
Abstract
Material selection in orthotic and prosthetic practice directly affects wear comfort, and thus treatment efficacy and adherence. In the pressure therapy of hypertrophic scars, insert materials made of thermoplastic (e.g. Plastazote®) are often placed underneath pressure garments to increase the local pressure for effective scar treatment. However, the currently used insert materials are barely breathable and quite uncomfortable. In this study, spacer fabric is proposed as a potential insert material. The physical properties and compression behaviour of five types of spacer fabrics are evaluated. The pressure delivered by the pressure gloves and spacer fabric inserts onto the hands of 10 subjects are measured. The results show that the spacer fabrics are not only able to provide much lower air resistance (0.05–0.12 kPa s/m) and higher water vapour transmission rate (34.35–102.39 g/h·m2) than Plastazote®, but also produce an interfacial pressure that is comparable to Plastazote® at various locations on the hand dorsum. The results of a 24-week clinical study in which spacer fabric inserts are applied to four hypertrophic scarred hands also support that the inserts are found to be effective in scar treatment by providing good comfort and breathability, and hence pressure treatment acceptance and compliance are increased.
In rehabilitation treatment, materials which include leather, metal, wood, plastics, composites and viscoelastic polymer are commonly used in the practice of orthotics and prosthetics. 1 As they can be easily moulded and adjusted for custom fits, thermoplastics, such as acrylic, polyethylene, polypropylene, etc., are widely used for orthoses and prostheses. Traditionally, the aim in the selection of material fabrication was to optimise functional performance and intended outcome of rehabilitation treatment, but not compromise much of the wearing comfort and treatment adherence. Materials with high rigidity have better stability and are less likely to deform during wear, thus providing a better supporting quality, but lower tolerance to wear.2,3 Soft thermoplastic materials are regularly used as cushioning padding to relieve pain and maintain suitable interfacial pressure between the body and orthoses.4,5 However, many of the materials used retain heat and cause perspiration problems.
Pressure therapy garments are a non-invasive treatment for hypertrophic scars that are caused by burn or scald injuries. A continuous pressure of 25 mmHg can inhibit the growth of scars and increase their maturation.6–8 The recommended range of pressure garment therapy is 25–40 mmHg. 9 Positive clinical results are also reported with pressure levels as low as 15 mmHg.10–12 The pressure garment alone is often insufficient to deliver the desired pressure to actively growing scars, especially in some of the anatomical zones with concave curvature. Therefore, insert materials are supplemented and added to the pressure garment to provide additional compression for treating hypertrophic scars that are actively growing or located on areas that the pressure garment may have difficulties in delivering enough pressure. Thermoplastic (for example, Plastazote®), foam, silicone gel sheets and hydrogels are the most commonly used insert materials that fit under pressure garments for increasing the local pressure.13,14 As the pressure garment and the insert have to conform to body shape and be worn continuously (24 hours a day), the insert materials are required to be resilient, elastic, durable and comfortable. Frequent modifications on the shape of the inserts are required to fit them to the changes of the scars. Yip et al. 15 provided an innovative suggestion of using Lego® as the insert material. Lego® is hard and rigid enough to provide a high degree of pressure and can easily combine to form different shapes to suit the scars. However, the rigid material can be difficult to fit the onto body parts that have high curvature and is uncomfortable. Therefore, relatively softer materials, such as foam, are crucial in providing a certain amount of flexibility to conform to body contours. Yelvington et al. 16 suggested the use of neoprene to make patches or splints for scar management and its effectiveness in treating hypertrophic scars was also proven. Nevertheless, an ideal pressure therapy should provide an adequate amount of pressure to treat scars with minimal and acceptable discomfort so as to maintain the therapy compliance of patients. The poor air permeability, moisture absorbance and wicking properties of traditional insert materials, however, cause patients to perspire as heat builds up and, hence, affect adherence to treatment.
Recently, the use of spacer fabrics has gained a great deal of attention. There are many studies on the unique structure of spacer fabrics and the relation with physical and mechanical properties. 17–20 The three-dimensional fabric structure of spacer fabrics consists of two surface layers and a connection layer (Figure 1). The surface layers are connected by pile yarns or filaments which use tuck stitches to form the connection layer. Spacer fabrics exhibit good compression ability and create a moisture free environment with high breathability. A recent study on the development of functional fabrics for pressure ulcer prevention indicated that the superior wicking ability of channelled polyester makes it ideal for the warp, pile and the top weft in the spacer structure, whilst cotton fibres are used as the bottom weft to improve fabric comfort by trapping the moisture delivered from the top layer.
21
Unfortunately, very little research work has been done on the clinical applications of 3D spacer fabrics. This study, therefore, aims to use weft-knitted spacer fabrics for the fabrication of pressure inserts to enhance the quality of pressure therapy treatment for hypertrophic scars.
Spacer fabric.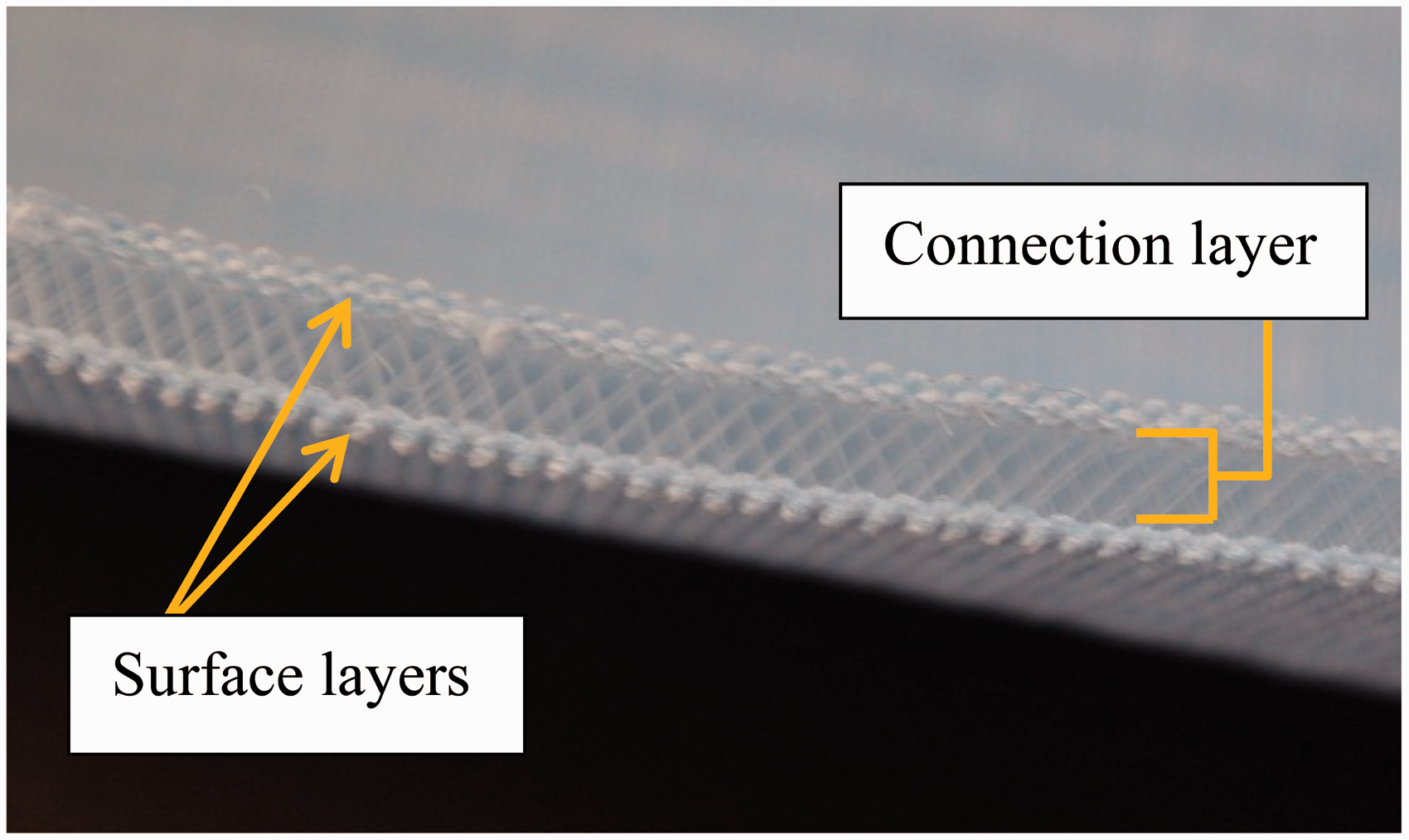
Experimental details
Samples
A 68/32 nylon/spandex powernet fabric which is currently used by clinicians and manufacturers to make pressure therapy garments was purchased for making the pressure glove samples in this study. A reduction factor (RF) of a pressure garment refers to the amount of reduction in circumferential dimensions from the actual measurement of body. Pressure therapy garments are usual made with a RF range from 10% to 20% to give a suitable pressure. However, a high RF (e.g. 20%) of pressure therapy glove can affect finger dexterity and wearing comfort.
22
In this study, low RFs of 5%, 10% and 15% were applied on pattern construction to evaluate the effect of insert materials on pressure delivery. The pressure glove samples were tailor-made for each subject based on their actual hand dimensions. All of the gloves had the same design with open fingertips. A 4 cm × 4 cm square was marked on the hand dorsal side of each glove to identify the location to place the insert and measure the interfacial pressure (Figure 2).
