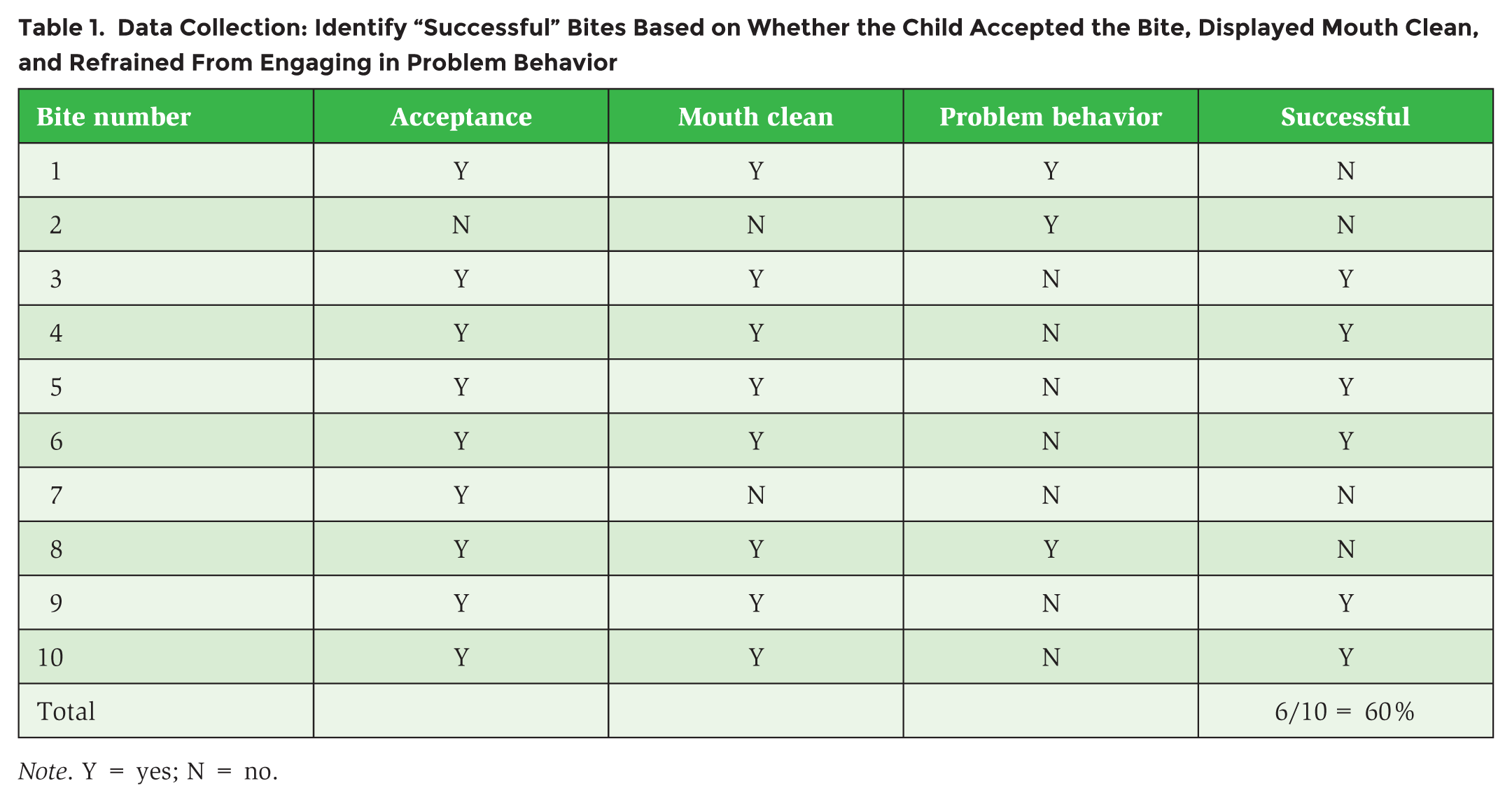
Note. Y = yes; N = no.
