
Abstract
The pressure developed beneath any compression system is governed by the tension in the compression fabric. Depending on the type of material – cotton or elastomer – compression systems may react differently under the same stress. The previous work of our group and experience related to compression systems showed that classification of bandage materials is required for manufacturers who want to create products with specific compression levels. One of the mathematical descriptions of the expected pressure due to a tensile force in the fabric is the modified Young–Laplace equation. However, the pressure achieved by real compression systems hardly matches with the estimated values. Two groups of elastic bandages – short stretch and long stretch – were selected and investigated within this work. The tensile forces were measured using a dynamometer, and the pressures deduced at a given maximal load (3 N/cm) were compared with the pressures measured beneath the bandage on living subjects. The results show that the interface pressure can be predicted from the tensile force at the inflexion point of the hysteresis curves. Calculated pressures were in a therapeutic range but were significantly different from practically applied pressures, indicating large differences between calculated and real pressures on the leg.
The introduction of empiric knowledge about compression treatment started in the 20th century, working on elastic fabrics and knitted garments to understand compression systems. 1 As a benefit of these medical experimental studies in phlebology, compression has proven a reliable treatment for venous disorders in the 21st century. In these investigations, interface pressure measured beneath the garment was very important for both the efficacy and the tolerability of the therapy. A new recommendation on how to measure this pressure was published by the International Compression Club (ICC) in 2010. 2 However, this recommendation seems not to consider the macro-molecular structure of elastic fabrics, which depends on their chemical properties. 3 Hence, the behavior of elastic fabrics includes the interaction of the material structure, processing, and chemical properties, including temperature factors, enabling calculations of the compression behavior.
These may be used by therapy and product developers as a basis for decisions about the type of bandage that could suit a customer's (not the healthcare professionals, but the legal manufacturer's) request, or for educative purposes. Rabe 4 described the mathematical estimation of the pressure as an indirect method for the assessment of the interface pressure. Kecelj Leskovec et al. 5 wrote a clinical study report about a distinguishable behavior between bandages constructed from man-made fibers and those constructed from natural fibers. They furthermore state that the pressure produced by the elastic bandages depends on the tension of the bandage, the number of layers applied, and the curvature of the limb, and that the relationship between pressure and curvature is expressed by Laplace's law. Schuren and Mohr 6 report that calculations using the mentioned equation do not reliably predict actually measured interface pressure.
Although the previously mentioned studies have determined formulas for calculating and devices for measuring the pressure, no study has provided a comparison between the measured and the predicted values, considering the textile material macro-molecular structure as well as the textile processing (short or long-stretch bandage), although this comparison would be of great importance for medical therapy decisions.
Therefore, this paper presents a first comparative study between the predicted and the applied pressure beneath compression systems in real-life, considering the impact of textile material macro-molecular structures as well as textile processing machinery.
Elastic properties of compression bandages
Compression bandages are fabricated mainly from naturally and synthetically occurring materials. Natural fibers have been used for many centuries for different human needs and even more so for compression therapy, including wood, rubber, cotton, wool, leather, and silk. The most often used material for the fabrication of bandages was and is still cotton. Meanwhile, textile technology processing tools have also made it possible to prepare elastic cotton fabrics.
Understanding the behavior of compression bandages or systems needs a fair interpretation approach of material properties. Henceforth, commercially available compression bandages were selected and sourced for this study. Two types of elastic materials are investigated that exist in compression medical devices, as depicted in Figure 1.
Polymer networks: (a) linear polymer; (b) cross-linked polymer.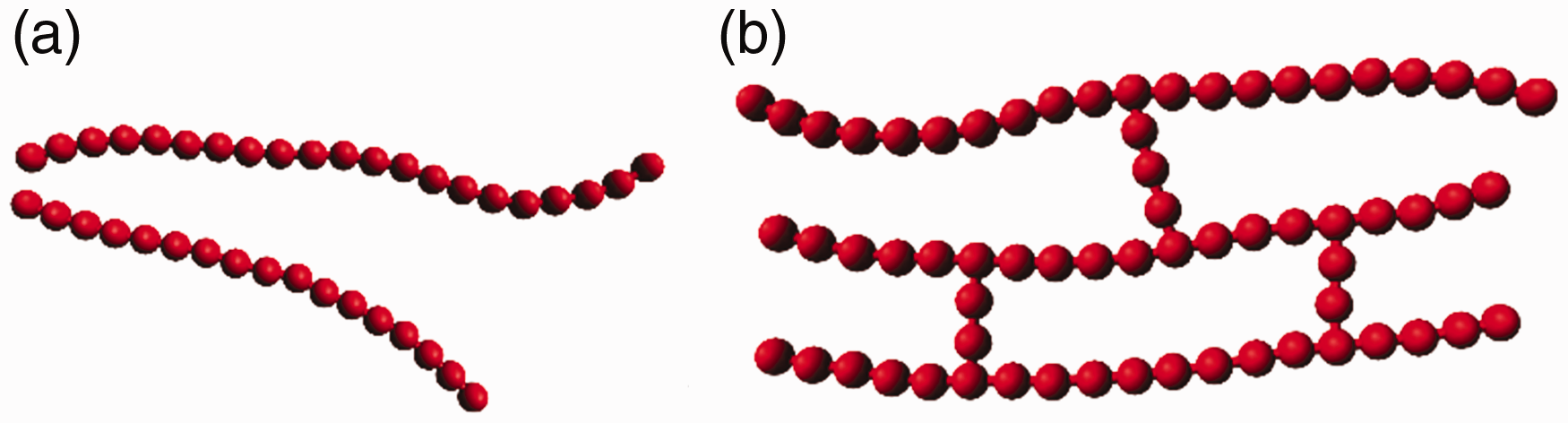
Synthetically occurring materials used in compression bandages are polymers with a good resiliency, 7 since they can be arranged in different polymer network structures, as illustrated in Figure 1. 8
Network polymers are multifunctional monomers forming two or three covalent bonds, making a three-dimensional shape (at the macro-molecular structure level) that prevents material fatigue at each physical loading or stress and thereby explains the good resiliency of elastomer-based compression bandages.
The network polymers used for compression bandages are highly cross-linked and have distinctive mechanical and thermal properties. 7 Such polymers are called thermoplastic elastomers. Furthermore, most elastomers hitherto used in compression bandages or stockings are so-called thermosets, because they are cross-linked during vulcanization. Of the several varieties of thermoplastic elastomers, one of the best known and widely used ones in compression bandages is a polyether–polyurea copolymer known as polyurethane. It is produced by reaction of a polyesterdiol with a diisocyanate and spun in a dry spinning process into elastane filaments (polyurethane solution), which are wrapped in textile processing with inelastic threads. The elastane filaments generated from such processes are also known as thermosets, because an elasticity limit is imparted to the filament throughout the spinning process.
The copolymer consists of block segments of a hard and rigid thermoplastic (commonly styrene) that alternates with block segments of a soft and flexible elastic material (often butadiene or isoprene). For a common thermoplastic elastomer, hard polymerized segments are located at chain ends, whereas each soft central region consists of polymerized butadiene or isoprene units (Figure 2).
8
Structure of thermoplastic polyurethane.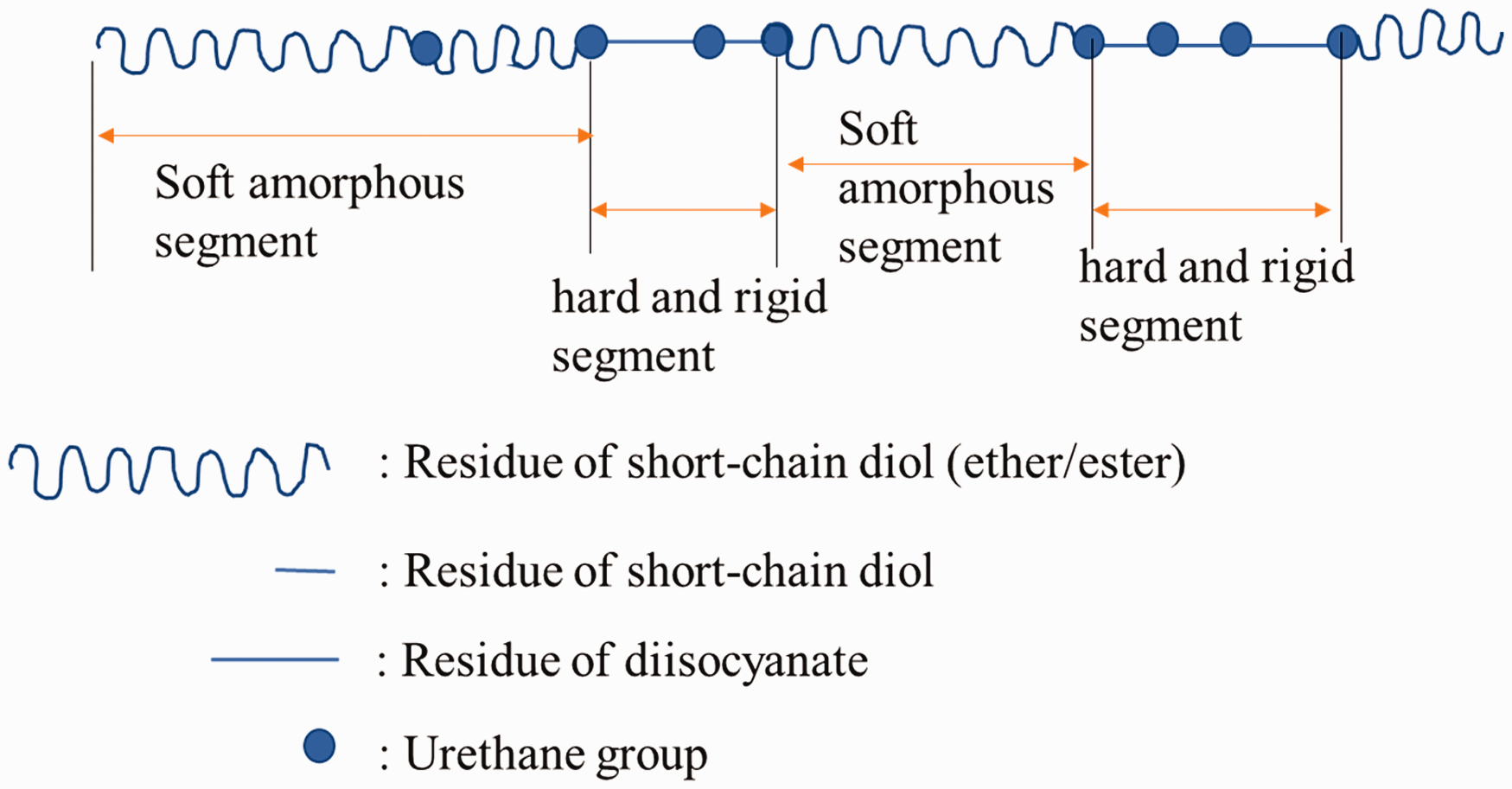
At ambient temperatures, the soft, amorphous central (butadiene or isoprene) segments impart the rubbery, elastomeric behavior to the material and enable the bandage stretch. The most often used elastomer threads in elastic compression bandages are elastane yarn. The products are shown in Figure 3 and listed in Table 1, respectively, with the brand names and materials; the pictures intend to help the reader to understand which types of products and materials were investigated. Furthermore, they show how relevant these products are for compression therapy.