Interfacial pressure measurement locations.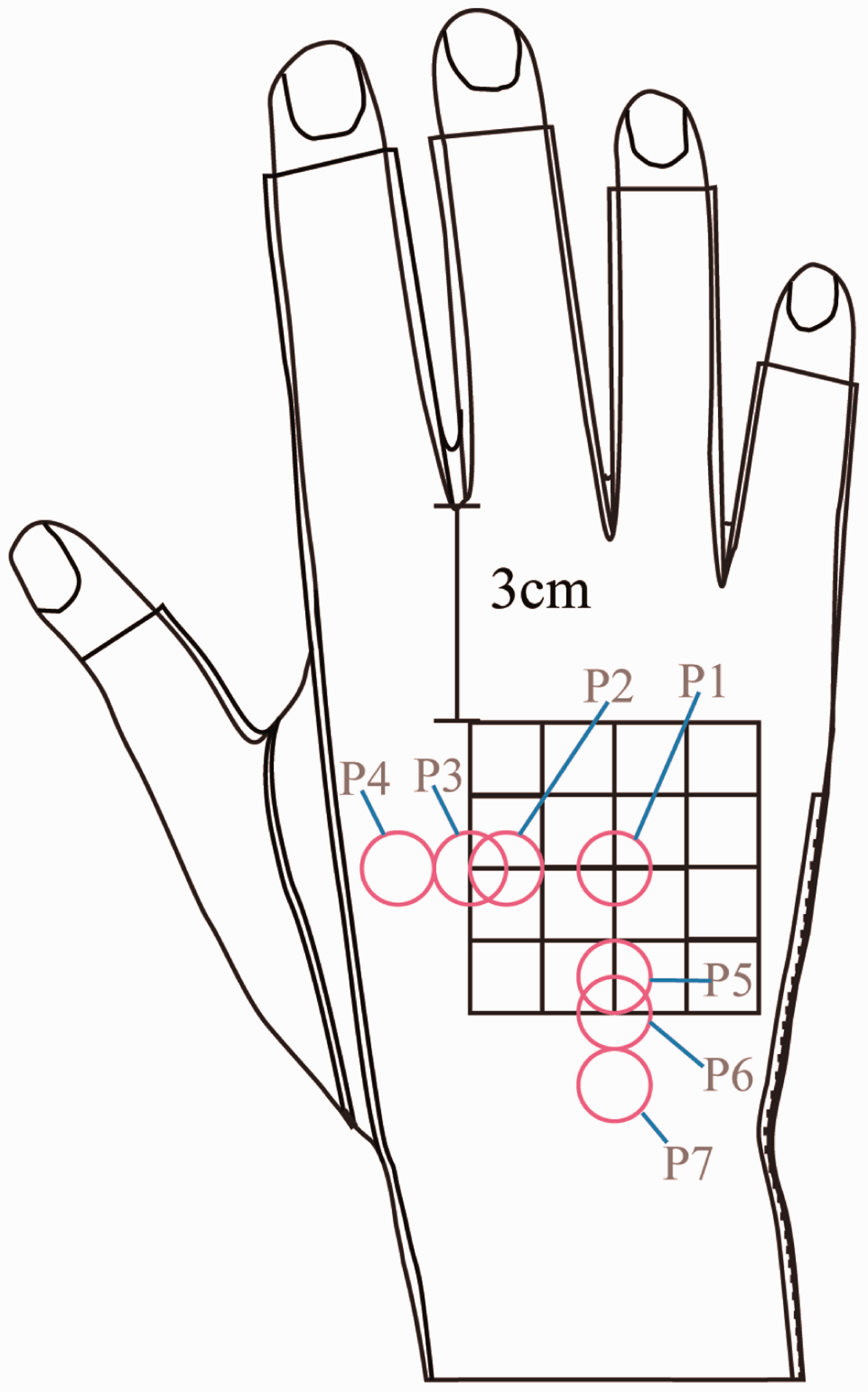
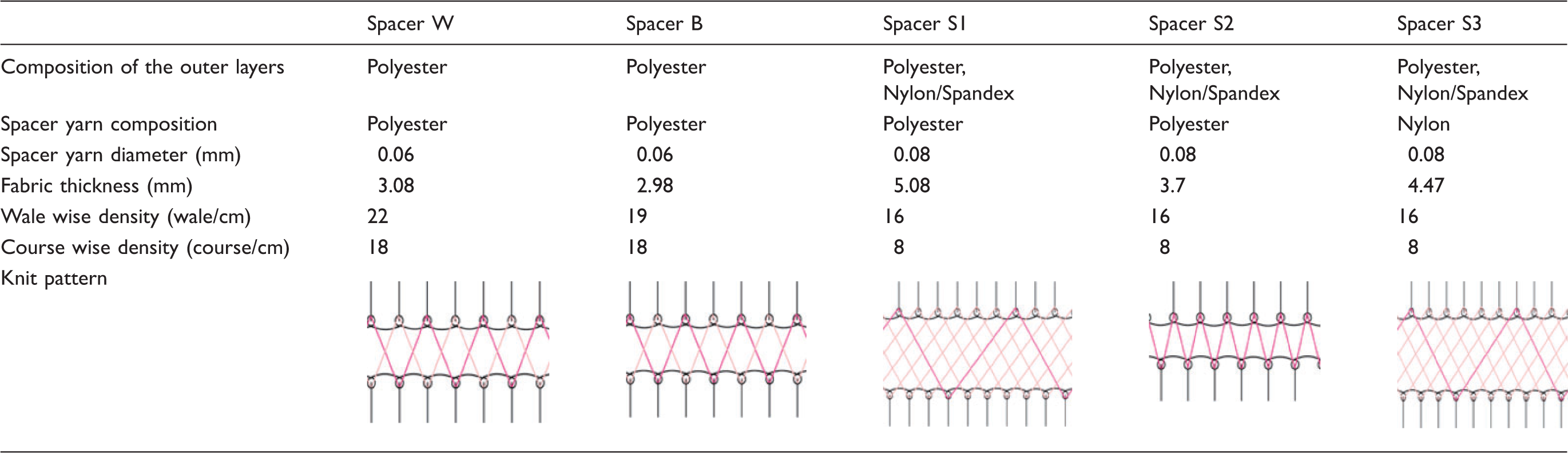
Specifications of spacer fabric samples
Physical properties, such as air permeability, water vapour transmission rate (WVTR) and surface properties of insert materials have been proven to have significant impacts on wearing comfort,23–25 whilst fabric compression properties contribute to the pressure delivering ability and thus affect treatment efficacy. In this study, fabric air permeability was measured by using a KES-F8-API air permeability tester from the Kawabata Standard Evaluation System (Kato Tech Co., Ltd., Japan). The WVTR was measured in accordance with the ASTM E96 upright cup method. The surface properties were measured by using a KES-FB4 automatic surface tester. The compression property was measured by using a KES-FB3 automatic compression tester. The compression test was carried at a speed of 0.08 mm/s with maximum compression stress of 250 gf/cm2. The compression stress (ɛ) is defined as the load applied divided by the area. The strain (σ) is defined as the difference between current and the original specimen thickness divided by the original specimen thickness. The compression strength is corresponding to the points on a stress–strain curve (ɛ, σ). The maximum compression force for standard measurement of normal fabric is 50 gf/cm2. As spacer fabric and Plastazote is much thicker than a normal single-layer fabric, a higher compression force is needed to understand their compression strength.
Interfacial pressure measurement
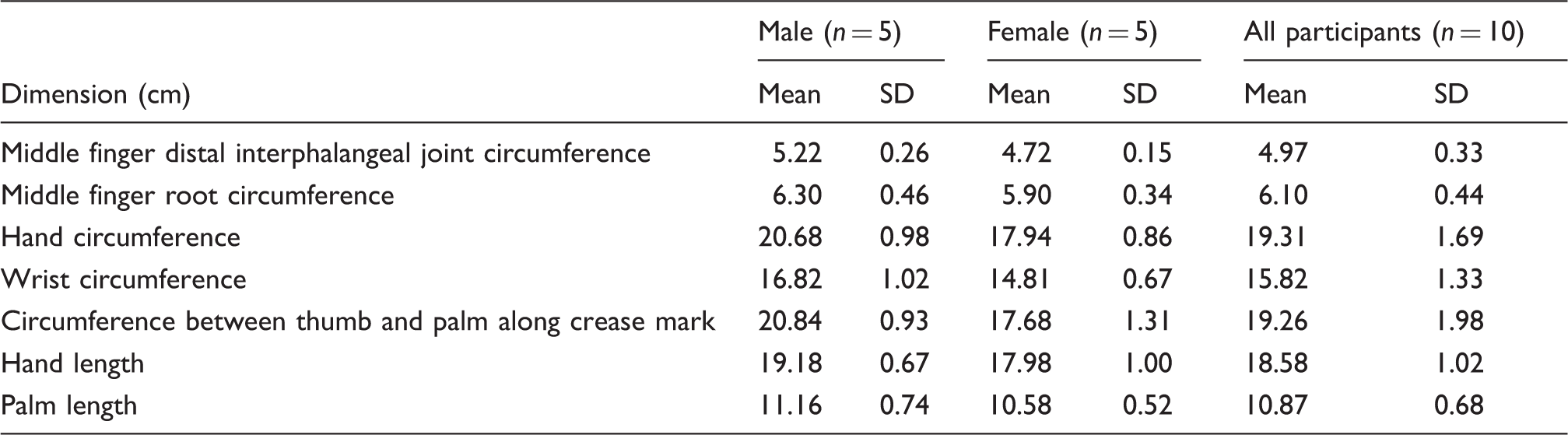
Hand anthropometric information of participants
The pressure delivery of each of the three pressure gloves inserted with the five different types of spacer fabrics and Plastazote® as well as that of a control (pressure glove only) was measured. The insert materials were prepared as a 4 cm × 4 cm square and placed in between the hand of the subjects and pressure glove under the marked location. A pressure sensor (Pliance X system, Novel, Germany) which has been validated in the measuring of interfacial pressure given by pressure garments was adopted (Figure 3).
26
The sensor consisted of a circular sensing area with a diameter of 10 mm (area = 78.54 mm2) and thickness of 0.95 mm. The pressure delivered by the glove and the insert materials in seven locations (see Figure 2) was measured by the pressure sensor. During the measuring of the interfacial pressure, the subjects were asked to perform three hand motions which included relaxing the hand on a table, holding a cylinder of 6.3 cm in diameter and clenching their fist.