Inappropriate mealtime or problem behavior occurs any time the child throws utensils, food, or liquid; aggresses toward others; engages in self-injury (e.g., slaps to the face); engages in negative vocalizations (e.g., crying, shouting no statements above normal conversational tone); flops to the ground; or attempts to leave the chair or table. Teachers may record each time problem behavior occurs or may break the meal apart into separate, smaller intervals (i.e., partial-interval data collection) to determine approximately how often the child engages in problem behavior during the meal. For example, the teacher could break a 20-minute meal into separate 5-minute sections and record yes or no for each interval based on whether problem behavior occurred during the interval (e.g., Minutes 1 to 5, no; Minutes 6 to 10, yes; Minutes 11 to 15, yes; Minutes 16 to 20, no; problem behavior occurred during 50% of the meal). Teachers also could record whether problem behavior occurred during bite presentations (e.g., problem behavior occurred during three of five bite presentations, or 60% of one five-bite session).
Steps in Treatment of Food Selectivity
On the basis of results of the assessment, teachers can develop an individualized treatment plan for the child. According to recent studies, interventions based on applied behavior analysis have the most empirical support as treatment for pediatric feeding disorders (Volkert & Piazza, 2012). Research has shown that the majority of children with feeding problems engage in inappropriate mealtime behavior to escape or avoid bites of novel or nonpreferred foods (Piazza et al., 2003). When escape is the function (cause) of inappropriate mealtime behavior, researchers recommend using escape extinction, which has extensive empirical support (Volkert & Piazza, 2012). In a feeding context, the feeder implements escape extinction using a procedure called nonremoval of the spoon. That is, during structured sessions and across a time-based bite-presentation schedule, the feeder presents the spoon to the child’s lips and follows the child’s lips until the child opens to accept the bite, regardless of inappropriate mealtime behavior.
Even though escape extinction is highly effective, extinction procedures can produce undesirable side effects, such as bursts in problem behavior, emotional responding, or extinction-induced aggression (Lerman, Iwata, & Wallace, 1999). Before using escape extinction to treat food selectivity, teachers should assess whether the conditions warrant this intervention and whether the surrounding environment is safe and appropriate. For example, it may not be appropriate to use escape extinction for children who are larger in stature or older in age, especially if the child has a history of engaging in more severe forms of problem behavior (e.g., aggression, self-injury). In addition, it may be unsafe to implement escape extinction in the middle of a full classroom, where there are many other students and distractions or limited safe-seating options. Finally, if the feeder has not received appropriate training for how to implement escape extinction with high fidelity, he or she could inadvertently worsen the problem over time. Each of these conditions could result in unsafe implementation, placing the child or feeder at risk. For example, without training and knowledge of the child’s medical history, a feeder could unknowingly place the child at risk by continuing to present bites. If Finn was suffering from aspiration, a dangerous condition in which repeated presentation of thin liquid increases the risk of pneumonia, respiratory failure, or even death, escape extinction could be very dangerous. For these reasons, we recommend refraining from conducting intensive procedures if the feeder has not received sufficient training or is not in contact with a behavior analyst with expertise in feeding disorders. In these situations, it is best to rely upon other strategies. There are many other options, given the growing support for antecedent- and positive-reinforcement-based treatments.
Before using escape extinction to treat food selectivity, teachers should assess whether the conditions warrant this intervention and whether the surrounding environment is safe and appropriate.
Step 9: Deliver Antecedent- and Positive-Reinforcement-Based Treatment
First, create a structured mealtime environment, similar to the structured baseline assessment described earlier. Begin by conducting one practice meal per day to work on feeding goals. Initially, there could be an increase in problem behavior, and it may take some time before the child is consistently taking enough bites of new foods to account for a full meal. Given that there are multiple meals across a given day in which the child is expected to eat and consume enough calories for growth, it may be challenging to target every meal all at once. Instead, once the child is successful during one daily practice meal, teachers can incorporate the same routines, structure, and treatment into other meals or provide recommendations for caregivers.