Compression bandages used in the study. List of materials involved in the study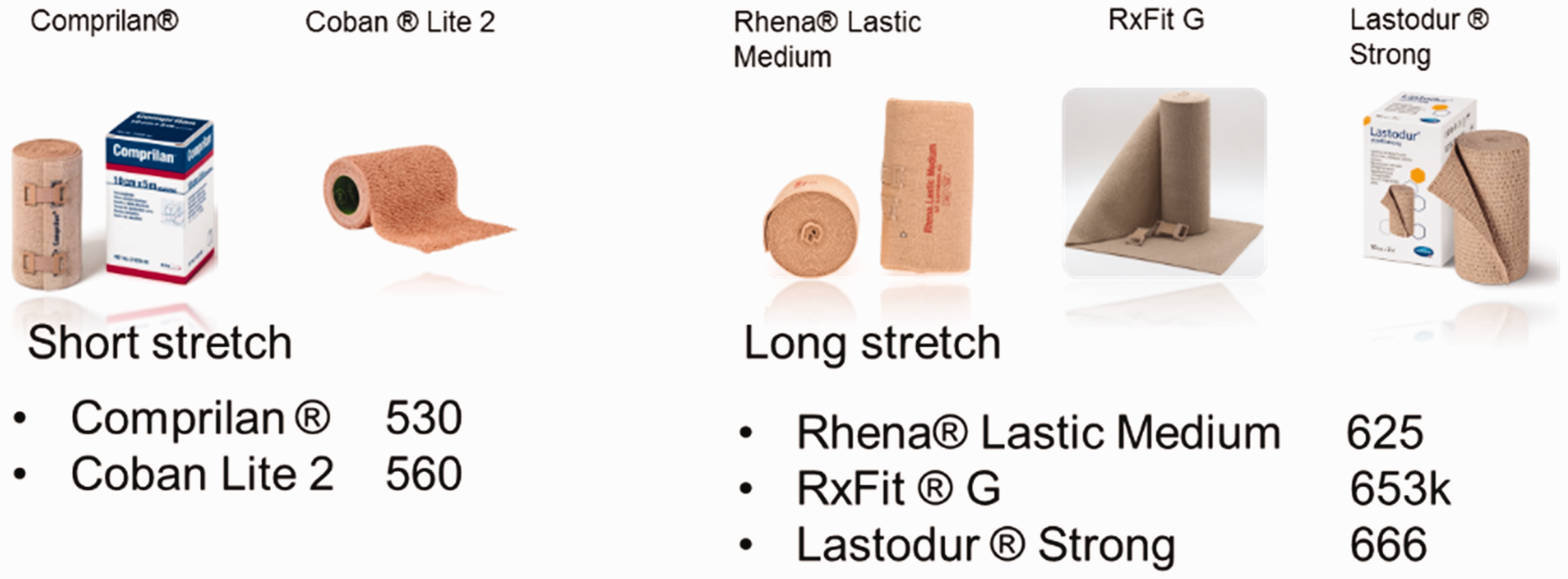

Obviously, cotton material is not elastic by nature, but special textile processing may impart this property to the cotton threads. This type of thread is used as an elastic component in the weaving of a special type of compression bandage that is predominantly used in European German-speaking countries (DE, CH, AT). These threads are produced with a high number of twists per meter. 7 The high twist enables shrinkage during the textile finishing (chemical reaction between cellulosic OH-group of cotton and water) process in the length of the fabric and allows the possible stretch in the later application. Table 1 and Figure 3 also show one compression bandage that has this type of cotton-elastic thread (Comprilan® 530).
Pathophysiology of compression therapy: clinical indication of the product
The short-stretch bandage 530 is clinically used in the acute phase of venous vascular disorders, such as venous leg ulcer, where the hemodynamic effect is needed to overcome the intravenous issues. From the leg study of Mosti et al. 9 where the relationship between the interface pressure and the volume of the leg due to compression is explained, it is also understandable that when the muscle pumping function and the venous valves fail to transport the blood from distal to proximal, this results in a fluid congestion and edema on the lower limb. Basically, compression therapy depends on the textile material and the calf muscle pump of patients (active or mobile). Hach et al. 10 reported in their study about venous insufficiency pathology that the reflux causing the edema also has a direct impact on the capillary filtration and disturbs the fluid exchange in the tissues. The pathophysiologic background of the chronic venous insufficiency is the venous ambulatory and capillary hypertonia through the venous valve mechanism and muscle pump function. Typically, the pressure exerted on the venous wall by the blood when standing is about 80–100 mm Hg. Through the muscle contraction that basically occurs in dorsiflexion, the muscle presses on the venous wall, and therefore enables a pumping effect and the blood returns to the heart. During pumping, the blood volume in the veins is reduced and the pressure falls to 10–20 mm Hg. 11 This natural pumping effect can representatively be fulfilled with cotton-based short-stretch bandages. However, in specific medical cases where subjects or patients cannot stand, long-stretch bandages or combinations of long and short-stretch bandages, such as bandages 625, 653k, 666, and 560, may be used because they continuously (with reference to their rubbery property) build a counter-pressure against gravity. The gravity pressure is the hydrostatic pressure, which acts also on the superficial and the perforating veins and causes inflammatory edema due to, for example, poor perfusion. 12 When applied with a low to medium extension, long-stretch bandages (625, 653k, 666) alone may not be able to induce venous hemodynamics and overcome the hydrostatic pressure in the deep veins. Therefore, such compression bandages are mainly used for support and relief, while providing a moderate compression on the tissue and increasing the blood perfusion rate. Lattimer et al. 12 showed in their study of the quantitative measurements of superficial venous insufficiency, including the Venous Arterial Flow Index (VAFI), the Saphenous Recirculation Index (RCI), the Venous Filling Index (VFI), and the Postural Diameter Change (PDC) of the saphenous trunk, that the VAFI can already be improved in the supine position; this means even light to moderate pressure of 25–30 mm Hg would support edema reduction of the superficial veins. Hence, elastomer-based compression bandages that are able to provide such pressure would most probably have a direct impact on the superficial veins, while natural fiber-based compression bandages would have a direct impact on the deep veins. Due to these implementations, investigating the macro-molecular structure of materials for predicting the interface pressure of compression bandages has become a necessity and thereby requests quantitative correctness. Meanwhile, it is important to mention that the commonly used human ankle's radius for the interface pressure prediction lacks scientific background, as the textile material is subjected to the pressure appraisal and not the human; however, it would be logical to use the human ankle's radius for the recalculation of the sub-bandage pressure after the bandage is applied.
Review of mathematical estimations of interface pressures
Driven by the intention to design effective compression systems to achieve the optimum interface pressure gradient, many manufacturers use mathematical equations that attempt to describe or predict the interface pressure theoretically. 13 The interface pressure is defined as the pressure that occurs at the interface between the body and the bandage. Significant challenges remain in understanding the interface pressure, especially related to the fabric construction of the bandage and how it affects the measurement of interface pressure. 14 It is commonly assumed that the macro-molecular structure of textile material affects overall interface pressure of the bandage. Furthermore, different materials make the pressure prediction quite ambiguous and allow doubts between researchers about the model rationality of the predicted pressure interface of bandages.
According to the Young–Laplace equation, the interface pressure p can be mathematically estimated as follows
7

It can be assumed that the hydrostatic force in the vascular system is equal to the vectoral force acting on the bandage

As the radius of the leg 



Hence, for n overlapping layers

The conversion factor k = 4623 (or 4620, as typically used in the literature 7 ) enables the unit conversions from Pa to mmHg as well as from N to kgf (kilogram-force).
Experimental details
The predicted value of the pressure is calculated based on the above-derived equation, which is typically used in phlebology. The technical parameters (tensile force and extensibility) used in the equation are gathered from tensile hysteresis testing using a dynamometer (ZwickiLine Materials Testing Machines Z0.5 up to Z2.5, Zwick GmbH & Co. KG, Ulm, Germany).
Afterward, the same samples are tested on healthy volunteers' legs using a Picopress® sensor (Microlab, Padua, Italy). This sensor is an airbladder transducer, which would contain about 10 ml air in a chamber, to sense the interaction between the leg and the applied bandage. The Picopress® device is a commonly used interface pressure measurement device and is portable. Partsch and Mosti 2 showed in their study “Comparison of three portable instruments to measure the compression pressure” that this commercially available device is the one with the best accuracy. Considering the Picopress® as the gold standard, a comparison between Picopress's results and the predicted ones is made. In the evaluation, one first correlates the calculated pressures and energy deployed by the bandages; this is intended to confirm whether the pressures are in the therapeutic range or not, and furthermore to confirm that the bandages maintain their elasticity after the test. Finally, pressures from the tensile hysteresis testing are compared with those of experiments on the volunteers' legs.