Setting for interfacial pressure measurement.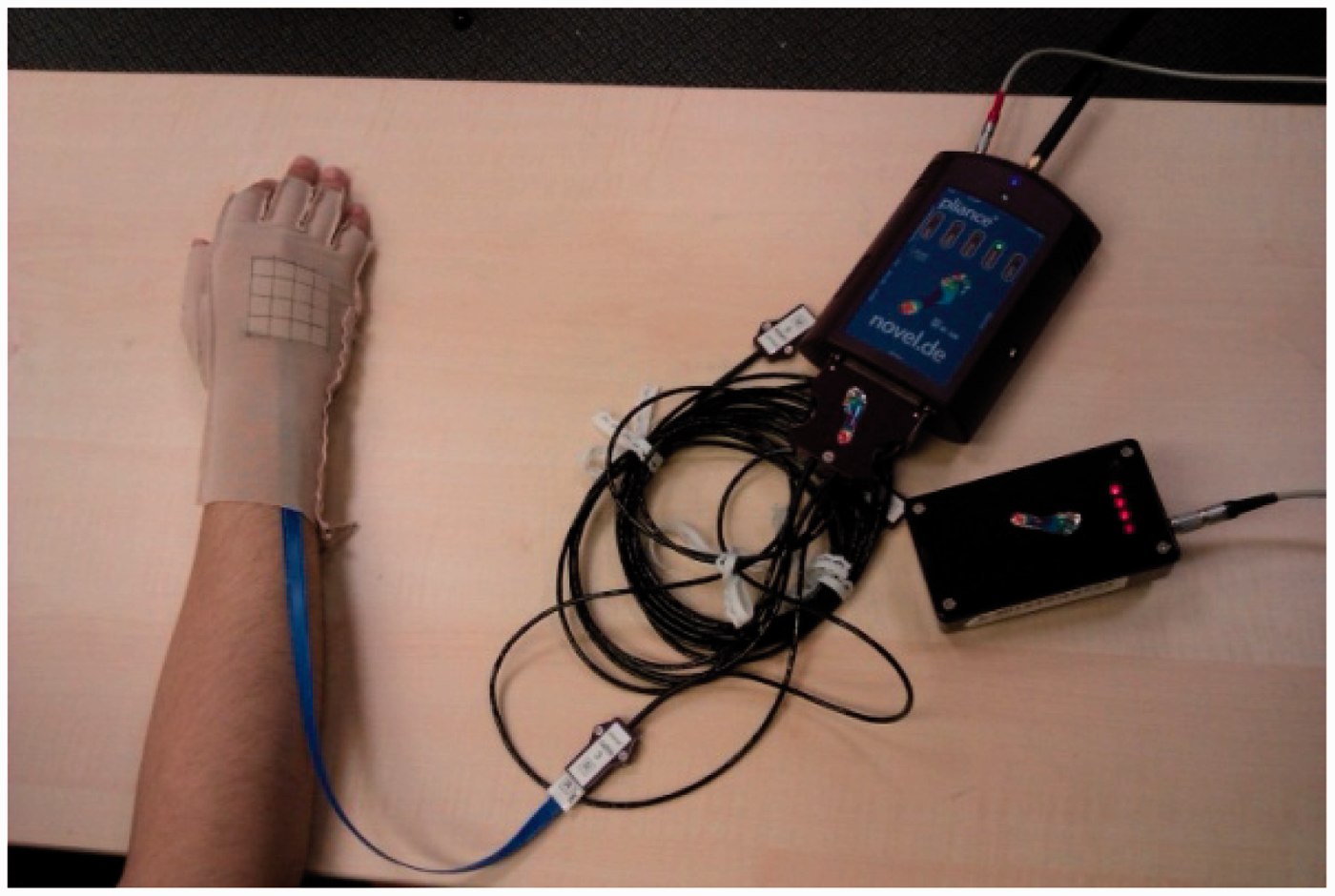
Clinical study
A clinical wear trial of an insert made with one of the spacer fabrics was carried out to examine the effectiveness on scar healing and the subjective feelings of the wearers toward the insert. A 24 week study on each subject was carried out. The study was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee prior to beginning the study.
Original modality and the use of textile insert in the treatment of hypertrophic scars
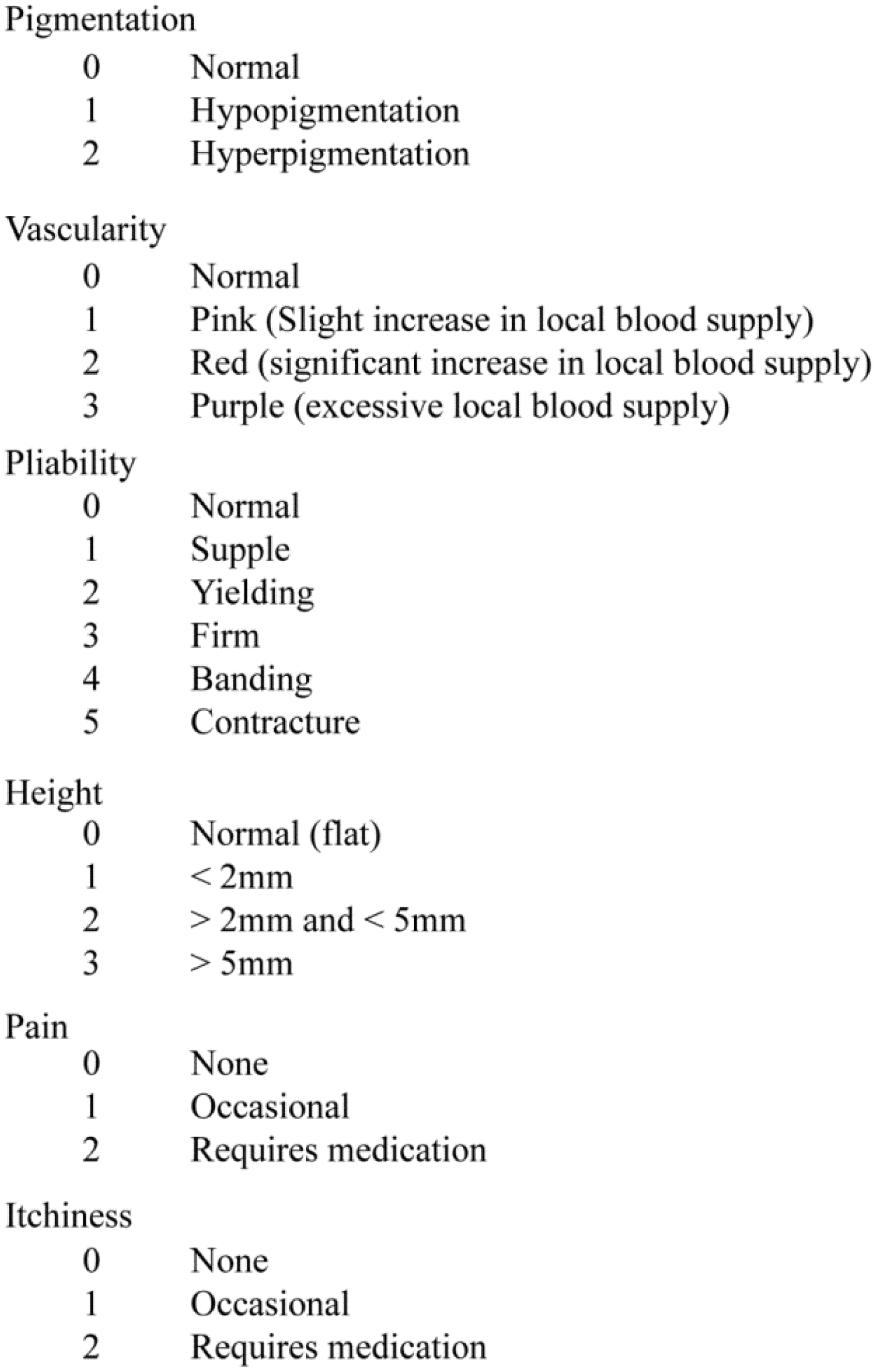
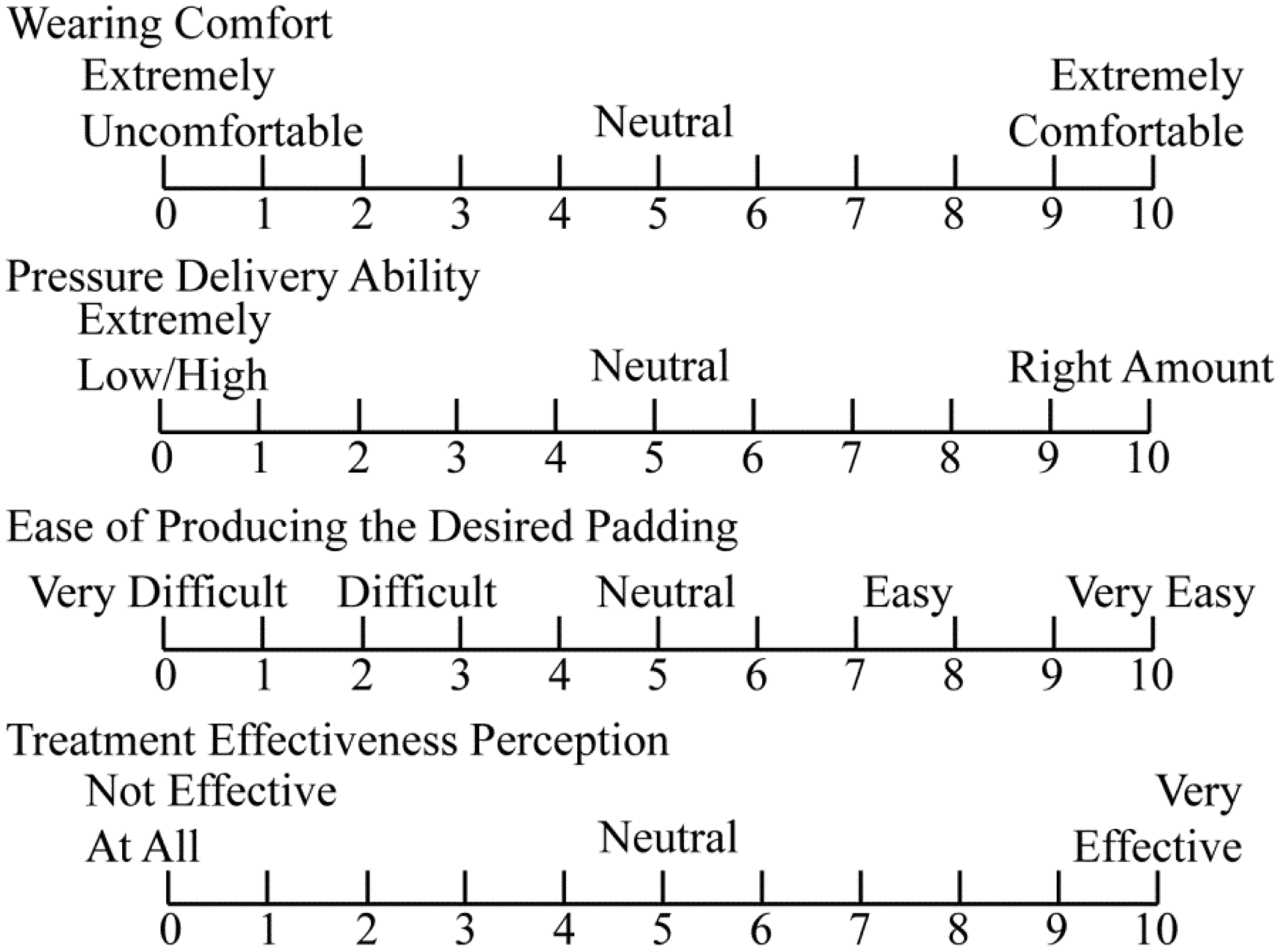
The participants were firstly requested to give a rating for their original treatment modality on the perception of fit, breathability, comfort, effectiveness of the insert, willingness to wear the inserts and perception of ease of hand motion respectively by using 11-point Likert scales (Figure 4). At every 4 weeks of the clinical study, scar conditions were assessed in terms of pigmentation, vascularity, pliability and height in accordance with the Vancouver Scar Scale (VSS) (Figure 5) conducted by the same occupational therapist. Assessments by the patients on pain and itchiness caused by the scars were also recorded. After 24 weeks of treatment with the spacer fabric insert, the participants were further invited to give a rating for the textile inserts. In addition, the occupational therapist who participated in the present study was also invited to assess the functional performance of the Plastazote® and spacer fabric inserts, see Figure 6.