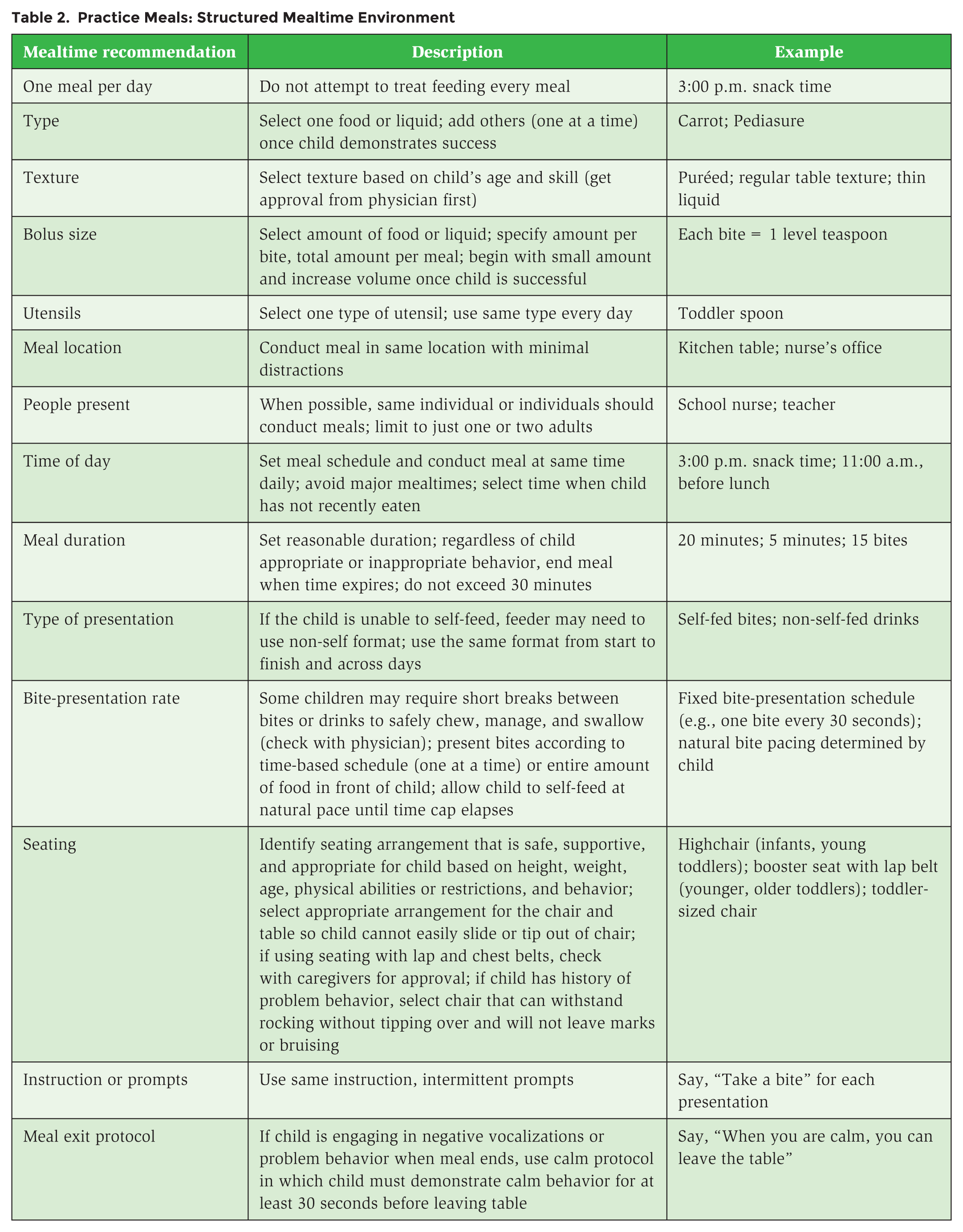
During the practice meal, create a structured mealtime environment that is as predictable and consistent for the child as possible. The structured mealtime environment consists of anything that has to do with the meal, including type, texture, and bolus size of food; utensil; location; people present; time of day; meal duration; presentation type; bite-presentation rate; seating; prompts; instructions; and exit criteria (see Table 2).
Practice Meals: Structured Mealtime Environment
Step 10: Evaluate and Refine Treatment
Collect data on child behavior to evaluate and refine the treatment over time. We encourage the use of single-case design to aid the teacher in determining whether a given treatment produces a change in behavior. With single-case design, one can use repeated observation of the child’s behavior to understand the treatment effects. Graphing and single-case design are beyond the scope of this article, but readers are encouraged to access tools about graphing and single-case design methods (e.g., Dixon et al., 2009).
If structuring the mealtime does not produce a change in behavior, refining the intervention to incorporate other antecedent-based strategies may help. For example, stimulus and demand fading in the treatment of feeding problems may involve gradually changing the concentration of preferred and nonpreferred foods (e.g., Mueller, Piazza, Patel, Kelley, & Pruett, 2004). Stimulus fading also may involve the gradual change of other stimulus features that may be aversive for the child, such as texture, amount, number of bites, or visual appearance of the food. For example, Patel, Piazza, Kelly, Ochsner, and Santana (2001) discovered that a child with a feeding disorder would drink water but not Carnation Instant Breakfast mixed with milk. Therefore, they gradually added Carnation Instant Breakfast in 5% to 10% increments to the water. Once the child was consuming 100% of the concentration of water mixed with Carnation Instant Breakfast, the authors faded the amount of water from the presentations while gradually adding milk to the presentations in 10% increments until the child was successful. Najdowski, Wallace, Doney, and Ghezzi (2003) presented an entire plate of highly preferred food contingent on a child’s taking one bite of nonpreferred food. Over time, the authors increased the number of nonpreferred bites and decreased the amount of preferred food as the child began consuming the nonpreferred food.