The experiment started with assessing the basic characteristic of bandages per textile testing standards DIN EN 1773 and DIN 61632.15,16 Furthermore, specimens of the bandages were prepared to measure the tensile hysteresis of each product, using a ZwickiLine materials testing machine. This test was followed by interface pressure measurement (compression tests) using in vivo measurement using the Picopress® device. To enable a fair comparison between the products, we found it necessary to draft a testing plan for each of the testing methods (ZwickiLine, Picopress®) as well as for sampling to eradicate failure due to any variability within bandages.
Test framework on the dynamometer: determine the tensile strength and estimate the pressure at a given extension
For the investigation of the extensibility of the bandages, a maximum force of 10 N/cm was applied, which is usually regarded as the absolute maximum value.
Furthermore, estimating the interface pressure is based on evaluation of stress–strain hysteresis loops to a maximum load of 3 N/cm, which approximately represents the application force used in real-life. In clinical studies with a medical grade of up to level 1, interface pressures of about 20–50 mm Hg are commonly reported. 17 Converting these interface pressures into forces per surface unit (N/cm2) reveals that bandages are applied with forces around 3 N/cm width of the fabric. Keller et al. 18 also showed in a controlled study with skilled health care professionals that bandages (with typical width 10 cm) are usually applied with forces of approximately 30 N or slightly more.
Finally, the data of the hysteresis curves (taken with 3 N/cm) are used to estimate the Dynamic Hysteresis Coefficient (DHC), which may be of interest for differentiation between compression systems. The DHC was defined in a previous study as the result of a quasi-dynamic five-cycle tensile test, which estimates the energy loss of the bandage between the first and the fifth elongation of the bandages
7
; it is illustrated in Figure 4 and given by Equation (4).
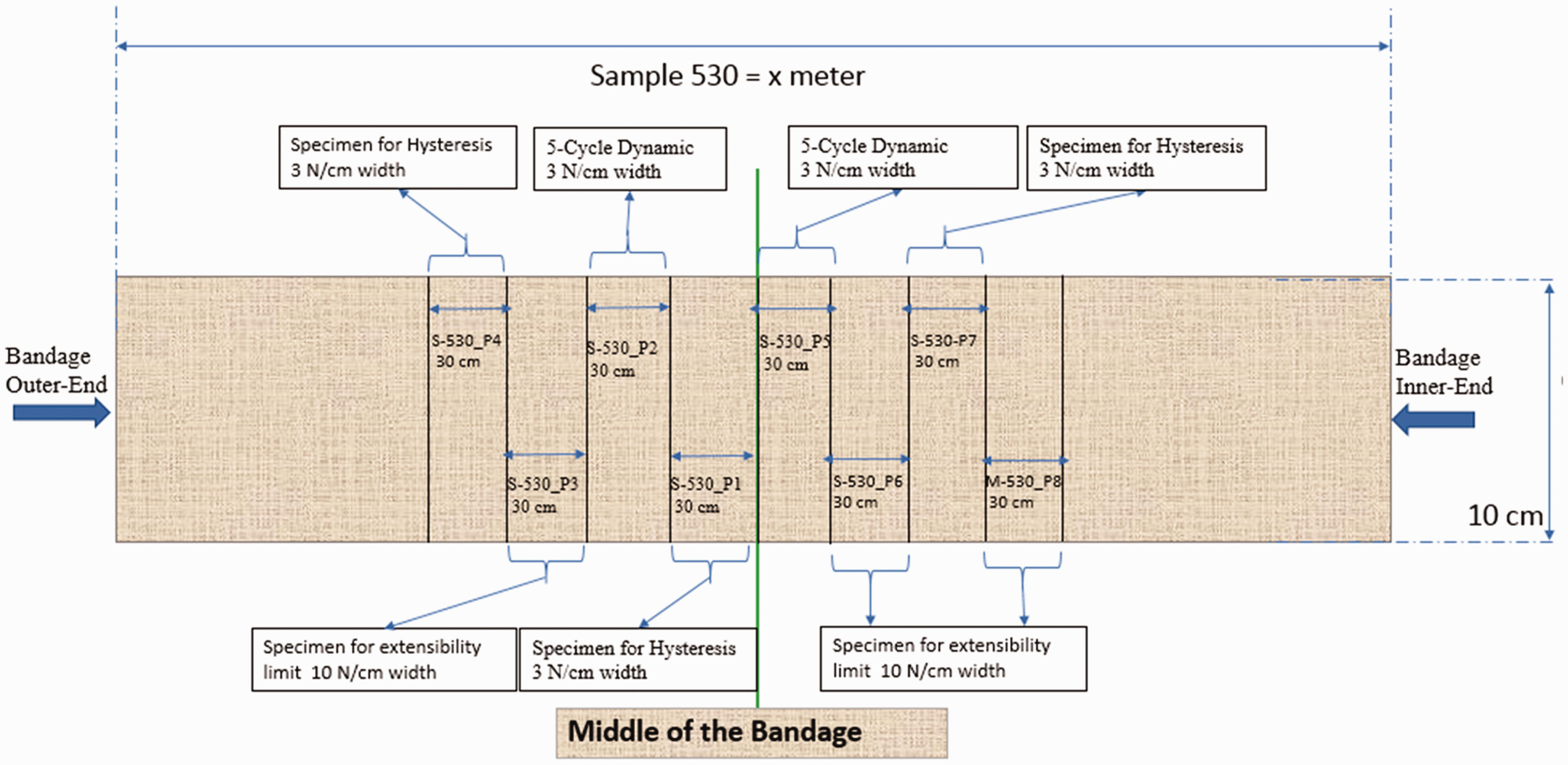
Illustration of the components of the Dynamic Hysteresis Coefficient (DHC). Example of specimen selection within a sample for ZwickiLine test method. The sketch is not true to scale.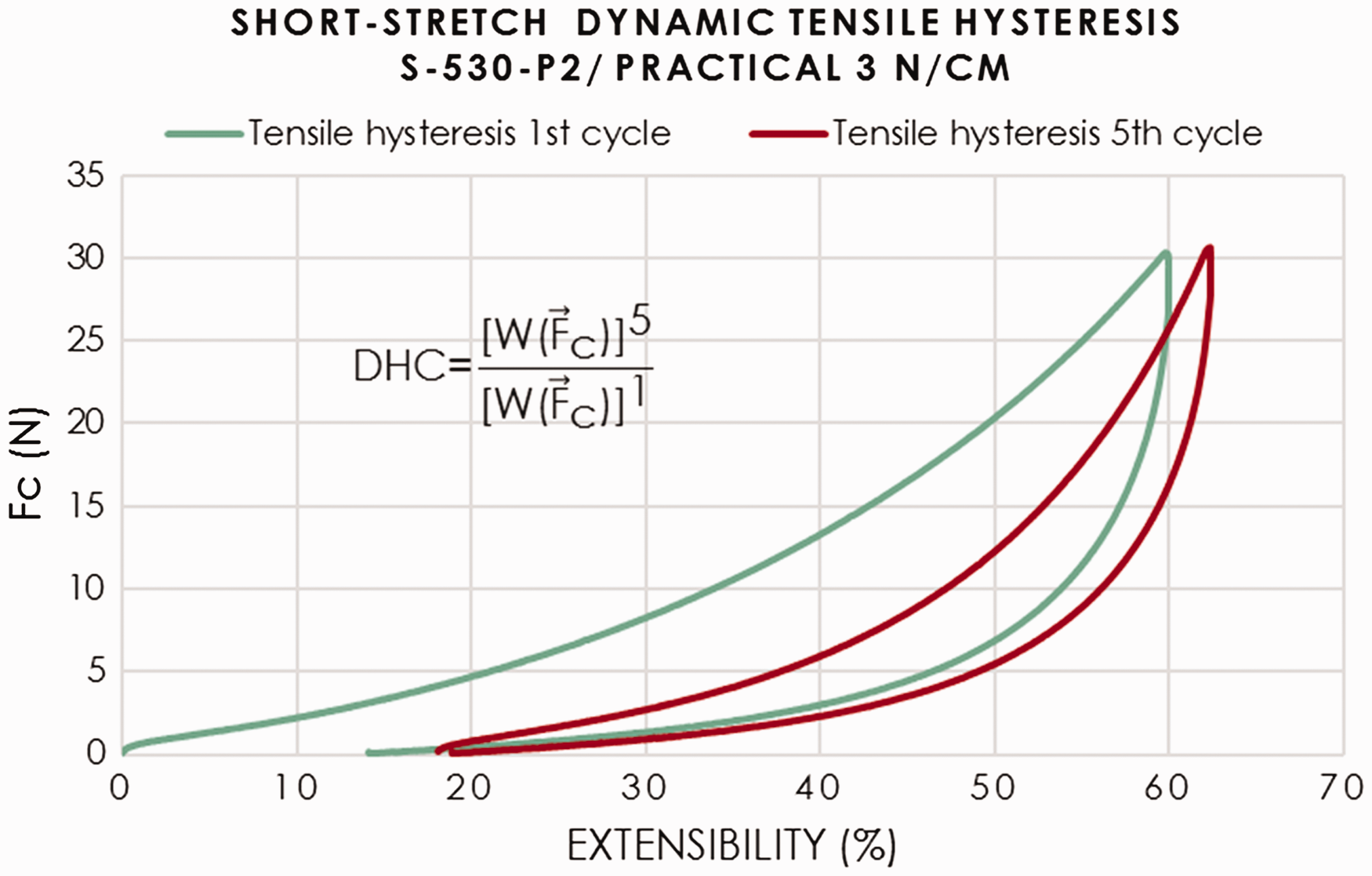
The DHC helps to compare the elasticity of bandages

ZwickiLine sample distribution within the test plan. The ID “S-530_P3-6-8,” for example, contains three specimens (specimens 3, 6, and 8), taken at the respective positions of sample S-530, as defined in Figure 5
As shown in Table 2 and Figure 5, the tensile hysteresis or extension behavior of 40 specimens per product (5 samples × 3 positions for extensibility measurements + 5 samples × 3 positions for hysteresis measurements + 5 samples × 2 positions for dynamic tests) have been tested in the lab for this study. As a similar physical behavior was observed for the tension-tests with 10 and 3 N/cm width in the given range of F ≤ 30 N, 15 specimens per product were finally considered in the evaluation of the macro-molecular impact of the material on the physical behavior of the bandages.