Perception scales for hypertrophic scar patients for rating the use of inserts underneath the pressure therapy gloves. Vancouver Scar Scale for assessment of scar conditions. Perception scales for occupational therapist for rating Plastazote® and spacer fabric inserts.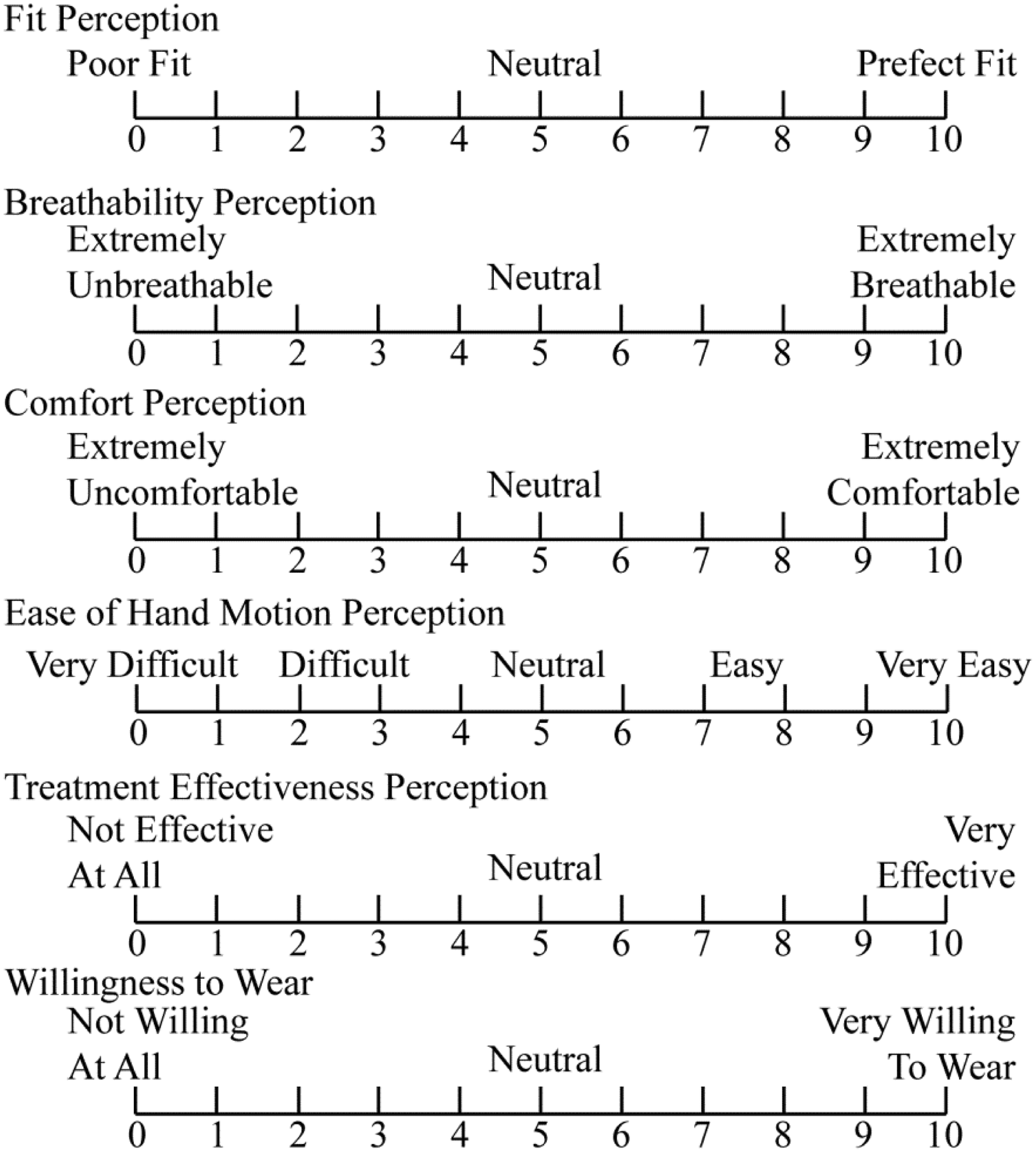
Results and discussion
Physical and mechanical properties of spacer fabrics
Physical properties of spacer fabrics and Plastazote®
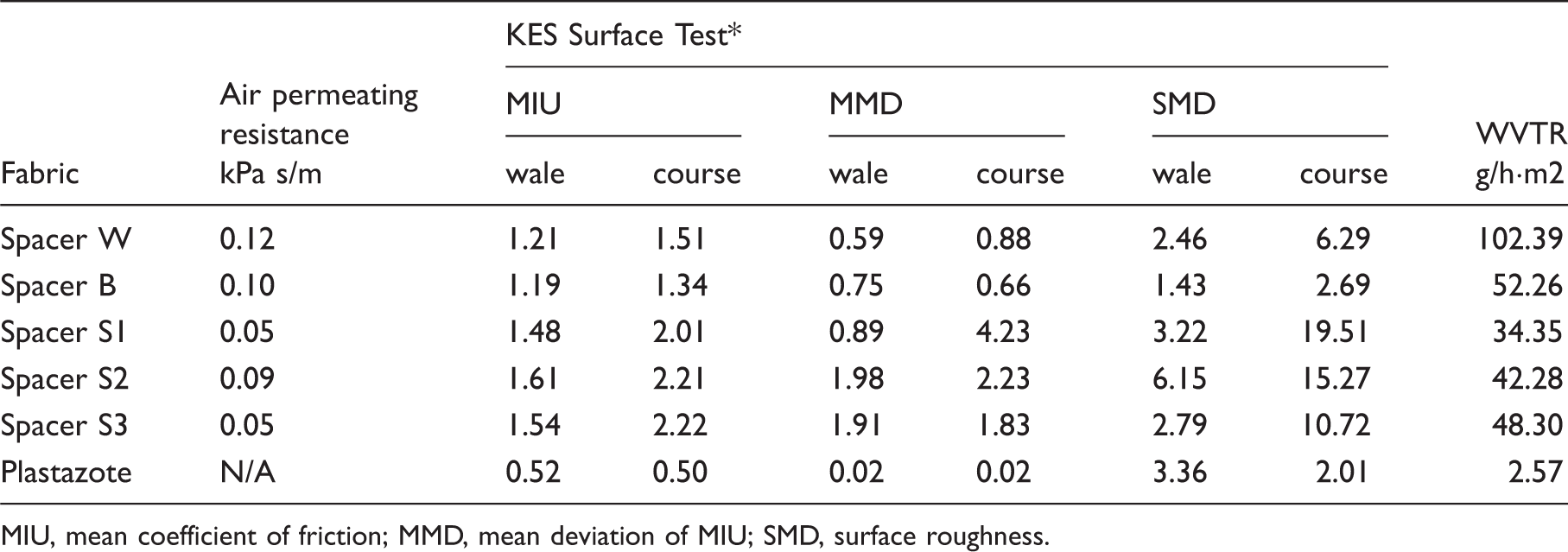
MIU, mean coefficient of friction; MMD, mean deviation of MIU; SMD, surface roughness.