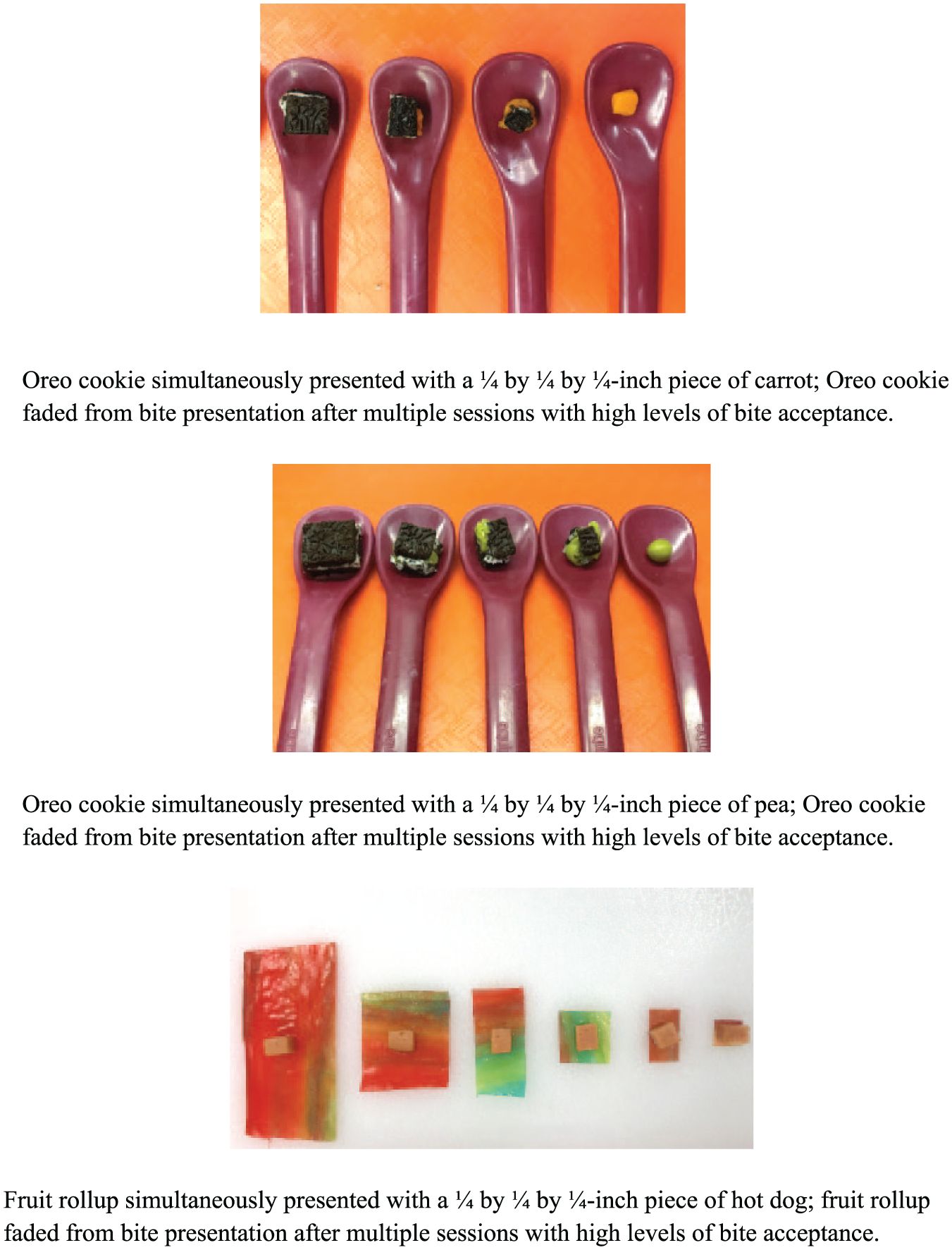
Simultaneous presentation is another antecedent intervention that involves presenting a novel or nonpreferred food at the same time as presenting a bite of familiar or preferred food. For example, during a simultaneous presentation treatment, the feeder might present one bite of carrot (novel food) at the same time and on the same spoon as a bite of donut (one of Finn’s familiar foods). The feeder can cover the target food with the familiar food or place them side by side (see Figure 4). Ahearn (2003) increased vegetable consumption in a child with ASD by presenting a bite of vegetable simultaneously with preferred condiments (e.g., ketchup, ranch dressing). Piazza et al. (2002) found similar results in that simultaneous presentation (e.g., a chip presented on top of broccoli) led to an increase in broccoli consumption for two participants.