According to our experience, compression bandages do not have a uniform extension all over their length. During manufacturing, the winding force and speed shall be adjusted to the increasing diameter of the bandage. For this reason, the larger the diameter of a bandage, the more probable it is that a variation of the extensibility will occur between the outer end, the middle, and the inner end of the bandage. Hence, using a sampling that would get rid of this possible source of errors was also of interest for the study (Figure 5).
Each specimen had a size of 10 cm × 30 cm (width × length). Testing the extensibility limit of bandages was also intended to classify the bandage either as long stretch or short stretch, according to Partsch. 19 Considering the possible impact of the macro-molecular structure of the bandage on the pressure calculation through the tensile test, it was also intended to evaluate whether the type of material has an impact on the interface pressure conversion factor k, which has been derived under the assumption of perfectly even surfaces and without taking into account the variation of the “tangential” force in a bandage due to the weave structure.
In vivo framework on living subjects to assess real-life interface pressure at a given extensibility
This test intends to quantify the interface pressure provided by each bandage applied to the lower leg of a volunteer. Compression bandages are generally worn for a period of time, but since this study does not focus on long-term efficacy of the bandage, the interface pressures were recorded within 1 hour. The bandages mentioned in Table 1 were applied on healthy volunteers who were randomly selected. Taking into account the Ethical Considerations Specific to Participants, defined in the National Statement on Ethical Conduct in Human Research (2007, updated May 2015), the selected volunteers were instructed about the intention of the study and no personal data were recorded. Finally, the volunteers gave their approval for participating in this study. This part of the study includes four volunteers, meeting inclusion/exclusion criteria. The selected volunteers were identified with letter codes accordingly: AH, AL, SK, and JS.
The inclusion criteria were as follows.
- Ankle brachial index (ABI): 0.8–1.2; capillary refill < 3 seconds; good general health and the ability to wear compression bandages on one or both legs for at least 1 hour.
The exclusion criteria were as follows.
- Absence of pulse in dorsalis pedis and/or posterior tibial; pallor and/or inflammation of leg and/or foot; champagne bottle leg/lipodermatosclerosis; hemosiderin staining; existing disease diagnosis; existing lesions distal to the knee; consistent drug and/or medication use.
Following the anonymity principle, the bandages were randomly applied.
Results and discussion
Prediction of interface pressure according to the modified Pascal and Laplace equation
While searching for the stretched length (strain) for which the tensile force (stress) on specimens would result in a therapeutic pressure, as happens in real-life, statistics of the tensile force and extensibility recorded by the dynamometer software were evaluated to estimate the pressure on the interface. The previously mentioned modified equation of Pascal and Laplace (Equation (3)) is used and translated as follows.
In the bandaging process, the leg circumference in a specific section is equal to the stretched length of the bandage (L1) that covers the limb after a turn; this stretch length can also be expressed by the strain or extension of the bandage. A single turn in the bandaging is equal to the stretched length of a specimen. The equation for the interface pressure that was calculated and is depicted in Figure 6 can now be written as

As mentioned above, the pressure expected from compression bandages may be estimated while considering an arbitrary stretch length, which may be caused by a loading and unloading force (Figure 6(a)).
(a) Stretched length corresponding to loading and unloading forces. (b) Resulting pressure.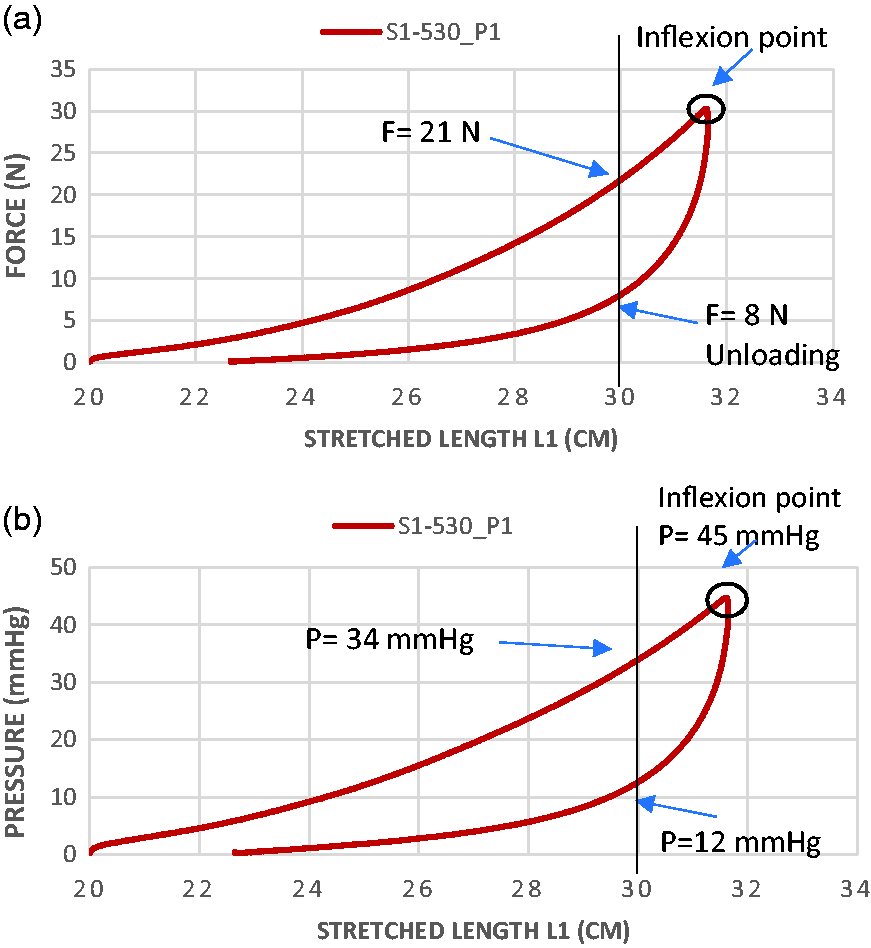
Short-stretch bandages, such as “product 530,” are mostly applied with a near to full stretch; this means for an initial length L0 = 20 cm that the bandage may be strained to a final length L1 ≤ 32 cm (according to Figure 6(a)), which represents a strain/extension of about 60%. Figure 6(a) also shows two forces (F = 21 N and F = 8 N) recorded at the same extension (L1 = 30 cm, which implies 50% extension); it raises the need to know which of those two forces act while straining and releasing the specimen, causing the pressure to be exerted on the vascular systems.
An observational survey of practical training of specialized nurses and therapists shows that stretching a short-stretch bandage by about 50% of its initial length would result in a pressure greater than 12 mm Hg.20,21 This implies that the calculation of the interface pressure shall most probably consider a force around the inflexion point as this would result in a pressure between 34 and 45 mmHg, which according to common compression practice is much more realistic. However, the inflexion point is a new aspect for pressure prediction. It is defined as the reversing point of the hysteresis curve where the force starts to decrease. It corresponds to the stretched length of the specimen at which the predictable force to act on the bandage is expected and will allow a significant comparison between a predicted and any measured sub-bandage pressure.
Moreover, as depicted in Figure 7, the estimated pressure was found to vary according to the position of the specimen (P1 – inner end, P4 – middle, and P7 – outer end) in the bandage; and selecting an arbitrary force on the linear part of the loading curve made the estimation less accurate. This problem shows the necessity to examine the entire curve. This examination reveals that the optimal stretched length and force for the most accurate calculation of the pressure would always be at the inflexion point of the curve, taking into account that the dynamometer strains the bandage at very low speed, which would be comparable to a human bandaging.
Pressure variability due to the position of specimens in the bandage.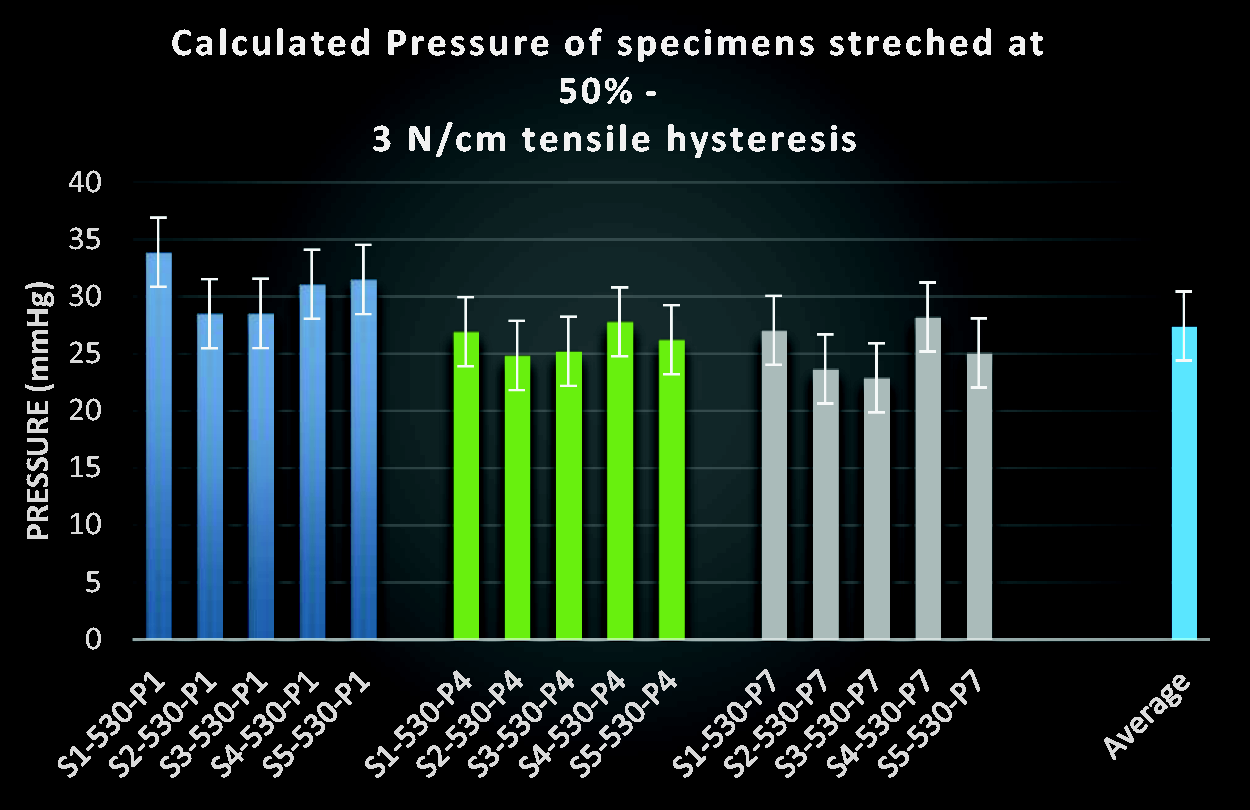
Hence, Figures 8 and 9 show how accurately the interface pressures were finally estimated using the force at the inflexion point. Figures 8 and 9 depict the calculated pressure of the short-stretch bandages – 530 and 560 – based on Equation (5). Due to some irregularity of bandage 560, only six specimens were evaluated.