An insert for pressure therapy that exhibits good air permeability can promote ventilation in the micro-climate under a pressure garment. The air permeating resistance of the five types of spacer fabrics ranges from 0.05 to 0.12 kPa s/m which excel the non-air-permeable Plastazote®. Amongst the five types of spacer fabrics, spacer W has the lowest air permeability. Spacers S1 and S3 are relatively thick fabrics with the same fabric structure, thus giving the best air permeability, even though they have different connections in yarn composition. Spacer S2, which differs from spacer S1 only in the structure of the connection layer and fabric thickness, has lower air permeability than spacer S1.
With high WVTR, heat and moisture can be transported away from the skin, thus improving the wearing comfort, especially in hot and humid weather. Spacer W has the highest WVTR of 102.39 g/h·m2. Even the fabric with the lowest WVTR, spacer S1, can transmit moisture at 34.35 g/h·m2 whereas the WVTR of Plastazote® is only 2.57 g/h·m2. Since it is a thinner fabric, the WVTR of Spacer S2 is better than spacer S1. The WVTR of the spacer fabric that uses nylon monofilament (spacer S3) as the connection yarn is higher than that which uses polyester (spacer S1).
A soft and smooth surface of the insert materials provides better comfort when in contact with the hand and avoids inflicting pain on the surface of the delicate scars during wearing. The surface friction and roughness of spacers W and B are relatively lower. The surface roughness of spacers S1, S2 and S3, especially in the course direction, is much higher. Spacers W and B have a higher fabric density and their connection layers are made of finer monofilaments, and the surface roughness caused by the tuck stitches of the connection layers is reduced. These two fabrics thus have a smoother surface but some of the air permeability is sacrificed. With reference to spacers S1 and S3, the surface roughness is also decreased due to the use of nylon monofilament. Spacer S2 has a higher surface roughness in the wale direction and surface friction in both directions as opposed to spacer S1.
One of the most commonly used insert materials, Plastazote®, has good surface smoothness, but is nearly non-air-permeable with a very low WVTR. The spacer fabrics that are recommended in the present study as a replacement have much better air permeability and WVTR when compared with Plastazote®. The spacer fabrics can provide good moisture transmission and air permeability to transport away moisture, sweat and heat from the skin so as to provide better wearing comfort.
Compression behaviour of spacer fabrics
An insert was placed underneath a pressure therapy glove and bore the compression force applied by the glove. The fabric with higher compression strength can better maintain the thickness of the insert and the amount of pressure delivery. From the compression stress–strain curves as shown in Figure 7, spacer S3 gives the best compression strength amongst the five types of spacer fabrics at a compression stress less than 50 gf/cm2. During the compression of the fabric at a force up to 250 gf/cm2, spacer S3 shows a stress–strain behaviour that has a typical compression performance for a spacer fabric. A gentler slope is observed at the initial stage of compression. In a spacer fabric, the outer and the connection layers are not tightly constrained against each other. The initial change of the fabric strain is caused by tightening the loosely compacted layers. When the compression further increases, the slope of the curve becomes steep, thus showing a stiffer behaviour. The monofilament and the crossing structure of the connection layer form a support against the compression force. A large increase of stress is needed to buckle the monofilament for further compression. The stress–strain curve of spacer S3 reaches the plateau stage at a stress of 160 gf/cm2. The nearly constant compression stress is caused by the shearing and shifting of the monofilament in the connection layer, which result in a great reduction in thickness and the collapse of the connection layer. At the end of this stage, more than half of the thickness of spacer S3 is reduced. After that, the stress rapidly increases again for the compression of the surface fabric layers and the monofilament of the collapsed connection layer. The other four types of spacer fabrics do not reach the plateau stage at the compression stress up to 250 gf/cm2. Spacer S3 was fabricated by using the same machine setting, fabric structure and surface layer yarns as those of spacer S1. The only difference was in the monofilament, which was used to compose the connection layer. Spacer S3 was changed to the use of nylon monofilament with the same diameter. The compression property was thus altered. With the use of nylon monofilament, spacer S3 gives a good compression strength at a low force of compression, but the connection layer collapses at the lowest compression stress amongst the five types of fabrics.
Compression stress–strain curves of the five spacer fabrics and Plastazote®.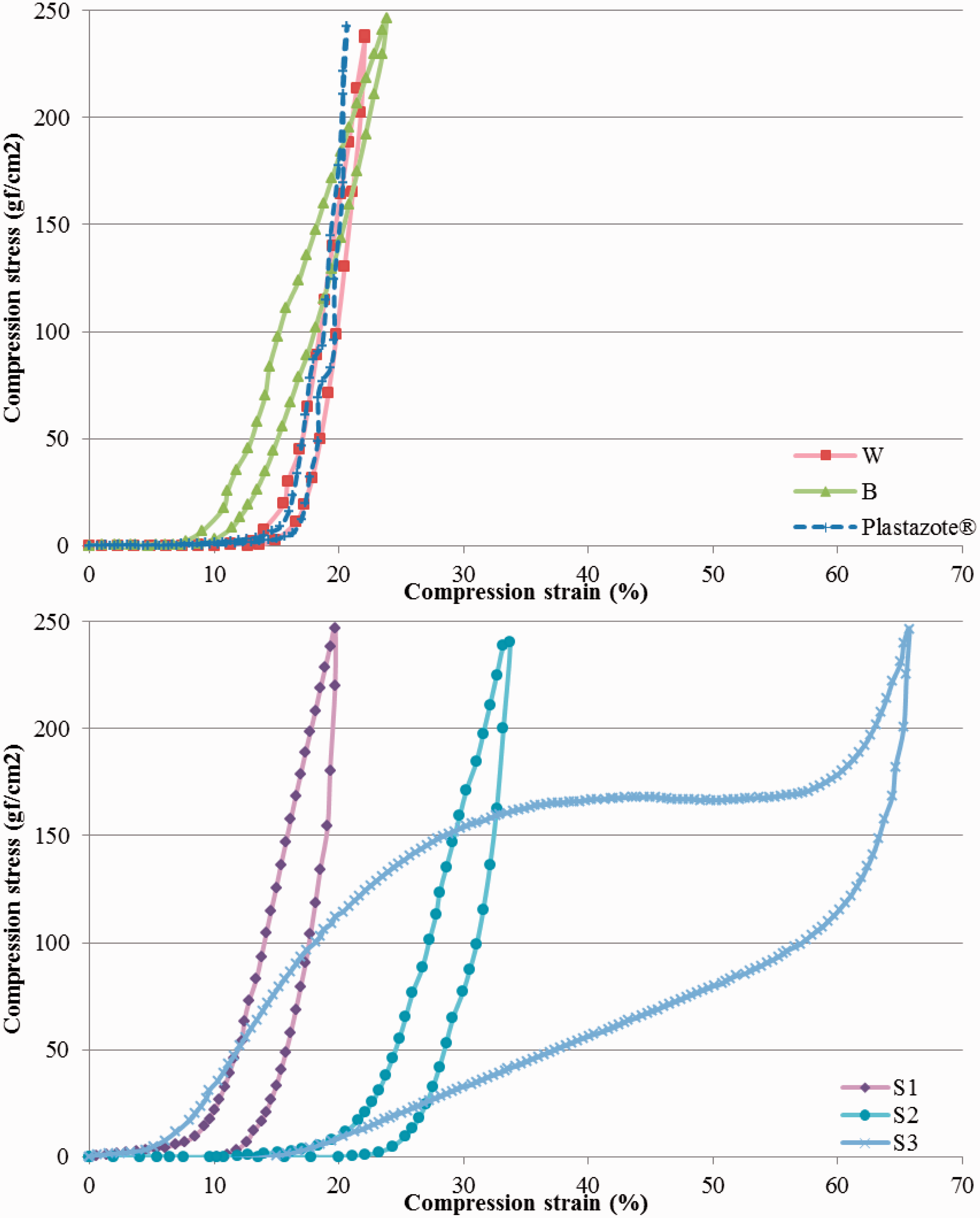
With regard to the other four types of spacer fabrics, spacer S2 has the lowest compression strength. Since it is a thicker fabric and used a monofilament with a large diameter, spacer S2 shows a compression strength that is even lower than that of spacers W and B. One of the reasons could be its lower course and wale fabric densities. A higher fabric density allows a denser composition of the monofilament in the connection layer, so as to provide strong support against compression. The compression property of spacer fabric is related to fabric density. Apart from this, the connection structure of spacer S2 is formed by the tuck stitch in every needle of the rib gaiting and hence involves only one monofilament in the formation of each fabric course. Spacers W and B are produced by interlock gaiting and involve two monofilaments in the formation of each fabric course. This structural difference can also affect the compression behaviour of the spacer fabric. Spacer S1 used a thicker monofilament for the connection layer and a connection structure formed by tuck stitches that shifted a distance of three needles, and was thus composed of six connection monofilaments in the formation of each course of the fabric. It is the thickest and exhibits the steepest compression stress–strain curve amongst the five types of spacer fabrics, thus showing good compression strength. The connection structure not only affects the thickness, but also the compression strength of a fabric.
Plastazote® is stiff and has high compression strength. The stress–strain curve for Plastazote® is the steepest with the smallest hysteresis loop, which indicates a small dissipation of energy during the compression/recovery cycle. Spacers S1 and B have better compression strength than Plastazote® for compression of 150 gf/cm2. For compression up to 250 gf/cm2, Spacer S1 still has higher compression strength than Plastazote®.