Simultaneous Presentation and Stimulus-Fading Steps
Given that it might be inappropriate to simultaneously present foods long term, teachers may combine stimulus fading with simultaneous presentation. That is, once the child is readily accepting and swallowing simultaneously presented bites, fade the amount of the familiar food from the presentation. Recently, our research team was able to increase consumption of three novel foods for two children with ASD and food selectivity using a combination of simultaneous presentation and stimulus fading (Peterson, Ibañez, Kirkwood, Crowley, & Piazza, 2018). For one participant, we simultaneously presented bites of target foods (pea, green bean, or apple) with bites of a familiar food (Oreo cookie) and observed high levels of consumption. We faded the amount of Oreo across presentations (i.e., reduced the size of Oreo on the spoon). As the child demonstrated mastery at each fading step, we moved onto the next step until the Oreo cookie was no longer present, but the child continued to consume bites of the target foods alone. We replicated this effect with a second participant across his foods (macaroni and cheese, hot dog, corn) and a familiar food (fruit rollup; see Figure 4 for examples).
In addition to or instead of antecedent interventions, teachers could evaluate positive reinforcement. Peterson, Volkert, and Zeleny (2015) increased two children’s acceptance of nonpreferred liquids from a cup using differential reinforcement of alternative behavior. Specifically, these researchers provided access to highly preferred toys immediately following drink acceptance, which resulted in an increase in acceptance.
Teachers should include positive reinforcement when possible. Within a positive reinforcement treatment, teachers could provide the child access to highly preferred toys, foods, drinks, or activities contingent on successful bites (e.g., “If you take one bite of strawberry, you can play on the iPad!”). If using positive reinforcement, teachers should withhold access to the reinforcers during other times so the child is highly motivated to work for the item. Keep the items out of reach and stored in a secure location until ready to conduct the meal. If using food reinforcers, teachers should not select a food the child relies on for calories, given the child’s diet is likely very limited. For example, if the child eats only macaroni and cheese for all three daily meals, select a different food or item to use as a reinforcer. In addition, moderate the amount of time or the size of the reinforcer (e.g., one potato chip instead of an entire bag; 30 seconds access to a highly preferred toy) so that the child does not quickly satiate on the items (i.e., become bored or full). Given that child preferences for foods or toys shift often, rotate reinforcers frequently. Finally, present the reinforcer immediately after the child engages in the desirable behavior for maximal effects and provide enthusiastic praise (e.g., “Wow! You did it! You get to play with the trains!”). If neither antecedent- nor positive-reinforcement-based interventions are effective, teachers should refer the child to a specialized feeding program.
Conclusion
Recall that for children with ASD, conclusions are unclear regarding how and why food selectivity develops. These children often insist on sameness of meal routines, display rigidity with the type or texture of foods, and engage in challenging behavior with novel foods. For children with food selectivity and ASD, an interdisciplinary approach to assessment and treatment works best. Given that feeding disorders are often the result of a combination of factors (e.g., medical, behavioral), at a minimum, consult with the child’s physician to determine whether there are any ongoing medical concerns that would preclude the child from participating in treatment.
Starting small by setting a reasonable number of goals with only a few target foods increases chances of success. Conducting just one practice meal per day is a great way to begin introducing new foods into the child’s diet without making things too challenging or overwhelming. It is essential to collect data on child behavior throughout structured baseline and treatment evaluations to determine whether the treatment is effective. Currently, there are many empirically supported interventions based on principles of behavior analysis. Use antecedent- or positive-reinforcement-based procedures first, especially if the child is older or larger or the teacher does not have training in other interventions. Teachers should not attempt intensive procedures alone unless they are board-certified behavior analysts with training in pediatric feeding disorders or are closely supervised by an individual with these credentials.