Cotton fiber-based short-stretch bandage: pressure repeatability at the inflexion point. Elastane fiber-based short-stretch bandage: estimated pressure repeatability at the inflexion point (F = 30 N).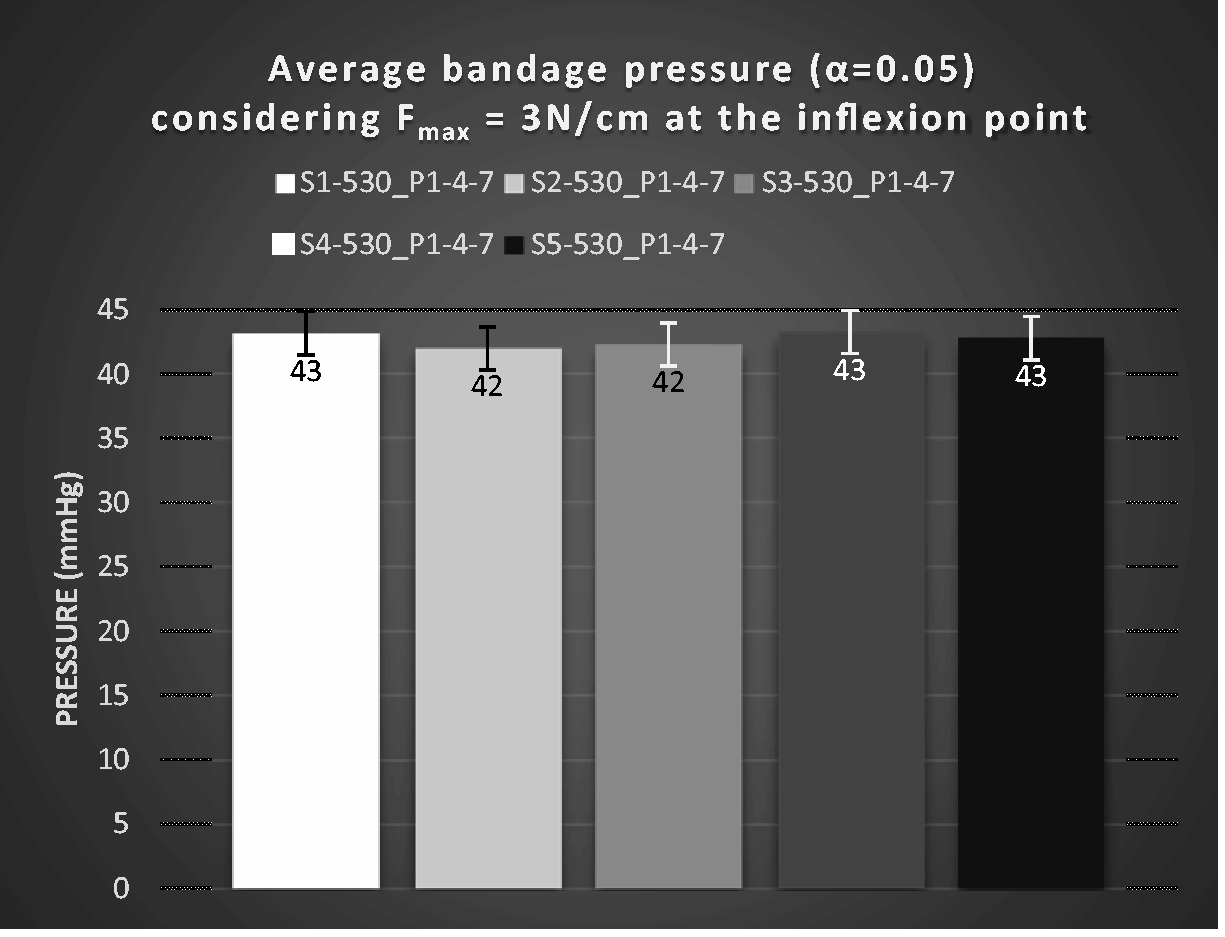

In a similar manner, the pressures of the long-stretch bandages – 666, 625, and 653 – were also calculated and are shown as the average values in Figures 10(a)–(c).
Depiction of the pressure repeatability calculated with forces at the inflexion point (F = 30 N).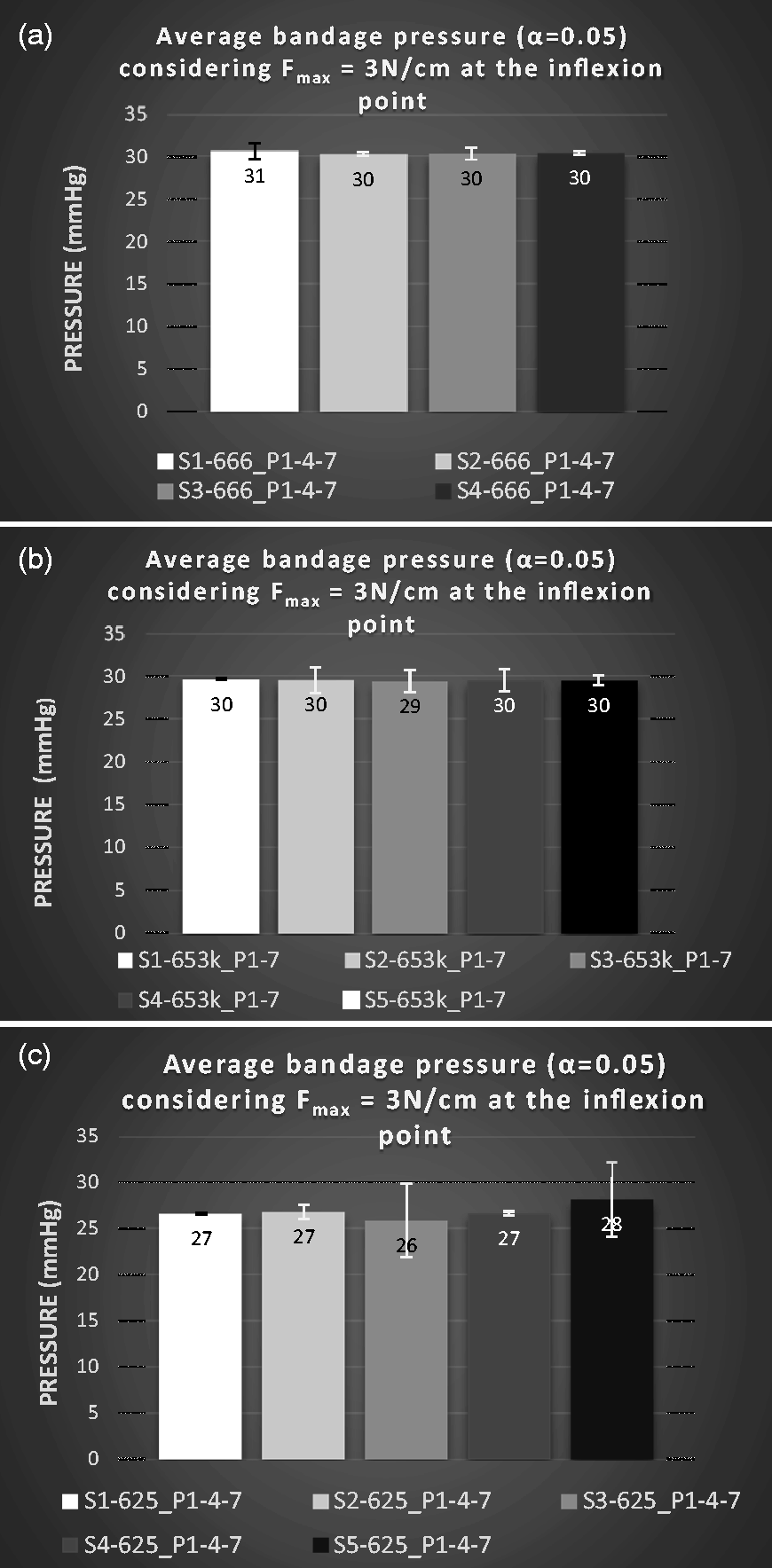
Discussion of the prediction of interface pressure
In summary, the estimation of sample pressures considering forces at inflexion points delivered quite reliable results. This can be observed on all specimens, which did not show significant deviations within each bandage type. On the other hand, the calculation of pressures considering any other point apart from the inflexion point was influenced by the extension variability depending on the position of the specimens within the bandages; this is, for example, the case for the results depicted in Figures 9 and 10(c). It was also noticed that this variability occurred for all bandages – either cotton- or elastane-based (Figures 10(c) and 8) materials.
The primary way to explore the cause of this dilemma consisted of verifying whether the variability could be material type-related, as assumed. Hence, the maximal stretch or the extensibility limit of three samples per bandage were measured based on DIN 61632:2009-12. This quality standard defines the elasticity of bandages by percent elongation following the application of a force of 10 N per cm bandage width.
22
The resulting maximal stretch percentage or extensibility limit categorizes bandages as short stretch and long stretch; in this definition, short stretch has maximum extensibility < 100% and long stretch maximum extensibility > 100% (Figure 11). According to the standard, it is recommended to measure the extensibility by stretching the entire bandage.
23
This would reduce the impact of the variability of the extensibilities within a bandage on the overall results. Manufacturers use a stretching table for this purpose, as illustrated in the standard. By testing on such an automatically controlled testing-table, accurate information about the useful length of the bandage is given.