Pressure delivering ability of spacer fabrics
The amount of pressure applied onto hypertrophic scars directly affects the outcomes of treatment. The tightness of the gloves was determined by their RFs, which refers to the amount of reduction in the circumferential dimensions from the actual measurement of the body. Due to the differences in hand curvatures and rigidity, the pressure distribution is different at various locations on the hand dorsum. From the experimental results, it was found that the pressure glove samples alone cannot provide a pressure that reaches 25 mmHg at the locations that we measured. When the hand was lying flat, the pressure gloves with 5%, 10% and 15% RFs could only provide a pressure of 0.8–2.14, 2.94–5.27 and 6.52–10.24 mmHg, respectively, at the seven locations. The amount of pressure delivered to the hand is related to the fabric tension and the curvature of the body.27,28 Higher body curvature means higher pressure delivered with the same fabric tension. The pressure applied by the gloves to the areas with a flat surface was relatively lower. Insert materials were therefore needed to assist the pressure garment to treat the scars.
Plastazote® is commonly used by clinicians and occupational therapists as insert materials. Clinicians often shape Plastazote® and sometimes combine several layers to make the desired insert. Spacer fabrics not only can easily be cut into the desired shape, but their flexibility and softness can also match the contour of the hand dorsal. In this study, the five spacer fabric samples have a thickness that ranges from 2.98 to 5.08 mm. A 3 mm Plastazote® was selected for comparison of the pressure delivery ability with the five types of spacer fabrics. The interfacial pressure given by the gloves and inserts showed a similar trend for three RFs. The horizontal locations of P2, P3 and P4 also showed a similar trend in pressure delivery with the corresponding locations (P5, P6 and P7) in the vertical direction. The results of the four locations when holding a cylinder are selected for illustration purposes in Figure 8. A repeated-measures analysis of variance (ANOVA) was carried to understand the effect of the six inserts on the interfacial pressure. Significant differences (p < 0.05) caused by the six inserts were found on more than one type of glove or hand motion at different measurement locations except for locations P4 and P7. At P1 and P2, which are fully covered by the inserts, spacer S1 gives the highest pressure followed by Plastazote®, and then spacer S3, followed by spacer S2. P3 is on the left edge of the inserts. Spacer S1 and Plastazote® continue to deliver relatively high pressure while spacer S3 gives the lowest pressure increment amongst the six types of insert materials. P4 is somewhat next to the edge of the insert. It can be observed that the control condition can give a pressure that is even higher than that with an insert at these locations. This is because the insert slightly lifts up the glove on the area just next to it, which results in a lower contact pressure. Amongst the five types of spacer fabrics, spacer S1 can deliver a pressure that is comparable to the 3 mm Plastazote®, which makes it a potential insert material for pressure therapy. Although spacer S1 induced slightly higher interfacial pressures than Plastazote® in some measuring locations, the amplitude of pressure can still be controlled within the effective pressure range of 25–40 mmHg for scar treatment. By using the same machine gauge for knitting and with the same surface layer structure and fibre contents, spacer S1 can still deliver a pressure higher than spacer S2. This is because the connection structure can affect the thickness and stiffness of the spacer fabric and hence the amount of pressure delivery when used as inserts. Although the other spacer fabrics cannot provide an increase in local pressure as much as that of spacer S1 and Plastazote®, they still can give a certain amount of pressure increment.
Interfacial pressures at four locations on the dorsal of the hand between the hand and the pressure gloves with 10% RF that have different inserts when the subject is holding a cylinder.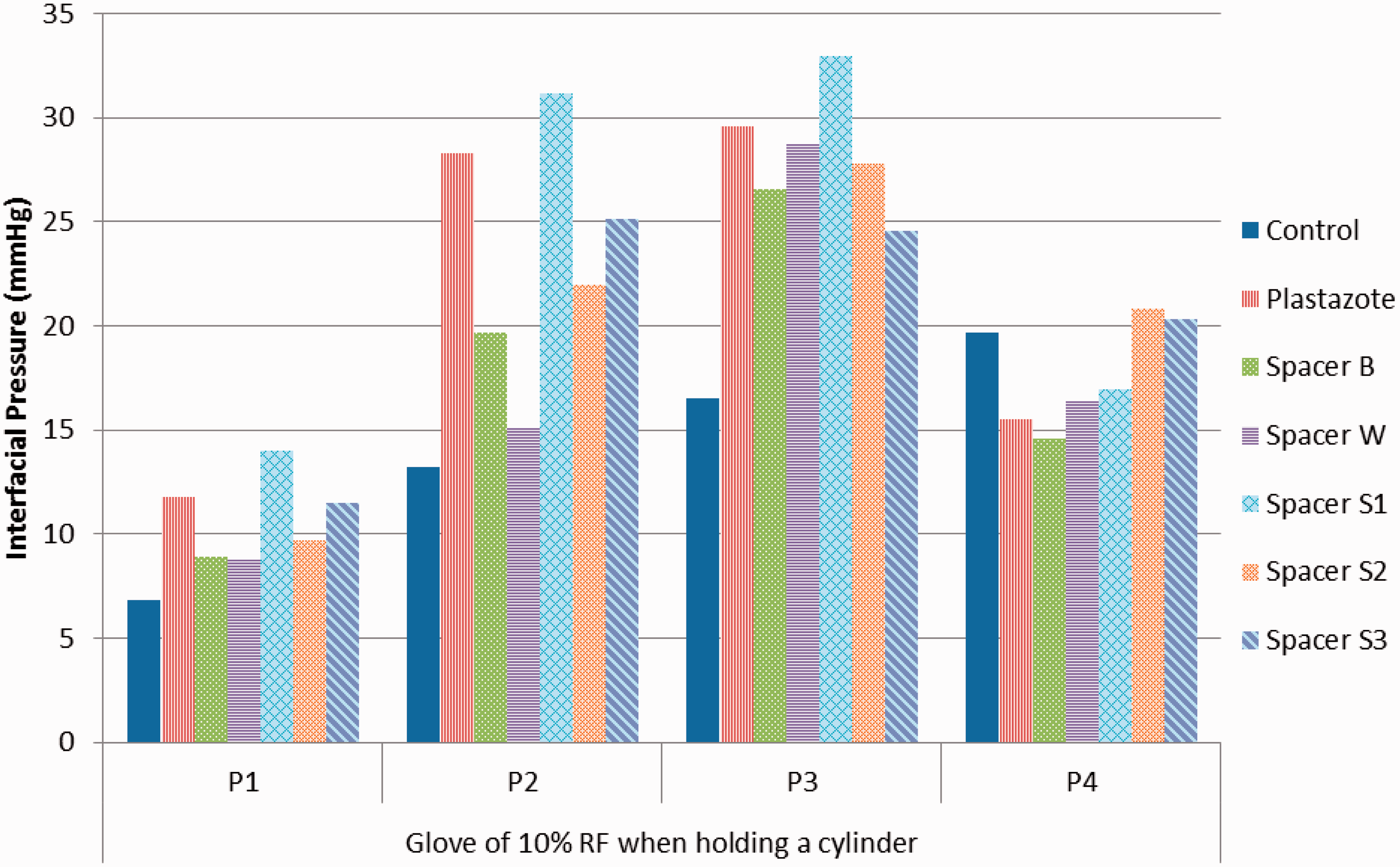
The magnitudes of the glove–skin interfacial pressure varied with changes in hand motions. The interfacial pressure increased when a cylinder is held and in a clenching motion which is in consistence with the finding of our previous study. 28 The pressure delivery from the different inserts shows a similar trend for the three hand motions.
Clinical study: impact on hypertrophic scar treatment
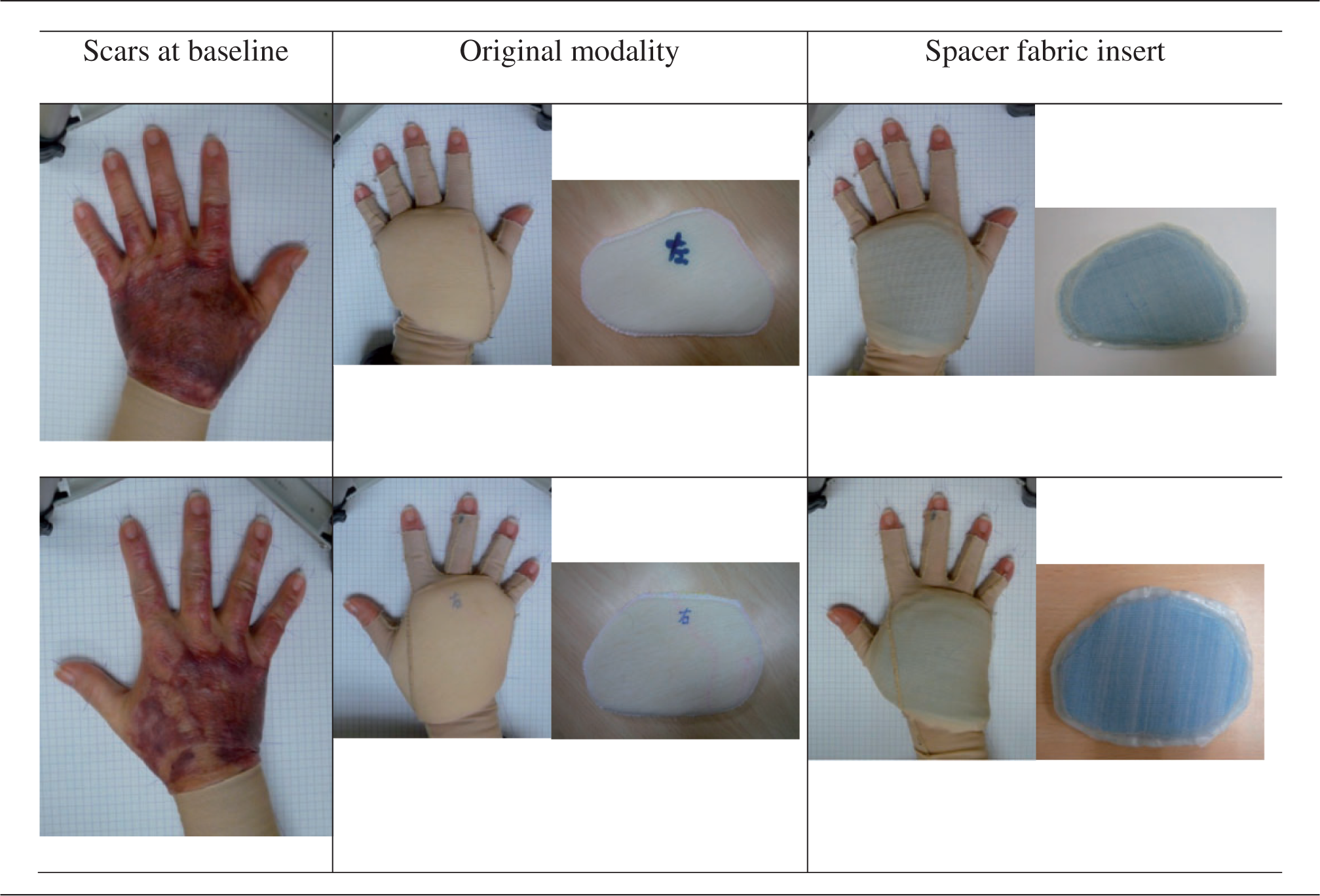
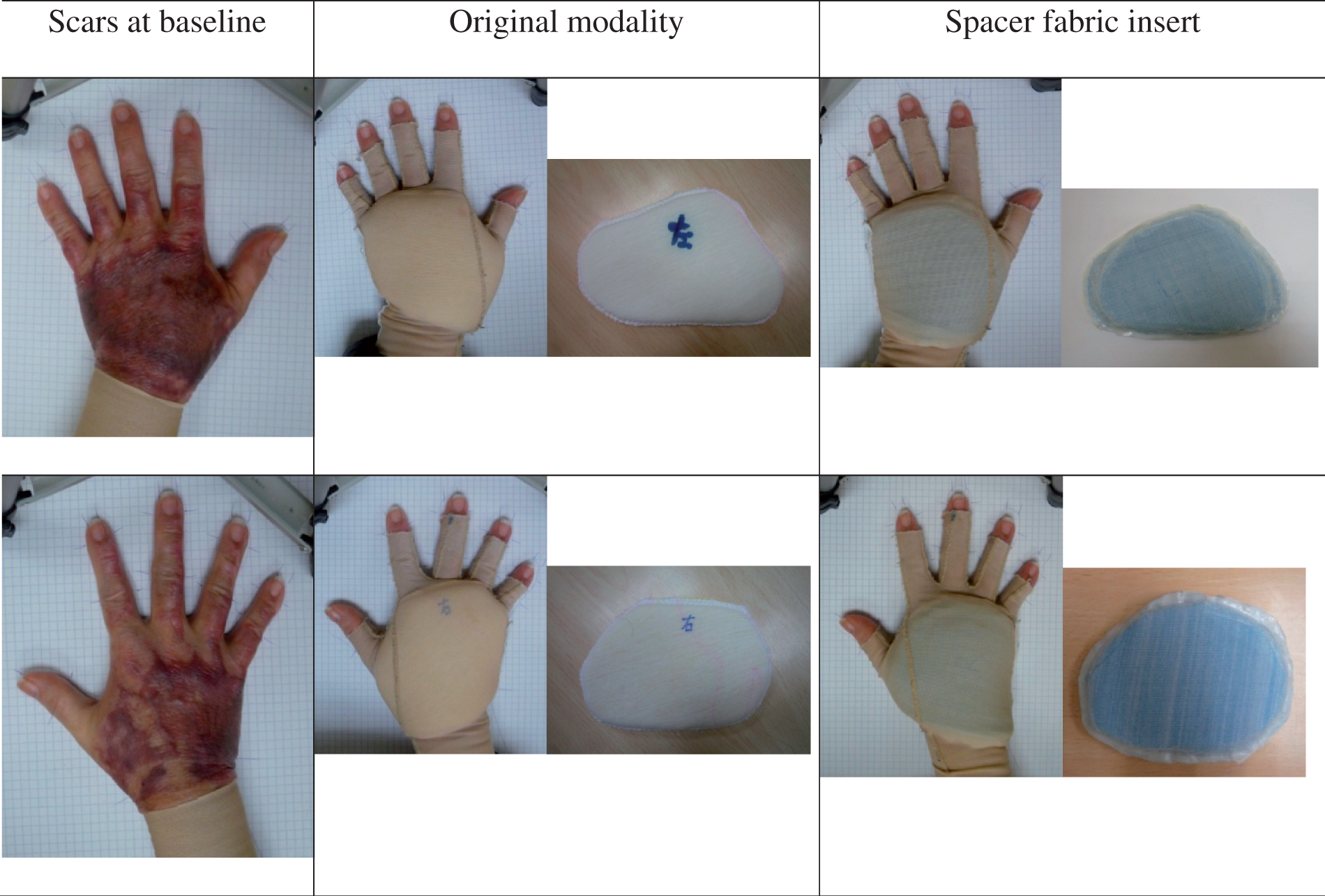
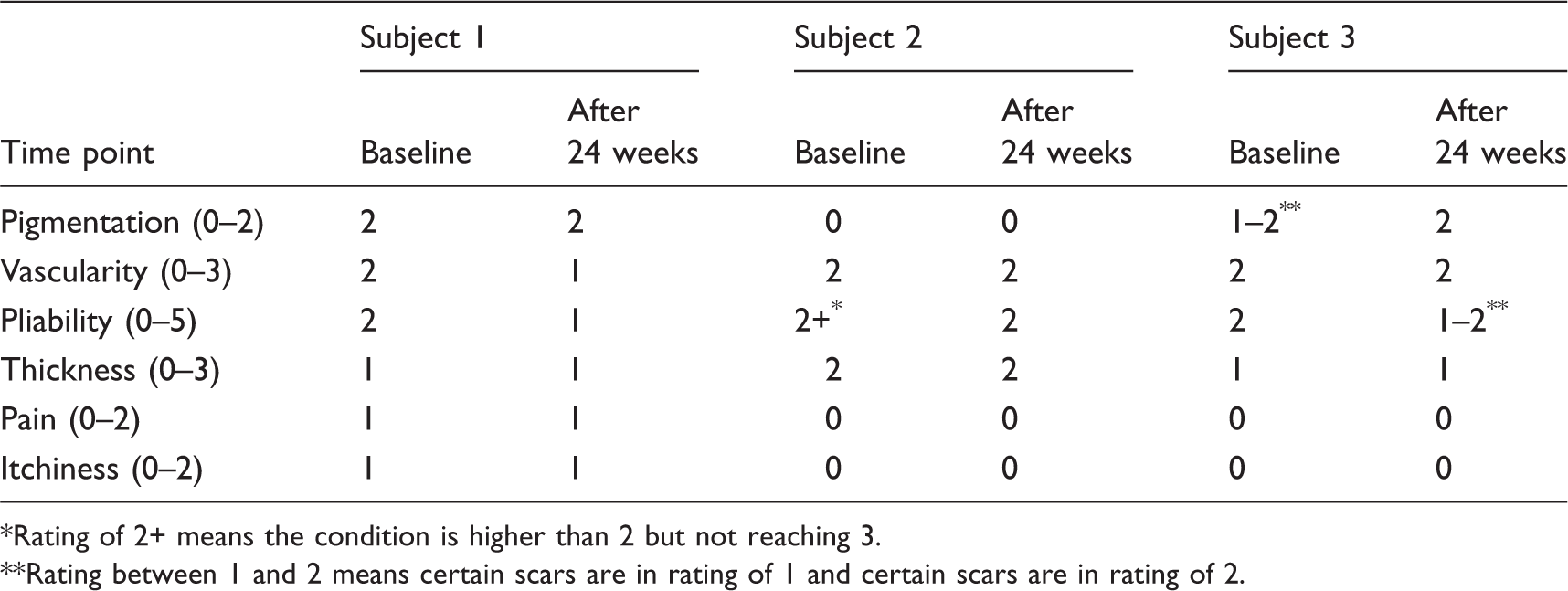
In order to understand the improvement of comfort with the use of spacer fabric and the effectiveness in suppressing the growth of scars, a study on patients with hypertrophic scars was conducted. With a relatively better air permeability, pressure delivery ability and compression strength, spacer S1 was selected to produce the inserts in the clinical study. An example of the scarred hands is presented in Figure 9. As shown, there is an observable improvement in the condition of each scar after 24 weeks of pressure therapy with the use of the spacer fabric insert. The VSS record presented in Table 5 also shows a certain improvement in scar conditions after the 24 weeks of pressure glove treatment with the use of spacer fabric inserts. The insert made of this type of spacer fabric can be an effective modality in treating hypertrophic scars.
Photos of hypertrophic scars at the beginning of the clinical study and after wearing the pressure glove and spacer fabric insert for 24 weeks. VSS record Rating of 2+ means the condition is higher than 2 but not reaching 3. Rating between 1 and 2 means certain scars are in rating of 1 and certain scars are in rating of 2.