Extensibility limits measured on a standardized automatic stretch-controlled table: (a) long stretch; (b) short stretch.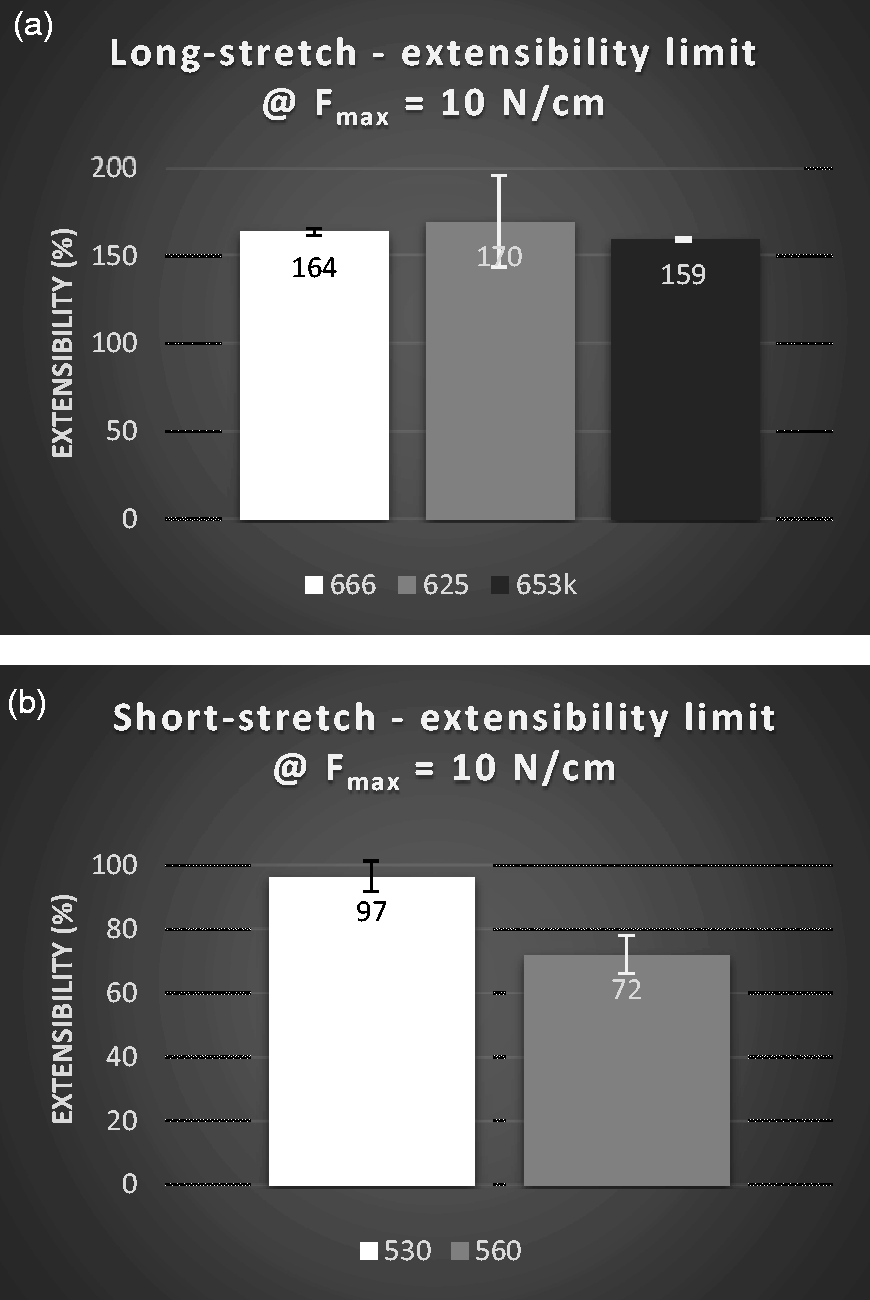
Figure 11 shows the average maximum extensibility of each sample, which unfortunately does not provide information about single forces acting on the stretching trajectory, as we simply placed 100 N on the end of a bandage to stretch it to its limit. Hence, using a dynamometer is still the most convenient method in assessing the force for predicting the interface pressure. Furthermore, Figure 11 also shows that the extension variability that was observed in some specimens tested on the dynamometer could also be observed here. The highest variability is visible for product 625, which shows an extensibility limit Ext% = (170 ± 26)%, for a given confidence α = 0.05.
This leads us to the assumption that the extension variability within a bandage may not be primarily caused by the macro-molecular structure of the material, but most probably by the bandage winding process during manufacturing, since this variability occurs in elastomer-based as well as in natural fiber-based bandages. In this process, the increasing diameter of the bandage permanently requires an adjustment of the winding speed of the machine and thereby causes a small difference of extensibility limit within the bandage.
Result of differentiation of the material macro-molecular structure based on the work/energy of the textile referring to the Dynamic Hysteresis Coefficient
Moreover, we investigated whether the force variability, related to the extensibility, limits each specimen or whether it could be neglected in real-life compression therapy, or whether the material macro-molecular structure impacts the compression therapy. In order to test these factors, the DHC is calculated. As mentioned in previous sections, this testing method compares the successive energies needed for compression function of bandages. In a previous study, the DHC was used to assess the material fatigue under a load of 100 N at the inflexion point (maximum extensibility of the bandage).
7
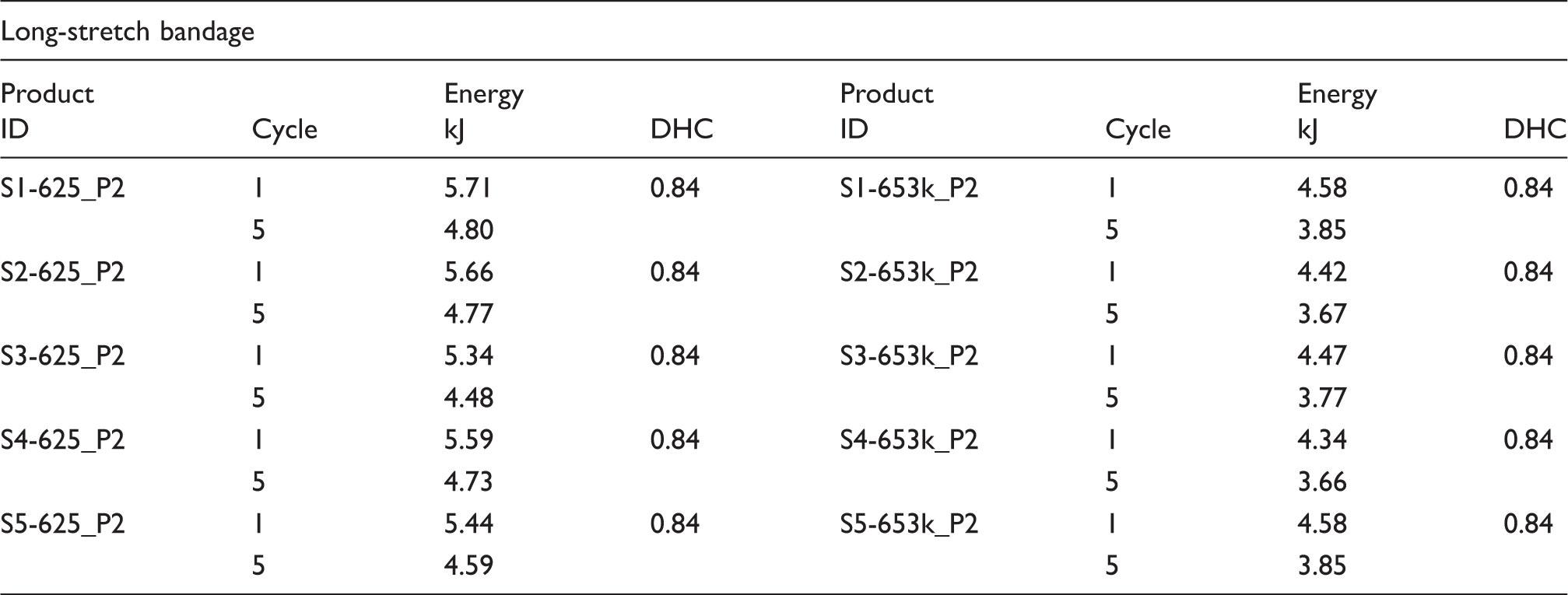
It can be expected that the DHC can become an alternative method in evaluating whether material properties may also be responsible for the extensibility variability within bandages when performed at only 30 N maximum load, as material fatigue and elasticity are mostly related to their macro-molecular structure. The DHC calculation considers the hysteresis curves of the first and fifth cycles, as depicted in Figure 12, by DHC = energy (cycle 5) / energy (cycle 1), with the energies being calculated as the integrals over the dynamic tensile hytereses.