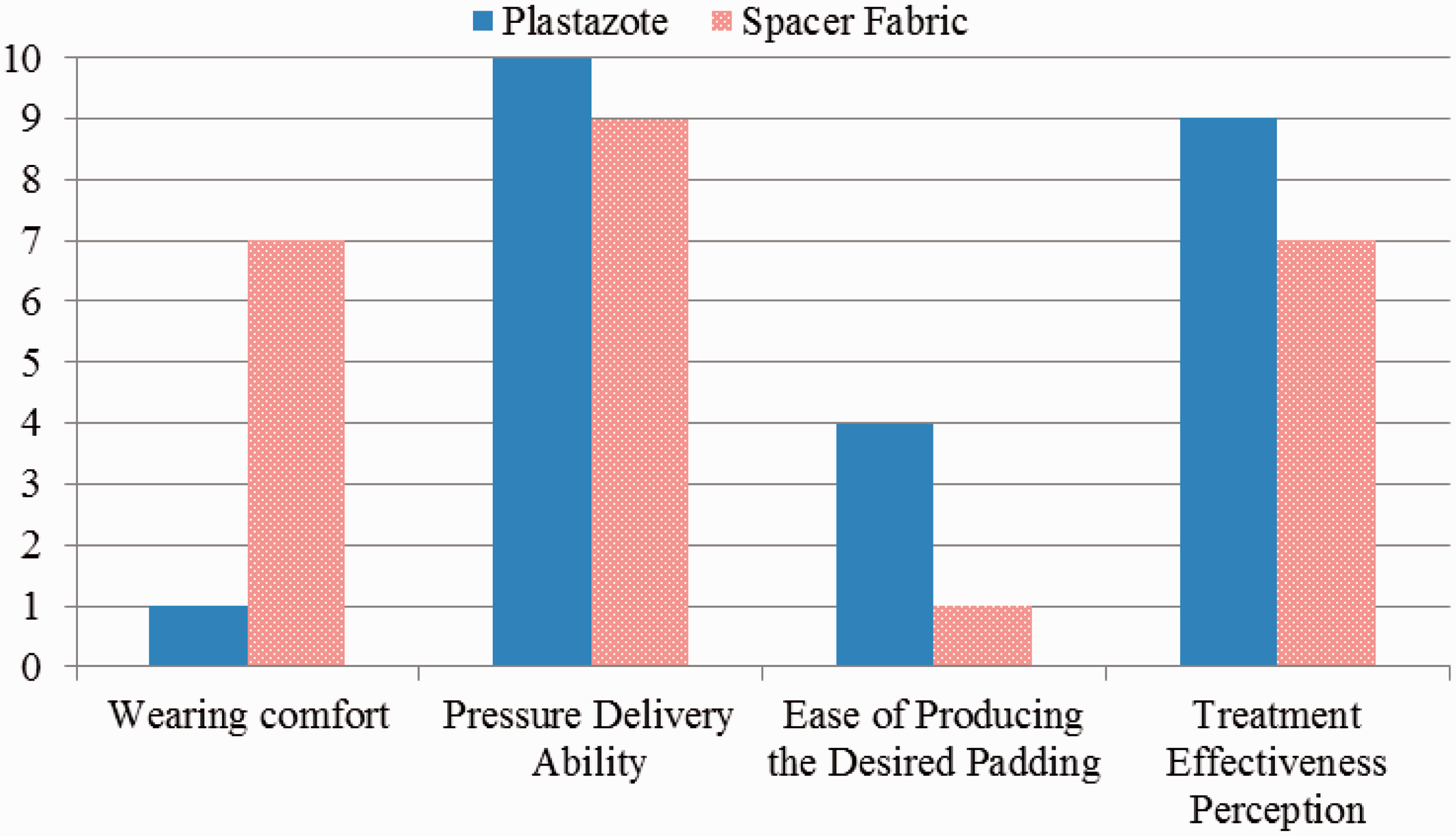
The results of the subjective ratings on the inserts made of the two types of materials from the patients and the occupational therapist are presented in Figures 10 and 11, respectively. The spacer fabric insert is perceived as a better insert material with consistently higher ratings than the Plastazote® insert by all three patients in terms of fit, breathability, comfort, treatment effectiveness, willingness to wear and ease of hand motion. From the viewpoint of the occupational therapist, the spacer fabric insert is somewhat lower in treatment effectiveness (rating of 7) and pressure delivery ability (rating of 9) when compared with the better performance of the Plastazote® insert (ratings of 9 and 10, respectively). Nevertheless, the occupational therapist indicated a problem with the spacer fabric insert which is the ease of production of a desired insert. Protruding monofilaments were found on the edges that additional edge finish is applied on the insert, increasing the complication in the production. However, considering the outstanding wearing comfort of the spacer fabric inserts, it is suggested as an alternative insert material for patients who find it difficult to accommodate a Plastazote® insert.
Subjective ratings given by hypertrophic scar patients on the original insert made of sponge or Plastazote®, and on the spacer fabric insert (error bars indicate SD). Subjective ratings given by the occupational therapist on inserts made of Plastazote® and spacer fabric.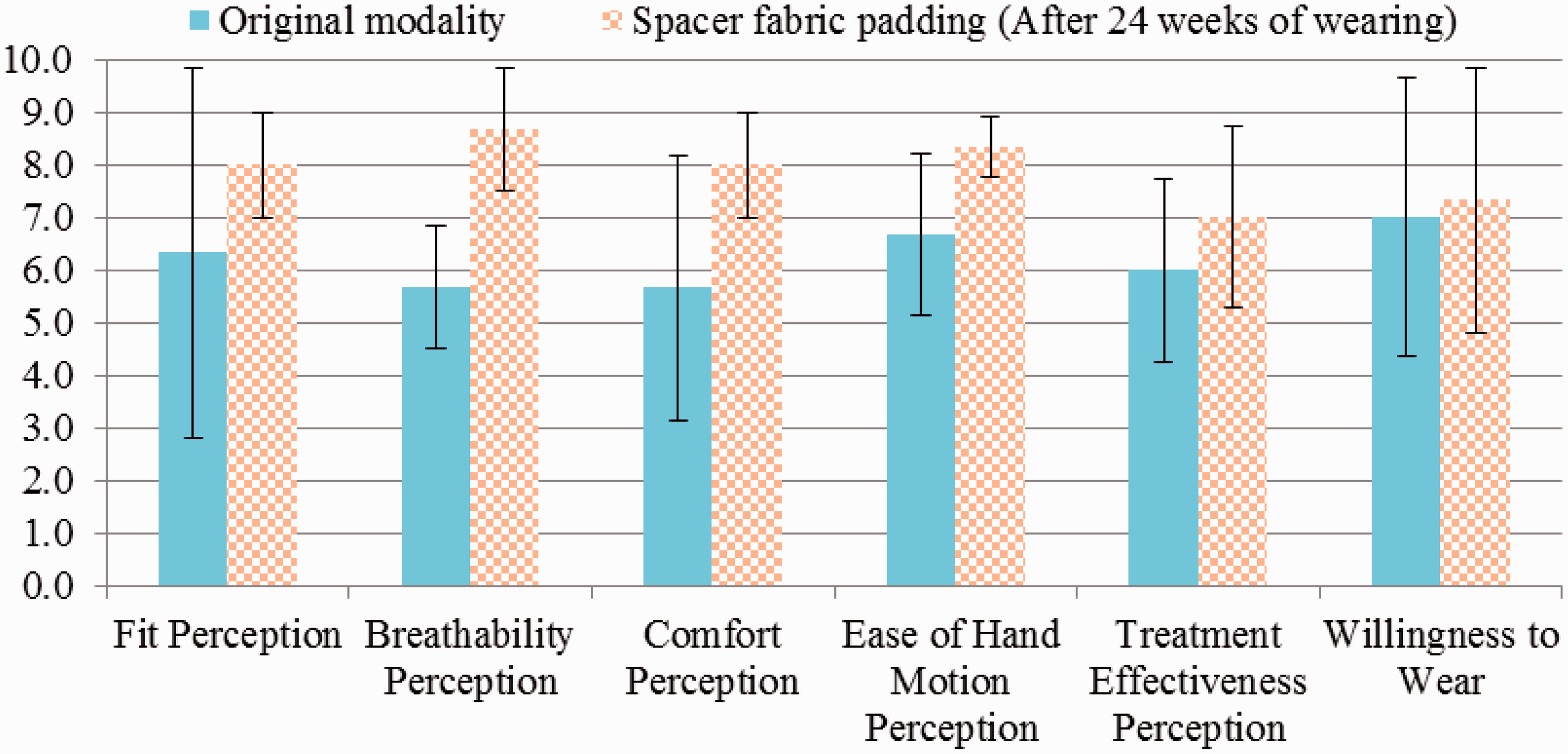
Conclusions
In this study, spacer fabrics are proposed as a possible material for inserts in pressure therapy in the treatment of hypertrophic scars. Spacer fabric can be produced from a normal knitting machine in a relatively low cost. Comparing with the traditional insert materials such as Plastazote®, the spacer fabric is more flexible to adjust its physical and mechanical properties by altering the yarn and filament used or the connection structure. 29 The spacer fabric used in this study are made of polyester, nylon and spandex which is the same as the materials usually used for making pressure garment with good biocompatibility. The spacer fabrics show outstanding air permeability and WVTR when compared with the insert material that is currently used. The softness of spacer fabrics can help to increase the glove–skin interfacial pressure on some of the concave areas of the hand dorsum. One of the fabric samples (spacer S1), which is 5.08 mm in thickness, can increase the interfacial pressure to a level that is comparable to that of a 3 mm Plastazote®. The structure of the connection layer of the spacer fabrics not only can affect the thickness, but also the compression properties, which hence influence the amount of pressure delivered onto the hand. The connection structure made by tuck stitches that shift a distance of three needles (spacer S1) can give a better compression strength than that by tuck stitching in every needle (spacer S2). The spacer fabric that uses a nylon monofilament for the connection layer can give better water vapour transmission and smoother surface than those that use a polyester monofilament. However, the compression strength of the spacer fabric with a nylon monofilament as the connection layer is only good at a stress level below 50 gf/cm2 and the connection structure collapses at 160 gf/cm2 which is much lower than the one with a polyester monofilament. As an insert placed underneath the pressure garment, the spacer fabric can improve the wearing comfort without sacrificing much the level of local pressure increment. From the 24-week clinical study on four scarred hands, the use of an insert made of spacer fabric is found to be effective in treating scars. With the improvement of wearing comfort, the pressure treatment acceptance and compliance would be consequently increased.
Footnotes
Acknowledgment
The authors acknowledge the supports from Occupational Therapy Services, Prince of Wales Hospital, Hospital Authority.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Research Committee Internal Grant (grant number G-UC36) and the Departmental Grant of the Institute of Textiles and Clothing, The Hong Kong Polytechnic University (grant number PolyU RPXS).