(a) Tensile hysteresis of a long-stretch bandage. (b) Short-stretch bandage specimens.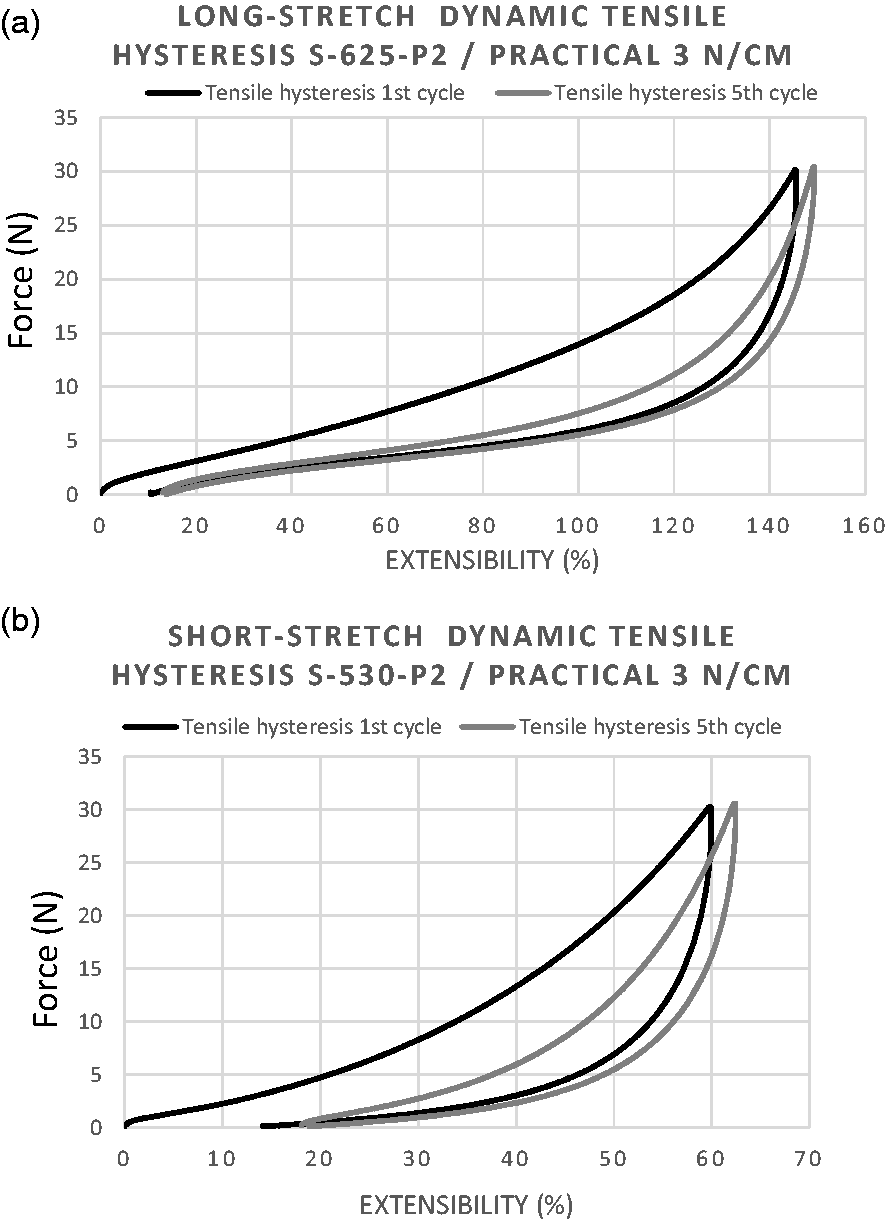
Dynamic Hysteresis Coefficient (DHC) calculation considering the energy deployed in the first and fifth cycles – long-stretch bandages
Dynamic Hysteresis Coefficient (DHC) calculation considering the energy deployed in the first and fifth cycles – short-stretch bandages
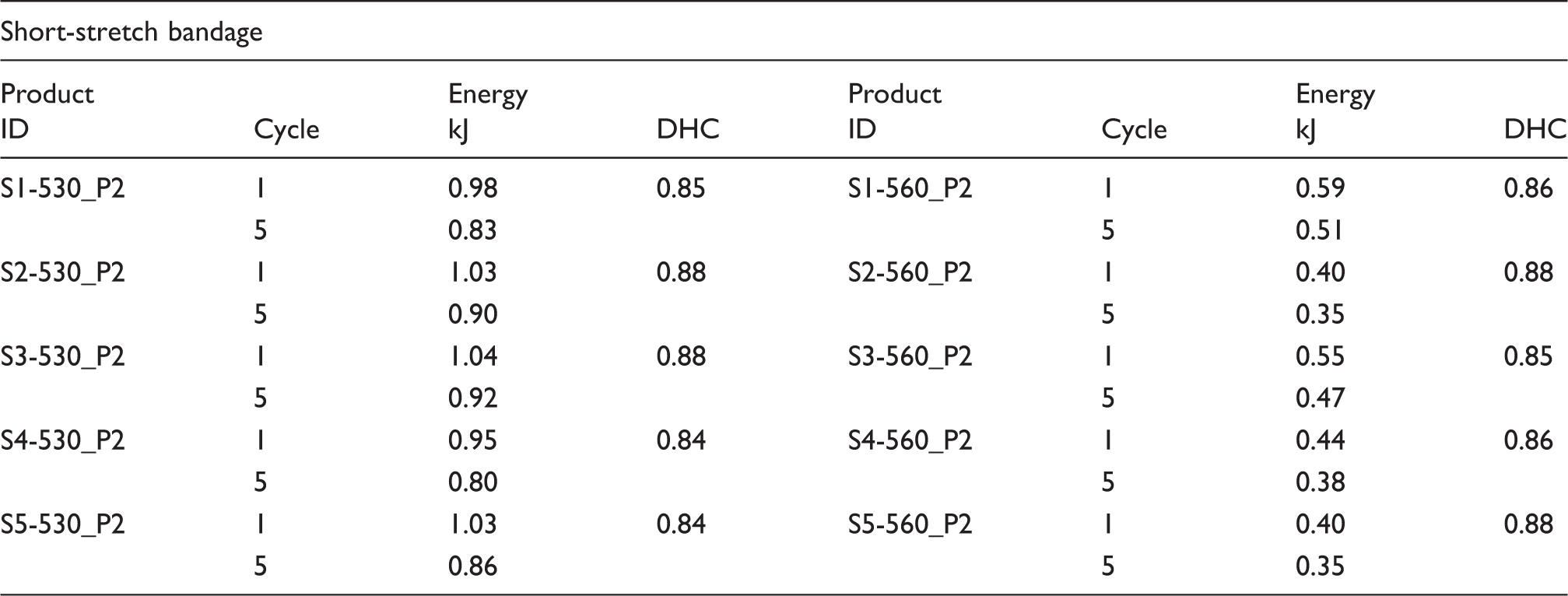
These results show clearly that the energies deployed by short- and long-stretch bandages under dynamic circumstances are not similar. This consequently implies that the material macro-molecular structure does indeed have an impact on the compression bandage effect during the therapy. Obviously, the material properties play an important role in the therapeutic pressure as the energy deployed most probably represents the permanent restoring force generated by the rubbery molecular segment of the thermoplastic polyurethane. Considering the single DHC values, it was unexpectedly observed that short-stretch bandages did not suffer from a higher fatigue in comparison to long-stretch bandages. This is also a proof that all bandages are elastic.
In summary, the extensibility variance within a bandage due to the winding process does not have a significant impact on the therapeutic effect, since the energy as well as the DHC generated by each product type (short or long stretch) were all similar within one product.
Pressure on the leg of living subjects using Picopress®
As defined in the in vivo framework, a small number of subjects were wrapped with the different samples. During the application, bandages were marked with a vertical line that served as a stretch indicator. By knowing how long the bandage was stretched during the application, it is possible to compare the interface pressure recorded from the Picopress® device and the pressure predicted according to the modified Pascal and Laplace equation.
Interface measurement with Picopress® sensor
Knowledge about the application of compression does not have a standard yet, as nurses apply bandages according to how they were taught to apply and not as recommended by the instruction of use. Heyer et al. 24 reported in a recent study that knowledge about compression bandages and their correct usage is the basis for an effective compression therapy.
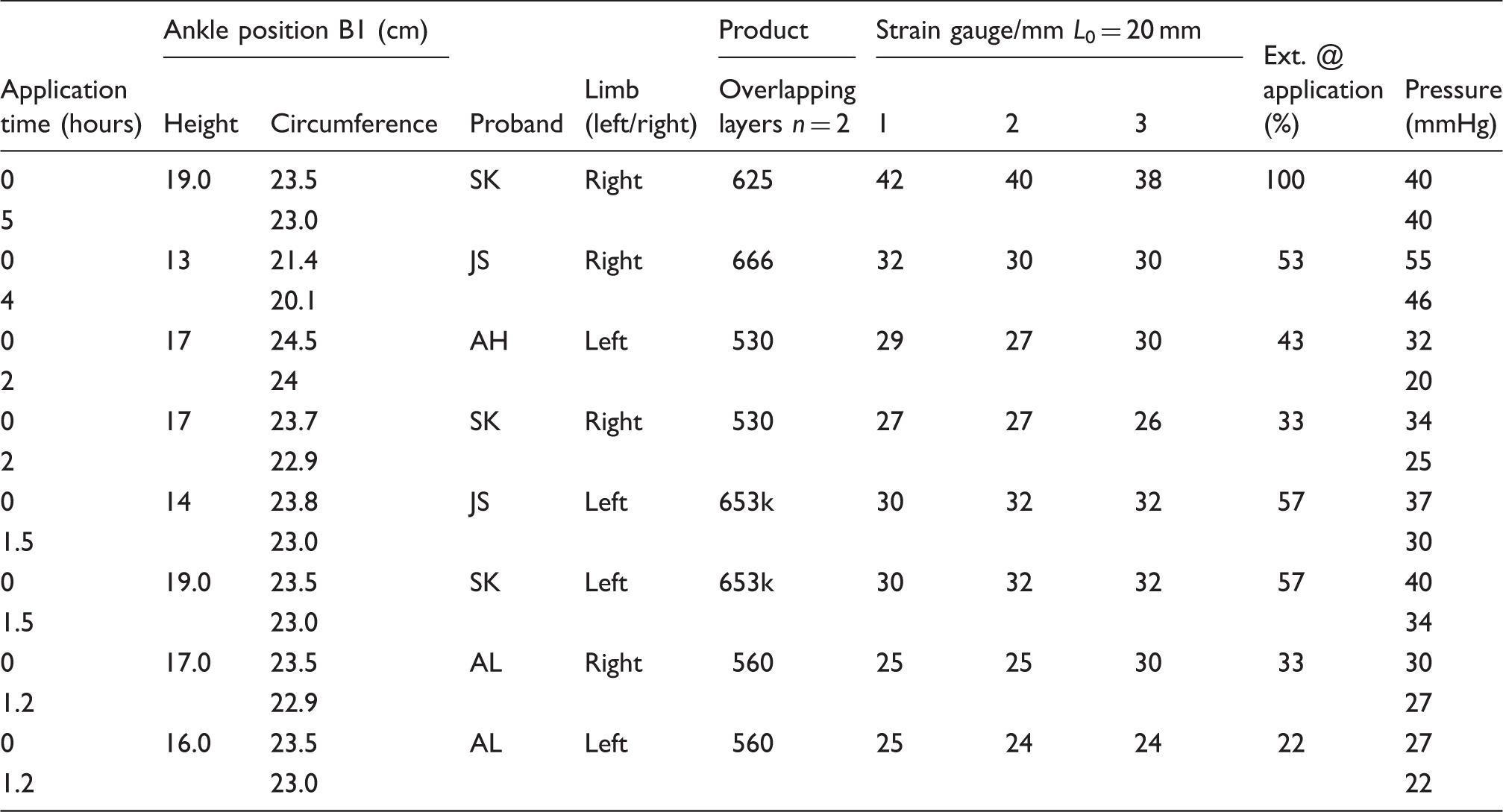
However, evaluation showed that only very few nurses can apply short- and long-stretch bandages correctly. Hence, to avoid variability in the therapeutic dosage and to ensure that the therapeutic pressure that is claimed for the treatment is reliably achieved by any nurse or user, it is regulatory recommended to prescribe the bandage elongation (extension at application) that would enable a pressure as mentioned in Table 5. This elongation at application is correlated with the application force of the bandage. By knowing this initial extension of the bandage, any nurse or user can be expected to achieve a similar pressure at the application of the compression bandage; however, some compression bandages with natural fiber material, such as product 530, may undergo a pressure drop over a period of time (Table 5), whereas synthetic fiber material-based compression bandages might be more suitable to maintain their pressure. The pressure loss in natural fiber-based compression bandages is hardly expected from the predicted pressure, as the machine does not stretch the bandage as humans do, and the stretching is controlled at a constant speed. For example, pre-testing on a tensile tester showed that the stretching speed of the bandage influences the force that normally causes the applied pressure (Figure 13). Moreover, if one considers the pressure estimation of the bandage (according to Figure 6(b)), where the pressure was more realistic at the inflexion point, there seems to be a good compromise in that the testing speed does influence the compression force predictability.
Stretching force of the bandage influenced by the testing speed.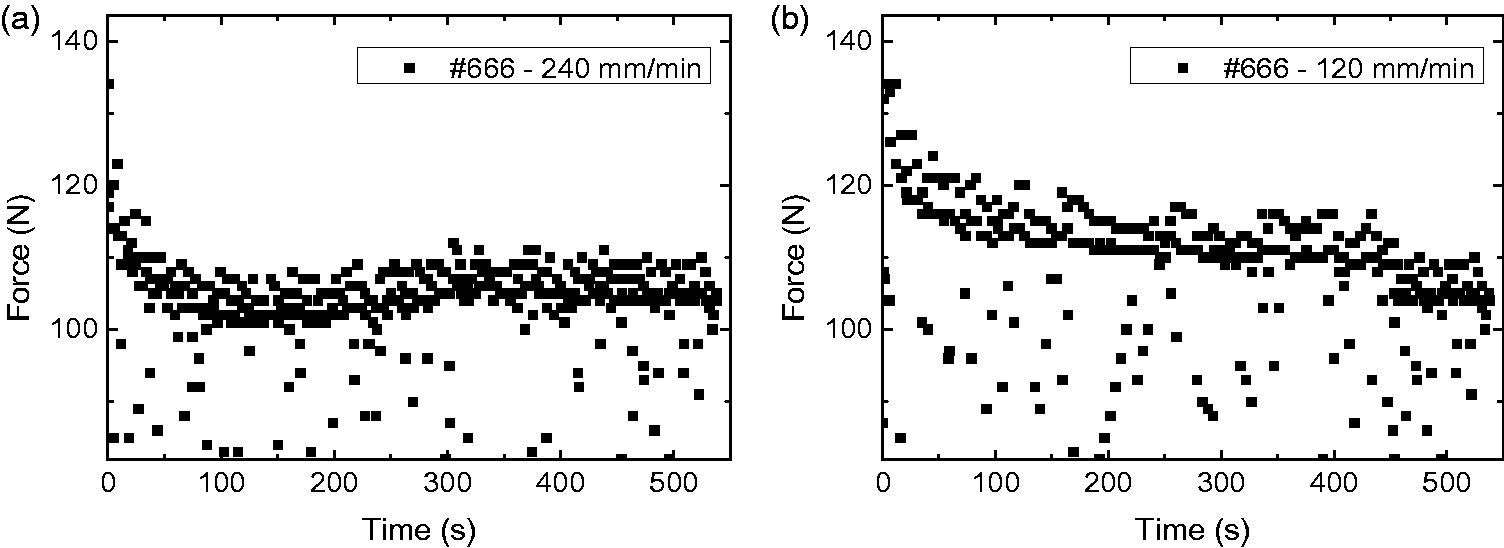
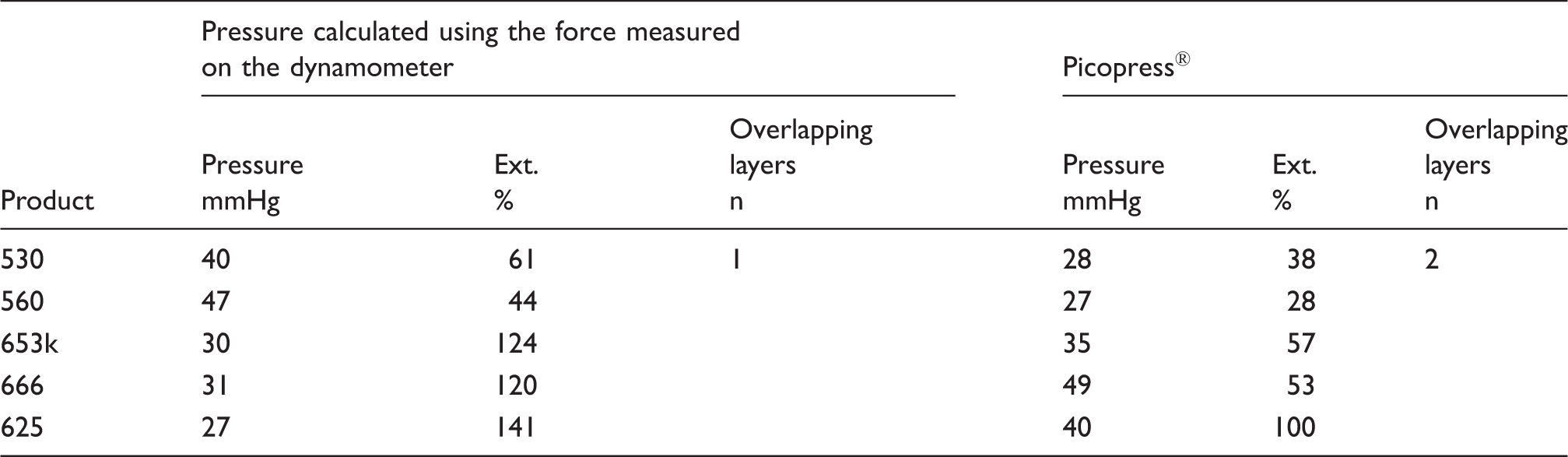
Taking into account the impact of the application speed and stretch control (Figure 13) may avoid misleading presuppositions and enable a better comparison than is shown in Table 5.
Approach of a comparison between calculated and applied pressures; Picopress values are averaged from Table 5
Discussion about the systemic error of the investigation
It may be assumed that the conversion factor (k = 4620) used in the modified equations of Pascal and Laplace to convert the primary forces acting on the bandage into medically useful information has to be adjusted in the prediction of the pressure if the material macro-molecular structure is different due to changes of the forces with time. Observation of the DHCs showed that bandages with naturally and synthetically occurring material significantly maintain their elasticity when submitted to a loading force of about 30 N even after five cycles of dynamic testing. Hence, no matter which type of bandage is used for compression, in a lower loading range, such as maximum 30 N, the bandages have very high tolerability of the variation of the applied forces and therefore disregard or reduce the impact of the systemic error on the pressure prediction. It would be interesting to conduct a follow-up study where the same extension is set for both – which is only possible by firstly performing the study on different probands to take into account the broad range of forces applied by different people during bandaging, the calculation of the pressure using the equation and the pressure measured with a transducer on subjects.
Conclusion
The prediction of an applied pressure according to the modified Young–Laplace equation is realistic for both cotton-based and elastomer-based bandages. The main new findings are the utilization of the specimen's stretched length for the prediction of the interface pressure in the modified equation, in contrast to the commonly found equation in the literature that uses a randomly picked human subject ankle's circumference to predict the pressure. In addition, it is also new to use the inflexion point as the point at which the most relevant force for the modified equation is found. These findings have not been mentioned in the literature.
Our study also showed that the primary physical component used for the calculation of the pressure – the force – is most probably influenced by the speed at which the bandage is strained during the testing on a dynamometer (Figure 13); this implies the importance of the pressure prediction using any force measured around the inflexion point, in the case in which bandage is tested at a speed of 500 mm/min or similar. According to this study, using a dynamometer to assess the force for the pressure prediction would be the most appropriate way, as the result showed that the variability that was observed in specimens tested on the dynamometer was also observed while testing on the automatic controlled extensibility test table (Figure 11). Extension variability within a bandage may not be primarily caused by the material macro-molecular structure, but most probably by the bandage winding process during manufacturing. Nevertheless, the differentiation between elastomer-based and natural fiber-based compression material – the macro-molecular structure – can clearly be seen on the extensibility axis of Figure 12.
Furthermore, the findings also showed that testing bandages at a maximal load of 3 N/cm enables consistent results, especially in the observation of the variability of the material physical properties, such as the DHC, which was quite similar for both cotton-based and elastomer-based material. The hypothesis that the macro-molecular structure could have an impact on the pressure calculation considering the conversion factor k, which needs to be adapted to the type of material (natural, elastomer), was found to be false. However, the impact of the macro-molecular structure on the compression material could be seen in the energy deployment results (cf. Tables 3 and 4).
The effectiveness of compression therapy depends on the pressure that is applied, and current clinical treatments do not measure the applied interface pressure. Rather, they calculate an initial pressure based on the modified Pascal and Laplace equation. Therefore, it is recommended that the stress–strain test of bandages in the laboratory is performed at lower speed, which will depict more consistent results that will be very useful for the decision as to which pressure should be applied for the treatment of any venous or lymphatic disorder.
Footnotes
Declaration of conflicting interests
The authors declared the conflicting interests for the research, authorship, and/or publication of this article: KOB is the original manufacturer of a few of the products that are being studied.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.